Embed Size (px)
Citation preview

Phone: 304-293-5801ext. 3207
Fax: 304-293-5994
[email protected]://www.as.wvu.edu/soca/
School of Applied Social Sciences Division Sociology and Anthropology
307 Knapp Hall PO Box 6326 Morgantown, WV 26506-6326
Eberly College of Arts and Sciences
October 27, 2008 Hon. Gary Johnson Chair, Court Improvement Program Oversight Board Nicholas County Courthouse 700 Main Street Summersville, WV 26651 Ms. Sue Hage Chair, MDT Study Committee WVDHHR, Bureau for Children and Familes 350 Capitol St. Rm 691 Charleston, WV 25301 Dear Judge Johnson and Ms. Hage: The Final Report on research activities for the 2007-2008 West Virginia Multidisciplinary Team Study is enclosed with this letter. This report presents findings from our observation of MDTs in 9 counties as well as from a survey of more than 430 MDT participants. Please feel free to contact me with any questions or concerns at the mail address, phone number, or email address provided below. I am available to discuss the contents of this report at any time. I thank the Court Improvement Program for the opportunity to conduct this research. Very truly yours, Corey J. Colyer, Ph.D.

!"#$%&%'(%)#%*+,-./0+1'.%*.20'$.3%,4%*%+.
Final Report 2007 – 2008 West Virginia Multidisciplinary Team Study
Prepared for the West Virginia Court Improvement Program
Corey J. Colyer, PhD – Principal Investigator L. Christopher Plein, PhD – Co investigator
School of Applied Social Sciences
West Virginia University Morgantown, WV 26506-6326
10/27/2008

TABLE!OF!CONTENTS!Executive Summary ............................................................................................................. 1!
Introduction ........................................................................................................................ 4!
Survey Research Methods ................................................................................................... 6!
Description!of!the!Sample!.........................................................................................................................!7!
Description!of!The!Survey!.......................................................................................................................!11!
Findings ............................................................................................................................. 15!
Variations!in!MDT!Preparation!and!Implementation!.............................................................................!17!
Training!Experiences!...........................................................................................................................!17!
Team!Management!&!Leadership!.......................................................................................................!18!
Perceptions!of!the!MDT!Process!across!the!Two!Cultures!.....................................................................!24!
Perceptions!of!Participation!&!Involvement!...........................................................................................!32!
Variance!in!MDT!Practices!......................................................................................................................!40!
Discussion, Conclusions & Recommendations ................................................................. 42!
Recommendations!..................................................................................................................................!43!
Recommendation!1:!Provide!More!Facilitation!Support!for!MDTs!....................................................!45!
Recommendation!2:!!Create!Multidisciplinary!Training!for!Multidisciplinary!Teams!........................!46!
Recommendation!3:!!Reassess!the!Objectives,!Goals,!and!Purposes!of!the!MDT!Process.!...............!46!
Recommendation!4:!Attend!to!the!Practical!Needs!of!All!Stakeholders!............................................!47!
Recommendation!5:!!Recognize!the!Developmental!Character!of!Treatment!Planning!....................!48!
Recommendation!6:!!A!Study!of!the!Parent!&!Child’s!Experience!is!Necessary!.................................!48!
References ......................................................................................................................... 50!
Appendices ........................................................................................................................ 51!
Appendix!A!–!Statistical!Models!..............................................................................................................!52!
Appendix!B:!Map!of!DHHR’s!Administrative!Regions!.............................................................................!53!
Appendix!C:!!Solicitation!Letter!...............................................................................................................!56!
Appendix!D:!Survey!Instruments!............................................................................................................!58!
Appendix!E:!Interim!Report!on!Phase!I!Activities!...................................................................................!92!

LIST!OF!TABLES! Table 1: The Participants Categorized by Role ................................................................... 8!Table 2: Proportion of Survey Responses DHHR’s Region .............................................. 10!Table 3: Questionnaire Items in the experience & perception batteries .......................... 13!Table 4: Ordinal Response Categories .............................................................................. 14!Table 5: Comparison of Battery Indexes by Sample ......................................................... 16!Table 6: MDT Training and Inservice ................................................................................ 17!Table 7: Location of MDTs ............................................................................................... 19!Table 8: Who Facilitates the MDT? .................................................................................. 20!Table 9: Percentage Distribution of Responses for Treatment Outcome Questions ....... 24!Table 10: Scheduling Frequency and Sufficiency ............................................................. 25!Table 11: Percentage Distribution of Responses on Sensitivity Measures ....................... 27!Table 12: Distribution of Responses Concerning Outcomes ............................................ 29!Table 13: Effectiveness on ASFA Policy Outcomes ........................................................... 31!Table 14: Distribution of Involvement in MDTs ............................................................... 33!

Multidisciplinary Teams in West Virginia Page | 1
EXECUTIVE!SUMMARY!
This is the final report of the 2007-2008 West Virginia Multidisciplinary Team
Study. This study was commissioned by the West Virginia Court Improvement Program
and undertaken by researchers in the School of Applied Social Sciences at West Virginia
University. The purpose of the study was to examine and document variation in
multidisciplinary team (MDT) processes and procedures implemented across the state.
The study focused on those MDTs that are charged with developing and implementing
service plans for children and families in abuse and/or neglect cases. The report first
identifies core questions that organized the inquiry, and then explains the
methodological approach used to conduct the study, documents the findings and
provides recommendations for future action.
This report draws on data gathered from 435 MDT participants who completed
an internet based survey. The internet survey asked respondents for their perceptions
concerning: 1) How do MDT practices vary across West Virginia?; and 2) How do MDT
participants experience the MDT process? The study also draws on field research based
on site visits at MDTs in process across West Virginia. This field research yielded
important contextual information that guided the development of a survey instrument
and which provides further understanding of the dynamics of MDT practices in West
Virginia. A fuller treatment of the field research can be found in a preliminary study
prepared for this project which delivered in May of 2008. A copy of this earlier report is
provided as an appendix and readers are encouraged to review it in context of this study.
While we found variation in MDT practices across different localities in the state,
our most significant finding involves differences in attitudes and perceptions expressed

Multidisciplinary Teams in West Virginia Page | 2
by DHHR professionals and the attorneys that are involved in the process. The data
and analysis provided in this report suggests that there are two professional cultures
that interplay in the MDT process. While at times complementary, these "two cultures"
of the DHHR and the legal profession can lead to differing perceptions, frustration, and
disagreement about the efficacy of the MDT process. The findings suggest that DHHR
staff view the processes, procedures, and effectiveness of the MDTs more favorably than
do attorneys. This two cultures problem deserves careful consideration by the Court
Improvement Program and West Virginia’s policymakers.
The findings of this report highlight the sometimes stark differences that exist
between DHHR professionals and attorneys involved in the process. The report also
finds that while daunting, the challenges involved are not insurmountable. We found
that in general, MDT participants view the process and procedures as effective tools in
the child welfare tool kit. But there is also the sentiment that the process can be
improved.
The report offers six recommendations for future action: 1) MDTs should
incorporate third-party facilitators to seek balance and to promote collaborative effort;
2) Training for MDT participants should be enhanced through more collaborative or
multidisciplinary instruction that involve stakeholders from the DHHR and the legal
community; 3) Policies governing the MDT process should be re-evaluated to ascertain
that clear objectives have been established and to identify any contradictions in
direction and purposes; 4) The Court Improvement Program should further encourage
each circuit to emphasize the importance of MDTs and where possible eliminate
practical impediments to participation; 5) The exploratory nature of service plan
development and the need for their adjustment in implementation should be well

Multidisciplinary Teams in West Virginia Page | 3
recognized by all MDT stakeholders in order to further emphasize that plan
development and management is often a case-specific and contingent process; and 6)
further research and evaluation should be focused on the role of parent and children in
the MDT process.

Multidisciplinary Teams in West Virginia Page | 4
INTRODUCTION!
According to state law (West Virginia Code §49-5D-3) multidisciplinary
treatment teams are designed to assess needs, then prepare and implement service
plans for children and families where abuse and/or neglect is suspected, or alternatively
where children are undergoing delinquency (and status offense) proceedings. The code
section mandates that this service plan be tailored to the family’s unique circumstances,
and the team is expected to particulate in court proceedings. This article of the code
differentiates between investigatory and treatment-oriented MDTs. The former is
tasked with assessing safety, while the later is responsible for formulating an
appropriate intervention or response.
The School of Applied Social Sciences at West Virginia University was contacted
by the West Virginia Court Improvement Program to undertake an evaluation of the
MDT process in West Virginia. The scope of this inquiry was restricted to treatment
MDTs in Chapter 49 Child Abuse and Neglect cases. Investigatory MDTs or MDTs
mobilized for youth services (e.g., delinquency or status offense) cases were not part of
the study. The research was conducted in coordination with a team of stakeholders
assembled by the West Virginia Court Improvement Program who provided valuable
insights, suggestions, and feedback in research design and implementation. The
purpose of this study was to review:
! How MDTs are constituted in terms of participants and levels of involvement.
! MDT performance and efficacy, as measured by assessments and evaluations
of stakeholders and participants.
! Unintended consequences of utilizing MDTs, especially in context of how
agencies and stakeholders interact in the child welfare system.

Multidisciplinary Teams in West Virginia Page | 5
Each of these themes frame essential questions in evaluating the MDT experience
in West Virginia. These can be grouped around such topics as: Who participates, in
what capacity, and how satisfied are the participants in the process? Do the MDTs
consistently operate within the parameters of their statutory guidelines? Do they arrive
at collaborative decisions which are then communicated to the presiding judge? How do
they handle dissent or disagreement? Do participants judge the process as productive?
How do MDT members negotiate the complicated relationships necessary for a team to
function properly?
Each of these themes was examined through various methodologies that are
grounded in program evaluation studies. These involved direct observation of MDTs in
practice; a survey of key MDT participants; and a review of the relevant literature and
available administrative data. The evaluation was carried out in two stages.
In the first, preliminary phase, we observed a cross section of MDT sessions
across the State of West Virginia. Several MDTs from each of the DHHR’s four
administrative regions were included in these observations. We sought to identify
patterns of consistency and variation in the MDT process across the State. Our
observations identified several ways in which MDT practices are consistent across the
State: (a) the group dynamics in MDTs evolve, (b) most MDTs do not generate
complete unanimity or consensus, and (c) it is difficult to maximize MDT member
participation. We also identified key ways in which MDT practices vary from one
jurisdiction to the other: (a) differences in the influence of agencies and institutions; (b)
differences in the roster of participants who typically attend MDT sessions; and (c)
differences in the organization, facilitation, and administration of MDT sessions. The

Multidisciplinary Teams in West Virginia Page | 6
detailed results from the Phase I analysis were reported to the Court Improvement
Program in an Interim Report submitted in May of 2008.1
In the second phase of the study, we solicited self-report feedback from MDT
participants through internet-based surveys. We asked the respondents to describe
their experience in, expectations for, and frustrations with MDTs. Four hundred and
thirty two participants responded to the survey over a two month period. Their
responses support the inferences we drew from our site visits and suggest several key
dimensions in which MDT participants differ. In the remainder of this report, we draw
on the evidence from both phases of the study to document variation in MDT practices
and procedures. However we wish to emphasize that the two reports are
complementary and should be considered together to constitute the full set of findings
from this study.
SURVEY!RESEARCH!METHODS!
Surveys offer a useful way to measure variation in perspective and impressions.
In the first phase of this research we observed variations in participation, facilitation,
and the participating institutional influences on MDTs. In the second phase of the
project, we wished to measure this variation with more precision and capture the
complete range of participant perceptions on participation, facilitation, and
effectiveness. To gather such data we designed questionnaires for key MDT
participants.
1 Colyer, Corey J. & L. Christopher Plein. “Building Trust: A Report on Phase I Activities in the 2007 – 2008 West Virginia Multidisciplinary Team Study.” Interim Report Prepared for the West Virginia Court Improvement Program. May 2, 2008. Attached as Appendix E.

Multidisciplinary Teams in West Virginia Page | 7
Two internet or “web” surveys were created over a three month period (from
November 2007 to February 2008). The original questions were drafted by the research
team and then modified through consultation with the Court Improvement Program’s
MDT study task force chaired by Sue Hage. Personnel from DHHR’s Bureau for
Children and Families were invited to complete one web-survey, while attorneys
practicing in Chapter 49 Abuse and Neglect cases were invited to complete the other. A
link to the DHHR personnel was distributed via an email from Jason Najmulski,
Commissioner of the Bureau for Children and Families. Mr. Najmulski encouraged
employees to fill out the survey during work hours and emphasized the importance of
this research project for the agency. A link to the Attorney survey was distributed in two
ways: (1) a letter written by Supreme Court Justice Robin Davis, requesting
participation from attorneys practicing in Chapter 49 Abuse and Neglect cases, was
distributed on the West Virginia Bar Association listserv; (2) An email invitation by Dr.
Colyer was sent to a select list of 379 attorneys whose name appeared on a mailing list
maintained by the Court Improvement Program.
Description!of!the!Sample!
In all, 432 respondents began the survey. Table 1 presents a description of the
responding sample. Since two separate surveys were distributed we have identified the
respondents according to the instrument that they completed. Those who completed
the survey distributed to DHHR employees are henceforth identified as the “DHHR
sample”, while those who completed the instrument distributed through the West
Virginia Bar Association list serve are labeled as the “attorney sample”. From the

Multidisciplinary Teams in West Virginia Page | 8
distribution of responses we can see that respondents from the DHHR outnumber
responding attorneys by a 3 to 1 ratio.
Table!1:!The!Participants!Categorized!by!Role!
% of Sample
%of Total N
DHHR Supervisor 14.8 40.4 45
DHHR Caseworker 54.9 38.7 167
DHHR Other 30.3 21.3 92
Subtotal of DHHR Respondents 100.0 70.4 304
Counsel to Adult Respondent 52.3 15.5 67
Guardian Ad Litem 34.4 10.2 44
Counsel to DHHR2 13.3 3.9 17
Sub Total of Attorney Responses 100.0 29.6 128
Grand Total 100.0 432
Note that within the DHHR sample, more than half the respondents identified
themselves as caseworkers.3 Descriptions offered by the nearly one-third of the sample
who checked “other” include adoption specialists, case aides, youth services caseworkers
and youth services supervisors.4 We understand that many attorneys who participate in
MDTs serve in different capacities. The questionnaire distributed to attorneys asked
2 Several survey respondents identified themselves as “counsel to the petitioner”. This category combines these respondents with those identifying themselves as prosecutors. 3 We categorically recoded respondents into this category if they marked “other” and described themselves as being an “Intake Worker”, “Ongoing Worker”, or “Investigative Worker”. While there certainly are important differences in the completion of these roles, formally these employees are all caseworkers. 4 Though the respondents were directed to only consider their experiences in Abuse and Neglect MDTs, our analysis of these data suggest that many “youth services” caseworkers based their responses on MDTs for delinquent or status offenders. Statistical comparisons between those identifying themselves as youth services workers against the rest of the DHHR sample were statistically significantly different. However, since we cannot definitively know that the youth services respondents were referring to abuse and neglect cases in their responses to the survey, we retain them in the analysis. (As a check against contamination, we conducted separate analyses excluding these cases. The results did not fundamentally differ from analyses when they are included. Therefore the analyses reported in this document include all the cases).

Multidisciplinary Teams in West Virginia Page | 9
them to identify all the capacities in which they’ve served on MDTs in the past year.
More than half indicated that they have served as counsel to the adult respondent and as
counsel to children. Therefore, we asked the respondents to identify the category they
serve in most often. Table 1 reports the distribution of that response. The most
common role is the counsel to adult respondents, followed by counsel to children and
lastly counsel to the petitioner, DHHR.
While we aspired to obtain as much information as possible, the survey was
designed to capture the perspective and sentiments of current MDT participants. We
defined a current participant as someone who was a member of an MDT at any point in
the twelve months prior to their completing this questionnaire. Approximately 15% of
those responding to the survey did not meet that criterion. We did ask these
respondents for some background information about themselves and provided them the
opportunity to provide feedback on the open-ended questions. They were not, however,
asked the specific questions about current MDT practices and procedures. This
effectively dropped the number of cases available for statistical analysis (i.e., the N)
from 432 to 361.5
We achieved participation from respondents located across the State of West
Virginia. While we would like to provide a county level overview of this participation,
relatively small numbers of respondents in some counties prevent us from doing so.
Table 2 locates the survey respondents within DHHR’s administrative regions.
Appendix B provides a map of the state locating counties within their regions. Roughly,
Region I encompasses the northwestern counties; Region II includes the southwestern 5 Missing data on specific questions further reduces the N reported for any particular analysis. If a respondent opted not to answer a particular question, his or her response is dropped from any quantitative analysis involving that measure. For this reason, the N in the tables that follow is rarely larger than 310.

Multidisciplinary Teams in West Virginia Page | 10
counties; Region III covers the northeastern area of the state (including the Eastern
panhandle and the Potomac Highlands), while Region IV covers the southeastern
counties of West Virginia.
Table!2:!Proportion!of!Survey!Responses!DHHR’s!Region!
DHHR Attorney
Region I 24.7 39.8
Region II 42.4 16.4
Region III 15.5 21.1
Region IV 17.4 22.7
N 304 128
!2 = 18.86, 3 df (Pr < 0.001)6
There are statistically significant differences in the samples. The DHHR sample
appears to disproportionately include respondents from Region II (the region
containing Charleston) while the Attorney sample appears to disproportionally include
respondents from Region I (the region including Morgantown, Fairmont, Clarksburg,
and Parkersburg). Our information is insufficient to statistically determine whether
these responses are significantly disproportionate to the population of practitioners.
That is, we do not know if the distribution of respondents is proportionate to the
distribution of practitioners in West Virginia. 6!2 (Chi-Square) is a simple statistical test that compares the observed distribution of cross-classified data against what we would expect to see if there was no association between the two variables. The test value
is a ratio produce by the formula: 5 6789:;<:=.>:??.@;:AB:CDEFGHI:DJ:=.>:??.@;:AB:CDEKLGHI:DJ:=.>:??.@;:AB:CDM:9 . This ratio ranges from 0 to
". The ratio can be fit against an expected distribution yielding a probability. The probability tells us how likely the two measures are to be independent. The higher the ratio, the lower the corresponding probability will be. A lower the probability of independence suggests that the difference between the measure is not random. In technical terms the association is said to be statistically significant.

Multidisciplinary Teams in West Virginia Page | 11
In a study of this nature, sampling is always a challenge. Ideally, a survey will
include participants drawn at random from a known population. Without
randomization, surveys can be compromised by response bias. Specifically, since the
entire population was invited to participate, those who opted to participate may be
fundamentally different than those who opted not to participate. The result is that in
surveys of this nature, highly motivated respondents may influence the patterns found
in the data. The analysis to follow should be interpreted with this caveat in mind.
Description!of!The!Survey!
The surveys were conducted through SurveyMonkey™, an internet or web-based
polling platform.7 Respondents were sent an email containing a hyperlink uniform
resource locator (e.g., url or “web link”) to the survey which was hosted on
SurveyMonkey’s servers. The respondents’ answers to the survey questions were stored
in a database on the server. Once the data collection was complete, we downloaded the
responses and analyzed them with statistical software.
The surveys were designed to capture data on two important concerns: (1) How
do the MDT practices identified in the earlier observational phase vary across West
Virginia; and (2) how do MDT participants experience the MDT process? Both surveys
were organized around common groups of questions that respond to the above
concerns:
(1) The respondent’s background, experience, and exposure to training on MDT
policy;
7 See http://www.surveymonkey.com

Multidisciplinary Teams in West Virginia Page | 12
(2) The respondent’s recollection of MDT logistics (location, scheduling,
frequency & duration, facilitation, etc);
(3) The respondent’s perception of the MDT’s adequacy in terms of:
(a) treatment planning
(b) meeting the needs of various constituents
(c) building consensus and achieving desired outcomes
(d) maximizing stakeholder participation and contribution.
Additionally, the surveys asked respondents to offer thoughtful answers to four open-
ended questions:
(1) What should MDTs accomplish?
(2) How can the MDT process be improved?
(3) Who is not currently involved in MDTs that should be?
(4) What things haven’t we asked about that are important for understanding
MDT?
As we documented in the Interim Report, our observations from site visits
suggested that the core members of the MDT perceive the process differently. The
survey was organized to test the validity of those observations and quantify the extent to
which various MDT members perceive the process differently. We organized these
perception questions into batteries or groups of common items. Each battery includes
questions that address different dimensions of similar issues or topics. This strategy
allows us to compare a range of responses on a particular topic across respondent types
(e.g., attorneys, DHHR personnel, etc). The specific survey items measuring those
perceptions are provided in Table 3 below.
!

