Embed Size (px)
Citation preview
Early Mobility Program: An Interdisciplinary Approach
UMRN Conference Chris Wells, PhD, PT, CCS, ACT
Julie Pittas, DPTStephanie Harte, MPT
Objectives
1. Discuss the clinical problem: Chronic Critical Illness (CCI) & Post Intensive Care Syndrome (PICS)
2. Discuss the current national trends in early mobility
3. Discuss the UMMS Early Mobility Programs
4. Discuss thoughts for next steps
ICU Demographics
Over 5 million patients annually admitted• Respiratory failure• Post operative management• Ischemic heart disease• Sepsis• Heart Failure
Growing rise in geriatric ICU admissions• 1.4 million older adults ICU admissions
SCCM.org; 2015
Contributors to Adverse ICU Outcomes
• Sedation• Prolonged mechanical ventilation• Sleep disturbance• Malnutrition• Medications side effects• Poor pain management• Immobility• Loss of self control & dignity
Chronic Critical Illness
14 days post ICU admissions:• 50% treated for sepsis
• 25 – 30% mortality rate
• 15 -20% will have new cognitive deficits• 40% will have at least 1 new ADL limitation• 80-100% will have persistent skeletal muscle
impairments
SCCM.org; 2015
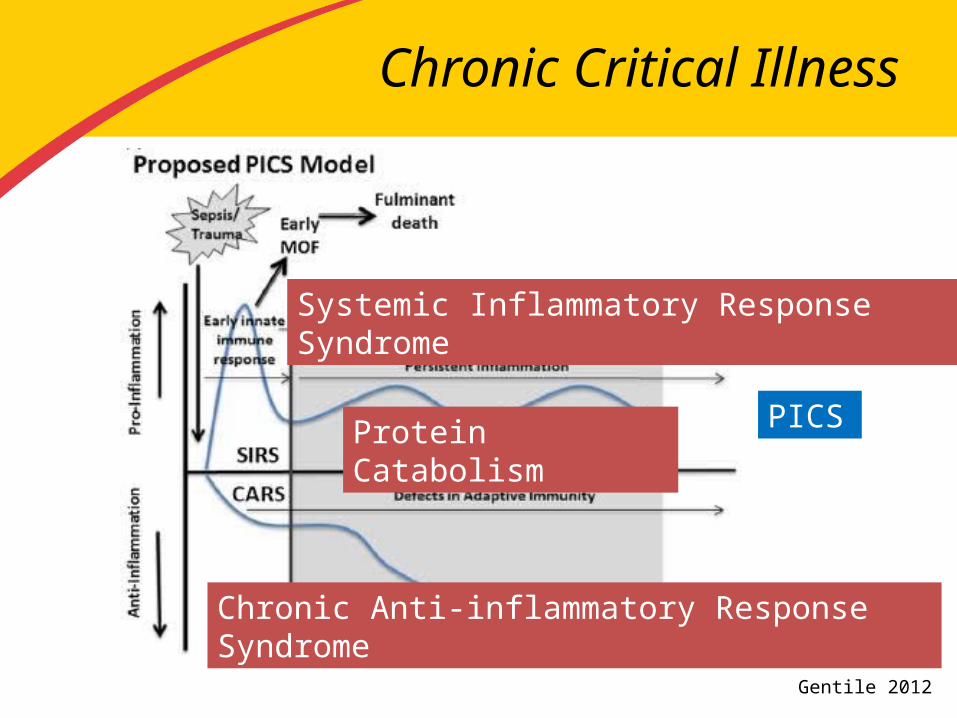
Chronic Critical Illness
Systemic Inflammatory Response Syndrome
Chronic Anti-inflammatory Response Syndrome
Protein Catabolism PICS
Gentile 2012
PICS or Post Sepsis Syndrome (PSS)
Persistent Cognitive Impairments• Modeling mild to moderate TBI or Alzheimer’s
Disease• Impairments in executive function skills
Jackson 2003,Iwashyma 2012
PICS
• Persistent Psychological Problems• 35% PTSD at 2 years• 60% Anxiety• 40% Depression
• 25- 40% still out of work at 1 year
Puthucheary, 2013,Needham 2010; Morris 2008
PICS
• Persistent Muscle Impairment/Functional Limitations
• 50% develop ICU Acquired Weakness in 1week Protein catabolism Protein synthesis Muscle fiber necrosis
PICS
• ICU Acquired Weakness• Prolonged mechanical ventilation• 35 – 45% Functional limitations
Mechanisms:• Atrophy• Mitochondrial dysfunction• Neuromuscular decoupling
Who is at Risk?
