Embed Size (px)
Citation preview

DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
httpwwwneurologyorgcontent7811796fullhtmllocated on the World Wide Web at
The online version of this article along with updated information and services is
Enterprises Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2012 by AAN
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology
Early EEG correlates of neuronal injuryafter brain anoxia
Andrea O Rossetti MDEmmanuel Carrera MDMauro Oddo MD
ABSTRACT
Objectives EEG and serum neuron-specific enolase (NSE) are used for outcome prognosticationin patients with postanoxic coma however it is unclear if EEG abnormalities reflect transientneuronal dysfunction or neuronal death To assess this question EEG abnormalities were corre-lated with NSE Moreover NSE cutoff values and hypothermic EEG features related with pooroutcome were explored
Methods In a prospective cohort of 61 adults treated with therapeutic hypothermia (TH) aftercardiac arrest (CA) multichannel EEG recorded during TH was assessed for background reactiv-ity and continuity presence of epileptiform transients and correlated with serum NSE collectedat 24ndash48 hours after CA Demographic clinical and functional outcome data (at 3 months) werecollected and integrated in the analyses
Results In-hospital mortality was 41 and 82 of survivors had good neurologic outcome at 3months Serum NSE and EEG findings were strongly correlated (Spearman rho 045 p
0001) Median NSE peak values were higher in patients with unreactive EEG background (p
0001) and discontinuous patterns (p 0001) While all subjects with nonreactive EEG died 5survivors (3 with good outcome) had NSE levels 33 gL
Conclusion The correlation between EEG during TH and serum NSE levels supports the hypoth-esis that early EEG alterations reflect permanent neuronal damage Furthermore this study con-firms that absent EEG background reactivity and presence of epileptiform transients are robustpredictors of poor outcome after CA and that survival with good neurologic recovery is possibledespite serum NSE levels 33 gL This underscores the importance of multimodal assess-ments in this setting Neurologyreg 201278796ndash802
GLOSSARYAAN American Academy of Neurology CA cardiac arrest CPC Cerebral Performance Categories FPR false-positiverate NSE neuron-specific enolase SIRPIDS stimulus-induced rhythmic periodic or irritative discharges SSEP so-matosensory evoked potentials TH therapeutic hypothermia VF ventricular fibrillation
Therapeutic hypothermia (TH) improves outcome in comatose survivors of cardiac arrest(CA) but may also alter prognostic clinical features especially motor response to painfulstimuli1ndash3 In this context EEG may represent an important tool to improve prognostication inpostanoxic coma While recent works emphasized the importance of EEG background reactiv-ity following return to normothermia3ndash5 prognostic values of recordings performed duringhypothermia have received far less attention Two studies addressed quantitative EEG featuresand identified burst-suppression ratio presence of status epilepticus and entropy characteris-tics as promising prognosticators67 while our group reported lack of visually assessed EEGbackground reactivity as a robust predictor of poor outcome in 34 patients8 Nevertheless theseobservations did not address the neuronal correlates subtending EEG changes
Neuron-specific enolase (NSE) is a 780-kDa intracellular enzyme found in neurons andother cells of neuroectodermal origin9 Elevation of serum NSE 1ndash3 days after CA is regardedas a severity marker of postanoxic neuronal injury it has been shown to be released in the
From the Departments of Clinical Neurosciences (AOR EC) and Intensive Care Medicine (MO) University Hospital and Faculty of Biologyand Medicine Lausanne Switzerland
Disclosure Author disclosures are provided at the end of the article
Editorial page 774
Correspondence amp reprintrequests to Dr Rossettiandrearossettichuvch
796 Copyright copy 2012 by AAN Enterprises Inc
serum of patients after CA with a half-life ofabout 24 hours1011 The American Academyof Neurology (AAN) practice parameterswhich considered studies from the prehypo-thermia era suggest a cutoff of 33 gL atdays 1ndash3 after CA as a robust predictor forpoor outcome12
Multichannel EEG and NSE have beeninvestigated separately in patients withhypoxic-ischemic encephalopathy to ourknowledge however no studies have specif-ically addressed a potential correlation be-tween these variables In the present studywe hypothesized that abnormal EEG find-ings reflect the degree of postanoxic neuro-nal injury and investigated whether earlyEEG abnormalities recorded during THcorrelate with serum NSE levels sampled24 ndash 48 hours after CA
METHODS Patients We prospectively studied a cohort ofconsecutive comatose adults admitted between December2009 and April 2011 to the Department of Intensive CareMedicine of our hospital after successful resuscitation fromCA and treated with TH according to our local protocol13
All patients were resuscitated according to recent recommen-dations14 and treated with mild TH to 33degC for 24 hoursusing ice packs and IV ice-cold fluids for the rapid inductionof cooling and a surface cooling device (Arctic Sun SystemMedivance Louisville CO) for the maintenance of TH In astandardized approach midazolam (01 mgkgh) and fenta-nyl (15 gkgh) were given for sedation-analgesia and ve-curonium (01 mgkg boluses) was administered to controlshivering Patients diagnosed as being in brain death uponrewarming or without signs of EEG activity (ldquoflat record-ingrdquo) were not included in the study
Standard protocol approvals registrations and patientconsents This study was approved by our Institutional ReviewBoard patient consent was not required as this was a purelyobservational study and all procedures were part of standard pa-tient care
EEG data Video-EEGs (Viasys Neurocare Madison WI)were performed during TH with 9 to 21 electrodes according tothe international 10ndash20 system EEG was continuously recordedfor 24ndash48 hours8 or due to practical limitations for 20ndash30minutes Background reactivity was tested on-site as detailed inour previous study8 using repetitive auditory visual and nocice-ptive stimulations at least 6 hours after CA All recordings werevisually interpreted by 2 EEG-certified neurologists blinded toNSE levels EEG findings were categorized according to thepresence or absence of the following 3 variables 1) EEG back-ground reactivity defined as an activity 10 V (regardless offrequency) and if the background showed presence of any clearand reproducible change in amplitude or frequency upon stimula-tion excluding stimulus-induced rhythmic periodic or irritativedischarges (SIRPIDS) and muscle artifacts 2) spontaneous discon-tinuous (burst-suppression) pattern defined as an EEG background
interrupted by flat periods 3) epileptiform activity defined as any
periodic or rhythmic spikes sharp waves spike-waves or rhythmic
waves evolving in amplitude frequency or field38
NSE Serum NSE was sampled at 24 and 48 hours after CA To
avoid hemolysis and false-positive test results samples for NSE
measurement were manually handled and transported to central
laboratory For accurate determination of NSE levels an auto-
mated immunofluorescent assay (Thermo Scientific Brahms
NSE Kryptorreg Immunoassay) was used
Neurologic assessment antiepileptic therapy andtreatment withdrawal At least 36 hours after CA after re-
warming at a core temperature 35degC and off sedation repeated
neurologic examination standard (20ndash30 minutes) EEG with
the above mentioned stimulations and cortical somatosensory
evoked potentials (SSEP) were performed Patients with EEG
evidence of status epilepticus were treated with IV antiepilep-
tic drugs discontinued if no clinical improvement was noted
after at least 72 hours While physicians were not blinded to
these results hypothermic EEG findings and NSE values
were not used for the interdisciplinary decision on withdrawal
of intensive care support This has been described previously3
and is based on a multimodal approach including at least 2 of
the following (assessed in normothermia at least 48 ndash72 hours
after CA) incomplete recovery of brainstem reflexes early
myoclonus unreactive normothermic EEG and bilaterally
absent cortical SSEP
Outcome assessment Functional neurologic outcome was
assessed at 3 months through a phone interview by trained per-
sonnel of the EEG unit who had no access to study data and
categorized according to the Glasgow-Pittsburgh Cerebral Per-
formance Categories (CPC) (1 good recovery 2 moderate
disability 3 severe disability with dependency for daily life
activity 4 vegetative state and 5 death15) in line with the
vast majority of studies on this topic outcome was dichotomized
as good (CPC 1ndash2) vs poor (CPC 3ndash5)
Data collection All variables were collected prospectively
Baseline demographics included initial arrest rhythm (ventricu-
lar fibrillation [VF] vs non-VF including asystole and pulseless
electrical activity) and duration of CA (ie the time from col-
lapse to return of spontaneous circulation) Hypothermic EEG
findings included background reactivity burst-suppression pat-
tern and epileptiform activity as described previously Serum
values of NSE at 24 and 48 hours were recorded
Statistical analysis Wilcoxon rank sum Student t and 2
tests were used as needed to compare groups and the Spearman
rank test was used to examine the correlation between EEG find-
ings and NSE For this purpose according to EEG findings dur-
ing TH (reactive vs unreactive background continuous vs
discontinuous background presence vs absence of epileptiform
transients) an EEG score was given to each patient with a min-
imum of 0 and a maximum of 3 For each patient the peak
serum NSE value was used for the correlation Significance was
assumed at p 005 unless corrected after Bonferroni in cases of
multiple comparisons Calculations were performed with the
Stata software version 9 (College Station TX)
RESULTS Patients and outcome During the studyperiod 80 consecutive patients were treated withTH after CA 18 of them did not have EEG dur-
Neurology 78 March 13 2012 797
ing TH and 1 lacked NSE data Table 1 illustratesdemographic clinical characteristics and the out-come of the remaining 61 subjects included in thepresent analysis 23 of them were part of a previ-ously published series8 which did not addressNSE In the majority of patients CA was due toVF In-hospital mortality was 2561 (41) and2834 (82) survivors assessed at 3 monthsreached a good neurologic outcome (CPC 1ndash2)while 6 had CPC 3 and 2 additional patients diedIn-hospital mortality of excluded patients did not
differ from that of the studied group (818 vs 2561 p 043 2)
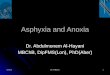
Correlation between EEG and NSE Considering sig-nificance conservatively at p 0016 (3 compari-sons) median NSE peak values were higher inpatients with unreactive EEG background (93 vs 18gL p 0001 Wilcoxon) and discontinuous(burst-suppression) patterns (633 vs 197 gL p 0001 Wilcoxon) In contrast only some trendtoward higher serum NSE levels in patients with epilep-tiform discharges was found (295 vs 239 gL p 0229 Wilcoxon) (figure) For each patient we alsoanalyzed the relationship between NSE and EEGfindings using the 3 main EEG abnormalities addedtogether to obtain an EEG sum score a strong corre-lation was found between NSE and EEG findings(Spearman rho 045 p 0001)
EEG features In the 61 included patients EEG dur-ing hypothermia was initiated after mean of 154hours (SD 58 hours) following CA During TH29 patients had a continuous EEG monitoring and32 were assessed with routine EEG HypothermicEEG features NSE values and normothermic clini-cal and electrophysiologic variables are given accord-ing to the functional outcome assessed at 3 monthsin table 2 Occurrence of abnormal EEG findingsduring TH differed clearly between the 2 outcomegroups (p 0001 Wilcoxon rank-sum) Of note
Table 1 Characteristics of 61 patients treatedafter cardiac arrest with EEGrecorded during hypothermia andserum NSE values
Demographics Values
Age y mean (SD) 637 (122)
Female n () 18 (30)
Cardiologic variables
Non VF cardiac arrest n () 21 (34)
Time to ROSC mean (SD) 227 (139)
Outcome
In-hospital mortality n () 2561 (41)
CPC 1ndash2 at 3 months n () 2861 (46)
Abbreviations CPC Cerebral Performance CategoriesNSE neuron-specific enolase ROSC return of sponta-neous circulation VF ventricular fibrillation
Figure Associations between serum neuron-specific enolase (NSE) and EEG duringtherapeutic hypothermia
Box plots represent serum NSE values (in gL y-axis) stratified according to EEG findings including background reactiv-ity background continuity and epileptiform activity Box plots represent median (horizontal lines) and 25thndash75th percen-tiles bars represent 10thndash90th percentiles
798 Neurology 78 March 13 2012
all patients with epileptiform transients also had anonreactive EEG background Two of 23 (9) sub-jects without EEG reactivity during TH recoveredreactivity after rewarming however both of themdied despite intensive care support for at least 5 addi-tional days While in patients who had a continuousmonitoring EEG recording was started earlier thanin those who had routine EEG (135 hours vs 171hours p 0015 t test) assessment of EEG reactiv-ity was performed at least 6 hours after CA in allpatients this is reflected by a similar prevalence ofabsent EEG background reactivity (1129 vs 1232p 097 2) and a comparable mortality rate(1229 vs 1332 p 095 2)
NSE Serum NSE was measured at least once in all61 studied subjects patients (n 28) with a CPC1ndash2 had lower serum NSE peak levels than those(n 33) with a CPC 3ndash5 at 3 months (see table 2p 0001 Wilcoxon rank-sum) Of note a totalof 5 survivors (328 subjects with CPC 1ndash2 and26 patients with CPC 3) had serum NSE levelsabove 33 gL (335 356 51 and 401 404gL respectively)
DISCUSSION The principal finding of this study isthat early abnormal EEG findings during TH corre-late strongly with peak serum NSE levels at 24ndash48hours after CA To our knowledge this is the first
clinical study showing an early correlation betweenmultichannel EEG alterations and a serum marker ofpostanoxic brain injury and these findings expandprevious observations demonstrating the value ofEEG in patients with hypoxic-ischemic encephalop-athy even when performed early in the intrahypo-thermic period Our data also confirm that absentEEG background reactivity and the presence of epi-leptiform transients during TH are strong predictorsof poor outcome after CA and further show thatsurvival after CA with good neurologic recovery ispossible despite serum NSE levels above the AANguidelines cutoff of 33 gL
A preliminary study published in Chinese re-ported an association of EEG background with se-rum NSE values after neonatal hypoxia although nocorrelation analysis was provided16 A recent study on34 comatose adults found an association between aflat or discontinuous bispectral index after TH andNSE levels17 However the relationship between se-rum markers and multichannel EEG during TH hasnot been addressed so far Although elevations ofNSE in the blood may be favored by bloodndashbrainbarrier dysfunction18 animal studies have convinc-ingly demonstrated that serum NSE correlates withstructural neuronal injury rather than transitory neu-ronal dysfunction1920 moreover elevated NSE levelshave been found in conditions related to neuronaldeath in humans such as brain trauma21ndash23 andstroke2425 Thus the present findings suggest thatEEG abnormalities are not simply a sign of transientpost-CA global dysfunction but rather represent apathophysiologic correlate of postanoxic neuronalinjury Pending confirmation in other cohorts ourfindings have important clinical implications as theEEG is a readily available widespread tool In ourcohort EEG lack of reactivity and discontinuousbackground but not the presence of epileptiformdischarges accounted for the relationship of NSEWhile this finding may be due to the relatively lownumber of patients with epileptiform transients itmay also suggest that paroxysmal neuronal firingcannot occur in subjects in whom the cerebral cortexhas sustained a nearly maximal damage the recentScandinavian study that also identified a substantialnumber of patients with status epilepticus and nor-mal NSE seems to corroborate this hypothesis17
In a previous preliminary analysis of continuousEEG during TH8 we found that lack of reactivityepileptiform features and discontinuous backgroundwere 100 predictive of nonawakening from post-anoxic coma Similar findings were described by ourand other groups when EEG was recorded after re-warming3ndash5 Indeed we found in the present studythat 2838 (74) of patients with preserved EEG
Table 2 Clinical characteristics of 61 patients with hypothermic EEGaccording to their neurologic outcome at 3 months
CPC 1ndash2(28 patients)
CPC 3ndash5(33 patients)
EEG unfavorable features (during hypothermia)
a Nonreactive background n () 0 23 (70)
b Discontinuous background (burst-suppression)n ()
2 (7) 26 (79)
c Epileptiform transients n ()a 0 10 (30)
Sum of EEG unfavorable features (andashc) median(range)b
0 (0ndash1) 2 (0ndash3)
Other clinical and electrophysiologic variables(in normothermic conditions after hypothermia)
Incomplete return of brainstem reflexes n () 3 (11) 21 (64)
Myoclonus n () 2 (7) 7 (21)
Extension or no motor response to pain n () 2 (7) 24 (73)
Nonreactive EEG background n () 0 20 (61)
Bilaterally absent N20 on SSEP n ()c 028 1131 (35)
NSE gL median (range) 178 (80ndash510)d 344 (111ndash2910)e
Abbreviations CPC Cerebral Performance Categories NSE neuron-specific enolaseSSEP somatosensory evoked potentialsa All also had a nonreactive backgroundb Of 6 patients with CPC 3 3 had a sum of 0 and 3 of 1 (all with discontinuous back-ground only)c A total of 59 patients assessedd A total of 328 patients had values 33 Le A total of 1733 patients had values 33 L
Neurology 78 March 13 2012 799
reactivity had a favorable neurologic outcome con-firming our previous observations In addition thisstudy provides other important data first discontin-uous EEG is not an obligate predictor of death since428 (14) patients with this pattern awoke and 2had a good neurologic outcome The point-estimateof the false-positive rate (FPR 1 specificity) ofdiscontinuous background for prediction of poorfunctional outcome was 7 and raised to 12 fordeath while the FPR for the other 2 EEG featureswas 0 for both outcome endpoints It has been sug-gested4 that lack of EEG reactivity may reflect awidespread damage of the aminergic reticular acti-vating system26 and thus a severe impairment ofanoxia-resistant brainstem pathways The strongrelationship between increasing EEG abnormali-ties and elevated serum NSE seems to support thishypothesis although further studies aiming to de-termine the exact brain structural damage follow-ing hypoxic-ischemic encephalopathy eg withdiffusion-weighted MRI are needed
Our observation expands previous findings onEEG performed on neurologically normal subjectsduring hypothermia27 describing appearance of peri-odic complexes on a pharyngeal temperature of296 3 degC however anesthetic doses were notreported in that study It is indeed very interesting tonote that in our cohort patients with coma after CAwho received a moderate sedation with midazolamand fentanyl and eventually awoke did not showany periodic pattern Furthermore none of our pa-tients with epileptiform transients recorded under se-dation (thus with drugs that have antiepilepticproperties) and during TH awoke despite furtherspecific antiepileptic treatment This confirms thatthese EEG patterns are probably different from epi-leptiform features appearing off sedation after THwhich do not preclude awakening in some patients1728
Finally although 9 of patients who showed nonreac-tive EEG background during TH recovered EEG reac-tivity after rewarming both died despite continuedintensive care this again emphasizes the strong predic-tive value of early EEG findings
The AAN-recommended serum NSE prognosticcutoff of 33 gL12 is based on a single class I study29
In patients treated with TH these cutoffs have beenconfirmed by some71017 but not all530 groups In thelatter 2 studies cutoff values of serum NSE up to 78gL were necessary to reach an FPR of 0 Ourdata are in line with those observations 5 subjectswith serum NSE 33 gL awoke and 3 had a goodneurologic outcome implying an FPR for poor out-come and death of 11 and 15 respectively Sinceone of the excluded patients (without hypothermicEEG) having an NSE of 75 gL recovered a CPC of
