Embed Size (px)
Citation preview

Edema: At what point is a work up needed?
Andrew Teklinski, MD, FACC

2
• Answer: all the time ‒ The edema may be indicative of a life threatening
problem on one of the scale, to a benign condition on the other end.
‒ Understanding the cause will direct the treatment ‒ Its not all heart failure

Goals
3
• Be able to define edema • Understand Starlings law of the capillary • Understand the pathophysiology of edema formation • Understand the scheme to evaluate edema based on
its presentation • Know the common causes of lower extremity edema
and their associated clinical syndromes

Edema
4
• Definition ‒ A perceptible increase in the volume of fluid in the skin
and subcutaneous tissue, characteristically indented with pressure
• Common problem for cardiologists and primary care alike
• Very prevalent, but no guidelines exist • Does not become clinically apparent until the
interstitial volume has increased by 2.5-3 liters
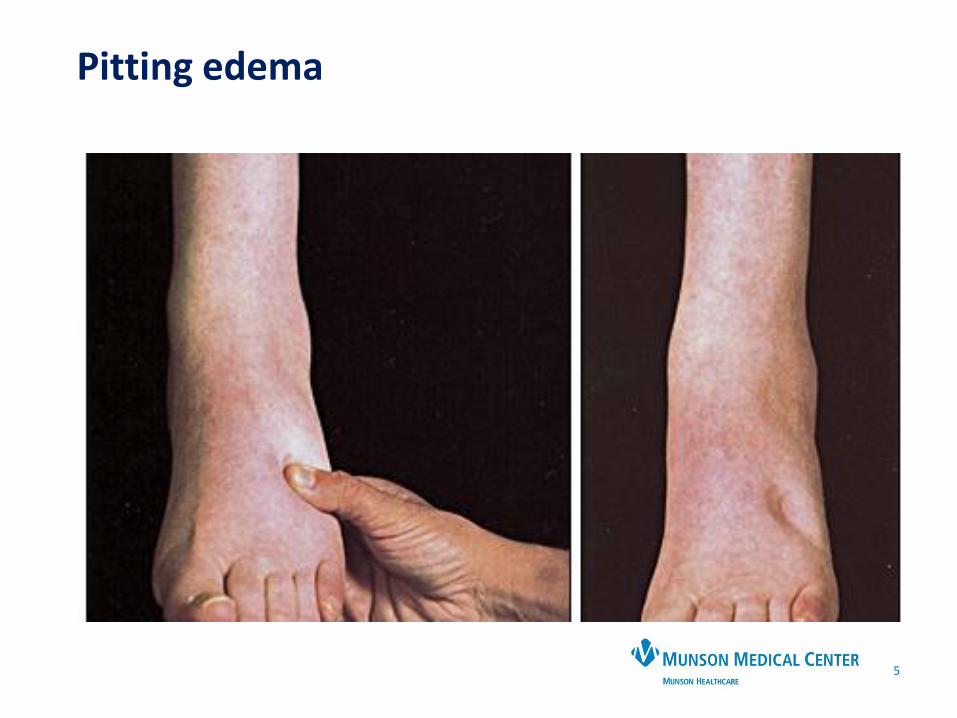
Pitting edema
5

Grading
Edema
6

Starlings Law of the Capillary
7

Relation of vessels at the capillary level
8
QuickTime™ and a decompressor
are needed to see this picture.
QuickTime™ and a decompressor
are needed to see this picture.

Factors precipitating edema
9
• Increased capillary hydrostatic pressure ‒ HF, venous obstruction, gravitational force
• Decreased plasma oncotic pressure ‒ Hypoproteinemia (malnutrition, liver disease, nephrotic
syndrome)
• Increased capillary permeability caused by proinflammatory mediators or damage to capillary structural integrity ‒ Tissue trauma, burns, dermatitis
• Lymphatic obstruction ‒ Tissue injury, obstruction, congenital abnormalities
2 types
Classification of edema
10
• Venous edema ‒ Consists of low viscosity protein-poor interstitial fluid
resulting from increased capillary filtration that cannot be accomodated by a normal lymphatic system
• Lymphedema ‒ Consists of excess protein-rich interstitial fluid within the
skin and subcutaneous tissue resulting from lymphatic dysfunction
• Lipidema ‒ Not really edema ‒ More accurately a form of fat maldistribution.
• Myxedema ‒ Deposition of mucopolysaccharides in the subcutaneous
tissues

