Embed Size (px)
Citation preview
Laboratory Genetics User Manual
POL003 Version No. 20
Available as a pdf from Department Website
https://www.nhstayside.scot.nhs.uk/OurServicesA
Human Genetics Intranet site: http://staffnet.tayside.scot.nhs.uk/OurWebsites/HumanGenetics/index.htm
East of Scotland Regional Genetic Service
Laboratory Genetics
Information for Users
Laboratory Genetics User Manual Page 1
Available as a pdf from Department Website: www.esrg.scot.nhs.uk or
https://www.nhstayside.scot.nhs.uk/OurServicesA-Z/Genetics/index.htm
http://staffnet.tayside.scot.nhs.uk/OurWebsites/HumanGenetics/index.htm
East of Scotland Regional Genetic Service
Laboratory Genetics
Information for Users
1 of 21
August 2021
East of Scotland Regional Genetic Service
Laboratory Genetics User Manual Page 2 of 21
POL003 Version No. 20 August 2021
Contents The Service 3
Contacting the laboratory 4
Laboratory Staff 4
Sending a sample to the laboratory 5
Referral reasons 5
Completing the Human Genetics request form 5
Referral information 6
Specimen labels 7
Specimen rejection 7
Sample Collection 7
High Risk Specimens 7
Sample Transport to the Laboratory 7
Transport Medium 8
Specimen requirements 9
Blood samples for postnatal microarray analysis (molecular karyotyping) 9
Blood samples for postnatal karyotyping (conventional chromosome analysis) 9
Blood samples for hereditary genetic conditions 9
Blood samples for noninvasive prenatal testing (NIPT) 9
Amniotic fluids for microarray (molecular karyotyping) and rapid trisomy testing 9
Chorionic villus samples for microarray (molecular karyotyping) and rapid trisomy testing 10
Fetal tissue samples 10
Other fresh tissue samples 11
Formalin fixed paraffin embedded tissue (FFPE) 11
Haemato-oncology (karyotyping) 11
Myeloma FISH 12
Haemato-oncology (DNA testing) 12
Other specimen types 12
RNA extraction 12
Sample storage 13
Reporting 13
Directory of Laboratory Tests 13
Timescale for requesting additional tests 19
Quality assurance and accreditation 19
Contacts for clinical advice 20
Complaints and suggestions 20
Other Scottish Genetic Consortium Laboratories 21
Further Information 21
Laboratory Genetics User Manual Page 3 of 21
POL003 Version No. 20 August 2021
The Service
The Laboratory Genetic Service offers both karyotyping and nucleic acid-based testing for both acquired and inherited genetic conditions and encompasses testing for solid tumours and haematological malignancies for Tayside and North East Fife. The Service is located on Level 6 of the laboratory block at Ninewells Hospital and with Clinical Genetics and Genetic Counselling forms the East of Scotland Regional Genetic Service. The Service is a member of both the Scottish Genetics Laboratories Consortium and the Scottish Molecular Pathology Consortium that are commissioned by National Services Division (NSD) to provide a comprehensive specialist genetic testing service for Scottish patients. The Service works closely with its clinical users and a User Survey is circulated every two years, and a link to the survey is sent with every report that is emailed from LIMS. In addition comments and suggestions about the Service from users are always welcome via the survey (https://www.surveymonkey.co.uk/r/5LG9PF5). The Service (Medical Laboratory 8806) is accredited by United Kingdom Accreditation Service (UKAS) in accordance with the recognized Internation al Standard ISO 15189:2012 Medical Laboratories – Requirements for Quality and Compete nce. This accreditation is based on a defined scope of accreditation for the Service as d etailed on the UKAS website. http://www.ukas.com/wp-content/uploads/schedule_uploads/00007/8806%20Medic al%20Multple.pdf The types of testing offered by the Service include:
• Conventional karyotyping (chromosome analysis)
• Microarray comparative genomic hybridisation
• Fluorescent in-situ hybridisation (FISH)
• Variant detection using DNA and RNA analysis for both inherited and acquired genetic
conditions.
• Non-invasive Prenatal Testing
• Nucleic acid extraction and storage from a range of patient samples.
• Cell culture and storage.
All Highland samples for cytogenetic investigations (Karyotyping and FISH) and constitutional bloods for microarray analysis are sent via the Pathology Laboratory at Raigmore. Contact Highland Pathology lab: Tel: 01463 705979 (ext 5979) or 01463 704269 (ext 4269)
Laboratory Genetics User Manual Page 4 of 21
POL003 Version No. 20 August 2021
Contacting the laboratory
Laboratory Hours Monday - Friday 8.30am-5.00pm Out-of-Hours Service The laboratory does not operate formal out of hours services, but every attempt is made to meet urgent clinical need. For service provision out-with laboratory hours please arrange in advance by contacting the Genetic Duty Scientist. Address for correspondence and samples East of Scotland Regional Genetics Service, NHS Tayside, Level 6, Ninewells Hospital & Medical School, Dundee, DD1 9SY
For general laboratory advice and information contact: Duty Scientist Tel: 01382 740533 (or ext 40533 when dialling internally) Email: [email protected] The Duty Scientist email account should be used for all clinical requests and correspondence. Patient identifiable information should not be sent to any other laboratory email address. Laboratory Staff
Director of Genetic Laboratory Services Dr. Norman Pratt, Consultant Clinical Scientist Tel: 01382 492680 (Ext 32680) Email: [email protected]
Head of Laboratory Genetics Dr. David Baty Tel: 01382 496271 (Ext 36271) Email: [email protected] Deputy Head of Laboratory Genetics Nicola Andrew Tel: 01382 740534 (Ext 40534) Email: [email protected]
Senior Clinical Scientists Joan Cunningham Michelle McConnachie Tel : 01382 740534 (Ext 40534)
Laboratory Genetics User Manual Page 5 of 21
POL003 Version No. 20 August 2021
Technical Team Lead Gillian McGregor, Advanced Healthcare Practitioner Tel: 01382 496735 (Ext 36735) Quality Manager Helen Reavy Tel: 01382 740304 (Ext 40304) Email: [email protected]
Sending a sample to the laboratory Each request accepted by the laboratory for testing is considered an agreement between the User and the Laboratory. Referral reasons The laboratory uses a range of techniques to carry out testing for a wide range of hereditary and acquired genetic disorders (haematological malignancy and solid tumours). The types of investigation include:
• Inherited constitutional karyotype analysis • Acquired karyotype analysis of abnormalities in malignancy • Molecular cytogenetic testing (FISH and array CGH) for constitutional or acquired
abnormalities • Confirmation or exclusion of a diagnosis for inherited and acquired disorders • Carrier testing and risk assessment in families with a known genetic disorder • Presymptomatic or predictive testing in individuals at risk of a late-onset genetic disorder • Prenatal diagnosis of genetic conditions, where appropriate • Noninvasive prenatal testing (NIPT) • Pharmacogenetic testing to determine drug treatment options • Testing genes for prognosis/therapeutic decision making in cancer
The laboratory offers testing for a range of core disorders plus a set of more specialist services for which samples are received on a national basis. The full list of tests offered by the laboratory is shown in the Directory of Laboratory Tests from p13. The laboratory, if appropriate, can forward DNA samples to other UK genetic laboratories for testing. Please note that samples referred out-with Scotland for testing usually have an associated cost. In addition, specific referral forms may require to be completed to accompany referred samples. Therefore users who wish to arrange genetic testing out-with Scotland should consult with a member of their local Clinical Genetic Service beforehand to ensure that associated costs will be met by National Services Division (NHS Scotland). If this procedure is not followed, the referring clinical department may be liable for any associated costs.
Completing the Human Genetics request form For NHS Tayside users, tests should be requested electronically via ICE where possible. If the test required cannot be found on ICE please use a paper request form. More information can be found in the document ‘Genetics ICE: Guidance for Users’ accessed via the following link: http://staffnet.tayside.scot.nhs.uk/NHSTaysideDocs/groups/it_training/documents/documents/prod_284141.pdf
Laboratory Genetics User Manual Page 6 of 21
POL003 Version No. 20 August 2021
Paper request forms can be downloaded from the departmental website www.esrg.scot.nhs.uk or accessed via the Trust site http://staffnet.tayside.scot.nhs.uk/OurWebsites/HumanGenetics/index.htm NIPT testing must be requested using the specific paper referral form:- ‘NIPT REQUEST FORM FOR HIGHER CHANCE SCREENING RESULT’. NB: Verbal requests for testing on either new or existing samples MUST be confirmed by email to the Duty Scientist ([email protected]) within 72hrs or tests will not be initiated. It is the duty of the clinician/or other health professional to obtain consent from the patient (or patient’s representative) for genetic testing to be carried out. In submitting a sample, the clinician confirms that consent has been obtained: (a) for testing and storage, (b) for the use of this sample and the information generated from it to be shared with members of the patient’s family and their healthcare professionals (if appropriate). Information on issues relating to confidentiality in genetics are contained in the document Consent and Confidentiality in Genetic Practice which can be downloaded from the British Society of Genetic Medicine www.bsgm.org.uk Referral information The following patient information must be supplied legibly with each sample on the referral form/ICE request: Patient information
• Surname • Prename • Gender • Date of birth • CHI number or other unique identifier • Patient location and postcode • Date and time of sampling • Details and location of individual taking the sample • Referring clinician and location
Clinical information (as appropriate)
• Clinical information including suspected disorder • Stage of disease (i.e: diagnosis, monitoring, relapse, post-BMT, any treatment etc.) • Family history and the results of any previous genetic studies • Other references eg Pathology Number • Sample type, and, if applicable, anatomic site • Tests required • LMP/gestation for prenatal samples
When sending samples from an individual with a known family history please provide specific details of any known index case and variant details if available. This is essential for full interpretation of results, and should be discussed with the patient when seeking informed consent. Please note that additional forms are required for some conditions eg breast and colon cancer, diabetes studies, familial hypercholesterolaemia, HOCM, long QT syndrome and endocrine disorders. Please contact the Duty Scientist for details. Information can also be found on Staffnet at: http://staffnet.tayside.scot.nhs.uk/OurWebsites/HumanGenetics/index.htm or in ICE.
