Embed Size (px)
DESCRIPTION
ECG Interpretation Part 2. Carolyn M. Malone RN,MSN,FNP-C. Review of Rhythms. Atrial Arrhythmia. Premature atria contraction or PAC impulse occurs earlier than predicted in the cycle causing the p-wave to look different. Usually does not require any treatment unless the patient is symptomatic. - PowerPoint PPT Presentation
Citation preview
ECG InterpretationECG InterpretationPart 2Part 2
Carolyn M. Malone Carolyn M. Malone RN,MSN,FNP-CRN,MSN,FNP-C

Review of RhythmsReview of Rhythms

Atrial ArrhythmiaAtrial Arrhythmia
Premature atria contraction or PAC Premature atria contraction or PAC impulse occurs earlier than predicted impulse occurs earlier than predicted in the cycle causing the p-wave to in the cycle causing the p-wave to look different. Usually does not look different. Usually does not require any treatment unless the require any treatment unless the patient is symptomaticpatient is symptomatic
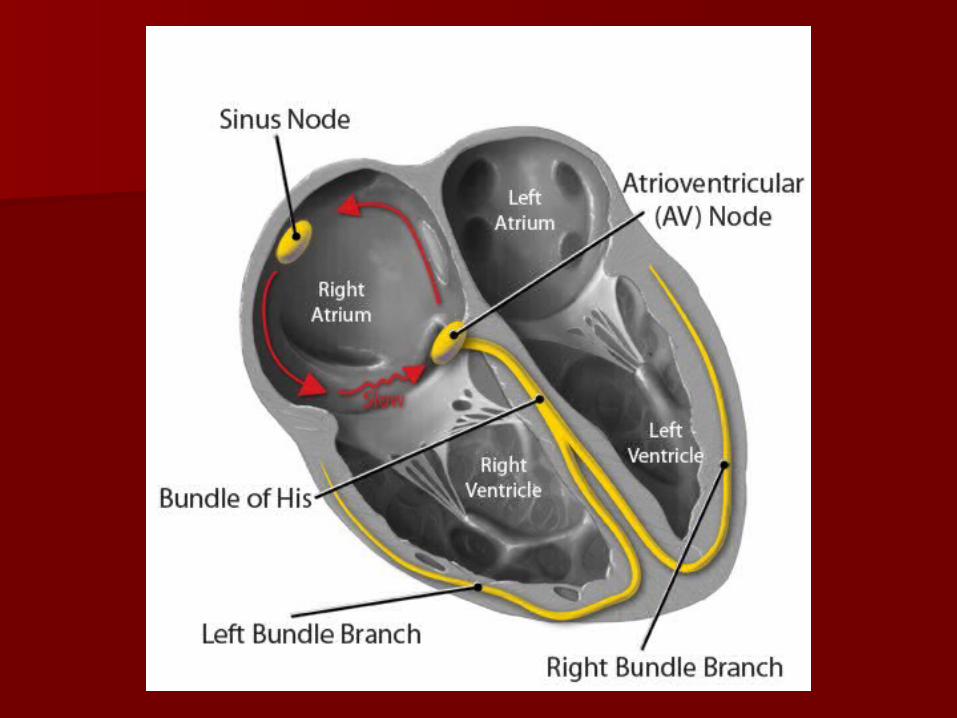
Atrial FlutterAtrial Flutter
Characterized by classis saw-toothed waves instead of classis p-Characterized by classis saw-toothed waves instead of classis p-wave. If there is a rapid ventricular response this rhythm is wave. If there is a rapid ventricular response this rhythm is grouped as Narrow Complex Tachycardia.grouped as Narrow Complex Tachycardia.
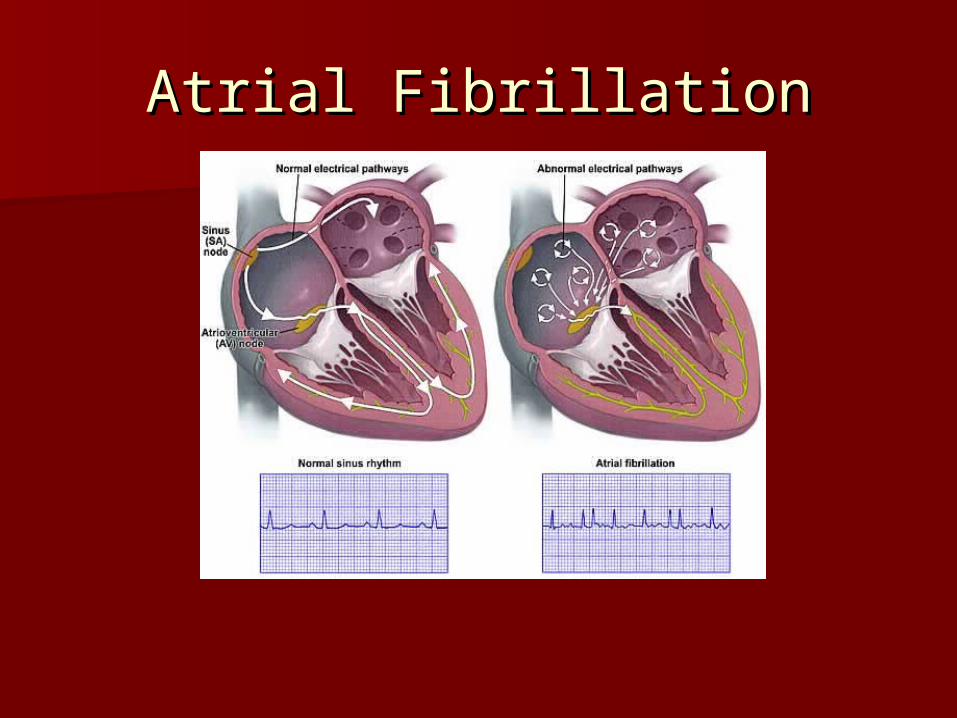
Atrial FibrillationAtrial Fibrillation
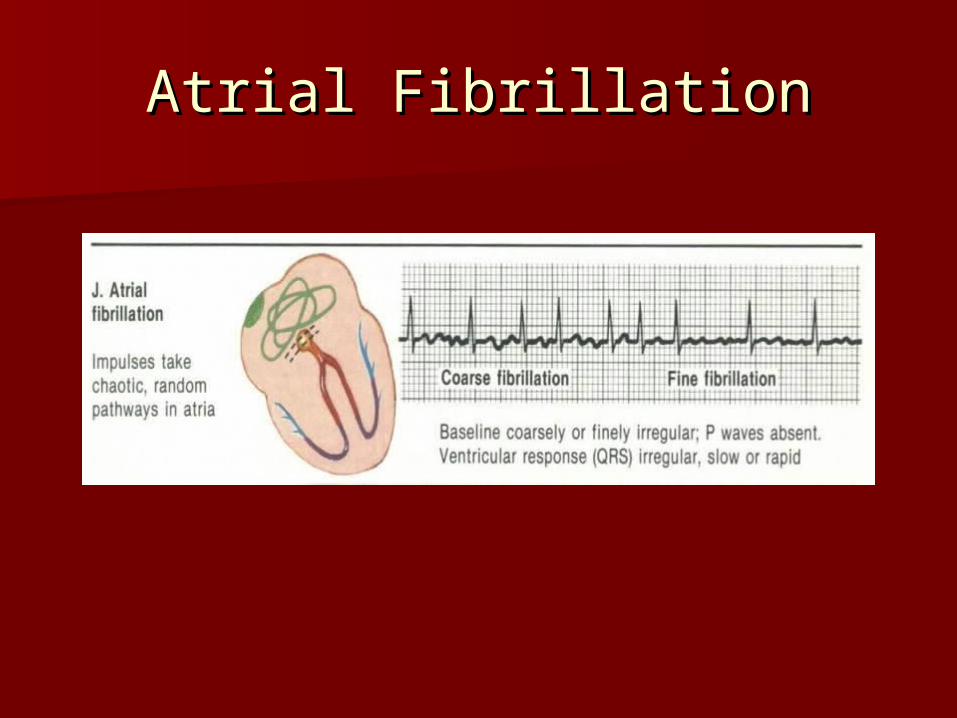
Atrial FibrillationAtrial Fibrillation

Narrow Complex Tachycardia Narrow Complex Tachycardia TreatmentTreatment
This term is assigned to This term is assigned to tachyarrhythmias with a narrow QRS tachyarrhythmias with a narrow QRS typically seen with atrial fibrillation typically seen with atrial fibrillation or atrial flutter with rapid ventricular or atrial flutter with rapid ventricular responses or A-Fir RVRresponses or A-Fir RVR
Assess ABC’S Assess ABC’S →→ apply oxygen apply oxygen →→place place patient on monitor patient on monitor →→ obtain blood obtain blood pressure and oximetry pressure and oximetry →→ obtain IV access obtain IV access Is the QRS narrow (0.12 seconds)?Is the QRS narrow (0.12 seconds)?
Narrow Complex Tachycardia Narrow Complex Tachycardia TreatmentTreatment
Is the rhythm regular? If yes attempt Is the rhythm regular? If yes attempt vagal maneuvers vagal maneuvers →→ administer administer Adenosine (Adenocard) 6mg rapid IV push Adenosine (Adenocard) 6mg rapid IV push prefer IV site at a/c level If not effective prefer IV site at a/c level If not effective may repeat at 12 mg IV rapid push. may repeat at 12 mg IV rapid push. Adenosine slows conduction time through Adenosine slows conduction time through the AV node and reentrant pathways the AV node and reentrant pathways restoring NSR. If the rhythm does convert restoring NSR. If the rhythm does convert continue to monitor the patient. If it does continue to monitor the patient. If it does not convert consider other medications.not convert consider other medications.
Narrow Complex Tachycardia Narrow Complex Tachycardia TreatmentTreatment
Diltiazem (Cardizem) inhibits calcium from Diltiazem (Cardizem) inhibits calcium from entering the slow channels during entering the slow channels during depolarization producing a relaxation of depolarization producing a relaxation of vascular smooth muscle and coronary vascular smooth muscle and coronary vasodilatation and increases myocardial oxygen vasodilatation and increases myocardial oxygen delivery in patients with vasospastic angina. delivery in patients with vasospastic angina.
Dose is typically 0.25mg/kg typically 20mg Dose is typically 0.25mg/kg typically 20mg bolus over 2 minutes may repeat at 0.35mg/kg, bolus over 2 minutes may repeat at 0.35mg/kg, usually 25mg bolus. If patient rhythm is not usually 25mg bolus. If patient rhythm is not resolve pt will require drip typically at resolve pt will require drip typically at 5-10mg/hr 5-10mg/hr

