Embed Size (px)
Citation preview

Early Predictors of Corticosteroid Treatment Failure inIcteric Presentations of Autoimmune Hepatitis
Andrew D. Yeoman, Rachel H. Westbrook, Yoh Zen, Paola Maninchedda, Bernard C. Portmann, John Devlin,
John G. O’Grady, Phillip M. Harrison, and Michael A. Heneghan
Autoimmune hepatitis (AIH) typically responds to treatment in 90% of patients. Earlyprediction of treatment outcome would be advantageous in clinical practice. We evaluatedwhether parameters at initiation of therapy or changes in these parameters at day 3 andday 7 following corticosteroid initiation predicted treatment failure. Treatment-naive,jaundiced patients presenting to our tertiary unit between 1999-2009 were identified andmathematical models of prognosis in liver disease scores calculated at day 0, day 3, andday 7. Overall, 72 patients were identified (48 women, 24 men). Treatment failureoccurred in 18% (13/72) of patients. At diagnosis, higher median bilirubin (451 lmol/Lversus 262 lmol/L, P 5 0.02), INR (1.62 versus 1.33, P 5 0.005), model for endstageliver (MELD) score (26 versus 20, P 5 0.02), MELD-sodium (Na) score (27 versus 22,P 5 0.03) and United Kingdom endstage liver disease score (UKELD) score (59 versus 57,P 5 0.01) significantly correlated with treatment failure. Analysis of area under the re-ceiver operator characteristic curve (AUROC) values at day 7 identified change (D) biliru-bin (AUROC 0.68), D creatinine (0.69), D MELD (0.79), D MELD-Na (0.83) and DUKELD (0.83) best predicted treatment failure. Specifically, a fall in UKELD of less than2 points predicted treatment failure with a sensitivity of 85% and specificity of 68%. Of13 treatment failures, nine required second-line immunosuppression, three required emer-gency transplant, and one died of sepsis. In total, four patients died in the treatment fail-ure group compared with one in the responder group (4/13 5 31% versus 1/59 5 1.7%,P 5 0.003). Conclusion: Approximately 20% of icteric AIH presentations fail corticoste-roid therapy. This is associated with significant mortality and the need for emergencytransplantation. Treatment failure is best predicted by change in MELD-Na and UKELDat day 7. Early identification of nonresponders may allow timely escalation of immunosup-pression to prevent clinical deterioration. (HEPATOLOGY 2011;53:926-934)
Standard induction therapy of autoimmune hepa-titis (AIH) typically involves treatment with cor-ticosteroids alone or in combination with aza-
thioprine.1 Responsiveness to immunosuppressive
therapy remains a characteristic feature of the diseaseand has been shown to improve outcomes in AIHeven in acute, severe presentations.2-6 As a conse-quence, �80%-90% of patients experience clinical andbiochemical remission with standard therapy.7,8
Although �20% of patients with AIH presentacutely,7 the frequency at which patients progress tosubacute liver failure is uncertain. Moreover, it remainsdifficult to identify which patients will develop suba-cute liver failure from the outset. Consequently, earlydiagnosis of patients with AIH is essential and theidentification of treatment failure remains of clinicalimportance, especially in severe acute disease, sinceescalation of immunosuppressive therapy may preventthe progression to liver failure and obviate the needfor liver transplantation (LT).Although it has been reported that treatment
responsiveness can be determined at 2 weeks following
Abbreviations: AIH, autoimmune hepatitis; AST, aspartate aminotransferase;AUROC, area under the receiver operator characteristic curve; CLD, chronicliver disease; IgG, immunoglobulin G; INR, international normalized ratio;LT, liver transplantation; MELD, model for endstage liver disease; TIPSS,transjugular intrahepatic portosystemic shunts; UKELD, United Kingdomendstage liver disease score.From the Institute of Liver Studies, Kings College Hospital NHS Trust
Foundation Trust, Denmark Hill, London, UK.Received September 15, 2010; accepted December 12, 2010.Address reprint requests to: Dr. Michael A. Heneghan, Consultant
Hepatologist, Institute of Liver Studies, Kings College Hospital NHS FoundationTrust, Denmark Hill, London, United Kingdom, SE5 9RS. E-mail: [email protected] 2010 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24141Potential conflict of interest: Nothing to report.
926

initiation of corticosteroids, this was based on death asthe outcome measure in just five patients.2 Further-more, no single parameter was identified as a predictorof death in this series, either at diagnosis or at 2weeks.2 In addition, this study reflects an era prior tothe diagnosis of AIH being accurately codified.9
The model for endstage liver disease (MELD) scorewas originally developed to risk stratify patients whounderwent transjugular intrahepatic portosystemicshunts (TIPSS),10 but its utility has been evaluated inpredicting outcome in alcoholic hepatitis, hepatitis Bvirus infection, variceal bleeding, and critically ill cir-rhotic patients.11-15 In AIH, MELD has been shownto correlate with treatment responsiveness, with non-responders demonstrating higher MELD scores andbilirubin levels at diagnosis than responders.16 Thesame study, however, only evaluated MELD score atdiagnosis, and did not examine the effect of changeover time in response to treatment. This is fundamen-tally important since analysis of change over time,rather than the absolute initial values, may more accu-rately reflect the dynamic interaction between immu-nosuppression and disease activity.In the United Kingdom, a scoring system akin to
MELD-sodium (MELD-Na) has been developed tofacilitate minimal listing criteria for LT in patientswith chronic liver disease (CLD).17 This system, theUnited Kingdom endstage liver disease score(UKELD), incorporates serum sodium and reduces theweighting of creatinine to obtain its score.17 AUKELD score of greater than 49 points in patientswith CLD predicts a 1-year mortality of 9% and rep-resents the minimal listing threshold for LT in theUK.17 Although UKELD has not been analyzed inclinical scenarios other than CLD, its utility and pre-dictive value in the setting of acute liver dysfunction isof interest, in a fashion similar to the utility of MELDor MELD-Na beyond their original intentions.With this in mind, we set out to ascertain what
clinical, laboratory, or scoring system parameters at ini-tiation of treatment were associated with treatmentfailure in patients with icteric presentations of AIH. Inaddition, we wished to determine whether changes inthese values and parameters in the very early posttreat-ment period predicted treatment failure to facilitateprompt augmentation of immunosuppression.