Laboratory Genetics User Manual Page 7 of 21
POL003 Version No. 20 August 2021
If further clarification is required in order to complete the request form, please contact the Duty Scientist. It may at times be necessary for the laboratory to contact the referring clinician in order to clarify the request; this could result in a delay in processing the sample. Specimen labels All sample tubes/containers should be clearly labelled with at least the patient surname, forename and date of birth/CHI number. Please ensure that where multiple labels are attached to the sample tube/container, patient details are not obscured. For ICE requests labels are generated which must be adhered to the sample with the barcode edge of the Test Requesting label aligned with the sample tube label edge and applied covering the existing tube label, leaving a small gap. This gap is necessary for visual inspection of tube contents. The barcode should always run vertically on the tube or container. The label should never run around any container as it cannot be scanned at the laboratory. Refer to the ‘Genetics ICE: Guidance for Users’ document mentioned on page 6 of this document for further information. Specimen rejection Samples without the above information (e.g. at least 2 unique identifiers on sample tube) may be rejected. Samples may also be rejected if the sample tube details do not match those on the accompanying request form or if the wrong specimen type is referred for testing. Where samples are rejected, the referring user will be informed. Sample collection Details of the sample requirements for genetic investigations are provided on pages 9-12. Patient preparation prior to sample collection is the responsibility of the clinical team in accordance with the patient’s requirements and consent. Patient preparation, sample collection and disposal of contaminated sharps should be in accordance with local Health and Safety policies and procedures. Correct sample tubes/containers must be used and be within any expiry date. All sample tubes/containers must be securely capped. When taking a blood sample, immediately after collection, gently invert each blood tube several times to distribute the anticoagulant throughout the sample. NB: Clotted samples are not suitable for genetic analysis. High-Risk specimens The laboratory does not have containment facilities to accept samples from individuals with confirmed/suspected cases of prion disease (eg vCJD) or tuberculosis. These samples will be discarded by the laboratory. Sample transport to the laboratory ICE requests: Please use GREEN bags for Genetics ICE requests. Samples for each request should be placed in a separate bag. Please under no circumstances put samples from multiple patients in one bag. For tests where multiple samples are required for the same patient, each label will have the same accession number (e.g. GE14) printed at the top left of the ICE label so samples should be sent together in one bag. Non-ICE requests: Samples sent internally within NHS Tayside should be in sealed plastic bags, with the accompanying form in a separate compartment and folded to display the lab address clearly without exposing patient details. Local arrangements should be followed for sending samples to the laboratory at Ninewells Hospital. Urgent neonatal blood samples are telephoned through by the Neonatal Unit and can be collected by a genetics staff member to prevent delay, if necessary.
Laboratory Genetics User Manual Page 8 of 21
POL003 Version No. 20 August 2021
For samples sent through the post, Royal Mail approved packaging must be used which must be rigid and leak-proof. This is available from the laboratory on request. All samples should be sent to the address shown on p4. NIPT samples taken in Ninewells Hospital are hand delivered by the midwives. For clinics out with Ninewells Hospital specific NIPT sample packs are supplied. The STRECK blood sample must be taken on a Monday or Tuesday only and sent to our laboratory, using the pack provided, the day it is taken. Email the duty scientist to inform them a NIPT sample has been sent. The sample is stable at room temperature and should not be refrigerated. Prior to posting, keep a record of the Royal Mail tracking reference. The envelope has tracked 24 hour pre-paid postage. If a sample is not received in time for the weekly run an email will be sent on a Thursday to inform the midwife of this. To request more NIPT sample packs please email the duty scientist at least 2 weeks prior to them being required. If, upon sample receipt, the packaging is found to be damaged or the integrity of the sample otherwise compromised, or that the safety of the courier or others was jeopardised, the laboratory will contact the referring clinician or laboratory immediately and advise them on appropriate corrective actions to prevent recurrence. All samples should be sent to the laboratory as soon as possible after being taken. If this is not possible, please store samples at 4oC until transport can be arranged (see above, not NIPT samples). Please note that delays in transit can adversely affect genetic investigations which may necessitate re-sampling. When samples are sent to the ESRG laboratory from out with NHS Tayside it is recommended that the exporting laboratory request a receipt to confirm the samples have arrived in our department. This will allow the exporting laboratory to identify samples which have not arrived in a timely manner. Transport medium To obtain transport medium, contact the Duty Scientist with the sample type, and we will supply the appropriate media. The department provides specialised transport media for
• bone marrow aspirates and trephines • lymph node samples • skin biopsies or tumour biopsies, • pregnancy loss and products of conception • chorionic villus samples
Media should be stored at 4oC until the expiry date, and discarded once this has passed.
Laboratory Genetics User Manual Page 9 of 21
POL003 Version No. 20 August 2021
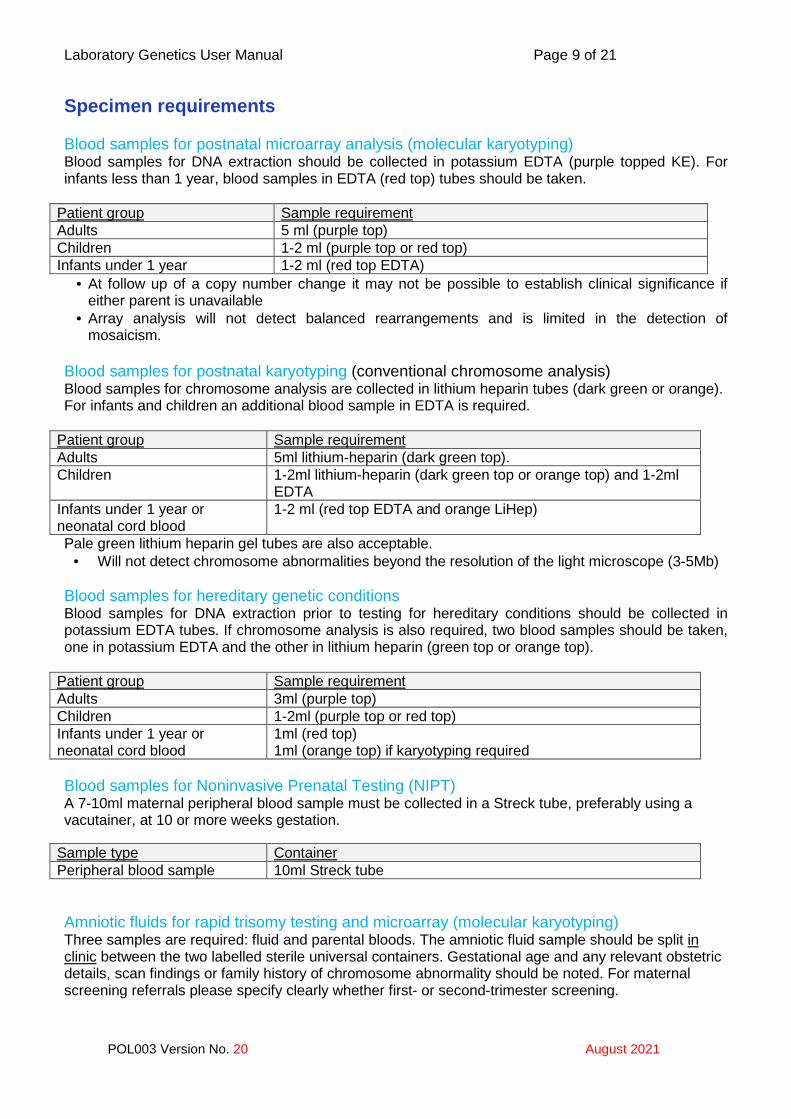
Specimen requirements Blood samples for postnatal microarray analysis (molecular karyotyping) Blood samples for DNA extraction should be collected in potassium EDTA (purple topped KE). For infants less than 1 year, blood samples in EDTA (red top) tubes should be taken.
Patient group Sample requirement Adults 5 ml (purple top) Children 1-2 ml (purple top or red top) Infants under 1 year 1-2 ml (red top EDTA)
• At follow up of a copy number change it may not be possible to establish clinical significance if either parent is unavailable
• Array analysis will not detect balanced rearrangements and is limited in the detection of mosaicism.
Blood samples for postnatal karyotyping (conventional chromosome analysis) Blood samples for chromosome analysis are collected in lithium heparin tubes (dark green or orange). For infants and children an additional blood sample in EDTA is required.