• Comorbidities• Age• Mechanical ventilation• Corticosteroid use• ? NM blocking agents
ABCDE Bundle
The ABCDE bundle is a group of evidence-based practices that help to
prevent some of the unintended consequences of hospitalization.
AACN, SCCM
F,G, & H have recently been added to assist with appropriate transition out of ICU
Goals of ABCDE Bundle
• Minimize sedation• Prevent and manage delirium• Liberate from mechanical ventilation• Mitigate effects of immobility• Promote team communication• Involve and educate family
Goal: ICU Liberation
Created by CL Wells, Modified from Putman & Alexander 2011 Desai 2011, Balas 2013
ABCDE Bundle
ABCDE: Early Mobilization
Feasibility, efficacy and safety• Mechanical ventilation supported days• ICU LOS, ? Hospital LOS• Delirium• Functional loss• Improve pulmonary function
Morris 2008, Schweickert, et al., 2009, Needham 2011 – 2013, Hough, 2010
Early Mobility Goals
• Patient activity level
• Hospital associated complications
• Prevent further muscle atrophy/weakness
• LOS
• Improve level of discharge
• Increase awareness about mobility and discharge outcomes

Rise & Shine InitiativeUMMC
Rise & Shine
• Interdisciplinary Committee • Nursing, Physician, Respiratory Therapy, Pharmacy, Information
Technology, Rehabilitation
• Planning began 2012
• Implementation of components Fall 2013
• Initial Focus included all adult ICUs
• Standardized ICU practice when appropriate
Cardiac surgery Cardiology
Medical Surgical
Neurology/Neurosurgery Multi-trauma Neuro-trauma
Rise & Shine
Interdisciplinary Training Components•RN
• Use of Richmond Agitation and Sedation Scale (RASS) and Confusion Assessment Method for the ICU (CAM ICU)
•RT
• Performance and timing of spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT)
•MD/Pharmacy
• New order set
• Pharmacological selection
• Guidelines for administration•Rehab/RN
• Early Mobility Program •Team communication during rounds (daily goals sheet)