Patients and Methods
A prospectively collected and updated database ofpatients attending the Institute of Liver Studies at
King’s College Hospital with AIH was retrospectivelyanalyzed for patients who presented with jaundice.Such patients were chosen since they are likely to rep-resent acute, severe AIH (although no standardizeddefinition currently exists for this entity). All patientswere treatment-naive. AIH was diagnosed in accord-ance with accepted diagnostic criteria.9 Other causes ofacute liver disease were excluded by a combination ofclinical history, comprehensive serological testing (forhepatitis A, B, C, E, Epstein-Barr virus, cytomegalovi-rus, Wilson’s disease, and hemochromatosis) and histo-logical assessment of available biopsy material.All patients in this database were managed in a
standardized fashion as reported,18 with initial therapyof AIH consisting of prednisolone 40-60 mg per day,based on the results of published controlled se-ries.7,19,20 The six patients who presented duringchildhood were subjected to higher prednisolone doses(2 mg/kg/day or maximum 60 mg/day).21
Only patients who presented during the period1999-2009 inclusive were evaluated for the purposesof this study, as this period coincides with the imple-mentation of an electronic patient record system atKing’s College Hospital. This allowed ascertainment ofcomplete laboratory parameters (particularly serum cre-atinine and sodium) pertinent to calculation ofMELD, MELD-Na, and UKELD scores. For the pur-poses of this study a bilirubin of 40 lmol/L or greaterin the context of a new diagnosis of AIH was consid-ered to represent an icteric presentation.The laboratory parameters of serum bilirubin, aspar-
tate aminotransferase (AST), international normalizedratio (INR), and globulin levels as well as serum creati-nine and sodium were recorded at initiation of treat-ment (day 0) and at days 3 and 7 posttreatment. Theglobulin concentration was used instead of the morespecific immunoglobulin G (IgG) fraction as it consti-tutes part of the standard biochemical profile at ourinstitution and was therefore available in all patients atall time intervals. Although autoantibodies pertinent toAIH (antismooth muscle, antinuclear antibody, andantiliver-kidney microsomal 1 antibody) were routinelyassessed at presentation, these were not reassessed inthe early posttreatment period as titers correlate poorlywith disease severity and treatment outcomes.22
The timepoints of days 3 and 7 postinitiation oftreatment were chosen as comparators, since a singlestudy (published in abstract form) has suggested thatfailure to improve liver function tests by day 3 corre-sponds with poor outcomes in fulminant forms ofAIH.23 We feel, however, that day 3 may be too earlyto detect significant changes in either liver
HEPATOLOGY, Vol. 53, No. 3, 2011 YEOMAN ET AL. 927

biochemistry or liver synthetic function, and thereforeday 7 may represent an interval early enough to evokechanges in patient management and modify outcome,yet at the same time allow a sufficient period to assesscorticosteroid responsiveness.All liver biopsy material obtained prior to initiation
of corticosteroid therapy was re-reviewed in a blindedfashion by two histopathologists (Y.Z. and B.C.P.)with the aim of identifying which, if any, histologicalfeatures correlated with treatment failure. Grading ofnecroinflammatory activity and fibrosis stage weremeasured using the Ishak scoring system.24 In addi-tion, the degree of zonal necrosis, canalicular cholesta-sis, cholangiolar cholestasis, hepatocyte rosetting, andgiant cell change were graded as 0-3 scale (Table 1).The primary outcome measure was treatment failure
which, for the purposes of this study, was defined asthe requirement for second-line therapies within 90days, the progression to subacute liver failure or deathduring the index presentation. Second-line therapies inthis study were not instituted according to a set proto-col but based on a global (laboratory and clinical)assessment of the patient. Patients were excluded fromanalysis if they were not icteric at presentation (biliru-bin <40 lmol/L), did not have available clinical dataat the time of initiation of immunosuppressive therapy,or at 7 days posttreatment.Statistical Analysis. All data are reported as median
and range or percentage. Differences in recorded varia-bles between treatment responders and treatment fail-ures were recorded and analysis of proportions under-taken by the chi-squared test, unless the number ofvariables was less than 5, in which case Fisher’s exacttest was used. Continuous variables were analyzed bythe Mann-Whitney U test on the basis that they werenot normally distributed as determined by the Smir-nov-Kolmogorov method. Area under the receiver op-erator characteristic curves (AUROC) were generatedfor all recorded variables at initiation of treatment (day0) and at days 3 and 7 posttreatment to identify thebest early predictors of treatment failure. The P values
for the AUROC curves relate to the significance of theresults in relation to an area under the curve of 0.5.Results of statistical analysis were considered significantif the P value was equal or less than 0.05. All statisticalanalysis was performed using SPSS statistical packagev. 15.0 (Chicago, IL).