Multidisciplinary Teams in West Virginia Page | 13
Table!3:!Questionnaire!Items!in!the!experience!&!perception!batteries!
1 Treatment Outcome Objectives: The following questions are concerned with how well multidisciplinary treatment teams implement treatment objectives.
a Develop individualized service plans for the children and families
b Base Treatment Planning on Comprehensive Assessments of Children and Families
c Coordinate treatment plans for the child with resources available in the community
d Coordinate treatment plans for the family with resources available in the community
2 Scheduling Frequency and Sufficiency. The next group of questions are concerned with the frequency, duration, and location of MDT meetings in abuse and neglect cases.
a MDT sessions occur frequently enough to aide in designing, implementing, and monitoring treatment plans
b MDT sessions last long enough to adequately address the needs of the case c MDT sessions are scheduled at times that are convenient for me to attend
d MDT sessions are scheduled in places that are convenient for me to attend.
3 Sensitivity of MDT procedures to various parties. The next group of questions are concerned with the extent to which MDTs are sensitive to the needs and/or concerns of their constituent members.
The MDT process is sensitive to the needs and/or concerns of [children, parents, co-petitioners or interveners, caseworkers, GALs, counsel to the adult respondent, and prosecutor]
4 Perception of Consensus and teamwork. The questions that follow concern the extent to which MDTs yield agreement and consensus.
a The members of the MDT are able to come to a consensus concerning the treatment plan for particular cases
b The multidisciplinary team is able to formulate recommendations to the court that reflect member consensus
c The multidisciplinary team generates an official report communicating recommendations to the court.
d Recommendations that come from the multidisciplinary team reflect the full range of members’ opinions concerning the case.
5 Perception of MDT effectiveness on policy objectives. The next group of questions are concerned with the extent to which multidisciplinary team proceedings achieve the ideal goals as set by state policy.
a MDT practices contribute to the overall goal of making reasonable efforts to preserve or reunify the family.
b MDT practices contribute to the overall goal of maximizing the safety of children. c MDT practices contribute to the overall goal of achieving permanency for children in a timely
manner. 6 Identification of MDT participants. The next group of questions are concerned with the
constitution or makeup of multidisciplinary treatment teams. For each question, please tell us how frequently each of the following participants attended MDT meetings
A list of 14 potential participants were offered. (See survey instrument in Appendix C for the full list.
7 Ranking of participant involvement. Other studies of MDTs have shown that member participation, engagement, or involvement, varies from extremely passive to extremely active. Thinking about your experiences in the MDTs over the past year (since February 2007), please rate the typical involvement of the following people. If a person listed does not routinely participate in MDT meetings in your county, please check “never or almost never present.”
A list of 14 potential participants were offered. (See survey instrument in Appendix C for the full list.

Multidisciplinary Teams in West Virginia Page | 14
For all of these questions, respondents were offered four potential responses. One
set of response options were offered in the first six batteries, while a slightly different
response set was offered in the seventh battery. These are ordinal responses. That
means that they imply a rank ordering but do not imply precise measurement. We
assigned numeric values or weights (from 0 to 3) to each response item for the purpose
of statistical analysis (see Table 4).
Table!4:!Ordinal!Response!Categories!
Value Response Category (Batteries 1 to 6) Response Category (Battery 7)
0 Never or almost never Never or almost never present
1 Occasionally Extremely Passive
2 Much of the time Balanced between Passive and Active
3 Always or almost always Extremely Active
For each battery of responses, we created cumulative index scales which
additively combine the numeric values for all of the questions in the category. The
scores on for these scales provide a summary measure of each respondent’s assessment
of the MDT. High index scale scores suggest that the MDT mostly performs as intended
by the policies, while low index scores suggest that the MDT does not perform as
intended.
!

Multidisciplinary Teams in West Virginia Page | 15
FINDINGS!
The MDT, as implemented under West Virginia’s statute, appears to be rooted in
two distinct cultures. The English physicist and novelette C.P. Snow (1905 – 1980)
coined the term “two-cultures” to explained emergent conflict in the interactions
between government and science (Snow 1959, 1960). This concept has been applied in
other contexts where distinct organizational or professional cultures interface. The
survey data published in this report are highly suggestive that two cultures exist
between the DHHR personnel and the attorneys who participate in the MDT process.
Respondents from the DHHR view the processes, procedures, and efficacy of
MDTs more favorably than the attorneys do. This does lead to conflict, disagreements,
and inefficiencies in the MDT process. Our analysis of the data demonstrates that there
are statistically significant differences between the respondents from the two samples.
This two cultures problem deserves careful consideration by the Court Improvement
Program and state policy makers. Table 5 compares the mean (0r average values) of all
seven cumulative indexes between the two samples. We used student’s t-test to
determine if differences between the samples are statistically significant.8
! !
8 A statistically significant difference in the comparison between the samples is a difference that is larger than what we would expect to be produced by chance alone. A t-test produces a ratio based on the
following formula: NOPPQRQSTQ.UQVWQQS.XRYZ[.\Q]S^
^V]SN]RNO_QN.`]RO]UOaOVb.WOVcOS.VcQ.XRYZ[^. Like the Chi-Square ratio, each t-value or ratio
may be located within a probability distribution. In the social sciences we consider a probably associated with t-values that are less than or equal to .05 (i.e., <.05) to be statistically significant. .

Multidisciplinary Teams in West Virginia Page | 16
!Table!5:!Comparison!of!Battery!Indexes!by!Sample!
Battery Scale Range DHHR Mean ATTY Mean T Prob
Treatment Outcomes 0-12 8.64 8.71 -0.21 < 0.83
Scheduling Frequency and Sufficiency 0-12 9.28 8.77 1.79 < 0.07
Sensitivity of MDT procedures to various parties
0-24 15.41 13.67 3.66 < 0.001
Do MDT proceedings yield effective outcomes? 0-12 8.85 8.05 2.81 < 0.01
Do MDT proceedings achieve the expectations set forth in policy?
0-12 7.64 6.16 6.35 < 0.001
Who participates? 0-24 21.41 20.19 1.79 < 0.07
How involved are the participants? 0-24 21.83 19.53 2.67 < 0.01
Four of the batteries produced statistically significant different means between
the samples (indicated by bold type in the probability column). On average,
respondents from the DHHR perceived the MDT to be more sensitive to the needs of
various parties; to yield effective outcomes and achieve the expectations set forth in
policy more frequently; and to be more inclusive in the involvement of all parties, as
compared to the attorneys who responded to the survey. There were also marginal
differences between the samples on the measures of scheduling frequency and
sufficiency as well as recollection of participants, but those differences were not
statistically significant.

Multidisciplinary Teams in West Virginia Page | 17
The measurement of these differences combined with our observations of MDT
sessions across the state, suggest that MDTs are often complicated by differing
perspectives, principles, visions, and norms between the DHHR and the Attorneys. The
remainder of this analysis will explore the dynamics between the DHHR and Attorney
samples. In addition we examine patterns of variation in MDT practices across the
state. However, those differences pale in comparison to differences between the
samples.
Variations!in!MDT!Preparation!and!Implementation!
This section of the report provides an analysis of the survey questions concerning
how the MDT statue (e.g., West Virginia Code §49-5D-1, et seq.) has been implemented
in practice and policy. Specifically, we asked the respondents to answer questions about
their training experiences, where MDTs are located, and how the MDTs are facilitated.
Training!Experiences!
Responses to the survey indicate that there are clear differences between the
samples in terms of exposure to training.
Table!6:!MDT!Training!and!Inservice!
DHHR Attorney
Ever exposed to training or in service 90.5 69.3
Trained in past year? 26.2 37.9
Identified training as effective 66.5 47.1
N 210 87

Multidisciplinary Teams in West Virginia Page | 18
A far greater percentage of DHHR-based participants have been to a training or
in-service on MDT policies and procedures. Nearly 91% of the DHHR respondents
indicate that they have been exposed to training or in-service in their careers, while less
than 70% of the attorneys who participate in MDTs recall attending training. However,
attorneys are more likely to report having been to training in the past year; 38% of
attorneys report attending a training or in-service in the past year compared to a quarter
of the DHHR respondents indicate being to a recent training. Lastly, the respondents
from DHHR were more likely than attorneys to report their training experience as
effective (67% vs 47%).
Team!Management!&!Leadership!
MDT processes and procedure also vary on the basis of which organization hosts
and facilitates the meeting. There are two dominant organizations in West Virginia
Multidisciplinary Teams: the DHHR and the Circuit Court.9 By dominant, we mean that
these organizations set the agenda for the team meeting and influence the deliberations.
The primacy of these organizations is evident in the locations where MDTs take place.
Table 7 tallies the “most common location of MDTs” as reported by survey respondents.
9 For more about institutional dominance in West Virginia MDTs see the Interim Report, “Building Trust: A report on Phase I Activities in the 2007 – 2008 West Virginia Multidisciplinary Team Study” provided as Appendix E.

Multidisciplinary Teams in West Virginia Page | 19
!
Table!7:!!Location!of!MDTs!
DHHR AttyTotal
Sample
DHHR Office 63.6 63.1 63.4
Court House 28.2 30.1 29.1
Child Advocacy Center 3.4 4.5 3.8
Law Firm Offices 2.4 1.8 2.2
Municipal Building 2.4 0.0 1.6
N 209 111 320
!2= 3.18, 4 df (Pr = 0.53)
There were no measurable differences between the two samples. The table
clearly illustrates that nearly all the respondents reported that they usually attend MDTs
at their county’s DHHR office (63%), or at a facility associated with the courthouse
(29%). These data are consistent with our observations across the state. In all but three
of our site visits, the MDTs were hosted in the DHHR offices. Locations of the other site
visits were (a) a child advocacy center, and (b) county municipal buildings. The physical
location of a meeting conveys a sense of ownership and influences who attends the
meetings.
For instance, we noted in our site visits that prosecutor participation was much
greater at the neutral (or non DHHR) sites as compared to the DHHR offices. In
contrast, at the three sites conducting meetings in municipal buildings or the child
advocacy center, a prosecutor was present and involved. Our observations were
reinforced by the survey data. The respondents who report that they attend MDTs

Multidisciplinary Teams in West Virginia Page | 20
mostly at the courthouse were more than five times more likely than those attending
MDTs at the DHHR office to indicate that a prosecutor regularly participates in the
MDT.10
In addition to their hosting, MDTs vary according to which participant leads or
facilitates the meeting. Table 8 presents the distribution of survey responses to the
question, “in your experience, who is responsible for leading and directing MDT
meetings?”
Table!8:!Who!Facilitates!the!MDT?!
DHHR Atty Total Sample
DHHR Caseworker 83.3 72.3 79.5
Prosecuting Attorney 8.1 8.0 8.1
Not Sure 2.9 10.7 5.6
MDT Coordinator or 3rd Party Facilitator 4.3 1.8 3.4
DHHR Supervisor 1.4 4.5 2.5
Guardian ad Litem 0.0 2.7 0.9
N 210 112 322
!2 = 18.86, 5 df (Pr < 0.01)
First, this table shows rather striking differences (which are statistically
significant) between the DHHR and Attorney samples. In both samples, the majority
indicate that MDTs are facilitated by the by the family’s caseworker. More than 83% of
10 This odds-ratio was estimated through a logistic regression procedure which predicts the odds that a discrete event will occur. The model also estimated greater odds of prosecutor participation in municipal building and Child Advocacy Center MDTs, however those estimates were not statistically significant (meaning, there was sufficient variation in the data to undermine our confidence in the estimated parameter). Nonetheless these estimates strongly suggest an association between “turf” and participation. Full participation patterns are broken down by percentage later in this report. Results from the regression model are provided in Appendix C.

Multidisciplinary Teams in West Virginia Page | 21
the case workers and 72% of the attorneys reported that the caseworker usually
facilitates the MDT. The next largest proportion of respondents (8%) identified the
prosecuting attorney as the MDT leader, which was followed by 6% of respondents who
were unsure. However, almost 11% of the attorneys, a far greater proportion than the
DHHR respondents, indicated that they did not know who typically facilitates their
MDTs. This is an important finding.
It is likely that different respondents interpret the meaning of facilitation in a
variety of ways. We observed several MDT sessions where the caseworker clearly called
the meeting to order, but once under way did not maintain control of the agenda. We
noted that the caseworker’s role requires her to simultaneously start the discussion,
participate in dialogue, and record details of the conversation. Some of the caseworkers
told us that they have trouble fulfilling all these duties in the MDT. Those sentiments
were reiterated by the survey respondents from both samples. These respondents
expressed concern that the existing policy may ask too much of the caseworker.
Consider, for example, the following comments offered in the survey responses.
Having a coordinator there to keep notes and monitor the schedule is extremely helpful. It allows the worker to concentrate on other things during the meeting. [DHHR – Social Services Worker]
We need SOMEONE to take notes so we can focus on the issues at hand instead of writing the entire time. Key issues are often left out of the notes for this reason. [DHHR - CPS Caseworker]
Other participants expressed concern that without a neutral party to facilitate the
meeting, the MDT can become unnecessarily adversarial or partisan. They remind us
that meetings must be guided and it can be difficult for the case manager to guide a

Multidisciplinary Teams in West Virginia Page | 22
meeting in which he or she is already substantively involved as a participant. The next
two comments articulate the need to ensure that MDTs are led by truly neutral parties.
The Department should hire MDT Facilitators. A non-biased person that has no relationship to the family to facilitate all MDTs. This person would also be responsible for scheduling all MDTs that are mandated by law. Hopefully, this person would have enough pull to get all the necessary parties around the table. [DHHR - Social Service Coordinator]
We must have a neutral third-party conduct every MDT. In my county, respondents are often intimidated by the DHHR worker who they do not perceive to be neutral. Also, it is not appropriate for the prosecuting attorney to facilitate and control the MDT. [Attorney]
These comments highlight a key observation that must be broached in any critical
examination of the MDT process. The MDTs are not necessarily neutral. The
participants are drawn from sponsoring organizations with particular interests and
agendas. While “the best interest of the child” may be the organizing principle of child
welfare, reasonable people disagree as to which course of action most appropriately
achieves that “best interest.” In the second quote above, an attorney who represents
adult respondents indicates that her clients often experience the DHHR caseworker as
intimidating. Another attorney compared the MDTs in his county to the Spanish
Inquisition.
MDTs are supposed to provide a free exchange of information and brain-busting to come up with solutions to the problems facing the family. In our area they often are more like an inquisitor trial from the Middle Ages, with the DHHR and the GAL acting as the main interrogators of parents whose attorneys fail to show up or show up late.
Still, another attorney echoed this sentiment in a slightly different way:
No matter what respondents or their counsel argue or present, the DHHR/State position is what ends up in the case plan. If the respondents are doing well, it is at best a 15-minute “keep up the good work”. However, most of the time, we all

Multidisciplinary Teams in West Virginia Page | 23
get to sit and listen to the DHHR worker(s) recite a litany of all the things the respondents have messed up on during the last month and how if they don't get their acts together they're going to file a motion to revoke and never see their kids again. I'm still waiting to attend one where the focus was more visitation, more frequent visitation and how soon they can get the kids back in the home.
These comments point to difficulties in meeting facilitation or leadership.
Insofar as the MDT is supposed to generate a multidisciplinary assessment of the
treatment plan and progress, it often fails to achieve this. The attorneys quoted above
object to a perceived lack of neutrality in the MDT proceedings and suggest that (at least
in some locations) not all participants are equal members. These attorneys view the
MDT as a frustrating institutionalized attack on their clients.11 The opposite side of that
concern is articulated by DHHR respondents who indicate that the attorneys often use
the MDT as a place to argue philosophical points, rather than to discuss specific plans
that will help the family resolve underlying problems. For instance, in response to the
question: “What would improve MDTs?” one CPS supervisor wrote: “Don’t let the
parent’s counsel use the MDT setting to argue their case. We’re supposed to identify
issues and develop reasonable case plans to alleviate those issues.” Many others echoed
the complaint that MDTs too often become unnecessarily adversarial.
It is interesting to note that the majority of the complaints that surfaced in this
survey are rooted in the two cultures dynamic. Insofar as they had complaints, the
caseworkers, CPS supervisors, and other respondents from the Bureau for Children and
Families complained about attorney advocacy. In contrast, the attorneys retained by
parents or assigned to be the respondent’s counsel complained that there are
insufficient due process considerations hardwired into the process. As we will detail in
11 It would be useful to empirically measure how parents (or respondents) experience the MDT as an attack. Such an inquiry was beyond the scope this study.

Multidisciplinary Teams in West Virginia Page | 24
the discussion section of this report, these are longstanding issues in child welfare
across the United States which will not be remedied in the short term. The centrality of
these two cultures dynamics became visible as we observed MDT sessions in different
jurisdictions.
Perceptions!of!the!MDT!Process!across!the!Two!Cultures!
Fundamental differences between the cultures became more clearly visible when
we analyzed the individual survey items that constituted the battery indexes reported in
Table 5 in the previous section.
The first response battery concerned the effectiveness of MDTs for achieving
certain treatment outcomes. Table 9 presents the distribution of responses (in
percentage form) for each of the 4 items included in the battery.
Table!9:!Percentage!Distribution!of!Responses!for!Treatment!Outcome!Questions!
IndividualTx Plans
Base plan on Comp
Assessment
Coordinate Child’s plan
with available resources
Coordinate Family’s
plan with available resources
DHHR Atty DHHR Atty DHHR Atty DHHR Atty
Never or almost never 2.4 3.7 2.9 2.8 3.8 4.6 4.3 4.6
Occasionally 14.5 6.4 16.8 26.1 15.3 10.1 9.6 12.8
Much of the time 48.8 44.0 48.6 41.3 41.2 44.0 43.8 41.3
Always or Almost Always 34.3 45.9 31.7 29.4 39.7 41.3 42.3 41.3
N 207 109 208 109 209 109 208 109
Chi2 !2= 7.21, 3dfP < 0.07*
!2= 4.34, 3dfP < 0.23
!2= 1.73, 3df P < 0.63
!2= 4.34, 3dfP < 0.23

Multidisciplinary Teams in West Virginia Page | 25
Generally speaking, most respondents view the MDT’s accomplishments in terms
of treatment objectives favorably. That is, the majority of respondents report that in the
MDTs they attend, treatment planning is individualized, based on comprehensive
assessments, and is coordinated with available resources. These perceptions did not
generally differ across the samples. However, there was a statistically significant
difference (p < .07)12 between the samples on the question of individualized treatment
plans. The DHHR respondents indicated that individualized treatment plans occur less
frequently than was recalled by attorneys. This is consistent with the different foci these
respondents bring to the MDT.
The next battery of responses was concerned with the extent to which the
scheduling of MDTs is sufficient in terms of frequency, duration and in convenient times
or places.
Table!10:!Scheduling!Frequency!and!Sufficiency!
Sufficient Frequency
Sufficient Duration
Convenient Times
Convenient Locations
DHHR Atty DHHR Atty DHHR Atty DHHR Atty
Never or almost never 2.5 2.8 1.0 1.9 1.0 7.4 2.0 4.7
Occasionally 16.7 21.5 7.3 8.3 14.2 20.4 7.3 4.7
Much of the time 46.6 47.7 44.9 39.8 39.0 44.4 30.4 32.7
Always or Almost Always 34.3 28.0 46.8 50.0 45.9 27.8 60.3 57.9
N 204 107 205 109 205 108 204 107
Chi2 !2= 1.80, 3dfP < 0.61
!2= 1.09, 3dfP < 0.78
!2= 17.2, 3df P < 0.001***
!2= 2.76, 3dfP < 0.43
12 Due to the contribution of measurement error to overall variance, we will use a more relaxed threshold for statistical significance in these analyses. Any Chi-Squared test corresponding to a probability less than .10 will be considered statistically significant for discussion purposes.