Patient group Sample requirement Adults 5ml lithium-heparin (dark green top). Children 1-2ml lithium-heparin (dark green top or orange top) and 1-2ml
EDTA Infants under 1 year or neonatal cord blood
1-2 ml (red top EDTA and orange LiHep)
Pale green lithium heparin gel tubes are also acceptable. • Will not detect chromosome abnormalities beyond the resolution of the light microscope (3-5Mb)
Blood samples for hereditary genetic conditions Blood samples for DNA extraction prior to testing for hereditary conditions should be collected in potassium EDTA tubes. If chromosome analysis is also required, two blood samples should be taken, one in potassium EDTA and the other in lithium heparin (green top or orange top).
Patient group Sample requirement Adults 3ml (purple top) Children 1-2ml (purple top or red top) Infants under 1 year or neonatal cord blood
1ml (red top) 1ml (orange top) if karyotyping required
Blood samples for Noninvasive Prenatal Testing (NIPT) A 7-10ml maternal peripheral blood sample must be collected in a Streck tube, preferably using a vacutainer, at 10 or more weeks gestation.
Sample type Container Peripheral blood sample 10ml Streck tube
Amniotic fluids for rapid trisomy testing and microarray (molecular karyotyping) Three samples are required: fluid and parental bloods. The amniotic fluid sample should be split in clinic between the two labelled sterile universal containers. Gestational age and any relevant obstetric details, scan findings or family history of chromosome abnormality should be noted. For maternal screening referrals please specify clearly whether first- or second-trimester screening.
Laboratory Genetics User Manual Page 10 of 21
POL003 Version No. 20 August 2021
Sample type Container 3ml Amniotic Fluid Sterile 20ml universal container Remainder of Amniotic Fluid (8mls minimum requirement)
Sterile 20ml universal container
Maternal Blood 3ml EDTA ( purple top) Paternal Blood 3ml EDTA ( purple top)
• Prompt dispatch to the laboratory is essential • Reporting times and interpretation may be affected if a prenatal sample is not accompanied by
parental bloods • Microarray does not detect balanced rearrangements and is limited in detection of mosaicism • Should the array fail chromosome analysis will be carried out from cultured amniocytes • Fetal karyotyping may not detect subtle chromosome abnormalities or mosaicism • Small or significantly blood stained samples may be unsuitable for QF-PCR
Chorionic villus samples for rapid trisomy testing and microarray (molecular karyotyping) Three samples are required: villi and parental bloods.
Sample type Container 10-20mg of villi Sterile 20ml universal containing transport medium Maternal Blood 3ml EDTA (purple top) Paternal Blood 3ml EDTA ( purple top)
• Chorionic villus samples are accepted by prior arrangement with the laboratory. • All samples MUST be accompanied by a 3ml maternal EDTA blood sample • A 3ml paternal EDTA blood sample is also requested • Reporting times and interpretation may be affected if a prenatal sample is not accompanied by
parental bloods • Sterile heparinised CVS collection medium is available from the Duty Scientist • Pre-warm media to room temperature before use and discard after expiry. • CVS collection medium is for IN VITRO use only • Samples MUST be promptly despatched to the laboratory (routinely hand delivered by a member
of Ultrasound staff). • A trisomy 13, 18 or 21 finding in the absence of an abnormal scan may require long term cultures
and/or amniocentesis follow-up for interpretation. • For technical reasons high-risk samples (eg: Hepatitis B, HIV), are prone to maternal cell
contamination, and amniocentesis sampling may be preferable. Fetal tissue samples Samples of fetal tissue (e.g skin, muscle) and a separate sample of placenta (1cm 3) should be sent from recurrent pregnancy losses (>/=3 losses) and TOPs (for fetal abnormality). Fetal skin samples should be “full depth”, not “skin peel” samples. Macerated samples are NOT suitable for cytogenetics and these cases require a placental sample only. For earlier losses, a sample of products of conception may be sent. Please send a maternal blood EDTA sample with these samples, which is used to exclude maternal cell contamination. No testing will be initiated until a maternal sample is provided. A paternal sample is not required unless specifically requested by the Genetics department. Fetal and placenta samples should be sent via Pathology(Highland)/Mortuary(Tayside) in sterile transport medium which is available upon request from the Duty Scientist.
Sample type Container Fetal Tissue Sterile 20ml universal containing transport medium Placental Sample Sterile 20ml universal containing transport medium Maternal Blood 4ml EDTA (purple top)
Laboratory Genetics User Manual Page 11 of 21
POL003 Version No. 20 August 2021
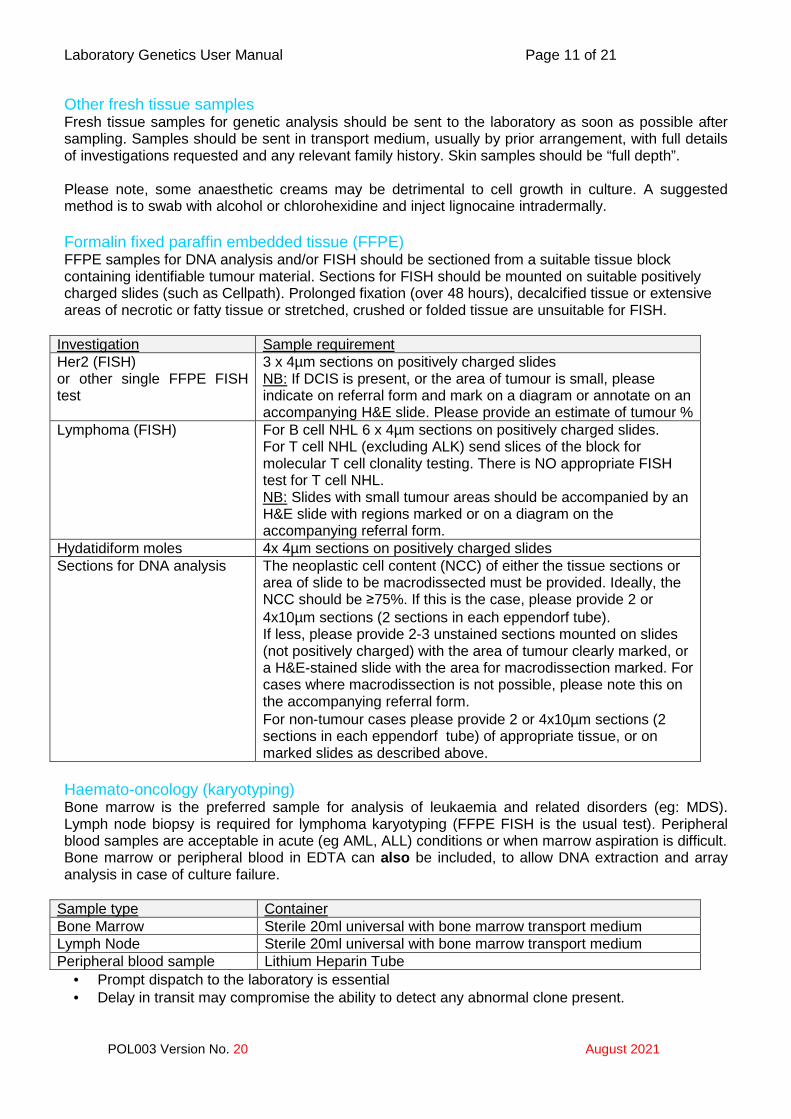
Other fresh tissue samples Fresh tissue samples for genetic analysis should be sent to the laboratory as soon as possible after sampling. Samples should be sent in transport medium, usually by prior arrangement, with full details of investigations requested and any relevant family history. Skin samples should be “full depth”. Please note, some anaesthetic creams may be detrimental to cell growth in culture. A suggested method is to swab with alcohol or chlorohexidine and inject lignocaine intradermally. Formalin fixed paraffin embedded tissue (FFPE) FFPE samples for DNA analysis and/or FISH should be sectioned from a suitable tissue block containing identifiable tumour material. Sections for FISH should be mounted on suitable positively charged slides (such as Cellpath). Prolonged fixation (over 48 hours), decalcified tissue or extensive areas of necrotic or fatty tissue or stretched, crushed or folded tissue are unsuitable for FISH.
Investigation Sample requirement Her2 (FISH) or other single FFPE FISH test
3 x 4µm sections on positively charged slides NB: If DCIS is present, or the area of tumour is small, please indicate on referral form and mark on a diagram or annotate on an accompanying H&E slide. Please provide an estimate of tumour %
Lymphoma (FISH) For B cell NHL 6 x 4µm sections on positively charged slides. For T cell NHL (excluding ALK) send slices of the block for molecular T cell clonality testing. There is NO appropriate FISH test for T cell NHL. NB: Slides with small tumour areas should be accompanied by an H&E slide with regions marked or on a diagram on the accompanying referral form.
Hydatidiform moles 4x 4µm sections on positively charged slides Sections for DNA analysis The neoplastic cell content (NCC) of either the tissue sections or
area of slide to be macrodissected must be provided. Ideally, the NCC should be ≥75%. If this is the case, please provide 2 or 4x10µm sections (2 sections in each eppendorf tube). If less, please provide 2-3 unstained sections mounted on slides (not positively charged) with the area of tumour clearly marked, or a H&E-stained slide with the area for macrodissection marked. For cases where macrodissection is not possible, please note this on the accompanying referral form. For non-tumour cases please provide 2 or 4x10µm sections (2 sections in each eppendorf tube) of appropriate tissue, or on marked slides as described above.