1 the safe cutoff for awakening in our cohort appearssimilar to that previously mentioned30 and suggeststhat TH significantly alters NSE values and thatNSE should not be used alone to predict awakeningfrom CA and TH
This study has some limitations First recordingswere not uniform in terms of time from CA to initi-ation of EEG and duration However EEG reactiv-ity was tested at least 6 hours following CA in allpatients suggesting a homogenous EEG assessmentThis is particularly important since the prehypother-mic era it is known that in the first few hours follow-ing brain anoxia even a flat EEG is not obligatorilypredictive of bad outcome3132 and at least in chil-dren electrographic seizures during TH only developafter at least 6 hours33 Of note EEG reactivity had acomparable prevalence between long- and short-termrecordings and the almost identical mortality ratereflects the homogeneity of the 2 EEG subgroupsarguing against different modalities for treatmentmanagement and measures to interrupt intensivecare This point also underscores that a self-fulfillingprophecy29 of hypothermic EEG features and NSEappears highly unlikely in this analysis as both werenot used to decide on patientsrsquo fate as opposed to arecent study17 This appears to be the best way tominimize this potentially major bias in observationalstudies on patients after CA3 Second EEG was notscored using quantitative analysis raising the possi-bility of subjectivity However this reflects commonclinical practice and the fact that the EEG readerswere blinded to the NSE levels renders a systematicbias unlikely Third serum NSE was not collectedcontinuously but the relatively long half-life of 24hours justifies this practice Fourth NSE does notseem to represent a perfect correlate of neurologicdamage in patients undergoing TH however highNSE values strongly predict a poor functional prog-nosis in our series the positive predictive value fordeath or significant handicap at 3 months was as highas 85 for a cutoff of 33 gL and 100 for acutoff of 52 gL
Presence of early EEG abnormal findings duringhypothermia strongly correlates with elevated levelsof serum NSE at 24ndash48 hours in patients with comaafter cardiac arrest This suggests that EEG back-ground is both a strong pathophysiologic correlate ofcerebral damage after CA and a robust predictor ofoutcome Our findings also argue in favor of a multi-modal prognostication approach where integrationof EEG and NSE to other clinical variables may helpin guiding therapy and clinical decisions during earlycritical care In this setting indeed decisions uponlife support should never been taken on a singleparameter
800 Neurology 78 March 13 2012
AUTHOR CONTRIBUTIONSDr Rossetti collected the data conducted the study drafted the initial
manuscript and carried out statistical analyses Dr Carrera collected the
data reviewed the text for important intellectual content and drafted the
figure Dr Oddo collected the data and reviewed the text for important
intellectual content
ACKNOWLEDGMENTThe authors thank Malin Maeder-Ingvar MD Christine Stahli RN the
EEG fellows and technologists and the ICU fellows for their help in data
collection
DISCLOSUREDr Rossetti has received research support from Pfizer Inc UCB Glaxo-
SmithKline Eisai Inc Janssen and Sandoz Dr Carrera reports no dis-
closures Dr Oddo is supported by a Grant from the European Society of
Intensive Care Medicine (ECCRN Clinical Research Award 2010)
Received June 14 2011 Accepted in final form August 31 2011
REFERENCES1 Al Thenayan E Savard M Sharpe M Norton L Young B
Predictors of poor neurologic outcome after induced mildhypothermia following cardiac arrest Neurology 2008711535ndash1537
2 Samaniego EA Mlynash M Caulfield AF Eyngorn I Wi-jman CA Sedation confounds outcome prediction in car-diac arrest survivors treated with hypothermia NeurocritCare (in press 2012)
3 Rossetti AO Oddo M Logroscino G Kaplan PW Prog-nostication after cardiac arrest and hypothermia a pro-spective study Ann Neurol 201067301ndash307
4 Thenayan EA Savard M Sharpe MD Norton L YoungB Electroencephalogram for prognosis after cardiac arrestJ Crit Care 201025300ndash304
5 Fugate JE Wijdicks EF Mandrekar J et al Predictors ofneurologic outcome in hypothermia after cardiac arrestAnn Neurol 201068907ndash914
6 Wennervirta JE Ermes MJ Tiainen SM et alHypothermia-treated cardiac arrest patients with goodneurological outcome differ early in quantitative variablesof EEG suppression and epileptiform activity Crit CareMed 2009372427ndash2435
7 Rundgren M Rosen I Friberg H Amplitude-integratedEEG (aEEG) predicts outcome after cardiac arrest and in-duced hypothermia Intens Care Med 200632836ndash842
8 Rossetti AO Urbano LA Delodder F Kaplan PW OddoM Prognostic value of continuous EEG monitoring dur-ing therapeutic hypothermia after cardiac arrest Crit Care201014R173
9 Schmechel D Marangos PJ Brightman M Neurone-specific enolase is a molecular marker for peripheral andcentral neuroendocrine cells Nature 1978276834ndash836
10 Oksanen T Tiainen M Skrifvars MB et al Predictivepower of serum NSE and OHCA score regarding 6-monthneurologic outcome after out-of-hospital ventricular fibril-lation and therapeutic hypothermia Resuscitation 200980165ndash170
11 Shinozaki K Oda S Sadahiro T et al S-100B andneuron-specific enolase as predictors of neurological out-come in patients after cardiac arrest and return of sponta-neous circulation a systematic review Crit Care 200913R121
12 Wijdicks EF Hijdra A Young GB Bassetti CL Wiebe SPractice parameter prediction of outcome in comatose
survivors after cardiopulmonary resuscitation (an evidence-based review) report of the Quality Standards Subcommitteeof the American Academy of Neurology Neurology 200667203ndash210
13 Oddo M Ribordy V Feihl F et al Early predictors ofoutcome in comatose survivors of ventricular fibrillationand non-ventricular fibrillation cardiac arrest treated withhypothermia a prospective study Crit Care Med 2008362296ndash2301
14 2005 American Heart Association Guidelines for Cardio-pulmonary Resuscitation and Emergency CardiovascularCare Circulation 2005112IV1ndash203
15 Booth CM Boone RH Tomlinson G Detsky AS Is thispatient dead vegetative or severely neurologically im-paired Assessing outcome for comatose survivors of car-diac arrest JAMA 2004291870ndash879
16 Dai HQ Luo YH [Changes of electroencephalographicbackground patterns and serum neuron specific enolaselevels in neonates with hypoxic-ischemic encephalopathy]Zhongguo Dang Dai Er Ke Za Zhi 200911173ndash176
17 Cronberg T Rundgren M Westhall E et al Neuron-specific enolase correlates with other prognostic markersafter cardiac arrest Neurology 201177623ndash630
18 Tiainen M Roine RO Pettila V Takkunen O Serumneuron-specific enolase and S-100B protein in cardiac ar-rest patients treated with hypothermia Stroke 2003342881ndash2886
19 Hans P Bonhomme V Collette J Moonen G Neuron-specific enolase as a marker of in vitro neuronal damagepart I assessment of neuron-specific enolase as a quantita-tive and specific marker of neuronal damage J NeurosurgAnesthesiol 19935111ndash116
20 Sankar R Shin DH Wasterlain CG Serum neuron-specific enolase is a marker for neuronal damage followingstatus epilepticus in the rat Epilepsy Res 199728129ndash136
21 Vos PE Lamers KJ Hendriks JC et al Glial and neuronalproteins in serum predict outcome after severe traumaticbrain injury Neurology 2004621303ndash1310
22 Berger RP Beers SR Richichi R Wiesman D AdelsonPD Serum biomarker concentrations and outcome afterpediatric traumatic brain injury J Neurotrauma 2007241793ndash1801
23 Naeimi ZS Weinhofer A Sarahrudi K Heinz T Vecsei VPredictive value of S-100B protein and neuron specific-enolase as markers of traumatic brain damage in clinicaluse Brain Inj 200620463ndash468
24 Jauch EC Lindsell C Broderick J Fagan SC Tilley BCLevine SR Association of serial biochemical markers withacute ischemic stroke the National Institute of Neurologi-cal Disorders and Stroke recombinant tissue plasminogenactivator Stroke Study Stroke 2006372508ndash2513
25 Oh SH Lee JG Na SJ Park JH Choi YC Kim WJPrediction of early clinical severity and extent of neuronaldamage in anterior-circulation infarction using the initialserum neuron-specific enolase level Arch Neurol 20036037ndash41
26 Vincent SR The ascending reticular activating systemndashfrom aminergic neurons to nitric oxide J Chem Neuro-anat 20001823ndash30
27 Stecker MM Cheung AT Pochettino A et al Deep hypo-thermic circulatory arrest I Effects of cooling on electro-encephalogram and evoked potentials Ann Thorac Surg20017114ndash21
Neurology 78 March 13 2012 801
28 Rossetti AO Oddo M Liaudet L Kaplan PW Predictorsof awakening from postanoxic status epilepticus after ther-apeutic hypothermia Neurology 200972744ndash749
29 Zandbergen EG Hijdra A Koelman JH et al Predictionof poor outcome within the first 3 days of postanoxiccoma Neurology 20066662ndash68
30 Steffen IG Hasper D Ploner CJ et al Mild therapeutichypothermia alters neuron specific enolase as an outcomepredictor after resuscitation 97 prospective hypothermiapatients compared to 133 historical non-hypothermia pa-tients Crit Care 201014R69
31 Bassetti C Bomio F Mathis J Hess CW Early prognosisin coma after cardiac arrest a prospective clinical electro-physiological and biochemical study of 60 patients J Neu-rol Neurosurg Psychiatry 199661610ndash615
32 Jorgensen EO Technical contribution Requirements forrecording the EEG at high sensitivity in suspected braindeath Electroencephalogr Clin Neurophysiol 19743665ndash69
33 Abend NS Topjian A Ichord R et al Electroencephalo-graphic monitoring during hypothermia after pediatriccardiac arrest Neurology 2009721931ndash1940
Refresh Your Annual Meeting Experience with New2012 AAN On Demand
More than 600 hours of cutting-edge educational content and breakthrough scientific research
Online access within 24 hours of end of program
Mobile streaming for most iPadreg iPhonereg and Androidreg devices
USB Flash Drive offers convenient offline access (shipped after the Annual Meeting)
Enhanced browser search and improved interface for better overall experience
Get a great value with special pricing on AAN On Demand and the Syllabi on CDPre-order and save up to $1200 Learn more at wwwaancomviewondemand2
Editorrsquos Note to Authors and Readers Levels of Evidence in Neurologyreg
Effective January 15 2009 authors submitting Articles or ClinicalScientific Notes to Neurologyreg
that report on clinical therapeutic studies must state the study type the primary research ques-tion(s) and the classification of level of evidence assigned to each question based on the AANclassification scheme requirements While the authors will initially assign a level of evidence thefinal level will be adjudicated by an independent team prior to publication Ultimately these levelscan be translated into classes of recommendations for clinical care For more information pleaseaccess the articles and the editorial on the use of classification of levels of evidence published inNeurology1-3
1 French J Gronseth G Lost in a jungle of evidence we need a compass Neurology 2008711634ndash1638
2 Gronseth G French J Practice parameters and technology assessments what they are what they are not and why youshould care Neurology 2008711639ndash1643
3 Gross RA Johnston KC Levels of evidence taking Neurologyreg to the next level Neurology 2009728ndash10
802 Neurology 78 March 13 2012
DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
ServicesUpdated Information amp
httpwwwneurologyorgcontent7811796fullhtmlincluding high resolution figures can be found at
Supplementary Material
e318249f6bbDC1htmlhttpwwwneurologyorgcontentsuppl20120209WNL0b013Supplementary material can be found at
References
httpwwwneurologyorgcontent7811796fullhtmlref-list-1at This article cites 32 articles 10 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7811796fullhtmlotherartiThis article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionprognosisPrognosis
httpwwwneurologyorgcgicollectioneeg_EEG
ease_strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

Early EEG correlates of neuronal injuryafter brain anoxia
Andrea O Rossetti MDEmmanuel Carrera MDMauro Oddo MD
ABSTRACT
Objectives EEG and serum neuron-specific enolase (NSE) are used for outcome prognosticationin patients with postanoxic coma however it is unclear if EEG abnormalities reflect transientneuronal dysfunction or neuronal death To assess this question EEG abnormalities were corre-lated with NSE Moreover NSE cutoff values and hypothermic EEG features related with pooroutcome were explored
Methods In a prospective cohort of 61 adults treated with therapeutic hypothermia (TH) aftercardiac arrest (CA) multichannel EEG recorded during TH was assessed for background reactiv-ity and continuity presence of epileptiform transients and correlated with serum NSE collectedat 24ndash48 hours after CA Demographic clinical and functional outcome data (at 3 months) werecollected and integrated in the analyses
Results In-hospital mortality was 41 and 82 of survivors had good neurologic outcome at 3months Serum NSE and EEG findings were strongly correlated (Spearman rho 045 p
0001) Median NSE peak values were higher in patients with unreactive EEG background (p
0001) and discontinuous patterns (p 0001) While all subjects with nonreactive EEG died 5survivors (3 with good outcome) had NSE levels 33 gL
Conclusion The correlation between EEG during TH and serum NSE levels supports the hypoth-esis that early EEG alterations reflect permanent neuronal damage Furthermore this study con-firms that absent EEG background reactivity and presence of epileptiform transients are robustpredictors of poor outcome after CA and that survival with good neurologic recovery is possibledespite serum NSE levels 33 gL This underscores the importance of multimodal assess-ments in this setting Neurologyreg 201278796ndash802
GLOSSARYAAN American Academy of Neurology CA cardiac arrest CPC Cerebral Performance Categories FPR false-positiverate NSE neuron-specific enolase SIRPIDS stimulus-induced rhythmic periodic or irritative discharges SSEP so-matosensory evoked potentials TH therapeutic hypothermia VF ventricular fibrillation
Therapeutic hypothermia (TH) improves outcome in comatose survivors of cardiac arrest(CA) but may also alter prognostic clinical features especially motor response to painfulstimuli1ndash3 In this context EEG may represent an important tool to improve prognostication inpostanoxic coma While recent works emphasized the importance of EEG background reactiv-ity following return to normothermia3ndash5 prognostic values of recordings performed duringhypothermia have received far less attention Two studies addressed quantitative EEG featuresand identified burst-suppression ratio presence of status epilepticus and entropy characteris-tics as promising prognosticators67 while our group reported lack of visually assessed EEGbackground reactivity as a robust predictor of poor outcome in 34 patients8 Nevertheless theseobservations did not address the neuronal correlates subtending EEG changes
Neuron-specific enolase (NSE) is a 780-kDa intracellular enzyme found in neurons andother cells of neuroectodermal origin9 Elevation of serum NSE 1ndash3 days after CA is regardedas a severity marker of postanoxic neuronal injury it has been shown to be released in the
From the Departments of Clinical Neurosciences (AOR EC) and Intensive Care Medicine (MO) University Hospital and Faculty of Biologyand Medicine Lausanne Switzerland
Disclosure Author disclosures are provided at the end of the article
Editorial page 774
Correspondence amp reprintrequests to Dr Rossettiandrearossettichuvch
796 Copyright copy 2012 by AAN Enterprises Inc
serum of patients after CA with a half-life ofabout 24 hours1011 The American Academyof Neurology (AAN) practice parameterswhich considered studies from the prehypo-thermia era suggest a cutoff of 33 gL atdays 1ndash3 after CA as a robust predictor forpoor outcome12
Multichannel EEG and NSE have beeninvestigated separately in patients withhypoxic-ischemic encephalopathy to ourknowledge however no studies have specif-ically addressed a potential correlation be-tween these variables In the present studywe hypothesized that abnormal EEG find-ings reflect the degree of postanoxic neuro-nal injury and investigated whether earlyEEG abnormalities recorded during THcorrelate with serum NSE levels sampled24 ndash 48 hours after CA
METHODS Patients We prospectively studied a cohort ofconsecutive comatose adults admitted between December2009 and April 2011 to the Department of Intensive CareMedicine of our hospital after successful resuscitation fromCA and treated with TH according to our local protocol13
All patients were resuscitated according to recent recommen-dations14 and treated with mild TH to 33degC for 24 hoursusing ice packs and IV ice-cold fluids for the rapid inductionof cooling and a surface cooling device (Arctic Sun SystemMedivance Louisville CO) for the maintenance of TH In astandardized approach midazolam (01 mgkgh) and fenta-nyl (15 gkgh) were given for sedation-analgesia and ve-curonium (01 mgkg boluses) was administered to controlshivering Patients diagnosed as being in brain death uponrewarming or without signs of EEG activity (ldquoflat record-ingrdquo) were not included in the study
Standard protocol approvals registrations and patientconsents This study was approved by our Institutional ReviewBoard patient consent was not required as this was a purelyobservational study and all procedures were part of standard pa-tient care
EEG data Video-EEGs (Viasys Neurocare Madison WI)were performed during TH with 9 to 21 electrodes according tothe international 10ndash20 system EEG was continuously recordedfor 24ndash48 hours8 or due to practical limitations for 20ndash30minutes Background reactivity was tested on-site as detailed inour previous study8 using repetitive auditory visual and nocice-ptive stimulations at least 6 hours after CA All recordings werevisually interpreted by 2 EEG-certified neurologists blinded toNSE levels EEG findings were categorized according to thepresence or absence of the following 3 variables 1) EEG back-ground reactivity defined as an activity 10 V (regardless offrequency) and if the background showed presence of any clearand reproducible change in amplitude or frequency upon stimula-tion excluding stimulus-induced rhythmic periodic or irritativedischarges (SIRPIDS) and muscle artifacts 2) spontaneous discon-tinuous (burst-suppression) pattern defined as an EEG background
interrupted by flat periods 3) epileptiform activity defined as any
periodic or rhythmic spikes sharp waves spike-waves or rhythmic
waves evolving in amplitude frequency or field38
NSE Serum NSE was sampled at 24 and 48 hours after CA To
avoid hemolysis and false-positive test results samples for NSE
measurement were manually handled and transported to central
laboratory For accurate determination of NSE levels an auto-
mated immunofluorescent assay (Thermo Scientific Brahms
NSE Kryptorreg Immunoassay) was used
Neurologic assessment antiepileptic therapy andtreatment withdrawal At least 36 hours after CA after re-
warming at a core temperature 35degC and off sedation repeated
neurologic examination standard (20ndash30 minutes) EEG with
the above mentioned stimulations and cortical somatosensory
evoked potentials (SSEP) were performed Patients with EEG
evidence of status epilepticus were treated with IV antiepilep-
tic drugs discontinued if no clinical improvement was noted
after at least 72 hours While physicians were not blinded to
these results hypothermic EEG findings and NSE values
were not used for the interdisciplinary decision on withdrawal
of intensive care support This has been described previously3
and is based on a multimodal approach including at least 2 of
the following (assessed in normothermia at least 48 ndash72 hours
after CA) incomplete recovery of brainstem reflexes early
myoclonus unreactive normothermic EEG and bilaterally
absent cortical SSEP
Outcome assessment Functional neurologic outcome was
assessed at 3 months through a phone interview by trained per-
sonnel of the EEG unit who had no access to study data and
categorized according to the Glasgow-Pittsburgh Cerebral Per-
formance Categories (CPC) (1 good recovery 2 moderate
disability 3 severe disability with dependency for daily life
activity 4 vegetative state and 5 death15) in line with the
