Embed Size (px)
Citation preview
EBM Revisited: a brief refresher
Introduction and Description of the ADEPT Course
Andrew Booth & Marishona Ortega
Why ADEPT?• librarians need to be able to support
Evidence Based Healthcare
• users need to be able to do their own focused searching
• only a small proportion (about 1%) of the medical literature is clinically relevant
The Ingredients of EBM
• Focused questions• Hierarchy of evidence• Filters• Problem based learning
– Scenarios– Anatomy of the question
– Shared expertise (SEE-ONE, DO-ONE, TEACH-ONE)
Focusing the question
• Helping requester to break information need down into EBM anatomy clarifies the originating question.
• “OR” within categories and “AND” between categories.
Understanding study design
• Adds to your ability to recognise “good studies”and “bad studies”.
• Helps you to identify the question being answered by an article.
Using methodological filters
• One line, sensitive and specific versions
• rely on publication types or occurrence of textwords to identify methodologically superior studies
• are also used to compile pre-filtered database products e.g.. Cochrane Library (clinical trials), DARE (reviews) & NHS EED (economic evaluations)
Topics
Types of question - primary studies
• Diagnosis
• Etiology
• Prognosis
• Therapy
Types of article - secondary studies
• Reviews• Economic Evaluations• Guidelines
[and now Qualitative]
The Process• Clinical Scenario
• Focusing the question
• Translating into MeSH terms
• Conducting the literature search
• Applying the methodological filters
• Filtering for quality studies
• Specialist resources
ResourcesFor each study:• User Guides from
JAMA• ACP Journal Club or
EBM MEDLINE Guides
• CASP filters page http://www.phru.org.uk/ ~casp/filters.htm
About ADEPT:• Becoming ADEPT:
Project Overview - HLR Dec 1997.
• Becoming ADEPT: delivering distance learning on EBM to Librarians - HLR Sept 1998.
Principles of Study Design: a librarian’s perspective
Andrew Booth
Scenario
You are a postgraduate medical librarian in Kleptovale NHS Trust. You have bid for a Nicksnix Library security system. The postgraduate Dean wants some evidence that it is effective. There is no published evidence so you will need to conduct an original study. What are you going to do?
Lower forms of evidence
• Anecdote (I once knew a librarian who……)
• Case study
• Case series
Answer. A Case-control study• You call up the Regional Library Unit.
Details of 10 libraries with book losses of >5% (cases) and of 10 libraries with losses of <1% (controls).
• Phone all 20 libraries and ask “Do you use a library security system?” Yes/No
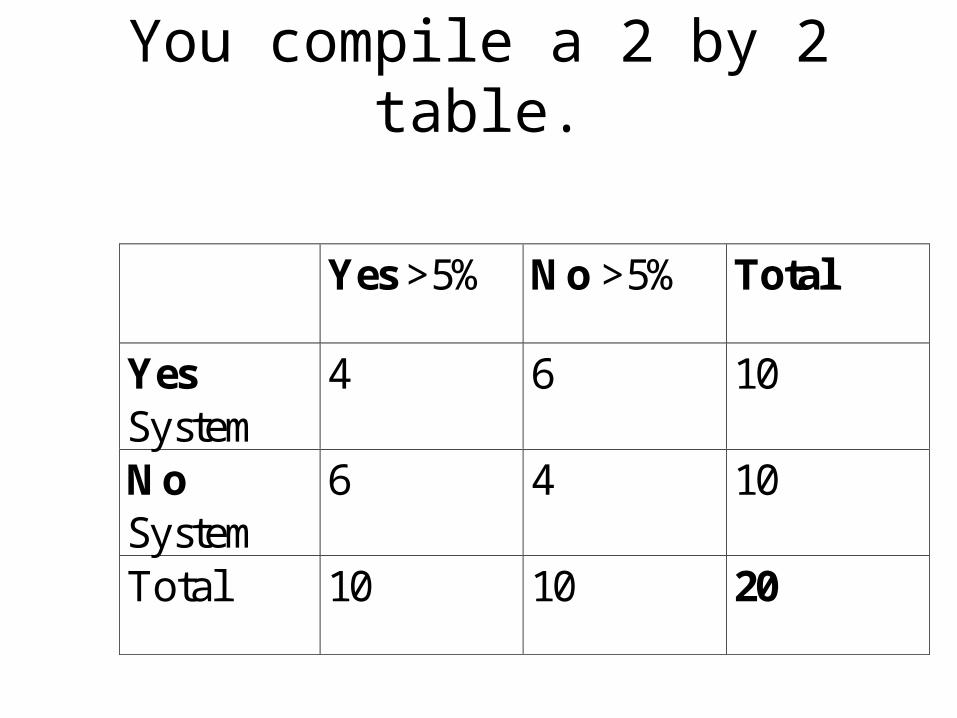
You compile a 2 by 2 table.