Early Mobility Guidelines• Formulated by an interdisciplinary team• Create a framework for:
• LIPs to determine if a patient is appropriate for OOB• Nursing to determine by what means a patient is most appropriate to get OOB and/or ambulate
• Dependent technique• Standing transfer
• Assignment of a Mobility Level to communicate the patient’s mobility status to the interdisciplinary team
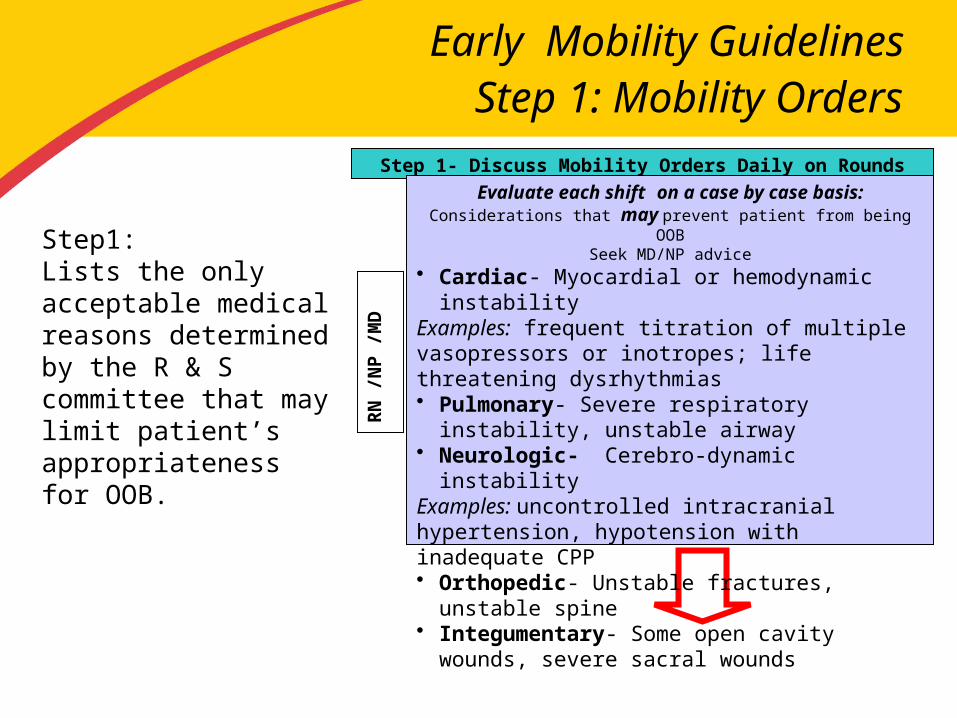
Early Mobility Guidelines Step 1: Mobility Orders
Step1:Lists the only acceptable medical reasons determined by the R & S committee that may limit patient’s appropriateness for OOB.
RN
/N
P /
MD
Step 1- Discuss Mobility Orders Daily on Rounds
Evaluate each shift on a case by case basis:Considerations that may prevent patient from being OOB
Seek MD/NP advice• Cardiac- Myocardial or hemodynamic instability Examples: frequent titration of multiple vasopressors or inotropes; life threatening dysrhythmias• Pulmonary- Severe respiratory instability, unstable
airway • Neurologic- Cerebro-dynamic instabilityExamples: uncontrolled intracranial hypertension, hypotension with inadequate CPP• Orthopedic- Unstable fractures, unstable spine• Integumentary- Some open cavity wounds, severe
sacral wounds
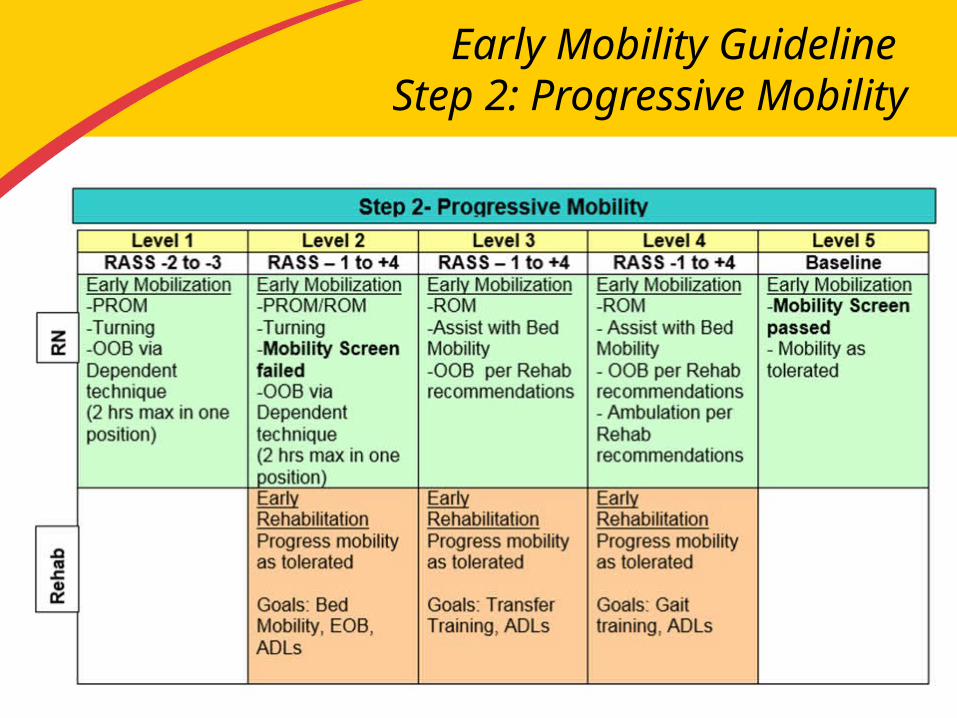
Early Mobility Guideline Step 2: Progressive Mobility
UMMC Mobility Screen
Purpose:• Nursing tool to assess functional ability
Goals for use:• Safe patient handling• Activity engagement • Standardize assessment of patient ability• Communication• Patient handling associated injuries
Utilization of Mobility Screen
Patient safety:• Determine safety for transfers and walking
Staff safety:• Risk of employee injuries
Referrals:• Determine if a PT or OT consult should be
obtained
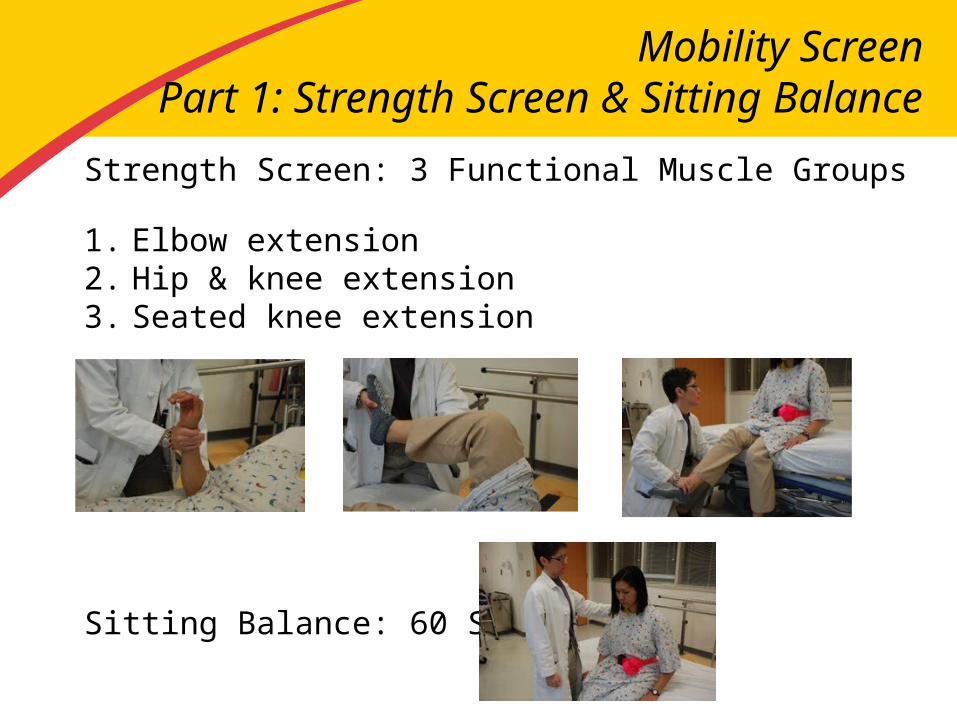
Mobility ScreenPart 1: Strength Screen & Sitting Balance
Strength Screen: 3 Functional Muscle Groups