vast majority of studies on this topic outcome was dichotomized
as good (CPC 1ndash2) vs poor (CPC 3ndash5)
Data collection All variables were collected prospectively
Baseline demographics included initial arrest rhythm (ventricu-
lar fibrillation [VF] vs non-VF including asystole and pulseless
electrical activity) and duration of CA (ie the time from col-
lapse to return of spontaneous circulation) Hypothermic EEG
findings included background reactivity burst-suppression pat-
tern and epileptiform activity as described previously Serum
values of NSE at 24 and 48 hours were recorded
Statistical analysis Wilcoxon rank sum Student t and 2
tests were used as needed to compare groups and the Spearman
rank test was used to examine the correlation between EEG find-
ings and NSE For this purpose according to EEG findings dur-
ing TH (reactive vs unreactive background continuous vs
discontinuous background presence vs absence of epileptiform
transients) an EEG score was given to each patient with a min-
imum of 0 and a maximum of 3 For each patient the peak
serum NSE value was used for the correlation Significance was
assumed at p 005 unless corrected after Bonferroni in cases of
multiple comparisons Calculations were performed with the
Stata software version 9 (College Station TX)
RESULTS Patients and outcome During the studyperiod 80 consecutive patients were treated withTH after CA 18 of them did not have EEG dur-
Neurology 78 March 13 2012 797
ing TH and 1 lacked NSE data Table 1 illustratesdemographic clinical characteristics and the out-come of the remaining 61 subjects included in thepresent analysis 23 of them were part of a previ-ously published series8 which did not addressNSE In the majority of patients CA was due toVF In-hospital mortality was 2561 (41) and2834 (82) survivors assessed at 3 monthsreached a good neurologic outcome (CPC 1ndash2)while 6 had CPC 3 and 2 additional patients diedIn-hospital mortality of excluded patients did not
differ from that of the studied group (818 vs 2561 p 043 2)
Correlation between EEG and NSE Considering sig-nificance conservatively at p 0016 (3 compari-sons) median NSE peak values were higher inpatients with unreactive EEG background (93 vs 18gL p 0001 Wilcoxon) and discontinuous(burst-suppression) patterns (633 vs 197 gL p 0001 Wilcoxon) In contrast only some trendtoward higher serum NSE levels in patients with epilep-tiform discharges was found (295 vs 239 gL p 0229 Wilcoxon) (figure) For each patient we alsoanalyzed the relationship between NSE and EEGfindings using the 3 main EEG abnormalities addedtogether to obtain an EEG sum score a strong corre-lation was found between NSE and EEG findings(Spearman rho 045 p 0001)
EEG features In the 61 included patients EEG dur-ing hypothermia was initiated after mean of 154hours (SD 58 hours) following CA During TH29 patients had a continuous EEG monitoring and32 were assessed with routine EEG HypothermicEEG features NSE values and normothermic clini-cal and electrophysiologic variables are given accord-ing to the functional outcome assessed at 3 monthsin table 2 Occurrence of abnormal EEG findingsduring TH differed clearly between the 2 outcomegroups (p 0001 Wilcoxon rank-sum) Of note
Table 1 Characteristics of 61 patients treatedafter cardiac arrest with EEGrecorded during hypothermia andserum NSE values
Demographics Values
Age y mean (SD) 637 (122)
Female n () 18 (30)
Cardiologic variables
Non VF cardiac arrest n () 21 (34)
Time to ROSC mean (SD) 227 (139)
Outcome
In-hospital mortality n () 2561 (41)
CPC 1ndash2 at 3 months n () 2861 (46)
Abbreviations CPC Cerebral Performance CategoriesNSE neuron-specific enolase ROSC return of sponta-neous circulation VF ventricular fibrillation
Figure Associations between serum neuron-specific enolase (NSE) and EEG duringtherapeutic hypothermia
Box plots represent serum NSE values (in gL y-axis) stratified according to EEG findings including background reactiv-ity background continuity and epileptiform activity Box plots represent median (horizontal lines) and 25thndash75th percen-tiles bars represent 10thndash90th percentiles
798 Neurology 78 March 13 2012
all patients with epileptiform transients also had anonreactive EEG background Two of 23 (9) sub-jects without EEG reactivity during TH recoveredreactivity after rewarming however both of themdied despite intensive care support for at least 5 addi-tional days While in patients who had a continuousmonitoring EEG recording was started earlier thanin those who had routine EEG (135 hours vs 171hours p 0015 t test) assessment of EEG reactiv-ity was performed at least 6 hours after CA in allpatients this is reflected by a similar prevalence ofabsent EEG background reactivity (1129 vs 1232p 097 2) and a comparable mortality rate(1229 vs 1332 p 095 2)
NSE Serum NSE was measured at least once in all61 studied subjects patients (n 28) with a CPC1ndash2 had lower serum NSE peak levels than those(n 33) with a CPC 3ndash5 at 3 months (see table 2p 0001 Wilcoxon rank-sum) Of note a totalof 5 survivors (328 subjects with CPC 1ndash2 and26 patients with CPC 3) had serum NSE levelsabove 33 gL (335 356 51 and 401 404gL respectively)
DISCUSSION The principal finding of this study isthat early abnormal EEG findings during TH corre-late strongly with peak serum NSE levels at 24ndash48hours after CA To our knowledge this is the first
clinical study showing an early correlation betweenmultichannel EEG alterations and a serum marker ofpostanoxic brain injury and these findings expandprevious observations demonstrating the value ofEEG in patients with hypoxic-ischemic encephalop-athy even when performed early in the intrahypo-thermic period Our data also confirm that absentEEG background reactivity and the presence of epi-leptiform transients during TH are strong predictorsof poor outcome after CA and further show thatsurvival after CA with good neurologic recovery ispossible despite serum NSE levels above the AANguidelines cutoff of 33 gL
A preliminary study published in Chinese re-ported an association of EEG background with se-rum NSE values after neonatal hypoxia although nocorrelation analysis was provided16 A recent study on34 comatose adults found an association between aflat or discontinuous bispectral index after TH andNSE levels17 However the relationship between se-rum markers and multichannel EEG during TH hasnot been addressed so far Although elevations ofNSE in the blood may be favored by bloodndashbrainbarrier dysfunction18 animal studies have convinc-ingly demonstrated that serum NSE correlates withstructural neuronal injury rather than transitory neu-ronal dysfunction1920 moreover elevated NSE levelshave been found in conditions related to neuronaldeath in humans such as brain trauma21ndash23 andstroke2425 Thus the present findings suggest thatEEG abnormalities are not simply a sign of transientpost-CA global dysfunction but rather represent apathophysiologic correlate of postanoxic neuronalinjury Pending confirmation in other cohorts ourfindings have important clinical implications as theEEG is a readily available widespread tool In ourcohort EEG lack of reactivity and discontinuousbackground but not the presence of epileptiformdischarges accounted for the relationship of NSEWhile this finding may be due to the relatively lownumber of patients with epileptiform transients itmay also suggest that paroxysmal neuronal firingcannot occur in subjects in whom the cerebral cortexhas sustained a nearly maximal damage the recentScandinavian study that also identified a substantialnumber of patients with status epilepticus and nor-mal NSE seems to corroborate this hypothesis17
In a previous preliminary analysis of continuousEEG during TH8 we found that lack of reactivityepileptiform features and discontinuous backgroundwere 100 predictive of nonawakening from post-anoxic coma Similar findings were described by ourand other groups when EEG was recorded after re-warming3ndash5 Indeed we found in the present studythat 2838 (74) of patients with preserved EEG
Table 2 Clinical characteristics of 61 patients with hypothermic EEGaccording to their neurologic outcome at 3 months
CPC 1ndash2(28 patients)
CPC 3ndash5(33 patients)
EEG unfavorable features (during hypothermia)
a Nonreactive background n () 0 23 (70)
b Discontinuous background (burst-suppression)n ()
2 (7) 26 (79)
c Epileptiform transients n ()a 0 10 (30)
Sum of EEG unfavorable features (andashc) median(range)b
0 (0ndash1) 2 (0ndash3)
Other clinical and electrophysiologic variables(in normothermic conditions after hypothermia)
Incomplete return of brainstem reflexes n () 3 (11) 21 (64)
Myoclonus n () 2 (7) 7 (21)
Extension or no motor response to pain n () 2 (7) 24 (73)
Nonreactive EEG background n () 0 20 (61)
Bilaterally absent N20 on SSEP n ()c 028 1131 (35)
NSE gL median (range) 178 (80ndash510)d 344 (111ndash2910)e
Abbreviations CPC Cerebral Performance Categories NSE neuron-specific enolaseSSEP somatosensory evoked potentialsa All also had a nonreactive backgroundb Of 6 patients with CPC 3 3 had a sum of 0 and 3 of 1 (all with discontinuous back-ground only)c A total of 59 patients assessedd A total of 328 patients had values 33 Le A total of 1733 patients had values 33 L
Neurology 78 March 13 2012 799
reactivity had a favorable neurologic outcome con-firming our previous observations In addition thisstudy provides other important data first discontin-uous EEG is not an obligate predictor of death since428 (14) patients with this pattern awoke and 2had a good neurologic outcome The point-estimateof the false-positive rate (FPR 1 specificity) ofdiscontinuous background for prediction of poorfunctional outcome was 7 and raised to 12 fordeath while the FPR for the other 2 EEG featureswas 0 for both outcome endpoints It has been sug-gested4 that lack of EEG reactivity may reflect awidespread damage of the aminergic reticular acti-vating system26 and thus a severe impairment ofanoxia-resistant brainstem pathways The strongrelationship between increasing EEG abnormali-ties and elevated serum NSE seems to support thishypothesis although further studies aiming to de-termine the exact brain structural damage follow-ing hypoxic-ischemic encephalopathy eg withdiffusion-weighted MRI are needed
Our observation expands previous findings onEEG performed on neurologically normal subjectsduring hypothermia27 describing appearance of peri-odic complexes on a pharyngeal temperature of296 3 degC however anesthetic doses were notreported in that study It is indeed very interesting tonote that in our cohort patients with coma after CAwho received a moderate sedation with midazolamand fentanyl and eventually awoke did not showany periodic pattern Furthermore none of our pa-tients with epileptiform transients recorded under se-dation (thus with drugs that have antiepilepticproperties) and during TH awoke despite furtherspecific antiepileptic treatment This confirms thatthese EEG patterns are probably different from epi-leptiform features appearing off sedation after THwhich do not preclude awakening in some patients1728
Finally although 9 of patients who showed nonreac-tive EEG background during TH recovered EEG reac-tivity after rewarming both died despite continuedintensive care this again emphasizes the strong predic-tive value of early EEG findings
The AAN-recommended serum NSE prognosticcutoff of 33 gL12 is based on a single class I study29
In patients treated with TH these cutoffs have beenconfirmed by some71017 but not all530 groups In thelatter 2 studies cutoff values of serum NSE up to 78gL were necessary to reach an FPR of 0 Ourdata are in line with those observations 5 subjectswith serum NSE 33 gL awoke and 3 had a goodneurologic outcome implying an FPR for poor out-come and death of 11 and 15 respectively Sinceone of the excluded patients (without hypothermicEEG) having an NSE of 75 gL recovered a CPC of
1 the safe cutoff for awakening in our cohort appearssimilar to that previously mentioned30 and suggeststhat TH significantly alters NSE values and thatNSE should not be used alone to predict awakeningfrom CA and TH
This study has some limitations First recordingswere not uniform in terms of time from CA to initi-ation of EEG and duration However EEG reactiv-ity was tested at least 6 hours following CA in allpatients suggesting a homogenous EEG assessmentThis is particularly important since the prehypother-mic era it is known that in the first few hours follow-ing brain anoxia even a flat EEG is not obligatorilypredictive of bad outcome3132 and at least in chil-dren electrographic seizures during TH only developafter at least 6 hours33 Of note EEG reactivity had acomparable prevalence between long- and short-termrecordings and the almost identical mortality ratereflects the homogeneity of the 2 EEG subgroupsarguing against different modalities for treatmentmanagement and measures to interrupt intensivecare This point also underscores that a self-fulfillingprophecy29 of hypothermic EEG features and NSEappears highly unlikely in this analysis as both werenot used to decide on patientsrsquo fate as opposed to arecent study17 This appears to be the best way tominimize this potentially major bias in observationalstudies on patients after CA3 Second EEG was notscored using quantitative analysis raising the possi-bility of subjectivity However this reflects commonclinical practice and the fact that the EEG readerswere blinded to the NSE levels renders a systematicbias unlikely Third serum NSE was not collectedcontinuously but the relatively long half-life of 24hours justifies this practice Fourth NSE does notseem to represent a perfect correlate of neurologicdamage in patients undergoing TH however highNSE values strongly predict a poor functional prog-nosis in our series the positive predictive value fordeath or significant handicap at 3 months was as highas 85 for a cutoff of 33 gL and 100 for acutoff of 52 gL
Presence of early EEG abnormal findings duringhypothermia strongly correlates with elevated levelsof serum NSE at 24ndash48 hours in patients with comaafter cardiac arrest This suggests that EEG back-ground is both a strong pathophysiologic correlate ofcerebral damage after CA and a robust predictor ofoutcome Our findings also argue in favor of a multi-modal prognostication approach where integrationof EEG and NSE to other clinical variables may helpin guiding therapy and clinical decisions during earlycritical care In this setting indeed decisions uponlife support should never been taken on a singleparameter
800 Neurology 78 March 13 2012
AUTHOR CONTRIBUTIONSDr Rossetti collected the data conducted the study drafted the initial
manuscript and carried out statistical analyses Dr Carrera collected the
data reviewed the text for important intellectual content and drafted the
figure Dr Oddo collected the data and reviewed the text for important
intellectual content
ACKNOWLEDGMENTThe authors thank Malin Maeder-Ingvar MD Christine Stahli RN the
EEG fellows and technologists and the ICU fellows for their help in data
collection
DISCLOSUREDr Rossetti has received research support from Pfizer Inc UCB Glaxo-
SmithKline Eisai Inc Janssen and Sandoz Dr Carrera reports no dis-
closures Dr Oddo is supported by a Grant from the European Society of
Intensive Care Medicine (ECCRN Clinical Research Award 2010)
Received June 14 2011 Accepted in final form August 31 2011
REFERENCES1 Al Thenayan E Savard M Sharpe M Norton L Young B
Predictors of poor neurologic outcome after induced mildhypothermia following cardiac arrest Neurology 2008711535ndash1537
2 Samaniego EA Mlynash M Caulfield AF Eyngorn I Wi-jman CA Sedation confounds outcome prediction in car-diac arrest survivors treated with hypothermia NeurocritCare (in press 2012)
3 Rossetti AO Oddo M Logroscino G Kaplan PW Prog-nostication after cardiac arrest and hypothermia a pro-spective study Ann Neurol 201067301ndash307
4 Thenayan EA Savard M Sharpe MD Norton L YoungB Electroencephalogram for prognosis after cardiac arrestJ Crit Care 201025300ndash304
5 Fugate JE Wijdicks EF Mandrekar J et al Predictors ofneurologic outcome in hypothermia after cardiac arrestAnn Neurol 201068907ndash914
6 Wennervirta JE Ermes MJ Tiainen SM et alHypothermia-treated cardiac arrest patients with goodneurological outcome differ early in quantitative variablesof EEG suppression and epileptiform activity Crit CareMed 2009372427ndash2435
7 Rundgren M Rosen I Friberg H Amplitude-integratedEEG (aEEG) predicts outcome after cardiac arrest and in-duced hypothermia Intens Care Med 200632836ndash842
8 Rossetti AO Urbano LA Delodder F Kaplan PW OddoM Prognostic value of continuous EEG monitoring dur-ing therapeutic hypothermia after cardiac arrest Crit Care201014R173
9 Schmechel D Marangos PJ Brightman M Neurone-specific enolase is a molecular marker for peripheral andcentral neuroendocrine cells Nature 1978276834ndash836
10 Oksanen T Tiainen M Skrifvars MB et al Predictivepower of serum NSE and OHCA score regarding 6-monthneurologic outcome after out-of-hospital ventricular fibril-lation and therapeutic hypothermia Resuscitation 200980165ndash170
11 Shinozaki K Oda S Sadahiro T et al S-100B andneuron-specific enolase as predictors of neurological out-come in patients after cardiac arrest and return of sponta-neous circulation a systematic review Crit Care 200913R121
12 Wijdicks EF Hijdra A Young GB Bassetti CL Wiebe SPractice parameter prediction of outcome in comatose
survivors after cardiopulmonary resuscitation (an evidence-based review) report of the Quality Standards Subcommitteeof the American Academy of Neurology Neurology 200667203ndash210
13 Oddo M Ribordy V Feihl F et al Early predictors ofoutcome in comatose survivors of ventricular fibrillationand non-ventricular fibrillation cardiac arrest treated withhypothermia a prospective study Crit Care Med 2008362296ndash2301
14 2005 American Heart Association Guidelines for Cardio-pulmonary Resuscitation and Emergency CardiovascularCare Circulation 2005112IV1ndash203
15 Booth CM Boone RH Tomlinson G Detsky AS Is thispatient dead vegetative or severely neurologically im-paired Assessing outcome for comatose survivors of car-diac arrest JAMA 2004291870ndash879
16 Dai HQ Luo YH [Changes of electroencephalographicbackground patterns and serum neuron specific enolaselevels in neonates with hypoxic-ischemic encephalopathy]Zhongguo Dang Dai Er Ke Za Zhi 200911173ndash176
17 Cronberg T Rundgren M Westhall E et al Neuron-specific enolase correlates with other prognostic markersafter cardiac arrest Neurology 201177623ndash630
18 Tiainen M Roine RO Pettila V Takkunen O Serumneuron-specific enolase and S-100B protein in cardiac ar-rest patients treated with hypothermia Stroke 2003342881ndash2886
19 Hans P Bonhomme V Collette J Moonen G Neuron-specific enolase as a marker of in vitro neuronal damagepart I assessment of neuron-specific enolase as a quantita-tive and specific marker of neuronal damage J NeurosurgAnesthesiol 19935111ndash116
20 Sankar R Shin DH Wasterlain CG Serum neuron-specific enolase is a marker for neuronal damage followingstatus epilepticus in the rat Epilepsy Res 199728129ndash136
21 Vos PE Lamers KJ Hendriks JC et al Glial and neuronalproteins in serum predict outcome after severe traumaticbrain injury Neurology 2004621303ndash1310
22 Berger RP Beers SR Richichi R Wiesman D AdelsonPD Serum biomarker concentrations and outcome afterpediatric traumatic brain injury J Neurotrauma 2007241793ndash1801
23 Naeimi ZS Weinhofer A Sarahrudi K Heinz T Vecsei VPredictive value of S-100B protein and neuron specific-enolase as markers of traumatic brain damage in clinicaluse Brain Inj 200620463ndash468
24 Jauch EC Lindsell C Broderick J Fagan SC Tilley BCLevine SR Association of serial biochemical markers withacute ischemic stroke the National Institute of Neurologi-cal Disorders and Stroke recombinant tissue plasminogenactivator Stroke Study Stroke 2006372508ndash2513
25 Oh SH Lee JG Na SJ Park JH Choi YC Kim WJPrediction of early clinical severity and extent of neuronaldamage in anterior-circulation infarction using the initialserum neuron-specific enolase level Arch Neurol 20036037ndash41
26 Vincent SR The ascending reticular activating systemndashfrom aminergic neurons to nitric oxide J Chem Neuro-anat 20001823ndash30
27 Stecker MM Cheung AT Pochettino A et al Deep hypo-thermic circulatory arrest I Effects of cooling on electro-encephalogram and evoked potentials Ann Thorac Surg20017114ndash21
Neurology 78 March 13 2012 801
28 Rossetti AO Oddo M Liaudet L Kaplan PW Predictorsof awakening from postanoxic status epilepticus after ther-apeutic hypothermia Neurology 200972744ndash749
