Embed Size (px)
Citation preview
OBESITY AND SCREENING FOR BIRTH DEFECTS
E. Rebecca Pschirrer, MD, MPH
Dartmouth Medical School
Maternal Fetal Medicine
Objectives
Review risks of obesity and congenital anomalies
Impact of BMI on screening
Review screening options
Best choices for obese patients
Background
2 – 3% live births affected by structural anomaly2.25% cardiac defect1 per 1500 neural tube defect
Majority of birth defects occur in euploid fetuses
Obesity Epidemic
2003-2004 National Health and Nutrition Examination Survey (NHANES)
Women 20 – 39 years old28.9 % BMI ≥ 30 kg/m2
8.0 % BMI ≥ 40 kg/m2
1999
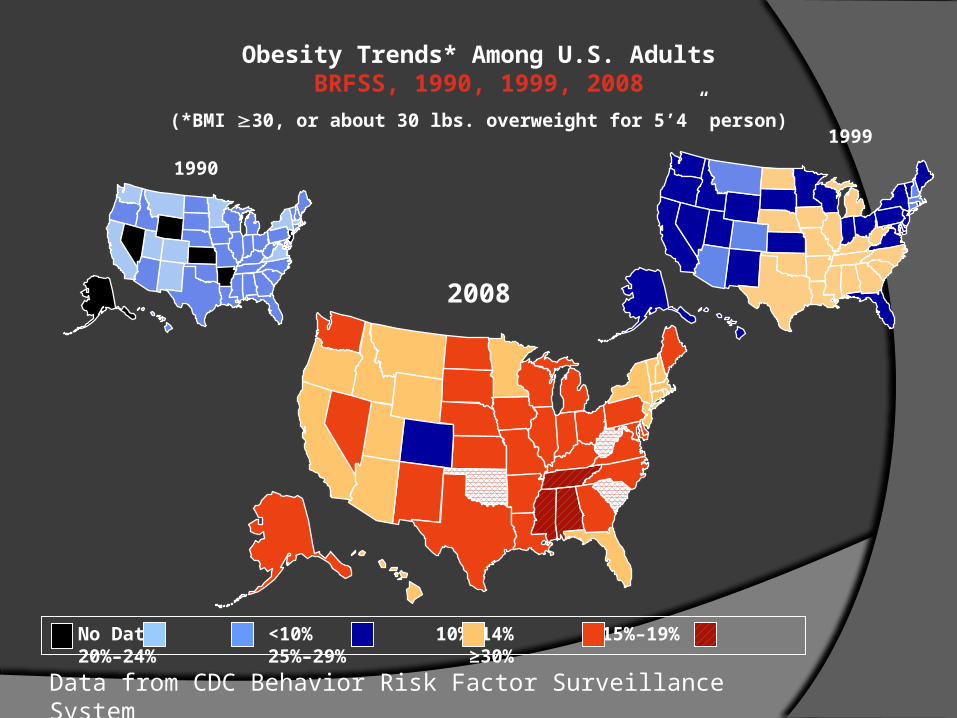
Obesity Trends* Among U.S. AdultsBRFSS, 1990, 1999, 2008
(*BMI 30, or about 30 lbs. overweight for 5’4” person)
