Embed Size (px)
Citation preview

Early Nutrition and Adult Non-communicable diseases: A vital link
that must be broken
Commonwealth Health Ministers’ MeetingWHO, Geneva May 14, 2011
1
Anna Lartey (Associate Professor)Department of Nutrition & Food Science
University of Ghana

2
“…NCD deaths are projected to increase by 15% globally between 2010 and 2020. The greatest increases will be in Africa, the Eastern Mediterranean, and South-East Asia, where they will increase by over 20%”
Global status report on non-communicable disease (WHO, April 2010)

3
Total deaths by broad cause group by WHORegion and by sex
Source: Global status report on non-communicable disease (WHO, April 2010)

4
Age standardized prevalence of diabetes by WHORegion and by sex
Source: Global status report on non-communicable disease (WHO, April 2010)

5
Age standardized prevalence of Hypertension in adults ages 25+ years by WHO Region and by sex
Source: Global status report on non-communicable disease (WHO, April 2010)

6
Age standardized prevalence of overweight in adults ages 20+ years by WHO Region and by sex
Source: Global status report on non-communicable disease (WHO, April 2010)

7
Nutrition Transition

8
Early Nutritional influences on NCDs (Developmental Origins of Adult Health and Disease (DOHAD)
In the last 15 years new information suggest the nutritional influences encountered earlier in life may be of equal importance in determining CVD risk
Maternal nutrition, fetal nutrition and disease in later life (Barker D;1992)

9
Adverse environmental conditions
Fetus
Dies Adaptation to survive
Metabolic/Nutritional Programming

10
Fetal under-nutrition
Brain sparing
Impaired development:Blood vessels, liver, kidney and pancreas
Down regulation of growth
Reduced insulin secretion and sensitivity
Altered Body composition
Reduced Muscle
HyperlipidemiaHypertension
Central Obesity Insulin Resistance
Type 2 Diabetes and CHD in Adult life
Metabolic Programming
Source: C. Fall 2009

11
Evidence in support of Developmentalorigins of disease from animal studies
In rats, maternal diet (protein) restriction in pregnancy
High blood pressureImpaired glucose toleranceInsulin resistanceAltered hepatic function
in the adult offspring
(Woodall et al 1996; Langley et al 1994; Pickard et al 1996)

12
Evidence in support of Developmental origins of disease from Humans
Indian children: study examined that association between LBW and CVD risk factors (Bavdekar, et al 2000)
At 4 years: LBW was associated with higher plasma concglucose after an oral glucose load
At 8 years:LBW children had high LDL cholesterol, higher systolic pressure and insulin resistance

13
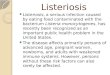
0 10 20 30 40 50 600
10
20
30
40
50
60
70
Regions
South America
Middle America / Caribbean
South East Asia
South Asia
Near East / North Africa
Sub-Saharan Africa
China
Prevalence of Low Birth Weight (%)
Prev
alen
ce o
f stu
ntin
g (%
)
Extracted from: ACC/SCN, 1997
The prevalence of Low Birth Weight and Stunting
Source of slide: R Uauy
Low Birth Weight and Stunting are Related

14
Maternal Underweight & LBW are Related
UN/SCN 6th WNR 2010Source of slide: R Uauy

15
Proportion of babies born low birth weight by region
0
5
10
15
20
25
30
SSA MENA S. ASIA L. America All developing Countries
Pe
rce
nta
ge
Regions
SSA= Sub Saharan Africa; MENA= Middle East and North Africa
Source of data: UNICEF State of the World’s Children, 2009

16
Implications of Developmental origins of adult disease for Developing countries
Identification of critical periods during which conditions can be programmed (-9 to 24mo) raisesconcern about the potential for huge increase in the prevalence of NCDs in low income countries, especially countries going through the nutrition transition.
Good news: We have knowledge on what to do to avoid disease programming in utero and during early infancy.