29 Zandbergen EG Hijdra A Koelman JH et al Predictionof poor outcome within the first 3 days of postanoxiccoma Neurology 20066662ndash68
30 Steffen IG Hasper D Ploner CJ et al Mild therapeutichypothermia alters neuron specific enolase as an outcomepredictor after resuscitation 97 prospective hypothermiapatients compared to 133 historical non-hypothermia pa-tients Crit Care 201014R69
31 Bassetti C Bomio F Mathis J Hess CW Early prognosisin coma after cardiac arrest a prospective clinical electro-physiological and biochemical study of 60 patients J Neu-rol Neurosurg Psychiatry 199661610ndash615
32 Jorgensen EO Technical contribution Requirements forrecording the EEG at high sensitivity in suspected braindeath Electroencephalogr Clin Neurophysiol 19743665ndash69
33 Abend NS Topjian A Ichord R et al Electroencephalo-graphic monitoring during hypothermia after pediatriccardiac arrest Neurology 2009721931ndash1940
Refresh Your Annual Meeting Experience with New2012 AAN On Demand
More than 600 hours of cutting-edge educational content and breakthrough scientific research
Online access within 24 hours of end of program
Mobile streaming for most iPadreg iPhonereg and Androidreg devices
USB Flash Drive offers convenient offline access (shipped after the Annual Meeting)
Enhanced browser search and improved interface for better overall experience
Get a great value with special pricing on AAN On Demand and the Syllabi on CDPre-order and save up to $1200 Learn more at wwwaancomviewondemand2
Editorrsquos Note to Authors and Readers Levels of Evidence in Neurologyreg
Effective January 15 2009 authors submitting Articles or ClinicalScientific Notes to Neurologyreg
that report on clinical therapeutic studies must state the study type the primary research ques-tion(s) and the classification of level of evidence assigned to each question based on the AANclassification scheme requirements While the authors will initially assign a level of evidence thefinal level will be adjudicated by an independent team prior to publication Ultimately these levelscan be translated into classes of recommendations for clinical care For more information pleaseaccess the articles and the editorial on the use of classification of levels of evidence published inNeurology1-3
1 French J Gronseth G Lost in a jungle of evidence we need a compass Neurology 2008711634ndash1638
2 Gronseth G French J Practice parameters and technology assessments what they are what they are not and why youshould care Neurology 2008711639ndash1643
3 Gross RA Johnston KC Levels of evidence taking Neurologyreg to the next level Neurology 2009728ndash10
802 Neurology 78 March 13 2012
DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
ServicesUpdated Information amp
httpwwwneurologyorgcontent7811796fullhtmlincluding high resolution figures can be found at
Supplementary Material
e318249f6bbDC1htmlhttpwwwneurologyorgcontentsuppl20120209WNL0b013Supplementary material can be found at
References
httpwwwneurologyorgcontent7811796fullhtmlref-list-1at This article cites 32 articles 10 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7811796fullhtmlotherartiThis article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionprognosisPrognosis
httpwwwneurologyorgcgicollectioneeg_EEG
ease_strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

serum of patients after CA with a half-life ofabout 24 hours1011 The American Academyof Neurology (AAN) practice parameterswhich considered studies from the prehypo-thermia era suggest a cutoff of 33 gL atdays 1ndash3 after CA as a robust predictor forpoor outcome12
Multichannel EEG and NSE have beeninvestigated separately in patients withhypoxic-ischemic encephalopathy to ourknowledge however no studies have specif-ically addressed a potential correlation be-tween these variables In the present studywe hypothesized that abnormal EEG find-ings reflect the degree of postanoxic neuro-nal injury and investigated whether earlyEEG abnormalities recorded during THcorrelate with serum NSE levels sampled24 ndash 48 hours after CA
METHODS Patients We prospectively studied a cohort ofconsecutive comatose adults admitted between December2009 and April 2011 to the Department of Intensive CareMedicine of our hospital after successful resuscitation fromCA and treated with TH according to our local protocol13
All patients were resuscitated according to recent recommen-dations14 and treated with mild TH to 33degC for 24 hoursusing ice packs and IV ice-cold fluids for the rapid inductionof cooling and a surface cooling device (Arctic Sun SystemMedivance Louisville CO) for the maintenance of TH In astandardized approach midazolam (01 mgkgh) and fenta-nyl (15 gkgh) were given for sedation-analgesia and ve-curonium (01 mgkg boluses) was administered to controlshivering Patients diagnosed as being in brain death uponrewarming or without signs of EEG activity (ldquoflat record-ingrdquo) were not included in the study
Standard protocol approvals registrations and patientconsents This study was approved by our Institutional ReviewBoard patient consent was not required as this was a purelyobservational study and all procedures were part of standard pa-tient care
EEG data Video-EEGs (Viasys Neurocare Madison WI)were performed during TH with 9 to 21 electrodes according tothe international 10ndash20 system EEG was continuously recordedfor 24ndash48 hours8 or due to practical limitations for 20ndash30minutes Background reactivity was tested on-site as detailed inour previous study8 using repetitive auditory visual and nocice-ptive stimulations at least 6 hours after CA All recordings werevisually interpreted by 2 EEG-certified neurologists blinded toNSE levels EEG findings were categorized according to thepresence or absence of the following 3 variables 1) EEG back-ground reactivity defined as an activity 10 V (regardless offrequency) and if the background showed presence of any clearand reproducible change in amplitude or frequency upon stimula-tion excluding stimulus-induced rhythmic periodic or irritativedischarges (SIRPIDS) and muscle artifacts 2) spontaneous discon-tinuous (burst-suppression) pattern defined as an EEG background
interrupted by flat periods 3) epileptiform activity defined as any
periodic or rhythmic spikes sharp waves spike-waves or rhythmic
waves evolving in amplitude frequency or field38
NSE Serum NSE was sampled at 24 and 48 hours after CA To
avoid hemolysis and false-positive test results samples for NSE
measurement were manually handled and transported to central
laboratory For accurate determination of NSE levels an auto-
mated immunofluorescent assay (Thermo Scientific Brahms
NSE Kryptorreg Immunoassay) was used
Neurologic assessment antiepileptic therapy andtreatment withdrawal At least 36 hours after CA after re-
warming at a core temperature 35degC and off sedation repeated
neurologic examination standard (20ndash30 minutes) EEG with
the above mentioned stimulations and cortical somatosensory
evoked potentials (SSEP) were performed Patients with EEG
evidence of status epilepticus were treated with IV antiepilep-
tic drugs discontinued if no clinical improvement was noted
after at least 72 hours While physicians were not blinded to
these results hypothermic EEG findings and NSE values
were not used for the interdisciplinary decision on withdrawal
of intensive care support This has been described previously3
and is based on a multimodal approach including at least 2 of
the following (assessed in normothermia at least 48 ndash72 hours
after CA) incomplete recovery of brainstem reflexes early
myoclonus unreactive normothermic EEG and bilaterally
absent cortical SSEP
Outcome assessment Functional neurologic outcome was
assessed at 3 months through a phone interview by trained per-
sonnel of the EEG unit who had no access to study data and
categorized according to the Glasgow-Pittsburgh Cerebral Per-
formance Categories (CPC) (1 good recovery 2 moderate
disability 3 severe disability with dependency for daily life
activity 4 vegetative state and 5 death15) in line with the
vast majority of studies on this topic outcome was dichotomized
as good (CPC 1ndash2) vs poor (CPC 3ndash5)
Data collection All variables were collected prospectively
Baseline demographics included initial arrest rhythm (ventricu-
lar fibrillation [VF] vs non-VF including asystole and pulseless
electrical activity) and duration of CA (ie the time from col-
lapse to return of spontaneous circulation) Hypothermic EEG
findings included background reactivity burst-suppression pat-
tern and epileptiform activity as described previously Serum
values of NSE at 24 and 48 hours were recorded
Statistical analysis Wilcoxon rank sum Student t and 2
tests were used as needed to compare groups and the Spearman
rank test was used to examine the correlation between EEG find-
ings and NSE For this purpose according to EEG findings dur-
ing TH (reactive vs unreactive background continuous vs
discontinuous background presence vs absence of epileptiform
transients) an EEG score was given to each patient with a min-
imum of 0 and a maximum of 3 For each patient the peak
serum NSE value was used for the correlation Significance was
assumed at p 005 unless corrected after Bonferroni in cases of
multiple comparisons Calculations were performed with the
Stata software version 9 (College Station TX)
RESULTS Patients and outcome During the studyperiod 80 consecutive patients were treated withTH after CA 18 of them did not have EEG dur-
Neurology 78 March 13 2012 797
ing TH and 1 lacked NSE data Table 1 illustratesdemographic clinical characteristics and the out-come of the remaining 61 subjects included in thepresent analysis 23 of them were part of a previ-ously published series8 which did not addressNSE In the majority of patients CA was due toVF In-hospital mortality was 2561 (41) and2834 (82) survivors assessed at 3 monthsreached a good neurologic outcome (CPC 1ndash2)while 6 had CPC 3 and 2 additional patients diedIn-hospital mortality of excluded patients did not
differ from that of the studied group (818 vs 2561 p 043 2)
Correlation between EEG and NSE Considering sig-nificance conservatively at p 0016 (3 compari-sons) median NSE peak values were higher inpatients with unreactive EEG background (93 vs 18gL p 0001 Wilcoxon) and discontinuous(burst-suppression) patterns (633 vs 197 gL p 0001 Wilcoxon) In contrast only some trendtoward higher serum NSE levels in patients with epilep-tiform discharges was found (295 vs 239 gL p 0229 Wilcoxon) (figure) For each patient we alsoanalyzed the relationship between NSE and EEGfindings using the 3 main EEG abnormalities addedtogether to obtain an EEG sum score a strong corre-lation was found between NSE and EEG findings(Spearman rho 045 p 0001)
EEG features In the 61 included patients EEG dur-ing hypothermia was initiated after mean of 154hours (SD 58 hours) following CA During TH29 patients had a continuous EEG monitoring and32 were assessed with routine EEG HypothermicEEG features NSE values and normothermic clini-cal and electrophysiologic variables are given accord-ing to the functional outcome assessed at 3 monthsin table 2 Occurrence of abnormal EEG findingsduring TH differed clearly between the 2 outcomegroups (p 0001 Wilcoxon rank-sum) Of note
Table 1 Characteristics of 61 patients treatedafter cardiac arrest with EEGrecorded during hypothermia andserum NSE values
Demographics Values
Age y mean (SD) 637 (122)
Female n () 18 (30)
Cardiologic variables
Non VF cardiac arrest n () 21 (34)
Time to ROSC mean (SD) 227 (139)
Outcome
In-hospital mortality n () 2561 (41)
CPC 1ndash2 at 3 months n () 2861 (46)
Abbreviations CPC Cerebral Performance CategoriesNSE neuron-specific enolase ROSC return of sponta-neous circulation VF ventricular fibrillation
Figure Associations between serum neuron-specific enolase (NSE) and EEG duringtherapeutic hypothermia
Box plots represent serum NSE values (in gL y-axis) stratified according to EEG findings including background reactiv-ity background continuity and epileptiform activity Box plots represent median (horizontal lines) and 25thndash75th percen-tiles bars represent 10thndash90th percentiles
798 Neurology 78 March 13 2012
all patients with epileptiform transients also had anonreactive EEG background Two of 23 (9) sub-jects without EEG reactivity during TH recoveredreactivity after rewarming however both of themdied despite intensive care support for at least 5 addi-tional days While in patients who had a continuousmonitoring EEG recording was started earlier thanin those who had routine EEG (135 hours vs 171hours p 0015 t test) assessment of EEG reactiv-ity was performed at least 6 hours after CA in allpatients this is reflected by a similar prevalence ofabsent EEG background reactivity (1129 vs 1232p 097 2) and a comparable mortality rate(1229 vs 1332 p 095 2)
NSE Serum NSE was measured at least once in all61 studied subjects patients (n 28) with a CPC1ndash2 had lower serum NSE peak levels than those(n 33) with a CPC 3ndash5 at 3 months (see table 2p 0001 Wilcoxon rank-sum) Of note a totalof 5 survivors (328 subjects with CPC 1ndash2 and26 patients with CPC 3) had serum NSE levelsabove 33 gL (335 356 51 and 401 404gL respectively)
DISCUSSION The principal finding of this study isthat early abnormal EEG findings during TH corre-late strongly with peak serum NSE levels at 24ndash48hours after CA To our knowledge this is the first
clinical study showing an early correlation betweenmultichannel EEG alterations and a serum marker ofpostanoxic brain injury and these findings expandprevious observations demonstrating the value ofEEG in patients with hypoxic-ischemic encephalop-athy even when performed early in the intrahypo-thermic period Our data also confirm that absentEEG background reactivity and the presence of epi-leptiform transients during TH are strong predictorsof poor outcome after CA and further show thatsurvival after CA with good neurologic recovery ispossible despite serum NSE levels above the AANguidelines cutoff of 33 gL
A preliminary study published in Chinese re-ported an association of EEG background with se-rum NSE values after neonatal hypoxia although nocorrelation analysis was provided16 A recent study on34 comatose adults found an association between aflat or discontinuous bispectral index after TH andNSE levels17 However the relationship between se-rum markers and multichannel EEG during TH hasnot been addressed so far Although elevations ofNSE in the blood may be favored by bloodndashbrainbarrier dysfunction18 animal studies have convinc-ingly demonstrated that serum NSE correlates withstructural neuronal injury rather than transitory neu-ronal dysfunction1920 moreover elevated NSE levelshave been found in conditions related to neuronaldeath in humans such as brain trauma21ndash23 andstroke2425 Thus the present findings suggest thatEEG abnormalities are not simply a sign of transientpost-CA global dysfunction but rather represent apathophysiologic correlate of postanoxic neuronalinjury Pending confirmation in other cohorts ourfindings have important clinical implications as theEEG is a readily available widespread tool In ourcohort EEG lack of reactivity and discontinuousbackground but not the presence of epileptiformdischarges accounted for the relationship of NSEWhile this finding may be due to the relatively lownumber of patients with epileptiform transients itmay also suggest that paroxysmal neuronal firingcannot occur in subjects in whom the cerebral cortexhas sustained a nearly maximal damage the recentScandinavian study that also identified a substantialnumber of patients with status epilepticus and nor-mal NSE seems to corroborate this hypothesis17
In a previous preliminary analysis of continuousEEG during TH8 we found that lack of reactivityepileptiform features and discontinuous backgroundwere 100 predictive of nonawakening from post-anoxic coma Similar findings were described by ourand other groups when EEG was recorded after re-warming3ndash5 Indeed we found in the present studythat 2838 (74) of patients with preserved EEG
Table 2 Clinical characteristics of 61 patients with hypothermic EEGaccording to their neurologic outcome at 3 months
CPC 1ndash2(28 patients)
CPC 3ndash5(33 patients)
EEG unfavorable features (during hypothermia)
a Nonreactive background n () 0 23 (70)
b Discontinuous background (burst-suppression)n ()
2 (7) 26 (79)
c Epileptiform transients n ()a 0 10 (30)
Sum of EEG unfavorable features (andashc) median(range)b
0 (0ndash1) 2 (0ndash3)
Other clinical and electrophysiologic variables(in normothermic conditions after hypothermia)
Incomplete return of brainstem reflexes n () 3 (11) 21 (64)
Myoclonus n () 2 (7) 7 (21)
Extension or no motor response to pain n () 2 (7) 24 (73)
Nonreactive EEG background n () 0 20 (61)
Bilaterally absent N20 on SSEP n ()c 028 1131 (35)
NSE gL median (range) 178 (80ndash510)d 344 (111ndash2910)e
Abbreviations CPC Cerebral Performance Categories NSE neuron-specific enolaseSSEP somatosensory evoked potentialsa All also had a nonreactive backgroundb Of 6 patients with CPC 3 3 had a sum of 0 and 3 of 1 (all with discontinuous back-ground only)c A total of 59 patients assessedd A total of 328 patients had values 33 Le A total of 1733 patients had values 33 L
Neurology 78 March 13 2012 799
reactivity had a favorable neurologic outcome con-firming our previous observations In addition thisstudy provides other important data first discontin-uous EEG is not an obligate predictor of death since428 (14) patients with this pattern awoke and 2had a good neurologic outcome The point-estimateof the false-positive rate (FPR 1 specificity) ofdiscontinuous background for prediction of poorfunctional outcome was 7 and raised to 12 fordeath while the FPR for the other 2 EEG featureswas 0 for both outcome endpoints It has been sug-gested4 that lack of EEG reactivity may reflect awidespread damage of the aminergic reticular acti-vating system26 and thus a severe impairment ofanoxia-resistant brainstem pathways The strongrelationship between increasing EEG abnormali-ties and elevated serum NSE seems to support thishypothesis although further studies aiming to de-termine the exact brain structural damage follow-ing hypoxic-ischemic encephalopathy eg withdiffusion-weighted MRI are needed
Our observation expands previous findings onEEG performed on neurologically normal subjectsduring hypothermia27 describing appearance of peri-odic complexes on a pharyngeal temperature of296 3 degC however anesthetic doses were notreported in that study It is indeed very interesting tonote that in our cohort patients with coma after CAwho received a moderate sedation with midazolamand fentanyl and eventually awoke did not showany periodic pattern Furthermore none of our pa-tients with epileptiform transients recorded under se-dation (thus with drugs that have antiepilepticproperties) and during TH awoke despite furtherspecific antiepileptic treatment This confirms thatthese EEG patterns are probably different from epi-leptiform features appearing off sedation after THwhich do not preclude awakening in some patients1728
Finally although 9 of patients who showed nonreac-tive EEG background during TH recovered EEG reac-tivity after rewarming both died despite continuedintensive care this again emphasizes the strong predic-tive value of early EEG findings
The AAN-recommended serum NSE prognosticcutoff of 33 gL12 is based on a single class I study29
In patients treated with TH these cutoffs have beenconfirmed by some71017 but not all530 groups In thelatter 2 studies cutoff values of serum NSE up to 78gL were necessary to reach an FPR of 0 Ourdata are in line with those observations 5 subjectswith serum NSE 33 gL awoke and 3 had a goodneurologic outcome implying an FPR for poor out-come and death of 11 and 15 respectively Sinceone of the excluded patients (without hypothermicEEG) having an NSE of 75 gL recovered a CPC of
1 the safe cutoff for awakening in our cohort appearssimilar to that previously mentioned30 and suggeststhat TH significantly alters NSE values and thatNSE should not be used alone to predict awakeningfrom CA and TH