Major causes of edema by primary mechanism
11
• Increased plasma volume due to renal sodium
retention ‒ Heart failure, including cor pulmonale ; causes about 1% ‒ Primary renal sodium retention ‒ Renal disease, including the nephrotic syndrome
Refeeding edema ‒ Pregnancy and premenstrual edema ‒ Idiopathic edema: most common cause in females less
than 50 ‒ Sodium or fluid overload: Parenteral antibiotics or other
drugs with large amounts of sodium, sodium bicarbonate, or excessive or overly rapid fluid replacement

Major causes of edema
12
Venous obstruction or insufficiency
‒ Cirrhosis or hepatic venous obstruction ‒ Acute pulmonary edema ‒ Local venous obstruction ‒ Venous thrombosis ‒ Venous stenosis ‒ Chronic venous insufficiency: most common cause in greater
than 50 ‒ Post thrombotic syndrome ‒ May-Thurner syndrome

Major causes of edema
13
• Nonsteroidal antiinflammatory drugs (NSAIDs), • Steroids: glucocorticoids, fludrocortisone, • Diabetes: thiazolidinediones (glitazones), insulins, • Hormones: estrogens, progestins, androgens,
testosterone, aromatase inhibitors, tamoxifen; • Antihypertensives: vasodilators (hydralazine,
minoxidil, diazoxide) and calcium channel blockers (particularly dihydropyridines, ie, amlodipine, nifedipine)
• Anticonvulsant: Gabapentin, pregabalin • Antineoplastic: Docetaxel, cisplatin • Antiparkinson: Pramipexole, ropinirole
Major causes of edema
14
• Arteriolar vasodilation ‒ Drugs ‒ Idiopathic edema
• Hypoalbuminemia ‒ Protein loss
• Nephrotic syndrome
• Protein-losing enteropathy
‒ Reduced albumin synthesis • Liver disease
• Malnutrition
Major causes of edema
15
• Increased capillary permeability ‒ Idiopathic edema (?) ‒ Burns ‒ Trauma ‒ Inflammation or sepsis ‒ Allergic reactions, including certain forms of angioedema ‒ Adult respiratory distress syndrome ‒ Diabetes mellitus ‒ Interleukin-2 therapy ‒ Malignant ascites

Major causes of edema
16
Lymphatic obstruction or increased interstitial oncotic pressure • Lymph node dissection • Nodal enlargement due to malignancy • Hypothyroidism • Malignant ascites • Congenital lymphatic disorders • Obstruction/inactivity

Chronic venous insufficiency
17

Idiopathic edema
18
• Menstruating women • Most common in the 20-30 age range • Should be distinguished from premenstrual edema • Causes include vascular permeability and
mineralocorticoid excess • Weight gain of > 1.4 kg as the day progresses • Face, hand and leg edema • Spironolactone is the drug of choice, HCTZ if necessary • Intermittent recumbency, avoiding environmental
heat, low salt diet, avoiding excessive fluid intake and weight loss

Complex regional pain syndrome (CRPS)
19
• Chronic, unilateral, pitting
• Sweating, pallor, irregular hair growth
• Hx of traumatic injury
• Therapeutic exercise

Ruptured Baker’s Cyst
20
• Acute, unilateral, pitting • Redness, warmth, trickling feeling • Hx of knee complications • Rest, elevation, compression

May Thurner syndrome
21

Post thrombotic syndrome
22
• Chronic, unilateral or bilateral, pitting
• History of DVT causing deep venous insufficiency
• Blood clotting disorder
• Wound care, compression
• Consider referral to a vein specialist

Common causes of leg edema in the United States
23
Unilateral
• Acute (<72 hours) ‒ DVT
• Chronic ‒ Venous insufficiency
Bilateral
• Chronic ‒ Venous insufficiency ‒ Pulmonary hypertension ‒ Heart failure ‒ Idiopathic edema ‒ Lymphedema ‒ Drugs ‒ Premenstrual edema ‒ Pregnancy ‒ Obesity