17
Window of opportunity to break link on nutrition programming (-9 to 24 mo)

18
Early nutrition matters
•Improve maternal nutrition before and during pregnancy (diet is nutrient dense, adequate micronutrients). Adequate maternal diet is
important to break the intergenerational effect of low birth weight

19
Early nutrition matters
Promote Exclusive Breastfeeding
Early nutrition matters

Risk of Overweight in Adolescence by Duration of Breastfeeding in Infancy
1.4
1.2
1.0
0.8
0.6
0.4
1 1- 3 4 - 6 7 - 9 >9
Duration of Breastfeeding (mo)
Odd
s R
atio
(95
% C
I)
Source: Gillman et al., 2001
Protective effect of breastfeeding on obesity

21
Early nutrition matters:Promote adequate complementary feeding
0
5
10
15
20
25
30
35
40
45
Kenya Ghana Zimbabwe Morocco
% o
f chi
ldre
n un
der
5 y
stun
ted
<6 mo 6-<12 mo 12-36 mo >36 mo
Stunting prevalence by age categories (Source of data: Country DHS data)

90% of All Stunted Children Live in Just 36 Countries
PAPER 1

Consequences of stunting
Short termy Increased infant morbidityy Increased perinatal mortalityy Increased risk of maternal
mortalityy Delayed motor developmenty Adverse cognitive
development
Long termy Reduced adult staturey Lower educational attainmenty Lower adult productivity and
income earningsy Increased risk of obesityy Processes leading to stunting
(poor maternal diet) are associated with insulin resistance, diabetes and CVD in offspring later in life
y Inter-generational effects of stunting in girls
23

24
Early nutrition matters:Promote adequate complementary feeding
*Improve the nutritional quality of complementaryfoods (feeding a variety of foods to improve dietary diversity).
*Micronutrient fortified complementary foods may be needed where local complementary food qualityis poor.

y Promotion of Breastfeedingy Complementary feedingy Improved hygienic practicesy Vitamin A supplementationy Zinc supplements for diarrhea
managementy Multiple micronutrient
powdersy De-worming y Iron-folic acid supplements for
pregnant womeny Iodized oil capsules
y Salt iodizationy Iron fortification of staple
foodsy Prevention and treatment of
moderate undernutrition with special foods
y Treatment of severe undernutrition with ready-to-use therapeutic foods (RUTF)
25
Thirteen evidence-based interventions that when scaled up will make a difference(Lancet series 2008)

26
What will it cost to scale up these 13 interventions in high malnutrition burden countries?
Annually: 10.3 billion USD
Benefit: Prevent annually1.1 million deaths,
30 million cases of stunting,Avert the loss of 30 million disability adjusted life years ;Substantial economic gains

27
Scaling Up Nutrition movement
SUN: Scaling Up Nutrition Documents

28
Scaling Up Nutrition movement
Scaling Up Nutrition (SUN) is a framework that lays out a new approach to improving nutrition for mothers and children during the window of opportunity from pregnancy to age two. SUN focuses on 13 key direct nutrition interventions.
SUN is led by a cross-sector, multi-partner Transition Team, chaired by Dr. David Nabarro, Special Representative of the UN Secretary General for Food Security and Nutrition

29
Scaling Up Nutrition movement
SUN works with donors, development agencies, civil society and others within countries and at an international level, to align programs and investments with national plans.

30
Early Riser countries:
These are early adopters of the SUN framework. These countries have committed to establishing national nutrition priorities and developing plans that align with the SUN approach of scaling up Nutrition
Countries must apply with a formal letter of request from a high-ranking government official (e.g. Headof Government or Minister of health) to
David Nabarro: [email protected]
Scaling Up Nutrition movement

31
Early Riser countries:
Ethiopia, Guatemala, Ghana, Laos, Malawi, Mali, Niger, Peru, Uganda, Zambia
Others: Bangladesh, Nepal, Senegal, Tanzania
Scaling Up Nutrition movement

32
Take Home Messages:
Early nutrition matters when addressing NCDs
Take advantage of the window of opportunity (-9-
24 mo) to break the link
As Ministers of Health: take advantage of the SUN
activities and make nutrition a priority