This study has some limitations First recordingswere not uniform in terms of time from CA to initi-ation of EEG and duration However EEG reactiv-ity was tested at least 6 hours following CA in allpatients suggesting a homogenous EEG assessmentThis is particularly important since the prehypother-mic era it is known that in the first few hours follow-ing brain anoxia even a flat EEG is not obligatorilypredictive of bad outcome3132 and at least in chil-dren electrographic seizures during TH only developafter at least 6 hours33 Of note EEG reactivity had acomparable prevalence between long- and short-termrecordings and the almost identical mortality ratereflects the homogeneity of the 2 EEG subgroupsarguing against different modalities for treatmentmanagement and measures to interrupt intensivecare This point also underscores that a self-fulfillingprophecy29 of hypothermic EEG features and NSEappears highly unlikely in this analysis as both werenot used to decide on patientsrsquo fate as opposed to arecent study17 This appears to be the best way tominimize this potentially major bias in observationalstudies on patients after CA3 Second EEG was notscored using quantitative analysis raising the possi-bility of subjectivity However this reflects commonclinical practice and the fact that the EEG readerswere blinded to the NSE levels renders a systematicbias unlikely Third serum NSE was not collectedcontinuously but the relatively long half-life of 24hours justifies this practice Fourth NSE does notseem to represent a perfect correlate of neurologicdamage in patients undergoing TH however highNSE values strongly predict a poor functional prog-nosis in our series the positive predictive value fordeath or significant handicap at 3 months was as highas 85 for a cutoff of 33 gL and 100 for acutoff of 52 gL
Presence of early EEG abnormal findings duringhypothermia strongly correlates with elevated levelsof serum NSE at 24ndash48 hours in patients with comaafter cardiac arrest This suggests that EEG back-ground is both a strong pathophysiologic correlate ofcerebral damage after CA and a robust predictor ofoutcome Our findings also argue in favor of a multi-modal prognostication approach where integrationof EEG and NSE to other clinical variables may helpin guiding therapy and clinical decisions during earlycritical care In this setting indeed decisions uponlife support should never been taken on a singleparameter
800 Neurology 78 March 13 2012
AUTHOR CONTRIBUTIONSDr Rossetti collected the data conducted the study drafted the initial
manuscript and carried out statistical analyses Dr Carrera collected the
data reviewed the text for important intellectual content and drafted the
figure Dr Oddo collected the data and reviewed the text for important
intellectual content
ACKNOWLEDGMENTThe authors thank Malin Maeder-Ingvar MD Christine Stahli RN the
EEG fellows and technologists and the ICU fellows for their help in data
collection
DISCLOSUREDr Rossetti has received research support from Pfizer Inc UCB Glaxo-
SmithKline Eisai Inc Janssen and Sandoz Dr Carrera reports no dis-
closures Dr Oddo is supported by a Grant from the European Society of
Intensive Care Medicine (ECCRN Clinical Research Award 2010)
Received June 14 2011 Accepted in final form August 31 2011
REFERENCES1 Al Thenayan E Savard M Sharpe M Norton L Young B
Predictors of poor neurologic outcome after induced mildhypothermia following cardiac arrest Neurology 2008711535ndash1537
2 Samaniego EA Mlynash M Caulfield AF Eyngorn I Wi-jman CA Sedation confounds outcome prediction in car-diac arrest survivors treated with hypothermia NeurocritCare (in press 2012)
3 Rossetti AO Oddo M Logroscino G Kaplan PW Prog-nostication after cardiac arrest and hypothermia a pro-spective study Ann Neurol 201067301ndash307
4 Thenayan EA Savard M Sharpe MD Norton L YoungB Electroencephalogram for prognosis after cardiac arrestJ Crit Care 201025300ndash304
5 Fugate JE Wijdicks EF Mandrekar J et al Predictors ofneurologic outcome in hypothermia after cardiac arrestAnn Neurol 201068907ndash914
6 Wennervirta JE Ermes MJ Tiainen SM et alHypothermia-treated cardiac arrest patients with goodneurological outcome differ early in quantitative variablesof EEG suppression and epileptiform activity Crit CareMed 2009372427ndash2435
7 Rundgren M Rosen I Friberg H Amplitude-integratedEEG (aEEG) predicts outcome after cardiac arrest and in-duced hypothermia Intens Care Med 200632836ndash842
8 Rossetti AO Urbano LA Delodder F Kaplan PW OddoM Prognostic value of continuous EEG monitoring dur-ing therapeutic hypothermia after cardiac arrest Crit Care201014R173
9 Schmechel D Marangos PJ Brightman M Neurone-specific enolase is a molecular marker for peripheral andcentral neuroendocrine cells Nature 1978276834ndash836
10 Oksanen T Tiainen M Skrifvars MB et al Predictivepower of serum NSE and OHCA score regarding 6-monthneurologic outcome after out-of-hospital ventricular fibril-lation and therapeutic hypothermia Resuscitation 200980165ndash170
11 Shinozaki K Oda S Sadahiro T et al S-100B andneuron-specific enolase as predictors of neurological out-come in patients after cardiac arrest and return of sponta-neous circulation a systematic review Crit Care 200913R121
12 Wijdicks EF Hijdra A Young GB Bassetti CL Wiebe SPractice parameter prediction of outcome in comatose
survivors after cardiopulmonary resuscitation (an evidence-based review) report of the Quality Standards Subcommitteeof the American Academy of Neurology Neurology 200667203ndash210
13 Oddo M Ribordy V Feihl F et al Early predictors ofoutcome in comatose survivors of ventricular fibrillationand non-ventricular fibrillation cardiac arrest treated withhypothermia a prospective study Crit Care Med 2008362296ndash2301
14 2005 American Heart Association Guidelines for Cardio-pulmonary Resuscitation and Emergency CardiovascularCare Circulation 2005112IV1ndash203
15 Booth CM Boone RH Tomlinson G Detsky AS Is thispatient dead vegetative or severely neurologically im-paired Assessing outcome for comatose survivors of car-diac arrest JAMA 2004291870ndash879
16 Dai HQ Luo YH [Changes of electroencephalographicbackground patterns and serum neuron specific enolaselevels in neonates with hypoxic-ischemic encephalopathy]Zhongguo Dang Dai Er Ke Za Zhi 200911173ndash176
17 Cronberg T Rundgren M Westhall E et al Neuron-specific enolase correlates with other prognostic markersafter cardiac arrest Neurology 201177623ndash630
18 Tiainen M Roine RO Pettila V Takkunen O Serumneuron-specific enolase and S-100B protein in cardiac ar-rest patients treated with hypothermia Stroke 2003342881ndash2886
19 Hans P Bonhomme V Collette J Moonen G Neuron-specific enolase as a marker of in vitro neuronal damagepart I assessment of neuron-specific enolase as a quantita-tive and specific marker of neuronal damage J NeurosurgAnesthesiol 19935111ndash116
20 Sankar R Shin DH Wasterlain CG Serum neuron-specific enolase is a marker for neuronal damage followingstatus epilepticus in the rat Epilepsy Res 199728129ndash136
21 Vos PE Lamers KJ Hendriks JC et al Glial and neuronalproteins in serum predict outcome after severe traumaticbrain injury Neurology 2004621303ndash1310
22 Berger RP Beers SR Richichi R Wiesman D AdelsonPD Serum biomarker concentrations and outcome afterpediatric traumatic brain injury J Neurotrauma 2007241793ndash1801
23 Naeimi ZS Weinhofer A Sarahrudi K Heinz T Vecsei VPredictive value of S-100B protein and neuron specific-enolase as markers of traumatic brain damage in clinicaluse Brain Inj 200620463ndash468
24 Jauch EC Lindsell C Broderick J Fagan SC Tilley BCLevine SR Association of serial biochemical markers withacute ischemic stroke the National Institute of Neurologi-cal Disorders and Stroke recombinant tissue plasminogenactivator Stroke Study Stroke 2006372508ndash2513
25 Oh SH Lee JG Na SJ Park JH Choi YC Kim WJPrediction of early clinical severity and extent of neuronaldamage in anterior-circulation infarction using the initialserum neuron-specific enolase level Arch Neurol 20036037ndash41
26 Vincent SR The ascending reticular activating systemndashfrom aminergic neurons to nitric oxide J Chem Neuro-anat 20001823ndash30
27 Stecker MM Cheung AT Pochettino A et al Deep hypo-thermic circulatory arrest I Effects of cooling on electro-encephalogram and evoked potentials Ann Thorac Surg20017114ndash21
Neurology 78 March 13 2012 801
28 Rossetti AO Oddo M Liaudet L Kaplan PW Predictorsof awakening from postanoxic status epilepticus after ther-apeutic hypothermia Neurology 200972744ndash749
29 Zandbergen EG Hijdra A Koelman JH et al Predictionof poor outcome within the first 3 days of postanoxiccoma Neurology 20066662ndash68
30 Steffen IG Hasper D Ploner CJ et al Mild therapeutichypothermia alters neuron specific enolase as an outcomepredictor after resuscitation 97 prospective hypothermiapatients compared to 133 historical non-hypothermia pa-tients Crit Care 201014R69
31 Bassetti C Bomio F Mathis J Hess CW Early prognosisin coma after cardiac arrest a prospective clinical electro-physiological and biochemical study of 60 patients J Neu-rol Neurosurg Psychiatry 199661610ndash615
32 Jorgensen EO Technical contribution Requirements forrecording the EEG at high sensitivity in suspected braindeath Electroencephalogr Clin Neurophysiol 19743665ndash69
33 Abend NS Topjian A Ichord R et al Electroencephalo-graphic monitoring during hypothermia after pediatriccardiac arrest Neurology 2009721931ndash1940
Refresh Your Annual Meeting Experience with New2012 AAN On Demand
More than 600 hours of cutting-edge educational content and breakthrough scientific research
Online access within 24 hours of end of program
Mobile streaming for most iPadreg iPhonereg and Androidreg devices
USB Flash Drive offers convenient offline access (shipped after the Annual Meeting)
Enhanced browser search and improved interface for better overall experience
Get a great value with special pricing on AAN On Demand and the Syllabi on CDPre-order and save up to $1200 Learn more at wwwaancomviewondemand2
Editorrsquos Note to Authors and Readers Levels of Evidence in Neurologyreg
Effective January 15 2009 authors submitting Articles or ClinicalScientific Notes to Neurologyreg
that report on clinical therapeutic studies must state the study type the primary research ques-tion(s) and the classification of level of evidence assigned to each question based on the AANclassification scheme requirements While the authors will initially assign a level of evidence thefinal level will be adjudicated by an independent team prior to publication Ultimately these levelscan be translated into classes of recommendations for clinical care For more information pleaseaccess the articles and the editorial on the use of classification of levels of evidence published inNeurology1-3
1 French J Gronseth G Lost in a jungle of evidence we need a compass Neurology 2008711634ndash1638
2 Gronseth G French J Practice parameters and technology assessments what they are what they are not and why youshould care Neurology 2008711639ndash1643
3 Gross RA Johnston KC Levels of evidence taking Neurologyreg to the next level Neurology 2009728ndash10
802 Neurology 78 March 13 2012
DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
ServicesUpdated Information amp
httpwwwneurologyorgcontent7811796fullhtmlincluding high resolution figures can be found at
Supplementary Material
e318249f6bbDC1htmlhttpwwwneurologyorgcontentsuppl20120209WNL0b013Supplementary material can be found at
References
httpwwwneurologyorgcontent7811796fullhtmlref-list-1at This article cites 32 articles 10 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7811796fullhtmlotherartiThis article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionprognosisPrognosis
httpwwwneurologyorgcgicollectioneeg_EEG
ease_strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

ing TH and 1 lacked NSE data Table 1 illustratesdemographic clinical characteristics and the out-come of the remaining 61 subjects included in thepresent analysis 23 of them were part of a previ-ously published series8 which did not addressNSE In the majority of patients CA was due toVF In-hospital mortality was 2561 (41) and2834 (82) survivors assessed at 3 monthsreached a good neurologic outcome (CPC 1ndash2)while 6 had CPC 3 and 2 additional patients diedIn-hospital mortality of excluded patients did not
differ from that of the studied group (818 vs 2561 p 043 2)
Correlation between EEG and NSE Considering sig-nificance conservatively at p 0016 (3 compari-sons) median NSE peak values were higher inpatients with unreactive EEG background (93 vs 18gL p 0001 Wilcoxon) and discontinuous(burst-suppression) patterns (633 vs 197 gL p 0001 Wilcoxon) In contrast only some trendtoward higher serum NSE levels in patients with epilep-tiform discharges was found (295 vs 239 gL p 0229 Wilcoxon) (figure) For each patient we alsoanalyzed the relationship between NSE and EEGfindings using the 3 main EEG abnormalities addedtogether to obtain an EEG sum score a strong corre-lation was found between NSE and EEG findings(Spearman rho 045 p 0001)
EEG features In the 61 included patients EEG dur-ing hypothermia was initiated after mean of 154hours (SD 58 hours) following CA During TH29 patients had a continuous EEG monitoring and32 were assessed with routine EEG HypothermicEEG features NSE values and normothermic clini-cal and electrophysiologic variables are given accord-ing to the functional outcome assessed at 3 monthsin table 2 Occurrence of abnormal EEG findingsduring TH differed clearly between the 2 outcomegroups (p 0001 Wilcoxon rank-sum) Of note
Table 1 Characteristics of 61 patients treatedafter cardiac arrest with EEGrecorded during hypothermia andserum NSE values
Demographics Values
Age y mean (SD) 637 (122)
Female n () 18 (30)
Cardiologic variables
Non VF cardiac arrest n () 21 (34)
Time to ROSC mean (SD) 227 (139)
Outcome
In-hospital mortality n () 2561 (41)
CPC 1ndash2 at 3 months n () 2861 (46)
Abbreviations CPC Cerebral Performance CategoriesNSE neuron-specific enolase ROSC return of sponta-neous circulation VF ventricular fibrillation
Figure Associations between serum neuron-specific enolase (NSE) and EEG duringtherapeutic hypothermia
Box plots represent serum NSE values (in gL y-axis) stratified according to EEG findings including background reactiv-ity background continuity and epileptiform activity Box plots represent median (horizontal lines) and 25thndash75th percen-tiles bars represent 10thndash90th percentiles
798 Neurology 78 March 13 2012
all patients with epileptiform transients also had anonreactive EEG background Two of 23 (9) sub-jects without EEG reactivity during TH recoveredreactivity after rewarming however both of themdied despite intensive care support for at least 5 addi-tional days While in patients who had a continuousmonitoring EEG recording was started earlier thanin those who had routine EEG (135 hours vs 171hours p 0015 t test) assessment of EEG reactiv-ity was performed at least 6 hours after CA in allpatients this is reflected by a similar prevalence ofabsent EEG background reactivity (1129 vs 1232p 097 2) and a comparable mortality rate(1229 vs 1332 p 095 2)
NSE Serum NSE was measured at least once in all61 studied subjects patients (n 28) with a CPC1ndash2 had lower serum NSE peak levels than those(n 33) with a CPC 3ndash5 at 3 months (see table 2p 0001 Wilcoxon rank-sum) Of note a totalof 5 survivors (328 subjects with CPC 1ndash2 and26 patients with CPC 3) had serum NSE levelsabove 33 gL (335 356 51 and 401 404gL respectively)
DISCUSSION The principal finding of this study isthat early abnormal EEG findings during TH corre-late strongly with peak serum NSE levels at 24ndash48hours after CA To our knowledge this is the first
clinical study showing an early correlation betweenmultichannel EEG alterations and a serum marker ofpostanoxic brain injury and these findings expandprevious observations demonstrating the value ofEEG in patients with hypoxic-ischemic encephalop-athy even when performed early in the intrahypo-thermic period Our data also confirm that absentEEG background reactivity and the presence of epi-leptiform transients during TH are strong predictorsof poor outcome after CA and further show thatsurvival after CA with good neurologic recovery ispossible despite serum NSE levels above the AANguidelines cutoff of 33 gL
A preliminary study published in Chinese re-ported an association of EEG background with se-rum NSE values after neonatal hypoxia although nocorrelation analysis was provided16 A recent study on34 comatose adults found an association between aflat or discontinuous bispectral index after TH andNSE levels17 However the relationship between se-rum markers and multichannel EEG during TH hasnot been addressed so far Although elevations ofNSE in the blood may be favored by bloodndashbrainbarrier dysfunction18 animal studies have convinc-ingly demonstrated that serum NSE correlates withstructural neuronal injury rather than transitory neu-ronal dysfunction1920 moreover elevated NSE levelshave been found in conditions related to neuronaldeath in humans such as brain trauma21ndash23 andstroke2425 Thus the present findings suggest thatEEG abnormalities are not simply a sign of transientpost-CA global dysfunction but rather represent apathophysiologic correlate of postanoxic neuronalinjury Pending confirmation in other cohorts ourfindings have important clinical implications as theEEG is a readily available widespread tool In ourcohort EEG lack of reactivity and discontinuousbackground but not the presence of epileptiformdischarges accounted for the relationship of NSEWhile this finding may be due to the relatively lownumber of patients with epileptiform transients itmay also suggest that paroxysmal neuronal firingcannot occur in subjects in whom the cerebral cortexhas sustained a nearly maximal damage the recentScandinavian study that also identified a substantialnumber of patients with status epilepticus and nor-mal NSE seems to corroborate this hypothesis17
In a previous preliminary analysis of continuousEEG during TH8 we found that lack of reactivityepileptiform features and discontinuous backgroundwere 100 predictive of nonawakening from post-anoxic coma Similar findings were described by ourand other groups when EEG was recorded after re-warming3ndash5 Indeed we found in the present studythat 2838 (74) of patients with preserved EEG
Table 2 Clinical characteristics of 61 patients with hypothermic EEGaccording to their neurologic outcome at 3 months
CPC 1ndash2(28 patients)
CPC 3ndash5(33 patients)
EEG unfavorable features (during hypothermia)
a Nonreactive background n () 0 23 (70)
b Discontinuous background (burst-suppression)n ()
2 (7) 26 (79)
c Epileptiform transients n ()a 0 10 (30)
Sum of EEG unfavorable features (andashc) median(range)b
0 (0ndash1) 2 (0ndash3)
Other clinical and electrophysiologic variables(in normothermic conditions after hypothermia)
Incomplete return of brainstem reflexes n () 3 (11) 21 (64)
Myoclonus n () 2 (7) 7 (21)
Extension or no motor response to pain n () 2 (7) 24 (73)
Nonreactive EEG background n () 0 20 (61)
Bilaterally absent N20 on SSEP n ()c 028 1131 (35)
NSE gL median (range) 178 (80ndash510)d 344 (111ndash2910)e
Abbreviations CPC Cerebral Performance Categories NSE neuron-specific enolaseSSEP somatosensory evoked potentialsa All also had a nonreactive backgroundb Of 6 patients with CPC 3 3 had a sum of 0 and 3 of 1 (all with discontinuous back-ground only)c A total of 59 patients assessedd A total of 328 patients had values 33 Le A total of 1733 patients had values 33 L
Neurology 78 March 13 2012 799
reactivity had a favorable neurologic outcome con-firming our previous observations In addition thisstudy provides other important data first discontin-uous EEG is not an obligate predictor of death since428 (14) patients with this pattern awoke and 2had a good neurologic outcome The point-estimateof the false-positive rate (FPR 1 specificity) ofdiscontinuous background for prediction of poorfunctional outcome was 7 and raised to 12 fordeath while the FPR for the other 2 EEG featureswas 0 for both outcome endpoints It has been sug-gested4 that lack of EEG reactivity may reflect awidespread damage of the aminergic reticular acti-vating system26 and thus a severe impairment ofanoxia-resistant brainstem pathways The strongrelationship between increasing EEG abnormali-ties and elevated serum NSE seems to support thishypothesis although further studies aiming to de-termine the exact brain structural damage follow-ing hypoxic-ischemic encephalopathy eg withdiffusion-weighted MRI are needed