2008
1990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Data from CDC Behavior Risk Factor Surveillance System
Congenital Anomalies
Overweight & obesity associated with risk structural anomaliesNeural tube defects
Cardiovascular anomalies
Orofacial clefting
Other congenital anomalies
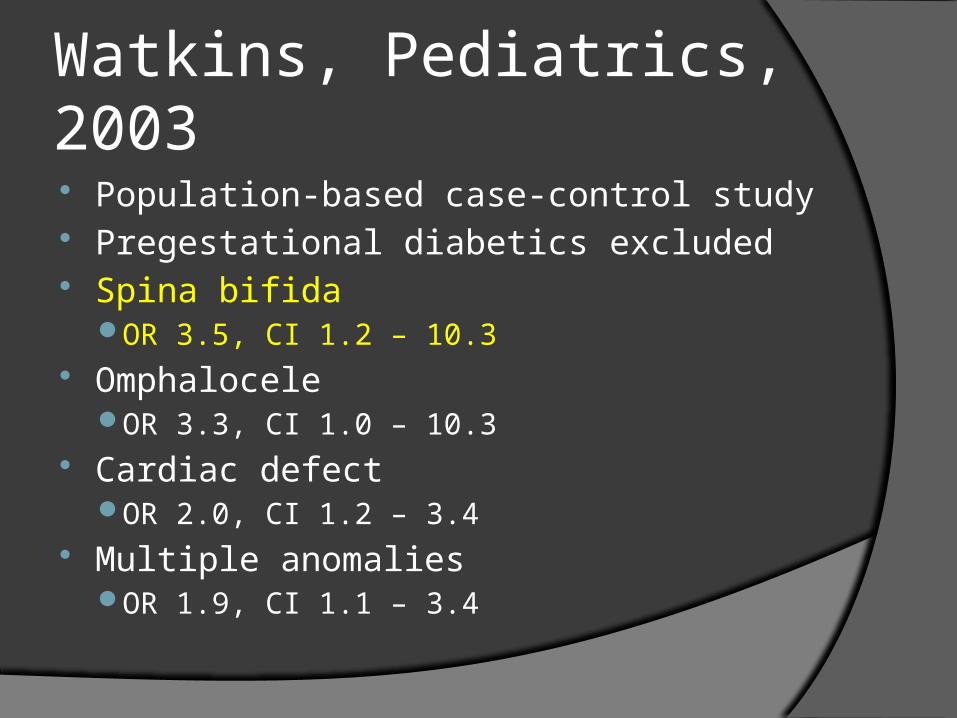
Watkins, Pediatrics, 2003 Population-based case-control study Pregestational diabetics excluded Spina bifida
OR 3.5, CI 1.2 – 10.3 Omphalocele
OR 3.3, CI 1.0 – 10.3 Cardiac defect
OR 2.0, CI 1.2 – 3.4 Multiple anomalies
OR 1.9, CI 1.1 – 3.4
Watkins, Pediatrics, 2003 Population-based case-control study Pregestational diabetics excluded Spina bifida
OR 3.5, CI 1.2 – 10.3 Omphalocele
OR 3.3, CI 1.0 – 10.3 Cardiac defect