Yes >5% No >5% Total
YesSystem
4 6 10
NoSystem
6 4 10
Total 10 10 20
But........• Controls might be underreporting their
losses to make system look good.
• People with security systems may be more security conscious (using other methods)
• Bias (flaw in research method) or confounding (some other factor not taken into account).
Case-control studies [Retrospective]
Advantages• Quick and cheap• It’s the only method
for rare events• Requires fewer
subjects than other designs
Disadvantages• Relies on
recall/records• Open to confounding• Selection of controls
is difficult• Potential bias in recall
or selection.
Answer: A Cohort Study
Convince 110 members of HLG to take part in a prospective cohort study. Over a two year period you record who uses the system [Exposed] and who doesn’t [Non-Exposed]. At end of two years you calculate rate of heavy losses within both groups.
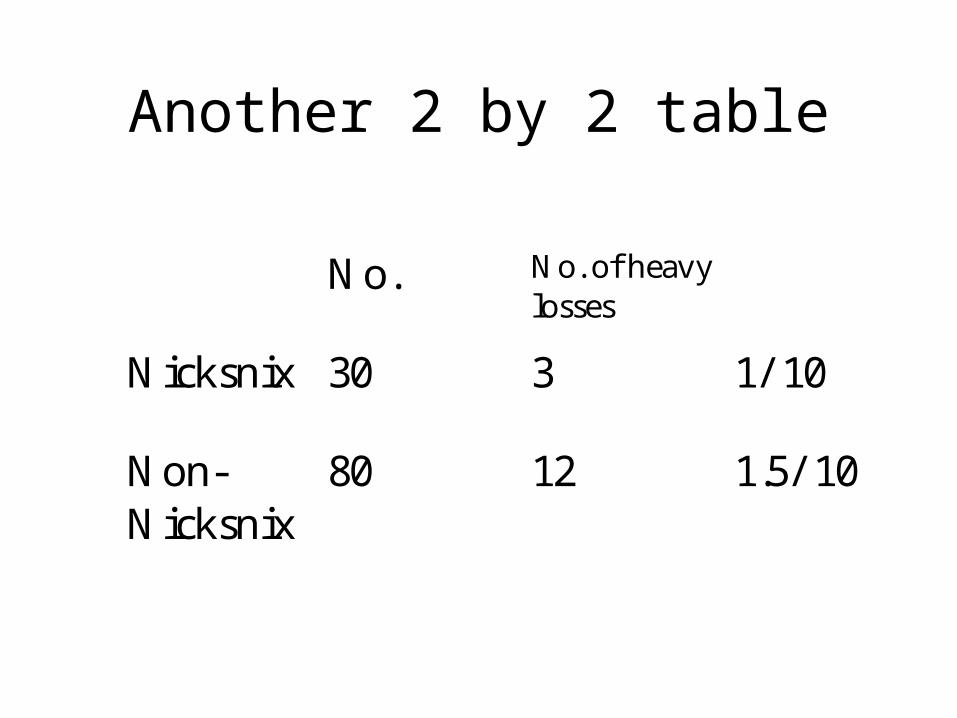
Another 2 by 2 table
No. No. of heavylosses
Nicksnix 30 3 1/ 10
Non-Nicksnix
80 12 1.5/ 10
But.....• OK so you may have eliminated recall and
reporting bias through baseline data collection, but
• Libraries with security systems may be in richer areas and less prone to theft anyway.
Cohort studies
Advantages• Subjects can be
matched• Eligibility criteria can
be standardised• Easier to run than an
RCT.
Disadvantages• Blinding is difficult• Randomisation is not
present• Requires a large
sample and longer follow up.
Answer: An RCT• You go for a sponsored Randomised
Controlled Trial. You recruit another group of HLG members. You randomly assign half with a free NicksNix system and the others must go without. After a year you have the following results.