Less common causes of leg edema in the United States
24
Unilateral
Acute (<72 hours) • Ruptured Bakers cyst • Ruptured head of the
gastrocnemius • Compartment syndrome
Chronic • Secondary lymphedema
• Tumor, radiation, surgery, infection
• Pelvic tumor causing external pressure on veins
• CRPS
Bilateral
• Acute ‒ Bilateral DVT ‒ Acute worsening of
systemic cause (HF, renal disease)
• Chronic ‒ Renal disease ‒ Liver disease ‒ Pelvic tumor ‒ Pre ecclampsia ‒ Lipidema

Rare causes of leg edema in the United States
25
Unilateral
• Chronic • Primary lymphedema • Congenital venous
malformations • May Thurner syndrome
Bilateral
• Chronic ‒ Primary lymphedema ‒ Protein losing
enteropathy ‒ Pericardial constriction ‒ Restrictive
cardiomyopathy ‒ Myxedema
History
Clinical approach
26
• What is the duration of the edema? • Acute < 72 hours:
• Unilateral: DVT, Bakers cyst, trauma, compartment syndrome, MTS.
• Bilateral: DVT, acute worsening of systemic disease
• Chronic: • Unilateral: CVI, lymphedema, MTS, CRPS, congenital venous
malformations
• Bilateral: CVI, Pulmonary hypertension, CHF, Idiopathic edema,Lymphedema, Drugs, Premenstrual edema, Pregnancy, Obesity

History
Clinical approach
27
• Is the edema painful? • Yes: DVT, CRPS, ruptured Bakers cyst, post phlebitic
syndrome, trauma • Maybe: Chronic venous insufficiency (low grade aching) • No: Lymphedema
• What drugs are being taken? • Is there a history of systemic disease?
• Endocrine, cardiac, renal, hepatic
• Is there a history of pelvic/abdominal neoplasm or radiation
• Does the edema improve overnight? • Yes: venous edema, idiopathic edema
• Are there features suggestive of sleep apnea?

Exam Clinical approach
28
• BMI: obesity associated with OSA, CVI • Distribution of the edema:
‒ Unilateral: usually due to local causes: DVT, CVI, lymphedema, ruptured Bakers cyst
‒ Bilateral: local vs systemic: HF, kidney disease ‒ Generalized: systemic ‒ Dorsum of foot: spared in lipidema, but prominently
involved in lymphedema
• Tenderness ‒ Yes: DVT, lipidema ‒ No: Lymphedema
• Pitting ‒ Yes: DVT, CVI, early lymphedema ‒ No: Myxedema, advanced fibrotic form of lymphedema

Exam
Clinical approach
29
• Varicose veins: suggest CVI, but can occur without them
• Stemmer sign: Inability to pinch a fold of skin on the dorsum of the foot at the base of the second toe ‒ Advanced fibrosis in lymphedema
• Skin changes: ‒ Warty texture (hyperkeratosis) with brawny induration
are suggestive of lymphedema ‒ Brown hemosiderin deposits on the lower legs and ankles
suggest venous inufficiency ‒ Warm tender skin with increased sweating, later shiny
and cool suggests CRPS
• Signs of systemic disease ‒ JVD, crackles on lung exam ‒ Ascites, spider hemangiomas, jaundice

Myxedema
30

Myxedema
31

Lipidema
32

Lymphedema
33

Lymphedema
34
Stemmers sign

Chronic venous insufficiency
35

Chronic venous insufficiency
36

Ancillary studies
37
• Screening tests for systemic disease ‒ CBC, TSH, BMP, glucose, albumin, UA
• For suspected cardiac disease ‒ EKG, echo, BNP
• For suspected idiopathic edema ‒ Morning and evening weights. >1.4 kg change is
suggestive ‒ Water load test: 20 mL/kg water AM on 2 days, walking
or standing day 1, supine day 2. Collect urine for 4 hours after the load. Positive if <55% excreted upright, or >65% recumbent
• D dimer • Lipids
‒ Nephrotic syndrome