OR 2.0, CI 1.2 – 3.4 Multiple anomalies
OR 1.9, CI 1.1 – 3.4
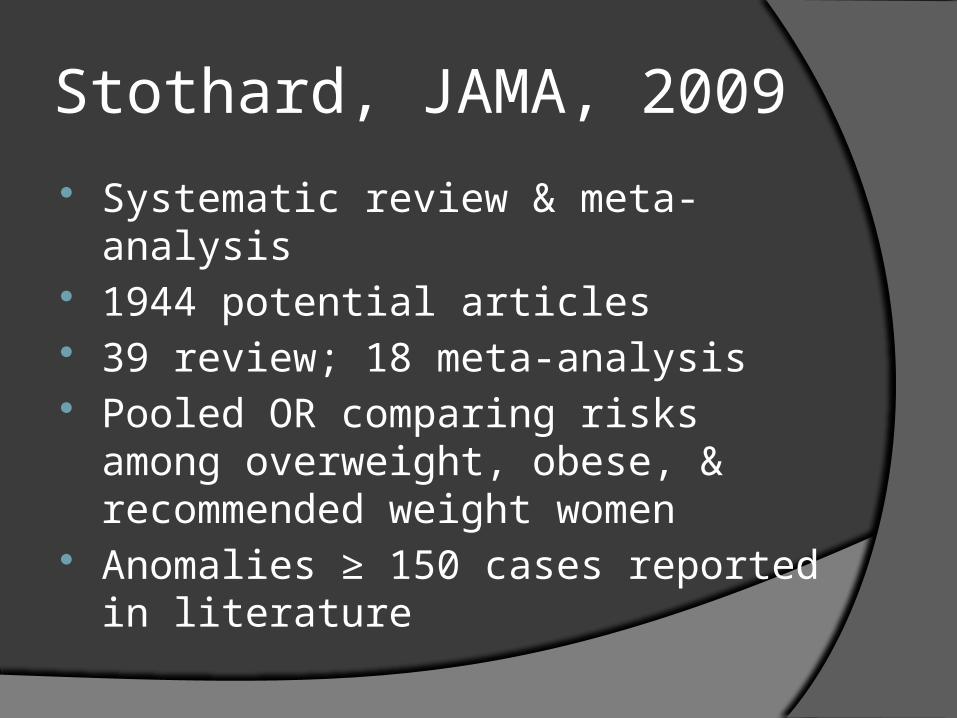
Stothard, JAMA, 2009
Systematic review & meta-analysis 1944 potential articles 39 review; 18 meta-analysis Pooled OR comparing risks among
overweight, obese, & recommended weight women
Anomalies ≥ 150 cases reported in literature
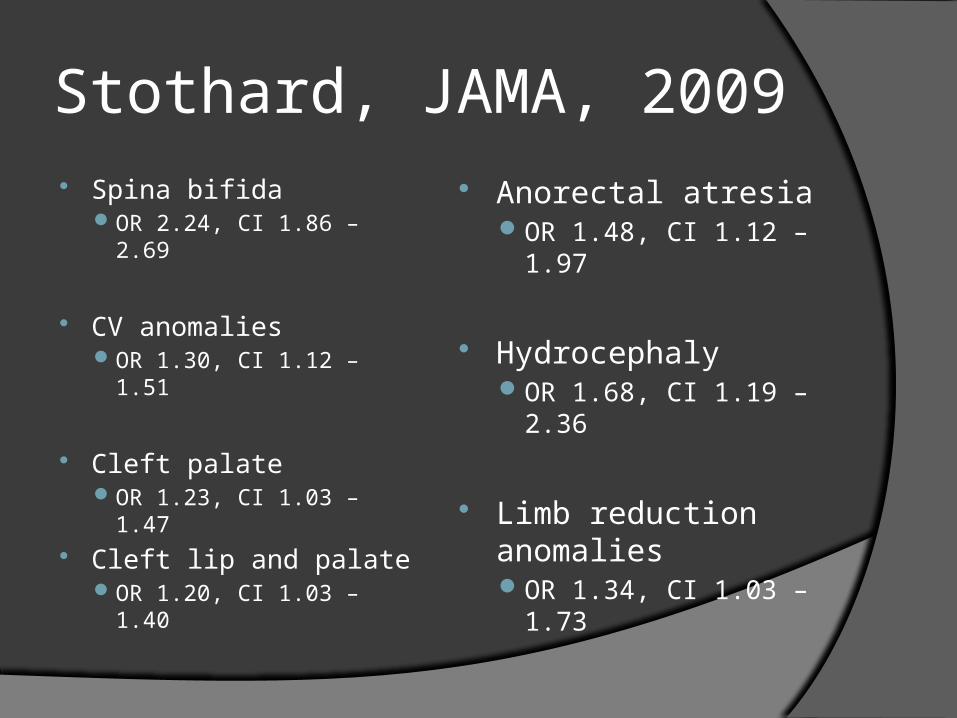
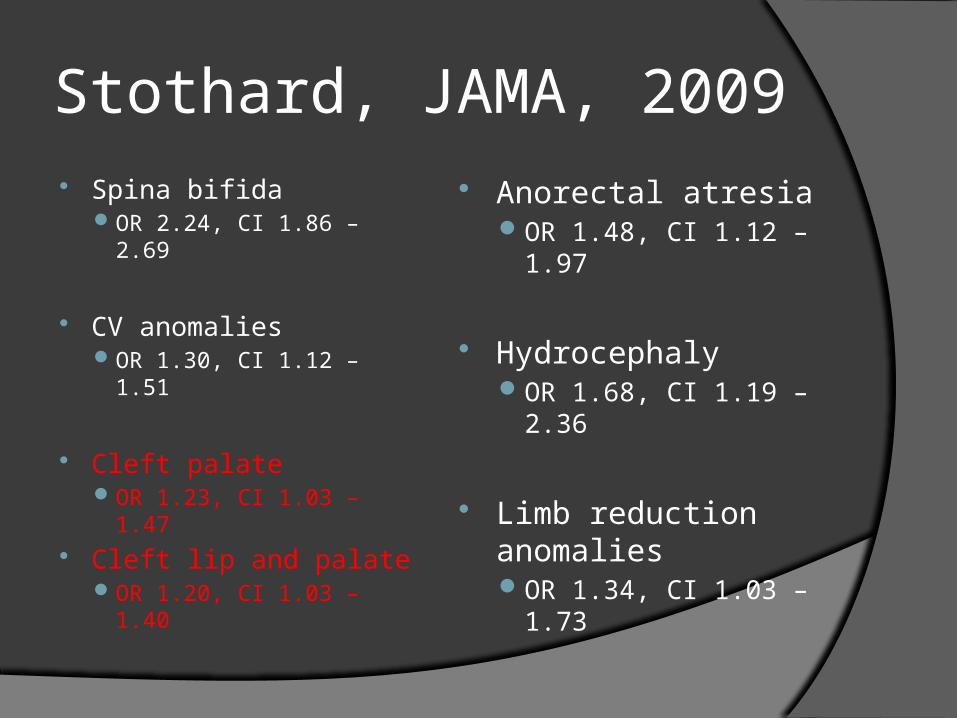
Stothard, JAMA, 2009 Spina bifida
OR 2.24, CI 1.86 – 2.69
CV anomalies OR 1.30, CI 1.12 – 1.51
Cleft palate OR 1.23, CI 1.03 – 1.47
Cleft lip and palate OR 1.20, CI 1.03 – 1.40
Anorectal atresia OR 1.48, CI 1.12 –
1.97
Hydrocephaly OR 1.68, CI 1.19 –
2.36
Limb reduction anomalies OR 1.34, CI 1.03 –
1.73
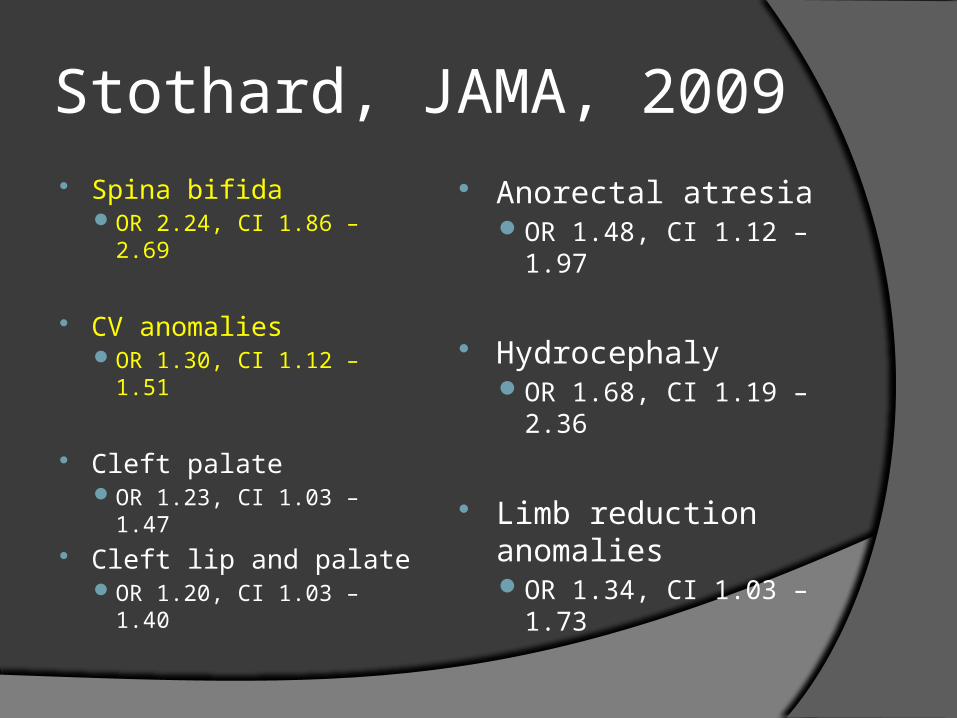