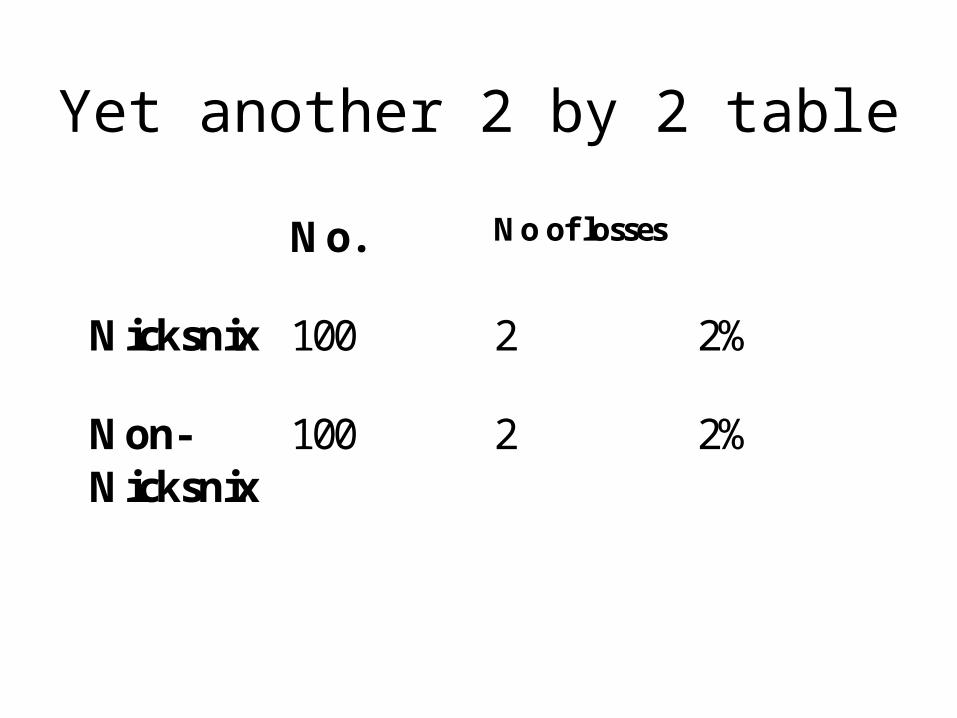
Yet another 2 by 2 table
No. No of losses
Nicksnix 100 2 2%
Non-Nicksnix
100 2 2%
Finally....
After three years and thirty minutes and three separate studies the Postgraduate Dean believes he has the right answer:-
No difference, No Nicksnix,
No comment!!!
Randomised Controlled Trials
Advantages• Unbiased distribution
of confounders• Blinding more
possible• Randomisation
facilitates statistical analysis
Disadvantages• Expensive in time and
money• Volunteer bias• Ethical problems,
sometimes• May create artificial
behaviour
Postscript
Practically, you wouldn’t go to all that effort. Maybe use a cross-over design where one Library (n-of-1 study) or more went through periods without and then with a system. You would need to make sure that there was a washout period. Also you would have to guard against a placebo effect.
Hierarchy of effectiveness• Systematic Review
• Randomised Controlled Trial
• Cohort study [Prospective]
• Case-control [Retrospective] (May be contemporary or historical)
• Case series
• Individual case study
There are other hierarchies
E.g. Hierarchy of patient experience• Qualitative research study• Interviews/Surveys• Case study• Anecdote
• C.p. Signal to noise ratio (Edwards AG, Russell LT & Stott NCH (1998) Signal versus noise in the evidence base for medicine: an alternative to hierarchies of evidence? Family Practice 15 (4): 319-322)
Constructing a Question
Marishona Ortega
EBP Process
• Define problem
• Find evidence
• Appraise evidence
• Apply results of appraisal
• Evaluate change
• Redefine problem
Formulating a question using PICO
• Population/Patient/Condition
– Who is the question about?
• Intervention/Exposure
– What is being done to or happening to the patient/population?
• Comparison(s)
– What could be done instead of the intervention?
• Outcome(s)
– How does the intervention affect the patient/population?
