Embed Size (px)
DESCRIPTION
Reunión Hemisférica de la Red de Protección Social y Salud . Sep. 30-Oct. 1, 2010
Citation preview

Economic evaluation of coverage with an effective intervention of screening for diabetes and
hypertension in Mexico
Reunión Hemisférica de la Red de Protección Social y Salud
Mejorando la Prevención y Manejo de enfermedades crónicas en América Latina y el Caribe
Sep. 30-Oct. 1, 2010
Angélica Castro Ríos1 Act., MHE
Svetlana Doubova1MD., MSc
Silvia Martínez Valverde2 Ec., MSc
Irma Coria Soto3 MD., Msc
Ricardo Pérez-Cuevas1,2 MD., DrSc
1. Epidemiology and Health Services Research Unit, Instituto Mexicano del Seguro Social2. Center of Studies on Health Economics and Society. Hospital Infantil de Mexico Federico Gómez3. Consultant

• The Mexican Institute for Social Security (IMSS) was established in 1943, ever since provides:– Health care– Retirement funds– Pensions for disabled
workers– Social services (particularly
for older adults)– Children daycare centers
• 360,000 IMSS’ employees• 48 million enrollees
Instituto Mexicano del Seguro Social

2000
2050
Population pyramids for IMSS, other insured and uninsured 2000-2050
4.00 3.00 2.00 1.00 0.00 1.00 2.00 3.00 4.00
0-9
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90-99
100 y +
Others (ISSSTE, SEDENA, PEMEX, Marina)
4.00 3.00 2.00 1.00 0.00 1.00 2.00 3.00 4.00
0-9
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90-99
100 y +
IMSS
8.00 6.00 4.00 2.00 0.00 2.00 4.00 6.00 8.00
10-19
100 y +
0-9
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90-99
Uninsured (Seguro Popular)
IMSS’ CURRENT DEMOGRAPHIC AND EPIDEMIOLOGICAL CONDITIONS

Prevalence of hypertension by age group and sex IMSS and national
0
10
20
30
40
50
60
70
80
20 a 29 30 a 39 40 a 49 50 a 59 60 a 69 70 a 79 80 y mas
%
Age group
Men Women Men-National Women-National
Source: ENSANUT 2006.

* By 1,000 visits
0
50
100
150
200
250
300
350
00- 01
Años
01-04 05-09 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80 y más
DM HTA Osteoartritis
Rate of ambulatory visits*
DM, Hypertension and arthritis by age group 2006

Mortality by selected causes 1976-2008
Perinatal
mortality
Pneumonia
Cervical cancer
Diarrheal diseases
Tuberculosis
Diabetes
Ischemic heart
disease
Stroke
Breast cancer
Hypertension
complications
Chronic renal failure
Infectious diseases,
malnutrition and
reproductive health
Chronic diseases
% of total deaths % of total deaths
Source: IMSS

PreDM2 and PreHTA
• T2DM and HTA have highly prevalent, recognizable preclinical (asymptomatic) stages, prehypertension and prediabetes.
• Prehypertension (preHTA) is defined as a systolic blood pressure of 120-139 mmHg and/or diastolic blood pressure 80-89 mmHg.
• Prediabetes (preDM) is defined as impaired fasting glucose (plasma glucose level of 100 to <126 mg/dL after an overnight fast), impaired glucose tolerance (plasma glucose of 140 to <200 mg/dL after 2 h in an oral glucose tolerance test), or the presence of both
• PreDM and preHTA are identifiable through screening activities
8

+40% women, +50% men, +30% older adults are susceptible of modifying the progression from pre DM2 and/or PreHTA to T2DN and or HTA
Frequency of cases in ENCOPREVENIMSS-2006
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Mujeres Hombres Adultos
mayores
DM e HTA
DM y preHTA
preDM e HTA
DM
HTA
preDM y preHTA
preDM
preHTA
Sano
gravedad

Health gains associated with timely detection of T2DM
Type 2 diabetes
• The natural progression from the preclinical to the clinical stage of T2DM takes an average of 5-11 years
• PreDM can be identified and treated early through life style interventions
• Early detection and preventive care could cause a further 5-year delay before progression to clinical T2DM and appropriate care contributes to delay the progression to chronic complications
10

Health gains associated with timely detection of HTA
• The risk for cardiovascular events varies according to sex, age, blood pressure and blood glucose levels
• A cohort study assessed the hazard ratios (HZ) for cardiovascular disease.
– A person with preHTA was calculated to have an HZ of 1.8
– with preDM + preHTA to have an HZ of 2.12;
– with T2DM the HZ was calculated to be 2.9
– with preHTA+T2DM it was 3.7.
Each person could be classified as: healthy, preDM, T2DM, preHTA, HTA, preDM+preHTA, preDM+HTA, T2DM+preHTA or T2DM+HTA.
• This supports the importance to analyze the cardiovascular risk by considering alterations in blood pressure and blood glucose levels together rather than independently.
• Lowering diastolic blood pressure by 5 mmHg reduces the cardiovascular risk for stroke by 34% and for ischemic heart disease by 21%.
11

