PowerPoint Presentation
ARRHYTHMIA RECOGNITION DR. JETTY SEDYAWAN SpJP.Bagian Kardiologi
FKUI
EKG & ARITMIA
USEFULNESS OF The ECG1. Atrial and Ventricular Hypertrophy2.
Myocardial ischemia and infarction3. Arrhythmia4. Pericarditis5.
Systemic Disease that effect the heart6. Effect of cardiac drugs,
esp Digoxin and Quinidine7. Distribution in electrolyte
metabolisme
SA nodeSumber impuls normal/ alamiah , 60 100 AV nodeBisa
mengeluarkan impuls 40-50x/menitBerkas HisSerabut
PurkinjeVentrikelBisa mengeluarkan impuls30 x/menit
Atrial Depolarization
VentricleDepolarization0.12 second
Terminologi morfologi QRSqRsRsRrSQRQ/QSRsRrSr
JETSED
A. Jarak R R :
1 kotak sedang= 300 x / menit2 kotak sedang= 150 x / menit3
kotak sedang= 100 x / menit4 kotak sedang= 75 x / menit5kotak
sedang= 60 x / menit6 kotak sedang = 50 x / menit
B. Hitung jumlah R- R dalam 6 kotak besar = 6 detikJumlah R x 10
= heart rate / menit
C. 1500 / jarak R-R ( dlm mm ) = heart rate / menitMENGHITUNG
LAJU JANTUNG :
1 kotak kecil= 0.04 detik
5 kotak kecil= 1 kotak sedang= 0.2 detik
5 kotak sedang = 1 kotak besar= 1 detikPaper speed : 25
mm/second
CAUSE OF CARDIAC ARRHYTHMIAS :
Disturbances in automaticity : bertambah cepat atau bertambah
lambatnya suatu daerah otomatisitas. Misal di sinus node, AV node,
abnormal beats/ depolarisasi atrium, AV junction, ventrikel, VT,
dll.
Disturbances in conduction : konduksi terlalu cepat (WPW) atau
terlalu lambat (blok AV).
Combinations of altered automaticity and conduction.
Dr. Roy Martin SpAn.KIC
How to identify arrhythmias ?
Treat the patient, not the monitor
QRS complex Regular / irregular ?
QRS complexNormal-looking QRS complex?Wide / narrow ?P wave
?Relationship between P and QRS ?
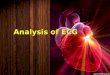
NORMAL SINUS RHYTHM
PSVT :
-due to re-entry mechanism-narrow QRS complex-regular-retrograde
atrial depolarization-P wave ?
PSVT
Atrial Fibrillation :
-from multiple area of re-entry within atria-or from multiple
ectopic foci-irregular, narrow QRS complex-very rapid atrial
electrical activity (400-700 x/min).-no uniform atrial
depolarization
Atrial Flutter :
The result of a re-entry circuit within the atriaIrregular /
regular QRS rateNarrow QRS complexRapid P waves (300x/min),
sawtooth
Junctional rhythm:
-AV junction can function as a pace maker (40-60 x/min).-due to
the failure of sinus node to initiate time impulse or conduction
problem.-normal-looking QRS.-retrograde P wave.-P wave may
preceede, coincide with, or follow the QRS
VESSR
SRSRSRSRSRSRVESVESSinus rhythm with Multifocal VES
Sinus rhythm with VES couplet
Sinus Rhythm with VES, R on T
THE BEAT GOES ON
Ventricular Tachycardia
Torsade de Pointes
Ventricular Fibrillation
Prolonged PR interval1st degree AV block
Missing QRS
Missing QRS2nd degree AV block, type 1
2nd degree AV block, type 2Missing QRS
PPPPPPPQRSQRSQRSTotal AV Block / 3rd degree AV block
PENGENALAN ARITMIAMONITORINGCEPAT dan TEPATSTATUS KLINIS??
MONIOR : VF / VT ?No: PEA,asistolYes
Untung gueUdah ikut Perioperative care
T
ARJOBambang Wahyu
VF dan VT pulseless90 % Kematian IMA Terjadi dalam 2 jam pertama
IMA Penatalaksanaan: 1. DEFIBRILASI 2. RJP termasuk ETT 3.
Farmakologis / obat-obatan* Epinefrin* Lidocaine, Amiodarone
JETSED P E ATERDAPAT AKTIFITAS ELEKTRIK JANTUNG, kecuali VT dan
VF , TETAPI TIDAK TERABA PULSASI Obat: EPINEFRIN SULFAS ATROPIN
AISSTOL
57