Haemato-oncology (karyotyping) Bone marrow is the preferred sample for analysis of leukaemia and related disorders (eg: MDS). Lymph node biopsy is required for lymphoma karyotyping (FFPE FISH is the usual test). Peripheral blood samples are acceptable in acute (eg AML, ALL) conditions or when marrow aspiration is difficult. Bone marrow or peripheral blood in EDTA can also be included, to allow DNA extraction and array analysis in case of culture failure.
Sample type Container Bone Marrow Sterile 20ml universal with bone marrow transport medium Lymph Node Sterile 20ml universal with bone marrow transport medium Peripheral blood sample Lithium Heparin Tube
• Prompt dispatch to the laboratory is essential • Delay in transit may compromise the ability to detect any abnormal clone present.
Laboratory Genetics User Manual Page 12 of 21
POL003 Version No. 20 August 2021
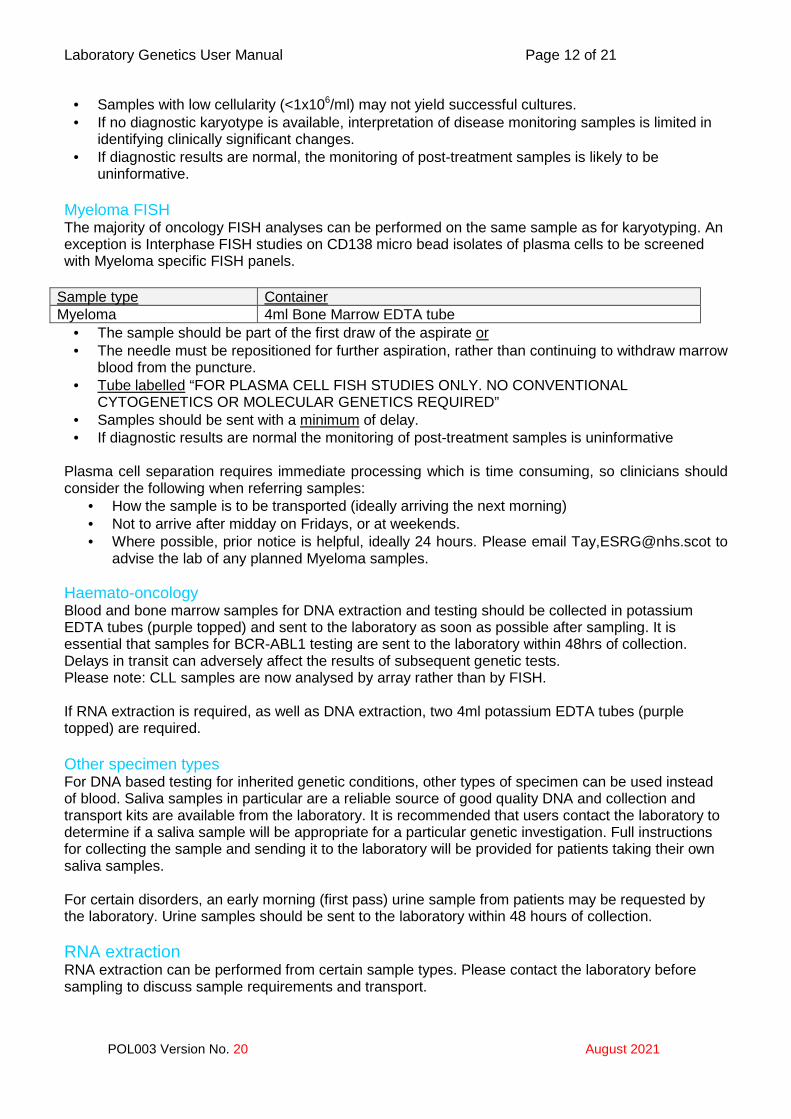
• Samples with low cellularity (<1x106/ml) may not yield successful cultures. • If no diagnostic karyotype is available, interpretation of disease monitoring samples is limited in
identifying clinically significant changes. • If diagnostic results are normal, the monitoring of post-treatment samples is likely to be
uninformative. Myeloma FISH The majority of oncology FISH analyses can be performed on the same sample as for karyotyping. An exception is Interphase FISH studies on CD138 micro bead isolates of plasma cells to be screened with Myeloma specific FISH panels.
Sample type Container Myeloma 4ml Bone Marrow EDTA tube
• The sample should be part of the first draw of the aspirate or • The needle must be repositioned for further aspiration, rather than continuing to withdraw marrow
blood from the puncture. • Tube labelled “FOR PLASMA CELL FISH STUDIES ONLY. NO CONVENTIONAL
CYTOGENETICS OR MOLECULAR GENETICS REQUIRED” • Samples should be sent with a minimum of delay. • If diagnostic results are normal the monitoring of post-treatment samples is uninformative
Plasma cell separation requires immediate processing which is time consuming, so clinicians should consider the following when referring samples:
• How the sample is to be transported (ideally arriving the next morning) • Not to arrive after midday on Fridays, or at weekends. • Where possible, prior notice is helpful, ideally 24 hours. Please email Tay,[email protected] to
advise the lab of any planned Myeloma samples.
Haemato-oncology Blood and bone marrow samples for DNA extraction and testing should be collected in potassium EDTA tubes (purple topped) and sent to the laboratory as soon as possible after sampling. It is essential that samples for BCR-ABL1 testing are sent to the laboratory within 48hrs of collection. Delays in transit can adversely affect the results of subsequent genetic tests. Please note: CLL samples are now analysed by array rather than by FISH. If RNA extraction is required, as well as DNA extraction, two 4ml potassium EDTA tubes (purple topped) are required. Other specimen types For DNA based testing for inherited genetic conditions, other types of specimen can be used instead of blood. Saliva samples in particular are a reliable source of good quality DNA and collection and transport kits are available from the laboratory. It is recommended that users contact the laboratory to determine if a saliva sample will be appropriate for a particular genetic investigation. Full instructions for collecting the sample and sending it to the laboratory will be provided for patients taking their own saliva samples. For certain disorders, an early morning (first pass) urine sample from patients may be requested by the laboratory. Urine samples should be sent to the laboratory within 48 hours of collection. RNA extraction RNA extraction can be performed from certain sample types. Please contact the laboratory before sampling to discuss sample requirements and transport.
Laboratory Genetics User Manual Page 13 of 21
POL003 Version No. 20 August 2021
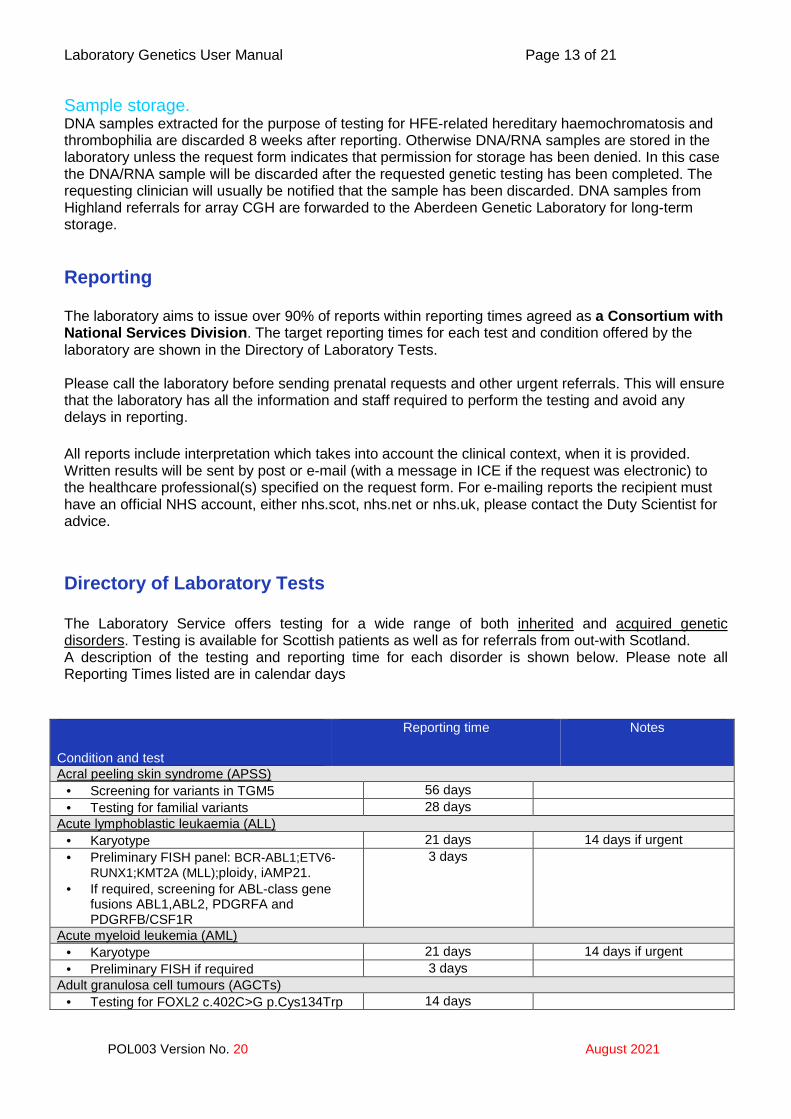