Narrow Complex Tachycardia Narrow Complex Tachycardia TreatmentTreatment
Verapamil (Calan) Inhibits calcium from Verapamil (Calan) Inhibits calcium from entering the slow channels during entering the slow channels during depolarization, produces relaxation of depolarization, produces relaxation of coronary smooth muscle and coronary coronary smooth muscle and coronary vasodilation, increases myocardial oxygen vasodilation, increases myocardial oxygen delivery, slows automaticity and delivery, slows automaticity and conduction of AV node.conduction of AV node.
Dose 2.5-5mg SIVP over 2 minutes second Dose 2.5-5mg SIVP over 2 minutes second dose at 5-10 mg 15-30 minutes after the dose at 5-10 mg 15-30 minutes after the first dose.first dose.
Narrow Complex Tachycardia Narrow Complex Tachycardia TreatmentTreatment
Betablockers Esmolol (Brevibloc). Betablockers Esmolol (Brevibloc). Competitively blocks response to Competitively blocks response to ββ1 1 adrenergic stimulation with little or adrenergic stimulation with little or no effect on no effect on ββ2 receptors except at 2 receptors except at high doses.high doses.
Dose is 500mcg/kg/min loading dose Dose is 500mcg/kg/min loading dose followed by a 50mcg/kg/min for 4 followed by a 50mcg/kg/min for 4 minutes and continue to increase at minutes and continue to increase at 50mcg/kg/min to achieve rate 50mcg/kg/min to achieve rate control.control.
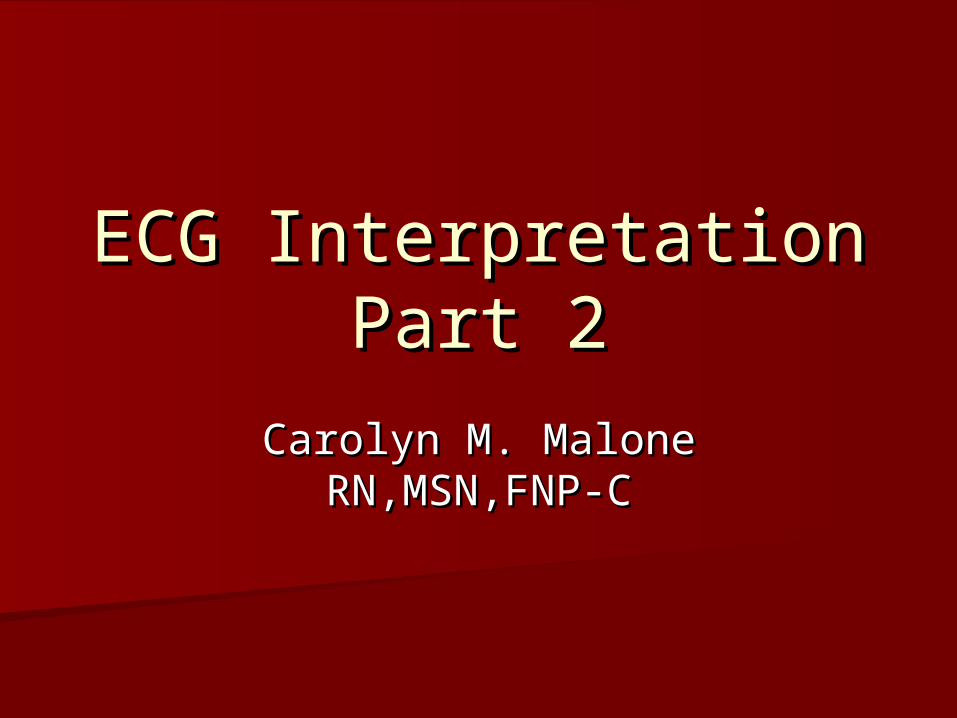
Intro to AV BlocksIntro to AV Blocks
It is the AV Node that is diseased in It is the AV Node that is diseased in atrioventricular blocks. The SA node atrioventricular blocks. The SA node usually functions normally.usually functions normally.– Since the SA node is not affected in AV Since the SA node is not affected in AV
blocks, the P waves occur at regular blocks, the P waves occur at regular rhythm.rhythm.
AV BlocksAV Blocks
Since the PR interval reflects the Since the PR interval reflects the impulse traveling through the AV impulse traveling through the AV node this measurement is one of the node this measurement is one of the criteria used to determine the type of criteria used to determine the type of AV block that is present.AV block that is present.– A prolonged PR interval signifies first-A prolonged PR interval signifies first-
degree AV block.degree AV block.
AV BlocksAV Blocks
There are three levels of AV block: There are three levels of AV block: first-degree, second-degree, and first-degree, second-degree, and third-degree AV Block.third-degree AV Block.
The number and pattern of impulses The number and pattern of impulses conducted through the AV node conducted through the AV node determines the presence and degree determines the presence and degree of AV block.of AV block.
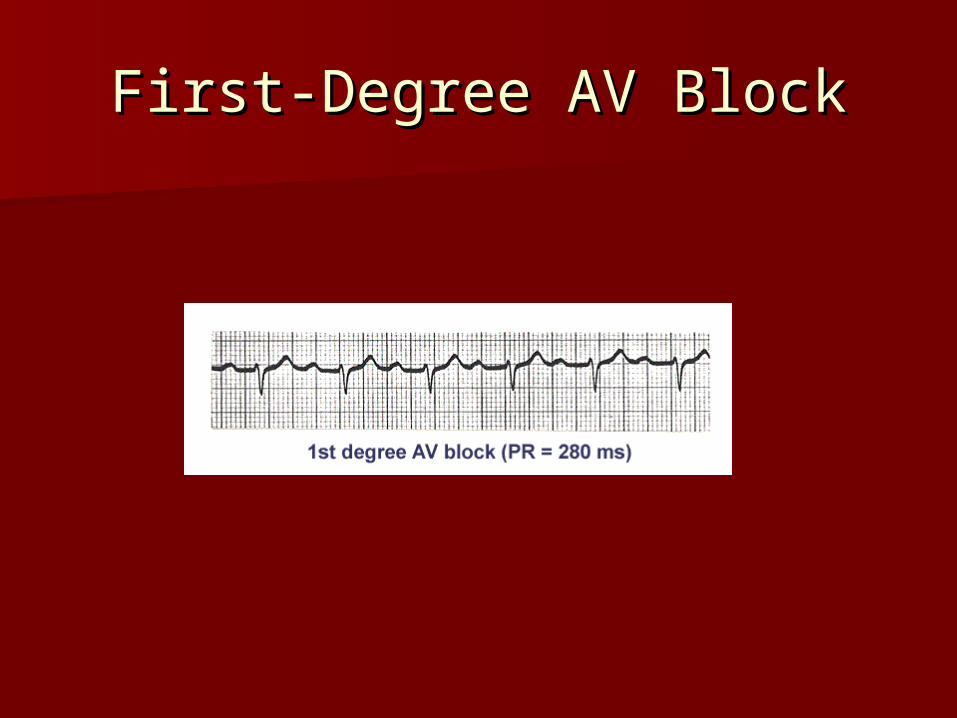
First-Degree AV BlockFirst-Degree AV Block
First-Degree AV BlockFirst-Degree AV Block
In first-degree AV Block, there is a 1:1 ratio In first-degree AV Block, there is a 1:1 ratio between P waves and QRS complexes. between P waves and QRS complexes.
All of the impulses are conducted to the All of the impulses are conducted to the ventricles, but are delayed in the AV node.ventricles, but are delayed in the AV node.– The delay results in a prolonged PR interval.The delay results in a prolonged PR interval.– The occurrence of first-degree AV block will be The occurrence of first-degree AV block will be
noted in addition to your interpretation of the noted in addition to your interpretation of the patient’s basic rhythm. There is no tx.patient’s basic rhythm. There is no tx.

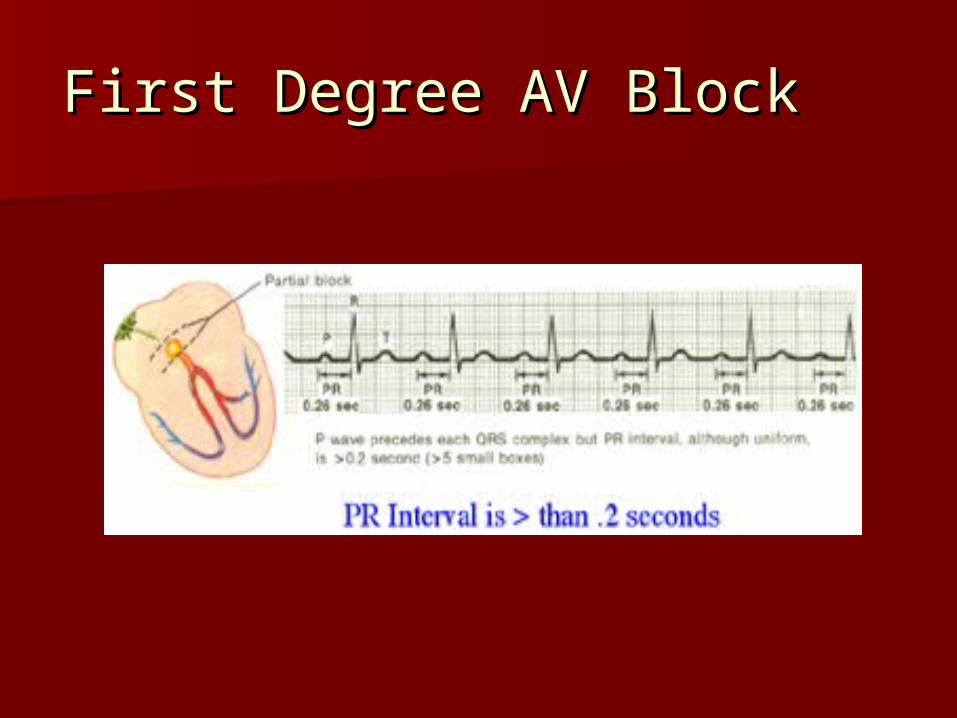
ECG Criteria: First-Degree AV ECG Criteria: First-Degree AV BlockBlock
P waves: similar, 1:1 with QRSP waves: similar, 1:1 with QRS Rhythm: Atrial – regularRhythm: Atrial – regular
Ventricular - regularVentricular - regular Rate: Usually 60-100/minuteRate: Usually 60-100/minute PR: greater than 0.20 second PR: greater than 0.20 second
(prolonged)(prolonged) QRS: 0.04-0.10 second (normal)QRS: 0.04-0.10 second (normal) QT: 0.32-0.44 second (normal)QT: 0.32-0.44 second (normal)
First Degree AV BlockFirst Degree AV Block
Possible Causes of Possible Causes of First-Degree AV BlockFirst-Degree AV Block
Conduction system diseaseConduction system disease Digitalis administrationDigitalis administration Antiarrhythmics, such as quinidine Antiarrhythmics, such as quinidine
and Amiodaroneand Amiodarone Acute MIAcute MI

Treatment First-Degree AV Treatment First-Degree AV BlockBlock
Treat underlying causeTreat underlying cause O2, Atropine for symptomatic O2, Atropine for symptomatic
bradycardiabradycardia