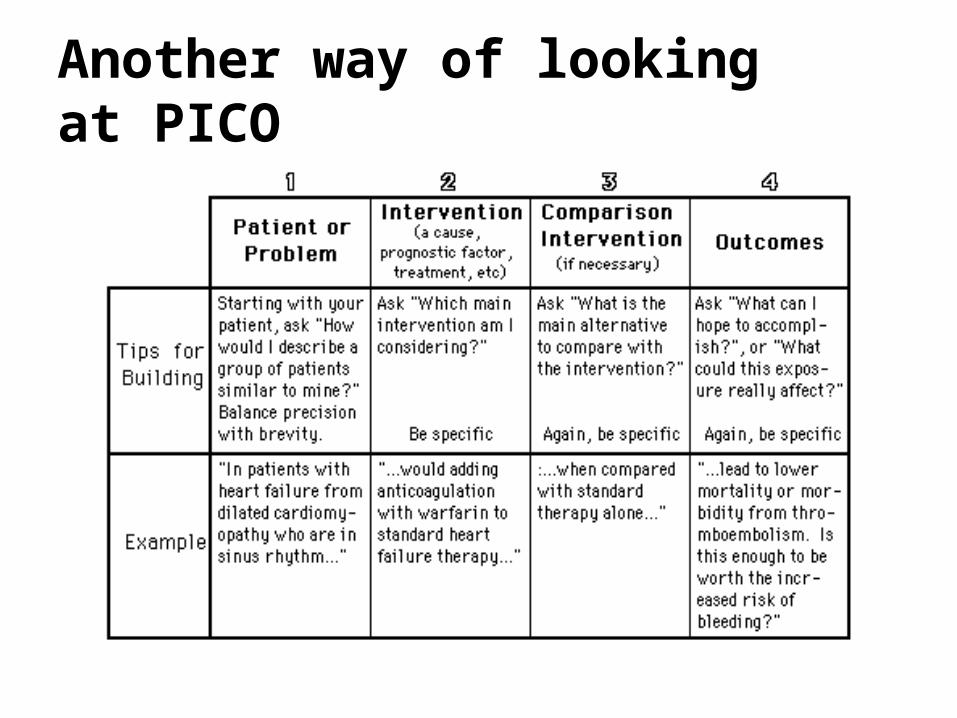
Another way of looking at PICO
Focused Questions - the benefits
• Guides search process
• Prompts for considering synonyms
and alternatives
• Saves time - increases relevance
Translating your question into a strategy
Your department is exploring the idea of introducing near-patient testing for Group A ß-Streptococcal throat infection. You have been asked by your manager to gather the evidence for this procedure with particular reference to sensitivity, specificity and cost.
PICO Applied:
• Patient/Condition– Group A ß -Streptococcal throat infection
• Intervention– Near-patient testing or rapid test
• Comparison– Laboratory testing
• Outcome– Sensitivity, specificity, cost
Now your turn…
As background to your service you are compiling information identifying the risks of infection from HIV, Hepatitis B & C and CMV following homologous blood transfusion.
How would you structure your search?
Now your turn - contd
• Patient/Population– Persons receiving blood transfusion
• Intervention– Homologous blood transfusion
• Comparison– Another form of blood transfusion i.e. autologous
• Outcome– Not becoming infected with HIV, Hepatitis B&C or
CMV
EBP Process
• Define problem
• Find evidence
• Appraise evidence
• Apply results of appraisal
• Evaluate change
• Redefine problem
Where do I start?
• Develop your question• Decide on the most appropriate
source(s)• Divide your search into
‘concepts’• Think of alternative terms for
each concept• Search each concept separately• Combine concepts using
Boolean logic

Therapy Studies: Design, Terminology and
Filters
Learning Objectives
• Describe the main characteristics of a rigorous therapy study.