Previous economic evaluations studies of screening programs of T2DM and HTA
• Early detection of T2DM has an acceptable cost-effectiveness ratio owing to the potential of reducing the cardiovascular risk and delaying/preventing the onset of clinical disease.
• These studies selected specific risk populations or had a local focus, and their recommendations should not be applied to the general population.
• The magnitude of the savings varied depending on the analysis horizon of the study and on the strategy of prevention, which was not always limited to screening but could include the treatment of detected cases
• The savings are observed a few years after the implementation.
• Not all studies concerning this topic have reported whether the screening program was cost saving.
12

DESCRIPTION OF THE POLICY TO
EVALUATE: PREVENIMSS

PREVENIMSS
• PREVENIMS is the acronym for IMSS Integrated Preventive Care Program
• This program was designed and implemented to improve provision of preventive services and includes strategies to evaluate its coverage.

PREVENIMSS main goals
• To change the focus of the programs previously oriented to prevent specific diseases and risks, towards protecting the health of population groups
• To provide IMSS affiliates a package of actions to promote and protect their health in accordance with their age and gender
• To increase coverage and effectiveness of preventive care
Age groups
1. Children 0-10 years
2. Adolescents 11-19 years
3. Women 20-59 years
4. Men 20-59 years
5. Older adults >=60 years
Processes
1. Health promotion
2. Nutrition
3. Prevention and disease control
4. Screening of selected diseases
5. Reproductive health

Coverage progress of screening for chronic diseases
16
Age group Screening 2003 2004 2005 2006Women
(20-59 years)
Breast cancer
Clinical examination
Mastography
42.6 45.3 50.4 62.4
-- 6.5 7.9 22.1
Cervical cancer 66.7 72.4 74.5 75.0
Type 2 Diabetes 45.3 55.1 56.8 66.5
Hypertension60.6 66.0 70.6 74.2
Men
(20-59)
Type 2 Diabetes38.6 41.7 44.4 57.8
Hypertension 48.4 49.1 56.5 64.0
Older adults Type 2 diabetes34.8 54.4 56.0 65.2
Hypertension 46.0 66.9 71.8 75.0
Source: ENCOPREVENIMSS 2003-2006

Economic evaluation of coverage with an
effective intervention of screening for
diabetes and hypertension in Mexico

Objectives
Primary Objective
• To analyze the potential economic benefit of screening activities for T2DM and HTA
• The analysis included measuring PREVENIMSS coverage with effective intervention
Secondary objective
• To explore whether an unmet need exists for young adults aged between 20-29 years and the potential gain of expanding screening to this age group

Study data and Methods
• Population
• Data about health states associated with T2DM and HTA, and effectiveness and effective coverage of the screening program were estimated from the subsample of the 2006 ENCOPREVENIMSS.
• The analysis comprised:
– adult women and adult men (30 to 59 years old
– older adults (60 years and older)
– young women and young men (20-29 years old)
• Each person was classified according to the possible health states associated with HTA and T2DM: healthy, preDM, T2DM, preHTA, HTA, preDM+preHTA, preDM+HTA, T2DM+preHTAand T2DM+HTA.

Definitions
• Coverage: proportion of individuals who needed and used the screening program. Coverage was estimated for each age group.
• Effectiveness was ascertained from an ex-post approach, based on the screening test opportunity.
• From an individual perspective, the T2DM screening program was effective when preDM cases were detected, while HTA screening effectiveness was defined as the identification of preHTA or HTA cases without cardiovascular disease.
• The overall effectiveness of the screening program was calculated as the percentage of people effectively detected.
• Effective coverage was taken from the concept of coverage with effective interventions and it was estimated as the proportion of people in need of screening who received intervention with effectiveness.
20

The economic model
• Analysis of the potential economic benefit of the T2DM and HTA screening program was estimated for the 2006 cohort by comparing two scenarios, “screening program” versus “no screening program”
• The analysis considered the perspective of the public health care provider (IMSS)
• The model included the healthcare costs associated with the different health states of HTA and T2DM in a 20-year horizon
• The “screening program” scenario considered the health and economic gains of the timely detection of each of the health states, including the costs of screening and preventive care for such cases.
• The “no screening program” scenario assumed no timely detections of these conditions and that effective coverage was equal to zero.
• The average costs (savings) per covered user and per user effectively covered were estimated for different groups at risk to obtain an adjusted indicator of the potential economic impact of the program.
21