Multidisciplinary Teams in West Virginia Page | 26
Note that there is more variation in the responses to questions in this battery
than in the previous one. The majority of respondents from both samples indicated that
MDTs are scheduled with sufficient frequency and duration; at convenient times and
places. However, there was a strong statistically significant difference between the
DHHR respondents and attorneys on the question of convenient times. A far greater
proportion of attorneys reported that MDTs are never or only occasionally scheduled at
times that are convenient to them. Almost half the DHHR respondents (46%) reported
that the MDTs are always scheduled at convenient times. This compares to just slightly
more than one quarter of the attorneys sharing that sentiment.
The third battery of responses asked respondents to evaluate the extent to which
the MDT process is sensitive to the needs or situations of various participants. The
responses to these questions, presented below in Table 11 highlight some important
crucially important variations.
!

Multidisciplinary Teams in West Virginia Page | 27
Table!11:!Percentage!Distribution!of!Responses!on!Sensitivity!Measures!
Child Adult
Respondent
Co-Petitioner/ Intervener
DHHR
DHHR Atty DHHR Atty DHHR Atty DHHR Atty
Never or almost never 1.0 1.0 0.5 8.5 3.9 12.3 3.4 0.9
Occasionally 5.3 9.4 8.3 29.3 18.8 34.0 21.6 10.3
Much of the time 35.3 37.4 53.4 48.1 51.2 46.2 48.1 43.9
Always or Almost Always 58.5 52.3 37.9 14.2 26.1 7.5 26.9 44.9
N 207 107 206 106 207 106 208 107
Chi2 !2= 2.27, 3dfP < 0.52
!2= 47.6, 3dfP < 0.001***
!2= 26.6, 3df P < 0.001***
!2= 13.9, 3dfP < 0.01**
Table 11 Cont. GAL Respondent’s
Counsel Prosecutor
DHHR Atty DHHR Atty DHHR Atty
Never or almost never 0.5 4.7 1.0 7.6 5.3 14.3
Occasionally 12.0 9.4 13.2 32.1 13.1 13.3
Much of the time 43.3 40.2 46.8 44.3 47.1 41.9
Always or Almost Always 44.2 45.8 39.0 16.0 34.5 30.5
N 208 107 205 106 206 105
Chi2 !2= 7.17, 3dfP < 0.07*
!2= 34.0, 3dfP < 0.001***
!2= 7.41, 3df P < 0.06*

Multidisciplinary Teams in West Virginia Page | 28
The two samples only agree in the question of sensitivity of MDT procedures to
the child. There are statistically significant differences between the samples on all of the
remaining measures. The respondents from DHHR generally view the MDT procedures
as being more sensitive to the needs of various participants than the attorneys.
However, DHHR respondents consider the sensitivity of MDT processes and procedures
to be less sensitive to the caseworker’s needs, than attorneys.
Perhaps the most important column in Table 11 bears the heading, Adult
Respondent. Almost 40% of the attorneys reported that the MDT procedures are never
or only occasionally sensitive to the Adult Respondent. In contrast, less than 10% of the
respondents from DHHR shared that sentiment. Indeed, almost 40% of DHHR’s
respondents reported that the MDT is always or almost always sensitive to the needs of
the adult respondent, compared to only 16% of attorneys sharing that sentiment.
The disconnect between perceptions is very important. On the one hand, we may
use the attorney’s perceptions as a proxy for the perception of parents (and other adult
respondents) themselves. These data suggest that the adult respondent does not always
experience the treatment MDT as a gathering that is sensitive to her needs; this is
something that her attorney recognizes but her caseworker may not. Similarly, these
data suggest that the caseworker, case aide, and other participants from DHHR
approach the MDT from a different perspective than the Attorneys. These differences
clearly point to “two-culture” dynamic at play in the MDTs. This dynamic is further
amplified by the measurements on MDT consensus reported below.
!

Multidisciplinary Teams in West Virginia Page | 29
Table!12:!Distribution!of!Responses!Concerning!Outcomes!
Consensus Recommend Formal Report
Reflects Full Range
DHHR Atty DHHR Atty DHHR Atty DHHR Atty
Never or almost never 0.0 1.9 1.0 2.8 6.7 11.4 1.0 13.2
Occasionally 11.1 9.4 7.7 12.3 10.1 13.3 12.1 23.6
Much of the time 65.2 67.9 57.2 58.5 33.2 27.6 43.0 36.8
Always or Almost Always 23.7 20.8 34.1 26.4 48.1 47.6 43.9 26.4
N 207 106 208 106 208 105 207 106
Chi2 !2= 4.43, 3dfP < 0.29
!2= 4.48, 3dfP < 0.21
!2= 1.90, 3df P < 0.59
!2= 32.6, 3dfP < 0.001
State law indicates that the MDT should derive consensus, and make official
recommendations to the court that reflect the full range of member opinion (see West
Virginia Code §49-5D-3). The responses to the survey questions in this battery suggest
that the members of the MDT perceive these outcomes unevenly. The majority of the
respondents in both samples reported that they do ordinarily achieve consensus much
of the time or always. Yet there is a noticeable minority in either sample that reports
consensus is only achieved occasionally. Similarly there are no statistically significant
differences between the samples on the measures of making recommendations to the
court or preparing a formal report. Approximately 85% of respondents report that their
MDTs offer recommendations to the Judge and submit a formal report much of the
time, or almost always.
Yet, the final column in Table 12 suggests substantial differences between the
samples on the measure: “Recommendations that come from the multidisciplinary
team reflect the full range of members’ opinions concerning the case.” Fully one third of

Multidisciplinary Teams in West Virginia Page | 30
the responding attorneys indicated that this occurs never or only occasional compared
to less than 15% of the respondents from DHHR with a similar view. In fact, 44% of
DHHR’s respondents suggest that the MDT reports or recommendations always reflect
the full range of opinion which is a sentiment only a quarter of the attorneys agreed
with. These data provide further evidence for our two culture argument. In general, the
respondents from DHHR experience their MDTs as a collaborative exercise. In
contrast, many of the attorneys (particularly those who serve as the counsel for the adult
respondent) complain that there is little capacity for minority viewpoints. Consider the
following complaint from an attorney who serves as counsel to adult respondents.
I like the process overall, but it still remains somewhat of a sham, as the DHHR runs the show and almost always gets what it wants. In our area, my advice to clients is to do everything the DHHR tells you to do, or else you may lose your kids. The DHHR personnel are typically not open to compromise, and refuse to believe they may have wrongly assessed a case. Therefore, MDTs mostly consist of everyone finding out what DHHR expects of them, and whether or not they are meeting those goals. I think it is a very rare occasion that an MDT fundamentally changes the viewpoint of the DHHR with respect to a case. On the other hand, it is still good to have these meeting to at least offer input, and to avoid adult respondents failing to meet goals.
The language used belies this attorney’s frustration with the MDT process. How
can this attorney communicate these concerns to the Judge? Clearly, her perception of
the MDT process is at odds with the collaborative ideal emphasized in policy. While
many MDTs undoubtedly accomplish consensus and make recommendations that
reflect the full range of team member input, comments like the one above remind us
that there are clear markers of conflict, disagreement, and misapplication of the MDT
process. The data repeatedly suggest this trend.

Multidisciplinary Teams in West Virginia Page | 31
The next battery of questions pertains to perceptions of how effective MDTs are
in achieving policy goals set under the Adoption and Safe Families Act. Specifically,
these questions are concerned with the extent to which MDTs foster reasonable efforts
to reunify or preserve families; minimize risks and maximize children’s safety, and
facilitate permanency planning for the child.
Table!13:!Effectiveness!on!ASFA!Policy!Outcomes!
Reasonable Efforts to
Preserve or Reunify Families
Maximizing the Safety of Children
Achieving Permanency
DHHR Atty DHHR Atty DHHR Atty
Never or almost never 0.5 6.6 1.0 2.8 0.0 8.7
Occasionally 4.4 23.6 5.8 12.3 9.1 21.2
Much of the time 31.4 36.8 25.5 34.9 35.6 44.2
Always or Almost Always 63.8 33.0 67.8 50.0 55.3 25.9
N 207 106 208 106 208 106
Chi2 !2= 47.19, 3df P < 0.001***
!2= 11.03, 3df P < 0.01**
!2= 40.07, 3df P < 0.001***
There are statistically significant differences between the samples on all three
questions. First, whereas almost 95% of the respondents from DHHR indicated that
MDTs contribute to reasonable efforts to preserve or unify families, less than 70% of the
responding attorneys responded in kind. Indeed, more than a quarter of the attorneys
indicated that MDTs never, or only occasionally contribute to reasonable efforts.
Similarly, respondents from DHHR were more likely to report that MDTs assist in
keeping children safe. Perhaps the most striking finding in Table 13 is in the right-most
column. Fully one third of the responding attorneys report that MDTs never, or only

Multidisciplinary Teams in West Virginia Page | 32
occasionally, contribute to permanency efforts. In all three measures, attorneys were
more pessimistic about the accomplishments of MDTs than respondents from the
DHHR.
Perceptions!of!Participation!&!Involvement!
In our survey data, we found important differences of opinion regarding
perceptions of MDT practices. These differences fell between the perceptions of DHHR
staff and attorneys involved in MDTs. Through the surveys, we sought assessments of
the presence and involvement of the 13 potential participants named in state code who
are expected to play a role in MDTs. These assessments are limited of course, to the two
main groups represented in the process and making up our survey sample – DHHR
personnel and attorneys involved in the MDT process. We asked these respondents the
following questions and asked them to provide the following assessments:
! Survey respondents were asked to recall “How frequently each of the following
attended MDT meetings” over the past year. The response options were: 1) Never
or almost never, 2) Occasionally, 3) Much of the Time, or 4) Always or almost
Always.
! Survey respondents were asked, “Thinking your experiences in MDTs over the
past year (since February 2007), please rate the typical involvement of the
following people. If the person listed does not routinely participate in MDT
meetings in your county, please check ‘Never or almost never present.’ Response
categories for those present were: 1) Extremely Passive, 2) Balanced between
Passive and Active, and 3) Extremely Active.

Multidisciplinary Teams in West Virginia Page | 33
Table!14:!Distribution!of!Involvement!in!MDTs!
% Present “Much of the time”, or “Almost Always”
% Described as “Extremely
Active” when present
DHHR Atty DHHR Atty
DHHR Caseworkers 99.5 100.0 87.3 79.6
DHHR Supervisors 23.4 18.23 24.1 34.2
Prosecutor (or self-described counsel to the Petitioner)
51.7 54.4 49.7 42.1
Counsel to Parent 82.1 96.2 51.3 46.6
Guardian Ad Litem 90.4 98.1 68.2 73.3
The Child or Children 20.1 3.9 12.3 4.2
Parents 89.4 96.2 27.9 22.3
Foster Care Provider 38.1 27.6 9.8 6.9
Court Appointed Special Advocates
39.1 28.4 34.9 20.8
Child Advocacy Center Personnel
15.3 13.5 14.3 14.3
Approved Service Organization Personnel
60.1 56.2 17.8 12.6
Behavioral Health Specialist (e.g., Counselor)
38.7 27.6 17.1 17.9
Representative from Schools
16.4 3.9 8.9 7.9
Other Party (most often described as Co-Interveners)
21.0 15.9 14.1 5.71
N 208 105

Multidisciplinary Teams in West Virginia Page | 34
Our findings reinforce the “two cultures” perspective described earlier in this
analysis, but also reveals some consistency and agreement among the parties involved in
the MDT process. For example, as Table 14 illustrates, there was wide agreement that
DHHR Caseworkers play a prominent role in the proceedings. Almost all of the
respondents noted that they are present “much of the time” or “almost always” and that
their involvement is “extremely” active. Both DHHR personnel and attorneys largely
agree that prosecutors or those who serve as counsel to the petitioner (i.e. the state) are
not as frequently involved or active in the proceedings. As Table 15 shows, these
individuals are seen as present “much of the time” or “always” little more than half of
the time when MDTs are convened. Additionally, they are rated as being “extremely
active” by less than 50 percent of the DHHR respondents and only by 42 percent of the
attorneys surveyed.
As the table illustrates, there is general consensus that Guardian Ad Litems are
both present and active in the proceedings. Interestingly, other key parties, such as
Counsel to Parents and Parents themselves are generally perceived as being present
“much of the time”or “almost always” by both groups of respondents. However, their
efficacy in the process – as measured by opinions of whether these parties are
“extremely active” in the process is different. Counsel to Parents are seen as being
“extremely active” in the proceedings by little more than half of the DHHR survey
respondents and by only 47 percent of the survey respondents from the legal profession.
Most significantly, parents are rarely perceived as being “extremely active” in the
process – only 28 percent of the DHHR respondents and 22 percent of the responding
attorneys rated them as such.

Multidisciplinary Teams in West Virginia Page | 35
The analysis suggests that there are five core groups of participants in the MDT
process – DHHR caseworkers, prosecutors or counsel to the petitioner, guardian ad
litem, counsel to parent, and the parent. Of these, prosecutors or counsel to the
petitioner do not appear to be present to the same degree as the other four stakeholder
groups. And among the core institutional players (DHHR, guardian ad litem, and
counsel to parent) their active engagement lags behind their counterparts. This lack of
participation is notable and requires additional discussion.
By cross-classifying measures of presence and involvement, we can develop
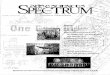
different conceptual models of MDT arrangements. Figure 1 arrays MDT participants
along these two dimensions. Recall that West Virginia Code §49-5D-3 indicates that
MDT participants should include: the child (when deemed appropriate), a guardian ad
litem, the adult respondent(s) along with legal representation, a designee from the
prosecutor’s office, and other available parties deemed appropriate by circumstance
(foster parents, CASA volunteers, any other person or an agency representative who may
assist in providing recommendations for the particular needs of the child and family).
However, our field observations along with the survey responses discussed above,
suggest that their constitution and makeup varies widely. Among the MDTs we
observed, some involved only the adult respondent and DHHR personnel, while others
involved so many people that it was difficult for us to construct a list of participants.

Multidisciplinary Teams in West Virginia Page | 36
Figure!1!"!Presence"Involvement!Matrix!
The cell located in the upper left corner can be described as the core of
multidisciplinary team. The caseworker, guardian ad litem, respondent, and
respondent’s counsel perceive their stakes in the outcome of the MDT to be high. Their
participation reflects that perception. Similarly, the prosecutor (who serves as legal
counsel to the caseworker) should have important stake in the outcomes. Many survey
respondents complained about the lack of prosecutor involvement, which they argue

Multidisciplinary Teams in West Virginia Page | 37
undermines the effectiveness of the MDT process. For instance, a caseworker from a
smaller county remarked: “They [MDT’s] could be better if the Department’s attorney
from the county would show up and know what’s going on.” An attorney practicing in
one of the State’s larger counties similarly complained, “In ____ County, the
prosecuting attorney is almost never present at meetings. The prosecutor needs to be
involved so they are more aware of the progress of the case.”
The data show that when present, the prosecutors are usually involved in MDT
processes (see Table 14). However, the fact is that prosecutor’s presence in MDTs is
uneven across West Virginia. Several survey respondents commented on this general
unevenness.
For some reason, the Prosecutor feels he does not have to attend due to conflict. The Prosecutor has reported that the Prosecuting Attorney’s Institute has said it would be a conflict for him to attend.13 Yet, in other counties, Prosecutor’s are present when MDT’s occur. This is partly why, when we have court, the Prosecutor is not fully aware of what is occurring in that particular case. [DHHR Intake Supervisor]
This comment suggests that in at least one jurisdiction, the prosecutor’s office
operates on the presumption that participating in MDTs will create a conflict of interest
in their handling of other duties in the case. This position suggests diverging visions or
confusion of the prosecutor’s role in child welfare proceedings. Serving as a prosecutor,
does not necessarily align with serving as the department’s legal counsel. This role is at
odds with the duties expected of the prosecutor’s office. Some of the prosecutors we
13 Philip W. Morrison, Executive Director of the West Virginia Prosecuting Attorneys Institute counters that the institute would not make such a statement as a blanket recommendation. He told us that the institute may have recommended that a prosecutor not participate in particular MDT where specific circumstances led to clear conflicts, but he could not recall any specific case where this recommendation was made. (Personal Communication, 9/5/2008).

Multidisciplinary Teams in West Virginia Page | 38
spoke with expressed frustration with the expectation that they function as “social
workers” in these cases.
This tension is further exacerbated by the workload demands in the prosecutor’s
office. More than one fifth of West Virginia’s counties employ only one prosecutor; this
prosecutor is solely responsible for more than 80 statutory duties (Phillip W. Morrison,
personal communication 9/5/2008). Expecting the prosecutor’s office to operate as the
DHHR’s legal counsel in MDTs perpetuates an underfunded mandate. In one county,
we spoke to a part-time assistant prosecutor who is responsible for all child welfare
proceedings in the jurisdiction. When asked about his workload, he indicated that his
involvement in these cases exceeds a part-time commitment. He does put in the extra
uncompensated time because he believes that the MDTs are important. However, this
has become a hardship for him. We spoke with another part-time assistant prosecutor
who indicated he never attends treatment MDTs due to time constraints (though he
does attend every investigatory MDT). Thus, it is important to recognize that resource
limitation affects both sides of the institutional divide.
The remaining potential MDT members are classified in the medium to low
categories of both presence and participation. We find that approved service providers
are often present but play a limited participatory role in the MDT proceedings. Our
observations of these providers during site visits suggest that their primary role is to
report on the child, parent(s), or family’s progress in their program or service. Rarely
did these participants influence the meetings trajectory or take a more active role in the
interaction.
Similar to service providers, the survey data suggest that other professional
contributors to MDTs play a supporting role when they are present. Foster care

Multidisciplinary Teams in West Virginia Page | 39
providers, representatives from the schools, and behavioral health professionals attend
MDTs infrequently, but are moderately involved when present. Based on our
observation of MDTs, foster parents typically give a report on the children’s progress or
development in their home. Similarly, the behavioral health specialists we observed at
site visits limited their participation to reporting on progress in therapy. Two other
participant-types, court appointed special advocates and child advocacy center
personnel, fall into this category. However, many jurisdictions do not have or utilize
these types of service. In our site visits, our notes indicate that when these
organizations are present they tend to take an active role in the MDT.
Lastly, we note that the majority of respondents indicate that children rarely
attend or actively participate in the MDT sessions. 14 This may reflect that the majority
of these cases involve children too young to actively participate in their case plan.
However, that is an empirical question worthy of further investigation. Over the course
of our observations, we witnessed only a small handful of children present in MDT
sessions and in only one case could we describe the child as an active participant in the
session. If the state wishes to increase children’s participation in this process, this
observation requires examination and thought.
From this discussion we can conclude that the core of the MDT is centralized in
the activities of DHHR, the families receiving services, and the legal counsel hired or
assigned to assist them. This observation is important as we situate the meaning of
team management and leadership.
14 “The child may participate in multidisciplinary treatment team meetings if such is deemed appropriate by the multidisciplinary treatment team (see West Virginia Code § 49-5D-3).” Of course, involvement children in the MDT process pose additional complications. As a philosophical matter we should provide children with every opportunity to influence the processes that affect their lives. However, there are practical reasons to exclude the child from participation. MDTs involve the entire family unit. As such, on occasion, there are matters deliberated in MDTs from which the child should be protected. .

Multidisciplinary Teams in West Virginia Page | 40
Variance!in!MDT!Practices!
There is no one single prevailing model of MDT practice or operation. Instead
our research shows MDT practices and procedures vary considerably. The types of
variation fall along several dimensions. First, the patterns of participation and
involvement of team members varies considerably across the State. Second, the teams
are managed and led in a variety of ways. Third, clear differences in the institutional
cultures of the specific circuit courts and county DHHR offices influence the MDTs.
Fourth, and finally, participants filling different roles within the MDT report stark
differences in their experiences as members. We provide detailed discussion of each of
these findings in the sections that follow.
The survey’s initial goal was to measure the extent to which MDTs differ in
substantive ways. We asked each survey respondent to identify the county or counties
in which they participate in MDTs. We observed substantial variation in our site visits.
Clearly, in their implementation, MDTs assume local characteristics or flavor. For
instance, we observed MDTs in three geographically proximate counties. Though they
are all in the same region and include participants who practice in all three jurisdictions,
they could not be more different. In county 1, MDTs are scheduled every 90 days (or
more often when deemed necessary by the members), are convened at the county
DHHR office, and are facilitated by a CPS supervisor.15 The prosecutor’s office does not
send a representative to the meetings to be the petitioner’s counsel (a point that several
respondent’s attorney wished for us to note). In county 2, MDTs are scheduled every 30
days but last only 20 minutes each. They are convened in a municipal meeting room
15 The caseworker begins the meeting and leads discussion about the case, but the supervisor remains in the room and plays an active role in steering discussion. This differs considerably from some other locations where the CPS supervisor does not come to MDTs.