1. Elbow extension2. Hip & knee extension3. Seated knee extension
Sitting Balance: 60 Seconds
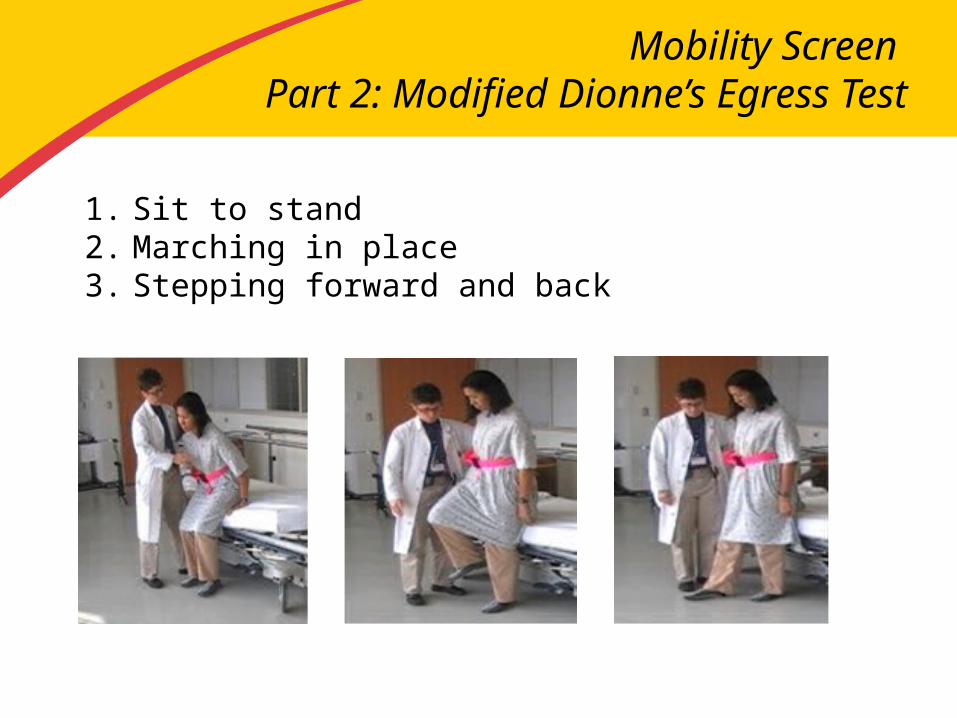
Mobility Screen Part 2: Modified Dionne’s Egress Test
1. Sit to stand2. Marching in place3. Stepping forward and back
Mobility Screen: Nursing Key Factors
Does the patient:
• Follow your commands?
• Push with sufficient force?
• Push throughout the full motion?
When to utilize:
• When initiating OOB activities
• Every shift as indicated
• Change in patient’s status
Mobility Screen Pass =
• Pt able to perform all tasks required throughout entire screen with minimal assistance or less of the nurse• Standing transfer can be performed• Ambulation can be performed
Fail =• Pt is not able to perform a portion of the screen• The screen is halted and a dependent technique is utilized
Mobility Level Signs
RN and rehab shared responsibility for signage

RN Role in Early Mobility Program• Discuss patient readiness for OOB with team
• Assess patient mobility Mobility Screen
• Promote OOB and edge of bed activities
• Perform ROM and ADL activities
• Screen for rehabilitation consults
• Assist rehab services in practice of functional activities as indicated
Rehab Role in Early Mobility Program
• Focus on patients at Mobility Levels 2-4• Progression of mobility per rehab POC• Discharge planning • Mobility recommendations documentation
• Facilitates interdisciplinary POC
University of MD Shore Medical Center at Easton and Dorchester
ABCDE Protocol
ABCDE Protocol Demographics
• Began September 2013• Easton: 10 general ICU beds• Dorchester: combined 8 Tele/ICU beds• Same intensivist covers both hospitals• Some RNs cover both hospitals
Implementation
• Prior to implementation:• Rehabilitation consults at discretion of provider
• High variability of consult timing and OOB activity
• Implementation of protocol driven by nursing• Multidisciplinary committee formed to establish