Sample storage. DNA samples extracted for the purpose of testing for HFE-related hereditary haemochromatosis and thrombophilia are discarded 8 weeks after reporting. Otherwise DNA/RNA samples are stored in the laboratory unless the request form indicates that permission for storage has been denied. In this case the DNA/RNA sample will be discarded after the requested genetic testing has been completed. The requesting clinician will usually be notified that the sample has been discarded. DNA samples from Highland referrals for array CGH are forwarded to the Aberdeen Genetic Laboratory for long-term storage. Reporting The laboratory aims to issue over 90% of reports within reporting times agreed as a Consortium with National Services Division . The target reporting times for each test and condition offered by the laboratory are shown in the Directory of Laboratory Tests. Please call the laboratory before sending prenatal requests and other urgent referrals. This will ensure that the laboratory has all the information and staff required to perform the testing and avoid any delays in reporting. All reports include interpretation which takes into account the clinical context, when it is provided. Written results will be sent by post or e-mail (with a message in ICE if the request was electronic) to the healthcare professional(s) specified on the request form. For e-mailing reports the recipient must have an official NHS account, either nhs.scot, nhs.net or nhs.uk, please contact the Duty Scientist for advice. Directory of Laboratory Tests The Laboratory Service offers testing for a wide range of both inherited and acquired genetic disorders. Testing is available for Scottish patients as well as for referrals from out-with Scotland. A description of the testing and reporting time for each disorder is shown below. Please note all Reporting Times listed are in calendar days
Condition and test
Reporting time Notes
Acral peeling skin syndrome (APSS) • Screening for variants in TGM5 56 days • Testing for familial variants 28 days
Acute lymphoblastic leukaemia (ALL) • Karyotype 21 days 14 days if urgent • Preliminary FISH panel: BCR-ABL1;ETV6-
RUNX1;KMT2A (MLL);ploidy, iAMP21. • If required, screening for ABL-class gene
fusions ABL1,ABL2, PDGRFA and PDGRFB/CSF1R
3 days
Acute myeloid leukemia (AML) • Karyotype 21 days 14 days if urgent • Preliminary FISH if required 3 days
Adult granulosa cell tumours (AGCTs) • Testing for FOXL2 c.402C>G p.Cys134Trp 14 days
Laboratory Genetics User Manual Page 14 of 21
POL003 Version No. 20 August 2021
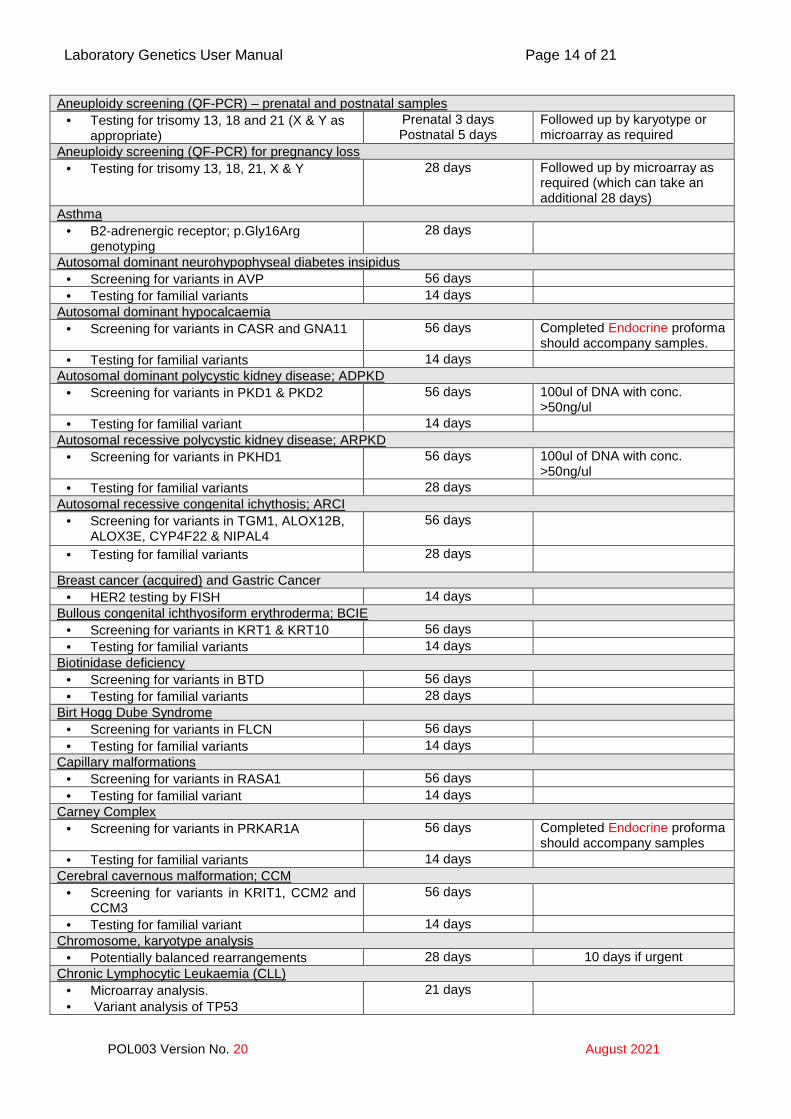
Aneuploidy screening (QF-PCR) – prenatal and postnatal samples • Testing for trisomy 13, 18 and 21 (X & Y as
appropriate) Prenatal 3 days Postnatal 5 days
Followed up by karyotype or microarray as required
Aneuploidy screening (QF-PCR) for pregnancy loss • Testing for trisomy 13, 18, 21, X & Y 28 days Followed up by microarray as
required (which can take an additional 28 days)
Asthma • B2-adrenergic receptor; p.Gly16Arg
genotyping 28 days
Autosomal dominant neurohypophyseal diabetes insipidus • Screening for variants in AVP 56 days • Testing for familial variants 14 days
Autosomal dominant hypocalcaemia • Screening for variants in CASR and GNA11 56 days Completed Endocrine proforma
should accompany samples. • Testing for familial variants 14 days
Autosomal dominant polycystic kidney disease; ADPKD • Screening for variants in PKD1 & PKD2 56 days 100ul of DNA with conc.
>50ng/ul • Testing for familial variant 14 days
Autosomal recessive polycystic kidney disease; ARPKD • Screening for variants in PKHD1 56 days 100ul of DNA with conc.
>50ng/ul • Testing for familial variants 28 days
Autosomal recessive congenital ichythosis; ARCI • Screening for variants in TGM1, ALOX12B,
ALOX3E, CYP4F22 & NIPAL4 56 days
• Testing for familial variants 28 days
Breast cancer (acquired) and Gastric Cancer • HER2 testing by FISH 14 days
Bullous congenital ichthyosiform erythroderma; BCIE • Screening for variants in KRT1 & KRT10 56 days • Testing for familial variants 14 days
Biotinidase deficiency • Screening for variants in BTD 56 days • Testing for familial variants 28 days
Birt Hogg Dube Syndrome • Screening for variants in FLCN 56 days • Testing for familial variants 14 days
Capillary malformations • Screening for variants in RASA1 56 days • Testing for familial variant 14 days
Carney Complex • Screening for variants in PRKAR1A 56 days Completed Endocrine proforma
should accompany samples • Testing for familial variants 14 days
Cerebral cavernous malformation; CCM • Screening for variants in KRIT1, CCM2 and
CCM3 56 days
• Testing for familial variant 14 days Chromosome, karyotype analysis
• Potentially balanced rearrangements 28 days 10 days if urgent Chronic Lymphocytic Leukaemia (CLL)
• Microarray analysis. • Variant analysis of TP53
21 days
Laboratory Genetics User Manual Page 15 of 21
POL003 Version No. 20 August 2021
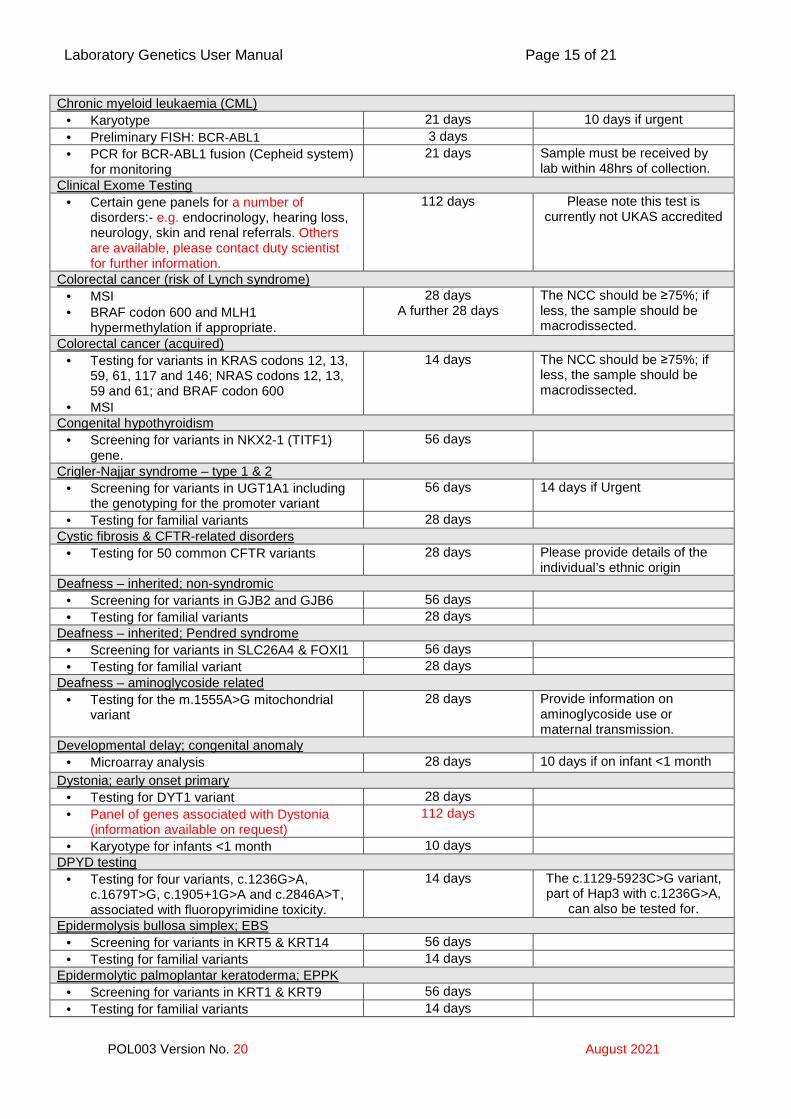
Chronic myeloid leukaemia (CML) • Karyotype 21 days 10 days if urgent • Preliminary FISH: BCR-ABL1 3 days • PCR for BCR-ABL1 fusion (Cepheid system)
for monitoring 21 days
Sample must be received by lab within 48hrs of collection.