Multidisciplinary Teams in West Virginia Page | 41
(though in the same building where DHHR’s offices are located). A supervisor from CPS
facilitates the meeting and an assistant prosecuting attorney participates as the
petitioner’s counsel. Lastly, in the third county, MDTs are convened at an independent
agency every 90 days (or more often when necessary). The director of the local child
advocacy center initiates the meeting and intercedes as necessary in the capacity of a
neutral arbiter. An assistant prosecuting attorney is present and takes an active role in
the MDT deliberations.
Measurement of these county-to-county differences, easily observed in the
qualitative study, proved difficult to capture in the quantitative data. Statistical analysis
of variance (ANOVA) tests did not yield statistically significant differences by region or
county on any of the experience or perception batteries described in Table 3 (the results
of the ANOVA are provided in Appendix A). This should not be interpreted as evidence
for the absence of county-to-county variation. Rather, the statistical analysis of self-
reported retrospective survey measurements was an inadequate tool for this task.
Comparisons made between DHHR’s administrative regions mask intraregional
differences between the constituent counties. A county level analysis would be
preferable, but was precluded in this study by prohibitively small N’s in many of the
counties.16
Despite our inability to adequately measure the differences observed at site visits,
we hypothesized that they are a function of the organizational ecology and the localized
culture unique to each jurisdiction. This ecology is shaped by dynamics at the local level
that influence the relationships between the courts, the Department of Health and 16 There were ten or fewer responses from 40 counties. A statistical test including t-tests, ANOVA, and multiple regressions requires that there be multiple cases for each category under comparison. Absent a sufficient number of cases, estimated differences are inefficient and are compromised by variability among the data points.

Multidisciplinary Teams in West Virginia Page | 42
Human Resources, social service providers, and other stakeholder participants. These
differences are also a function of variation in the infrastructure specific to different
jurisdictions. For instance, some counties have strong Court Appointed Special
Advocate (CASA) programs that are tightly integrated into child welfare proceedings,
while other counties have no such resource. Some counties have access to a broad range
of approved service organization (ASO) providers, while in other counties the
availability and variety of service providers is more limited. MDTs reflect their broader
organizational ecology.
DISCUSSION,!CONCLUSIONS!&!RECOMMENDATIONS!
We initiated this study with the working hypothesis that we would find
substantial variation across the state in MDT practices. To this end, we were not
surprised that our initial assumptions were confirmed through survey analysis and field
work. There appear to be significant differences among the counties. We suggest that
these are a function of factors that are distinct to each jurisdiction along with
established patterns and lines of relationships between those involved that have their
own unique dynamic.
What we did not fully anticipate in the development of this evaluation and which
is the most startling conclusion that we draw from the study is the clear difference of
opinion and attitude expressed toward the MDT by two crucial stakeholder groups in
the process – DHHR personnel and the attorneys that represent various parties in the
process. In our field work and through our survey research we find often startling
differences of opinion and perception of the efficacy and performance of West Virginia’s
MDT system.

Multidisciplinary Teams in West Virginia Page | 43
West Virginia’s multidisciplinary teams are constituted with participants drawn
from two distinct institutional cultures. The MDT has become a middle ground between
the arenas of law and social service. It is clear that the participants from one arena do
not always comprehend the circumstance, aspirations, and motivations of the other.
This lack of clarity breeds frustration and inefficiencies in the process. To be clear, the
problems born from this two culture problem largely appear to be benign. The survey
results are unequivocable in that the majority of respondents from either sample
perceive MDTs to be working toward their intended ends. Yet, the survey also provides
evidence of systematic points of friction between the two cultures. Since the MDT
process is designed to serve the welfare of children, we believe these issues deserve
careful consideration by policy makers and by those who design training curricula.
When disagreements render the divisions visible, we found that DHHR personnel
are more likely to see the MDT as efficacious and legitimate and a process for planning
and developing treatment plans. In contrast, attorneys appear to be more likely to see
the MDTs as a pro-forma exercise run by the social workers. They articulate concern
that should they express reservations about the collaborative process, they may put their
client’s interest at risk. As we conclude, we do not believe that these differences are
insurmountable. Instead, we argue that those vested in the MDT process must be
cognizant of these differences and undertake steps in MDT training, logistics, and
practices that take these distinctions into account.
Recommendations!
In offering our recommendations, we emphasize that West Virginia is not alone
in its challenges to initiate and sustain effective MDT programming. A review of the

Multidisciplinary Teams in West Virginia Page | 44
literature emphasizes the difficulties and challenges that are involved in establishing
and maintaining such arrangements. Numerous studies note that the effective
operation of such teams is no easy task. Much of what we know about MDTs comes from
their application in health care settings – where the multidisciplinary approach was first
pioneered. We argue that lessons from this experience are applicable to child welfare
MDTs as well. One of the major barriers is "interprofessional rivalry" (Jones, 1996: 19).
In these settings, profession and position seem to work against the dialogue,
cooperation, and communication needed for effective MDTs (Jones, 1996: 26-27).
Another barrier is found in a lack of clearly established processes and purposes
for team function. Without clearly shared goals and the opportunity for frequent and
meaningful interaction, MDTs are prone to be ineffective. This is due to the fact that in
the absence of such guideposts, participants fall back on established practices and rely
on their own professional norms, biases, or worldviews rather than engage in
meaningful participation (Fay et al., 2006: 564). Effective MDTs must have
"superordinate goals" that are clearly shared and adhered to by participants (Fay et al.,
2006: 556). This is another way of saying that MDT’s must have a "shared vision" or
purpose in order to work effectively (Anderson and West, 1998: 240).
Establishing a shared sense of purpose and objective may prove difficult in
developing treatment plans. As has been noted by one study, it may be more difficult to
manage the more open-ended commitments involved in treatment planning than in
MDTs that are investigating child neglect and abuse cases (Lalayants and Epstein, 2005:
435). Those who have studied MDTs in child welfare settings recognize that their form
and functions may vary greatly (Kolbo, 1997; Lalayant and Epstein 2005). This further
complicates efforts for teams in any one setting or context to learn from the best

Multidisciplinary Teams in West Virginia Page | 45
practices of others. While guidebooks for MDT in the child welfare context exist (see
Ells 2004), their recommendations tend to be general and non-specific. Thus, we can
conclude that the creation and operation of effective MDTs is a complex undertaking.
We can also conclude that while the lessons from others are valuable, the primary
responsibility for building and improving our own system rests on self assessment and
evaluation.
Recommendation!1:!Provide!More!Facilitation!Support!for!MDTs!
There are many advantages to adopting a facilitation model where the MDT is
directed by a person not party to the proceedings. This allows the caseworkers,
attorneys, and other substantively involved persons to focus on the dialogue and
deliberation rather than try to keep the discussion on point, or capture details necessary
for a report. Insofar as an authoritative third-party can preside over the MDT process
ensuring and attending to administrative details, the efficacy of the deliberative
interaction will be enhanced. Increasing such support will improve the gathering of
administrative data necessary to populate fields in the FACTS database and satisfy court
reporting requirements.
Also, given our discovery of the ‘two culture’ problem, a third party facilitator has
the capacity to mediate should conflict emerge. A facilitator should be instrumental in
ensuring that the focus of the MDT remains directed at serving the best interests of the
children and their families. Establishing a neutral facilitation model would go a long
way towards countering the minority perception that MDTs are “a sham” or “an
inquisition.”

Multidisciplinary Teams in West Virginia Page | 46
Recommendation!2:!!Create!Multidisciplinary!Training!for!Multidisciplinary!Teams!
However benign the conflict may be, misunderstandings between the two
cultures creates obstacles for the MDT process which undermines its efficacy. The most
immediate strategy for addressing this problem is to design new training and in-service
curricula that explicitly recognizes the various parties in the MDT and their roles. Such
instructional sessions should remind the participants that MDTs bring together a
multiplicity of contributors who have been socialized in different institutional milieus.
We also recommend that the Court Improvement Program encourage
multidisciplinary training for MDT participants. Though we did not obtain specific
information from the survey respondents as to the types of training they received, we
suspect that the majority of those attending training in the past year did so within the
framework of their specific professional continuing education mechanisms. That is, we
suspect that DHHR personnel were trained along with other employees of the Bureau
for Children and Families, by an instructor retained by the Bureau. In contrast, we
suspect that the attorneys reporting that they have been trained on MDT issues in the
past year, refer to continuing legal education activities sponsored by the Bar Association
and other legal groups. The DHHR should join forces with the Bar Association and the
Court Improvement Program to design and deliver a thorough instructional program
that addresses the policies from a variety of perspectives. Such curricula are ideally
delivered in a setting where all the parties of an MDT participate.
Recommendation!3:!!Reassess!the!Objectives,!Goals,!and!Purposes!of!the!MDT!Process.!
Chapter 49 of the West Virginia Code is designed to provide a coordinated system
of child welfare and juvenile justice for the children of this state that has goals to

Multidisciplinary Teams in West Virginia Page | 47
promote safety AND where possible strengthen the ties between children and their
families (see West Virginia Code §49-1-1). It is clear from our site visits and analysis of
the survey data that some MDTs fail to develop a common vision among the members to
achieve these goals. This is understandable given the paradox inherent in delivering
contemporary child welfare. The MDT is supposed to simultaneously, or concurrently,
provide services to the family while at the same time plan for the children’s permanency
should reunification not be possible.
We recommend that the State of West Virginia reconsider the policies
promulgated to comply with the article implementing MDTs (see West Virginia Code §
49-5D-1 et seq.). Whereas the explicit goal of the MDT is to “provide a system for
evaluation of and coordinated service delivery for children who may be victims of abuse
or neglect” (West Virginia Code § 49-5D-1), we propose that the Court Improvement
Program encourage all jurisdictions to embrace a collaborative process, involving all the
key stakeholders, in achieving the expectations.
Recommendation!4:!Attend!to!the!Practical!Needs!of!All!Stakeholders!
Our research shows that the capacity to participate on MDTs varies considerably
across the role categories. Many potential participants, persons who maintain a stake in
the life of a child or her family, such as a school counselor, are often unable to
participate due to the time and location of scheduling. Likewise, many attorneys are
unable to attend MDTs because their scheduling conflicts with motions, hearings, and
the demands placed on their time by other clients. Therefore, we recommend that care
be taken in the planning and scheduling of MDTs to increase the participation of
relevant stakeholders. We note that several jurisdictions have implemented routinized

Multidisciplinary Teams in West Virginia Page | 48
scheduling. Under this model, the judges and magistrates in the circuit do their best to
avoid scheduling motions or hearings on days and times when the MDTs ordinarily
convene. Our analyses of the Survey data suggest that participation is greater in MDTs
that occur in these counties. We recommend that the Court Improvement Program
encourage the circuits to work with the Department of Health and Human Resources to
emphasize the importance of MDTs.
Recommendation!5:!!Recognize!the!Developmental!Character!of!Treatment!Planning!
The MDT is designed to facilitate treatment planning and service delivery.
Assessing needs, planning treatment, and delivering services are all tasks that pursue a
moving target. As such, MDT policies and procedures must recognize that treatment
provision is an uncertain process which unfolds differently on a case-by-case basis. This
contrasts with the more definitive process adopted by investigatory MDTs (see West
Virginia Code §49-5D-2). These contingencies and ambiguities are recognized in the
scholarly literature on MDTs (see Lalayants and Epstein 20005). Treatment MDTs
should be encouraged to approach their task with flexibility and patience. To the
greatest extent possible, stakeholders in the MDT must be encouraged to continually
assess the ongoing process for each individual case.
Recommendation!6:!!A!Study!of!the!Parent!&!Child’s!Experience!is!Necessary!
Lastly, this study was conducted without the input from two important
stakeholders in the MDT process. The child welfare system is designed to promote the
safety of children and promote strong family ties. Parents (or adult respondents) are
crucial participants in the MDT. In this report, we provide sobering evidence that while
parents are almost always present at MDTs, they are rarely viewed by the others as a

Multidisciplinary Teams in West Virginia Page | 49
“extremely active” participants. This suggests that in many jurisdictions, the MDT
process has become something that is done to parents, rather than with parents. The
data for children is even more striking. Children rarely attend MDTs and when they are
present, the others perceive them as inactive.
Child welfare policy is rooted in assumptions about how parents and children
experience the system. These assumptions inform direct practice. Yet, we don’t really
have a clear sense for how the purported beneficiaries of these policies really experience
them. West Virginia would be on the cutting edge if they commissioned a thorough
scientific study of the experiences of these stakeholders and then used the information
to sponsor change.

Multidisciplinary Teams in West Virginia Page | 50
REFERENCES!
Anderson, Neil R. and Michael A. West. 1998. "Measuring Climate for Work Group Innovation: Development and Validation of the Team Climate Inventory." Journal of Organizational Behavior 19: 235-258.
Ells, Mark. 2000. Forming A Multidisciplinary Team To Investigate Child Abuse.
Washington, D.C.: U.S. Department of Justice, Office of Justice Programs, Office of Juvenile Justice and Delinquency Prevention.
Fay, Doris, Carol Borrill, Ziv Amir, Robert Haward, and Michael A. West. 2006. Getting
the Most Out of Multidisciplinary Teams: A Multi-Sample Study of Team Innovation in Health Care." Journal of Occupational and Organizational Psychology. 79: 553-567.
Jones, Adrian. 2006. "Multidisciplinary Team Working: Collaboration and Conflict."
International Journal of Mental Health Nursing. 15: 19-28. Kolbo, Jerome R. and Edith Strong. 1997. "Multidisciplinary Team Approaches to the
Investigation and Resolution of Child Abuse and Neglect: A National Survey." Child Maltreatment 2(1): 61-72.
Lalayants, Marina and Irwin Epstein. 2005. "Evaluating Multidisciplinary Child Abuse
and Neglect Teams: A Research Agenda." Child Welfare 84(4): 433-458. Snow, C.P. 1960. Science and Government. Cambridge, MA: Harvard University Press Snow, C.P. 1959. The Two Cultures and the Scientific Revolution. New York:
Cambridge University Press.

Multidisciplinary Teams in West Virginia Page | 51
APPENDICES!

Multidisciplinary Teams in West Virginia Page | 52
Appendix!A!–!Statistical!Models!
Analysis of Variance Are there Statistically Significant Variations across West Virginia’s Administrative Regions? Battery F Prob > F Explanation
Treatment Outcomes 0.55 < 0.65 There were no statistically significant differences between the mean values of the treatment batteries across regions.
Scheduling Frequency and Sufficiency
0.52 < 0.52
Sensitivity of MDT procedures to various parties
0.24 < 0.86
Do MDT proceedings yield effective outcomes?
0.48 < 0.70
Do MDT proceedings achieve the expectations set forth in policy?
0.24 <0.87
Who participates? 1.00 <0.39
Logistic Regression Model: Logged Odds Ratio Predicting Prosecutor
Participation
Logistic!regression!Number!of!obs!!!=! 310LR!chi2(4)!!!!!!=! 27.3Prob!>!chi2!!!!!=! 0
Log!likelihood!=!"166.46207! Pseudo!R2!!!!!!!=! 0.0758
Odds!Ratio!Odds!Ratio!
Std.!Err.! z! Prob! 95!%!Confidence!Interval!
Courthouse! 5.09! 1.94 4.26 <!0.001***! 2.41! 10.7555Municipal!Building! 2.21! 2.49 0.70 0.48! 0.24! 20.14631Child!Advocacy!Center! 6.07! 6.41 1.71 0.09*! 0.77! 48.02869Law!Firm! 0.33! 0.45 "0.81 0.42! 0.02! 4.735993

Multidisciplinary Teams in West Virginia Page | 53
Appendix!B:!Map!of!DHHR’s!Administrative!Regions!


Multidisciplinary Teams in West Virginia Page | 56
Appendix!C:!!Solicitation!Letter!



Multidisciplinary Teams in West Virginia Page | 58
Appendix!D:!Survey!Instruments!

Page 1
2008 West Virginia MDT Survey - DHHR Version
1. Respondent Background
This survey is designed to gather information concerning formal multidisciplinary treatment team (MDT) proceedings in West Virginia Child Abuse and Neglect Proceedings.
In the questions that follow, please base your answers on experience with treatment MDTs for abuse and neglect cases only.
1. Which of the following best describes your current duties within West Virginia's Department of Health and Human Resources?
2. In which county or district do you currently work? If you work in more than one county or district please select location where you work most frequently from the drop down list and specify the others in the comment box that follows.
3. Approximately how long have you been employed by the Department of Health and Human Resources in Child Protective Services? Please round your answer to the nearest quarter year (e.g., 2.0, 2.25, 2.50, 2.75)
4. Approximately how long have you been employed in your current position? Please round your answer to the nearest quarter year (e.g., 2.0, 2.25, 2.50, 2.75).
5. The remaining questions in this survey are concerned with your experiences in formal Child Abuse & Neglect MDTs. Did you participate as a team member in any MDTs in the past year (since February 1, 2007)?
6. Now, thinking about the past year (since February 1, 2007), in approximately how many MDT meetings did you participate?
7. Now, thinking about the month of January 2008, in approximately how many MDT meetings did you participate?
CPS Supervisor
CPS Caseworker nmlkjnmlkj
Other (e.g., permancy worker, social services supervisor, etc). Please specify below.
nmlkj
If you work in multiple counties, please select the primary county (e.g., where you work the most) above and enter the other counties
below. (Please separate multiple counties with a comma: Monongalia, Marion).
Yes
No nmlkjnmlkj
Please enter the number of meetings. If you are unsure, estimate.
Please enter the number of meetings. If you are unsure, estimate.

Page 2
2008 West Virginia MDT Survey - DHHR Version
2. MDT Training
Now we would like to ask you some questions concerning your experiences with MDT training and other in-service opportunities.
8. Have you ever attended a formal training session (e.g., a session with an instructor and a defined curriculum) concerning Multidisciplinary Team processes and procedures?
Yes
No nmlkjnmlkj

Page 3
2008 West Virginia MDT Survey - DHHR Version
3. Training Experiences
9. Approximately how long has it been since your last MDT training?
10. Considering all of your MDT training taken as a whole, how effective have these training sessions been in preparing you for your responsibilities as an MDT participant?
11. Considering the last MDT training session that you attended, how effective was that session in preparing you for your responsibilities as an MDT participant?
Less than one month ago
Between one and six months ago
More than six months but less than a year ago
Between one and two years ago
More than two years ago
nmlkjnmlkjnmlkjnmlkjnmlkj
Extremely effective
Effective
Neither effective nor ineffective
Ineffective
Extremely ineffective
nmlkjnmlkjnmlkjnmlkjnmlkj
Extremely effective
Effective
Neither effective nor ineffective
Ineffective
Extremely ineffective
nmlkjnmlkjnmlkjnmlkjnmlkj

Page 4
2008 West Virginia MDT Survey - DHHR Version
4. Location and Scheduling of MDTs
For the next group of questions, we are interested to learn about how typical MDTs operate in your county.
12. About how many miles on average do you travel from your office to attend MDT sessions? (If most MDTs are held in your office building, please enter zero).
13. We are interested to know about how much time you invest in preparation for MDT sessions.
14. Does your agency or office provide support staff to assist you in preparation for MDT meetings?
15. Thinking about your participation in MDTs in the past year, please identify all the locations where MDTs meet in your county. (Check all that apply)
16. Thinking about your participation in MDTs in the past year, please identify the location where MDTs meet most frequently in your county. (Check only one)
17. Some counties schedule MDTs on set days during the month (e.g., every other Thursday), while other counties do not schedule MDTs on set days. How are MDTs typically scheduled in your county?
Approximately how much time in minutes do you spend preparing for a
typical MDT session?
Considering all of your cases in calendar year 2007, what was the longest
period of time (in minutes) that you spent preparing for a MDT session?
Yes
No nmlkjnmlkj
DHHR Office
Court House
Municipal Building (neither courthouse, nor DHHR offices)
Child Advocacy Center
Law Firm Offices
gfedcgfedcgfedcgfedcgfedc
Other (please specify)
gfedc
DHHR Office
Court House
Municipal Building (neither courthouse, nor DHHR offices)
Child Advocacy Center
Law Firm Offices
nmlkjnmlkjnmlkjnmlkjnmlkj
Other (please specify)
nmlkj
My county schedules most MDTs on set days
My county does not schedule most MDTs on set days nmlkjnmlkj

Page 5
2008 West Virginia MDT Survey - DHHR Version18. In your experience, who is responsible for leading and directing MDT meetings?
19. In your experience, which office or agency is responsible for scheduling meetings and notifying participants?
20. We understand MDT meetings vary in length. Considering all the MDTs in which you participated last year:
DHHR Supervisor
DHHR Caseworker
Prosecuting Attorney
Personnel from the Child Advocacy Center
It's not clear to me that any one person is responsible for leading and directing the meeting
nmlkjnmlkjnmlkjnmlkjnmlkj
Other (please specify)
nmlkj
Please specify if you checked "agency other than what's listed here"
DHHRProsecuting
Attorney's Office
Child Advocacy
CenterI don't know
An agency other
than what's listed
here (please specify
below)
Responsible for
Schedulingnmlkj nmlkj nmlkj nmlkj nmlkj
Responsible for Notifying nmlkj nmlkj nmlkj nmlkj nmlkj
How many minutes long was the the shortest MDT session?
How many minutes long was the longest MDT session?
How many minutes long was the average or typical MDT session?