Results
Seventy-two consecutively acquired, treatment-naive,AIH patients were identified with a complete datasetat days 0 and 7. These comprised 48 women and 24men. Median age at treatment initiation was 40 years(range 12-85). Seventy-one patients fulfilled the crite-ria for a diagnosis of probable or definite AIH basedon the 1999 revised international autoimmune hepati-tis group (IAIHG) diagnostic criteria (median score17, range 9-28). The patient who did not meet the1999 diagnostic criteria pretreatment did so posttreat-ment, consequent upon corticosteroid responsivenessand subsequent relapse following treatment with-drawal. Ten patients were not biopsied prior to com-mencement of corticosteroids due to presence of severecoagulopathy. All 10 of these patients met the 1999IAIHG criteria for probable (seven cases) or definiteAIH (three cases) even without biopsy. Importantly,utilization of the simplified IAIHG criteria would haveled to only 6 of these 10 being identified as probable(four cases) or definite AIH (two cases). All but onepatient was subsequently biopsied.No patient had encephalopathy at the time of treat-
ment initiation. At initiation, all patients were treatedwith prednisolone at a median dose of 40 mg per dayin accordance with standard algorithms.1,25 Threepatients were treated with dual therapy (prednisoloneand azathioprine) as induction therapy.
Treatment Failure. Treatment failure, as defined bythe requirement for second line therapies within 90days, progression to subacute liver failure, or deathduring the index presentation, occurred in 13/72patients (18%). There was no significant difference in
Table 1. Histological Classification of Degree of Zonal Necrosis, Canalicular Cholestasis, Cholangiolar Cholestasis,Rosetting, and Giant Cell Change
Histological Parameter
Score
0 1 2 3
Zonal necrosis Absent Zone 3 necrosis Bridging necrosis Pan-acinar necrosis
Canalicular cholestasis Absent Mild (1 or 2 foci) Moderate (3-5 foci) Severe (5 or more foci)
Cholangiolar cholestasis Absent Mild (1 or 2 foci) Moderate (3-5 foci) Severe (5 or more foci)
Copper binding protein Absent Mild (1 or 2 foci) Moderate (3-5 foci) Severe (5 or more foci)
Rosetting Absent Mild (1 or 2 foci) Moderate (3-5 foci) Severe (5 or more foci)
Giant cell change Absent Mild (1 or 2 foci) Moderate (3-5 foci) Severe (5 or more foci)
928 YEOMAN ET AL. HEPATOLOGY, March 2011

age, gender, or presence of cirrhosis at diagnosisbetween responders and treatment failures. All treat-ment failures met the 1999 IAIHG criteria for a prob-able or definite diagnosis of AIH, whereas only 12/14(85%) met the simplified IAIHG diagnostic criteria.The median prednisolone dose was identical (40 mg/day) in both treatment responders and failures. Allthree patients treated with combination prednisoloneand azathioprine as initial treatment were subsequenttreatment responders.
Factors Associated with Treatment Failure at Ini-tiation of Therapy. At initiation of treatment (day 0),a significantly higher median bilirubin (451 lmol/L ver-sus 262 lmol/L P ¼ 0.02), INR (1.62 versus 1.33 P ¼0.005), MELD (26 versus 20 P ¼ 0.02), MELD-Na
(27 versus 22 P ¼ 0.03), and UKELD score (59 versus57 P ¼ 0.01) were observed in patients with treatmentfailure when compared to treatment responders. Themedian values of clinical and laboratory parameters,MELD, MELD-Na, and UKELD scores in treatmentfailures and responders are summarized in Table 2.AUROC curves for recorded parameters at day 0
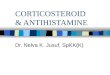
corroborate these findings and identified serum biliru-bin (AUC 0.68 P ¼ 0.04), INR (AUC 0.75 P ¼0.005), MELD score (0.71 P ¼ 0.02), MELD-Nascore (0.69 P ¼ 0.03), and UKELD score (AUC 0.70P ¼ 0.03) as being the only parameters that signifi-cantly predicted treatment failure. The AUROC curvesof these and other observed parameters are presentedin Fig. 1A.
Table 2. Clinical, Demographic, and Laboratory Features at Initiation of Therapy in Responders and Treatment Failures
Variable (Median or Percentage) Total Cohort n572 Treatment Responders n559 Treatment Failures n513 P-value
Bilirubin lmol/l (3-20) (range) 277 (42-1208) 262 (42-1208) 451 (88-705) 0.02
AST mmol/l (10-50) (range) 815 (121-2762) 899 (121-2762) 570 (125-1961) 0.22
INR (0.9-1.2) (range) 1.39 (0.90-2.63 1.34 (0.90-2.63) 1.63 (1.1-2.62) 0.004
Creatinine lmol/l (45-120) (range) 95 (49-210) 94 (49-210) 96 (62-174) 0.94
Sodium mmol/l (135-145) (range) 136 (128-143) 136 (128-143) 135 (130-142) 0.43
Globulin g/dl (25-35) (range) 44 (14-96) 42 (14-96) 47 (30-77) 0.09
MELD (range) 21 (6-42) 20 (6-42) 26 (16-35) 0.02
MELD-Na (range) 23 (9-42) 22 (9-42) 27 (19-36) 0.03
UKELD (range) 57 (48-67) 57 (48-65) 59 (55-67) 0.01
Cirrhosis % 47% 46% 54% 0.60
Age at diagnosis (range) 40 (12-85) 37 (12-80) 46 (19-85) 0.38
Female gender % 67% 69% 54% 0.28
1999 IAIHG score (range) 17 (9-28) 18 (9-28) 16 (11-26) 0.30
Simplified IAIHG score (range) 7 (2-8) 7 (2-8) 6 (2-8) 0.39
Mortality % 5.6% 1.7% 30.8% 0.003
Fig. 1. (A) ROC curves depicting the utility of liver-specific prognostic scoring systems as predictors of treatment failure at initiation of cortico-steroid therapy (day 0). (B) ROC curves depicting the utility of delta the change in liver-specific prognostic scores as predictors of treatment fail-ure at day 7 of postinitiation of corticosteroid therapy.