Stothard, JAMA, 2009 Spina bifida
OR 2.24, CI 1.86 – 2.69
CV anomalies OR 1.30, CI 1.12 – 1.51
Cleft palate OR 1.23, CI 1.03 – 1.47
Cleft lip and palate OR 1.20, CI 1.03 – 1.40
Anorectal atresia OR 1.48, CI 1.12 –
1.97
Hydrocephaly OR 1.68, CI 1.19 –
2.36
Limb reduction anomalies OR 1.34, CI 1.03 –
1.73
Stothard, JAMA, 2009 Spina bifida
OR 2.24, CI 1.86 – 2.69
CV anomalies OR 1.30, CI 1.12 – 1.51
Cleft palate OR 1.23, CI 1.03 – 1.47
Cleft lip and palate OR 1.20, CI 1.03 – 1.40
Anorectal atresia OR 1.48, CI 1.12 –
1.97
Hydrocephaly OR 1.68, CI 1.19 –
2.36
Limb reduction anomalies OR 1.34, CI 1.03 –
1.73
Stothard, JAMA, 2009
Congenital anomalies not analyzed in meta-analysis:Risk of omphalocele and risk of multiple
congenital anomalies significantly higher among obese women
Not included in meta-analysis due to low power / less than 150 cases reported
Malformation Etiology
Undiagnosed or unrecognized diabetes Altered metabolism ( insulin,
triglycerides, uric acid, estrogen)Increased insulin resistance Fuel mediated teratogenesis
Nutritional deficits Low folate levels
Supplementation not found to decrease risk
Challenges of Diagnosis
Poor sensitivity of ultrasound
“Ultrasound was limited by maternal habitus”
Spine & heart views particularly challenging in obese patients
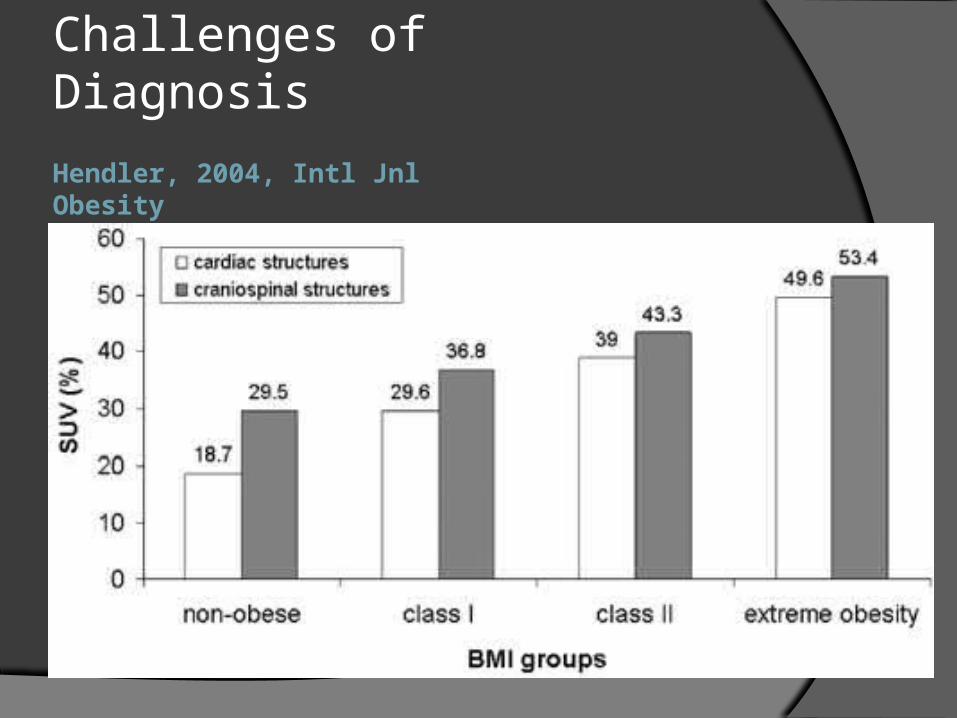
Hendler, 2004, Intl Jnl Obesity
Challenges of Diagnosis
Dashe, J Ult Med, 2009
Challenges of Diagnosis
Retrospective cohort, singleton pregnancies, standard second trimester ultrasound exam (AIUM)