Our observation expands previous findings onEEG performed on neurologically normal subjectsduring hypothermia27 describing appearance of peri-odic complexes on a pharyngeal temperature of296 3 degC however anesthetic doses were notreported in that study It is indeed very interesting tonote that in our cohort patients with coma after CAwho received a moderate sedation with midazolamand fentanyl and eventually awoke did not showany periodic pattern Furthermore none of our pa-tients with epileptiform transients recorded under se-dation (thus with drugs that have antiepilepticproperties) and during TH awoke despite furtherspecific antiepileptic treatment This confirms thatthese EEG patterns are probably different from epi-leptiform features appearing off sedation after THwhich do not preclude awakening in some patients1728
Finally although 9 of patients who showed nonreac-tive EEG background during TH recovered EEG reac-tivity after rewarming both died despite continuedintensive care this again emphasizes the strong predic-tive value of early EEG findings
The AAN-recommended serum NSE prognosticcutoff of 33 gL12 is based on a single class I study29
In patients treated with TH these cutoffs have beenconfirmed by some71017 but not all530 groups In thelatter 2 studies cutoff values of serum NSE up to 78gL were necessary to reach an FPR of 0 Ourdata are in line with those observations 5 subjectswith serum NSE 33 gL awoke and 3 had a goodneurologic outcome implying an FPR for poor out-come and death of 11 and 15 respectively Sinceone of the excluded patients (without hypothermicEEG) having an NSE of 75 gL recovered a CPC of
1 the safe cutoff for awakening in our cohort appearssimilar to that previously mentioned30 and suggeststhat TH significantly alters NSE values and thatNSE should not be used alone to predict awakeningfrom CA and TH
This study has some limitations First recordingswere not uniform in terms of time from CA to initi-ation of EEG and duration However EEG reactiv-ity was tested at least 6 hours following CA in allpatients suggesting a homogenous EEG assessmentThis is particularly important since the prehypother-mic era it is known that in the first few hours follow-ing brain anoxia even a flat EEG is not obligatorilypredictive of bad outcome3132 and at least in chil-dren electrographic seizures during TH only developafter at least 6 hours33 Of note EEG reactivity had acomparable prevalence between long- and short-termrecordings and the almost identical mortality ratereflects the homogeneity of the 2 EEG subgroupsarguing against different modalities for treatmentmanagement and measures to interrupt intensivecare This point also underscores that a self-fulfillingprophecy29 of hypothermic EEG features and NSEappears highly unlikely in this analysis as both werenot used to decide on patientsrsquo fate as opposed to arecent study17 This appears to be the best way tominimize this potentially major bias in observationalstudies on patients after CA3 Second EEG was notscored using quantitative analysis raising the possi-bility of subjectivity However this reflects commonclinical practice and the fact that the EEG readerswere blinded to the NSE levels renders a systematicbias unlikely Third serum NSE was not collectedcontinuously but the relatively long half-life of 24hours justifies this practice Fourth NSE does notseem to represent a perfect correlate of neurologicdamage in patients undergoing TH however highNSE values strongly predict a poor functional prog-nosis in our series the positive predictive value fordeath or significant handicap at 3 months was as highas 85 for a cutoff of 33 gL and 100 for acutoff of 52 gL
Presence of early EEG abnormal findings duringhypothermia strongly correlates with elevated levelsof serum NSE at 24ndash48 hours in patients with comaafter cardiac arrest This suggests that EEG back-ground is both a strong pathophysiologic correlate ofcerebral damage after CA and a robust predictor ofoutcome Our findings also argue in favor of a multi-modal prognostication approach where integrationof EEG and NSE to other clinical variables may helpin guiding therapy and clinical decisions during earlycritical care In this setting indeed decisions uponlife support should never been taken on a singleparameter
800 Neurology 78 March 13 2012
AUTHOR CONTRIBUTIONSDr Rossetti collected the data conducted the study drafted the initial
manuscript and carried out statistical analyses Dr Carrera collected the
data reviewed the text for important intellectual content and drafted the
figure Dr Oddo collected the data and reviewed the text for important
intellectual content
ACKNOWLEDGMENTThe authors thank Malin Maeder-Ingvar MD Christine Stahli RN the
EEG fellows and technologists and the ICU fellows for their help in data
collection
DISCLOSUREDr Rossetti has received research support from Pfizer Inc UCB Glaxo-
SmithKline Eisai Inc Janssen and Sandoz Dr Carrera reports no dis-
closures Dr Oddo is supported by a Grant from the European Society of
Intensive Care Medicine (ECCRN Clinical Research Award 2010)
Received June 14 2011 Accepted in final form August 31 2011
REFERENCES1 Al Thenayan E Savard M Sharpe M Norton L Young B
Predictors of poor neurologic outcome after induced mildhypothermia following cardiac arrest Neurology 2008711535ndash1537
2 Samaniego EA Mlynash M Caulfield AF Eyngorn I Wi-jman CA Sedation confounds outcome prediction in car-diac arrest survivors treated with hypothermia NeurocritCare (in press 2012)
3 Rossetti AO Oddo M Logroscino G Kaplan PW Prog-nostication after cardiac arrest and hypothermia a pro-spective study Ann Neurol 201067301ndash307
4 Thenayan EA Savard M Sharpe MD Norton L YoungB Electroencephalogram for prognosis after cardiac arrestJ Crit Care 201025300ndash304
5 Fugate JE Wijdicks EF Mandrekar J et al Predictors ofneurologic outcome in hypothermia after cardiac arrestAnn Neurol 201068907ndash914
6 Wennervirta JE Ermes MJ Tiainen SM et alHypothermia-treated cardiac arrest patients with goodneurological outcome differ early in quantitative variablesof EEG suppression and epileptiform activity Crit CareMed 2009372427ndash2435
7 Rundgren M Rosen I Friberg H Amplitude-integratedEEG (aEEG) predicts outcome after cardiac arrest and in-duced hypothermia Intens Care Med 200632836ndash842
8 Rossetti AO Urbano LA Delodder F Kaplan PW OddoM Prognostic value of continuous EEG monitoring dur-ing therapeutic hypothermia after cardiac arrest Crit Care201014R173
9 Schmechel D Marangos PJ Brightman M Neurone-specific enolase is a molecular marker for peripheral andcentral neuroendocrine cells Nature 1978276834ndash836
10 Oksanen T Tiainen M Skrifvars MB et al Predictivepower of serum NSE and OHCA score regarding 6-monthneurologic outcome after out-of-hospital ventricular fibril-lation and therapeutic hypothermia Resuscitation 200980165ndash170
11 Shinozaki K Oda S Sadahiro T et al S-100B andneuron-specific enolase as predictors of neurological out-come in patients after cardiac arrest and return of sponta-neous circulation a systematic review Crit Care 200913R121
12 Wijdicks EF Hijdra A Young GB Bassetti CL Wiebe SPractice parameter prediction of outcome in comatose
survivors after cardiopulmonary resuscitation (an evidence-based review) report of the Quality Standards Subcommitteeof the American Academy of Neurology Neurology 200667203ndash210
13 Oddo M Ribordy V Feihl F et al Early predictors ofoutcome in comatose survivors of ventricular fibrillationand non-ventricular fibrillation cardiac arrest treated withhypothermia a prospective study Crit Care Med 2008362296ndash2301
14 2005 American Heart Association Guidelines for Cardio-pulmonary Resuscitation and Emergency CardiovascularCare Circulation 2005112IV1ndash203
15 Booth CM Boone RH Tomlinson G Detsky AS Is thispatient dead vegetative or severely neurologically im-paired Assessing outcome for comatose survivors of car-diac arrest JAMA 2004291870ndash879
16 Dai HQ Luo YH [Changes of electroencephalographicbackground patterns and serum neuron specific enolaselevels in neonates with hypoxic-ischemic encephalopathy]Zhongguo Dang Dai Er Ke Za Zhi 200911173ndash176
17 Cronberg T Rundgren M Westhall E et al Neuron-specific enolase correlates with other prognostic markersafter cardiac arrest Neurology 201177623ndash630
18 Tiainen M Roine RO Pettila V Takkunen O Serumneuron-specific enolase and S-100B protein in cardiac ar-rest patients treated with hypothermia Stroke 2003342881ndash2886
19 Hans P Bonhomme V Collette J Moonen G Neuron-specific enolase as a marker of in vitro neuronal damagepart I assessment of neuron-specific enolase as a quantita-tive and specific marker of neuronal damage J NeurosurgAnesthesiol 19935111ndash116
20 Sankar R Shin DH Wasterlain CG Serum neuron-specific enolase is a marker for neuronal damage followingstatus epilepticus in the rat Epilepsy Res 199728129ndash136
21 Vos PE Lamers KJ Hendriks JC et al Glial and neuronalproteins in serum predict outcome after severe traumaticbrain injury Neurology 2004621303ndash1310
22 Berger RP Beers SR Richichi R Wiesman D AdelsonPD Serum biomarker concentrations and outcome afterpediatric traumatic brain injury J Neurotrauma 2007241793ndash1801
23 Naeimi ZS Weinhofer A Sarahrudi K Heinz T Vecsei VPredictive value of S-100B protein and neuron specific-enolase as markers of traumatic brain damage in clinicaluse Brain Inj 200620463ndash468
24 Jauch EC Lindsell C Broderick J Fagan SC Tilley BCLevine SR Association of serial biochemical markers withacute ischemic stroke the National Institute of Neurologi-cal Disorders and Stroke recombinant tissue plasminogenactivator Stroke Study Stroke 2006372508ndash2513
25 Oh SH Lee JG Na SJ Park JH Choi YC Kim WJPrediction of early clinical severity and extent of neuronaldamage in anterior-circulation infarction using the initialserum neuron-specific enolase level Arch Neurol 20036037ndash41
26 Vincent SR The ascending reticular activating systemndashfrom aminergic neurons to nitric oxide J Chem Neuro-anat 20001823ndash30
27 Stecker MM Cheung AT Pochettino A et al Deep hypo-thermic circulatory arrest I Effects of cooling on electro-encephalogram and evoked potentials Ann Thorac Surg20017114ndash21
Neurology 78 March 13 2012 801
28 Rossetti AO Oddo M Liaudet L Kaplan PW Predictorsof awakening from postanoxic status epilepticus after ther-apeutic hypothermia Neurology 200972744ndash749
29 Zandbergen EG Hijdra A Koelman JH et al Predictionof poor outcome within the first 3 days of postanoxiccoma Neurology 20066662ndash68
30 Steffen IG Hasper D Ploner CJ et al Mild therapeutichypothermia alters neuron specific enolase as an outcomepredictor after resuscitation 97 prospective hypothermiapatients compared to 133 historical non-hypothermia pa-tients Crit Care 201014R69
31 Bassetti C Bomio F Mathis J Hess CW Early prognosisin coma after cardiac arrest a prospective clinical electro-physiological and biochemical study of 60 patients J Neu-rol Neurosurg Psychiatry 199661610ndash615
32 Jorgensen EO Technical contribution Requirements forrecording the EEG at high sensitivity in suspected braindeath Electroencephalogr Clin Neurophysiol 19743665ndash69
33 Abend NS Topjian A Ichord R et al Electroencephalo-graphic monitoring during hypothermia after pediatriccardiac arrest Neurology 2009721931ndash1940
Refresh Your Annual Meeting Experience with New2012 AAN On Demand
More than 600 hours of cutting-edge educational content and breakthrough scientific research
Online access within 24 hours of end of program
Mobile streaming for most iPadreg iPhonereg and Androidreg devices
USB Flash Drive offers convenient offline access (shipped after the Annual Meeting)
Enhanced browser search and improved interface for better overall experience
Get a great value with special pricing on AAN On Demand and the Syllabi on CDPre-order and save up to $1200 Learn more at wwwaancomviewondemand2
Editorrsquos Note to Authors and Readers Levels of Evidence in Neurologyreg
Effective January 15 2009 authors submitting Articles or ClinicalScientific Notes to Neurologyreg
that report on clinical therapeutic studies must state the study type the primary research ques-tion(s) and the classification of level of evidence assigned to each question based on the AANclassification scheme requirements While the authors will initially assign a level of evidence thefinal level will be adjudicated by an independent team prior to publication Ultimately these levelscan be translated into classes of recommendations for clinical care For more information pleaseaccess the articles and the editorial on the use of classification of levels of evidence published inNeurology1-3
1 French J Gronseth G Lost in a jungle of evidence we need a compass Neurology 2008711634ndash1638
2 Gronseth G French J Practice parameters and technology assessments what they are what they are not and why youshould care Neurology 2008711639ndash1643
3 Gross RA Johnston KC Levels of evidence taking Neurologyreg to the next level Neurology 2009728ndash10
802 Neurology 78 March 13 2012
DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
ServicesUpdated Information amp
httpwwwneurologyorgcontent7811796fullhtmlincluding high resolution figures can be found at
Supplementary Material
e318249f6bbDC1htmlhttpwwwneurologyorgcontentsuppl20120209WNL0b013Supplementary material can be found at
References
httpwwwneurologyorgcontent7811796fullhtmlref-list-1at This article cites 32 articles 10 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7811796fullhtmlotherartiThis article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionprognosisPrognosis
httpwwwneurologyorgcgicollectioneeg_EEG
ease_strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

all patients with epileptiform transients also had anonreactive EEG background Two of 23 (9) sub-jects without EEG reactivity during TH recoveredreactivity after rewarming however both of themdied despite intensive care support for at least 5 addi-tional days While in patients who had a continuousmonitoring EEG recording was started earlier thanin those who had routine EEG (135 hours vs 171hours p 0015 t test) assessment of EEG reactiv-ity was performed at least 6 hours after CA in allpatients this is reflected by a similar prevalence ofabsent EEG background reactivity (1129 vs 1232p 097 2) and a comparable mortality rate(1229 vs 1332 p 095 2)
NSE Serum NSE was measured at least once in all61 studied subjects patients (n 28) with a CPC1ndash2 had lower serum NSE peak levels than those(n 33) with a CPC 3ndash5 at 3 months (see table 2p 0001 Wilcoxon rank-sum) Of note a totalof 5 survivors (328 subjects with CPC 1ndash2 and26 patients with CPC 3) had serum NSE levelsabove 33 gL (335 356 51 and 401 404gL respectively)
DISCUSSION The principal finding of this study isthat early abnormal EEG findings during TH corre-late strongly with peak serum NSE levels at 24ndash48hours after CA To our knowledge this is the first
clinical study showing an early correlation betweenmultichannel EEG alterations and a serum marker ofpostanoxic brain injury and these findings expandprevious observations demonstrating the value ofEEG in patients with hypoxic-ischemic encephalop-athy even when performed early in the intrahypo-thermic period Our data also confirm that absentEEG background reactivity and the presence of epi-leptiform transients during TH are strong predictorsof poor outcome after CA and further show thatsurvival after CA with good neurologic recovery ispossible despite serum NSE levels above the AANguidelines cutoff of 33 gL
A preliminary study published in Chinese re-ported an association of EEG background with se-rum NSE values after neonatal hypoxia although nocorrelation analysis was provided16 A recent study on34 comatose adults found an association between aflat or discontinuous bispectral index after TH andNSE levels17 However the relationship between se-rum markers and multichannel EEG during TH hasnot been addressed so far Although elevations ofNSE in the blood may be favored by bloodndashbrainbarrier dysfunction18 animal studies have convinc-ingly demonstrated that serum NSE correlates withstructural neuronal injury rather than transitory neu-ronal dysfunction1920 moreover elevated NSE levelshave been found in conditions related to neuronaldeath in humans such as brain trauma21ndash23 andstroke2425 Thus the present findings suggest thatEEG abnormalities are not simply a sign of transientpost-CA global dysfunction but rather represent apathophysiologic correlate of postanoxic neuronalinjury Pending confirmation in other cohorts ourfindings have important clinical implications as theEEG is a readily available widespread tool In ourcohort EEG lack of reactivity and discontinuousbackground but not the presence of epileptiformdischarges accounted for the relationship of NSEWhile this finding may be due to the relatively lownumber of patients with epileptiform transients itmay also suggest that paroxysmal neuronal firingcannot occur in subjects in whom the cerebral cortexhas sustained a nearly maximal damage the recentScandinavian study that also identified a substantialnumber of patients with status epilepticus and nor-mal NSE seems to corroborate this hypothesis17
In a previous preliminary analysis of continuousEEG during TH8 we found that lack of reactivityepileptiform features and discontinuous backgroundwere 100 predictive of nonawakening from post-anoxic coma Similar findings were described by ourand other groups when EEG was recorded after re-warming3ndash5 Indeed we found in the present studythat 2838 (74) of patients with preserved EEG
Table 2 Clinical characteristics of 61 patients with hypothermic EEGaccording to their neurologic outcome at 3 months
CPC 1ndash2(28 patients)
CPC 3ndash5(33 patients)
EEG unfavorable features (during hypothermia)
a Nonreactive background n () 0 23 (70)
b Discontinuous background (burst-suppression)n ()
2 (7) 26 (79)
c Epileptiform transients n ()a 0 10 (30)
Sum of EEG unfavorable features (andashc) median(range)b
0 (0ndash1) 2 (0ndash3)
Other clinical and electrophysiologic variables(in normothermic conditions after hypothermia)
Incomplete return of brainstem reflexes n () 3 (11) 21 (64)
Myoclonus n () 2 (7) 7 (21)
Extension or no motor response to pain n () 2 (7) 24 (73)
Nonreactive EEG background n () 0 20 (61)
Bilaterally absent N20 on SSEP n ()c 028 1131 (35)
NSE gL median (range) 178 (80ndash510)d 344 (111ndash2910)e
Abbreviations CPC Cerebral Performance Categories NSE neuron-specific enolaseSSEP somatosensory evoked potentialsa All also had a nonreactive backgroundb Of 6 patients with CPC 3 3 had a sum of 0 and 3 of 1 (all with discontinuous back-ground only)c A total of 59 patients assessedd A total of 328 patients had values 33 Le A total of 1733 patients had values 33 L
Neurology 78 March 13 2012 799
reactivity had a favorable neurologic outcome con-firming our previous observations In addition thisstudy provides other important data first discontin-uous EEG is not an obligate predictor of death since428 (14) patients with this pattern awoke and 2had a good neurologic outcome The point-estimateof the false-positive rate (FPR 1 specificity) ofdiscontinuous background for prediction of poorfunctional outcome was 7 and raised to 12 fordeath while the FPR for the other 2 EEG featureswas 0 for both outcome endpoints It has been sug-gested4 that lack of EEG reactivity may reflect awidespread damage of the aminergic reticular acti-vating system26 and thus a severe impairment ofanoxia-resistant brainstem pathways The strongrelationship between increasing EEG abnormali-ties and elevated serum NSE seems to support thishypothesis although further studies aiming to de-termine the exact brain structural damage follow-ing hypoxic-ischemic encephalopathy eg withdiffusion-weighted MRI are needed
Our observation expands previous findings onEEG performed on neurologically normal subjectsduring hypothermia27 describing appearance of peri-odic complexes on a pharyngeal temperature of296 3 degC however anesthetic doses were notreported in that study It is indeed very interesting tonote that in our cohort patients with coma after CAwho received a moderate sedation with midazolamand fentanyl and eventually awoke did not showany periodic pattern Furthermore none of our pa-tients with epileptiform transients recorded under se-dation (thus with drugs that have antiepilepticproperties) and during TH awoke despite furtherspecific antiepileptic treatment This confirms thatthese EEG patterns are probably different from epi-leptiform features appearing off sedation after THwhich do not preclude awakening in some patients1728
Finally although 9 of patients who showed nonreac-tive EEG background during TH recovered EEG reac-tivity after rewarming both died despite continuedintensive care this again emphasizes the strong predic-tive value of early EEG findings