HEPATOLOGY, Vol. 53, No. 3, 2011 YEOMAN ET AL. 929

Changes (D) in Biochemical and Scoring Sys-tem Parameters as Early Predictors of TreatmentFailure. At day 3 posttreatment, clinical data wereavailable in 57/70 (81%) patients. Only the changes(D) in the scores of the scoring systems MELD(AUROC 0.670 P ¼ 0.04), MELD-Na (0.71 P ¼0.03), and UKELD (0.69 P ¼ 0.04) predicted treat-ment failure. In contrast, at day 7 posttreatment, DUKELD (AUROC 0.83 P ¼ <0.001), D MELD-Na(AUROC 0.83 P ¼ <0.001), D MELD (AUROC0.79 P ¼ 0.001), and D bilirubin (AUROC 0.69 P ¼0.04) all predicted treatment failure. The ROC curvesfor the changes in these variables at day 7 are pre-sented in Fig. 1B. Table 3 presents the AUROC, 95%confidence intervals, and P values (in relation to anAUC of 0.5) for all observed parameters at all time-points in the study cohort.
Histological Features Among Study Cohort. Sixty-two patients (86%) had a liver biopsy prior to initia-tion of corticosteroid therapy, of which 56 (78%) wereavailable for formal histological regrading. The remain-ing six specimens were not obtainable from the refer-
ring institution and so could not be analyzed. Treat-ment failure occurred in 3/10 (30%) of patients whodid not undergo biopsy at diagnosis compared with10/60 (17%) of those who were biopsied but this didnot reach significance (P ¼ 0.38).There were no significant differences between any
aspects of the Ishak scoring system, degree of zonal ne-crosis, canalicular cholestasis, cholangiolar cholestasis,presence of hepatocyte rosetting or frequency of giantcell change between treatment responders and nonres-ponders. Furthermore, the presence of parenchymalcollapse was not associated with treatment failure.These results are presented in Table 4.
Clinical Outcomes Among Treatment Failures. Ofthe 13 treatment failures, 11 received second-line ther-apy, of whom nine were rescued with such treatment.This was achieved by tacrolimus (seven patients),mycophenolate mofetil (one patient), and plasmapha-resis (one patient). These were initiated at a mediantime of 17 days following commencement of predniso-lone. The demographic, clinical, laboratory, and treat-ment response characteristics of these patients are
Table 3. Area Under the Receiver Operator Curves (AUROC), 95% Confidence Intervals, and P-Values for Analyzed Variablesat Initiation of Treatment (Day-0), Day-3, Day-7, or Day-28 Postcorticosteroid Treatment
Day Bilirubin AST INR Creatinine Sodium MELD MELD-Na UKELD
0
n ¼ 72
0.71
(0.56-0.86)
P ¼ 0.02
0.39
(0.21-0.57)
P ¼ 0.22
0.76
(0.62-0.89)
P ¼ 0.004
0.51
(0.32-0.70)
P ¼ 0.94
0.43
(0.25-0.61)
P ¼ 0.43
0.71
(0.54-0.87)
P ¼ 0.02
0.70
(0.54-0.86)
P ¼ 0.03
0.72
(0.55-0.85)
P ¼ 0.01
3
n ¼ 60
0.64
(0.47-0.81)
P ¼ 0.15
0.62
(0.42-0.83)
P ¼ 0.19
0.49
(0.31-0.68)
P ¼ 0.95
0.62
(0.45-0.80)
P ¼ 0.20
0.40
(0.21-0.58)
P ¼ 0.27
0.70
(0.53-0.87)
P ¼ 0.035
0.71
(0.55-0.87)
P ¼ 0.025
0.69
(0.52-0.86)
P ¼ 0.042
7
n ¼ 72
0.68
(0.52-0.85)
P ¼ 0.04
0.62
(0.44-0.80)
P ¼ 0.19
0.55
(0.37-0.73)
P ¼ 0.57
0.69
(0.52-0.87)
P ¼ 0.03
0.60
(0.42-0.78)
P ¼ 0.27
0.79
(0.66-0.93)
P ¼ 0.002
0.83
(0.70-0.96)
P ¼ <0.001
0.83
(0.69-0.98)
P ¼ <0.001
28
n ¼ 43
0.62
(0.44-0.80)
P ¼ 0.26
0.55
(0.33-0.77)
P ¼ 0.63
0.47
(0.27-0.68)
P ¼ 0.79
0.69
(0.49-0.90)
P ¼ 0.07
0.70
(0.53-0.88)
P ¼ 0.05
0.82
(0.70-0.95)
P ¼ 0.002
0.84
(0.72-0.95)
P ¼ 0.001
0.80
(0.68-0.93)
P ¼ 0.004
Table 4. Histological Features at Accession and Their Relationship to Treatment Response, n 5 56
Histological Parameter Total CohortMedian (Range)/% Treatment FailuresMedian (Range)/% Treatment RespondersMedian (Range)/% P-Value
Ishak
Interface hepatitis 3 (0-4) 3 (1-4) 3 (0-4) 0.79
Confluent necrosis 3 (0-6) 4 (0-6) 4 (0-6) 0.67
Focal necrosis 3 (0-4) 3 (0-4) 3 (1-4) 0.28
Portal inflammation 2 (0-4) 2 (1-4) 2 (0-4) 0.84
Total NI grade 12 (1-17) 12 (2-17) 12 (1-17) 0.72
Fibrosis stage 4 (1-6) 4 (2-6) 4 (1-6) 0.13
Fresh zonal necrosis 1 (0-3) 2 (0-3) 1 (0-3) 0.37
Canalicular cholestasis 0 (0-3) 0 (0-3) 0 (0-3) 0.92
Cholangiolar cholestasis 0 (0-2) 0 (0-2) 0 (0-2) 0.77
Copper binding 0 (0-3) 0 (0-3) 0 (0-3) 0.43
Hepatocyte rosetting 0 (0-3) 0 (0-3) 0 (0-3) 0.71
Giant cell change 39% 39% 39% 0.99
Parenchymal collapse 54% 70% 50% 0.31
930 YEOMAN ET AL. HEPATOLOGY, March 2011

summarized in Table 5. Three patients (23%) pro-gressed to subacute liver failure and were listed foremergency transplant. All subsequently underwenttransplantation at 8, 31, and 39 days following initia-tion of corticosteroid therapy. The remaining patientwho failed initial treatment was not considered foradditional immunosuppression due to the developmentof sepsis and LT was not considered for this individualdue an age of 85 years.Four of the 13 (31%) treatment failures died, all
from complications of sepsis. Two of the deathsoccurred in patients who underwent LT, with deathoccurring at 31 and 121 days posttransplantation or 39and 163 days following initiation of treatment. The lat-ter patient was treated with tacrolimus and prednisoloneprior to LT. The other deaths occurred in a patient whorequired tacrolimus rescue therapy but who died at 356days after initiation of corticosteroids and an elderlypatient, described above, who developed sepsis on pred-nisolone monotherapy and subsequently died of multi-organ failure. Overall, death occurred in a significantlyhigher proportion of treatment failures than responders(4/13 ¼ 31% versus 1/59 ¼ 1.7% P ¼ 0.003).