18 – 23+6 weeks EGA 10 components analyzed for adequacy
of visualizationCerebral ventricles, posterior fossa, midline
face, 4-chamber heart, spine, ventral wall, umbilical cord, stomach, kidneys, bladder
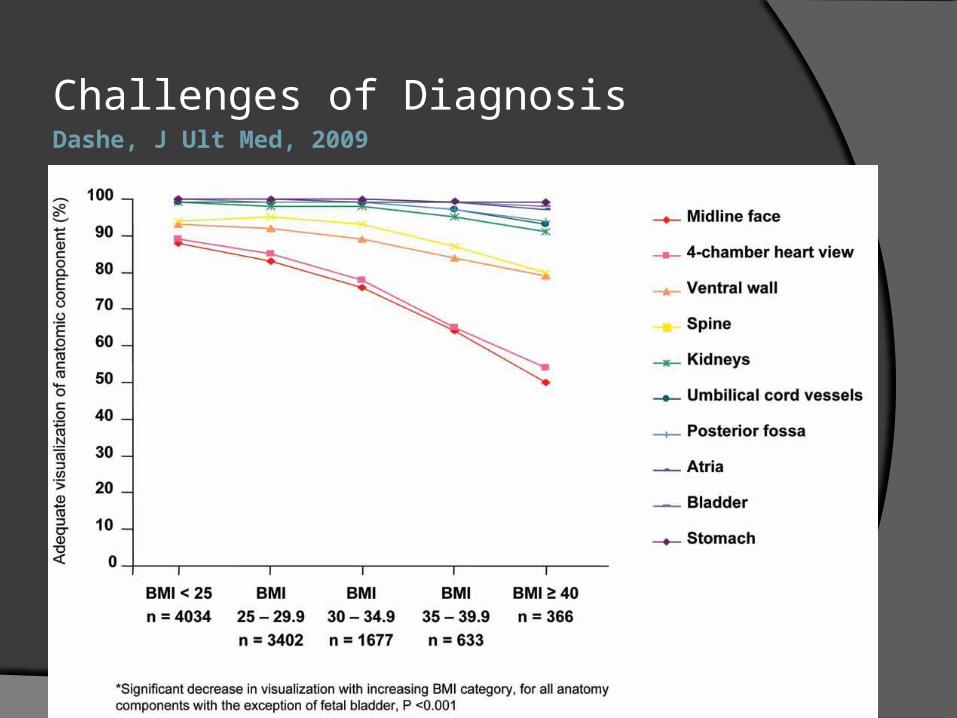
Dashe, J Ult Med, 2009
Challenges of Diagnosis
Exclusion criteria: indication for targeted ultrasoundPregestational DM, teratogen exposure, family
history, increased risk on screening 10,112 women 2676 (26%) obese Results: decrease in ability to adequately
visualize fetal anatomy with increasing maternal BMIClass 1 57%, class 2 41%, class 3 30%
Dashe, J Ult Med, 2009
Challenges of Diagnosis
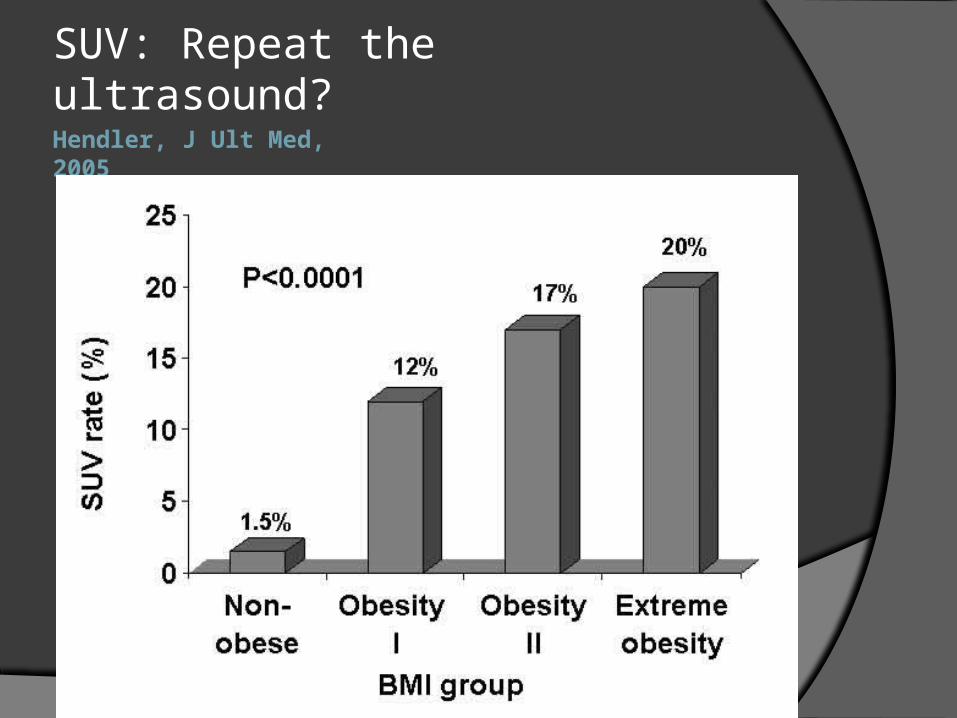
Hendler, J Ult Med, 2005
SUV: Repeat the ultrasound?