Clinical Exome Testing • Certain gene panels for a number of
disorders:- e.g. endocrinology, hearing loss, neurology, skin and renal referrals. Others are available, please contact duty scientist for further information.
112 days Please note this test is currently not UKAS accredited
Colorectal cancer (risk of Lynch syndrome) • MSI • BRAF codon 600 and MLH1
hypermethylation if appropriate.
28 days A further 28 days
The NCC should be ≥75%; if less, the sample should be macrodissected.
Colorectal cancer (acquired) • Testing for variants in KRAS codons 12, 13,
59, 61, 117 and 146; NRAS codons 12, 13, 59 and 61; and BRAF codon 600
• MSI
14 days The NCC should be ≥75%; if less, the sample should be macrodissected.
Congenital hypothyroidism • Screening for variants in NKX2-1 (TITF1)
gene. 56 days
Crigler-Najjar syndrome – type 1 & 2 • Screening for variants in UGT1A1 including
the genotyping for the promoter variant 56 days 14 days if Urgent
• Testing for familial variants 28 days Cystic fibrosis & CFTR-related disorders
• Testing for 50 common CFTR variants 28 days Please provide details of the individual’s ethnic origin
Deafness – inherited; non-syndromic • Screening for variants in GJB2 and GJB6 56 days • Testing for familial variants 28 days
Deafness – inherited; Pendred syndrome • Screening for variants in SLC26A4 & FOXI1 56 days • Testing for familial variant 28 days
Deafness – aminoglycoside related • Testing for the m.1555A>G mitochondrial
variant 28 days Provide information on
aminoglycoside use or maternal transmission.
Developmental delay; congenital anomaly • Microarray analysis 28 days 10 days if on infant <1 month
Dystonia; early onset primary • Testing for DYT1 variant 28 days • Panel of genes associated with Dystonia
(information available on request) 112 days
• Karyotype for infants <1 month 10 days DPYD testing
• Testing for four variants, c.1236G>A, c.1679T>G, c.1905+1G>A and c.2846A>T, associated with fluoropyrimidine toxicity.
14 days The c.1129-5923C>G variant, part of Hap3 with c.1236G>A,
can also be tested for. Epidermolysis bullosa simplex; EBS
• Screening for variants in KRT5 & KRT14 56 days • Testing for familial variants 14 days
Epidermolytic palmoplantar keratoderma; EPPK • Screening for variants in KRT1 & KRT9 56 days • Testing for familial variants 14 days
Laboratory Genetics User Manual Page 16 of 21
POL003 Version No. 20 August 2021
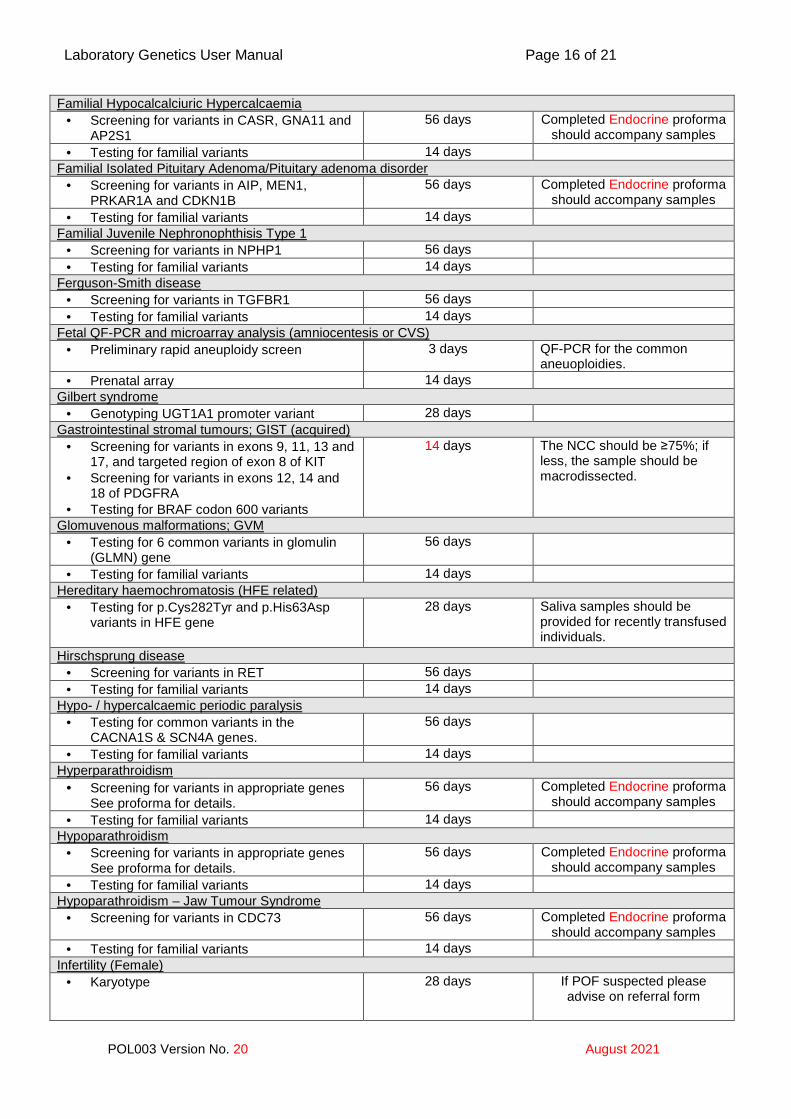
Familial Hypocalcalciuric Hypercalcaemia • Screening for variants in CASR, GNA11 and
AP2S1 56 days Completed Endocrine proforma
should accompany samples • Testing for familial variants 14 days
Familial Isolated Pituitary Adenoma/Pituitary adenoma disorder • Screening for variants in AIP, MEN1,
PRKAR1A and CDKN1B 56 days Completed Endocrine proforma
should accompany samples • Testing for familial variants 14 days
Familial Juvenile Nephronophthisis Type 1 • Screening for variants in NPHP1 56 days • Testing for familial variants 14 days
Ferguson-Smith disease • Screening for variants in TGFBR1 56 days • Testing for familial variants 14 days
Fetal QF-PCR and microarray analysis (amniocentesis or CVS) • Preliminary rapid aneuploidy screen 3 days QF-PCR for the common
aneuoploidies. • Prenatal array 14 days
Gilbert syndrome • Genotyping UGT1A1 promoter variant 28 days
Gastrointestinal stromal tumours; GIST (acquired) • Screening for variants in exons 9, 11, 13 and
17, and targeted region of exon 8 of KIT • Screening for variants in exons 12, 14 and
18 of PDGFRA • Testing for BRAF codon 600 variants
14 days The NCC should be ≥75%; if less, the sample should be macrodissected.
Glomuvenous malformations; GVM • Testing for 6 common variants in glomulin
(GLMN) gene 56 days
• Testing for familial variants 14 days Hereditary haemochromatosis (HFE related)
• Testing for p.Cys282Tyr and p.His63Asp variants in HFE gene
28 days Saliva samples should be provided for recently transfused individuals.
Hirschsprung disease • Screening for variants in RET 56 days • Testing for familial variants 14 days
Hypo- / hypercalcaemic periodic paralysis • Testing for common variants in the
CACNA1S & SCN4A genes. 56 days
• Testing for familial variants 14 days Hyperparathroidism
• Screening for variants in appropriate genes See proforma for details.
56 days Completed Endocrine proforma should accompany samples
• Testing for familial variants 14 days Hypoparathroidism
• Screening for variants in appropriate genes See proforma for details.