Page 6
2008 West Virginia MDT Survey - DHHR Version
5. Perception of MDT Processes - Treatment Effectiveness
We would like to ask you some questions concerning your experiences as a participant in Child Abuse and Neglect treatment MDTs. For each of the following questions, please think about the MDT sessions that you attended over the past year (since February of 2007).
21. The following questions are concerned with how well multidisciplinary treatment teams implement treatment objectives. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the multidisciplinary team accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
Develop individualized
service plans for the
children and families?
nmlkj nmlkj nmlkj nmlkj
Base treatment planing
on comprehensive
assessments of children
and families?
nmlkj nmlkj nmlkj nmlkj
Coordinate treatment
plans for the child with
resources available in the
community?
nmlkj nmlkj nmlkj nmlkj
Coordinate treatment
plans for the family with
resources available in the
community?
nmlkj nmlkj nmlkj nmlkj

Page 7
2008 West Virginia MDT Survey - DHHR Version
6. Perception of MDT Processes - Frequency & Duration
22. The next group of questions are concerned with the frequency, duration, and location of MDT meetings in abuse and neglect cases. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the MDT accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
MDT sessions occur
frequently enough to
aide in designing,
implementing, and
monitoring treatment
plans.
nmlkj nmlkj nmlkj nmlkj
MDT sessions last long
enough to adequately
address the needs of the
case.
nmlkj nmlkj nmlkj nmlkj
MDT sessions are
scheduled at times that
are convenient for me to
attend.
nmlkj nmlkj nmlkj nmlkj
MDT sessions are
scheduled in places that
are convenient for me to
attend.
nmlkj nmlkj nmlkj nmlkj

Page 8
2008 West Virginia MDT Survey - DHHR Version
7. Perception of Multidisciplinary Team Processes - Responsiveness
We would like to ask you some questions concerning your experiences as a participant in MDT proceedings. For each of the following questions, please think about the MDT sessions that you attended over the past year (since February of 2007).
23. The next group of questions are concerned with the extent to which MDTs are sensitive to the needs and/or concerns of their constituent members. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the multidisciplinary team accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
The MDT process is
sensitive to the needs
and/or concerns of the
child(ren).
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of the
adult respondents
(usually the parents).
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of co-
petitioners or intervenors.
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of DHHR
caseworkers.
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of the
Legal counsel for the
Children.
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of the
Legal counsel for the
adult respondent(s).
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of the
prosecutor.
nmlkj nmlkj nmlkj nmlkj

Page 9
2008 West Virginia MDT Survey - DHHR Version24. Are there parties, other than those listed above, involved in the MDT meetings, who are affected by the MDT process? If so, who are they and how are they affected?

Page 10
2008 West Virginia MDT Survey - DHHR Version
8. Perception of MDT Processes - Consensus & Outcomes
We would like to ask you some questions concerning your experiences as a participant in MDT proceedings. For each of the following questions, please think about the MDT sessions that you attended over the past year (since February of 2007).
25. The questions that follow concern the extent to which MDTs yield agreement and consensus. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the multidisciplinary team accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
The members of the
multidisciplinary team are
able to come to a
consensus concerning the
treatment plan for
particular cases.
nmlkj nmlkj nmlkj nmlkj
The multidisciplinary
team is able to formulate
recommendations to the
court that reflect member
consensus.
nmlkj nmlkj nmlkj nmlkj
The multidisciplinary
team generates an
official report
communicating
recommendations to the
court.
nmlkj nmlkj nmlkj nmlkj
Recommendations that
come from the
multidisciplinary team
reflect the full range of
members' opinions
concerning the case.
nmlkj nmlkj nmlkj nmlkj

Page 11
2008 West Virginia MDT Survey - DHHR Version
9. Perception of MDT Processes - Implications for Policy
We would like to ask you some questions concerning your experiences as a participant in MDT proceedings. For each of the following questions, please think about the MDT sessions that you attended over the past year (since February of 2007).
26. The next group of questions are concerned with the extent to which multidisciplinary treatment team proceedings achieve the ideal goals as set by state policy. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the multidisciplinary team accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
Multidisciplinary team
practices contribute to the
overall goal of making
reasonable efforts to
preserve or reunify
families.
nmlkj nmlkj nmlkj nmlkj
Multidisciplinary team
practices contribute to the
overall goal of
maximizing the safety of
children.
nmlkj nmlkj nmlkj nmlkj
Multidisciplinary team
practices contribute to the
overall goal of achieving
permanency for children
in a timely manner.
nmlkj nmlkj nmlkj nmlkj

Page 12
2008 West Virginia MDT Survey - DHHR Version
10. Constitution of Multidisciplinary Teams
A diverse pool of people are involved in West Virginia Multidisciplinary Teams. Your answers to the following series of questions will help us better understand who participates in MDTs and in what capacity.
27. The next group of questions are concerned with the constitution or makeup of multidisciplinary treatment teams. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how frequently each of the following participants attended MDT meetings.
Which parties fall under other?
Never or almost never Occasionally Much of the time Always or almost always
DHHR Caseworker nmlkj nmlkj nmlkj nmlkj
DHHR Supervisor nmlkj nmlkj nmlkj nmlkj
Prosecuting Attorney nmlkj nmlkj nmlkj nmlkjAttorney for Adult
Respondent (often the
Parent)
nmlkj nmlkj nmlkj nmlkj
Attorney for the Child or
Childrennmlkj nmlkj nmlkj nmlkj
The Child or Children nmlkj nmlkj nmlkj nmlkjAdult Respondent (often
the Parent)nmlkj nmlkj nmlkj nmlkj
Foster Care Provider nmlkj nmlkj nmlkj nmlkjCourt Appointed Special
Advocatenmlkj nmlkj nmlkj nmlkj
Child Advocacy Center
Personnelnmlkj nmlkj nmlkj nmlkj
Representatives from
Contracting or Fee-For-
Service Providers
(Homebase, Parenting
Instruction, etc)
nmlkj nmlkj nmlkj nmlkj
Representatives from
Behavioral Healthcare
Providers (Counselors,
Psychologists, etc)
nmlkj nmlkj nmlkj nmlkj
Representatives from the
Schoolsnmlkj nmlkj nmlkj nmlkj
Other parties not listed
above (such as Co-
Petioners or Intervenors)
please describe in the
comment box below
nmlkj nmlkj nmlkj nmlkj

Page 13
2008 West Virginia MDT Survey - DHHR Version
11. Member Contributions to MDT Processes
28. Other studies of MDTs have shown that member participation, engagement, or involvement, varies from extremely passive to extremely active. Thinking about your experiences in MDTs over the past year (since February of 2007), please rate the typical involvement of the following people. If a person listed does not routinely participate in MDT meetings in your county, please check "never or almost never present."
If you rated the "other" category, please describe
Never or almost never
present Extremely Passive
Balanced between
Passive and ActiveExtremely Active
DHHR Caseworker nmlkj nmlkj nmlkj nmlkj
DHHR Supervisor nmlkj nmlkj nmlkj nmlkj
Prosecuting Attorney nmlkj nmlkj nmlkj nmlkjAttorney for Adult
Respondent (often the
parent)
nmlkj nmlkj nmlkj nmlkj
Attorney for the Child or
Childrennmlkj nmlkj nmlkj nmlkj
The Child or Children nmlkj nmlkj nmlkj nmlkjAdult Respondent (often
the parent)nmlkj nmlkj nmlkj nmlkj
Foster care provider nmlkj nmlkj nmlkj nmlkjCourt Appointed Special
Advocatenmlkj nmlkj nmlkj nmlkj
Child Advocacy Center
Personnelnmlkj nmlkj nmlkj nmlkj
Representatives from
contracting or fee-for-
service providers
(Homebase, Parenting
Instruction, etc)
nmlkj nmlkj nmlkj nmlkj
Representatives from
behavioral health care
providers (Counselors,
Psychologists, etc)
nmlkj nmlkj nmlkj nmlkj
Representative from the
Schoolsnmlkj nmlkj nmlkj nmlkj
Other parties not listed
above (such as co-
petioners or intervenors)
please describe in the
comment box below
nmlkj nmlkj nmlkj nmlkj

Page 14
2008 West Virginia MDT Survey - DHHR Version
12. Open ended Questions
In this survey, we have asked you several questions concerning the processes and procedures of West Virginia Multidisciplinary Teams. Now we would like to give you the opportunity to tell us what you think is most important and offer us recommendations for improving policies and procedures.
29. What should MDTs accomplish?
30. Can you offer any suggestions on how the Multidisciplinary Team process could be improved?
31. Some critics argue that our current MDT process fails to involve key participants who would contribute positively to the MDT. In your opinion, who else should be involved in MDTs?

Page 15
2008 West Virginia MDT Survey - DHHR Version32. Finally, is there anything else about MDTs that you think is important for us to know, or that you would like to share?

Page 1
2008 West Virginia MDT Survey - Attorney Version
1. Respondent Background
This survey is designed to gather information concerning formal multidisciplinary treatment team (MDT) meetings in West Virginia child abuse and neglect cases. W.Va. Code § 49-6-1, et seq.
Multidisciplinary treatment teams are to “assess, plan and implement a comprehensive individualized service plan for children who are victims of abuse or neglect and their families when a judicial proceeding has been initiated involving the child or children.” W.Va. Code § 49-5D-3. This survey is part of a larger effort to examine the processes and procedure implemented to satisfy these requirements.
In the questions that follow, please base your answers on experience with treatment MDTs for abuse and neglect cases only.
1. This survey seeks your input pertaining to treatment MDTs in West Virginia Child Abuse and Neglect proceedings. Approximately how long (in years) have you been representing parties in West Virginia Child Abuse and Neglect Proceedings? Please round your answer to the nearest quarter year (e.g., 2.0, 2.25, 2.50, 2.75).
2. Thinking about the past year (since February 2007), in which county do you represent clients in Abuse and Neglect proceedings? If you represent clients in Abuse and Neglect cases in more than one county, please select the county where you practice most from the drop down list, then specify the other counties in the comment box that follows.
3. Thinking about your practice over the past year, in which of the following capacities have you represented clients in Abuse and Neglect Proceedings? (Please select all that apply)
If you practice in multiple counties, please select the primary county (e.g., where you work the most) above and enter the other
counties below. (Please separate multiple counties with a comma: Monongalia, Marion).
Counsel to Adult Respondent
Counsel to Co-Petitioner
Counsel to intervenor
Guardian ad Litem
gfedcgfedcgfedcgfedc
Other Capacity (please describe)
gfedc

Page 2
2008 West Virginia MDT Survey - Attorney Version4. Thinking about your practice over the past year, in which of the following capacities have you most represented clients in Abuse and Neglect Proceedings? (Please select only one)
5. Approximately how long have you been practicing law? Please round your answer to the nearest quarter year (e.g., 2.0, 2.25, 2.50, 2.75).
6. The remaining questions in this survey are concerned with your experiences in formal Child Abuse & Neglect MDTs. Did you participate as a team member in any MDTs in the past year (since February 1, 2007)?
7. Now, thinking about the past year (since February 1, 2007), in approximately how many MDT meetings did you participate?
8. Now, thinking about the month of January 2008, in approximately how many MDT meetings did you participate?
Counsel to Adult Respondent
Counsel to Co-Petitioner
Counsel to intervenor
Guardian ad Litem
nmlkjnmlkjnmlkjnmlkj
Other Capacity (pleae describe)
nmlkj
Yes
No nmlkjnmlkj
Please enter the number of meetings. If you are unsure, estimate.
Please enter the number of meetings. If you are unsure, estimate.

Page 3
2008 West Virginia MDT Survey - Attorney Version
2. MDT Training
Now we would like to ask you some questions concerning your experiences with MDT training and other in-service opportunities.
9. Have you ever attended a formal training session, CLE or MCLE (e.g., a session with an instructor and a defined curriculum) concerning Multidisciplinary Treatment Team processes and procedures?
Yes
No nmlkjnmlkj

Page 4
2008 West Virginia MDT Survey - Attorney Version
3. Training Experiences
10. Approximately how long has it been since your last MDT training?
11. Considering all of your MDT training taken as a whole, how effective have these training sessions been in preparing you for your responsibilities as an MDT participant?
12. Considering the last MDT training session that you attended, how effective was that session in preparing you for your responsibilities as an MDT participant?
Less than one month ago
Between one and six months ago
More than six months but less than a year ago
Between one and two years ago
More than two years ago
nmlkjnmlkjnmlkjnmlkjnmlkj
Extremely effective
Effective
Neither effective nor ineffective
Ineffective
Extremely ineffective
nmlkjnmlkjnmlkjnmlkjnmlkj
Extremely effective
Effective
Neither effective nor ineffective
Ineffective
Extremely ineffective
nmlkjnmlkjnmlkjnmlkjnmlkj

Page 5
2008 West Virginia MDT Survey - Attorney Version
4. Location and Scheduling of MDTs
For the next group of questions, we are interested to learn about how typical MDTs operate in your county.
13. About how many miles on average do you travel from your office to attend MDT sessions? (If most MDTs are held in your office building, please enter zero).
14. We are interested to know about how much time you invest in preparation for MDT sessions.
15. Does your participation in MDTs involve uncompensated work (e.g., activities that are un-billable or non-reimbursable)? If Yes, please elaborate in the comment field below.
16. Thinking about your participation in MDTs in the past year, please identify all the locations where MDTs meet in your county. (Check all that apply)
17. Thinking about your participation in MDTs in the past year, please identify the location where MDTs meet most frequently in your county. (Check only one)
Approximately how much time in minutes do you spend preparing for a
typical MDT session?
Considering all of your cases in calendar year 2007, what was the longest
period of time (in minutes) that you spent preparing for a MDT session?
Yes
No nmlkjnmlkj
If you answered yes, please elaborate
DHHR Office
Court House
Municipal Building (neither courthouse, nor DHHR offices)
Child Advocacy Center
Law Firm Offices
gfedcgfedcgfedcgfedcgfedc
Other (please specify)
gfedc
DHHR Office
Court House
Municipal Building (neither courthouse, nor DHHR offices)
Child Advocacy Center
Law Firm Offices
nmlkjnmlkjnmlkjnmlkjnmlkj
Other (please specify)
nmlkj

Page 6
2008 West Virginia MDT Survey - Attorney Version18. Some counties schedule MDTs on set days during the month (e.g., every other Thursday), while other counties do not schedule MDTs on set days. How are MDTs typically scheduled in your county?
19. How frequently do you encounter scheduling conflicts that make it difficult to participate in MDTs?
20. In your experience, who is responsible for leading and directing MDT meetings?
21. In your experience, which office or agency is responsible for scheduling meetings and notifying participants?
22. Do you receive adequate notification of pending MDT meetings involving your clients?
My county schedules most MDTs on set days
My county does not schedule most MDTs on set days nmlkjnmlkj
Never or almost never
Occasionally
Much of the time
Always or almost always
nmlkjnmlkjnmlkjnmlkj
DHHR Supervisor
DHHR Caseworker
Prosecuting Attorney
Personnel from the Child Advocacy Center
It's not clear to me that any one person is responsible for leading and directing the meeting
nmlkjnmlkjnmlkjnmlkjnmlkj
Other (please specify)
nmlkj
Please specify if you checked "agency other than what's listed here"
DHHRProsecuting
Attorney's Office
Child Advocacy
CenterI don't know
An agency other
than what's listed
here (please specify
below)
Responsible for
Schedulingnmlkj nmlkj nmlkj nmlkj nmlkj
Responsible for Notifying nmlkj nmlkj nmlkj nmlkj nmlkj
Yes
No nmlkjnmlkj
If you checked No, could you elablorate?

Page 7
2008 West Virginia MDT Survey - Attorney Version23. We understand MDT meetings vary in length. Considering all the MDTs in which you participated last year:How many minutes long was the the shortest MDT session?
How many minutes long was the longest MDT session?
How many minutes long was the average or typical MDT session?

Page 8
2008 West Virginia MDT Survey - Attorney Version
5. Perception of MDT Processes - Treatment Effectiveness
We would like to ask you some questions concerning your experiences as a participant in Child Abuse and Neglect treatment MDTs. For each of the following questions, please think about the MDT sessions that you attended over the past year (since February of 2007).
24. The following questions are concerned with how well multidisciplinary treatment teams implement treatment objectives. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the multidisciplinary team accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
Develop individualized
service plans for the
children and families?
nmlkj nmlkj nmlkj nmlkj
Base treatment planning
on comprehensive
assessments of children
and families?
nmlkj nmlkj nmlkj nmlkj
Coordinate treatment
plans for the child with
resources available in the
community?
nmlkj nmlkj nmlkj nmlkj
Coordinate treatment
plans for the family with
resources available in the
community?
nmlkj nmlkj nmlkj nmlkj

Page 9
2008 West Virginia MDT Survey - Attorney Version
6. Perception of MDT Processes - Frequency & Duration
25. The next group of questions are concerned with the frequency, duration, and location of MDT meetings in abuse and neglect cases. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the MDT accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
MDT sessions occur
frequently enough to
aide in designing,
implementing, and
monitoring treatment
plans.
nmlkj nmlkj nmlkj nmlkj
MDT sessions last long
enough to adequately
address the needs of the
case.
nmlkj nmlkj nmlkj nmlkj
MDT sessions are
scheduled at times that
are convenient for me to
attend.
nmlkj nmlkj nmlkj nmlkj
MDT sessions are
scheduled in places that
are convenient for me to
attend.
nmlkj nmlkj nmlkj nmlkj

Page 10
2008 West Virginia MDT Survey - Attorney Version
7. Perception of Multidisciplinary Team Processes - Responsiveness
We would like to ask you some questions concerning your experiences as a participant in MDT proceedings. For each of the following questions, please think about the MDT sessions that you attended over the past year (since February of 2007).
26. The next group of questions are concerned with the extent to which MDTs are sensitive to the needs and/or concerns of their constituent members. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the multidisciplinary team accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
The MDT process is
sensitive to the needs
and/or concerns of the
child(ren).
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of the
adult respondents
(usually the parents).
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of co-
petitioners or intervenors.
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of DHHR
caseworkers.
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of the
Legal counsel for the
Children.
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of the
Legal counsel for the
adult respondent(s).
nmlkj nmlkj nmlkj nmlkj
The MDT process is
sensitive to the needs
and/or concerns of the
prosecutor.
nmlkj nmlkj nmlkj nmlkj

Page 11
2008 West Virginia MDT Survey - Attorney Version27. Are there parties, other than those listed above, involved in the MDT meetings, who are affected by the MDT process? If so, who are they and how are they affected?