• Recognise some of the terminology associated with studies of therapy
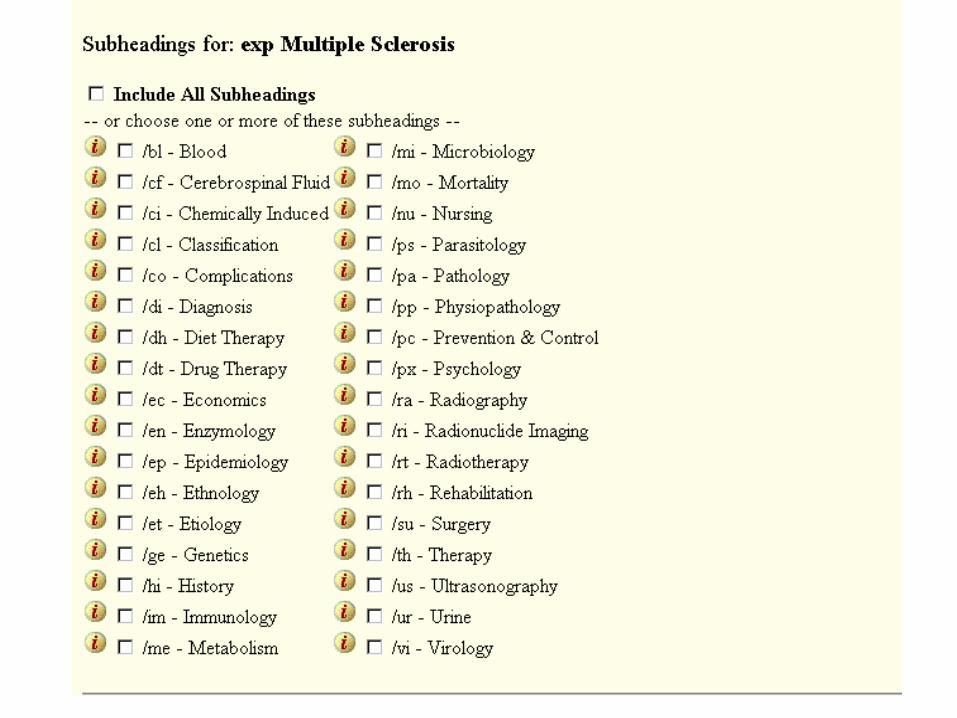
• Itemise sub-headings associated with treatment• Avoid common pitfalls associate with searching
for therapy studies• Utilise the methodological filters associated with
therapy literature searches
What is a therapy study?
• Treatment or management of a condition– Objective of treatment– Choice of treatment– Target of treatment
• Literature-based evidence can assist with all three aspects, but most particularly “Choice of treatment”
Therapy Studies
• A search for therapy studies focuses on the decision between treatment choices
• Therefore the evidence will be comparative
• The preferred design for a therapy study is a RANDOMISED CONTROLLED TRIAL (RCT)

Searching for therapy studies
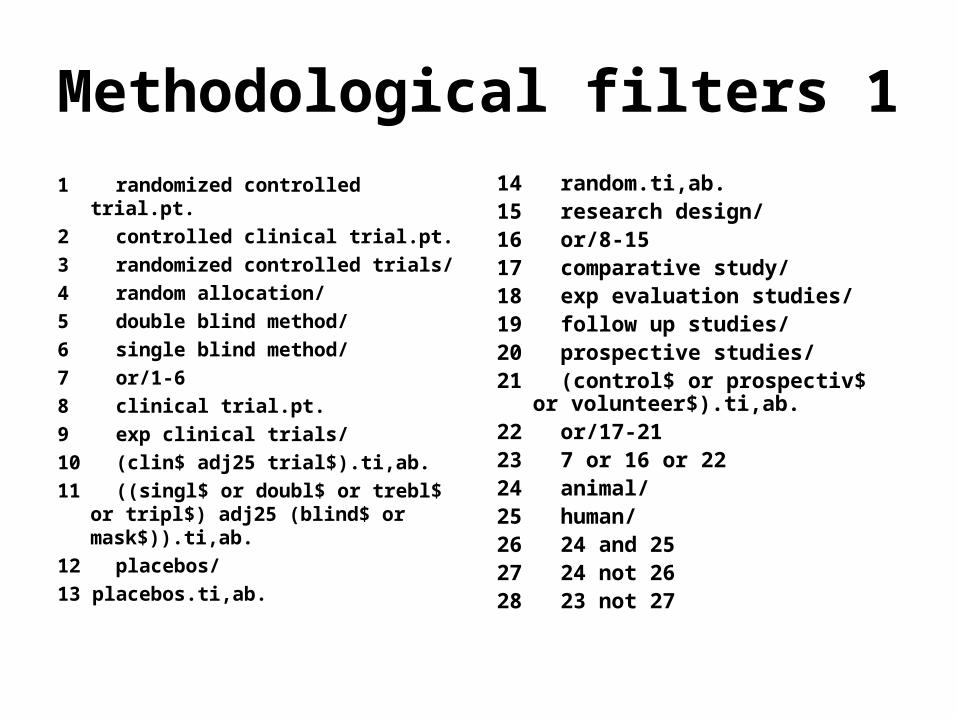
Methodological filters 1
1 randomized controlled trial.pt.