Ancillary studies
38
• Lymphoscintigraphy
‒ Distinguish between venous edema and lymphatic edema, and to determine the cause
• Venous ultrasound ‒ Venous anatomy, DVT
• Venous insufficiency study ‒ Evaluates venous anatomy, hemodynamics, DVT
• Sleep study • Venogram
‒ CT, MR, venography
• IVUS
Case 1
39
• 75 year old female with chronic bilateral lower extremity non painful edema. No other systemic symptoms. No changes with recumbency or overnight. No response to escalating doses of furosemide by her cardiologist
• PMH: HTN, CAD, history of PCI. Normal LVEF. No history of malignancy.
• PSH: choly • Meds: ASA, atorvastatin, furosemide, amlodipine • Exam: Normotensive, flat neck veins, clear lungs, no
murmur or S3, normal abdomen, lower extremity edema without other abnormal skin findings
• Labs: normal TSH, renal and liver function • EKG: NSR

Case 1
40

Case 1
41
• What would be the next step? ‒ A. Increase the furosemide ‒ B. Echocardiogram ‒ C. CT scan of abdomen ‒ D. Venous insufficiency ultrasound ‒ E. Stop the amlodipine
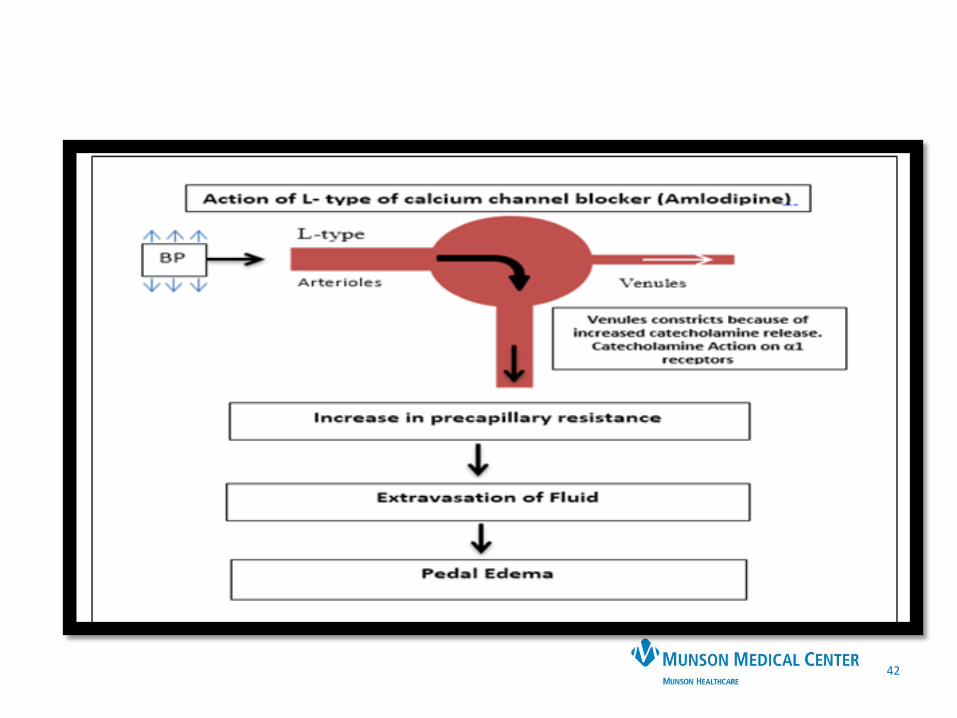
42

Edema with calcium channel blockers
43

Case 2
44
• 30 year old female with 2-3 week history of left lower extremity achiness and swelling that improves with elevation. No antecedent trauma or travel. No systemic symptoms
• PMH: None • PSH: None • Meds: none • Exam: Vitals:nl, Cardiac, pulmonary, GI exams normal,
extremities: LLE edematous, dusky, not painful • Labs: Normal CBC, TSH, LFT, BNP, D dimer • LLE US: “no DVT”, but nonpulsatile flow noted

Case 2
45

Normal vs abnormal venous flow
46

Case 2
47
• What next? ‒ A. Furosemide ‒ B. Lymphoscintigraphy ‒ C. Echo ‒ D. Bone scan ‒ E. CT venogram