Dashe, Obstet Gyn, 2009
Retrospective cohort, 5 year period 10,112 standard u/s 1,098 targeted u/s
79 fetuses with undiagnosed anomalies, 0.7%
Decreased detection of anomalies with increasing BMI with either standard or targeted ultrasound Detection even less in pregnancies complicated by
pregestational diabetes38% vs. 88%, p < 0.001
Challenges of Diagnosis:
Decreased Detection
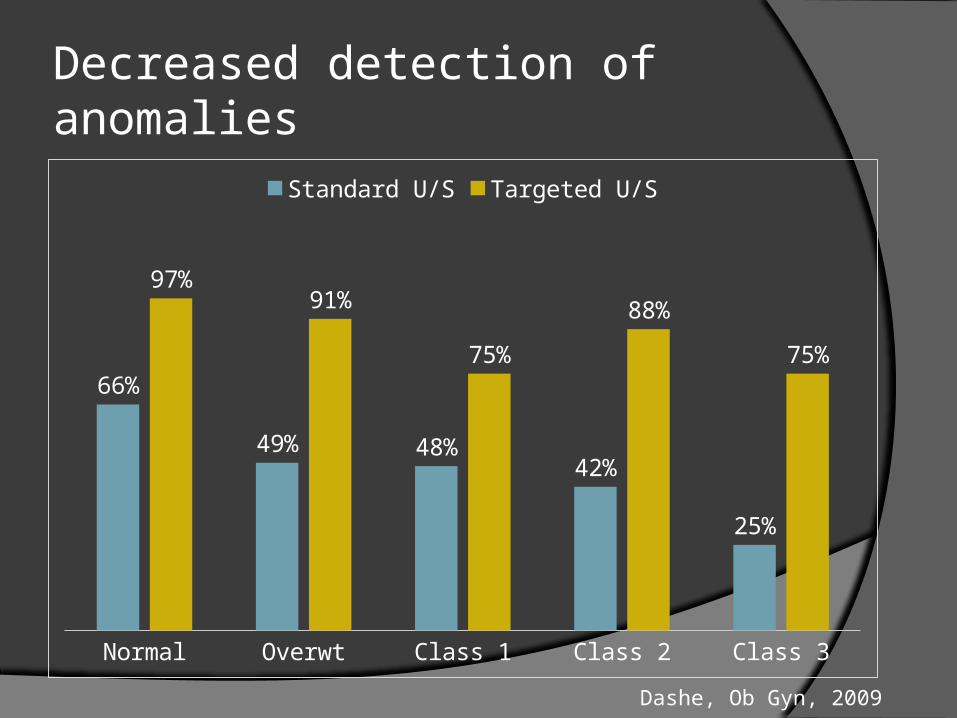
Decreased detection of anomalies
Normal Overwt Class 1 Class 2 Class 3
66%
49% 48%42%
25%
97%91%
75%
88%
75%
Standard U/S Targeted U/S
Dashe, Ob Gyn, 2009
Dashe, Obstet Gyn, 2009
Broad range of anomalies not detectedStraight forward: endocardial cushion defectChallenging: micrognathiaNot detectable at 18 – 24 wks: GI atresiaNot detectable: absent ear canal
Residual risk after normal U/S:0.4% normal BMI1% BMI ≥ 30
Challenges of Diagnosis: Residual Risk
What to do?
Image enhancing modalitiesHarmonic imagingCompound imagingSpeckle reduction filters
Approach through least SQ adiposePeriumbilical, suprapubic, R / L iliac fossae
Endovaginal ultrasound
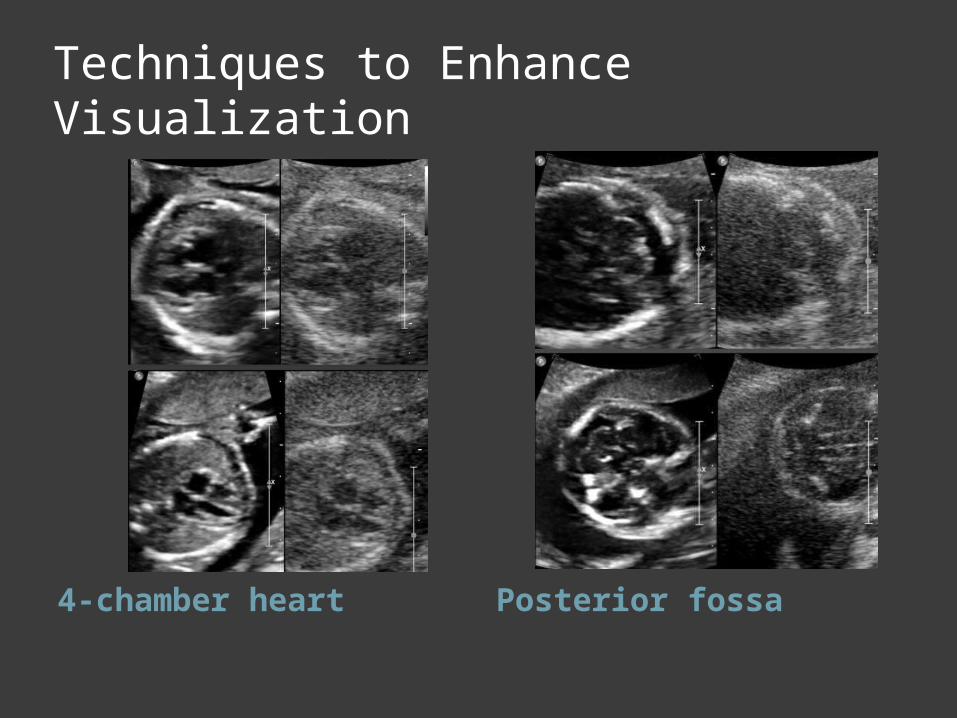
Techniques to Enhance Visualization
4-chamber heart Posterior fossa
First trimester anatomy?
