Embed Size (px)
Citation preview

ECMO에대한이해와환자관리
2013. 4. 26
강영애, CNS
흉부외과 중환자실
서울아산병원

Clinical decision making (1)♣ 47y/M CABG 시행후 ICU care

CVP
PAP
ECMO insertion
Clinical decision making (2)
Volume replacement
Inotropics maximal infusion
BP drop
Increased CVP
Tissue malperfusion sign
Sustained
low cardiac output state

ECMO indication
◈ Cardiogenic shock
- Inadequate tissue perfusion manifested as
hypotension, low cardiac output despite optimal
vascular volume
- AMI, myocarditis, decompensated heart failure,
recurrent life threatening arrhythmia
- Bridge to transplant /implantable circulatory
support
◈ Respiratory failure

Concepts
• ECMO : ExtraCorporeal Membrane Oxygenator
• ECLS : ExtraCorporeal Life Support
• ECLS is the use of mechanical devices to
temporarily support heart or lung function
(partially or totally) during cardiopulmonary failure,
leading to organ recovery or replacement

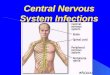
Basic principle of ECMO
Blood is drained from the right atrium
Blood is oxygenated
Excess CO2 is removed
Oxygenated blood is returned to the aorta
- (or for VV ECMO into the right atrium)
ECMO blood mixes with blood ejected
from left ventricle


Advantage of ECMO
Provide of cardiac and pulmonary support
Simple & rapid peripheral insertion of cannulas
Performed during cardiopulmonary resuscitation
-> time to recovery
Less costly than other forms of mechanical
circulatory support

CAPIOX EBS (Terumo)

QUADROX PLS (MAQUET)

BIO pump (Medtronic)

Configuration
Membrane
oxygenator
Blood
pump Drainage cannula
: inlet cannula
Return cannula
: outlet cannula
Control
console

Centrifugal pump
• Stir your coffee!
• Fluid is forced to the
outside of the path of
rotation (toward pump
outlet)
• Create a low pressure
zone in the center (at
the pump inlet)
• Controlled by RPM

Control console
Operator interface
Set pump RPM
Display flow
measurement
Incorporate pressure
monitoring, alarm

Improved centrifugal pump
• 1st and 2nd generation centrifugal pump
: high friction & heat generation
-> greater hemolysis
• Newest generation centrifugal pump
: jewel bearing, magnetic levitation,
improved flow dynamics, mechanic efficiency
-> very low friction & hemolysis,
negligible heat generation

Principle in practice
• Set RPM -> Pump flow is constant
• But pump flow is dependent on preload and sensitive to afterload
• Reduced preload = reduced pump flow
Hypovolemia, venous cannula occlusion
• Increased afterload = reduced pump flow
Circuit obstruction, small arterial cannula,
blood viscosity

Oxygenator
Hollow fiber diffusion
membrane
Gas diffusion through
membrane
Eliminate plasma leakage,
prevent formation of
microbubble
-> increased valid time

Gas blender
CO2 제거 FiO2 조절 Membrane
oxygenator연결

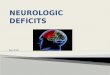
ECMO types
A. Veno-venous type
- for respiratory support,
- no hemodynamic
support
B. Veno-arterial type
- for cardiac support,
- appropriate for
respiratory support
A. B

Vascular access in VA type ECMO
• Non-postcardiotomy
- Percutaneous femoral artery & vein (rapid access),
- Percutaneous jugular vein
(advance to Rt. atrium if possible),
- Common carotid artery via surgical exploration
• Postcardiotomy
- Intrathoracic cannula

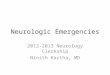
Vascular access

Optimal cannula position

Hemodynamic parameter
• Bypass flow : 4 L/min
• Cardiac index : at least 2.4 L/min/m2
• Setting : Pump RPM, FiO2 & gas flow control
• Check the volume status
( Volume fluctuation )
• Check oxygenator function
( Oxygenator ABGA )

Ventilator management
• Ventilator manage at low setting to allow lung rest
• Minimize atelectasis, maximize oxygenation
• Low rate with long inspiratory time,
low plateau inspiratory pressure (<25mmHg),
low FiO2 (<30%),
PEEP at any level (high PEEP level inhibit
venous return)
• Blood gas management : ECMO >> ventilation

Anticoagulation
• Heparin ivs (50-100u/kg) at the time of cannulation,
continuous infusion 10-15u/kg/hr
• Nafamostat mesilate (Futhan)
• Check ACT hourly until titration
ACT - whole blood clots in response to fibrin activating
agent
1.5 times normal ACT -> 150-180sec
ECMO weaning time (ECMO flow 1.5-2L/min)
-> 200-250sec

Two circulation syndrome (VA type)
• ECMO blood mixes with blood
ejected from Lt. ventricle
• Coronary & proximal arch
perfusion by unoxygenated blood
• Different PaO2 between upper
and lower extremities
• Management
- Minimize pulmonary circulation
: maximum drainage
- ABGA monitoring via Rt. arm
- Negative fluid balance

LA decompression
• Returning blood flow to Lt.
atrium
-> Interfere heart decompression
-> Lung congestion
-> Heart recovery delay
LA vent insertion

Management of distal vessels
• If the access is via the femoral artery, distal arterial flow
to leg is inadequate
• Separate perfusion line placed in the superficial femoral
artery (distal perfusion line)

Renal, fluid balance
• Normal body wt. no fluid overload
• MAP up to 70mmHg, CVP 5-10mmHg
• Acceptable urine output : 1-2ml/kg/hr
• Consider pulsatile perfusion
• Hemofiltration through EBS circuit
• Fluid management for ARF
: early CRRT
• Daily body weight check
: negative I/O balance

Infection & nutrition
• Prevention : if possible percutaneous ECMO
• Surveillance culture : blood, urine, sputum
• Disruption of normal infection barrier
- Prophylactic antibiotics, no standard policy
• Nutritional support
- Parenteral nutrition
- TPN << enteral feeding
- NG tube feeding within 48hr

Bleeding
• d/t systemic anticoagulation, thrombocytopenia,
thrombocytopathy
• Cannulation site, operation site, catheter passage,
mucous membrane, GI bleeding, brain parenchyma
• Optimal anticoagulation state
: optimal ACT,
platelet transfusion : > 80,000
hematocrit : 35~40%

• During cannulation & management for first 12-24hr
• To prevent air embolism by spontaneous breathing ,
to minimize metabolic rate, to avoid movement,
for patient comfort
• Depending on patient’s level anxiety & discomfort
• Sedation should be minimal, but be sure the risk of
decannulation
Sedation

Others
• Hourly neurologic exam
• Positioning & skin care
- Depending on primary condition,
Possible to extubate for cardiac support
• Check peripheral circulation, compartment syn.
• Temperature care
- Close to 37℃ or mild hypothermia(32-34℃) during first
24-72hr in condition which lead to hypoxic brain damage
• Check chest X-ray, echocardiography for cardiac support


◈ Trial off during VA type ECMO
• With evidence of improved hemodynamic parameter,
contraction on echocardiography
• Adjust the dose of inotropes, vasopressors & ventilator
setting
• Clamp off extracorporeal circuit (or bridge) and follow
perfusion and gas exchange
• Anticoagulation is continued during trial off
ECMO trial off

Decannulation
• After heparin stop for 30-60min
• Percutaneous access can be removed directly and
bleeding controlled by topical compression
• When removing venous cannula in spotaneous
breathing state, air can enter venous blood
-> valsalva maneuver on ventilator
or short-term pharmacological paralysis