May Thurner syndrome
Case 2
48

Case 2
49

May Thurner syndrome
Case 2
50
• Incidence is unknown, but ranges from 18-49% of patients with LLE DVT. (DVT is more common on the left than on the right)
• Chronic trauma to the left iliac vein from the overriding r iliac artery, resulting in intimal proliferation.
• Results in impaired venous return and risk for DVT • Diagnosis is with venography, CT veno, MRV or IVUS • Treatment is compression for mild symptoms, but for
more advanced symptoms, PCI/stent

51

Case 3
52
• 75 year old female with chronic bilateral lower extremity edema, getting progressively worse with time. Exacerbated by standing, relieved with walking, and elevation. The edema is better in the morning.
• ROS: Nocturnal leg cramping and RLS. No PND, orthopnea.
• PMH: HTN, DM • PSH: choly • Meds: Lisinopril, metformin • FH: Mother had vein stripping • SH: Non smoker. Former teacher

Case 3
53

Case 3
54
• Next step in the evaluation ‒ A. Furosemide ‒ B. Venous insufficiency ultrasound ‒ C. Echo ‒ D. D dimer ‒ E. CT venogram

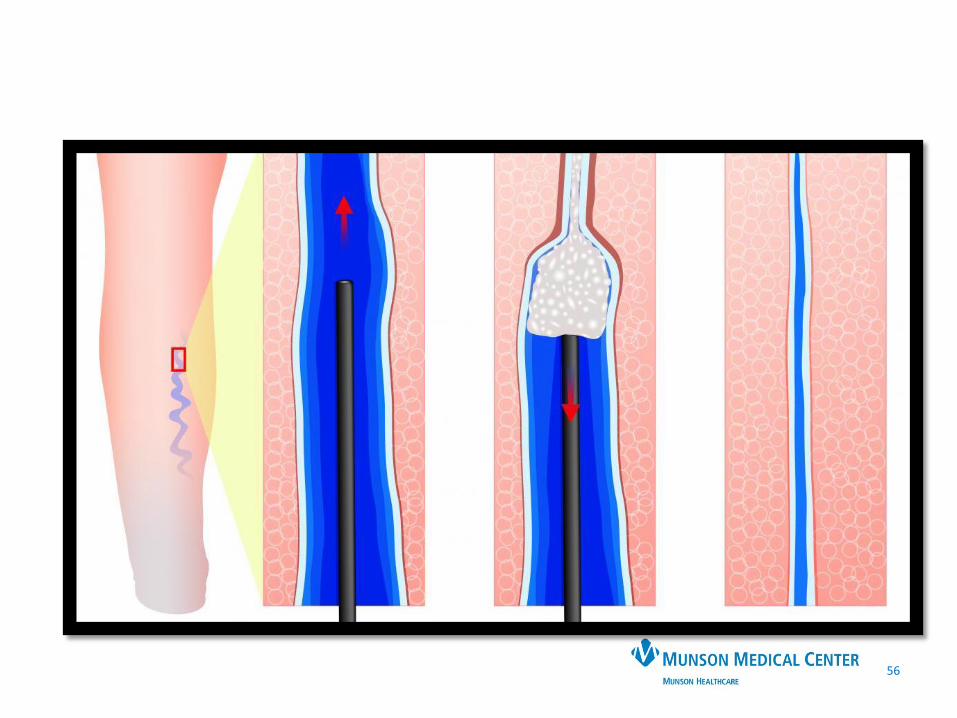
Venous insufficiency
55
• Affects 30% of the population • Various clinical presentations
‒ Symptoms: Heaviness, aching, edema provoked by standing, relieved with leg elevation
‒ Risk factors: family history, standing occupations, DVT, obesity
‒ Exam: Minimal skin findings to ulceration, pigmentation, edema
‒ Treatment • Conservative: elevation, ambulation, weight loss, compression
• Definitive: ablation (laser, radiofrequency, cyanoacrylate)
• Ra
56

57
Thank you

Major causes of bilateral lower extremity edema
58
Acute edema
Medications
Heart failure
Nephrotic syndrome
Venous thrombosis
Acute worsening of chronic causes