11 – 13+6 weeks Endovaginal & abdominal u/s Structural malformation detection rates
range 16 – 84% Possible 2 stage process Not ready for prime time
Research re: feasibility, outcomesCost benefit analysis
Aneuploidy Screening Tests Maternal age Quad Screen First Trimester Screen Integrated Screen Sequential Screen Serum Integrated Screen
Weight Correction of Serum Analytes Adjust analyte concentration or MoMs
for maternal weight Placental- or fetal-derived markers more
diluted in heavier women due to larger blood volume
Conversely, more concentrated in lighter women because of smaller blood volume
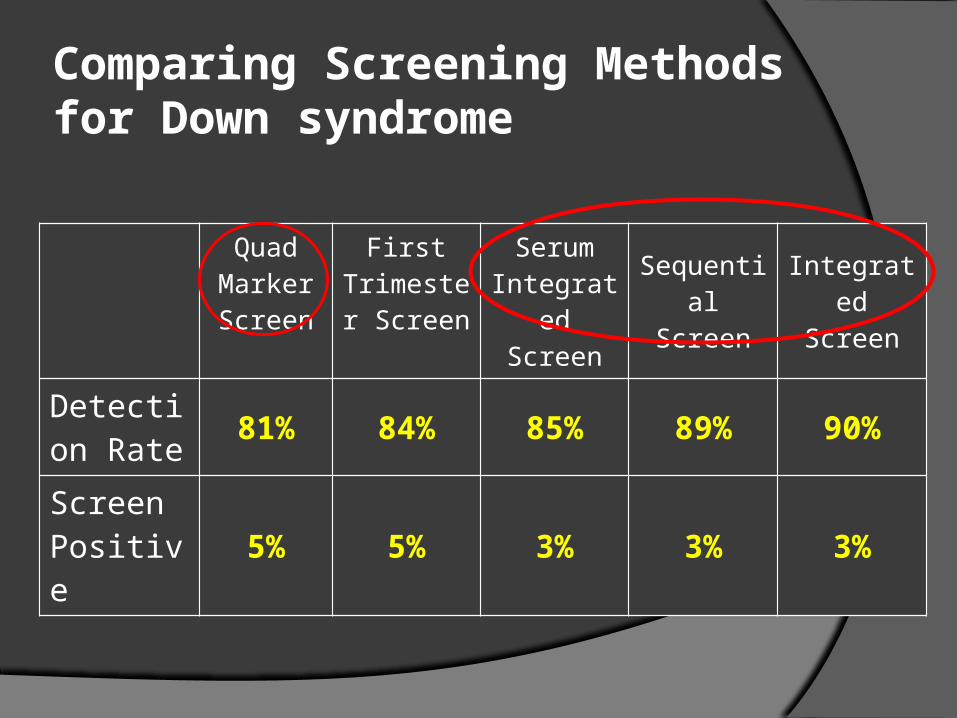
Comparing Screening Methods for Down syndrome
Quad Marker Screen
First Trimester Screen
Serum Integrated
Screen
SequentialScreen
IntegratedScreen
Detection Rate 81% 84% 85% 89% 90%
Screen Positive 5% 5% 3% 3% 3%
Conclusions
Screening for birth defects & aneuploidy is a significant challenge in obese women
Reduction in detection rate of congenital anomalies
Discussion & documentation of limitations with patients
Document BMI in ultrasound reports
Thank you.