Second Degree AV BlockSecond Degree AV Block
There are 2 type of second-degree AV block:There are 2 type of second-degree AV block:– Mobitz I (also called Type I or Wenckebach)Mobitz I (also called Type I or Wenckebach)– Mobitz II (also called Type II)Mobitz II (also called Type II)
The PR interval abnormality differentiate the The PR interval abnormality differentiate the two rhythms.two rhythms.
Mobitz II is a more serious dysrhythmia Mobitz II is a more serious dysrhythmia because the causes more often result in because the causes more often result in permanent changes. Mobitz II is also more permanent changes. Mobitz II is also more likely to develop into complete or third-likely to develop into complete or third-degree AV block.degree AV block.
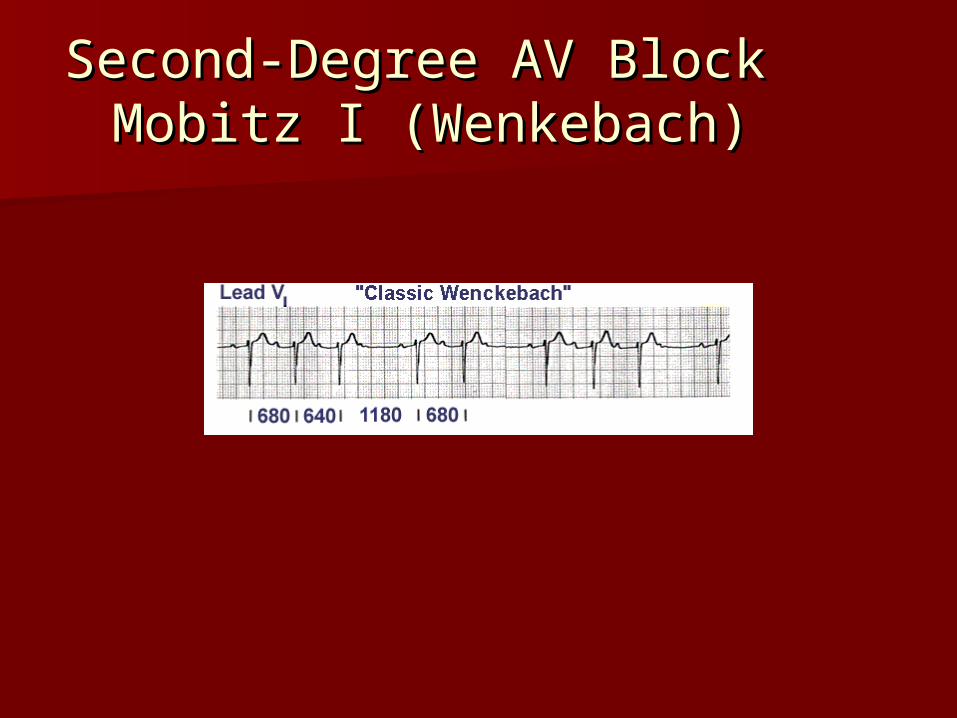
Second-Degree AV Block Second-Degree AV Block Mobitz I (Wenkebach)Mobitz I (Wenkebach)

Second Degree AV Block Second Degree AV Block Mobitz IMobitz I
Mobitz I - WenckebachMobitz I - Wenckebach
With Mobitz I, the PR interval gradually With Mobitz I, the PR interval gradually lengthens until an impulse is not lengthens until an impulse is not conducted. You will see a P wave without conducted. You will see a P wave without a corresponding QRS complex. The R-to-R a corresponding QRS complex. The R-to-R shortens until a QRS is dropped.shortens until a QRS is dropped.
It is as though the AV node is warning It is as though the AV node is warning that soon an impulse won’t get through. that soon an impulse won’t get through. – The P wave may be buried in another wave.The P wave may be buried in another wave.

ECG Criteria Mobitz Type I ECG Criteria Mobitz Type I Second Degree AV BlockSecond Degree AV Block
P waves: similar – more P waves than P waves: similar – more P waves than QRS’sQRS’s
Rhythm: Atrial – regularRhythm: Atrial – regular Ventricular - irregularVentricular - irregular Rate: Atrial: usually 60-100/minuteRate: Atrial: usually 60-100/minute
Ventricular – depends on the number Ventricular – depends on the number of blocked impulses; will be less than atrialof blocked impulses; will be less than atrial
PR: gradually increases until there is a P PR: gradually increases until there is a P wave with no QRS; it is a cyclic pattern.wave with no QRS; it is a cyclic pattern.
QRS: 0.04-0.10 second (normal)QRS: 0.04-0.10 second (normal) QT: 0.32-0.44 second (normal)QT: 0.32-0.44 second (normal)

Second-Degree AV Block Second-Degree AV Block Type IType I
Possible Causes for Mobitz IPossible Causes for Mobitz I
Increased vagal stimulation (such as Increased vagal stimulation (such as vomiting or straining)vomiting or straining)
Post myocardial infarction (usually Post myocardial infarction (usually inferior wall of left ventricle)inferior wall of left ventricle)
Medications (such as digitalis, beta-Medications (such as digitalis, beta-blockers, Quinidine, Procainamide)blockers, Quinidine, Procainamide)

Treatment - Mobitz Type ITreatment - Mobitz Type I
No treatment is usually needed for No treatment is usually needed for Mobitz I as the rhythm is well-tolerated. Mobitz I as the rhythm is well-tolerated. Assess ABC’S apply oxygen, place the Assess ABC’S apply oxygen, place the
patient on the monitor and oximetry, patient on the monitor and oximetry, establish IV access obtain blood establish IV access obtain blood pressure monitor for s&s of instability pressure monitor for s&s of instability i.e chest pain, SOB, hypotension, chest i.e chest pain, SOB, hypotension, chest pain, signs of shock, continue to pain, signs of shock, continue to monitor AV block, such as Mobitz II or monitor AV block, such as Mobitz II or third degree.third degree.

Second-Degree AV Block Second-Degree AV Block Mobitz Type IIMobitz Type II

Second-Degree AV Block Second-Degree AV Block Mobitz IIMobitz II
With Mobitz II, the PR interval is With Mobitz II, the PR interval is constant, but some impulses are not constant, but some impulses are not conducted. There are P waves conducted. There are P waves without QRS complexes. Unlike without QRS complexes. Unlike Mobitz I there is no warning that Mobitz I there is no warning that some of the impulses will be blocked.some of the impulses will be blocked.

ECG Criteria: Mobitz II Second-ECG Criteria: Mobitz II Second-Degree AV BlockDegree AV Block
P waves: similar, more P waves that QRSP waves: similar, more P waves that QRS Rhythm: Atrial – regularRhythm: Atrial – regular
Ventricular - irregularVentricular - irregular Rate: Atrial – usually 60-100/minuteRate: Atrial – usually 60-100/minute Ventricular – depends on the number of Ventricular – depends on the number of
blocked impulses; will be less that atrial rateblocked impulses; will be less that atrial rate PR: constant for conducted beatsPR: constant for conducted beats QRS: may be normal but often > 0.10 secondQRS: may be normal but often > 0.10 second QT: 0.32-0.44 second (normal)QT: 0.32-0.44 second (normal)

Second-Degree AV Block Second-Degree AV Block Type IIType II
Possible Causes for Mobitz IIPossible Causes for Mobitz II Acute Myocardial Infarction – usually Acute Myocardial Infarction – usually
anterior wall of left ventricleanterior wall of left ventricle HypoxiaHypoxia Chronic hypertensionChronic hypertension Ischemic heart failureIschemic heart failure
Symptoms depend on frequency of dropped Symptoms depend on frequency of dropped beats/ventricular ratebeats/ventricular rate
The causes of Mobitz II are likely due to The causes of Mobitz II are likely due to irreversible damage to the conduction irreversible damage to the conduction systemsystem

TreatmentTreatment The physician should be notified as soon as The physician should be notified as soon as
possible when this rhythm develops. Mobitz possible when this rhythm develops. Mobitz II is often associated with a poor prognosis II is often associated with a poor prognosis since development of complete AV block since development of complete AV block should be anticipated. A temporary should be anticipated. A temporary pacemaker may be inserted pacemaker may be inserted prophylactically/permanentlyprophylactically/permanently
Assess ABC’S provide oxygen, place on monitor Assess ABC’S provide oxygen, place on monitor establish rhythm obtain blood pressure, oximetry, establish rhythm obtain blood pressure, oximetry, obtain IV access obtain IV access
Atropine dose is 0.5mg may be repeated up to a Atropine dose is 0.5mg may be repeated up to a total of 3mg prepare to transcutaneous pace total of 3mg prepare to transcutaneous pace
Epinephrine 2-10mcg/min Dopamine Epinephrine 2-10mcg/min Dopamine 2-10mcg/kg/min vasoactive drips2-10mcg/kg/min vasoactive drips
Third Degree AV BlockThird Degree AV Block
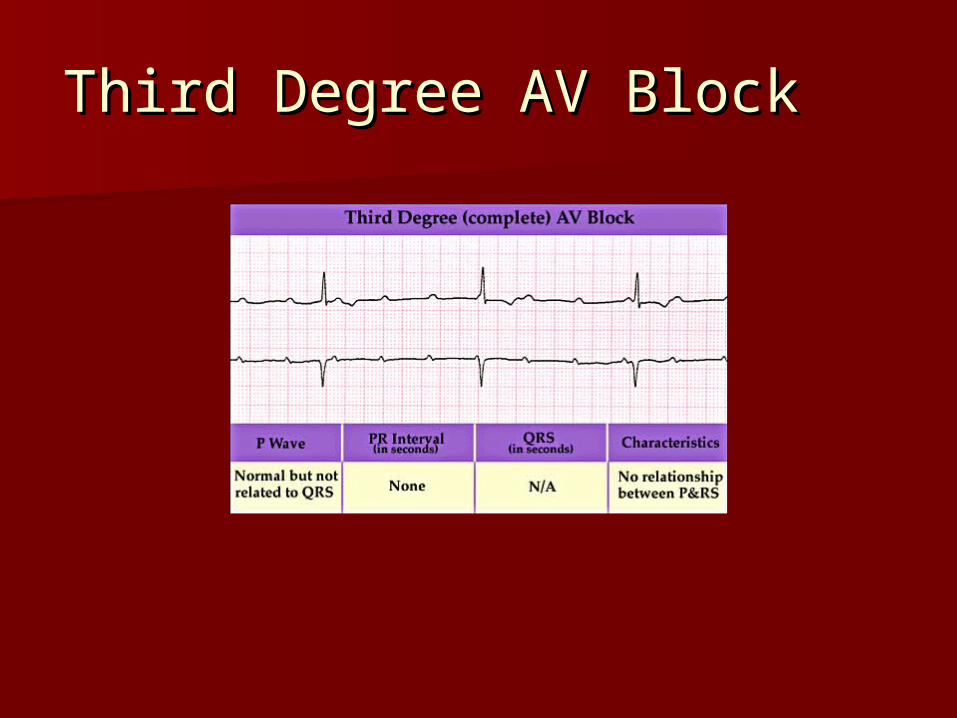
Third-Degree AV BlockThird-Degree AV Block
Complete (or third-degree) AV block Complete (or third-degree) AV block indicated absence of conduction indicated absence of conduction between the atria and ventricles.between the atria and ventricles.
The block can be in the AV node or in The block can be in the AV node or in the bundle of His. The atria are the bundle of His. The atria are paced by the SA Node and an paced by the SA Node and an independent pacemaker generates independent pacemaker generates impulses for the ventricles. Thus, impulses for the ventricles. Thus, the atrial and ventricular the atrial and ventricular contractions are not synchronized.contractions are not synchronized.
Third degree AV BlockThird degree AV Block
The ECG rhythm is characterized by The ECG rhythm is characterized by separate, but regular, atrial and separate, but regular, atrial and ventricular rhythms and rates. ventricular rhythms and rates. Because of the different rates and Because of the different rates and because there are two separate because there are two separate pacemakers, there is no correlation pacemakers, there is no correlation between the P waves and the QRS between the P waves and the QRS complexes. As a results, there is no complexes. As a results, there is no true PR interval.true PR interval.

