Embed Size (px)
Citation preview

Economics of
prevention in Australia Prof Theo Vos
for the ACE-Prevention Research Team
Journées de la Prévention, INPES June 7th 2013

Assessing Cost Effectiveness—Prevention
ACE-Prevention Research Team
n Principal investigators Theo Vos Rob Carter
n Researchers Jonathan Anderson Isaac Asamoah Jan Barendregt Melanie Bertram Josh Byrnes Dominique Cadilhac Daphni Chao Linda Cobiac Siobhan Dickinson Chris Doran
2
Jun Fen Megan Forster Michael Gascoigne Shahram Ghaffari Hideki Higashi Linda Kemp Yong Yi Lee Anne Magnus Cathy Mihalopoulos Vittal Mogasale
Marj Moodie Farid Najavi Shamesh Naidoo Katherine Ong Michael Otim Sophy Shih Utsana Tonmukayakul Kiu Tay Teo Lennert Veerman Angela Wallace

Assessing Cost Effectiveness—Prevention
Overview of the Session
1. Introduction to ACE-Prevention 2. ACE-Prevention results
a) Intervention pathways b) Costs/health gain/cost savings from
recommended packages 3. Interpretation of results
3

Assessing Cost Effectiveness—Prevention 4
Brief History
n ACE-Prevention was a 5 year NHMRC Health Services Research Grant (2005-2009) ¨ Across 2 sites (University of Queensland and Deakin)
n Followed on from earlier ACE studies funded by both government & competitive grants
n Focus in ACE studies is priority setting ¨ What to do? (‘allocative efficiency’) ¨ How to do it? (‘technical efficiency’)

Assessing Cost Effectiveness—Prevention
Why are governments now more interested in explicit priority setting?
n Three reasons given prominence in health economic literature ¨ Controlling health expenditure ¨ Increasing evidence of inefficiency ¨ Reluctance to rely too heavily on the free
market as mechanism of choice n can’t opt out n asymmetry in information
5

Assessing Cost Effectiveness—Prevention
Projected total health expenditure (2002–03 dollars) by cause, Australia, 2002–03 to 2032–33
6
Expenditure by year ($billion) Change 2003-2033 Cause 2002–03 2032–33 Per cent Cardiovascular 9.3 22.6 + 143 Respiratory 7.2 22.0 + 206 Injuries 6.7 14.4 + 115 Dental 5.9 14.9 + 153 Mental 5.2 12.1 + 133 Digestive 4.9 16.5 + 237 Neurological 4.7 21.5 + 357 Musculoskeletal 4.4 14.2 + 223 Genitourinary 3.7 10.9 + 195 Cancer 3.5 10.1 + 189 Diabetes 1.6 8.6 + 438 Other 28.0 78.3 + 180 Total health expenditure 85.1 246.1 + 189 Goss J. Projection of Australian health care expenditure by disease, 2003 to 2033. Health and Welfare Expenditure Series No. 36. Canberra: Australian Institute of Health and Welfare, 2008.

Assessing Cost Effectiveness—Prevention
Opportunities for change?
q Projections reflect ‘business as usual’ scenario
q Are there opportunities to improve? q Requires detailed information on the costs
and outcomes of current practice and alternative intervention approaches
q ACE-Prevention does this for prevention of non-communicable disease

Assessing Cost Effectiveness—Prevention 8
Origins of ACE approach n There is a theoretical underpinning to ACE n What is “ideal” approach to priority setting? n We developed checklist based on 4 rationales
¨ Economic theory ¨ Ethics & social justice ¨ Empirical evidence ¨ Needs of decision-makers
n Essence of ACE is trying to achieve balance between technical rigour and due process
Carter R, Vos T, Moodie M, Haby M, Magnus A, Mihalopoulos C (2008). Priority Setting in Health: Origins, Description and Application of the Assessing Cost Effectiveness (ACE) Initiative. Expert Review of Pharmacoeconomics and Outcomes Research, 8:593--617.