The AAN-recommended serum NSE prognosticcutoff of 33 gL12 is based on a single class I study29
In patients treated with TH these cutoffs have beenconfirmed by some71017 but not all530 groups In thelatter 2 studies cutoff values of serum NSE up to 78gL were necessary to reach an FPR of 0 Ourdata are in line with those observations 5 subjectswith serum NSE 33 gL awoke and 3 had a goodneurologic outcome implying an FPR for poor out-come and death of 11 and 15 respectively Sinceone of the excluded patients (without hypothermicEEG) having an NSE of 75 gL recovered a CPC of
1 the safe cutoff for awakening in our cohort appearssimilar to that previously mentioned30 and suggeststhat TH significantly alters NSE values and thatNSE should not be used alone to predict awakeningfrom CA and TH
This study has some limitations First recordingswere not uniform in terms of time from CA to initi-ation of EEG and duration However EEG reactiv-ity was tested at least 6 hours following CA in allpatients suggesting a homogenous EEG assessmentThis is particularly important since the prehypother-mic era it is known that in the first few hours follow-ing brain anoxia even a flat EEG is not obligatorilypredictive of bad outcome3132 and at least in chil-dren electrographic seizures during TH only developafter at least 6 hours33 Of note EEG reactivity had acomparable prevalence between long- and short-termrecordings and the almost identical mortality ratereflects the homogeneity of the 2 EEG subgroupsarguing against different modalities for treatmentmanagement and measures to interrupt intensivecare This point also underscores that a self-fulfillingprophecy29 of hypothermic EEG features and NSEappears highly unlikely in this analysis as both werenot used to decide on patientsrsquo fate as opposed to arecent study17 This appears to be the best way tominimize this potentially major bias in observationalstudies on patients after CA3 Second EEG was notscored using quantitative analysis raising the possi-bility of subjectivity However this reflects commonclinical practice and the fact that the EEG readerswere blinded to the NSE levels renders a systematicbias unlikely Third serum NSE was not collectedcontinuously but the relatively long half-life of 24hours justifies this practice Fourth NSE does notseem to represent a perfect correlate of neurologicdamage in patients undergoing TH however highNSE values strongly predict a poor functional prog-nosis in our series the positive predictive value fordeath or significant handicap at 3 months was as highas 85 for a cutoff of 33 gL and 100 for acutoff of 52 gL
Presence of early EEG abnormal findings duringhypothermia strongly correlates with elevated levelsof serum NSE at 24ndash48 hours in patients with comaafter cardiac arrest This suggests that EEG back-ground is both a strong pathophysiologic correlate ofcerebral damage after CA and a robust predictor ofoutcome Our findings also argue in favor of a multi-modal prognostication approach where integrationof EEG and NSE to other clinical variables may helpin guiding therapy and clinical decisions during earlycritical care In this setting indeed decisions uponlife support should never been taken on a singleparameter
800 Neurology 78 March 13 2012
AUTHOR CONTRIBUTIONSDr Rossetti collected the data conducted the study drafted the initial
manuscript and carried out statistical analyses Dr Carrera collected the
data reviewed the text for important intellectual content and drafted the
figure Dr Oddo collected the data and reviewed the text for important
intellectual content
ACKNOWLEDGMENTThe authors thank Malin Maeder-Ingvar MD Christine Stahli RN the
EEG fellows and technologists and the ICU fellows for their help in data
collection
DISCLOSUREDr Rossetti has received research support from Pfizer Inc UCB Glaxo-
SmithKline Eisai Inc Janssen and Sandoz Dr Carrera reports no dis-
closures Dr Oddo is supported by a Grant from the European Society of
Intensive Care Medicine (ECCRN Clinical Research Award 2010)
Received June 14 2011 Accepted in final form August 31 2011
REFERENCES1 Al Thenayan E Savard M Sharpe M Norton L Young B
Predictors of poor neurologic outcome after induced mildhypothermia following cardiac arrest Neurology 2008711535ndash1537
2 Samaniego EA Mlynash M Caulfield AF Eyngorn I Wi-jman CA Sedation confounds outcome prediction in car-diac arrest survivors treated with hypothermia NeurocritCare (in press 2012)
3 Rossetti AO Oddo M Logroscino G Kaplan PW Prog-nostication after cardiac arrest and hypothermia a pro-spective study Ann Neurol 201067301ndash307
4 Thenayan EA Savard M Sharpe MD Norton L YoungB Electroencephalogram for prognosis after cardiac arrestJ Crit Care 201025300ndash304
5 Fugate JE Wijdicks EF Mandrekar J et al Predictors ofneurologic outcome in hypothermia after cardiac arrestAnn Neurol 201068907ndash914
6 Wennervirta JE Ermes MJ Tiainen SM et alHypothermia-treated cardiac arrest patients with goodneurological outcome differ early in quantitative variablesof EEG suppression and epileptiform activity Crit CareMed 2009372427ndash2435
7 Rundgren M Rosen I Friberg H Amplitude-integratedEEG (aEEG) predicts outcome after cardiac arrest and in-duced hypothermia Intens Care Med 200632836ndash842
8 Rossetti AO Urbano LA Delodder F Kaplan PW OddoM Prognostic value of continuous EEG monitoring dur-ing therapeutic hypothermia after cardiac arrest Crit Care201014R173
9 Schmechel D Marangos PJ Brightman M Neurone-specific enolase is a molecular marker for peripheral andcentral neuroendocrine cells Nature 1978276834ndash836
10 Oksanen T Tiainen M Skrifvars MB et al Predictivepower of serum NSE and OHCA score regarding 6-monthneurologic outcome after out-of-hospital ventricular fibril-lation and therapeutic hypothermia Resuscitation 200980165ndash170
11 Shinozaki K Oda S Sadahiro T et al S-100B andneuron-specific enolase as predictors of neurological out-come in patients after cardiac arrest and return of sponta-neous circulation a systematic review Crit Care 200913R121
12 Wijdicks EF Hijdra A Young GB Bassetti CL Wiebe SPractice parameter prediction of outcome in comatose
survivors after cardiopulmonary resuscitation (an evidence-based review) report of the Quality Standards Subcommitteeof the American Academy of Neurology Neurology 200667203ndash210
13 Oddo M Ribordy V Feihl F et al Early predictors ofoutcome in comatose survivors of ventricular fibrillationand non-ventricular fibrillation cardiac arrest treated withhypothermia a prospective study Crit Care Med 2008362296ndash2301
14 2005 American Heart Association Guidelines for Cardio-pulmonary Resuscitation and Emergency CardiovascularCare Circulation 2005112IV1ndash203
15 Booth CM Boone RH Tomlinson G Detsky AS Is thispatient dead vegetative or severely neurologically im-paired Assessing outcome for comatose survivors of car-diac arrest JAMA 2004291870ndash879
16 Dai HQ Luo YH [Changes of electroencephalographicbackground patterns and serum neuron specific enolaselevels in neonates with hypoxic-ischemic encephalopathy]Zhongguo Dang Dai Er Ke Za Zhi 200911173ndash176
17 Cronberg T Rundgren M Westhall E et al Neuron-specific enolase correlates with other prognostic markersafter cardiac arrest Neurology 201177623ndash630
18 Tiainen M Roine RO Pettila V Takkunen O Serumneuron-specific enolase and S-100B protein in cardiac ar-rest patients treated with hypothermia Stroke 2003342881ndash2886
19 Hans P Bonhomme V Collette J Moonen G Neuron-specific enolase as a marker of in vitro neuronal damagepart I assessment of neuron-specific enolase as a quantita-tive and specific marker of neuronal damage J NeurosurgAnesthesiol 19935111ndash116
20 Sankar R Shin DH Wasterlain CG Serum neuron-specific enolase is a marker for neuronal damage followingstatus epilepticus in the rat Epilepsy Res 199728129ndash136
21 Vos PE Lamers KJ Hendriks JC et al Glial and neuronalproteins in serum predict outcome after severe traumaticbrain injury Neurology 2004621303ndash1310
22 Berger RP Beers SR Richichi R Wiesman D AdelsonPD Serum biomarker concentrations and outcome afterpediatric traumatic brain injury J Neurotrauma 2007241793ndash1801
23 Naeimi ZS Weinhofer A Sarahrudi K Heinz T Vecsei VPredictive value of S-100B protein and neuron specific-enolase as markers of traumatic brain damage in clinicaluse Brain Inj 200620463ndash468
24 Jauch EC Lindsell C Broderick J Fagan SC Tilley BCLevine SR Association of serial biochemical markers withacute ischemic stroke the National Institute of Neurologi-cal Disorders and Stroke recombinant tissue plasminogenactivator Stroke Study Stroke 2006372508ndash2513
25 Oh SH Lee JG Na SJ Park JH Choi YC Kim WJPrediction of early clinical severity and extent of neuronaldamage in anterior-circulation infarction using the initialserum neuron-specific enolase level Arch Neurol 20036037ndash41
26 Vincent SR The ascending reticular activating systemndashfrom aminergic neurons to nitric oxide J Chem Neuro-anat 20001823ndash30
27 Stecker MM Cheung AT Pochettino A et al Deep hypo-thermic circulatory arrest I Effects of cooling on electro-encephalogram and evoked potentials Ann Thorac Surg20017114ndash21
Neurology 78 March 13 2012 801
28 Rossetti AO Oddo M Liaudet L Kaplan PW Predictorsof awakening from postanoxic status epilepticus after ther-apeutic hypothermia Neurology 200972744ndash749
29 Zandbergen EG Hijdra A Koelman JH et al Predictionof poor outcome within the first 3 days of postanoxiccoma Neurology 20066662ndash68
30 Steffen IG Hasper D Ploner CJ et al Mild therapeutichypothermia alters neuron specific enolase as an outcomepredictor after resuscitation 97 prospective hypothermiapatients compared to 133 historical non-hypothermia pa-tients Crit Care 201014R69
31 Bassetti C Bomio F Mathis J Hess CW Early prognosisin coma after cardiac arrest a prospective clinical electro-physiological and biochemical study of 60 patients J Neu-rol Neurosurg Psychiatry 199661610ndash615
32 Jorgensen EO Technical contribution Requirements forrecording the EEG at high sensitivity in suspected braindeath Electroencephalogr Clin Neurophysiol 19743665ndash69
33 Abend NS Topjian A Ichord R et al Electroencephalo-graphic monitoring during hypothermia after pediatriccardiac arrest Neurology 2009721931ndash1940
Refresh Your Annual Meeting Experience with New2012 AAN On Demand
More than 600 hours of cutting-edge educational content and breakthrough scientific research
Online access within 24 hours of end of program
Mobile streaming for most iPadreg iPhonereg and Androidreg devices
USB Flash Drive offers convenient offline access (shipped after the Annual Meeting)
Enhanced browser search and improved interface for better overall experience
Get a great value with special pricing on AAN On Demand and the Syllabi on CDPre-order and save up to $1200 Learn more at wwwaancomviewondemand2
Editorrsquos Note to Authors and Readers Levels of Evidence in Neurologyreg
Effective January 15 2009 authors submitting Articles or ClinicalScientific Notes to Neurologyreg
that report on clinical therapeutic studies must state the study type the primary research ques-tion(s) and the classification of level of evidence assigned to each question based on the AANclassification scheme requirements While the authors will initially assign a level of evidence thefinal level will be adjudicated by an independent team prior to publication Ultimately these levelscan be translated into classes of recommendations for clinical care For more information pleaseaccess the articles and the editorial on the use of classification of levels of evidence published inNeurology1-3
1 French J Gronseth G Lost in a jungle of evidence we need a compass Neurology 2008711634ndash1638
2 Gronseth G French J Practice parameters and technology assessments what they are what they are not and why youshould care Neurology 2008711639ndash1643
3 Gross RA Johnston KC Levels of evidence taking Neurologyreg to the next level Neurology 2009728ndash10
802 Neurology 78 March 13 2012
DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
ServicesUpdated Information amp
httpwwwneurologyorgcontent7811796fullhtmlincluding high resolution figures can be found at
Supplementary Material
e318249f6bbDC1htmlhttpwwwneurologyorgcontentsuppl20120209WNL0b013Supplementary material can be found at
References
httpwwwneurologyorgcontent7811796fullhtmlref-list-1at This article cites 32 articles 10 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7811796fullhtmlotherartiThis article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionprognosisPrognosis
httpwwwneurologyorgcgicollectioneeg_EEG
ease_strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

reactivity had a favorable neurologic outcome con-firming our previous observations In addition thisstudy provides other important data first discontin-uous EEG is not an obligate predictor of death since428 (14) patients with this pattern awoke and 2had a good neurologic outcome The point-estimateof the false-positive rate (FPR 1 specificity) ofdiscontinuous background for prediction of poorfunctional outcome was 7 and raised to 12 fordeath while the FPR for the other 2 EEG featureswas 0 for both outcome endpoints It has been sug-gested4 that lack of EEG reactivity may reflect awidespread damage of the aminergic reticular acti-vating system26 and thus a severe impairment ofanoxia-resistant brainstem pathways The strongrelationship between increasing EEG abnormali-ties and elevated serum NSE seems to support thishypothesis although further studies aiming to de-termine the exact brain structural damage follow-ing hypoxic-ischemic encephalopathy eg withdiffusion-weighted MRI are needed
Our observation expands previous findings onEEG performed on neurologically normal subjectsduring hypothermia27 describing appearance of peri-odic complexes on a pharyngeal temperature of296 3 degC however anesthetic doses were notreported in that study It is indeed very interesting tonote that in our cohort patients with coma after CAwho received a moderate sedation with midazolamand fentanyl and eventually awoke did not showany periodic pattern Furthermore none of our pa-tients with epileptiform transients recorded under se-dation (thus with drugs that have antiepilepticproperties) and during TH awoke despite furtherspecific antiepileptic treatment This confirms thatthese EEG patterns are probably different from epi-leptiform features appearing off sedation after THwhich do not preclude awakening in some patients1728
Finally although 9 of patients who showed nonreac-tive EEG background during TH recovered EEG reac-tivity after rewarming both died despite continuedintensive care this again emphasizes the strong predic-tive value of early EEG findings
The AAN-recommended serum NSE prognosticcutoff of 33 gL12 is based on a single class I study29
In patients treated with TH these cutoffs have beenconfirmed by some71017 but not all530 groups In thelatter 2 studies cutoff values of serum NSE up to 78gL were necessary to reach an FPR of 0 Ourdata are in line with those observations 5 subjectswith serum NSE 33 gL awoke and 3 had a goodneurologic outcome implying an FPR for poor out-come and death of 11 and 15 respectively Sinceone of the excluded patients (without hypothermicEEG) having an NSE of 75 gL recovered a CPC of
1 the safe cutoff for awakening in our cohort appearssimilar to that previously mentioned30 and suggeststhat TH significantly alters NSE values and thatNSE should not be used alone to predict awakeningfrom CA and TH
This study has some limitations First recordingswere not uniform in terms of time from CA to initi-ation of EEG and duration However EEG reactiv-ity was tested at least 6 hours following CA in allpatients suggesting a homogenous EEG assessmentThis is particularly important since the prehypother-mic era it is known that in the first few hours follow-ing brain anoxia even a flat EEG is not obligatorilypredictive of bad outcome3132 and at least in chil-dren electrographic seizures during TH only developafter at least 6 hours33 Of note EEG reactivity had acomparable prevalence between long- and short-termrecordings and the almost identical mortality ratereflects the homogeneity of the 2 EEG subgroupsarguing against different modalities for treatmentmanagement and measures to interrupt intensivecare This point also underscores that a self-fulfillingprophecy29 of hypothermic EEG features and NSEappears highly unlikely in this analysis as both werenot used to decide on patientsrsquo fate as opposed to arecent study17 This appears to be the best way tominimize this potentially major bias in observationalstudies on patients after CA3 Second EEG was notscored using quantitative analysis raising the possi-bility of subjectivity However this reflects commonclinical practice and the fact that the EEG readerswere blinded to the NSE levels renders a systematicbias unlikely Third serum NSE was not collectedcontinuously but the relatively long half-life of 24hours justifies this practice Fourth NSE does notseem to represent a perfect correlate of neurologicdamage in patients undergoing TH however highNSE values strongly predict a poor functional prog-nosis in our series the positive predictive value fordeath or significant handicap at 3 months was as highas 85 for a cutoff of 33 gL and 100 for acutoff of 52 gL
Presence of early EEG abnormal findings duringhypothermia strongly correlates with elevated levelsof serum NSE at 24ndash48 hours in patients with comaafter cardiac arrest This suggests that EEG back-ground is both a strong pathophysiologic correlate ofcerebral damage after CA and a robust predictor ofoutcome Our findings also argue in favor of a multi-modal prognostication approach where integrationof EEG and NSE to other clinical variables may helpin guiding therapy and clinical decisions during earlycritical care In this setting indeed decisions uponlife support should never been taken on a singleparameter
800 Neurology 78 March 13 2012
AUTHOR CONTRIBUTIONSDr Rossetti collected the data conducted the study drafted the initial
manuscript and carried out statistical analyses Dr Carrera collected the
data reviewed the text for important intellectual content and drafted the
figure Dr Oddo collected the data and reviewed the text for important
intellectual content
ACKNOWLEDGMENTThe authors thank Malin Maeder-Ingvar MD Christine Stahli RN the
EEG fellows and technologists and the ICU fellows for their help in data
collection
DISCLOSUREDr Rossetti has received research support from Pfizer Inc UCB Glaxo-
SmithKline Eisai Inc Janssen and Sandoz Dr Carrera reports no dis-
closures Dr Oddo is supported by a Grant from the European Society of
Intensive Care Medicine (ECCRN Clinical Research Award 2010)
Received June 14 2011 Accepted in final form August 31 2011
REFERENCES1 Al Thenayan E Savard M Sharpe M Norton L Young B
Predictors of poor neurologic outcome after induced mildhypothermia following cardiac arrest Neurology 2008711535ndash1537
2 Samaniego EA Mlynash M Caulfield AF Eyngorn I Wi-jman CA Sedation confounds outcome prediction in car-diac arrest survivors treated with hypothermia NeurocritCare (in press 2012)
3 Rossetti AO Oddo M Logroscino G Kaplan PW Prog-nostication after cardiac arrest and hypothermia a pro-spective study Ann Neurol 201067301ndash307
4 Thenayan EA Savard M Sharpe MD Norton L YoungB Electroencephalogram for prognosis after cardiac arrestJ Crit Care 201025300ndash304
5 Fugate JE Wijdicks EF Mandrekar J et al Predictors ofneurologic outcome in hypothermia after cardiac arrestAnn Neurol 201068907ndash914
6 Wennervirta JE Ermes MJ Tiainen SM et alHypothermia-treated cardiac arrest patients with goodneurological outcome differ early in quantitative variablesof EEG suppression and epileptiform activity Crit CareMed 2009372427ndash2435
7 Rundgren M Rosen I Friberg H Amplitude-integratedEEG (aEEG) predicts outcome after cardiac arrest and in-duced hypothermia Intens Care Med 200632836ndash842
8 Rossetti AO Urbano LA Delodder F Kaplan PW OddoM Prognostic value of continuous EEG monitoring dur-ing therapeutic hypothermia after cardiac arrest Crit Care201014R173
9 Schmechel D Marangos PJ Brightman M Neurone-specific enolase is a molecular marker for peripheral andcentral neuroendocrine cells Nature 1978276834ndash836
10 Oksanen T Tiainen M Skrifvars MB et al Predictivepower of serum NSE and OHCA score regarding 6-monthneurologic outcome after out-of-hospital ventricular fibril-lation and therapeutic hypothermia Resuscitation 200980165ndash170