ECG Criteria: Third-Degree AV ECG Criteria: Third-Degree AV BlockBlock
P waves: similar – more P waves than QRS’sP waves: similar – more P waves than QRS’s Rhythm: Atrial – regularRhythm: Atrial – regular Ventricular - regularVentricular - regular Rate: Atrial – usually 60-100/minRate: Atrial – usually 60-100/min Ventricular – usually less than 40/min; Ventricular – usually less than 40/min;
it can be up to 60/min if the block is high in it can be up to 60/min if the block is high in the AV nodethe AV node
PR: varies – no true PR interval since atria PR: varies – no true PR interval since atria and ventricles conducting independentlyand ventricles conducting independently
QRS: Greater than 0.10 secondQRS: Greater than 0.10 second QT: may be normal or prolongedQT: may be normal or prolonged

Third-Degree AV BlockThird-Degree AV Block
Possible Causes for Third-Possible Causes for Third-Degree AV BlockDegree AV Block
Extensive myocardial infarction (usually Extensive myocardial infarction (usually anterior wall of the left ventricle)anterior wall of the left ventricle)
AcidosisAcidosis HypoxiaHypoxia HyperkalemiaHyperkalemia Digitalis toxicityDigitalis toxicity Extensive ventricular conduction Extensive ventricular conduction
system diseasesystem disease
Treatment – Third-Degree Treatment – Third-Degree BlockBlock
The MD should be notified immediately when The MD should be notified immediately when third-degree heart block develops. The third-degree heart block develops. The patient may not tolerate a sudden decrease patient may not tolerate a sudden decrease in cardiac output associated with the slow in cardiac output associated with the slow rate.rate.
Because the independent ventricular Because the independent ventricular pacemaker may be unreliable and may result pacemaker may be unreliable and may result in periods of asystole, third-degree heart in periods of asystole, third-degree heart block may become a lethal dysrhythmias.block may become a lethal dysrhythmias.
A temporary transcutaneous or transvenous A temporary transcutaneous or transvenous pacemaker is usually inserted. A permanent pacemaker is usually inserted. A permanent cardiac pacemaker is often necessary. cardiac pacemaker is often necessary.