Page 12
2008 West Virginia MDT Survey - Attorney Version
8. Perception of MDT Processes - Consensus & Outcomes
We would like to ask you some questions concerning your experiences as a participant in MDT proceedings. For each of the following questions, please think about the MDT sessions that you attended over the past year (since February of 2007).
28. The questions that follow concern the extent to which MDTs yield agreement and consensus. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the multidisciplinary team accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
The members of the
multidisciplinary team are
able to come to a
consensus concerning the
treatment plan for
particular cases.
nmlkj nmlkj nmlkj nmlkj
The multidisciplinary
team is able to formulate
recommendations to the
court that reflect member
consensus.
nmlkj nmlkj nmlkj nmlkj
The multidisciplinary
team generates an
official report
communicating
recommendations to the
court.
nmlkj nmlkj nmlkj nmlkj
Recommendations that
come from the
multidisciplinary team
reflect the full range of
members' opinions
concerning the case.
nmlkj nmlkj nmlkj nmlkj

Page 13
2008 West Virginia MDT Survey - Attorney Version
9. Perception of MDT Processes - Implications for Policy
We would like to ask you some questions concerning your experiences as a participant in MDT proceedings. For each of the following questions, please think about the MDT sessions that you attended over the past year (since February of 2007).
29. The next group of questions are concerned with the extent to which multidisciplinary treatment team proceedings achieve the ideal goals as set by state policy. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how often the multidisciplinary team accomplished each of the following:
Never or almost never Occasionally Much of the time Always or almost always
Multidisciplinary team
practices contribute to the
overall goal of making
reasonable efforts to
preserve or reunify
families.
nmlkj nmlkj nmlkj nmlkj
Multidisciplinary team
practices contribute to the
overall goal of
maximizing the safety of
children.
nmlkj nmlkj nmlkj nmlkj
Multidisciplinary team
practices contribute to the
overall goal of achieving
permanency for children
in a timely manner.
nmlkj nmlkj nmlkj nmlkj

Page 14
2008 West Virginia MDT Survey - Attorney Version
10. Constitution of Multidisciplinary Teams
A diverse pool of people are involved in West Virginia Multidisciplinary Teams. Your answers to the following series of questions will help us better understand who participates in MDTs and in what capacity.
30. The next group of questions are concerned with the constitution or makeup of multidisciplinary treatment teams. Please base your answers to these questions on your experience as a participant in MDTs over the past year (since February 1, 2007).
For each question, please tell us how frequently each of the following participants attended MDT meetings.
Which parties fall under other?
Never or almost never Occasionally Much of the time Always or almost always
DHHR Caseworker nmlkj nmlkj nmlkj nmlkj
DHHR Supervisor nmlkj nmlkj nmlkj nmlkj
Prosecuting Attorney nmlkj nmlkj nmlkj nmlkjAttorney for Adult
Respondent (often the
Parent)
nmlkj nmlkj nmlkj nmlkj
Attorney for the Child or
Childrennmlkj nmlkj nmlkj nmlkj
The Child or Children nmlkj nmlkj nmlkj nmlkjAdult Respondent (often
the Parent)nmlkj nmlkj nmlkj nmlkj
Foster Care Provider nmlkj nmlkj nmlkj nmlkjCourt Appointed Special
Advocatenmlkj nmlkj nmlkj nmlkj
Child Advocacy Center
Personnelnmlkj nmlkj nmlkj nmlkj
Representatives from
Contracting or Fee-For-
Service Providers
(Homebase, Parenting
Instruction, etc)
nmlkj nmlkj nmlkj nmlkj
Representatives from
Behavioral Healthcare
Providers (Counselors,
Psychologists, etc)
nmlkj nmlkj nmlkj nmlkj
Representatives from the
Schoolsnmlkj nmlkj nmlkj nmlkj
Other parties not listed
above (such as Co-
Petioners or Intervenors)
please describe in the
comment box below
nmlkj nmlkj nmlkj nmlkj

Page 15
2008 West Virginia MDT Survey - Attorney Version
11. Member Contributions to MDT Processes
31. Other studies of MDTs have shown that member participation, engagement, or involvement, varies from extremely passive to extremely active. Thinking about your experiences in MDTs over the past year (since February of 2007), please rate the typical involvement of the following people. If a person listed does not routinely participate in MDT meetings in your county, please check "never or almost never present."
If you rated the "other" category, please describe
Never or almost never
present Extremely Passive
Balanced between
Passive and ActiveExtremely Active
DHHR Caseworker nmlkj nmlkj nmlkj nmlkj
DHHR Supervisor nmlkj nmlkj nmlkj nmlkj
Prosecuting Attorney nmlkj nmlkj nmlkj nmlkjAttorney for Adult
Respondent (often the
parent)
nmlkj nmlkj nmlkj nmlkj
Attorney for the Child or
Childrennmlkj nmlkj nmlkj nmlkj
The Child or Children nmlkj nmlkj nmlkj nmlkjAdult Respondent (often
the parent)nmlkj nmlkj nmlkj nmlkj
Foster care provider nmlkj nmlkj nmlkj nmlkjCourt Appointed Special
Advocatenmlkj nmlkj nmlkj nmlkj
Child Advocacy Center
Personnelnmlkj nmlkj nmlkj nmlkj
Representatives from
contracting or fee-for-
service providers
(Homebase, Parenting
Instruction, etc)
nmlkj nmlkj nmlkj nmlkj
Representatives from
behavioral health care
providers (Counselors,
Psychologists, etc)
nmlkj nmlkj nmlkj nmlkj
Representative from the
Schoolsnmlkj nmlkj nmlkj nmlkj
Other parties not listed
above (such as co-
petioners or intervenors)
please describe in the
comment box below
nmlkj nmlkj nmlkj nmlkj

Page 16
2008 West Virginia MDT Survey - Attorney Version
12. Open ended Questions
In this survey, we have asked you several questions concerning the processes and procedures of West Virginia Multidisciplinary Teams. Now we would like to give you the opportunity to tell us what you think is most important and offer us recommendations for improving policies and procedures.
32. What should MDTs accomplish?
33. Can you offer any suggestions on how the Multidisciplinary Team process could be improved?
34. Some critics argue that our current MDT process fails to involve key participants who would contribute positively to the MDT. In your opinion, who else should be involved in MDTs?

Page 17
2008 West Virginia MDT Survey - Attorney Version35. Finally, is there anything else about MDTs that you think is important for us to know, or that you would like to share?

Multidisciplinary Teams in West Virginia Page | 92
Appendix!E:!Interim!Report!on!Phase!I!Activities!

d"%#&%*4./,"'$.e.f.g0)h,$.h*.ij+'0.k.f($%l%$%0'.%*.$j0.mnno.p.mnnq.20'$.3%,4%*%+.!"#$%&%'(%)#%*+,-./0+1.r$"&-.
Interim Report Prepared for the West Virginia Court Improvement Program
Corey J. Colyer, PhD – Principal Investigator L. Christopher Plein, PhD – Co investigator
School of Applied Social Sciences
West Virginia University Morgantown, WV 26506-6326
5/2/2008

!
TABLE!OF!CONTENTS!Executive Summary ............................................................................................................. 1!
Introduction ........................................................................................................................ 3!
The!Scope!of!the!Study!.............................................................................................................................!3!
Methodology!&!Approach!........................................................................................................................!5!
The!Sample!............................................................................................................................................!6!
Observation!Procedures!.......................................................................................................................!8!
Findings from Phase I ......................................................................................................... 9!
Dimensions!of!Similarity!.........................................................................................................................!10!
MDTs!Evolve!........................................................................................................................................!10!
Many!MDTs!do!not!Reach!Consensus!.................................................................................................!15!
Maximizing!Participation!is!Challenging!.............................................................................................!17!
Dimensions!of!Difference!........................................................................................................................!18!
Variations!in!Institutional!Control!.......................................................................................................!18!
Variations!in!Formality!........................................................................................................................!21!
Four!Ideal!Types!of!MDTs!...................................................................................................................!23!
Variations!in!Constitution!&!Facilitation!.............................................................................................!25!
Discussion and Implications ............................................................................................. 31!
The!Case!for!an!Evolving!MDT!Structure!................................................................................................!32!
Circuit!Courts!should!reinforce!MDT!importance!...................................................................................!33!
Each!Jurisdiction!Should!Consider!a!Neutral!Facilitation!Model!............................................................!34!
Next Steps .......................................................................................................................... 35!
Appendix A – Administrative order .................................................................................. 36!
Appendix B – Letter to MDT Participants ........................................................................ 38!

Page | 1
EXECUTIVE!SUMMARY!
This document reports on evaluation activities undertaken in Phase I of the 2007
– 2008 West Virginia Multidisciplinary Team study. This project was commissioned by
the West Virginia Court Improvement Program to examine and document variation in
processes and procedures implemented in treatment MDTs across the state. In this
report, we identify our methodological approach and identify preliminary findings.
We observed approximately 25 MDT meetings in 9 counties distributed across
West Virginia. These ethnographic observations focused on the practices and
procedures utilized by MDTs allowing us to identify the ways in which each county is
similar to and different from others. From these observations we draw the following
preliminary findings
First, we found that some practices, procedures, and issues are consistent from
one location to the next. These involve the evolution or progression of MDT group
dynamics over the life course of the team; general lack of unanimity or consensus in
MDT outcomes; and difficulties in maximizing participation of all appropriate
contributors.
Second, we found important differences among the MDTs that vary from one
location to the next. These observations include: the relative influence of contributing
institutions, such as DHHR1 and the court system vary on a county-to-county basis;
personnel who participate as team members differ by location; and practices or
1 The Department for Health and Human Resources is a large state agency. We recognize that a particular branch of DHHR, the Bureau for Children and Families (BCF), is responsible for abuse and neglect matters. However in this report will refer to BCF personnel as DHHR or “the Department” which is consistent with the ways in which attorneys and others referred to State social services.

Page | 2
procedures for implementing and facilitating MDT meetings reflect local arrangements
or cultures.
Based on these preliminary findings, we offer three recommendations for the
Court Improvement Program’s consideration. These recommendations include: (1)
consider developing a dynamic MDT structure that changes according to the
circumstances characteristic of a case’s evolution; (2) encourage circuit courts to
emphasize the value and importance of MDTs and implement scheduling strategies that
reinforce this priority; and (3) develop statewide guidelines for MDT facilitation to
include oversight by a neutral facilitator.
These preliminary findings from Phase I will be refined through the analysis of
survey data in Phase II. These data have been collected and we are in the process of
analysis. The expected completion date of our Phase II analysis is May 30th, 2008.

Page | 3
INTRODUCTION!
West Virginia State law (§49-5D-3) requires that each county establish
multidisciplinary teams (MDTs) to assist the courts and the Department of Health and
Human Services (DHHR) in child abuse and neglect proceedings2:
It is the further purpose of this article to establish, as a complement to other programs of the department of health and human resources, a multidisciplinary screening, advisory and planning system to assist courts in facilitating permanency planning, following the initiation of judicial proceedings, to recommend alternatives and to coordinate evaluations and in-community services.
State law further differentiates between investigative (§49-5D-2) and treatment
(§49-5D-3) MDTs. Investigatory MDTs are responsible for coordinating investigations
and making recommendations to the prosecuting attorney concerning “all civil and
criminal allegations pertinent to cases involving child sexual assault, child sexual abuse,
child abuse and neglect.” In contrast treatment MDTs are responsible for coordinating
treatment plans and service delivery for children and families involved in abuse and
neglect cases. The treatment MDT advises the court on treatment and placement
recommendations and then continues to monitor ongoing treatment delivery. This
study focuses on treatment MDTs.
The!Scope!of!the!Study!
This project was commissioned by the West Virginia Court Improvement
Program to examine and document variation in treatment MDT processes across the 2 Similar MDTs are statutorily mandated by this chapter of the code for children under going status offense and delinquency proceedings. Such “youth-services” MDTs were excluded from the focus of this study.

Page | 4
state. Anecdotal reports have long suggested that MDT practices and procedures vary
across the State. This study was designed to empirically assess the extent to which
treatment MDT practices vary, and identify the dimensions of this variation.
According to state law (§49-5D-3) multidisciplinary treatment teams should be
convened and directed by the DHHR case manager (either for the child or the family)
and consist of the following parties:
! The child, when deemed appropriate.3
! The Child’s custodial parent or parents, guardian or guardians, and
other immediate family members
! Legal counsel for the child and counsel for parents , guardians and any
intervening parties
! The prosecuting attorney (or a designated representative of the same).
! When appropriate and available, a court appointed special advocate
(CASA), a member of the child advocacy center, appropriate school
officials and “any other person or an agency representative who may
assist in providing recommendations for the particular needs of the
child and family.”
Other than directing the case manager to convene the MDT, that State law lacks
explicit guidance concerning the expected relationships between these participants.
Theoretically, each member of the MDT should be an equal contributor. However
studies in the sociology of small groups suggest that normal group dynamics create
divisions which can be magnified over time. The list of potential MDT participants
3 “The child may participate in multidisciplinary treatment team meetings if such is deemed appropriate by the multidisciplinary treatment team.”

Page | 5
brings together a diverse group of people representing different organizations and
institutions. Thus, the first objective in this study was to map participation patterns and
document group dynamics. Specifically, who participates in West Virginia MDTs and in
what capacity?
The second objective in this study was to examine variation in MDT procedures.
We note that other than the expectation that MDTs provide explicit recommendations to
the court, state law and policy is largely silent on MDT procedure. The Department of
Health and Human Resources (DHHR) has developed a protocol which they distribute
through training to personnel in the Bureau for Children and Families (BCF), but it is
unclear to the extent that this protocol is uniformly followed. Thus, the second objective
of this research study was to identify variations in MDT protocol and procedures.
Specifically, how are West Virginia MDTs organized and implemented?
Methodology!&!Approach!
Given the lack of concrete knowledge concerning the extent to which MDT
participation and practices vary, we first gathered data through observation and
informal conversation. Ethnographic methods involving direct observation allow the
researcher to observe group process as it implemented.4 By using an exploratory or
inductive approach, this method avoids preconceptions. Such preconceptions can lead
the researcher to prematurely restrict inquiry and prevent consideration of the full
range of experience and information.
4 Of course, the presence of strangers does alter group dynamics. Our presence at MDT sessions undoubtedly created reactive effects. Yet, as tool for identifying social processes in complex situations, ethnographic methods are superior to the alternatives of surveys, experiments, and interviews. We have no reason to believe that our presence observing MDTs radically changed the group’s procedures or outcomes.

Page | 6
The!Sample!
We initially proposed to observe MDT proceedings in 15 West Virginia counties,
strategically selected to maximize diversity in terms of geography, population density,
and known variations in MDT procedures. We selected at least two counties from each
of DHHR’s four administrative reasons. Once the counties were selected, we requested
an administrative order from the Circuit Court of that county, granting the research
team access to observe the sessions (see Appendix A).5 Once legal access was granted
through the administrative order, we contacted the DHHR Community Services
Manager (CSM) for the selected county and asked for their assistance in identifying
MDTs for us to observe. Typically, the CSM referred us to a child protective services
supervisor, or a social services coordinator, who helped us schedule observation
sessions and distributed a letter to participants which explained the study (see Appendix
B).6 Of the original 15 counties, we completed observation in nine. Of the six counties
where no observation was made, we were unable to secure administrative orders in
three and experienced scheduling conflicts in the other three. The list of counties is
presented in Figure 1 below.
5 Teresa Lyons of Byrne Hedges and Lyons in Morgantown prepared these orders and access. 6 In the counties where observations were conducted, the DHHR staff was gracious and accommodating. We would like to formally thank them for their efforts.

Figure!1
W
dispropo
Schedul
Norther
West Vir
Kanawh
August w
arrived a
to obser
D
still anal
1:!Counties
We note tha
ortionately
ing conflict
rn panhandl
rginia (Rale
ha counties
when sched
and therefo
rve MDTs in
Despite the p
lytically use
!in!the!Obs
at counties i
represente
ts prevented
les (Berkele
eigh). Whil
(South Cen
duling was d
ore we mad
n the remai
prepondera
eful. We ob
Compl
MonoMaHar
Lewis,!Ran
WoodMcD
servation!Sa
in the North
ed in the ob
d us from a
ey and Ohio
le we did ev
ntral region
difficult. A
e no attemp
ining count
ance of Nor
bserved MD
leted
ongalia,!arion,!rrison
Braxton,!ndolph
d,!Cabel,!Dowell
ample!Fram
h Central re
servation s
attending M
o Counties)
ventually re
n), these ord
A judicial ord
pt to schedu
ies where w
rth Central
DTs in some
Ob
me!
egion of the
ample. Thi
MDT session
) as well as
eceive judic
ders did not
der from M
ule observa
we have jud
counties, th
e of the mo
No!bservat
BerkeleO
(Scheduli
Clay,!Kan
(ProblemO
e state are
is was not i
ns in the Ea
in part of s
cial orders f
t arrive unt
Mingo Count
ation there.
dicial orders
his observa
st rural and
tion
ey,!RaleighOhio
ing!Conflic
nawha,!Min
ms!with!JudOrders)
Pag
intentional.
astern and
outh easter
for Clay and
til the end o
ty never
We still pl
s.
ation sampl
d densely
,!
ts)
ngo
icial!
ge | 7
.
rn
d
of
lan
e is

Page | 8
populated counties in the State concerning cases at the beginning, the middle, and the
end of their formal proceedings. Moreover, we observed considerable and consistent
variation in practices and procedures from one county to the next, even in adjacent
counties in the same DHHR region. Therefore, while we cannot claim that our
observations are truly representative of all MDTs in West Virginia, we believe we
observed a sufficient range and variety of MDT practices to draw meaningful
conclusions.
Observation!Procedures!
We attempted to schedule observation on days when it would be possible to
observe several MDT sessions. Upon setting the date, we asked DHHR personnel to
circulate a letter to the legal counsel for all involved parties, indicating that we planned
to observe their MDT session. This letter explained the purpose of our research project,
provided our contact information for clarifications7, and offered assurance that we
would not observe the session if their client objected to our presence. The text of this
letter is provided in Appendix B. To our knowledge, only one attorney raised questions
about our project and no one refused our presence.
On the date of the observation, the principal investigator (Colyer) traveled to the
MDT meeting site and passively observed the procedures. At the start of the meeting, he
was introduced by the leader as a researcher conducting a study on MDT procedures for
the Supreme Court and that he would respect the participant’s privacy and
confidentiality in his report. He sat at the table with the participants and took notes on
7 Teresa Lyons of Byrne Hedges and Lyons, Morgantown, was also listed as a contact on behalf of the Court Improvement Program.

Page | 9
a laptop computer. In nearly every county he signed the meeting attendance form
indicating that he was present.
We observed the proceedings from the standpoint of a neutral observer and
purposefully asked that we not be briefed on the case particulars before the meeting.
Our observation focused exclusively on procedures and dynamics, rather than case
specifics. However, where case background was formally addressed in the meeting, our
notes do reflect these specifics, particularly when they appear to illustrate some broader
process or procedure. Indeed, we draw on these examples in our analysis to follow. In
particular we paid attention the procedural structure of the meeting, general group
dynamics, and how conflict was mediated or consensus achieved.8
Whenever possible, following the MDT session, we informally interviewed the
participants. Some of the richest data we collected came from these conversations
where the participants expressed their thoughts pertaining to what had just happened.
While these interviews were not tape recorded or preserved, we did attempt to capture
detailed notes about these conversations as soon after the conversation as possible.
Taken together, these observations and conversations constitute a rich database for an
exploratory analysis of MDT practices and procedures in West Virginia. In the
remainder of this report, we identify the core themes that emerged from our analysis.
FINDINGS!FROM!PHASE!I!
We offer two clusters of findings from the observational phase of this study. The
first cluster concerns observations of practices, procedures, and issues that were similar
or consistent across the counties we visited in the summer and fall of 2007. These
8 We have altered some details to protect participants from indirect disclosure of their identity.