56 days Completed Endocrine proforma should accompany samples
• Testing for familial variants 14 days Hypoparathroidism – Jaw Tumour Syndrome
• Screening for variants in CDC73 56 days Completed Endocrine proforma should accompany samples
• Testing for familial variants 14 days Infertility (Female)
• Karyotype
28 days If POF suspected please advise on referral form
Laboratory Genetics User Manual Page 17 of 21
POL003 Version No. 20 August 2021
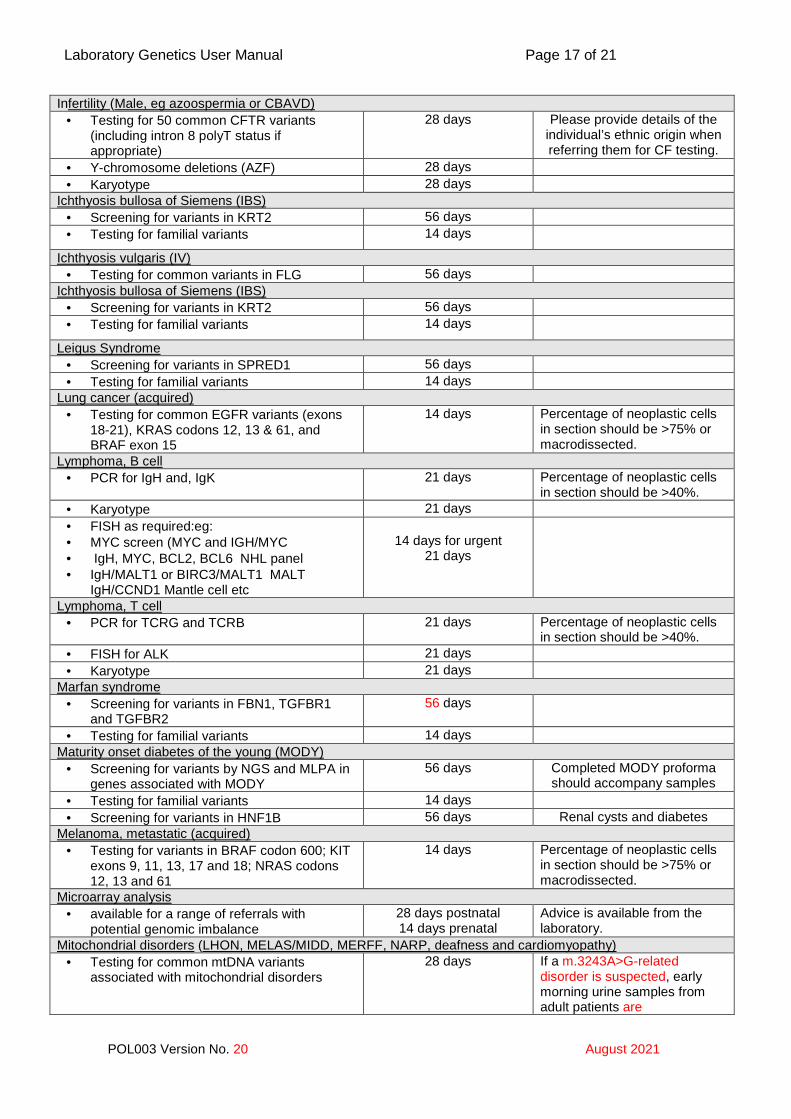
Infertility (Male, eg azoospermia or CBAVD) • Testing for 50 common CFTR variants
(including intron 8 polyT status if appropriate)
28 days Please provide details of the individual’s ethnic origin when referring them for CF testing.
• Y-chromosome deletions (AZF) 28 days • Karyotype 28 days
Ichthyosis bullosa of Siemens (IBS) • Screening for variants in KRT2 56 days • Testing for familial variants 14 days
Ichthyosis vulgaris (IV) • Testing for common variants in FLG 56 days
Ichthyosis bullosa of Siemens (IBS) • Screening for variants in KRT2 56 days • Testing for familial variants 14 days
Leigus Syndrome • Screening for variants in SPRED1 56 days • Testing for familial variants 14 days
Lung cancer (acquired) • Testing for common EGFR variants (exons
18-21), KRAS codons 12, 13 & 61, and BRAF exon 15
14 days Percentage of neoplastic cells in section should be >75% or macrodissected.
Lymphoma, B cell • PCR for IgH and, IgK 21 days Percentage of neoplastic cells
in section should be >40%. • Karyotype 21 days • FISH as required:eg: • MYC screen (MYC and IGH/MYC • IgH, MYC, BCL2, BCL6 NHL panel • IgH/MALT1 or BIRC3/MALT1 MALT
IgH/CCND1 Mantle cell etc
14 days for urgent
21 days
Lymphoma, T cell • PCR for TCRG and TCRB 21 days Percentage of neoplastic cells
in section should be >40%. • FISH for ALK 21 days • Karyotype 21 days
Marfan syndrome • Screening for variants in FBN1, TGFBR1
and TGFBR2 56 days
• Testing for familial variants 14 days Maturity onset diabetes of the young (MODY)
• Screening for variants by NGS and MLPA in genes associated with MODY
56 days Completed MODY proforma should accompany samples
• Testing for familial variants 14 days • Screening for variants in HNF1B 56 days Renal cysts and diabetes
Melanoma, metastatic (acquired) • Testing for variants in BRAF codon 600; KIT
exons 9, 11, 13, 17 and 18; NRAS codons 12, 13 and 61
14 days Percentage of neoplastic cells in section should be >75% or macrodissected.
Microarray analysis • available for a range of referrals with
potential genomic imbalance 28 days postnatal 14 days prenatal
Advice is available from the laboratory.
Mitochondrial disorders (LHON, MELAS/MIDD, MERFF, NARP, deafness and cardiomyopathy) • Testing for common mtDNA variants
associated with mitochondrial disorders 28 days If a m.3243A>G-related
disorder is suspected, early morning urine samples from adult patients are
Laboratory Genetics User Manual Page 18 of 21
POL003 Version No. 20 August 2021
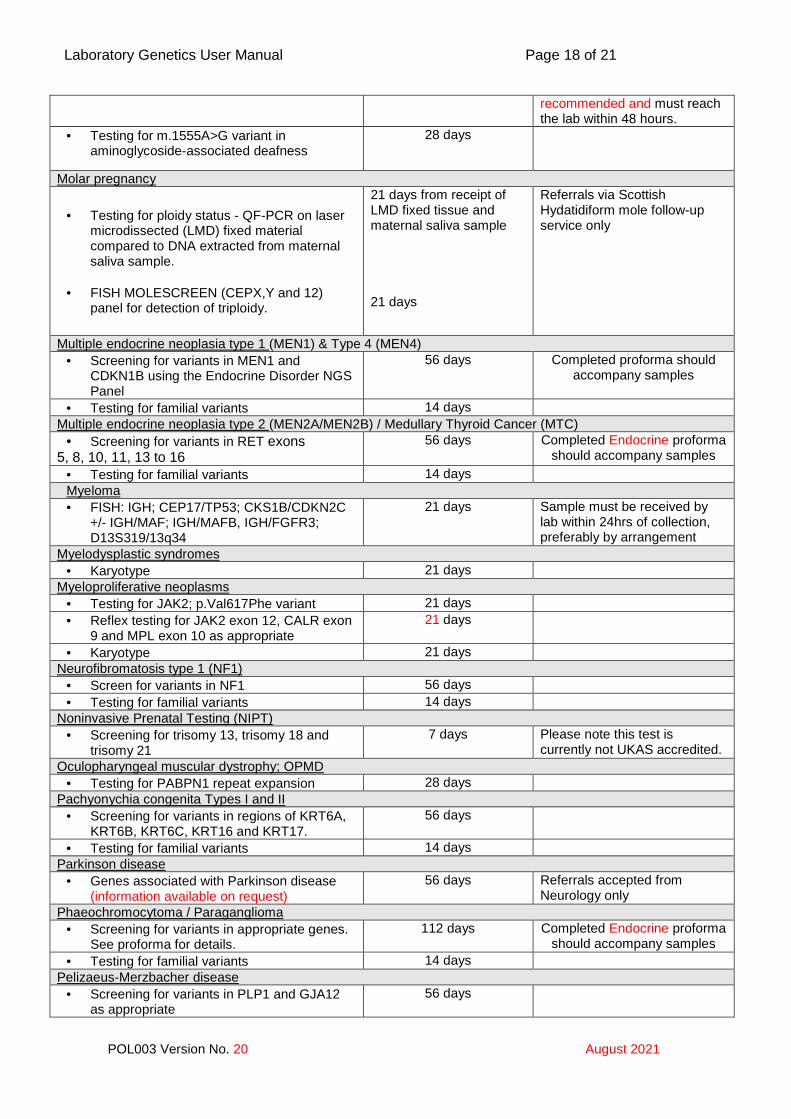
recommended and must reach the lab within 48 hours.
• Testing for m.1555A>G variant in aminoglycoside-associated deafness
28 days
Molar pregnancy
• Testing for ploidy status - QF-PCR on laser microdissected (LMD) fixed material compared to DNA extracted from maternal saliva sample.
• FISH MOLESCREEN (CEPX,Y and 12)
panel for detection of triploidy.