Long-Term Clinical Outcomes. Biochemical remis-sion (defined as normalization of both AST and globu-lin levels), occurred in 64/72 (89%), at a medianinterval of 77 (7-2,550) days. Normalization of ASTtook a median of 80 days (7-2,550) in responders and67 days (23-404) in treatment failures, P ¼ 0.4.Meanwhile, normalization of serum bilirubin occurredin 59/70 (84%) at a median of 80 days (14-2,086).
However, the time taken to normalization of bilirubinwas shorter in responders than treatment failures being72 days (range 14-2,086) versus 142 days (range 57-467), P ¼ 0.013. An elevated INR (>1.2) was notedin 47 patients (67%) one0third of whom had an INR>1.5. Normalization of INR occurred in 39 (83%)taking a median of 26 days (1-2,046), 20 days (1-2,046) in responders versus 58 days (10-392) in treat-ment failures, P ¼ 0.17. Biochemical relapse occurredin 11% of surviving nonresponders and 22% of sur-viving responders, although this did not reach statisti-cal significance (P ¼ 0.67).Ten patients (14% of cohort) were lost to follow-up
after a median of 91 days, having been dischargedback to the referring institution for ongoing manage-ment. Using intention to treat analysis, median sur-vival for the entire cohort was 1,470 days (range 9-3,786), 944 days for treatment failures (30-3,417) and1538 days (9-3,786) for responders, P ¼ 0.36. Amongearly treatment responders, one further patientrequired LT at 2,046 days following diagnosis due toan episode of decompensation in the immediate post-partum period. This patient also represented the onlydeath in the early treatment responder group, due tohemorrhagic complications following cesarean section7 years following diagnosis and initial treatment.
Discussion
Patients with AIH who present with jaundice consti-tute a subgroup with a higher likelihood of treatmentfailure. Such patients require close monitoring
Table 5. Individual Patient Demographic and Treatment Response Characteristics of Corticosteroid TreatmentFailures (n 5 13) Among the Study Cohort
Patient Age Sex
IAIHG
Score Cirrhotic
Initial
Steroid Dose
D Bili
Day 7
D MELD
Day 7
D MELD-Na
Day 7
D UKELD
Day 7
2nd- Line T
reatment
Time
to Rx
Time
to CBR
Clinical
Outcome
Survival
in Days
1 85 F 15 Yes 40mg/d 30 0 þ1 þ1 None 20 d na Died: Sepsis 30
2 43 F 26 Yes 40mg/d 124 5 6 6 MMF &
plasmapharesis
22 d 48 d Failed MMF: rescued
with plasmapharesis
3,417.*
3 40 F 19 Yes 40mg/d 161 1 þ2 0 Tacrolimus 12 d 404 d Tacrolimus responder 1,106.*
4 31 M 16 Yes 40mg/d 51 1 1 1 Tacrolimus 13 d 129 d Tacrolimus responder 100.*
5 66 F 16 No 40mg/d þ220 þ2 þ2 þ1 Tacrolimus 12 d 63 d Tacrolimus responder 1,290.*
6 19 M 11 No 40mg/d þ43 0 0 0 Tacrolimus 43 d 82 d Tacrolimus responder 2,067.*
7 53 M 12 No 40mg/d 71 þ13 þ13 þ3 None na na LT Died post LT 39
8 52 F 18 No 40mg/d þ92 þ4 þ3 þ2 Tacrolimus 14 d 58 d LT Died post LT 163
9 60 F 16 Yes 30mg/d 4 1 2 1 Tacrolimus &
plasmapharesis
16 d na Failed tacrolimus &
plasmapharesis: LT
3,339.*
10 48 M 14 Yes 40mg/d 75 5 3 1 Tacrolimus 31 d 70 d Tacrolimus responder
died later
356
11 20 M 16 Yes 40mg/d 12 þ2 1 1 MMF 79 d 258 d MMF responder 944.*
12 28 M 12 No 40mg/d 23 2 2 1 Tacrolimus 10 d 272 d Tacrolimus responder 731.*
13 19 F 18 No 40mg/d 33 3 3 3 Tacrolimus 17 d 42 d Tacrolimus responder 30.*
.*Patients still alive.