Page | 10
consistent patterns include: (1) evolution in MDT group dynamics over the life course of
cases; (2) general lack of unanimity or consensus in MDT outcomes; and (3) challenges
in maximizing participation. The second cluster focuses on core dimensions of
difference, or axes of variation. These include: (1) variation in the influence of
contributing institutions; (2) variety in the personnel who participate and comprise
MDTs; and (3) diversity in the practices and procedures implemented to facilitate and
complete MDT sessions. Readers are reminded that these observations are preliminary
and we will seek to confirm and elaborate upon them in Phase II of the research.
Dimensions!of!Similarity!
We begin our presentation of findings by cataloging the observations that
appeared to be consistent from one county to the next. As summarized above and
detailed below, these observations point to common realities and challenges facing
MDTs as they seek to work in the best interest of children and families. We address
each of the dimensions of similarity in turn.
MDTs!Evolve!!
The dynamics of an MDT fluctuate depending on the location of the case in its life
course. This is to be expected. Sociologists who study small groups have consistently
demonstrated that group dynamics evolve and change over time. Our observations
indicate that in the early stages of their process, MDTs are marked by caution and lack
of trust between different types participants. In these early sessions, the adult
respondent and their counsel can be less open and amenable to suggestions coming
from caseworker, the prosecutor’s office, or other perceived agents of the state. In
comparison, trust between these parties grows over time. Many MDT participants

Page | 11
identified rapport building as one of the most important early goals in their process. As
one prosecutor explained,
These meetings help parents see this as a collaborative process, rather than an adversarial hearing. Things go wrong and we address them. When we do this, the parent can see that we’re trying to work with them and not against them. 9
This prosecutor recognizes that in abuse and neglect cases many parties enter the
MDT process distrustful and with caution. The team must actively work to build trust.
Adult respondents have good reasons to be suspicious of the initial MDT meetings.
After all few enter this process voluntarily. Many begin the process with a mindset that
DHHR has taken (or wants to take) their children and therefore they participate under
duress. The team must convince these parents that they are, in fact, all on the same
team. This is a difficult message to communicate, particularly in the early stages of the
process. Our observation of early-stage cases suggests that many adult respondents
distrust the other members of the MDT.
We observed an initial MDT where the infant child was in state custody because
the parent, who had been diagnosed with mental illness, allegedly threatened to kill
herself and her baby. The prosecutor (who runs the MDT meetings in this county)
began this meeting indicating that the team’s goal was to work toward reunification of
the mother and child and then proceeded to review the case history and the judge’s
orders for supervised visitation. Within the first few minutes of the meeting, the parent
began arguing that the allegations were untrue. “I would never hurt my baby and I
never said that. That someone said I would is a lie and I won’t sit here and let you
9 Note, all dialog and quotes included in this report were reconstructed from the Principal Investigator’s field notes. These statements and accounts were not tape recorded or otherwise captured verbatim. Thus, while we have made every effort to accurately reproduce the speaker’s words, our reproductions should not be mistaken to be word-for-word quotes.

Page | 12
accuse me of doing something I didn’t do!” For the next several minutes, the focus of
the MDT meeting was on trying to convince this woman that these points had already
been settled in court. But she became increasingly upset, accusing the group of trying to
take her child even though her DHHR caseworker reported reunification to be the goal
of the treatment plan. By this point, any discussion of treatment plans and long term
goals were clearly counterproductive.
In this case, it’s doubtful that anything the team might do or say will convince the
parent that they are working with her, let alone communicate to her that everyone is on
the same team. Her behavior suggests that she did not differentiate the MDT from an
adversarial courtroom. This makes sense. Until this point, the majority of her
interactions with DHHR and the court had been adversarial. The State of West Virginia
had filed a petition for emergency custody of her child. They presented evidence in a
court of law which her attorney attempted to rebut in an adversarial fashion. At the end
of that proceeding, the judge ruled in favor of the State’s position and against hers. In
short, at the time of this MDT, there had yet to be an opportunity to her to experience
the child welfare process as collaborative. Likewise, the DHHR personnel, prosecutor,
counselors, and other participants in the MDT, at this point in the process, have little
reason to trust the respondent or to believe she tells the truth. There is no history
establishing a common bond. Our observations from cases farther along in their MDT
life course suggest that, when the process works, trust is built in both directions.
In contrast, we attended another MDT that was held just a week prior to the
case’s closure. The discussion in this session centered on ensuring continuation of
services. The family’s caseworker indicated that the department would keep their case
open for an additional 90 days to so that they could monitor and assist the family during

Page | 13
transition. The child in this case had a history of behavioral problems and one of the
parents expressed concerns that he could become unmanageable. The caseworker told
them, “We are going to help you connect with some other community services. Once
those relationships are in place, you can call them directly. You won’t need us to be
involved.” The parent then asked about continuing medical services and testing. The
guardian ad litem replied, “Make a list of the medical services and tests for me and I’ll
see that they are addressed in turn. I want you to know how I proud I am of the
progress that you have made with your son.”
While neither of these cases may be depicted as typical, they illustrate important
differences between early MDTs and late MDTs. In the early MDT, the parent viewed
the others in the room with fear and distrust. In the later MDT, the parent viewed the
others in the room as resources to be trusted. Though neither of the above cases should
be considered to be typical, they vividly illustrate the ways in which MDTs change over
time. Considering all of the MDTs we observed, group dynamics in early MDTs were
clearly different from those in later phases. Figure 2 offers a hypothetical and idealized
model for a case’s progression through the MDT process.

Figure!2
T
adversar
may be n
as the te
teamma
adversar
and the
W
approxim
progress
collabor
life cour
practice
2:!Idealized
This model r
rial process
necessary t
eam works t
ates builds t
rial. By the
team shoul
We find limi
mates this m
ses along th
ration from
rse. Moreov
s (see below
•Adversarial•Low!Trust•Reliance!onprocedure
Init
d!MDT!Prog
recognizes t
s. In these e
o rely on m
together th
trust, leadin
e end of the
ld be charac
ited eviden
model. How
his continuu
the onset, w
ver, county
w) may play
!formal!
tial!Stage
gression!ov
that child a
early phase
more formal
rough the i
ng to dynam
e process, th
cterized by
ce in our ob
wever, we c
um. Some
while other
y specific pr
y a role in s
•Progadve•Mo•Less•Incr
ver!the!Life
abuse and n
es of the MD
ized proced
mproveme
mics that ar
he need for
high conse
bservationa
certainly do
MDTs are c
rs fail to cul
rocedural an
shaping a ca
gressively!lesersarialre!trusts!formalreasing!conse
IntermeStage
e!Course!
neglect case
DT, where t
dures than i
nt period, t
re at once m
formalized
ensus and h
al sample th
o not claim
characterize
ltivate thes
nd instituti
ase’s progre
ss!
ensus
ediate!e(s)
es emerge fr
trust is pote
in later pha
the good fai
more collabo
d procedure
high trust.
hat case pro
that every M
ed by high t
e qualities o
onal influen
ession. Stil
•High!Con•High!Tru
Page
rom an
entially low
ases. Howe
ith effort of
orative and
es is minimi
ogression
MDT
trust and
over the ca
nces on MD
ll, we believ
nsensusst
End!Stage
e | 14
w, it
ever
f the
d less
ized
se
DT
ve
e

Page | 15
this model presents a functional roadmap for MDT participants concerning expected
team development.
Many!MDTs!do!not!Reach!Consensus!
While dissent is easy to identify, it is difficult to observe consensus. We actively
looked for evidence of consensus and dissent in MDT meetings. Consensus was most
clearly visible in MDTs that were nearing the end of the formal proceedings where the
parent(s) were preparing to regain custody and/or end supervision. But, it was much
more difficult to infer consensus in the large majority of cases where the outcome of the
case was still in question. In some cases, members of the team openly quarreled,
reflecting institutionalized positions however such disagreements were often not
brought to the surface in the MDT meeting.
For instance, we observed an argument after an MDT where there had been no
indication of disagreement during the meeting proper, while the parents were in the
room. This MDT was for a case was about halfway through its improvement period. Up
to this point, both parents (who were separated) had been compliant with the terms of
the family treatment plan, though the professional members of the MDT were
concerned that neither was progressing adequately to regain custody of their children.
Once the parents left, the prosecutor expressed frustration about this lack of progress.
Prosecutor: I just don’t know what we’re going to do in this case. Neither is progressing.
Counsel for Mother: What exactly is in the best interest of this child? The dad is never going to get custody; we all know this! It seems to me that there’s an element of bad faith in all this. Why even string him along suggesting that this is a possibility?
Prosecutor: The judge granted an improvement period and we are following it.

Page | 16
Counsel for Mother: I want to reunify the family, or at least preserve my client’s parental rights. It looks to me like visitation is going well and she’s doing what she’s been asked to do. She wants her children back. Is this real abuse & neglect, or is this a social engineering exercise where we are trying to find better homes for these kids?
Prosecutor: Well, what else do you want us to do to support your client? She just had her electricity turned of because she forgot to pay the bill. Her finances are a mess; housing is always going to be an issue with her. This is a woman who’s not ready to have a credit card, but you think she’s ready to raise kids?
This exchange highlights disagreements which are fundamentally anchored to
institutionalized positions of advocacy and professional orientations. The MDT
participants, in this case, a caseworker from DHHR, the prosecutor, the mother’s
attorney, and a court appointed special advocate (CASA), each represent a different
institutional organization, with its own purpose and mission. While all parties may
agree to work together “in the best interest of the child,” that does not necessarily imply
that everyone defines this interest in the same way. After the exchange, when the
attorney had left, the CASA volunteer expressed frustration to us, “honestly… it’s the
lawyers who create the biggest difficulty in the MDT process.” From his point of view, in
this case, reunification of this family will not be in the best interest of the child(ren) and
the attorney’s insistence that the mother’s parental rights be restored is ultimately
counterproductive. In contrast, we heard similar complaints from attorneys concerning
overzealous CASA volunteers and DHHR caseworkers. They have been appointed to
guard the respondent’s due process rights and had not seen evidence that termination of
parental rights is in the child’s best interest. Which of these positions will be
communicated to the Judge? It’s hard to say.
The case presented above is useful because these disagreement and conflict
publicly emerged, making it observable. However, in the vast majority of cases, it was

Page | 17
difficult to explicitly identify indicators of disagreements. We cannot conclude that the
absence of vocal dissent in the MDT proper is indication of consensus. On the contrary,
the institutionalized roles performed by MDT members would seem to ensure
disagreement in cases that are not progressing according to plan. To the extent that
Multidisciplinary teams are designed to unite professionals from a variety of
backgrounds in the common pursuit of the child’s best interest, we believe more data is
necessary. We will explore this finding further in the Phase II Survey.
Maximizing!Participation!is!Challenging!
Participation in MDT session is universally uneven. The barriers to participation
fall into two categories. First, scheduling conflicts often prevent team members from
attending the MDT session. Second, in some counties, certain team members play a
much less significant role in the MDT deliberations than others.
Scheduling conflicts appear to be universal challenges to West Virginia MDTs,
particularly for attorneys representing the children or adult respondents. Many of these
attorneys manage busy caseloads, representing clients in multiple counties. They often
experience scheduling conflicts where they are expected to represent one client in
motions or a hearing and another in an MDT. When this happens, attorneys tell us, the
MDT becomes a lower priority.
Some counties have addressed this problem by scheduling dedicated MDT days.
They attempt to only schedule MDTs on these days and work with the circuit court to
minimize scheduling conflicts. Our observations suggest that attorney participation is
greatest in these counties. We will explicitly attempt to measure this observation in the

Page | 18
Phase II survey. However, even in these counties, scheduling conflicts complicate the
MDT process.
Prosecutor participation is also uneven across the state. In fact, we conducted
more than a third of our observations before encountering a prosecutor participating in
a MDT. In most of the counties where no prosecutor was present, one or more
participants called our attention to their absence. One attorney said, “I hope you
noticed that there’s no one from the prosecutor’s office here.”
Dimensions!of!Difference!
We quickly identified aspects of MDT practice that vary from one location to the
next. Certainly, every MDT has distinct characteristics based on the specific
circumstances surrounding particular cases. However, MDT meetings reflect local
conditions, norms, patterns, and processes. These localized elements of MDT practice
translate into observable dimensions of difference on a county-to-county basis. We
observed three core dimensions of difference between the observation sites. These
dimensions include institutional participation, formality, and constitution or makeup.
We describe each in turn below.
Variations!in!Institutional!Control!
Multidisciplinary teams appear to be multidisciplinary in name only. A more
accurate term to describe what we observed would be “bi-disciplinary.” One of two
institutions (the circuit court under the auspices of the prosecutor’s office or the
department for health and human resources) control the dynamics and direction of
MDT meetings. These institutions reflect two professions (social services and the law).
Other constituent members, including lawyers for participants, Court Appointed Special

Page | 19
Advocates, Child Advocacy Center personnel, contract service providers, all fall under
these two disciplines. Moreover, their participation in the MDT reflects a secondary or
supportive role. The dominant institution (DHHR or the Court) sets the meeting’s
agenda and guides the process in ways that reflect its disciplinary leaning.
In court-dominated MDTs, the prosecutor’s office runs the meeting and sets the
agenda. In the court-dominated meetings that we observed, the agenda appeared to
focus on timelines and compliance with the terms set forth in the court order(s) more so
than on treatment planning and progress. While treatment plans were discussed, these
discussions were often couched within the context of pending court hearings. 10 One
prosecutor described the purpose of the MDT to be a pre-trial hearing. “There should be
no surprises when this case appears before the judge. We are getting our ducks in a row
and clarifying the issues in advance.” Thus, in this prosecutor’s eyes, the purpose of the
MDT is to serve the circuit court. The following example from our field notes illustrates
a typical court-oriented MDT:
DHHR Caseworker: We made arrangements to start counseling with [a local provider] but [the adult respondent] didn’t go back to them when it was scheduled to begin.
Respondent: My phone has been turned off.
Caseworker: It’s been over a month now and they need to complete your intake testing. We also need to complete the MMPI (a personality inventory). We can’t start the program until we do this. This is important, the Judge expects you to follow through!
Attorney: May I remind everyone that the Department has not filed its treatment plan yet. Therefore, everything that she’s done has been voluntary and I would think the Judge would be happy with that.
10 To be clear, this is not to say that court-oriented MDTs ignored treatment plans or progress. Rather, these concerns took subordinate position to concerns of the pending court hearing(s).

Page | 20
Caseworker: Yes, that’s true about the treatment plan. But her voluntary performance is an indicator of things to come.
The emphasis in this discussion was on compliance with court ordered directives.
It’s instructive to note that the while the department’s caseworker was reviewing the
respondent’s failure to live up to a treatment plan, the respondent’s attorney argued that
this treatment plan does not formally exist. The implication is that the treatment plan
must be formalized and recognized by the court before the team may draw inferences
about the respondent’s performance in relation to it.
In contrast, department-driven MDTs focused on progress reports from the
treatment oriented interventions prescribed for improvement. The team discussions
alternated between sharing of information and reviewing progress on the treatment
plan’s objectives. The following excerpt from our fieldnotes typify a department
oriented MDT.
The caseworker passed out notes from the counseling provider. They indicate that the respondents are doing well in therapy (both couples and individual). Then she informed the other MDT members that the father’s paternity tests are in and he has been confirmed as the child’s father. She was unsure what to do next because the child’s birth certificate lists a different father. One of the attorneys said that this problem could easily be resolved with a Judge’s order and that she’d take care of that. Then, a representative from the agency that provides parenting instruction reported that the couple completed the curriculum and has done well under supervised visitation. They recommend starting unsupervised visitation in the home. The CPS supervisor told the couple that they are doing well and everything was on track for reunification.
In this MDT the court was not mentioned at all. While a prosecutor was present,
he did not actively participate in the discussions. The focus of the meeting was placed
on the couple, their progress in court-mandated programs, and how they might resolve
the administrative inconvenience of getting a birth certificate record corrected. In

Page | 21
contrast to the court-oriented example, this MDT was clearly responsive to the dynamics
of the improvement period.
Variations!in!Formality!
MDT proceedings vary along a dimension of formality. More formal MDTs follow
relatively rigid procedures and protocols, while less formal MDTs maximize flexibility in
the meeting format to be responsive to unexpected developments.11 The following
examples from our field notes illustrate some key differences between a more formal
MDT as compared to a less formal MDT. Both the MDTs described below were
conducted in the same week and in the same region of West Virginia, however they were
in different counties.
Table!1:!Illustration!of!Formality!from!the!field!notes!
More Formal MDT Less Formal MDT
The prosecutor initiated the meeting. She announced, “we are in a post adjudicatory improvement period and our task is to make a recommendation to the judge.” The parents sat on either side of the table, with their attorneys. Attorneys are doing all the talking and representatives from the counseling agency are not present. But the attorneys are referring to written reports filed by those agencies. It appears that this meeting is a conversation between experts.
Everyone is arrayed around a square table, but the attorneys appear to be sitting behind their clients. The primary discussants appear to be the DHHR personnel (supervisor and caseworker), CASA volunteer, and CAC representative. They are asking the parents questions and the parents respond directly to them. The lawyers rarely speak. One of the lawyers did stop the meeting a few times to ask a clarifying question. When he got his answer, he wrote something down and the meeting continued.
In the more formal MDT, the meeting followed a predefined agenda. There was a
clear leader (the prosecutor) and the other team members conformed to assigned roles. 11 Please note that these dimensions of variation are “ideal types.” We emphasize the extremes of potential variation for conceptual clarity. We did not necessarily observe any MDTs on the poles of these continuums.

Page | 22
The purpose of the meeting was clearly stated at the onset and the leader kept the
proceedings on task. In contrast to the less formal MDT, here attorneys play an active
role in the proceedings, speaking on behalf of their clients and advocating positions.
Progress reports from treatment providers were filed in a written format and presented
as exhibits.12 If asked to describe this particular meeting succinctly, we would describe
it as a conversation among experts. Indeed, this observation struck us so clearly that we
wrote this down in our field notes.
Our example of a less formal MDT focuses on the role of attorneys. They are, by
and large, silent participants in the process. Indeed, this particular meeting took place
in a small conference room with a table that was not large enough to accommodate all
the participants. It was the attorneys, who sat away from the table behind their clients.
Rather than being a conversation between experts, this meeting struck us as a dialog
between clients and providers. When attorneys did speak, they appeared to seek
clarification or pin down commitments. While the informal meeting described above
was initiated by a CPS supervisor, it did not proceed along a preset agenda. Parties
spoke as their contribution appeared to be relevant in the context.
As MDTs become more formal, they are more organized and orderly. By
following a predefined agenda, the MDT is most likely to address all the issues that were
known in advance. However, rigid formality can reduce the MDTs effectiveness in
responding to changing circumstances on the ground. Many participants told us that
the MDT is designed to ensure that “nothing falls through the cracks.” Where the MDT
members regularly communicate with one another outside of the meeting, these formal
12 Note that in other MDTs in this county, treatment providers did participate. However, they’re role in the meeting appeared to be similar to the reports referenced here.

Page | 23
procedures are useful. However, where team members do not regularly communicate
with one another outside the MDT context, the formality of the proceeding can prevent
necessary information coming to light.
MDTs organized around a less formal model appear to maximize the flow of
information. As mentioned above, this is important where participants don’t regularly
interact outside of the proceedings. A looser structure creates space for salient issues to
surface and be addressed. However, with less formality comes greater disorganization
and uneven participation. Discussions can veer away from the meeting’s designed
intent and become inefficient. There are strengths and weaknesses to an extreme
adoption on either side of this range.
Four!Ideal!Types!of!MDTs!
Our observations suggest that MDT practices vary along both formality and
institutional dimensions. That is, some MDTs appear to be oriented toward the courts
and proceed formally, while others may be oriented to DHHR and proceed informally.
By cross classifying these dimensions, we can consider four ideal types of MDTs as
illustrated in figure 3 below.