Assessing Cost Effectiveness—Prevention 9
Overview of economic methods
n Clear criteria for selection of interventions n Standardised evaluation methods to minimise
methodological confounding n Evaluation conducted as integral part of
exercise (not collation from literature) n ‘Evidence’-based approach with extensive
uncertainty & sensitivity testing

Assessing Cost Effectiveness—Prevention 10
C/E analysis protocol
Perspective Health Sector (focus on government; key societal effects flagged)
Comparator Current practice + no interventions (‘null’) for analyses of intervention mix
Target pop Cohort of patients with conditions/risk factor of interest, Aust. population 2003
Time horizon Track costs & benefits 100 yrs or death
Discounting 3% Costs Best available unit costs (documented); Real costs $AUD 2003

Assessing Cost Effectiveness—Prevention 11
C/E analysis protocol Outcomes
Cost per DALY saved
Uncertainty analysis 95% uncertainty intervals using probabilistic analysis
Sensitivity analysis Test scenarios around key design features
Reporting cost-effectiveness ranges cost-effectiveness planes expansion path

Assessing Cost Effectiveness—Prevention 12
Total population Indigenous Topic Prevention Treatment Prevention Treatment Alcohol 9 2 Tobacco 8 Physical activity 6 Nutrition 26 Body mass 9 Blood pressure/cholesterol 12 5 Bone mineral density 3 Illicit drugs 2 1 Cancer 9 1 Diabetes 7 7 Renal disease 2 2 4 2 Mental disorders 11 10 Cardiovascular disease 1 5 Other 18 6 3 Total 123 27 19 2
Topic areas and interventions

Assessing Cost Effectiveness—Prevention
Overview of the Session
1. Introduction to ACE-Prevention 2. ACE-Prevention results
a) Intervention pathways: “ideal mix” b) Costs/health gain/cost savings from
recommended packages 3. Interpretation of results
13

Assessing Cost Effectiveness—Prevention 14
Results: DALYs, costs, cost-effectiveness ratios alcohol interventions
DALYs Intervention
cost Cost
offsets Net cost Cost-effectiveness
ratio averted $Million $Million $Million $$/DALY Taxation increase 30% 100,000 0.6 -530 -530 Dominant Volumetric taxation 11,000 0.6 -57 -56 Dominant Advertising bans 7,800 20 -31 -12 Dominant Minimum drinking age 21 150 0.6 -0.8 -0.2 Dominant Licensing controls 2,700 20 -11 9 3,300 Brief intervention 160 2.3 -1.2 1.1 6,800 Brief intervention + telemarketing 340 6.1 -2.6 3.5 10,000 Drink drive mass media 1,500 39 -11 28 14,000 Random breath testing 2,300 71 -17 54 24,000 Residential treatment & naltrexone 480 59 4.4 55 120,000 Residential treatment 190 37 -1.7 35 150,000
Cobiac L, Vos T, Doran C, Wallace A (2009).Cost-effectiveness of interventions to prevent alcohol-related disease and injury in Australia. Addiction, 104:1646-55
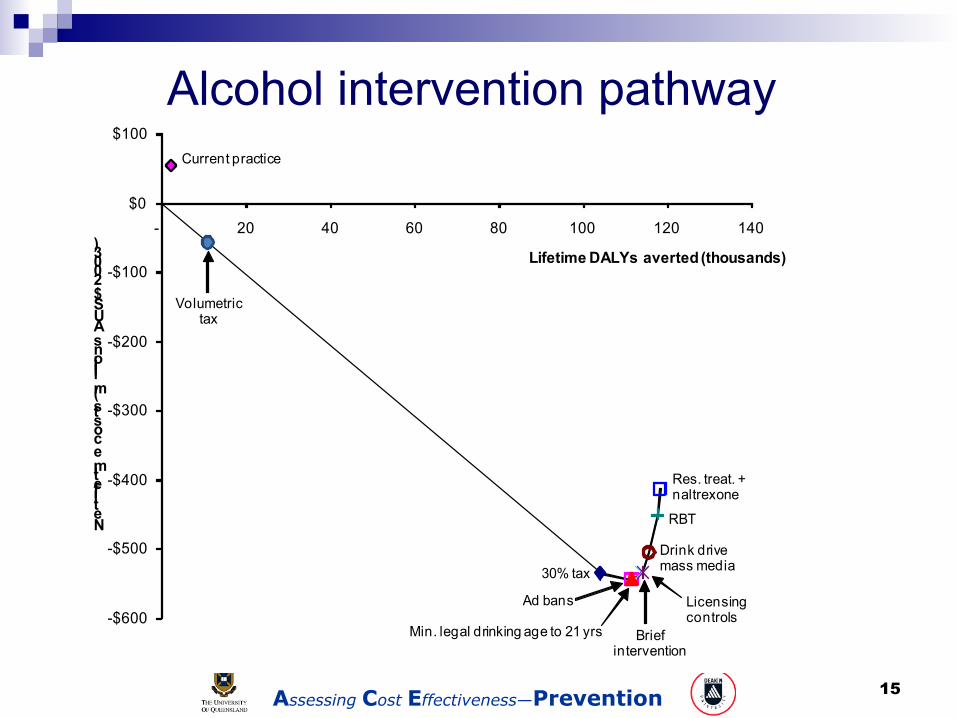
Assessing Cost Effectiveness—Prevention 15
Alcohol intervention pathway
-$600
-$500
-$400
-$300
-$200
-$100
$0
$100
- 20 40 60 80 100 120 140
Net lifetime costs (millions AUS$ 2003) Lifetime DALYs averted (thousands)
Ad bans
RBT
Drink drive mass media
Res. treat. + naltrexone
Licensing controls
Min. legal drinking age to 21 yrs Brief intervention
30% tax
Current practice
Volumetric tax