Abbreviations: IAIHG, International Autoimmune Hepatitis Group Score; mg/d, milligrams per day; LT, liver transplantation; Rx, treatment; CBR, complete biochem-
ical response; d, days.
HEPATOLOGY, Vol. 53, No. 3, 2011 YEOMAN ET AL. 931

following institution of treatment and, at least in thisstudy, failure of standard treatment in patients withAIH and jaundice is associated with an almost 25%risk of death and a similar need for emergency LT. Itis important to acknowledge, however, that these datarepresent the experience of a selected patient popula-tion in a tertiary referral center with significant experi-ence of managing complex presentations of AIH.Laboratory parameters at initiation of therapy that
were significantly associated with treatment failure,included a higher level of bilirubin and INR, whereaschange in MELD, MELD-Na, and UKELD scores atday 7 better predicted this outcome based on assess-ment of ROC curves. Whereas others have previouslyidentified MELD at diagnosis as a predictor of treat-ment responsiveness in AIH,16 in this study we haveidentified that MELD-Na and UKELD are equal ifnot better than MELD at predicting treatment failure.This suggests that the value of serum sodium (utilizedMELD-Na and UKELD but not MELD) has someutility in mortality prediction for acute presentationsof liver disease. Interestingly, the area under the ROCcurves for each of these scoring parameters increasedsequentially over time, being lowest at day 0 and high-est at day 7. This suggests that dynamic changes arebetter indicators of treatment failure than measuresviewed at a single timepoint at treatment initiation.Change in UKELD score at day 7 was identified asthe best predictor of treatment failure as evidenced bythe largest AUC. Failure of UKELD scores to fall bymore than 2 units 1 week following treatment initia-tion predicted treatment failure with a sensitivity of85% and specificity of 68%, giving a positive predic-tive value of 40% and a negative predictive value of96%. A fall in MELD of <2 points equated to a sen-sitivity of 70% and specificity of 75%, with the corre-sponding figures for a <2 point fall in MELD-Nabeing a sensitivity of 77% and specificity of 78%.It is critical to point out, however, that UKELD, in
contrast to MELD or MELD-Na has only been vali-dated in a United Kingdom population. Nonetheless,the performance of both MELD-Na and UKELD inthis context suggests that the role of serum sodium inoutcome prediction is not isolated to the patient withcirrhosis. Indeed, that the change in UKELD andMELD-Na score produced the highest AUC for treat-ment failure is somewhat surprising, given these scoreswere designed to predict mortality of patients withCLD being considered for LT. Furthermore, significantalterations in the serum sodium level (awarded thehighest integer weighting in UKELD) would not nec-essarily be expected in this clinical context, and, inter-
estingly, are not borne out by the individual changesin serum sodium among this cohort.In contrast to the performance of liver-specific prog-
nostic scores, individual laboratory parameters fare lesswell as predictors of treatment failure, with only thechange in bilirubin and creatinine at day 7 producingsignificant AUCs (0.68 and 0.69, respectively), whichare considerably lower than those observed for MELD,MELD-Na, and UKELD. In addition, the utility ofmeasuring a change in the AST as a predictor of short-term outcomes has no merit based on these data. Incontrast, previous work from this institution has iden-tified a high AST (>10 times upper limit of normal)at presentation as being associated with better long-term outcomes.26
These data also suggest that day 7 posttreatmentrepresents a useful timepoint to assess responsivenessto corticosteroid treatment for several reasons. First, itappears early enough to initiate change in patientmanagement as evidenced by the nine patients whoresponded to second-line therapies and did not requireLT. However, it must also be acknowledged that it isimpossible to know how many would have progressedto subacute liver failure without treatment modifica-tion. Second, it is a short enough time period that sep-tic complications are less likely to develop. Third, asthe AUCs suggest, predictability of treatment failure atday 0 is inferior to the dynamic change at day 7.However, this did not reach statistical significance andthis may relate to a type-II error. Nonetheless, assess-ment of parameters at day 7 may be a better predictorof treatment failure, since it incorporates both theaggressiveness of the clinical phenotype and thedynamic impact of immunosuppression. Finally,the ability to identify corticosteroid nonresponders at7 days following treatment has precedence in the liter-ature, as change in bilirubin level has recently beenidentified as being critical in prognosis of patients withalcoholic hepatitis.27
In this study we also evaluated findings on liver bi-opsy. Although liver biopsy remains important in con-firming the diagnosis of AIH, its utility, specifically asa predictor of outcome, has only rarely been studied.One such study, however, demonstrated an increasedrate of relapse and cirrhosis development followingtreatment withdrawal in patients with more advancedfibrosis and plasma cell activity.28 In this currentcohort, no single histological feature predicted treat-ment failure. Despite the lack of association betweenhistological features and treatment failure, one notablefeature was the frequency with which giant cell changewas noted. In this patient group, over a third (39%)
932 YEOMAN ET AL. HEPATOLOGY, March 2011

of patients exhibited at least some degree of giant cellchange, which is of interest as this phenomenon hastraditionally been felt to be a relatively rare occurrencein adults.29 Although reported at a prevalence of 29%in a previous study of 21 patients with AIH, based onthe combined experience it appears the finding ofgiant cell change is a valid phenomenon in thissetting.30