2 controlled clinical trial.pt.
3 randomized controlled trials/
4 random allocation/
5 double blind method/
6 single blind method/
7 or/1-6
8 clinical trial.pt.
9 exp clinical trials/
10 (clin$ adj25 trial$).ti,ab.
11 ((singl$ or doubl$ or trebl$ or tripl$) adj25 (blind$ or mask$)).ti,ab.
12 placebos/
13 placebos.ti,ab.
14 random.ti,ab. 15 research design/ 16 or/8-15 17 comparative study/ 18 exp evaluation studies/ 19 follow up studies/ 20 prospective studies/ 21 (control$ or prospectiv$ or
volunteer$).ti,ab. 22 or/17-21 23 7 or 16 or 22 24 animal/ 25 human/ 26 24 and 25 27 24 not 26 28 23 not 27
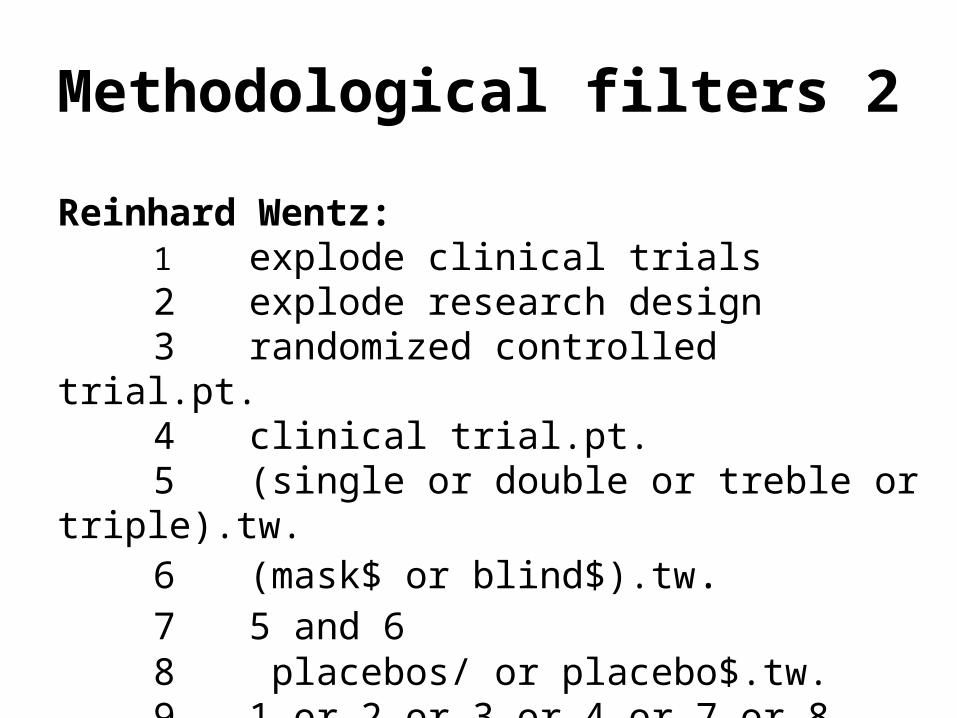
Methodological filters 2
Reinhard Wentz:1 explode clinical trials2 explode research design3 randomized controlled trial.pt.4 clinical trial.pt.5 (single or double or treble or triple).tw.6 (mask$ or blind$).tw.7 5 and 68 placebos/ or placebo$.tw.9 1 or 2 or 3 or 4 or 7 or 8
Methodological filters 3
Mid-range strategy from Health Information Research Unit, McMaster:
1 randomized controlled trial.pt.2 or dt.fs.3 or tu.fs.4 or random$.tw.5 or/1-4

And last but not least...
The one-line filter:
clinical trial.pt
• Retrieves 97% of rigorous therapy studies
• Only includes 3% of irrelevant studies
So how does this work in practice?A 17-year-old female was travelling home one night when
the car her friend was driving careered off the road. Fortunately, no-one was seriously injured but she presented to A&E with localised low back pain and was diagnosed with lumbar strain.
For some time the Senior Physio has been considering the treatment for low back pain and wonders if acupuncture might be a more effective and comfortable alternative. She asks you to run a search to find the relevant evidence.