Assessing Cost Effectiveness—Prevention
Physical inactivity
16
-$1,000
-$800
-$600
-$400
-$200
$00 10 20 30 40 50 60 70
Net lifetime cost (millionsAUS$2003)
Lifetime DALYs averted (thousands)
Pedometers
GP referralMass media
Internet
GP prescription
TravelSmart

Assessing Cost Effectiveness—Prevention 17
-4
0
4
8
12
16
0 200 400 600 Net
life
time
cost
s (2
008
A$
in b
illio
ns)
Lifetime DALYs averted
Salt Diuretic
H M L
Ca-channel blocker
H M
L
ACE-inhibitor H M
L ACE-inhibitor
H
M
L
Community heart health
Dietary counselling & sitostanols
Current practice
Blood pressure & cholesterol lowering

Assessing Cost Effectiveness—Prevention 18
Blood pressure & cholesterol lowering
Cost per year for 40 mg generic simvastatin: Australia: $400 New Zealand: <$20
Diuretic H Diuretic M CCB H
CCB M - ACEi H
ACEi M
Statin H
Statin M
ACEi M
ACEi H CCB M
CCB H Diuretic M Diuretic H StatinNZ M StatinNZ H
- $0.5
$0.0
$0.5
$1.0
$1.5
$2.0
$2.5
$3.0
0 20 40 60 80 100 120 140
Net
life
time
cost
s (2
008A
$)
Billions
Lifetime DALYs averted or QALYs gained Thousands
$50,000/DALY or QALY

Assessing Cost Effectiveness—Prevention 19
-4,000
-3,000
-2,000
-1,000
00 50 100 150 200 250 300
Net lifetime costs (million AUS $)
Lifetime DALYs averted (thousands)
Tax
Lapband
Diet & exercise
Weight loss

Assessing Cost Effectiveness—Prevention 20
Dialysis & transplant (current practice)
DM ( 50-79)
Dialysis only
- 200
0
200
400
600
800
5,000 10,000 15,000 20,000 Net
LIfe
time
Cos
t (m
illio
n A
U$
2003
)
Lifetime DALYs averted
Screening and early treatment
DM ( 40-49)
DM ( 25-39)
Non-DM ( 50-79)
Non-DM ( 40-49)
Non-DM ( 25-39)
Chronic Kidney disease