11 Shinozaki K Oda S Sadahiro T et al S-100B andneuron-specific enolase as predictors of neurological out-come in patients after cardiac arrest and return of sponta-neous circulation a systematic review Crit Care 200913R121
12 Wijdicks EF Hijdra A Young GB Bassetti CL Wiebe SPractice parameter prediction of outcome in comatose
survivors after cardiopulmonary resuscitation (an evidence-based review) report of the Quality Standards Subcommitteeof the American Academy of Neurology Neurology 200667203ndash210
13 Oddo M Ribordy V Feihl F et al Early predictors ofoutcome in comatose survivors of ventricular fibrillationand non-ventricular fibrillation cardiac arrest treated withhypothermia a prospective study Crit Care Med 2008362296ndash2301
14 2005 American Heart Association Guidelines for Cardio-pulmonary Resuscitation and Emergency CardiovascularCare Circulation 2005112IV1ndash203
15 Booth CM Boone RH Tomlinson G Detsky AS Is thispatient dead vegetative or severely neurologically im-paired Assessing outcome for comatose survivors of car-diac arrest JAMA 2004291870ndash879
16 Dai HQ Luo YH [Changes of electroencephalographicbackground patterns and serum neuron specific enolaselevels in neonates with hypoxic-ischemic encephalopathy]Zhongguo Dang Dai Er Ke Za Zhi 200911173ndash176
17 Cronberg T Rundgren M Westhall E et al Neuron-specific enolase correlates with other prognostic markersafter cardiac arrest Neurology 201177623ndash630
18 Tiainen M Roine RO Pettila V Takkunen O Serumneuron-specific enolase and S-100B protein in cardiac ar-rest patients treated with hypothermia Stroke 2003342881ndash2886
19 Hans P Bonhomme V Collette J Moonen G Neuron-specific enolase as a marker of in vitro neuronal damagepart I assessment of neuron-specific enolase as a quantita-tive and specific marker of neuronal damage J NeurosurgAnesthesiol 19935111ndash116
20 Sankar R Shin DH Wasterlain CG Serum neuron-specific enolase is a marker for neuronal damage followingstatus epilepticus in the rat Epilepsy Res 199728129ndash136
21 Vos PE Lamers KJ Hendriks JC et al Glial and neuronalproteins in serum predict outcome after severe traumaticbrain injury Neurology 2004621303ndash1310
22 Berger RP Beers SR Richichi R Wiesman D AdelsonPD Serum biomarker concentrations and outcome afterpediatric traumatic brain injury J Neurotrauma 2007241793ndash1801
23 Naeimi ZS Weinhofer A Sarahrudi K Heinz T Vecsei VPredictive value of S-100B protein and neuron specific-enolase as markers of traumatic brain damage in clinicaluse Brain Inj 200620463ndash468
24 Jauch EC Lindsell C Broderick J Fagan SC Tilley BCLevine SR Association of serial biochemical markers withacute ischemic stroke the National Institute of Neurologi-cal Disorders and Stroke recombinant tissue plasminogenactivator Stroke Study Stroke 2006372508ndash2513
25 Oh SH Lee JG Na SJ Park JH Choi YC Kim WJPrediction of early clinical severity and extent of neuronaldamage in anterior-circulation infarction using the initialserum neuron-specific enolase level Arch Neurol 20036037ndash41
26 Vincent SR The ascending reticular activating systemndashfrom aminergic neurons to nitric oxide J Chem Neuro-anat 20001823ndash30
27 Stecker MM Cheung AT Pochettino A et al Deep hypo-thermic circulatory arrest I Effects of cooling on electro-encephalogram and evoked potentials Ann Thorac Surg20017114ndash21
Neurology 78 March 13 2012 801
28 Rossetti AO Oddo M Liaudet L Kaplan PW Predictorsof awakening from postanoxic status epilepticus after ther-apeutic hypothermia Neurology 200972744ndash749
29 Zandbergen EG Hijdra A Koelman JH et al Predictionof poor outcome within the first 3 days of postanoxiccoma Neurology 20066662ndash68
30 Steffen IG Hasper D Ploner CJ et al Mild therapeutichypothermia alters neuron specific enolase as an outcomepredictor after resuscitation 97 prospective hypothermiapatients compared to 133 historical non-hypothermia pa-tients Crit Care 201014R69
31 Bassetti C Bomio F Mathis J Hess CW Early prognosisin coma after cardiac arrest a prospective clinical electro-physiological and biochemical study of 60 patients J Neu-rol Neurosurg Psychiatry 199661610ndash615
32 Jorgensen EO Technical contribution Requirements forrecording the EEG at high sensitivity in suspected braindeath Electroencephalogr Clin Neurophysiol 19743665ndash69
33 Abend NS Topjian A Ichord R et al Electroencephalo-graphic monitoring during hypothermia after pediatriccardiac arrest Neurology 2009721931ndash1940
Refresh Your Annual Meeting Experience with New2012 AAN On Demand
More than 600 hours of cutting-edge educational content and breakthrough scientific research
Online access within 24 hours of end of program
Mobile streaming for most iPadreg iPhonereg and Androidreg devices
USB Flash Drive offers convenient offline access (shipped after the Annual Meeting)
Enhanced browser search and improved interface for better overall experience
Get a great value with special pricing on AAN On Demand and the Syllabi on CDPre-order and save up to $1200 Learn more at wwwaancomviewondemand2
Editorrsquos Note to Authors and Readers Levels of Evidence in Neurologyreg
Effective January 15 2009 authors submitting Articles or ClinicalScientific Notes to Neurologyreg
that report on clinical therapeutic studies must state the study type the primary research ques-tion(s) and the classification of level of evidence assigned to each question based on the AANclassification scheme requirements While the authors will initially assign a level of evidence thefinal level will be adjudicated by an independent team prior to publication Ultimately these levelscan be translated into classes of recommendations for clinical care For more information pleaseaccess the articles and the editorial on the use of classification of levels of evidence published inNeurology1-3
1 French J Gronseth G Lost in a jungle of evidence we need a compass Neurology 2008711634ndash1638
2 Gronseth G French J Practice parameters and technology assessments what they are what they are not and why youshould care Neurology 2008711639ndash1643
3 Gross RA Johnston KC Levels of evidence taking Neurologyreg to the next level Neurology 2009728ndash10
802 Neurology 78 March 13 2012
DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
ServicesUpdated Information amp
httpwwwneurologyorgcontent7811796fullhtmlincluding high resolution figures can be found at
Supplementary Material
e318249f6bbDC1htmlhttpwwwneurologyorgcontentsuppl20120209WNL0b013Supplementary material can be found at
References
httpwwwneurologyorgcontent7811796fullhtmlref-list-1at This article cites 32 articles 10 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7811796fullhtmlotherartiThis article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionprognosisPrognosis
httpwwwneurologyorgcgicollectioneeg_EEG
ease_strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

AUTHOR CONTRIBUTIONSDr Rossetti collected the data conducted the study drafted the initial
manuscript and carried out statistical analyses Dr Carrera collected the
data reviewed the text for important intellectual content and drafted the
figure Dr Oddo collected the data and reviewed the text for important
intellectual content
ACKNOWLEDGMENTThe authors thank Malin Maeder-Ingvar MD Christine Stahli RN the
EEG fellows and technologists and the ICU fellows for their help in data
collection
DISCLOSUREDr Rossetti has received research support from Pfizer Inc UCB Glaxo-
SmithKline Eisai Inc Janssen and Sandoz Dr Carrera reports no dis-
closures Dr Oddo is supported by a Grant from the European Society of
Intensive Care Medicine (ECCRN Clinical Research Award 2010)
Received June 14 2011 Accepted in final form August 31 2011
REFERENCES1 Al Thenayan E Savard M Sharpe M Norton L Young B
Predictors of poor neurologic outcome after induced mildhypothermia following cardiac arrest Neurology 2008711535ndash1537
2 Samaniego EA Mlynash M Caulfield AF Eyngorn I Wi-jman CA Sedation confounds outcome prediction in car-diac arrest survivors treated with hypothermia NeurocritCare (in press 2012)
3 Rossetti AO Oddo M Logroscino G Kaplan PW Prog-nostication after cardiac arrest and hypothermia a pro-spective study Ann Neurol 201067301ndash307
4 Thenayan EA Savard M Sharpe MD Norton L YoungB Electroencephalogram for prognosis after cardiac arrestJ Crit Care 201025300ndash304
5 Fugate JE Wijdicks EF Mandrekar J et al Predictors ofneurologic outcome in hypothermia after cardiac arrestAnn Neurol 201068907ndash914
6 Wennervirta JE Ermes MJ Tiainen SM et alHypothermia-treated cardiac arrest patients with goodneurological outcome differ early in quantitative variablesof EEG suppression and epileptiform activity Crit CareMed 2009372427ndash2435
7 Rundgren M Rosen I Friberg H Amplitude-integratedEEG (aEEG) predicts outcome after cardiac arrest and in-duced hypothermia Intens Care Med 200632836ndash842
8 Rossetti AO Urbano LA Delodder F Kaplan PW OddoM Prognostic value of continuous EEG monitoring dur-ing therapeutic hypothermia after cardiac arrest Crit Care201014R173
9 Schmechel D Marangos PJ Brightman M Neurone-specific enolase is a molecular marker for peripheral andcentral neuroendocrine cells Nature 1978276834ndash836
10 Oksanen T Tiainen M Skrifvars MB et al Predictivepower of serum NSE and OHCA score regarding 6-monthneurologic outcome after out-of-hospital ventricular fibril-lation and therapeutic hypothermia Resuscitation 200980165ndash170
11 Shinozaki K Oda S Sadahiro T et al S-100B andneuron-specific enolase as predictors of neurological out-come in patients after cardiac arrest and return of sponta-neous circulation a systematic review Crit Care 200913R121
12 Wijdicks EF Hijdra A Young GB Bassetti CL Wiebe SPractice parameter prediction of outcome in comatose
survivors after cardiopulmonary resuscitation (an evidence-based review) report of the Quality Standards Subcommitteeof the American Academy of Neurology Neurology 200667203ndash210
13 Oddo M Ribordy V Feihl F et al Early predictors ofoutcome in comatose survivors of ventricular fibrillationand non-ventricular fibrillation cardiac arrest treated withhypothermia a prospective study Crit Care Med 2008362296ndash2301
14 2005 American Heart Association Guidelines for Cardio-pulmonary Resuscitation and Emergency CardiovascularCare Circulation 2005112IV1ndash203
15 Booth CM Boone RH Tomlinson G Detsky AS Is thispatient dead vegetative or severely neurologically im-paired Assessing outcome for comatose survivors of car-diac arrest JAMA 2004291870ndash879
16 Dai HQ Luo YH [Changes of electroencephalographicbackground patterns and serum neuron specific enolaselevels in neonates with hypoxic-ischemic encephalopathy]Zhongguo Dang Dai Er Ke Za Zhi 200911173ndash176
17 Cronberg T Rundgren M Westhall E et al Neuron-specific enolase correlates with other prognostic markersafter cardiac arrest Neurology 201177623ndash630
18 Tiainen M Roine RO Pettila V Takkunen O Serumneuron-specific enolase and S-100B protein in cardiac ar-rest patients treated with hypothermia Stroke 2003342881ndash2886
19 Hans P Bonhomme V Collette J Moonen G Neuron-specific enolase as a marker of in vitro neuronal damagepart I assessment of neuron-specific enolase as a quantita-tive and specific marker of neuronal damage J NeurosurgAnesthesiol 19935111ndash116
20 Sankar R Shin DH Wasterlain CG Serum neuron-specific enolase is a marker for neuronal damage followingstatus epilepticus in the rat Epilepsy Res 199728129ndash136
21 Vos PE Lamers KJ Hendriks JC et al Glial and neuronalproteins in serum predict outcome after severe traumaticbrain injury Neurology 2004621303ndash1310
22 Berger RP Beers SR Richichi R Wiesman D AdelsonPD Serum biomarker concentrations and outcome afterpediatric traumatic brain injury J Neurotrauma 2007241793ndash1801
23 Naeimi ZS Weinhofer A Sarahrudi K Heinz T Vecsei VPredictive value of S-100B protein and neuron specific-enolase as markers of traumatic brain damage in clinicaluse Brain Inj 200620463ndash468
24 Jauch EC Lindsell C Broderick J Fagan SC Tilley BCLevine SR Association of serial biochemical markers withacute ischemic stroke the National Institute of Neurologi-cal Disorders and Stroke recombinant tissue plasminogenactivator Stroke Study Stroke 2006372508ndash2513
25 Oh SH Lee JG Na SJ Park JH Choi YC Kim WJPrediction of early clinical severity and extent of neuronaldamage in anterior-circulation infarction using the initialserum neuron-specific enolase level Arch Neurol 20036037ndash41
26 Vincent SR The ascending reticular activating systemndashfrom aminergic neurons to nitric oxide J Chem Neuro-anat 20001823ndash30
27 Stecker MM Cheung AT Pochettino A et al Deep hypo-thermic circulatory arrest I Effects of cooling on electro-encephalogram and evoked potentials Ann Thorac Surg20017114ndash21
Neurology 78 March 13 2012 801
28 Rossetti AO Oddo M Liaudet L Kaplan PW Predictorsof awakening from postanoxic status epilepticus after ther-apeutic hypothermia Neurology 200972744ndash749
29 Zandbergen EG Hijdra A Koelman JH et al Predictionof poor outcome within the first 3 days of postanoxiccoma Neurology 20066662ndash68
30 Steffen IG Hasper D Ploner CJ et al Mild therapeutichypothermia alters neuron specific enolase as an outcomepredictor after resuscitation 97 prospective hypothermiapatients compared to 133 historical non-hypothermia pa-tients Crit Care 201014R69
31 Bassetti C Bomio F Mathis J Hess CW Early prognosisin coma after cardiac arrest a prospective clinical electro-physiological and biochemical study of 60 patients J Neu-rol Neurosurg Psychiatry 199661610ndash615
32 Jorgensen EO Technical contribution Requirements forrecording the EEG at high sensitivity in suspected braindeath Electroencephalogr Clin Neurophysiol 19743665ndash69
33 Abend NS Topjian A Ichord R et al Electroencephalo-graphic monitoring during hypothermia after pediatriccardiac arrest Neurology 2009721931ndash1940
Refresh Your Annual Meeting Experience with New2012 AAN On Demand
More than 600 hours of cutting-edge educational content and breakthrough scientific research
Online access within 24 hours of end of program
Mobile streaming for most iPadreg iPhonereg and Androidreg devices
USB Flash Drive offers convenient offline access (shipped after the Annual Meeting)
Enhanced browser search and improved interface for better overall experience
Get a great value with special pricing on AAN On Demand and the Syllabi on CDPre-order and save up to $1200 Learn more at wwwaancomviewondemand2
Editorrsquos Note to Authors and Readers Levels of Evidence in Neurologyreg
Effective January 15 2009 authors submitting Articles or ClinicalScientific Notes to Neurologyreg
that report on clinical therapeutic studies must state the study type the primary research ques-tion(s) and the classification of level of evidence assigned to each question based on the AANclassification scheme requirements While the authors will initially assign a level of evidence thefinal level will be adjudicated by an independent team prior to publication Ultimately these levelscan be translated into classes of recommendations for clinical care For more information pleaseaccess the articles and the editorial on the use of classification of levels of evidence published inNeurology1-3
1 French J Gronseth G Lost in a jungle of evidence we need a compass Neurology 2008711634ndash1638
2 Gronseth G French J Practice parameters and technology assessments what they are what they are not and why youshould care Neurology 2008711639ndash1643
3 Gross RA Johnston KC Levels of evidence taking Neurologyreg to the next level Neurology 2009728ndash10
802 Neurology 78 March 13 2012
DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
ServicesUpdated Information amp
httpwwwneurologyorgcontent7811796fullhtmlincluding high resolution figures can be found at
Supplementary Material
e318249f6bbDC1htmlhttpwwwneurologyorgcontentsuppl20120209WNL0b013Supplementary material can be found at
References
httpwwwneurologyorgcontent7811796fullhtmlref-list-1at This article cites 32 articles 10 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7811796fullhtmlotherartiThis article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionprognosisPrognosis
httpwwwneurologyorgcgicollectioneeg_EEG
ease_strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

28 Rossetti AO Oddo M Liaudet L Kaplan PW Predictorsof awakening from postanoxic status epilepticus after ther-apeutic hypothermia Neurology 200972744ndash749
29 Zandbergen EG Hijdra A Koelman JH et al Predictionof poor outcome within the first 3 days of postanoxiccoma Neurology 20066662ndash68
30 Steffen IG Hasper D Ploner CJ et al Mild therapeutichypothermia alters neuron specific enolase as an outcomepredictor after resuscitation 97 prospective hypothermiapatients compared to 133 historical non-hypothermia pa-tients Crit Care 201014R69
31 Bassetti C Bomio F Mathis J Hess CW Early prognosisin coma after cardiac arrest a prospective clinical electro-physiological and biochemical study of 60 patients J Neu-rol Neurosurg Psychiatry 199661610ndash615
32 Jorgensen EO Technical contribution Requirements forrecording the EEG at high sensitivity in suspected braindeath Electroencephalogr Clin Neurophysiol 19743665ndash69
33 Abend NS Topjian A Ichord R et al Electroencephalo-graphic monitoring during hypothermia after pediatriccardiac arrest Neurology 2009721931ndash1940
Refresh Your Annual Meeting Experience with New2012 AAN On Demand
More than 600 hours of cutting-edge educational content and breakthrough scientific research
Online access within 24 hours of end of program
Mobile streaming for most iPadreg iPhonereg and Androidreg devices
USB Flash Drive offers convenient offline access (shipped after the Annual Meeting)
Enhanced browser search and improved interface for better overall experience
Get a great value with special pricing on AAN On Demand and the Syllabi on CDPre-order and save up to $1200 Learn more at wwwaancomviewondemand2
Editorrsquos Note to Authors and Readers Levels of Evidence in Neurologyreg
Effective January 15 2009 authors submitting Articles or ClinicalScientific Notes to Neurologyreg
that report on clinical therapeutic studies must state the study type the primary research ques-tion(s) and the classification of level of evidence assigned to each question based on the AANclassification scheme requirements While the authors will initially assign a level of evidence thefinal level will be adjudicated by an independent team prior to publication Ultimately these levelscan be translated into classes of recommendations for clinical care For more information pleaseaccess the articles and the editorial on the use of classification of levels of evidence published inNeurology1-3
1 French J Gronseth G Lost in a jungle of evidence we need a compass Neurology 2008711634ndash1638
2 Gronseth G French J Practice parameters and technology assessments what they are what they are not and why youshould care Neurology 2008711639ndash1643
3 Gross RA Johnston KC Levels of evidence taking Neurologyreg to the next level Neurology 2009728ndash10
802 Neurology 78 March 13 2012
DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
ServicesUpdated Information amp
httpwwwneurologyorgcontent7811796fullhtmlincluding high resolution figures can be found at
Supplementary Material
e318249f6bbDC1htmlhttpwwwneurologyorgcontentsuppl20120209WNL0b013Supplementary material can be found at
References
httpwwwneurologyorgcontent7811796fullhtmlref-list-1at This article cites 32 articles 10 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7811796fullhtmlotherartiThis article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionprognosisPrognosis
httpwwwneurologyorgcgicollectioneeg_EEG
ease_strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

DOI 101212WNL0b013e318249f6bb201278796-802 Published Online before print February 8 2012Neurology
Andrea O Rossetti Emmanuel Carrera and Mauro OddoEarly EEG correlates of neuronal injury after brain anoxia
This information is current as of February 8 2012
ServicesUpdated Information amp
httpwwwneurologyorgcontent7811796fullhtmlincluding high resolution figures can be found at
Supplementary Material
e318249f6bbDC1htmlhttpwwwneurologyorgcontentsuppl20120209WNL0b013Supplementary material can be found at
References
httpwwwneurologyorgcontent7811796fullhtmlref-list-1at This article cites 32 articles 10 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7811796fullhtmlotherartiThis article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionprognosisPrognosis
httpwwwneurologyorgcgicollectioneeg_EEG
ease_strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online