Economic evaluation model of the
diabetes screening program
-10 -5 -1 1 5 10 15 20
Diagnosis after screening
glucose 100-125 mg/dl
Diagnosis DM (clinical manifestations)
Glucose + 126 mg/dl
Period in which the costs of care for people at risk (pre-diabetes stage) were estimated
Period in which the costs of care for diabetes and its complications were estimated
Period of effective coverage
for diabetes screening
years

Proportion of patients that received preventive care
• Three groups of patients were defined:
– patients who were effectively covered by the screening program and received preventive care
– Patients who were effectively covered by the screening program but did not receive preventive care
– patients who were not effectively covered by the screening program.
• The first group was labeled as preventive care, while the others were labeled as routine care groups.
• The proxy of appropriate care was based on IMSS reports concerning the adequate control of T2DM or HTA patients in primary care services.
• 83% of the HTA patients and 30% of T2DM patients had adequate control.Regarding those cases in which both figures (glucose and blood pressure) were abnormal, the proportion of appropriate care was assumed to be 50%.
23

Health care costs
• We estimated the direct costs of health care provided to patients in each health state associated with T2DM and HTA.
• The present-value of healthcare costs was discounted using a 3% year discount rate.
• In addition, timely detection was considered to determine the health gains and their differentiated annual costs.
• The annual healthcare costs comprised preventive care costs, treatment costs for the condition in primary care facilities, cost of the treatment for cardiovascular acute events and treatment costs for chronic complication associated with T2DM.
24

Health care costs
• The healthcare costs were estimated by assuming three models of disease progression:
• (a) progression from preDM to T2DM
• (b) progression from T2DM to chronic complications
• (c) progression to acute cardiovascular events.
• Each model considered the respective proportion of cases receiving preventive care.
• The costs were expressed in US dollars (the exchange rate on 31-12-2009 was 13.0659 Mexican pesos per US dollar).
25

RESULTS

Distribution of health status associated with T2DM and HTA
27

Results of the PREVENIMSS screening program for T2DM and HTA on the survey
28

Results of the PREVENIMSS screening program for T2DM and HTA on the survey
29


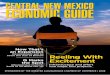
-$173.8
-$420.6
-$171.4
-$243.8
-$560.2
-$291.1-$316.3
-$669.5
-$240.1
-$325.3
-$930.2
-$483.4
-$1,000
-$900
-$800
-$700
-$600
-$500
-$400
-$300
-$200
-$100
$0
Young women
20-29 yrs
Adult women
30-59 yrs
Young men
20-29 yrs
Adult men
30-59 yrs
Older adults
scenario 1
Older adults
scenario 2
Savings per user covered Savings per user effectively covered
Gap: 82%
Gap: 59%
Gap: 40%
Gap. 33%
Gap: 66%
Gap: 66%
Potential average savings per user effectively covered by the PREVENIMSS screening program for T2DM and HTA, in
the 20-years horizon.

Potential economic benefit of the screening program for each group at risk (present value next 20 years)
32

Limitations of the study
• This is a secondary data analysis of a cross-sectional study and information regarding the follow-up of patients identified as preDM or preHTA was not available.
• The assumptions concerning the progression from preDM or preHTA to clinically established T2DM or HTA were based on literature reviews and the history of these conditions (progression to acute and long-term complications). The rates of progression for the Mexican population are unavailable.
• The model of progression to acute and chronic complications only considered the more severe stages of the diseases; the intermediate stages were not included and this could result in an underestimation of the medium term costs and the benefits of timely detection.
33

Limitations of the study
• The analysis did not include non-direct medical costs or indirect cost such as community care, transportation and loss of productivity.
• Including these costs would reinforce our findings, as they would increase the economic burden associated with the conditions that preventive care could avoid.
• PREVENIMSS criteria stated that screening for T2DM should be carried out every three years for people 30-45 years. Owing to the design of the survey, we were only able to ascertain if people had used the preventive services in the last year, and this could underestimate the actual coverage of the program for T2DM.
34

Conclusions
• The evaluation of the potential economic benefit of the PREVENIMSS program in a 20-years horizon produced positive results.
• For each dollar invested in the screening program, between US$84 to US$323 dollars would be saved in a 20-year horizon.
• The screening program was cost-saving for each of the three programmatic groups and the two non-programmatic young groups.
• The total amount of savings varied by group;
– older adults and adult women demonstrated higher average savings. For these groups, average savings increased as long as effectiveness and coverage increased.
– For adult men and young adults, the average savings would increase if the focus was on increasing coverage.
• It is important to consider the inclusion of younger groups in the routine screening program of PREVENIMSS.
35