What’s your Question?
• Patient/Condition– 17 year old female with low back
pain/lumbar strain
• Intervention– Acupuncture
• Comparison– Existing treatment
• Outcome– Pain relief
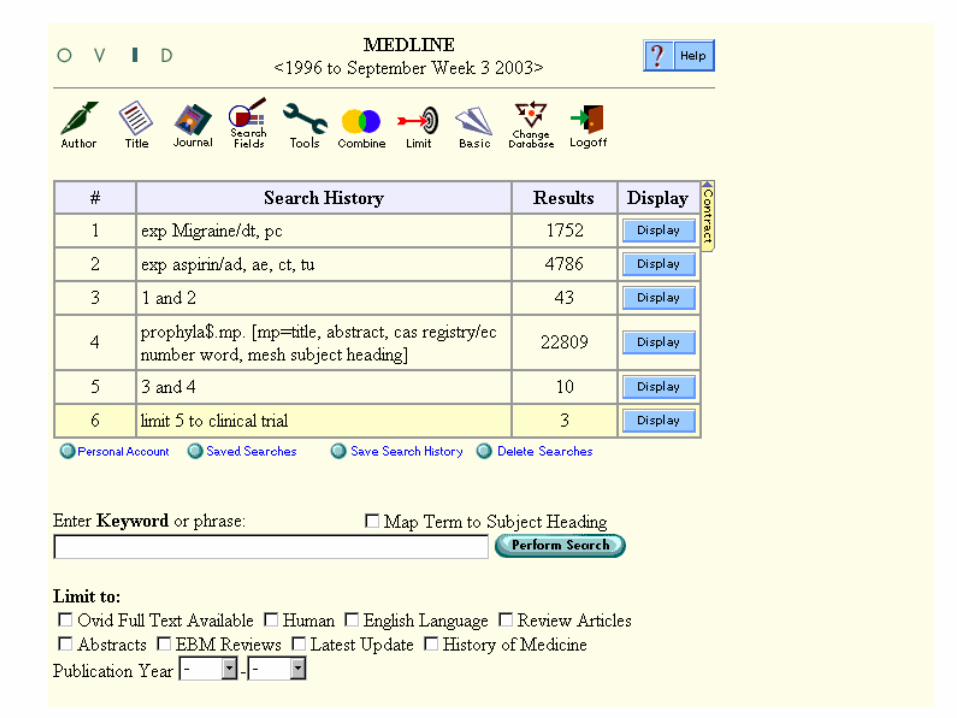
What’s your Strategy?
• Usually start with PATIENT/CONDITION and then the INTERVENTION
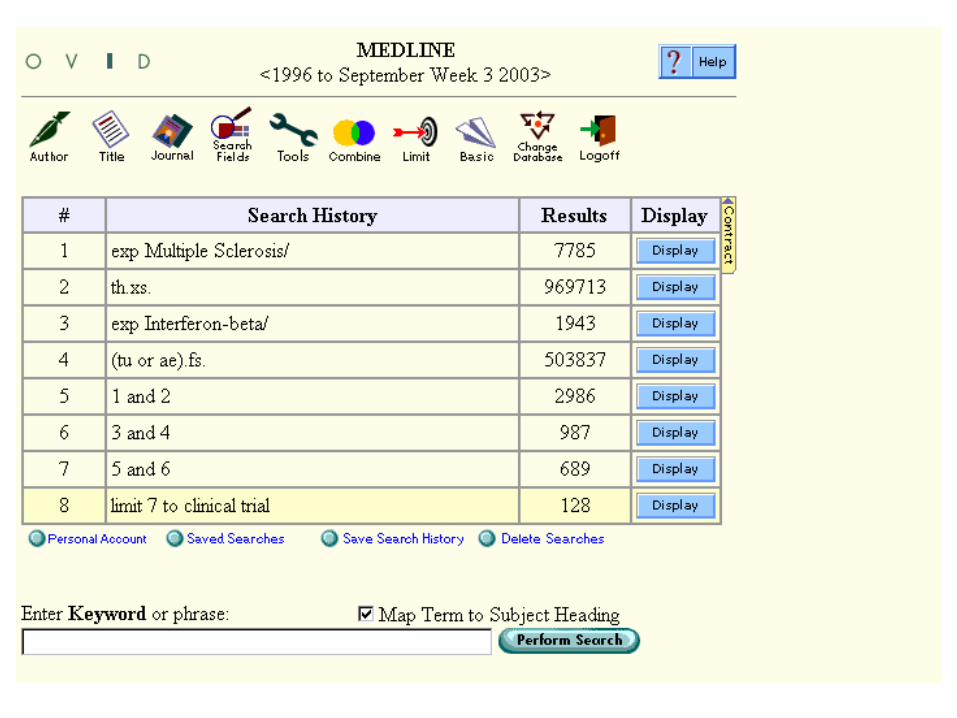
• Thus:1. low back pain2. acupuncture3. 1 and 24. limit 3 to clinical trial.pt
Practical Session
Go to:http://gateway.ovid.com
Username: trainshePassword: train123
If you need help - just ask!