The importance of acute severe AIH, as a cause ofsignificant morbidity, including fulminant hepatic fail-ure, is well established.3,31-33 The United States AcuteLiver Failure (USALF) study group report that 10% ofsuch patients are due to AIH.34 Additionally, a further30% of ALF cases are deemed ‘‘seronegative,’’ of whicha portion may have underlying AIH.35,36 Among thiscohort, the incidence of any degree of liver syntheticimpairment was high, with a third of patients havingan INR >1.5. Early diagnosis and treatment of theseindividuals remains essential to prevent clinical deterio-ration but the optimal strategy to apply if corticoste-roids fail remains uncertain. Although azathioprine iswell established in the management of AIH,20,37-39 itsonset of action is slow and is unlikely to be rapidenough to evoke any benefit in acute presentations.On the other hand, the efficacy of second-line immu-nosuppression with tacrolimus or MMF has not beensubjected to rigorous study, with most published dataemanating from relatively small case series.40-44 Tacro-limus has been the preferred second-line therapy atour institution due to its potent and rapid immuno-suppressive effects.Importantly, median survival was no different
between early corticosteroid failures and responders,despite a significantly higher mortality rate among theearly treatment failures, implying that if rescue therapyproves successful, then long-term outcome for thesepatients remains excellent. Although the day 7 changein MELD, MELD-Na, and UKELD scores showpromise in identifying those who will not respond tocorticosteroids at an early timepoint, they can onlyever be utilized as an adjunct to close clinical observa-tion so that signs of worsening liver synthetic functionand hepatic encephalopathy can be detected and actedupon.In conclusion, we describe a well-characterized
cohort of patients with acute, icteric presentations ofAIH among whom treatment failure occurred inalmost 20%. Change in MELD, MELD-Na, andUKELD and scores at day 7 represented the best pre-dictors of treatment failure. Therefore, patients whofail to reach this threshold may be considered for earlyaugmentation of immunosuppressive therapy, or if
encephalopathy develops, for LT. However, the clinicalutility of early changes in prognostic scores in predict-ing treatment failure as well as the efficacy and optimaltiming of second-line immunosuppressive therapy inicteric presentations of AIH who fail corticosteroidtreatment warrants further, prospective investigation.
References1. Heneghan MA, McFarlane IG. Current and novel immunosuppressive
therapy for autoimmune hepatitis. HEPATOLOGY 2002;35:7-13.2. Czaja AJ, Rakela J, Ludwig J. Features reflective of early prognosis in
corticosteroid-treated severe autoimmune chronic active hepatitis. Gas-troenterology 1988;95:448-453.
3. Nikias GA, Batts KP, Czaja AJ. The nature and prognostic implicationsof autoimmune hepatitis with an acute presentation. J Hepatol 1994;21:866-871.
4. Herzog D, Rasquin-Weber AM, Debray D, Alvarez F. Subfulminanthepatic failure in autoimmune hepatitis type 1: an unusual form of pre-sentation. J Hepatol 1997;27:578-582.
5. Viruet EJ, Torres EA. Steroid therapy in fulminant hepatic failure sec-ondary to autoimmune hepatitis. P R Health Sci J 1998;17:297-300.
6. Kessler WR, Cummings OW, Eckert G, Chalasani N, Lumeng L, KwoPY. Fulminant hepatic failure as the initial presentation of acute auto-immune hepatitis. Clin Gastroenterol Hepatol 2004;2:625-631.
7. Soloway RD, Summerskill WH, Baggenstoss AH, et al. Clinical, bio-chemical, and histological remission of severe chronic active liverdisease: a controlled study of treatments and early prognosis. Gastroen-terology 1972;63:820-833.
8. Schalm SW, Ammon HV, Summerskill WHJ. Failure of customarytreatment in chronic active liver disease: causes and management. AnnClin Res 1976;8:221-227.
9. Alvarez F, Berg PA, Bianchi FB, et al. International Autoimmune Hep-atitis Group Report: review of criteria for diagnosis of autoimmunehepatitis. J Hepatol 1999;31:929-938.
10. Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, Borg PC. Amodel to predict poor survival in patients undergoing transjugular in-trahepatic portosystemic shunts. HEPATOLOGY 2000;31:864-871.
11. Chan HLY CA, Lau JTF, Hui AY, Wong VWS, Sung JJY. Evaluationof model for end-stage liver disease for prediction of mortality indecompensated chronic hepatitis B. Am J Gastroenterol 2006;101:1516-1523.
12. Srikureja W, Kyulo NL, Runyon BA, Hu KQ. MELD score is a betterprognostic model than Child-Turcotte-Pugh score or DiscriminantFunction score in patients with alcoholic hepatitis. J Hepatol 2005;42:700-706.
13. Dunn W, Jamil LH, Brown LS, Wiesner RH, Kim WR, Menon KVN,et al. MELD accurately predicts mortality in patients with alcoholichepatitis. HEPATOLOGY 2005;41:353-358.
14. Chalasani N, Kahi C, Francois F, Pinto AO, Marathe A, Bini EJ, et al.Model for end-stage liver disease (MELD for predicting mortality inpatients with acute variceal bleeding. HEPATOLOGY 2002;35:1282-1284.
15. Wehler M, Koskoska J, Reulbach U, Hahn EG, Strauss R. Short-termprognosis in critically ill patients with cirrhosis assessed by prognosticscoring systems. HEPATOLOGY 2001;34:255-261.
16. Montano-Loza AJ, Carpenter HA, Czaja AJ. Features associated withtreatment failure in type 1 autoimmune hepatitis and predictive valueof the model of end-stage liver disease. HEPATOLOGY 2007;46:1138-1145.
17. Neuberger J, Gimson A, Davies M, et al. Selection of patients for livertransplantation andallocation of donated livers in the UK. GUT 2008;57:252-257.
18. Al-Chalabi T, Boccato S, Portmann BC, McFarlane IG, HeneghanMA. Autoimmune hepatitis (AIH) in the elderly: a systematic
HEPATOLOGY, Vol. 53, No. 3, 2011 YEOMAN ET AL. 933

retrospective analysis of a large group of consecutive patients with defi-nite AIH followed at a tertiary referral centre. J Hepatol 2006;45:575-583.
