Embed Size (px)
Citation preview

DATA ANALYSIS•Weight measures (i.e. IBW, ABW, LBW), renal clearance (using Cockcroft-Gault, MDRD, and CKD-EPI equations) and patient-specific PK values (e.g. ke, Vd, and Clvanc ) were determined for each patient (n=239).•All data were analyzed using SPSS 19.0 (Chicago, IL) with p-value < 0.05 being statistically significant.•Vancomycin Vd was normalized to all weight descriptors using ANOVA with post-hoc comparisons via Bonferroni test.•Ordinary least squares regression was used to compare renal clearance between Cockcroft-Gault, MDRD, and CKD-EPI, as a predictor of vancomycin clearance.
Life Beyond Cockcroft-Gault: Is there a better method to optimize vancomycin dosing?
•••••Elva Angelique Van Devender, Ph.D., Pharm.D., Ravina Kullar, Pharm.D., MPH, James Leggett, MD
Providence Health and Services • Portland, Oregon
BACKGROUND•Vancomycin is the mainstay of treatment for complicated Gram-positive resistant infections, such as methicillin-resistant Staphylococcus aureus (MRSA).
•The most appropriate weight descriptor for dosing vancomycin is unknown. Historically, vancomycin dosing has been based on total body weight (TBW).
•Vancomycin clearance is typically assessed using the Cockcroft-Gault equation. The utility of newer equations (the Modification of Diet in Renal Disease (MDRD) equation and the Chronic Kidney Disease-Epidemiology (CKD-EPI) equation) in vancomycin dosing is unknown.
METHODSPATIENT POPULATIONInclusion criteria: Adult patients >18 years old with > 2 documented vancomycin trough concentrations admitted to Providence St. Vincent Medical Center and Providence Portland Medical Center from January-October 2011. Exclusion criteria: Patients with rapidly changing or unstable renal function (SCr increase of > 0.5 from baseline or patients on hemodialysis).
DATA ABSTRACTED•Patient demographics, height, weight, BMI, serum creatinine, length of stay•Vancomycin doses, trough levels, indication for therapy
CONCLUSIONS•Trend toward TBW as the most accurate weight predictor (i.e. least variable) in between weight categories to best estimate vancomycin Vd (p > 0.567). IBW was the least accurate predictor (i.e. most variable) in between weight categories in predicting Vd (p < 0.023).•Mean Vd= 0.47 L/kg in our study•The Cockcroft-Gault equation using adjusted body weight (ABW) was the method most closely correlated to vancomycin clearance.
OBJECTIVES OF THE CURRENT STUDY•To determine which weight parameter (e.g. TBW, IBW, LBW, or ABW) best estimates vancomycin Vd
•To compare the Cockcroft-Gault, MDRD, and CKD-EPI equations to determine which method is the most precise in effectively dosing vancomycin
WHAT THEY
DID
• Pai et. al. optimized the dosing of aminoglycosides by evaluating a range of patient weights and various renal function equations.
WHAT THEY FOUND
• LBW best estimated Vd• CKD-EPI best predicted aminoglycoside clearance
AMINOGLYCOSIDE STUDY:1 SEPTEMBER 2011
LIMITATIONS•Assumed vancomycin Cmax of 40 for each patient•Small sample size; large percentage of Caucasian population•Not all patients were at steady state
DISCLOSURESAll authors have nothing to disclose.
RESULTS
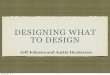
OBESITY CATEGORIES* (N=239) INDICATIONS FOR VANCOMYCIN
5.9% 29.7%
21.8%15.9
%
7.9%
18.8%
Underweight Normal WeightOverweight Moderate ObesitySevere Obesity Morbid Obesity
RESULTS PATIENT CHARACTERISTICS (N=239)
Characteristic Median (IQR) or n (%)
Age (years) 61 (49-75)
FemaleMale
102 (42.7%)137 (57.3%)
CaucasianAfrican AmericanAsianOther
225 (94.1%)6 (2.5%)5 (2.1%)3 (1.2%)
Height (inches) 68 (64-71)
Total body weight (kg) 82.1 (66-107.5)
Serum creatinine 0.93 (0.70-1.22)
* World Health Organization Definitions
PHARMACOKINETIC EQUATIONSKe = ln (Cmin/Cmax) /Δt Vd = (Dose/t') x (1 − e−kt')/ k (Cmax − [Cmin x e−keτ']) ClVANCO = Vd x ke
Cockcroft-Gault (mL/min): eCLcr= [(140-age) x (TBW/IBW/ABW/LBW)) x 0.85 (if female)] /(72 x SCr)
MDRD (mL/min/1.73 m2): eGFR =175 x (SCr)-1.154 x (Age)-0.203 x (0.742 if female) x (1.212 if black)
CKD-EPI (mL/min/1.73 m2): GFR = 141 X min(SCr/κ,1)α x max(SCr/κ,1)-1.209 x 0.993Age x 1.018 [if female] x 1.159 [if black]
(Where SCr =0.7 for females, 0.9 for males, α is –0.329 for females, –0.411 for males, min indicates the minimum of SCr/κ or 1, and max indicates the maximum of SCr/κ or 1.)
1. Pai MP, Nafziger AN, Bertino JS, Jr. Simplified Estimation of Aminoglycoside Pharmacokinetics in Underweight and Obese Adult Patients. Antimicrob Agents and Chemother 2011; 55:4006-4011 (3);785–790.