Feedback time:
How did you get on?!
Filtering for quality studies
Andrew Booth
1. A Comparison
• Drug A versus Drug B• Drug versus other
(alternative) therapy• Drug versus placebo• Service versus
“standard care”
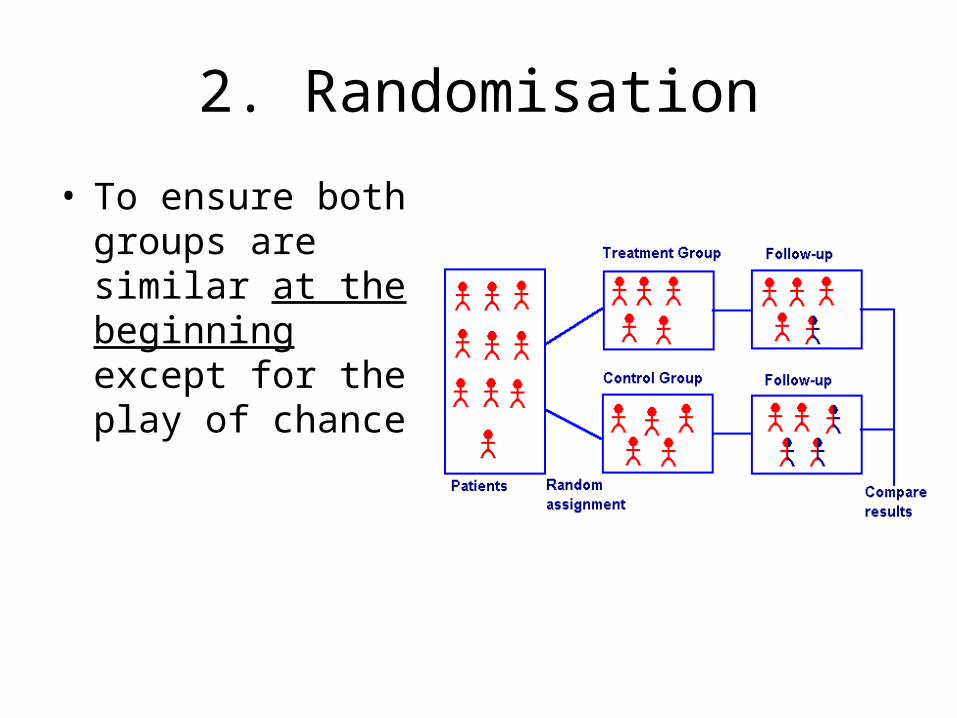
2. Randomisation
• To ensure both groups are similar at the beginning except for the play of chance
3. Blinding
• Subjects are blinded• Those delivering
treatment are blinded• Those doing analysis
are blinded
• Contrast: Concealment of allocation
4. Withdrawals and drop outs
• Are all those who entered into study accounted for at its conclusion
• Was an intention to treat analysis used?
5. Follow up
• Were all participants followed up and was data collected in the same way?
6. Sample size
• Were there enough participants to minimise the play of chance?
Preview of Distance Learning Module
Andrew Booth
Each module
1. Reading material
2. Worked exercise
3. Exercise with deadline date
4. Group (Anonymised) Feedback
Modules
• Reviews• Diagnosis• (A)etiology/Prognosis• Guidelines/Economic
Evaluations• Qualitative Research

Contact Us:
Marishona Ortega• [email protected]• 0114 222 0797Andrew Booth• [email protected] • 0114 222 0705Or leave a message with Tricia Campsell• 0114 222 0703





