19. Cook GC, Mulligan R, Sherlock S. Controlled prospective trial of cor-ticosteroid therapy in active chronic hepatitis. Q J Med 1971;40:159-185.
20. Murray-Lyon IM, Stern RB, Williams R. Controlled trial of predni-sone and azathioprine in active chronic hepatitis. Lancet 1973;1:735-737.
21. Gregorio GV, Portmann B, Reid F, et al. Autoimmune hepatitis inchildhood: a 20-year experience. HEPATOLOGY 1997;25:541-547.
22. Czaja AJ. Behavior and significance of autoantibodies in type 1 autoim-mune hepatitis. J Hepatol 1999;30:394-401.
23. Villamil AG, Casciato P, Eduardo M, Bustos D, Giunta D, CiardulloM, et al. Fulminant autoimmune hepatitis: clinical presentation, out-come and prognostic factors. Am J Transpl 2005;5(Suppl 11):278.
24. Ishak KG. Chronic hepatitis: morphology and nomenclature. ModPathol 1994;7:690-713.
25. Krawitt EL. Autoimmune hepatitis. N Engl J Med 2006;354:54-66.26. Al-Chalabi T, Underhill J, Portmann BC, McFarlane IG, Heneghan
MA. Effects of serum aspartate transaminase levels in patients withautoimmune hepatitis influence disease course and outcome. Clin Gas-troenterol Hepatol 2008;6:1389-1395.
27. Mathurin P, Abdelnour M, Ramond MJ, et al. Early change in biliru-bin levels is an important prognostic factor in severe alcoholic hepatitistreated with prednisolone. HEPATOLOGY 2003;38:1363-1369.
28. Verma S, Gunuwan B, Mendler M, Govindrajan S, Redeker A. Factorspredicting relapse and poor outcome in type I autoimmune hepatitis:role of cirrhosis development, patterns of transaminases during remis-sion and plasma cell activity in the liver biopsy. Am J Gastroenterol2004;99:1510-1516.
29. Lotz G, Koltai P, Schaff Z. Giant cell hepatitis in adults. Pathol OncolRes 1997;3:215-218.
30. Bach N, Thung SN, Schaffner F. The histological features of chronichepatitis C and autoimmune chronic hepatitis: a comparative analysis.HEPATOLOGY 1992;15:572-577.
31. Okano N, Yamamoto K, Sakaguchi K, et al. Clinicopathological fea-tures of acute-onset autoimmune hepatitis. Hepatol Res 2003;25:263-270.
32. Miyake Y, Iwasaki Y, Terada R, et al. Clinical characteristics of fulmi-nant-type autoimmune hepatitis: an analysis of eleven cases. AlimentPharmacol Ther 2006;23:1347-1353.
33. Ichai P, Duclos-Vallee J-C, Guettier C, Hamida SB, Antonini T, DelvartV, et al. Usefulness of corticosteroids for the treatment of severe and fulmi-nant forms of autoimmune hepatitis. Liver Transplant 2007;13:996-1003.
34. Ostapowicz G, Fontana RJ, Schiodt FV, Larson A, Davern TJ, HanSHB. Results of a prospective study of acute liver failure at 17 tertiarycare centers in the United States. Ann Intern Med 2002;137:947-954.
35. Czaja AJ, Carpenter HA, Santrach PJ, Moore SB, Homburger HA.The nature and prognosis of severe cryptogenic chronic active hepatitis.Gastroenterology 1993;104:1755-1761.
36. Bernal W, Ma Y, Smith HM, Portmann B, Wendon J, Vergani D. Thesignificance of autoantibodies and immunoglobulins in acute liver fail-ure: a cohort study. J Hepatol 2007;47:664-670.
37. Johnson PJ, McFarlane IG, Williams R. Azathioprine for long-termmaintenance of remission in autoimmune hepatitis. N Engl J Med1995;333:958-963.
38. Stellon AJ, Hegarty JE, Portmann B, Williams R. Randomised con-trolled trial of azathioprine withdrawal in autoimmune chronic activehepatitis. Lancet 1985;1:668-670.
39. Stellon AJ, Keating JJ, Johnson PJ, McFarlane IG, Williams R. Mainte-nance of remission in autoimmune chronic active hepatitis with aza-thioprine after corticosteroid withdrawal. HEPATOLOGY 1988;8:781-784.
40. Hlivko JT, Shiffman ML, Stravitz RT, et al. A single center review ofthe use of mycophenolate mofetil in the treatment of autoimmune hep-atitis. Clin Gastroenterol Hepatol 2008;6:1036-1040.
41. Hennes EM, Oo Y, Schramm C, Denzer U, Buggisch P, Wiegard Cea.Mycophenolate mofetil as second line therapy in autoimmune hepatitis?Am J Gastroenterol 2008;103:3063-3070.
42. Larsen FS, Vainer B, Eefsen M, Bjerring PN, Hansen BA. Low-dosetacrolimus ameliorates liver inflammation and fibrosis in steroid refrac-tory autoimmune hepatitis. World J Gastroenterol 2007;13:3232-3236.
43. Aqel BA, Machicao V, Rosser B, Satyanarayana R, Harnois DM, Dick-son RC. Efficacy of tacrolimus in the treatment of steroid refractoryautoimmune hepatitis. J Clin Gastroenterol 2004;38:805-809.
44. Heneghan MA, Rizzi P, McFarlane IG, Portmann B, Harrison PM.Low dose tacrolimus as treatment of severe autoimmune hepatitis:potential role in remission induction. Gut 1999;44:A61.
934 YEOMAN ET AL. HEPATOLOGY, March 2011