program- MD, RN, RT, Rehab, PharmD, IT
Early Mobility Safety Screen
• Performed daily by RN
• Assesses basic hemodynamic stability and appropriateness for participation in mobility
• PASS prompts order screen for physical and occupational therapy consult Therapy initiated and mobility progressed as per
therapy plan of care
Nursing Role
• Per policy, RN still has delineated role in early mobility
• A/PROM• Turning/repositioning every 2 hours• Continuous Lateral Rotation and chair position of
bed• EOB x 20 min, 3x/day
Outcomes of Pre and Post Implementation Study
• Decreased prevalence of delirium (UMSMC)• Decreased delirium days (UMSMC)• Increased patient activity level during IMC pilot;
No significant increase noted for ICU (UMMC)
Common Barriers: Implementation and Sustainability
• Inconsistent mobility dialog during patient rounds• Inconsistent rehabilitation presence• Inconsistent completion of mobility screen• Staff turn over• Documentation • Inconsistent placement of OOB orders• Equipment availability, training, and use
Moving Forward
• Assess protocol implementation• Educational model for training of:
Rehabilitation staff Nursing staff
• Compliance with program components
• Creation of sustainability model
Moving Forward
• Assess correlation with appropriate and timely therapy consultation
• Assess influence of program on:
• Staff safety
• Patient safety• Assess for most effective therapy prescription• Determine effective outcome assessment tool • Assess for impact on PICS
Panel Contact Information
Stephanie Harte: [email protected]
Julie Pittas: [email protected]
Christine Provance: [email protected]
Cynthia Roman: [email protected]
Jessica Rossi: [email protected]
Chris Wells: [email protected]
References
Baharestani, M.M, & Ratliff, C.R. Pressure Ulcers in Neonates and Children: An NPUAP White Paper. Advances in Sin & Wound Care, 20(44).