Treatment – Third-Degree Treatment – Third-Degree BlockBlock
Assess ABC’S Assess ABC’S →→ administer oxygen administer oxygen →→ obtain obtain blood pressure, place on ECG monitor oximetry blood pressure, place on ECG monitor oximetry →→ establish IV access establish IV access →→ assess perfusion assess perfusion status i.e. chest pain, mental status, status i.e. chest pain, mental status, hypotension, signs of shock hypotension, signs of shock →→ prepare for prepare for transcutaneous pacing transcutaneous pacing →→ consider Atropine at consider Atropine at 0.5mg IV may repeat for a total dose of 3mg 0.5mg IV may repeat for a total dose of 3mg →→ consider Epinephrine drip at 2-10mcg/min or consider Epinephrine drip at 2-10mcg/min or Dopamine 2-10mcg/kg/min while waiting for Dopamine 2-10mcg/kg/min while waiting for pacer or if pacing is ineffective.pacer or if pacing is ineffective.
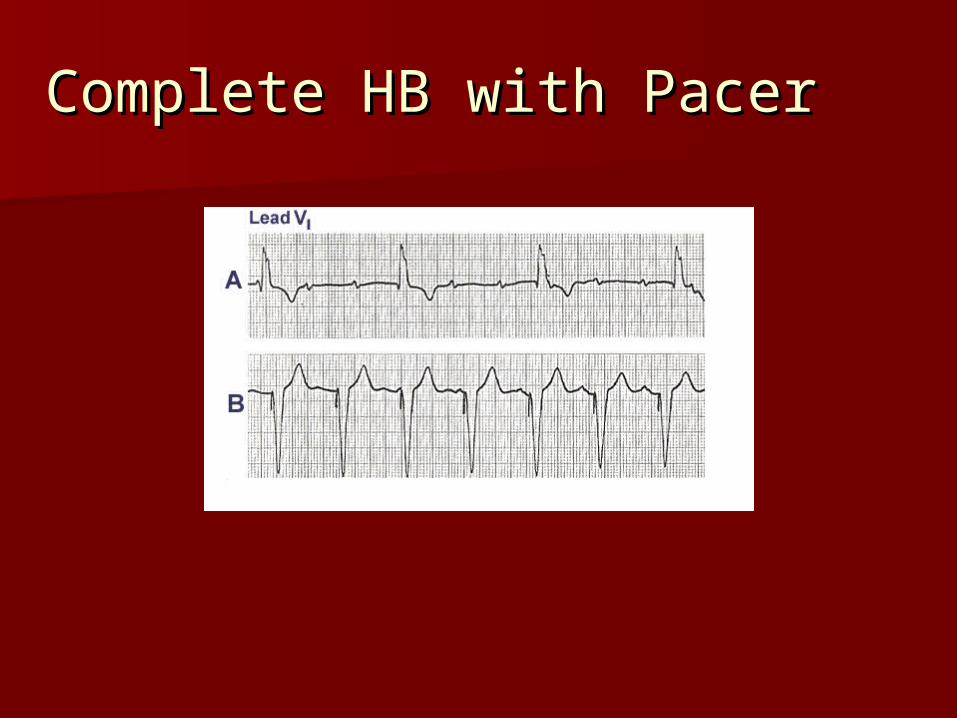
Complete HB with PacerComplete HB with Pacer
Modes of PacingModes of Pacing
Synchronous (demand) pacingSynchronous (demand) pacing1. Temporary pacing most common1. Temporary pacing most common2. Pacemaker's sensitivity set to client's beats2. Pacemaker's sensitivity set to client's beats3. If intrinsic rate is 3. If intrinsic rate is rate set, the pacemaker is rate set, the pacemaker is
inhibited from firinginhibited from firing4. If intrinsic rate is 4. If intrinsic rate is rate set, pacemaker fires to rate set, pacemaker fires to
stimulate depolarizationstimulate depolarization Asynchronous (fixed rate)Asynchronous (fixed rate)
1. Used for asystole or profound bradycardia1. Used for asystole or profound bradycardia2. Fires at a fixed rate regardless of client's intrinsic 2. Fires at a fixed rate regardless of client's intrinsic
rhythmrhythm3. Complications: pacemaker competition, R-on-T 3. Complications: pacemaker competition, R-on-T
phenomenonphenomenon
34-2434-24
Noninvasive Temporary Pacing (NTP)Noninvasive Temporary Pacing (NTP)
Two large patch electrodes attached to an external Two large patch electrodes attached to an external pulse generatorpulse generator
Electrical pulses transmitted transcutaneously to Electrical pulses transmitted transcutaneously to stimulate depolarization stimulate depolarization
Used as an emergency measure or prophylacticallyUsed as an emergency measure or prophylactically Complications: discomfort from cutaneous/muscle Complications: discomfort from cutaneous/muscle
stimulation, skin irritation and diaphoresis from stimulation, skin irritation and diaphoresis from patchespatches
Loss of captureLoss of capture Inappropriate pacingInappropriate pacing
34-2534-25
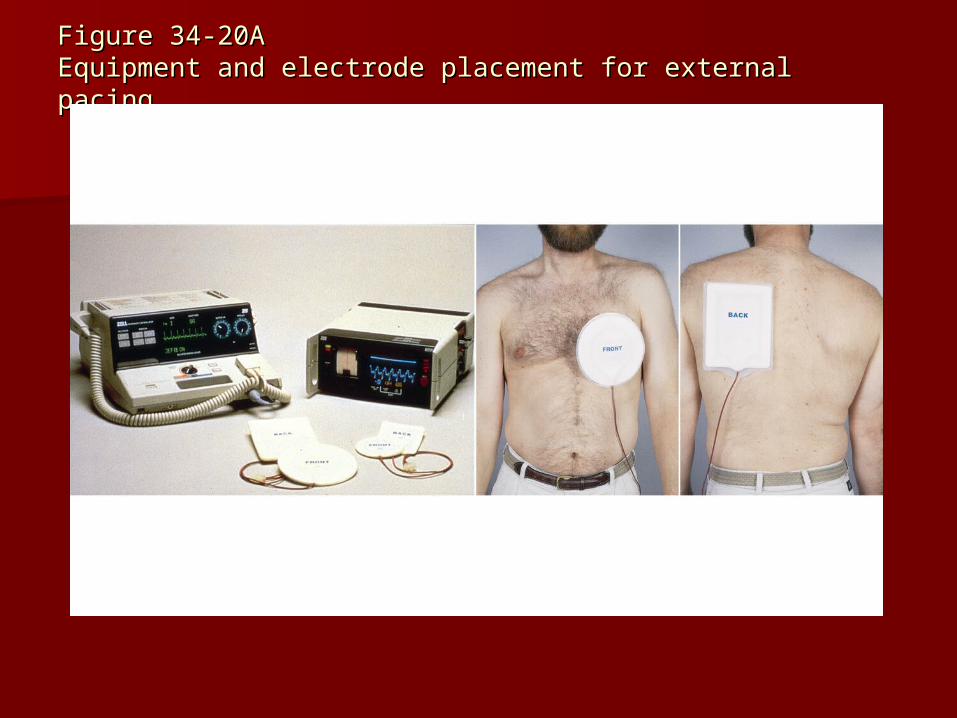
Figure 34-20AFigure 34-20AEquipment and electrode placement for external pacingEquipment and electrode placement for external pacing
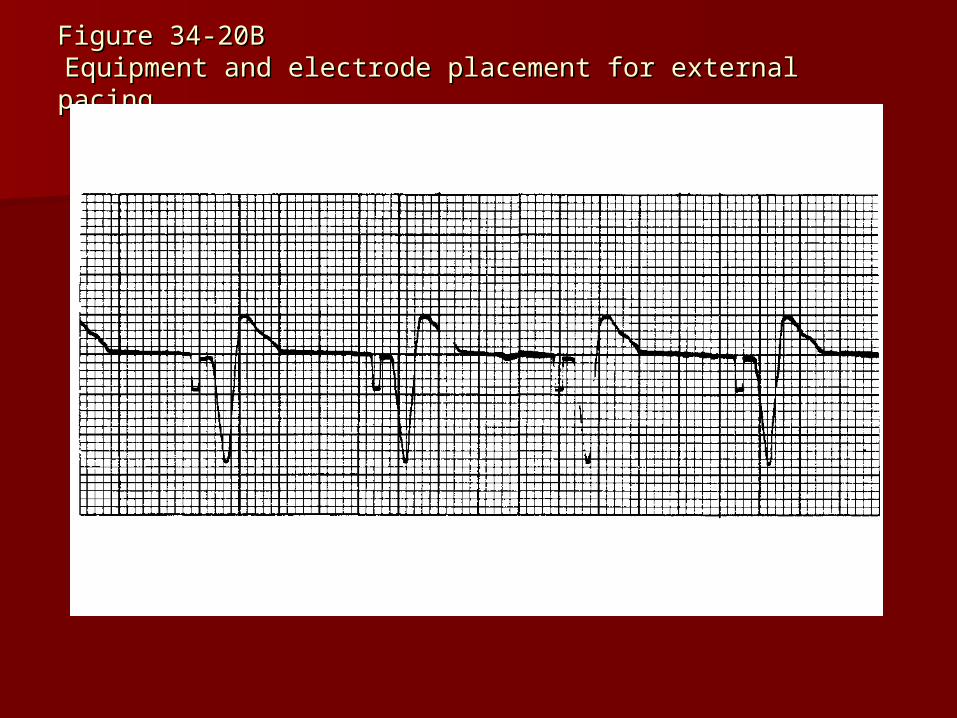
Figure 34-20BFigure 34-20B Equipment and electrode placement for external pacingEquipment and electrode placement for external pacing
Invasive Temporary PacingInvasive Temporary Pacing
Transvenous pacingTransvenous pacing Epicardial pacingEpicardial pacing Complications:Complications:
1. Infection/hematoma1. Infection/hematoma
2. Ectopic complexes2. Ectopic complexes
3. Loss of capture3. Loss of capture
4. Under-sensing/pacemaker competition/over-sensing4. Under-sensing/pacemaker competition/over-sensing
5. Electromagnetic interference5. Electromagnetic interference
6. Stimulation of chest wall or diaphragm6. Stimulation of chest wall or diaphragm
34-2634-26
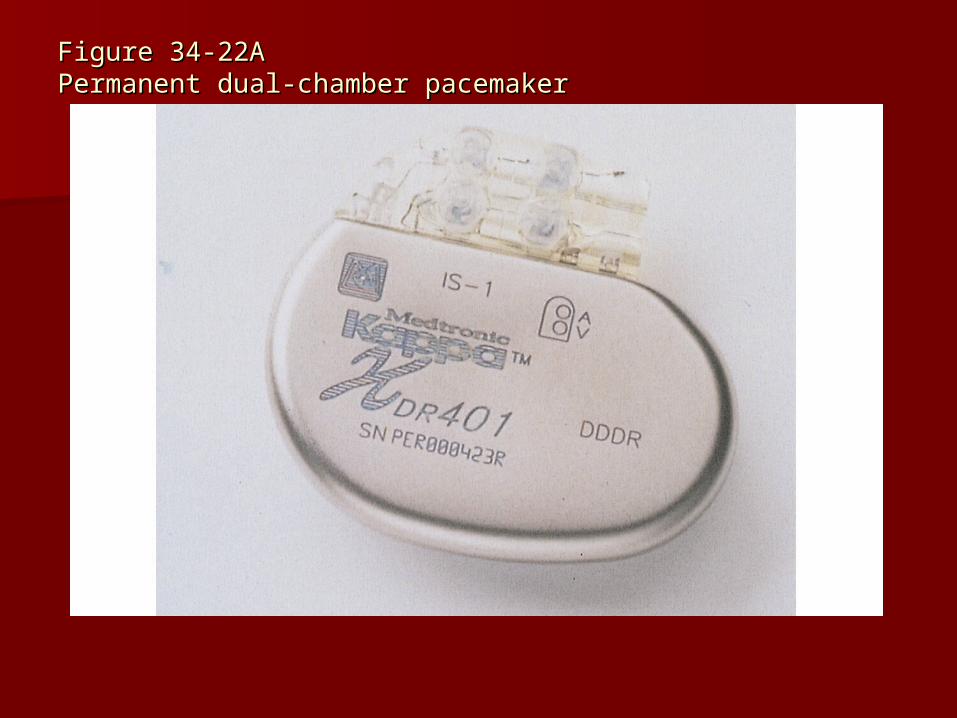
Figure 34-22AFigure 34-22APermanent dual-chamber pacemakerPermanent dual-chamber pacemaker
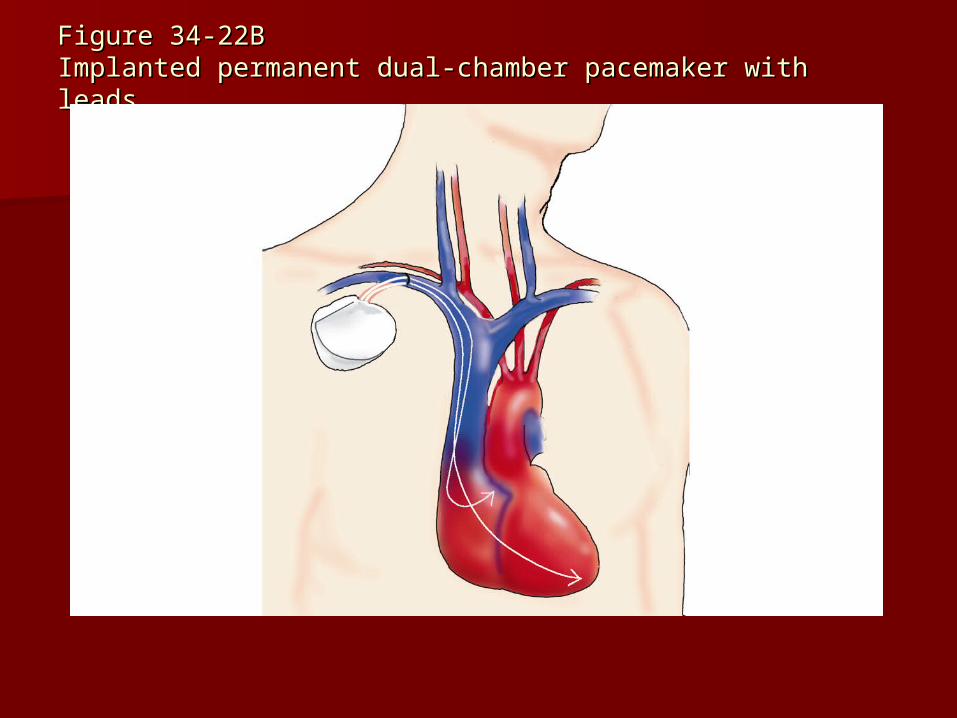
Figure 34-22BFigure 34-22BImplanted permanent dual-chamber pacemaker with leadsImplanted permanent dual-chamber pacemaker with leads
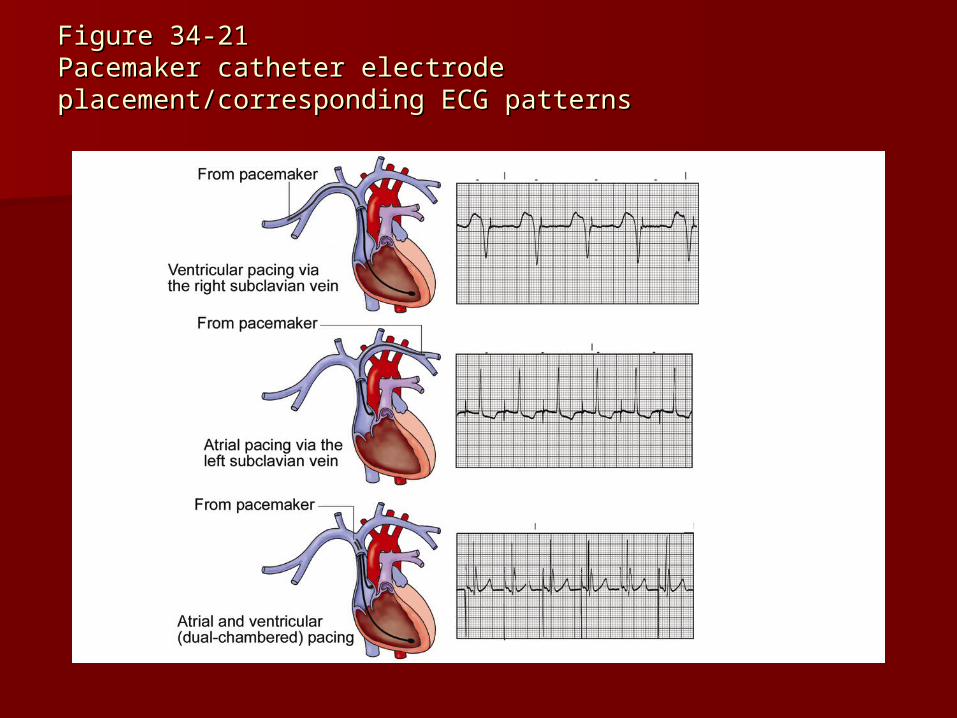
Figure 34-21Figure 34-21Pacemaker catheter electrode placement/corresponding Pacemaker catheter electrode placement/corresponding ECG patternsECG patterns
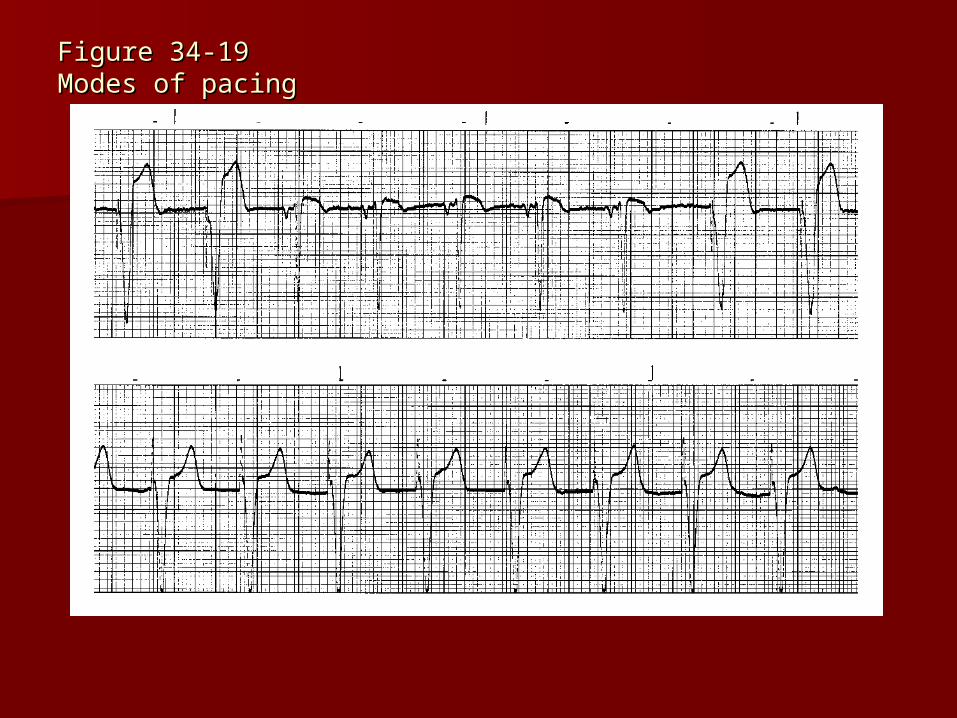
Figure 34-19Figure 34-19Modes of pacingModes of pacing
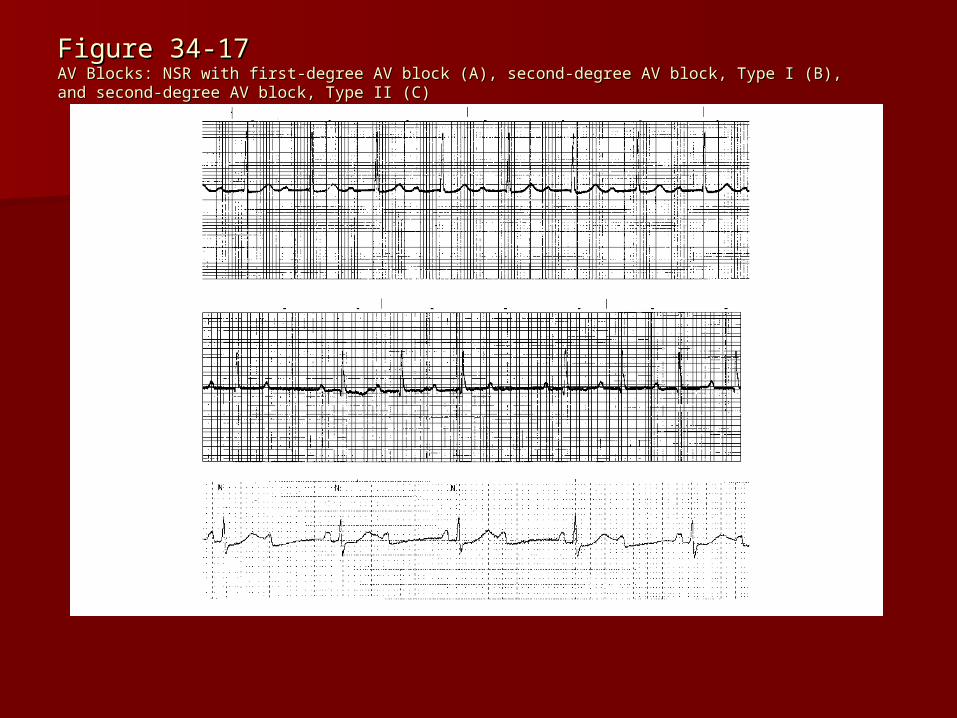
Figure 34-17Figure 34-17AV Blocks: NSR with first-degree AV block (A), second-degree AV block, Type I (B), and second-AV Blocks: NSR with first-degree AV block (A), second-degree AV block, Type I (B), and second-degree AV block, Type II (C)degree AV block, Type II (C)
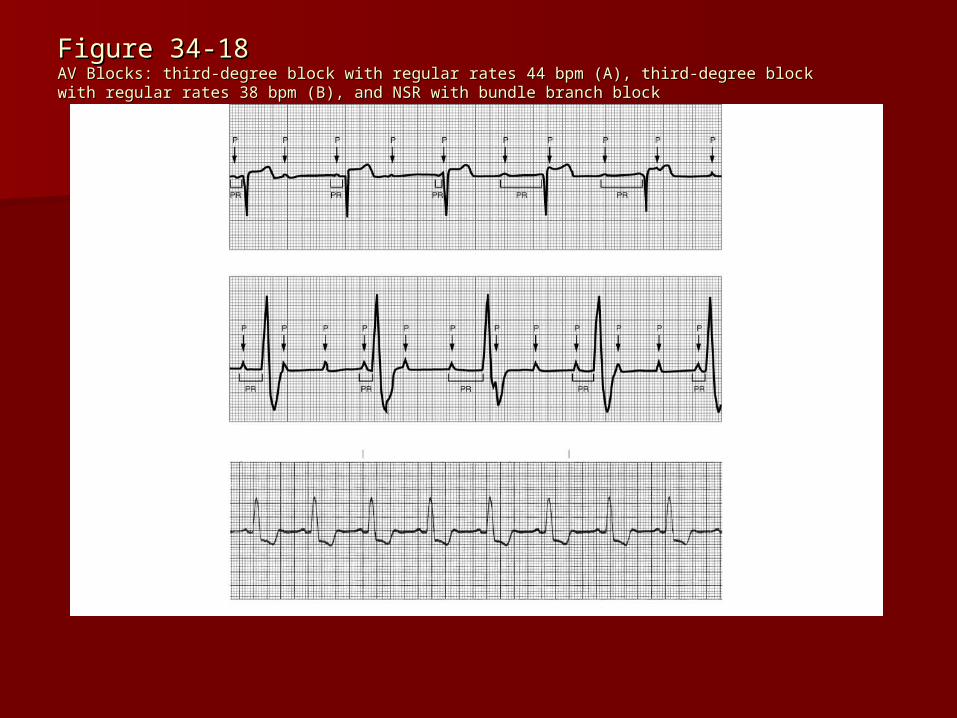
Figure 34-18Figure 34-18AV Blocks: third-degree block with regular rates 44 bpm (A), third-degree block with regular rates AV Blocks: third-degree block with regular rates 44 bpm (A), third-degree block with regular rates 38 bpm (B), and NSR with bundle branch block38 bpm (B), and NSR with bundle branch block
AsystoleAsystole
Asystole, a lethal dysrhythmia, is Asystole, a lethal dysrhythmia, is characterized by the absence of any characterized by the absence of any ventricular activity. It is also called ventricular activity. It is also called straight line.straight line.
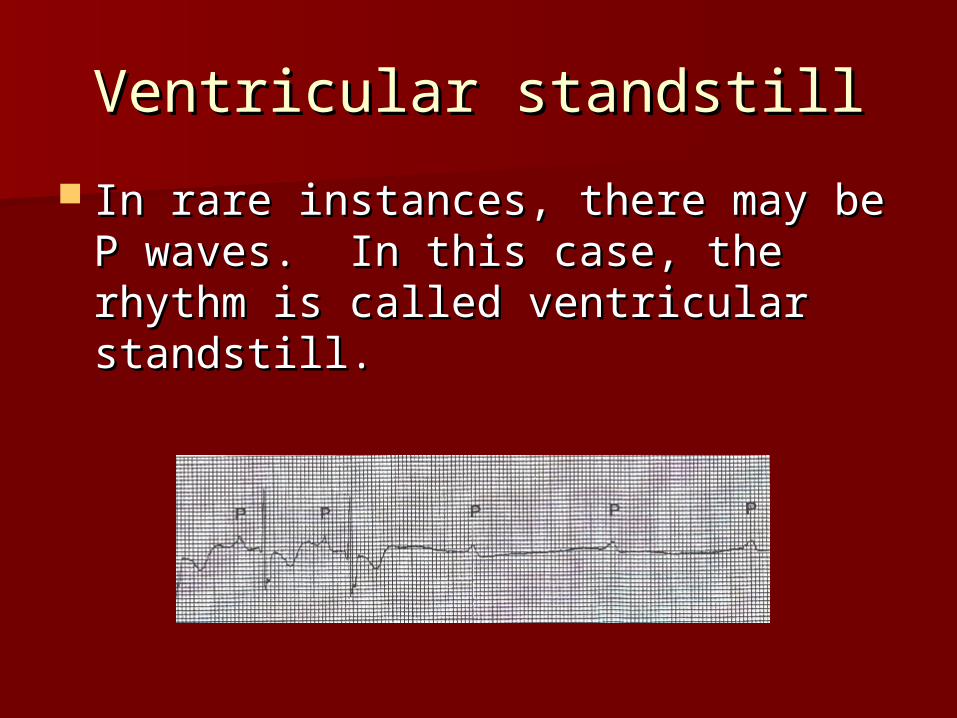
Ventricular standstillVentricular standstill
In rare instances, there may be P In rare instances, there may be P waves. In this case, the rhythm is waves. In this case, the rhythm is called ventricular standstill.called ventricular standstill.
Possible Causes of AsystolePossible Causes of Asystole
Severe hemorrhageSevere hemorrhage Air EmbolismAir Embolism Heart failureHeart failure Myocardial InfarctionMyocardial Infarction Electrical shockElectrical shock Severe acidosisSevere acidosis Ventricular dysrhythmiaVentricular dysrhythmia Cocaine overdoseCocaine overdose
TreatmentTreatment Asystole is lethal if not treated immediately Asystole is lethal if not treated immediately
often it is lethal even when treated often it is lethal even when treated accurately and aggressively. Treatment accurately and aggressively. Treatment consisted of initiation of CPR and the cardiac consisted of initiation of CPR and the cardiac arrest protocols.arrest protocols.
Assess ABC’S initiate CPR hard and fast Assess ABC’S initiate CPR hard and fast assess if shockable rhythm if not resume CPR assess if shockable rhythm if not resume CPR for 5 cycles administer epinephrine 1mg for 5 cycles administer epinephrine 1mg 10:10,000 q3-5 minutes after or during CPR 10:10,000 q3-5 minutes after or during CPR cycles and consider Atropine 1mg may repeat cycles and consider Atropine 1mg may repeat q3-5 minutes for a total of 3mg. Consider q3-5 minutes for a total of 3mg. Consider reversible causes 6H’s and 5 T’s reversible causes 6H’s and 5 T’s
Pulse Electrical ActivityPulse Electrical Activity(PEA)(PEA)
Formerly termed EMD, or electrical Formerly termed EMD, or electrical mechanical dissociation, is the term mechanical dissociation, is the term used to describe electrical activity used to describe electrical activity without mechanical contraction. without mechanical contraction. Always assess the patient for a pulse. Always assess the patient for a pulse. There may be electrical activity, but There may be electrical activity, but if there is no myocardial contraction if there is no myocardial contraction there will be no pulse, no cardiac there will be no pulse, no cardiac output, and no blood pressure.output, and no blood pressure.
Treatment – search for Treatment – search for underlying causesunderlying causes
6 H’s6 H’s– HypovolemiaHypovolemia– HypoxiaHypoxia– Hydrogen Ion (acidosis)Hydrogen Ion (acidosis)– Hyper-hypokalemiaHyper-hypokalemia– HypoglycemiaHypoglycemia– HypothermiaHypothermia
5 T’s5 T’s– ToxinsToxins– Tamponade (cardiac)Tamponade (cardiac)– Tension PneumothoraxTension Pneumothorax– Thrombosis (coronary and pulmonary)Thrombosis (coronary and pulmonary)– TraumaTrauma
Ventricular DysrhythmiasVentricular Dysrhythmias
PVC’s can occur with PVC’s can occur with a specific pattern. a specific pattern. Characterized as a Characterized as a wide QRS that occurs wide QRS that occurs early in the cycle early in the cycle followed by a followed by a compensatory pause.compensatory pause.
Identify the Identify the underlying rhythm, underlying rhythm, often NSRoften NSR
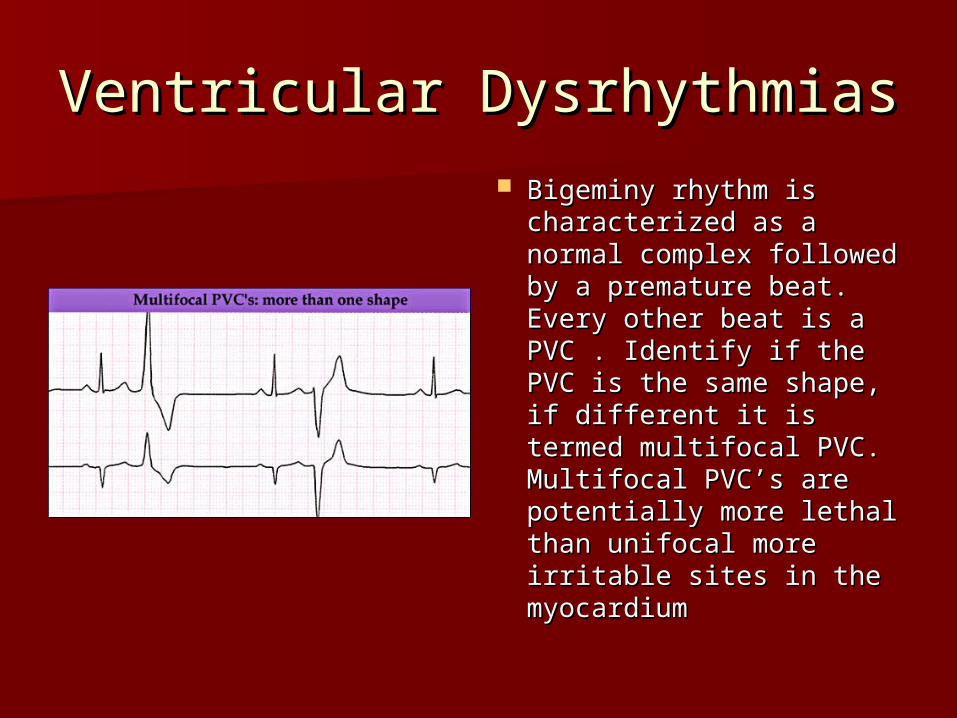
Ventricular DysrhythmiasVentricular Dysrhythmias Bigeminy rhythm is Bigeminy rhythm is
characterized as a characterized as a normal complex followed normal complex followed by a premature beat. by a premature beat. Every other beat is a PVC Every other beat is a PVC . Identify if the PVC is the . Identify if the PVC is the same shape, if different same shape, if different it is termed multifocal it is termed multifocal PVC. Multifocal PVC’s are PVC. Multifocal PVC’s are potentially more lethal potentially more lethal than unifocal more than unifocal more irritable sites in the irritable sites in the myocardium myocardium
Ventricular DysrhythmiasVentricular Dysrhythmias
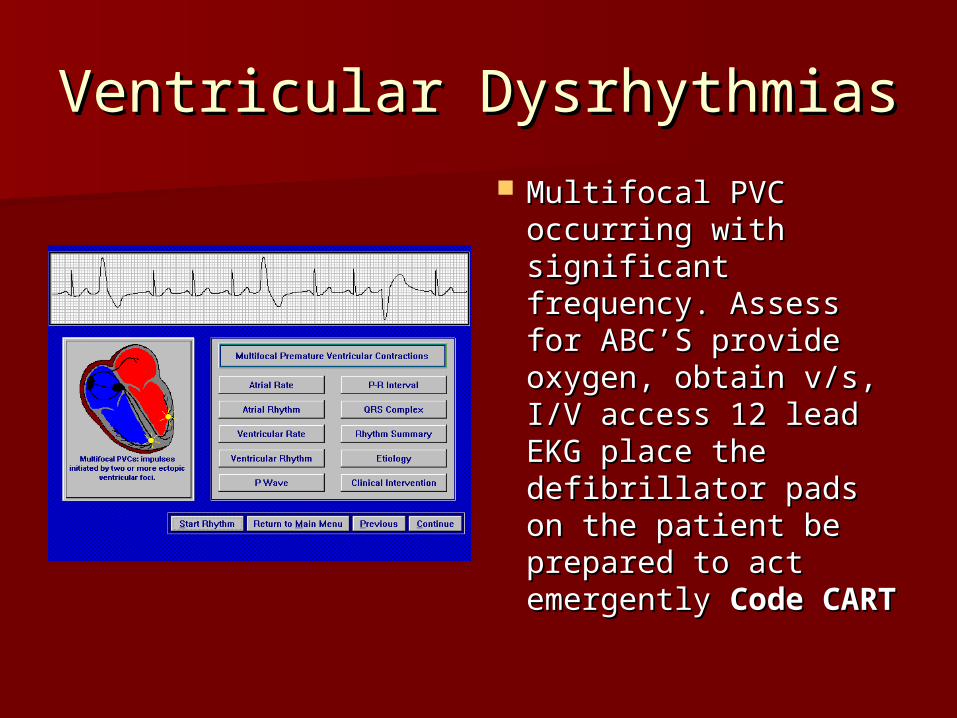
Multifocal PVC Multifocal PVC occurring with occurring with significant frequency. significant frequency. Assess for ABC’S Assess for ABC’S provide oxygen, provide oxygen, obtain v/s, I/V access obtain v/s, I/V access 12 lead EKG place the 12 lead EKG place the defibrillator pads on defibrillator pads on the patient be the patient be prepared to act prepared to act emergently emergently Code Code CARTCART