Assessing Cost Effectiveness—Prevention
Expansion pathway general vs Indigenous population
General population Indigenous population
DM ( 50-79)
DM (40-49)
DM (25-39)
Non-DM (50-79 )
Non-DM (40-49)
Non-DM (25-39)
-400
-200
0
200
400
600
800
0 5 000 10 000 15 000 20 000 25 000 30 000
Net
LIfe
time
Cos
t (m
illio
n A
U$
2003
)
Lifetime DALYs averted
DM
( 50-79)
Non-DM (50-79)
DM (40-49)
DM (25-39 )
Non-DM (40-49)
Non-DM (25-39)
DM
(50-79) Non-DM (50-79)
DM (40-49)
DM (25-39)
Non-DM (40-49)
Non-DM (25-39)
-40
-20
0
20
40
60
0 500 1 000 1 500 2 000
Net
LIfe
time
Cos
t (m
illio
n A
U$
2003
)
Lifetime DALYs averted
Chronic kidney disease intervention pathway (CKD screening, Indigenous population)
Remote

Assessing Cost Effectiveness—Prevention
Overview of the Session
1. Introduction to ACE-Prevention 2. ACE-Prevention results
a) Intervention pathways: “ideal mix” b) Costs/health gain/cost savings from
recommended packages 3. Interpretation of results
22

Assessing Cost Effectiveness—Prevention 23
23 dominant (cost-saving) preventive interventions

Assessing Cost Effectiveness—Prevention 24
23 dominant preventive interventions vs. current practice
-30
-10
10
30
50
70
-$600
-$200
$200
$600
$1,000
$1,400
2003 2010 2017 2024 2031 2038 2045 2052 2059 2066 2073 2080
DALYs averted
Thousands
Costs
Millions
Years
Cost offsets - Dominant package Intervention costs - Current practice
Intervention costs - Dominant package Cost offsets - Current practice
Health gain - Dominant package Health gain - Current practice

Assessing Cost Effectiveness—Prevention
-20
0
20
40
60
80
-$1
$0
$1
$2
$3
$4
2003 2010 2017 2024 2031 2038 2045 2052 2059 2066 2073 2080
DA
LYs
aver
ted
Mill
iers
Cos
ts
Mill
iard
s
Years
Intervention costs - Current practice Intervention costs - <$10,000/DALY package
Cost offsets - <$10,000/DALY package Health gain - <$10,000/DALY package
Combined impact 43 very cost-effective prevention measures
$4 billion upfront investment
Immediate cost savings in blood pressure & cholesterol
Treatment cost saved
1 million healthy life years