Page | 24
Figure!3:!Matrix!of!Ideal!Types!
Each quadrant in the matrix characterizes an archetype of MDTs. The purpose of
these characterizations is to provide a compass or orientation for classifying MDTs.
That is, very few MDTs fall exclusively into any one archetype, but by naming these
positions, we can begin to see what happens when the MDT becomes unbalanced along
these dimensions.
Beginning with the upper left quadrant, an MDT that is both formal and court-
focused, can be characterized as a pre-trial conference. Such MDTs are scheduled
because the law orders them to be scheduled and they provide the judge with necessary
information. The purpose of these MDTs is to identify the core issues, consensus, and
disagreements about a case so that the judge may make rulings. Formality in these
MDTs protect the respondent’s due process rights and ensures that the legal
proceedings will run smoothly. In contrast, the lower left quadrant characterizes an
MDT that is court oriented and informal. These MDTs are best described as procedural
check offs. Without formality to govern the process, these meetings simply satisfy the
statutory requirement that MDTs are scheduled every 90 days.
MDT!as!pre"trial!
Conference
MDT!as!therapeutic!planning
MDT!as!procedural!check"off
MDT!as!information!
trade
Court DHHR
Formal
Informal

Page | 25
The right hand side of the diagram characterizes DHHR oriented MDTS. In the
upper right quadrant, a MDT that is formal and department oriented can be described
as a therapeutic planning conference. The proceedings follow a formal protocol or
agenda, with the focus placed on reviewing past performance and identifying
modifications for the case’s future. In contrast, the informal departmental oriented
MDT in the lower right quadrant functions as an information trading session. Absent a
formal agenda and lacking the court’s more structured guidance, the MDT participants
share information about the case as doing see appears to be contextually relevant.
Variations!in!Constitution!&!Facilitation!
Recall that West Virginia Law (§43-5D-3) stipulates that MDT participants
should include: the child (when deemed appropriate), a guardian ad litem, the adult
respondent(s) along with legal representation, a designee from the prosecutor’s office,
and other available parties deemed appropriate by circumstance (foster parents, CASA
volunteers, any other person or an agency representative who may assist in providing
recommendations for the particular needs of the child and family). However, our
observation of MDT meetings suggests that their constitution and makeup varies widely.
Some MDT meetings involved only the adult respondent and DHHR personnel, while
others included a complement of participants so large that it was impossible for us to
construct a list of participants.
DHHR representatives were the only consistent contributors to the MDT process
across the state of West Virginia.13 Put differently, Department personnel were actively
involved in each of the MDTs that we observed. In most of the counties (5 of the 9 we’ve
13 However, this observation should be tempered by the fact that we coordinated our observations through the Department of Health and Human Resources. It’s possible (though not probable) that DHHR plays a lesser role in MDTs in one of the many counties we didn’t visit.

Page | 26
visited to date), DHHR schedules the meetings and sends out notifications to
participants. The majority of the MDTs (in 7 of 9 counties) took place at the DHHR
offices. Attorneys for the children and families were the second most common type of
participant we encountered in our observations. Though, as we describe in the previous
section, their participation was more uneven than the department personnel, they were
always invited and encouraged to participate in meetings.
Prosecutor participation was very uneven in our the sample of MDTs that we
observed. In some counties, the prosecutor’s office regularly sends a representative, but
he or she was unable to attend on the day that we observed. But for several others, the
prosecutor simply does not participate in the MDT sessions at all. In 4 of the 9 counties
we visited, we were told that prosecutors rarely participate in the MDTs. In two of the
counties where prosecutors do regularly participate, none was present on the day that
we observed. This is unevenness is an important issue for policy discussion and will be
further explored in the Phase II survey.
Among other potential MDT participants identified in the state code,
participation varies from one county to the next. In some counties, ASO service
providers regularly attend the MDT, while in others they send reports. In counties with
an active Court Appointed Special Advocate (CASA) program, CASA volunteers regularly
participate in the MDTs; however, not every county has this program. Likewise, in
counties with Child Advocacy Centers (CAC), CAC personnel attend the meetings, but
did not always actively engage as a participant. Our observations suggest that
participation is varied. In the forthcoming survey, we will seek to measure the extent to
which various MDT participants contribute to the meeting’s processes and outcome.

Page | 27
Beyond attendance and participation, MDTs also vary in terms of how they are
facilitated. We observed three distinct facilitation models and have been told about a
fourth, which we will observe before writing the final report. The four facilitation
models are:
! The MDT is facilitated by DHHR personnel (either the caseworker or a
supervisor
! The MDT is facilitated by the Prosecutor
! The MDT is facilitated by a neutral third party (CAC director)
! The MDT is facilitated by a facilitator employed by DHHR (but is not a
caseworker)
Facilitation by the caseworker or supervisor is the predominant strategy among
the counties that we observed. Typically, the caseworker is the most knowledgeable
member of the MDT concerning any given case. However, some caseworkers complain
that they have a hard time facilitating the meeting while simultaneously focusing on the
input of others. Ultimately it becomes their responsibility, or the responsibility of their
case aide to document the recommendations generated in the MDT. It is clear from our
observations that many caseworkers experience the MDT as an overwhelming
responsibility.
Facilitation by prosecutor is the second most common facilitation strategy that
we observed. MDTs facilitated by prosecutors struck us as being more formal than in
the meetings facilitated by the department. These MDTs were organized and orderly.
The prosecutors we observed effectively used their institutional authority to guide the
meeting. However, there were some drawbacks to the prosecutor lead model. As with
caseworkers, when the prosecutor facilitates the meeting, their attention can be drawn

Page | 28
away from their role as the department’s legal representative. Put differently, leading
the meeting requires effort and focus that detract from their other expected duties in the
MDT. Also, as the prosecutor becomes more involved in the MDT process, the process
can become more unbalanced in a court oriented direction.
As a response to the problem of divided attention in facilitating meetings, some
counties are experimenting with third party facilitation models. We observed an
innovative model in one county and have made arrangements to examine different
models of innovation in others. Since early 2006, one county’s MDT process has been
facilitated at a Child Advocacy Center (CAC) and facilitated by the center’s director.
This model was developed through collaborative dialog within a countywide child abuse
taskforce.
The taskforce was concerned that the MDTs were becoming too adversarial and
attorney driven. They reasoned that meetings held at a neutral site under the leadership
of a neutral facilitator would be more conducive to all the parties. A CPS representative
told us, “it’s a lot less intimidating to the family for the CAC to facilitate these meetings.
They’re on neutral ground.” Since adopting this model, DHHR caseworkers believe they
are under less pressure and are able to be more effective with the families. Since neither
the department, nor the prosecutor’s office runs the meeting, the caseworkers perceive
families to be less guarded in MDTs under this new model than in the past. According
to one caseworker, “now, fewer families view me as an enforcer.”
We spoke to a prosecuting attorney who regularly participates in MDTs who
appreciates this model. She told us, “I am free to focus on the case. She [the CAC
director] will keep the meeting on task and us in line.” As a neutral participant, the CAC
begins the meeting and then retreats to background. She only becomes an active

Page | 29
participant when the meeting needs to be redirected or ended. We observed this
dynamic in action and offer an extended account of this observation below. This case
involved a family nearing the end of an improvement period and DHHR was concerned
about their progress:
Caseworker: We have concerns about the home…
Prosecutor: Yes, I’ve seen the photographs and, well, we’re not there yet. We’ve been at this nine months and we’re approaching the disposition. The best case scenario is that the Judge might grant a post-dispositional improvement period but…
Respondent’s Counsel: Some of the pets have been sold.
Caseworker: It does appear that they’re trying… the problem is that this house is just not clean. It smelled horrendous. It was horrible… despicable. I can hardly describe it. It’s just not acceptable. We also have concerns about how they are going to feed the animals and the children.
At this point, the respondents began to disagree with these criticisms and the
mother began to cry. Their parenting counselor or coach tried to reframe the
discussion.
Counselor: You have made a lot of progress over the months that we’ve worked together. I remember when we first started you had an unclean smell. We talked about this and put a plan in motion, and when you worked hard on cleaning your house the smell went away. Well, when you came in for our last session, the smell was back. I think we need to do some more work.
Guardian ad litem: I have no problem pushing things back, but only if this is going to improve. I have to tell you that I’m not optimistic; we’ve been at this for a few years now.
Caseworker: We still have some major concerns that you have not addressed. Yes, you’ve followed the caseplan for employment and getting appropriate housing, but the condition of the house is deplorable and not acceptable.
Guardian ad litem: Would them getting a bigger place help things?

Page | 30
Prosecutor: Size might help the organizational problems, but not the cleanliness.
Respondent’s Counsel: Wait a minute now, the house has been a problem from the start and they’ve been working hard at resolving that. The kids have made substantial improvements and the parenting has improved as well. We should recognize these things!
Prosecutor: Look, I’m going to be forthright. The Judge can go a couple of ways. He can say that the improvement is insufficient and make a disposition. Or, he could look at what’s improving and order another improvement period. It’s a 50/50 thing so I don’t know which way he will go. And honestly, I don’t know what our position is going to be. I’m going to have to sit down and talk about this with the Department.
Then, the mother asked for clarification. The prosecutor explained that potential
legal outcomes at the next hearing included a dispositional improvement period (which,
she said, “are rare”), “an alt 5” (also called a disposition 5)14 which would rule that the
parents are not presently capable of caring for the children, but would not terminate
their parental rights, or he could terminate parental rights. “Termination is exactly
what it sounds like; there is no contact with the children unless they explicitly ask for it.”
Guardian ad litem: Will the department go out and take more photos before the hearing?
Caseworker: We’ve done this before and there was improvement while we were taking photos; but then it backslides. This has been a pattern for a long time, therefore we have a real problem with a post-dispositional improvement period.
Prosecutor: Get rid of the pets! They should be the first to go! I hate to be this harsh. But at this point, that’s where we’re at. Or maybe knock it down to one pet… or…
By now the mother was sobbing and everyone appeared to be frustrated. The
CAC director stopped the meeting proclaiming, “I believe the point has been made and
14 West Virginia Code: §49-6-5a(5)

Page | 31
it’s time for everyone to discuss this privately with their counsel. I think it’s time to
close off the discussion.” The MDT confirmed the pending court date and the meeting
ended. After the meeting, the CAC director explained that part of her role is to close off
discussion that has outlived its usefulness. The prosecutor nodded in agreement and
said, “she has a vantage point that I don’t; sometimes we all need to be told to stop.”
As the extended example shows, MDTs have the potential to veer off course or to
pursue an agenda item beyond its utility in the case. Having a neutral facilitator in the
room with the authority to end the discussion has merits. In some counties, the
prosecutor’s office fills this role adequately. In others, an employee of the DHHR
services as MDT coordinator and facilitator. In our travels about the state, several MDT
participants told us that they would like to have assistance in facilitating the MDTs in
order to take the burden off the caseworker, or case aide. We will attempt to measure
this sentiment with more precision in the Phase II Survey.
DISCUSSION!AND!IMPLICATIONS!
As discussed in the introduction, MDTs bring together a diverse group of people,
sponsored by different organizations or institutions, united around the common goal of
addressing treatment plans in a case of child abuse or neglect. In the abstract, the
multidisciplinary team model presumes a collegiality and unity of purpose. However in
practice, child abuse and neglect cases are contentious and bring together participants
with vested interests in adversarial positions. One of the most important observations
that we made in Phase I of this study was that it is difficult for MDT participants to free
themselves from their institutionally conferred roles. The best interest of the child may

Page | 32
look quite different depending on the vantage point. MDT policy, training, and
procedures, must recognize this institutional reality.
As detailed above, we observed three dimensions of similarity and three
dimensions of difference across the counties in West Virginia child abuse and neglect
MDTs. The similarities point to challenges in facilitating trust, consensus and full
participation. The differences reflect patterns of institutional influence, cultural norms
of formality, and modalities of facilitation. Each of these observations suggests salient
lessons for future practice. We offer three recommendations based on these
observations. (1) Consider adopting a dynamic MDT structure that changes according
the case’s development or life course. (2) So long as MDTs are to be a core element of
child welfare policy, the Circuit Courts should emphasize their value and clear time on
the dockets to encourage maximum participation. (3) Each county or district should
consider adopting a neutral facilitation model. We now turn to each of these
recommendations in turn.
The!Case!for!an!Evolving!MDT!Structure!
In West Virginia, where child abuse and neglect proceedings fall under the
original jurisdiction of the Circuit courts, cases initiate through adversarial proceedings.
The state brings a petition against the adult respondent (typically a parent) for abuse
and neglect, while the respondent seeks to defend him or herself from these charges.
Generally, the case is brought to an MDT only after the alleged incident has been
substantiated in court. Thus at the preliminary stages of an MDT, it’s reasonable to
presume that the team members will not share a common vision of the team’s goals, or
even trust one another. In the stage immediately prior, the sides were engaged in

Page | 33
dispute. We should recognize that it takes time for the loser of this struggle to see
DHHR, the prosecutor, or even a CASA volunteer as an advocate. Indeed, it was not
uncommon to hear parents in the early stages of MDTs express the sentiment, “I just
want to do whatever it takes to get my kids back.”
It may make sense to rely more on formal procedure in the early phases of the
MDT, which can be relaxed as trust builds. Formal procedures provide all the parties
with structure and space which can help the group establish its own dynamic over time.
By relying more on formal arrangements in the early stages, it will be easier to maximize
participation of the necessary contributors. As the case matures, the constitution, focus,
and tone of the MDT can be modified to fit the case needs. In cases where the family
requires more structure, the MDT can remain formal. However, where the family is
progressing according to the treatment plan, some of the formality requirements can be
relaxed and the meeting attendees should be tailored to the family’s changed
circumstances. This flexibility is one of the keys to maximizing productive participation.
Circuit!Courts!should!reinforce!MDT!importance!
If MDTs are to be a core component of West Virginia Child Welfare policy, we
believe it is imperative that the circuit courts reinforce this priority by minimizing the
barriers to participation. Participation was strongest in counties that scheduled MDTs
on specific days, coordinated with the circuit court calendar. Since many MDT
participants juggle large caseloads, the protecting specific times each month from
hearings, motions, and other court business will greatly reduce scheduling conflicts.
Similarly, it’s imperative that where they are currently not participating, the
prosecutor’s office should become more involved in the MDT process. We believe that

Page | 34
the flexible approach suggested above could be tailored to ensure prosecutor
participation in the early phases of the case life course and scaled back as trust and
consensus rise. But, so long as the MDT is prone to adversarial conflict, we agree with
the sentiments of a social services coordinator who declared, “if the clients get to have
their lawyer with them, we should have ours too.” The prosecutor is an officer of the
court. Where the prosecutor elects not to participate (in person or by proxy) his or her
office sends a message that the MDT is not important. We believe that this message
contributes to attendance problems in the MDT more broadly (which is a hypothesis we
intend to test in the Phase II Survey).
Each!Jurisdiction!Should!Consider!a!Neutral!Facilitation!Model!
Finally, we see the neutral third party facilitation model as a valuable tool for
treatment planning and reviewing progress. A neutral facilitator can referee
disagreements and foster discussion when meetings become tense. When meetings are
routine, he or she can remove some of the reporting and oversight burden from the
caseworker, supervisor, or prosecutor (depending on whom conveys the meeting at that
locale).
While the example provided above offers one exemplar (e.g., using the Child
Advocacy Center personnel) this is by no means the only alternative. We understand
that there might be resistance to broader dispersion of that model, particularly in
locations with long standing practices that have evolved from local norms.15 We also
know that “one size does not fit all.” It is important for innovations and practices to
reflect the availability of resources which clearly vary across the state. But nevertheless
15 We heard directly from MDT participants who believe the neutral facilitation model would not work in their counties.

Page | 35
every jurisdiction can positively learn from the best practices of others. In addition to
the observed model reported here, we are aware of a practice in other counties, where an
employee of DHHR participates in MDT meetings as a neutral facilitator.16
After comparing the full range of MDT practices in West Virginia, we believe that
the virtues of neutral facilitation outweigh potential flaws. However, we recognize that
any adaptation to the MDT model must reflect the local conditions where MDTs occur.
There are many ways to incorporate a neutral arbiter in the MDT process, and will
provide a catalog of these strategies in the final report for this study.
NEXT!STEPS!
We now advance this study to Phase II, which will include an internet-based
survey of MDT participants employed by DHHR , or who are members of the legal Bar.
These surveys will measure MDT practices with more precision and capture member
perceptions of participation, facilitation, and effectiveness. Upon completing the second
interim report on the survey data, we will prepare a comprehensive final report that
brings together both sets of data and draws specific conclusions.
16 We have made arrangements to observe MDTs in one of these counties and will include those observations in the final report for the study.

Page | 36
APPENDIX!A!–!ADMINISTRATIVE!ORDER!
IN THE CIRCUIT COURT OF ________ COUNTY, WEST VIRGINIA
IN RE: Abuse and Neglect Cases Multidisciplinary Treatment Team Study, 2007-2008
ADMINISTRATIVE ORDER
Whereas, the processes and procedures of child abuse and neglect cases in this State, including
multidisciplinary treatment teams, are the subject of ongoing study and review by the court system and
involved child welfare agencies of the State Department of Health and Human Resources ("DHHR"), and
the study and review is directed toward comprehensive systemic improvement in the handling and
management of such cases. The ultimate goal of this study is the facilitation of effective multidisciplinary
team meetings.
Whereas, incident to this effort to improve the effectiveness of multidisciplinary treatment teams
in child abuse and neglect cases, the Supreme Court Administrative Office and the Court Improvement
Oversight Board (CIP), with assistance from the consultant, the West Virginia University Research
Corporation, and Attorneys John M. Hedges and Teresa J. Lyons, will be conducting a study of
multidisciplinary treatment teams in 2007 and 2008, pursuant to a court improvement grant awarded by
the United States Department of Health and Human Services.
Whereas, field work for this assessment study will be conducted principally by Dr. Corey Colyer,
Ph.D., with assistance from Dr. Christopher Plein, Ph.D., who will be observing multidisciplinary
treatment teams meetings, conducting focus group discussions after multidisciplinary treatment team
meetings when possible, conducting a mail survey of multidisciplinary treatment team participants, and
preparing written reports. Consistent with the legal requirements and policies of confidentiality regarding
the records and proceedings in abuse and neglect cases, the confidentiality of all participants in the survey
will be maintained, and the identities of individuals will not be included in any written reports.
Additionally, the research will be monitored by the West Virginia University Institutional Review Board
which follows stringent privacy protection protocols. Further, all counsel will be notified in advance and
in writing that their multidisciplinary team meeting has been selected for observation.

Page | 37
Accordingly, for the purposes of the herein-described Multidisciplinary Treatment Team Study,
2007-2008, the Court upon its own motion, and pursuant to its constitutionally conferred rule-making
authority as administrative head of this Circuit Court, does hereby ORDER as follows:
1. That Dr. Colyer and Dr. Plein shall have permission to observe multidisciplinary
treatment team meetings in Berkeley County; shall have permission to conduct focus
group discussions; and shall have permission to provide surveys to multidisciplinary
treatment team participants;
2. That the officials involved in investigations, treatment and proceedings under Chapter 49
of the West Virginia Code, including prosecutors, circuit clerks, counsel for parties (to the
extent not in conflict with ethical considerations of client confidences), DHHR
employees, CASAs, and other investigative, treatment or child-welfare agency employees,
are permitted to discuss multidisciplinary treatment team meetings with Dr. Colyer and
Dr. Plein;
3. The Circuit Clerk shall provide a certified copy of this order to each judge of this circuit,
and four certified copies of this order to John M. Hedges and Teresa J. Lyons, Byrne
Hedges & Lyons, 141 Walnut Street, Morgantown, WV 26505.
ENTERED this _____ day of ____________________, 2007 _________________________________________ ____________________., CHIEF JUDGE
Prepared By: ____________________________ Teresa J. Lyons (WV Bar ID 8047) BYRNE HEDGES & LYONS 141 Walnut Street Morgantown, WV 26505

Page | 38
APPENDIX!B!–!LETTER!TO!MDT!PARTICIPANTS!
July 31, 2008
RE: Multidisciplinary Treatment Team Study
Dear Counsel:
I am writing to you concerning a Multidisciplinary Treatment Team Study that will beconducted by the Court Improvement Oversight Board (CIP) of the West Virginia SupremeCourt. I am a professor at West Virginia University, and I have been hired by the CIP to conduct this study.
As part of the MDT study, I will be attending MDTs throughout the State to observe and then to report the results of my research to the West Virginia Supreme Court. The MDT ofwhich you are a member has been selected for inclusion in this study. Although I will beobserving MDTs, the confidentiality of all participants will be maintained, and the identities of individuals will not be included in any written reports. At no time will I participate in the MDTor make any recommendations that are specific to your case.
I have received permission from the chief judge of your circuit by an administrative order and the DHHR regional director to attend MDTs in your county. I am also letting you know ahead of time about my attendance at the MDT in case you have any questions or you object tomy attendance. Because this study is important to improving MDTs throughout the State and my attendance will have no bearing on your case, I am hopeful that you and your client will not object to my attendance.
If you have any questions, you may telephone me at 304-293-5801 ext. 3207, or e-mail me at [email protected]. You may also contact Teresa J. Lyons, an attorney assistingwith the study, by phone at 304-296-0123, or by e-mail at [email protected].
Thank you for your attention to this matter.
Very truly yours,
Corey J. Colyer, Ph.D.