Ventricular DysrhythmiasVentricular Dysrhythmias
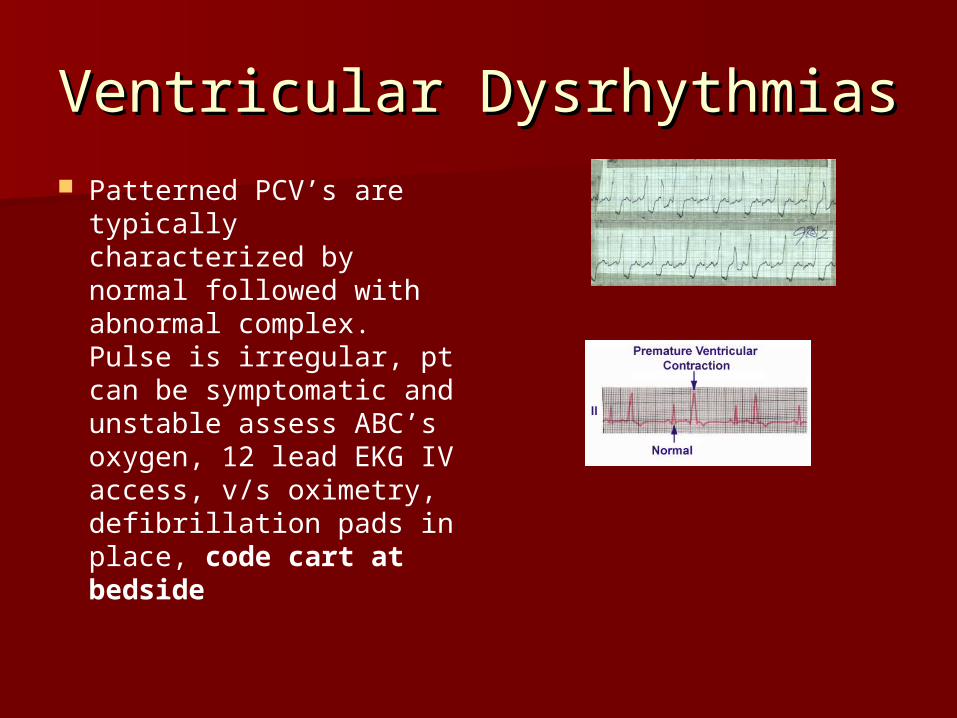
Ventricular Dysrhythmias Ventricular Dysrhythmias Patterned PCV’s are
typically characterized by normal followed with abnormal complex. Pulse is irregular, pt can be symptomatic and unstable assess ABC’s oxygen, 12 lead EKG IV access, v/s oximetry, defibrillation pads in place, code cart at bedside
Ventricular DysrhythmiasVentricular Dysrhythmias
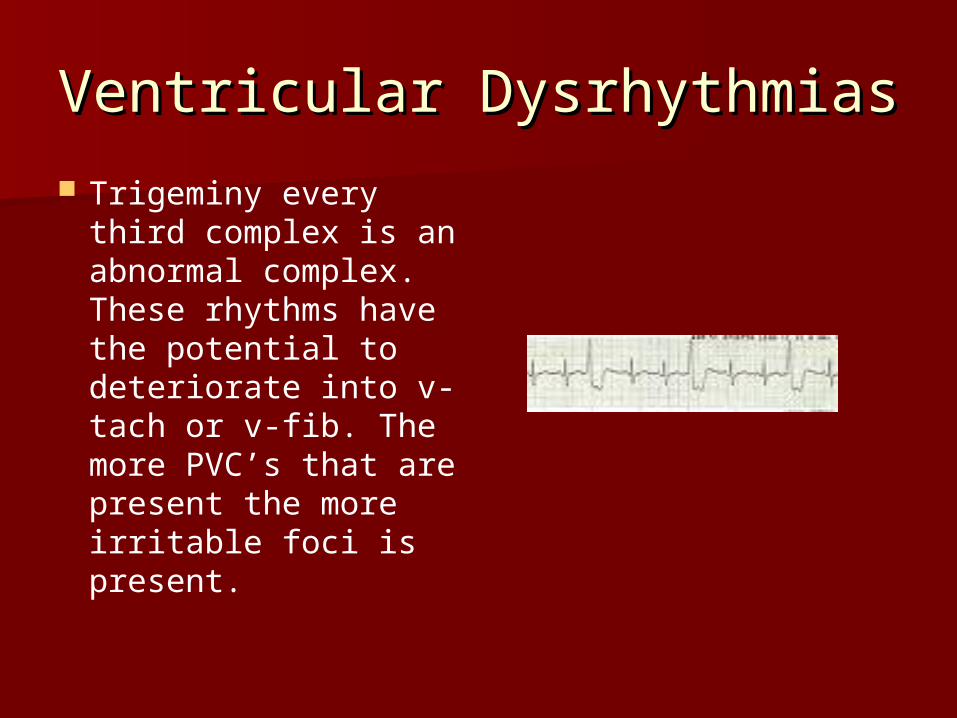
Trigeminy every third complex is an abnormal complex. These rhythms have the potential to deteriorate into v-tach or v-fib. The more PVC’s that are present the more irritable foci is present.
Ventricular TachycardiaVentricular Tachycardia
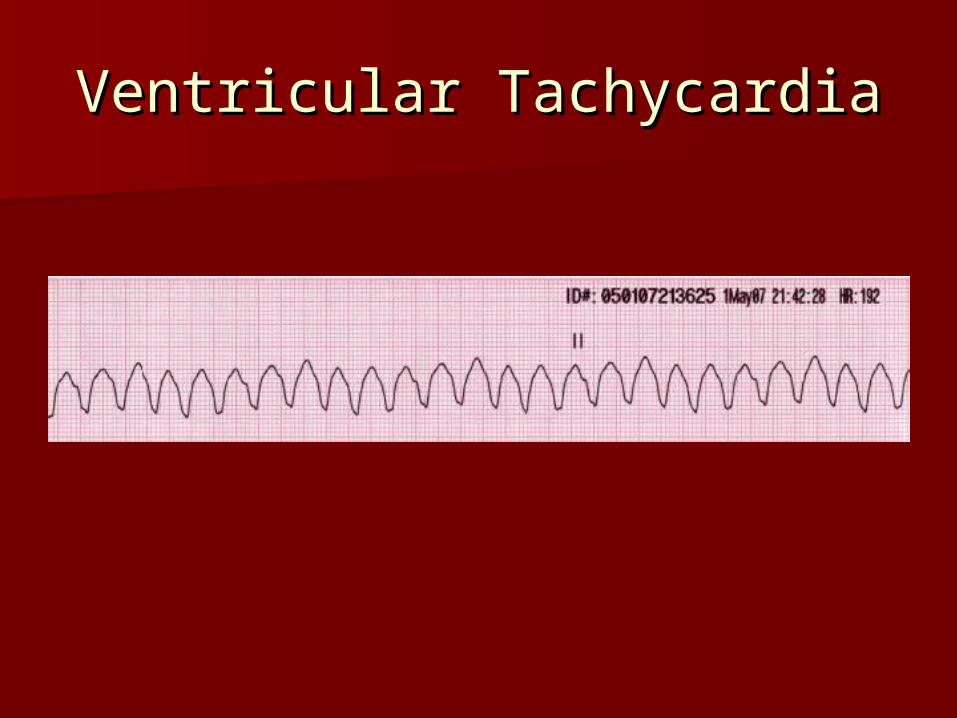
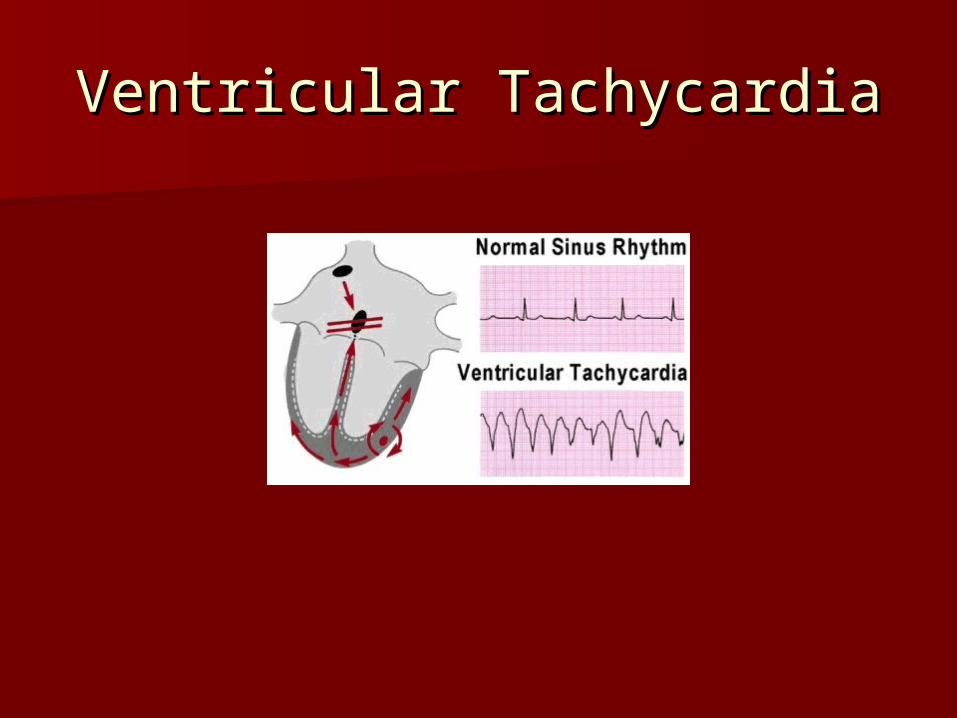
Ventricular TachycardiaVentricular Tachycardia