21 days from receipt of LMD fixed tissue and maternal saliva sample 21 days
Referrals via Scottish Hydatidiform mole follow-up service only
Multiple endocrine neoplasia type 1 (MEN1) & Type 4 (MEN4) • Screening for variants in MEN1 and
CDKN1B using the Endocrine Disorder NGS Panel
56 days Completed proforma should accompany samples
• Testing for familial variants 14 days Multiple endocrine neoplasia type 2 (MEN2A/MEN2B) / Medullary Thyroid Cancer (MTC)
• Screening for variants in RET exons 5, 8, 10, 11, 13 to 16
56 days Completed Endocrine proforma should accompany samples
• Testing for familial variants 14 days Myeloma • FISH: IGH; CEP17/TP53; CKS1B/CDKN2C
+/- IGH/MAF; IGH/MAFB, IGH/FGFR3; D13S319/13q34
21 days Sample must be received by lab within 24hrs of collection, preferably by arrangement
Myelodysplastic syndromes • Karyotype 21 days
Myeloproliferative neoplasms • Testing for JAK2; p.Val617Phe variant 21 days • Reflex testing for JAK2 exon 12, CALR exon
9 and MPL exon 10 as appropriate 21 days
• Karyotype 21 days Neurofibromatosis type 1 (NF1)
• Screen for variants in NF1 56 days • Testing for familial variants 14 days
Noninvasive Prenatal Testing (NIPT) • Screening for trisomy 13, trisomy 18 and
trisomy 21 7 days Please note this test is
currently not UKAS accredited. Oculopharyngeal muscular dystrophy; OPMD
• Testing for PABPN1 repeat expansion 28 days Pachyonychia congenita Types I and II
• Screening for variants in regions of KRT6A, KRT6B, KRT6C, KRT16 and KRT17.
56 days
• Testing for familial variants 14 days Parkinson disease
• Genes associated with Parkinson disease (information available on request)
56 days Referrals accepted from Neurology only
Phaeochromocytoma / Paraganglioma • Screening for variants in appropriate genes.
See proforma for details. 112 days Completed Endocrine proforma
should accompany samples • Testing for familial variants 14 days
Pelizaeus-Merzbacher disease • Screening for variants in PLP1 and GJA12
as appropriate 56 days
Laboratory Genetics User Manual Page 19 of 21
POL003 Version No. 20 August 2021
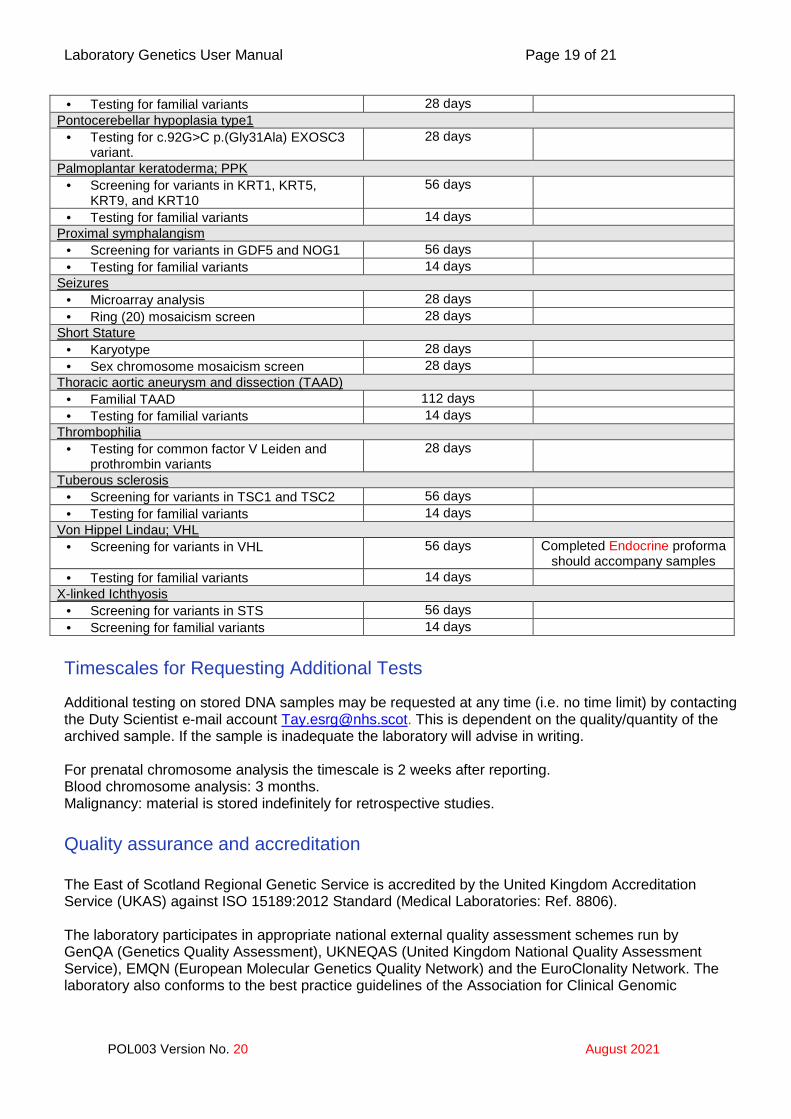
• Testing for familial variants 28 days Pontocerebellar hypoplasia type1
• Testing for c.92G>C p.(Gly31Ala) EXOSC3 variant.
28 days
Palmoplantar keratoderma; PPK • Screening for variants in KRT1, KRT5,
KRT9, and KRT10 56 days
• Testing for familial variants 14 days Proximal symphalangism
• Screening for variants in GDF5 and NOG1 56 days • Testing for familial variants 14 days
Seizures • Microarray analysis 28 days • Ring (20) mosaicism screen 28 days
Short Stature • Karyotype 28 days • Sex chromosome mosaicism screen 28 days
Thoracic aortic aneurysm and dissection (TAAD) • Familial TAAD 112 days • Testing for familial variants 14 days
Thrombophilia • Testing for common factor V Leiden and
prothrombin variants 28 days
Tuberous sclerosis • Screening for variants in TSC1 and TSC2 56 days • Testing for familial variants 14 days
Von Hippel Lindau; VHL • Screening for variants in VHL 56 days Completed Endocrine proforma
should accompany samples • Testing for familial variants 14 days
X-linked Ichthyosis • Screening for variants in STS 56 days • Screening for familial variants 14 days
Timescales for Requesting Additional Tests
Additional testing on stored DNA samples may be requested at any time (i.e. no time limit) by contacting the Duty Scientist e-mail account [email protected]. This is dependent on the quality/quantity of the archived sample. If the sample is inadequate the laboratory will advise in writing. For prenatal chromosome analysis the timescale is 2 weeks after reporting. Blood chromosome analysis: 3 months. Malignancy: material is stored indefinitely for retrospective studies. Quality assurance and accreditation The East of Scotland Regional Genetic Service is accredited by the United Kingdom Accreditation Service (UKAS) against ISO 15189:2012 Standard (Medical Laboratories: Ref. 8806). The laboratory participates in appropriate national external quality assessment schemes run by GenQA (Genetics Quality Assessment), UKNEQAS (United Kingdom National Quality Assessment Service), EMQN (European Molecular Genetics Quality Network) and the EuroClonality Network. The laboratory also conforms to the best practice guidelines of the Association for Clinical Genomic
Laboratory Genetics User Manual Page 20 of 21
POL003 Version No. 20 August 2021
Science (ACGS), which is a constituent organisation of the British Society for Genetic Medicine (BSGM). Users will be informed of any incidence of persistent poor performance in the external quality assurance schemes. Contacts for clinical advice Clinical advice is available from the Consultant Clinical Geneticists: Dr David Goudie (Clinical Lead) Tel: 01382 632151 (Ext 32151) Email: [email protected] Dr Jonathan Berg Tel: 01382 635716 (Ext 35716) Email: [email protected] Dr Catherine McWilliam Tel: 01382 740341 Email: [email protected] Advice about Genetic Counselling can be obtained from the Lead Genetic Counsellor Ms Jacqueline Dunlop Tel: 01382 496369 (Ext 36369; 32035) Email: [email protected] Complaints and suggestions Any comments, suggestions, concerns or complaints should be directed in the first instance to the Head of Laboratory Services, Consultant Clinical Scientists or Quality Manager. All complaints will be addressed promptly. Comments and suggestions may also be logged using the following link https://www.surveymonkey.co.uk/r/5LG9PF5 A report on the most recent user feedback survey can be downloaded from https://www.nhstayside.scot.nhs.uk/OurServicesA-Z/Genetics/PROD_295549/index.htm Formal complaints if deemed necessary should be sent to the Complaints and Feedback team at:
Complaints and Feedback Team, Ninewells Hospital, Dundee DD1 9SY Tel: 0800 027 5507 Email: [email protected]
Laboratory Genetics User Manual Page 21 of 21
POL003 Version No. 20 August 2021
Other Scottish Genetic Consortium Laboratories North of Scotland Regional Genetic Service Polwarth Building, University of Aberdeen Medical School, Foresterhill, Aberdeen AB25 2ZD Phone: 01224 553893 E-mail: [email protected] South East Scotland Genetics Service Molecular Medicine Centre Western General Hospital Crewe Road Edinburgh EH4 2XU Phone: 0131 651 1116 / 1270 E-mail [email protected] West of Scotland Genetics Service Laboratory Genetics Level 2B Laboratory Medicine Queen Elizabeth University Hospital Glasgow G514TF Phone: 0141 354 9330 E-mail: [email protected]
Further Information Further information is available on our Departmental web site www.esrg.scot.nhs.uk or www.nhstayside.scot.nhs.uk/OurServicesA-Z/Genetics/index.htm














![Molecular Genetics DNA: The Genetic Material [12.1]](https://img.pdfslide.net/doc/110x75/56649eca5503460f94bd860d/molecular-genetics-dna-the-genetic-material-121.jpg)