Unilateral or asymmetric leg edema
59
• Determine clinical probability of DVT ‒ Present in only 25% of cases ‒ Wells score/D-dimer ‒ Calf tenderness, circumference (most useful), warmth,
erythema, cord ‒ Homans sign (not reliable)

Acute unilateral or asymmetric leg edema
60
• Remaining 75% of causes ‒ Muscle strain, tear, or twisting injury-40% ‒ Leg swelling in a paralyzed limb-9% ‒ Lymphangitis or lymph obstruction-7% ‒ Venous insufficiency-7% ‒ Popliteal (Bakers) cyst-5% ‒ Cellulitis-3% ‒ Knee abnormality-2% ‒ Unknown-26%

Acute unilateral or asymmetric edema
61
• Clinical features to look for: ‒ Calf injury: supportive history, hematoma on US, bruising
at the ankle ‒ Cellulitis: May coexist with venous disease or
lymphedema ‒ Superficial thrombophlebitis: palpable tender veins, may
be a risk for DVT ‒ Bakers cyst: Posterior knee pain, knee stiffness, swelling
or mass behind the knee. Calf symptoms are common. May cause a secondary DVT from compression.
‒ Inflammatory pathology of the knee ‒ May-Thurner syndrome: young females (2d or 3d decade)
with acute pain and swelling the left lower extremity, with or without thrombus

Chronic unilateral or asymmetric edema
62
• Chronic venous disease • Lymphedema • Complex regional pain syndrome

Chronic unilateral or asymmetric edema
63
• Chronic venous disease: possible h/o DVT or thrombophlebitis. Classic pigmentary changes and skin ulceration
• Lymphedema: History of inguinal or pelvic node dissection or radiation therapy. The edema is initially pitting, but later is non pitting d/t cutaneous fibrosis
• Complex regional pain syndrome: 4-6 weeks after limb trauma. Pain, edema, and alteration in skin color or temperature

Chronic
Major causes of bilateral lower extremity edema
64
Venous insufficiency ‒ Heart failure ‒ Left-sided with preserved or reduced ejection fraction ‒ Right-sided ‒ Pulmonary hypertension (including sleep apnea) ‒ Constrictive pericarditis ‒ Restrictive cardiomyopathy ‒ Renal disease (including nephrotic syndrome) ‒ Liver disease (early cirrhosis) ‒ Premenstrual edema ‒ Pregnancy ‒ Malnutrition (including malabsorption and protein losing
enteropathy) ‒ Pelvic compression (including tumor or lymphoma) ‒ Dependent edema ‒ Sodium or fluid overload (including parenteral fluids,
antibiotics and other drugs with large amounts of sodium)
‒ Refeeding edema ‒ Idiopathic edema ‒ Inflammation (including sepsis) ‒ Medications ‒ Chronic lymphedema ‒ Primary lymphedema (presenting in childhood) ‒ Secondary lymphedema (including lymph node
dissection) ‒ Thyroid disease (myxedema)

Chronic
Major causes of bilateral lower extremity edema
65
‒ Pelvic compression (including tumor or lymphoma) ‒ Dependent edema ‒ Sodium or fluid overload (including parenteral fluids,
antibiotics and other drugs with large amounts of sodium)
‒ Refeeding edema ‒ Idiopathic edema ‒ Inflammation (including sepsis) ‒ Medications ‒ Chronic lymphedema ‒ Primary lymphedema (presenting in childhood) ‒ Secondary lymphedema (including lymph node
dissection) ‒ Thyroid disease (myxedema)

![Uveitic macular edema: a stepladder treatment paradigm€¦ · of macular edema [1,3–4], this review will focus on uveitic macular edema specifically. Uveitic macular edema Macular](https://img.pdfslide.net/doc/110x75/5ed770e44d676a3f4a7efe51/uveitic-macular-edema-a-stepladder-treatment-paradigm-of-macular-edema-13a4.jpg)



















![Fibro+Edema+Gelóide+-+power+point [Salvo automaticamente]](https://img.pdfslide.net/doc/110x75/55cf9b21550346d033a4db1b/fibroedemageloide-powerpoint-salvo-automaticamente.jpg)