Ventricular TachycardiaVentricular Tachycardia
Ventricular Tachycardia characterized by Ventricular Tachycardia characterized by wide QRS complex with the absence of atrial wide QRS complex with the absence of atrial depolarization. Major problem is there is depolarization. Major problem is there is poor cardiac output and hypoperfusion is a poor cardiac output and hypoperfusion is a concern along with cellular hypoxia to major concern along with cellular hypoxia to major organs.organs.
Assess ABCD’S check for the presence of a Assess ABCD’S check for the presence of a pulse. If pulse is absent it is treated the pulse. If pulse is absent it is treated the same as ventricular fibrillation. same as ventricular fibrillation.
D represents defibrillation not disabilityD represents defibrillation not disability
V-Tach TreatmentV-Tach Treatment
Assess and support ABC’s Assess and support ABC’s →→ give oxygen give oxygen place on monitor identify rhythm place on monitor identify rhythm →→establish IV establish IV access access →→ Is patient stable or unstable? Is patient stable or unstable? (unstable s&s are chest pain, SOB, hypotension, (unstable s&s are chest pain, SOB, hypotension, altered mental status altered mental status →→ Unstable patients Unstable patients require immediate require immediate Synchronized Synchronized cardioversioncardioversion. Provide sedation if the patient is . Provide sedation if the patient is awakeawake
Energy selection if monophasic use 100-200J in Energy selection if monophasic use 100-200J in biphasic wave form use 50-100J biphasic wave form use 50-100J
V-Tach Treatment V-Tach Treatment ContinuedContinued
Stable v-tach assess for ABC’S Stable v-tach assess for ABC’S →→ give give oxygenoxygen → → assess for the presence of assess for the presence of pulses pulses →→ obtain blood pressure obtain blood pressure →→ place place on monitor identify the rhythm on monitor identify the rhythm →→ establish establish IV access IV access →→ obtain 12 lead EKG obtain 12 lead EKG
Goal of therapy is to suppress this lethal Goal of therapy is to suppress this lethal arrhythmia since it has a high propensity arrhythmia since it has a high propensity to deteriorate to v-fib and cardiac output is to deteriorate to v-fib and cardiac output is compromise compromise