Assessing Cost Effectiveness—Prevention
Overview of the Session
1. Introduction to ACE-Prevention 2. ACE-Prevention results
a) Intervention pathways: “ideal mix” b) Costs/health gain/cost savings from
recommended packages 3. Interpretation of results
26
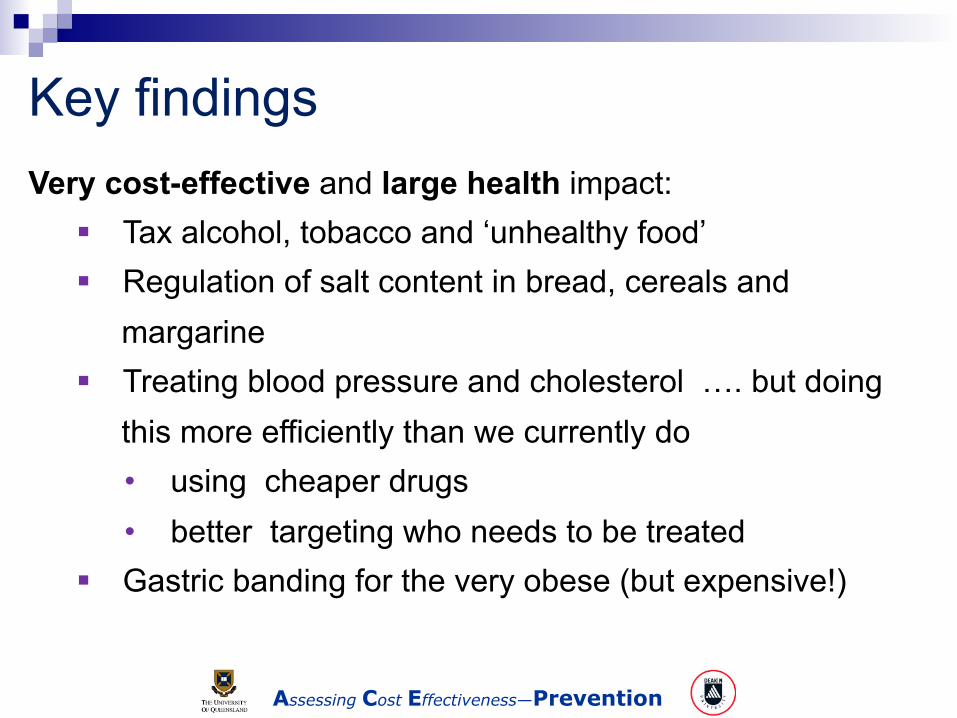
Assessing Cost Effectiveness—Prevention
Very cost-effective and large health impact: § Tax alcohol, tobacco and ‘unhealthy food’ § Regulation of salt content in bread, cereals and
margarine § Treating blood pressure and cholesterol …. but doing
this more efficiently than we currently do • using cheaper drugs • better targeting who needs to be treated
§ Gastric banding for the very obese (but expensive!)
Key findings

Assessing Cost Effectiveness—Prevention
Very cost-effective and moderate health impact:
§ Pedometers & mass media for physical activity
§ Smoking cessation drugs
§ Screen elderly women for osteoporosis & alendronate
§ Screen diabetics for chronic kidney disease

Assessing Cost Effectiveness—Prevention
Very cost-effective and more modest health impact:
§ Fluoride drinking water
§ Hepatitis B vaccination
§ A range of 7 measures to prevent mental disorders or
suicide
Key findings

Assessing Cost Effectiveness—Prevention
Other cost-effective measures:
§ Increased Sunsmart effort
§ HPV vaccination and Pap smear testing cervix cancer
§ Screen for pre-diabetes + drug or lifestyle intervention
§ Screen for chronic kidney disease + drug
§ Diet and exercise for overweight people (but limited
impact on weight loss)
Key findings

Assessing Cost Effectiveness—Prevention
Not recommended:
§ PSA testing for prostate cancer (more harm than good)
§ Weight watchers
§ Drugs for losing weight
§ Most fruit and veg interventions
§ Aspirin to prevent cardiovascular disease
§ School based drug interventions
§ Vaccination for shingles
Key findings

Assessing Cost Effectiveness—Prevention
Insufficient evidence of effectiveness:
§ Screening for vision loss
§ Dental check-ups
Key findings

Assessing Cost Effectiveness—Prevention 33
Summary of results
1. Taxation/regulation interventions tend to be very cost-effective (from health sector perspective) and have large health impact
2. Great potential to improve efficiency in CVD prevention thru blood pressure and cholesterol lowering and accelerate CVD decline
3. Untapped potential to address pre-diabetes, chronic kidney disease

Assessing Cost Effectiveness—Prevention 34
Summary of results
4. Emerging evidence for a substantial role in prevention of mental disorders
5. Targeted interventions with drug treatments in CVD prevention, pre-diabetes, chronic kidney disease, osteoporosis good credentials
6. Targeted interventions aiming to change behaviour tend not to be cost-effective and if so, have modest impact on population health outcomes

Assessing Cost Effectiveness—Prevention 35
http://www.sph.uq.edu.au/bodce-ace-prevention

Assessing Cost Effectiveness—Prevention 36
Assessing Cost Effectiveness—Prevention 37