Engel, H. ICU Early Mobilization at UCSF. Retrieved October 9, 2014 from http://ptrehab.ucsf.edu/sites/ptrehab.ucsf.edu/files/documents/Early%20Mobilization%20in%20the%20ICU.pdf
Hough, T. (2010). Early Mobilization in the ICU. Retrieved October 9, 2014 from https://depts.washington.edu/pulmcc/conferences/lungday/Hough%20Mobilization.pdf
Remondini, R., Valerio, N., Barcellos, P., Prado, C., & Santos, E. (2012). Early mobilization in children under invasive and noninvasive positive pressure ventilation: Description and preliminary results of a new protocol. Pediatric and Neonatal Critical Care.
Stevens, P. (2012). Beyond Cosmetic Concerns: Functional Deficits Associate with Deformational Plagiocephaly. Retrieved October 9, 2014 from http://www.oandp.com/articles/2012-04_02.asp
West, L. (2011). Early Mobilization: How one multidisciplinary team initiated an activity protocol to decrease ICU length of stay. Retrieved October 9, 2014 from http://physical-therapy.advanceweb.com/Archives/Article-Archives/Early-Mobilization.aspx
Zafiropoulos, B., Alison, J.A. & McCarren, B. (2004). Physiological responses to the early mobilisation of the intubated, ventilated abdominal surgery patient. Australian Journal of Physiotherapy, 50, 95-100.
References
Bailey, P., Thomsen, G.E., Spuhler, V.J., Blair, R., Jewkes, J., Bezdjian, L., et al. (2007). Early activity is feasible and safe in respiratory failure patients. Critical Care Medicine, 35 (1), p. 139-145.
Herridge, M.S., Cheung, A.M., Tansey, C.M., Matte-Martyn, A., Diaz-Granados, N.D., Al-Saidi, F., et al. (2003). One-year outcomes in survivors of the acute respiratory distress syndrome. The New England Journal of Medicine, 348(8), 683-693.
Morris, P.E., Goad, A., Thompson, C., Taylor, K., Harry, B., Passmore, L., et al. (2008). Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Critical Care Medicine, 36 (8), 2238-2243.
Pohlman, M.C., Schweickert, W.D., Pohlman, A.S., Nigos, C., Pawlik, A.J., et al. (2010). Feasibility of physical and occupational therapy beginning from initiation of mechanical ventilation. Critical Care Medicine, 38 (11), 2089-2094.
Schweickert, W.D., Pohlman, M.C., Pohlman, A.S., Nigos, C., Pawkil, A.J., Esbrook, E.L., et al. (2009). Early physical and occupational therapy in mechanically ventilated, critically ill patients: A randomized controlled trial. Lancet, 373, 1874-1882.
Stevens, R.D., Dowdy, D.W., Michaels, R.K., Mendez-Tellez, P.A., Pronovost, P.J., Needham, D.M. (2007). Neuromuscular dysfunction acquired in critical illness: a systemic review. Intensive Care Med, 33, 1876-1891.