V-Tach Treatment V-Tach Treatment ContinuedContinued
Goal standard of management is the use of Goal standard of management is the use of Amiodarone (Cordarone)150 mg IV over Amiodarone (Cordarone)150 mg IV over 10minutes mixed in 100 ml of D5W. Repeat 10minutes mixed in 100 ml of D5W. Repeat as needed for a max of 2.2 g/24 hours. as needed for a max of 2.2 g/24 hours. Once the rhythm is arrested place the Once the rhythm is arrested place the patient on an Amiodarone drip typically at patient on an Amiodarone drip typically at 1mg/min drip. Amiodarone affects Na+, K+ 1mg/min drip. Amiodarone affects Na+, K+ and Ca+ channels. Decreases AV node and and Ca+ channels. Decreases AV node and Sinus node conduction additionally it has Sinus node conduction additionally it has alpha & alpha & ββ adrenergic blocking properties. adrenergic blocking properties.
Ventricular Fibrillation Ventricular Fibrillation
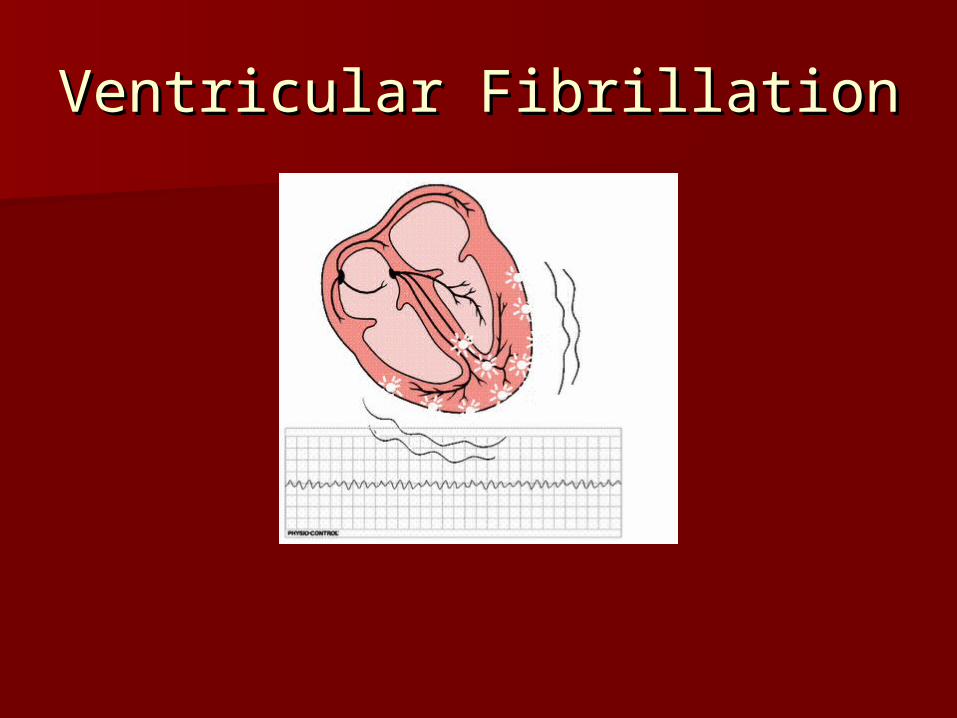
Ventricular FibrillationVentricular Fibrillation
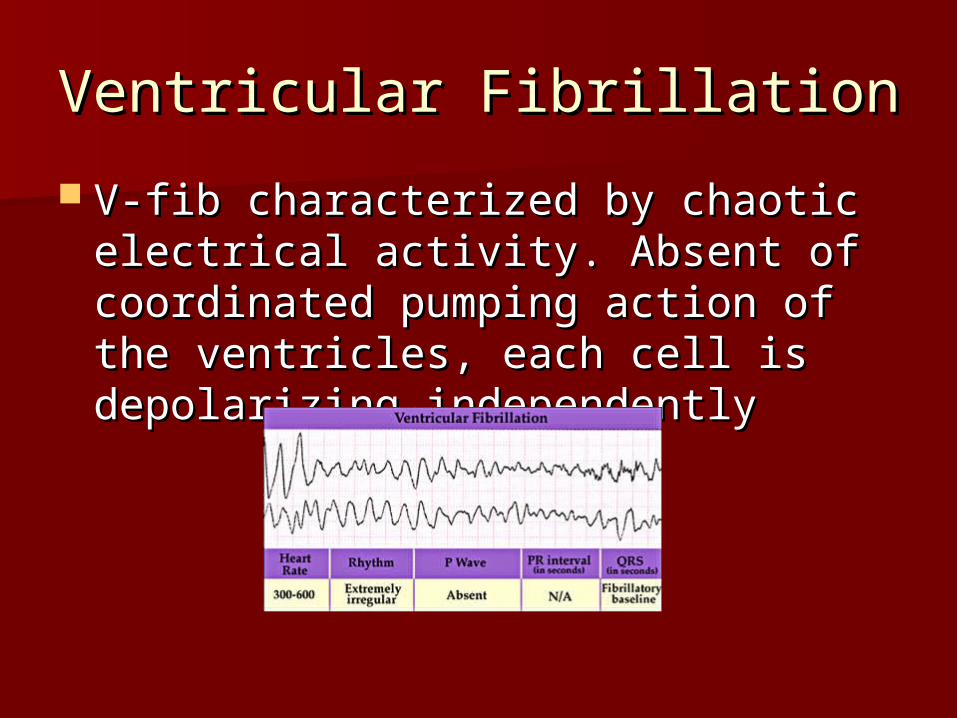
V-fib characterized by chaotic V-fib characterized by chaotic electrical activity. Absent of electrical activity. Absent of coordinated pumping action of the coordinated pumping action of the ventricles, each cell is depolarizing ventricles, each cell is depolarizing independentlyindependently
V-Fib ContinuedV-Fib Continued
Goal of treatment is to arrest this Goal of treatment is to arrest this rhythm. There is no pulse activity, this rhythm. There is no pulse activity, this is termed is termed Pulseless Arrest. Pulseless Arrest. Initiate Initiate BLS until an BLS until an AEDAED is available continue is available continue with chest compressions until the AED with chest compressions until the AED is in place. Stop chest compressions to is in place. Stop chest compressions to allow the AED to analyze the rhythm. allow the AED to analyze the rhythm. Follow the voice prompt and shock the Follow the voice prompt and shock the patient when advised by the monitor.patient when advised by the monitor.
V-Fib ContinuedV-Fib Continued Initial energy selection for biphasic monitors Initial energy selection for biphasic monitors
is 120J to 200J if monophasic start at 360J is 120J to 200J if monophasic start at 360J →→ resume CPR immediately for 5 cycles (or 2 resume CPR immediately for 5 cycles (or 2 minutes). Pump hard and fast to achieve a minutes). Pump hard and fast to achieve a rate of 100 beats/min rate of 100 beats/min →→ give one shock at give one shock at 120 to 200J if monophasic 360J 120 to 200J if monophasic 360J →→ resume resume CPR immediately after the shock CPR immediately after the shock → → establish establish IV or IO access administer Epinephrine 1mg IV or IO access administer Epinephrine 1mg or 1:10,000 concentration and repeat every or 1:10,000 concentration and repeat every 3-5 minutes 3-5 minutes →→ give 5 cycles of CPR give 5 cycles of CPR → → shock shock at 120 to 200 J or 360J at 120 to 200 J or 360J →→ resume CPR for 5 resume CPR for 5 cyclescycles
V-Fib ContinuedV-Fib Continued
Consider antiarrhythmics give during CPR or Consider antiarrhythmics give during CPR or before or after shock give Amiodarone before or after shock give Amiodarone 300mg IVP 300mg IVP →→ resume CPR for 5 cycles resume CPR for 5 cycles →→ check check rhythm if shockable shock at 120-200J or 360J for rhythm if shockable shock at 120-200J or 360J for monophasic monitors monophasic monitors →→ resume CPR for 5 cycles resume CPR for 5 cycles administer Epinephrine 1mg 1:10,000 IVP q 3-5 administer Epinephrine 1mg 1:10,000 IVP q 3-5 minutes and repeat Amiodarone 150mg IV/IO over minutes and repeat Amiodarone 150mg IV/IO over 3-5 minutes or Lidocaine at 1-1.5mg/kg dose for 3-5 minutes or Lidocaine at 1-1.5mg/kg dose for the first dose then 0.5mg-0.75mg/kg IV/IO the first dose then 0.5mg-0.75mg/kg IV/IO maximum of 3 doses or 3mg/kg maximum of 3 doses or 3mg/kg
V-Fib ContinuedV-Fib Continued
After 5 cycles check rhythm is it After 5 cycles check rhythm is it shockable? Shock with 120-200J or shockable? Shock with 120-200J or 360J for monophasic monitor 360J for monophasic monitor →→ resume resume CPR for 5 cycles consider Magnesium CPR for 5 cycles consider Magnesium loading dose of 1-2g diluted in 10ml of D5W loading dose of 1-2g diluted in 10ml of D5W IV/IO over 5-20 minutes for torsades de IV/IO over 5-20 minutes for torsades de pointes assess the rhythm and continue the pointes assess the rhythm and continue the cycle of CPR for 5 cycles or 2 minutes cycle of CPR for 5 cycles or 2 minutes →→ shock shock →→ CPR and medication CPR and medication → → shock etc. shock etc.