Embed Size (px)
Citation preview

Val M. Runge, MD Editor-in-Chief Investigative Radiology

Patients First – RSNA 2012
„The classical model of medical care – which portrays the authoritative physician evaluating and treating an obedient, non-inquisitive patient – is rapidly crumbling,“ „Patients have immediate access to countless resources for information. Radiologists should be a part of the movement to build another model in its place“
George S. Bisset III, MD (President, RSNA 2012)

Gd DTPA (Magnevist)
ASNR 1984
Cornelius G. Dyke Award
MR
CT
Cr EDTA
Courtesy of: Val M. Runge, MD
Kidney
Brain Abscess
RSNA 1982

1982
Aberdeen Vanderbilt
Courtesy of: Val M. Runge, MD

Magnevist
w AJR 142:619-624, March 1984
Hanns-Joachim Weinmann
AJR 142:619–624, March 1984 AJR 190:1433–1434, 2008

Primovist
Magn Reson Med 22:233-237, December 1991

Primovist
Magn Reson Med 22:233-237, December 1991
Invest Radiol 29:709-715, July 1994
Gadovist

Linear Gd Chelates Macrocyclic Gd Chelates

Perfusion, Permeability Invest Radiol 2012;47:252
Imaging faster, providing improved patient comfort, and obtaining assessments of disease hereto not possible
ORIGINAL ARTICLE
Quantification of Perfusion and Permeability in Multiple SclerosisDynamic Contrast-Enhanced MRI in 3D at 3T
Michael Ingrisch, MSc,* Steven Sourbron, PhD,† Dominik Morhard, MD,‡ Birgit Ertl-Wagner, MD,‡Tania Kumpfel, MD,§ Reinhard Hohlfeld, MD,§ Maximilian Reiser, MD,‡ and Christian Glaser, MD‡
Background and Purpose: The quantification of cerebral blood flow (CBF),cerebral blood volume (CBV), and blood-brain barrier permeability inscattered lesions in the brain is a methodological challenge. We aimed toinvestigate the feasibility of a 3D T1-weighted dynamic contrast-enhanced(DCE) MRI acquisition in combination with a 2-compartment modelingapproach for the quantification of CBF, CBV and permeability surface areaproduct (PS) in lesions, and normal-appearing white matter (NAWM) inpatients with multiple sclerosis (MS).Material and Methods: In all, 19 MS patients (mean age 35 years, 12female) underwent DCE-MRI with a 3D T1-weighted spoiled gradient-echosequence on a 3T MRI scanner. A total of 44 slices (thickness 3 mm) withan in-plane resolution of 1.7 ! 1.7 mm2 (matrix size 128 ! 104), providingcoverage of the whole brain, were acquired every 2.1 seconds over a totalmeasurement time of 420 s. Data postprocessing was performed using a setof 2-compartment models with automated model selection; CBF, CBV, andPS as a measure of blood-brain barrier leakage were determined in contrast-enhancing (CE) and nonenhancing lesions as well as in NAWM.Results: Perfusion quantification produced reasonable values in lesions aswell as in NAWM. In CE lesions, CBF (22.9 (22.7) vs. 15.8 (6.7) mL/100mL/min), CBV (1.18 (0.48) vs. 0.76 (0.19) mL/100 mL), and PS (0.98 (0.46)vs. 0.04 (0.03) mL/100 mL/min) were significantly (P " 0.001) higher thanin NAWM. In nonenhancing lesions, a weakly (P " 0.05) significantlyincreased CBV of 1.00 (0.35) mL/100 mL, compared with NAWM, wasobserved.Conclusion: Our study demonstrates the feasibility of 3D T1-weightedDCE-MRI for the quantitative assessment of CBF, CBV, and PS in NAWMas well as in multiple MS lesions scattered throughout the brain, evenwithout previous knowledge of their location. Quantification on the regionlevel produced reasonable values both in lesions and in NAWM, but parametermaps would benefit from an increase in contrast-to-noise ratio. The increasedvalues of CBF, CBV, and PS in CE lesions may reflect inflammatory activity,the heterogeneity of parameter estimates suggests a potential for lesion charac-terization. NAWM appears hypoperfused, this is in accordance with previousstudies, but requires validation with a control group.
Key Words: dynamic contrast-enhanced MRI, 3D, multiple sclerosis,quantification of perfusion
(Invest Radiol 2012;47: 252–258)
Assessing cerebral blood flow (CBF) and cerebral blood volume(CBV) in patients with a breakdown of the blood-brain barrier
(BBB) can be challenging. Traditionally, cerebral perfusion mea-surements using dynamic contrast-enhanced MRI (DCE-MRI) arebased on T2- or T2*-weighted sequences1 and are used, for exam-ple, for the assessment of tumor therapy response,2,3 although theabsolute quantification of perfusion remains subject to debate,4 inparticular in areas with BBB disruption. In contrast, T1-weightedsequences offer the advantage of quantifying perfusion also inlesions with BBB breakdown and may provide an additional param-eter of BBB leakage.5,6
Although T1-weighted acquisitions have long been used forthe assessment of BBB leakage,7–9 the feasibility of the simultane-ous quantification of CBF, CBV, and BBB leakage using a T1-weighted acquisition was demonstrated only recently6,10 in a varietyof lesions, such as cerebral metastases and primary brain tumors, aswell as in normal white and gray matter. However, a limitation ofthese studies is the incomplete coverage of the brain due to a 2Dapproach. This hindered the assessment of the entire lesion load aswell as longitudinal follow-up of intracranial lesions. A 3D approachwith full coverage of the neurocranium would therefore be desirable.
Multiple sclerosis (MS) is a chronic demyelinating disease ofthe central nervous system characterized by the presence of multiplelesions that may be in variable states of inflammatory activity.Lesional activity is usually assessed by evaluating lesional enhance-ment on T1-weighted images after the administration of gadolinium-based contrast agents (CAs).11,12 However, this approach providesonly binary information about locoregional vascularity and BBBpermeability; at most, lesional enhancement can be graded bycategories such as “weak” or “strong.” Moreover, the enhancementof a particular lesion not only depends on physiological factors, suchas increased CBV or BBB leakage caused by inflammatory pro-cesses, but also varies with MR imaging parameters, for example,the administered dose of CA or the delay between CA administra-tion and MRI acquisition.13,14 Changes in perfusion are known toprecede the development of BBB leakage and thus may form anearly step in the development of a new lesion.15,16 Moreover, severalstudies17–21 have reported reduced perfusion in normal-appearingwhite matter (NAWM) in patients with MS.
However, T1-weighted DCE-MRI in MS patients is challeng-ing because both a high spatial resolution and a large spatialcoverage are needed. Both demands could be addressed with a 3Dacquisition,22,23 but when the required high temporal resolution isachieved, a low contrast-to-noise ratio (CNR) usually ensues.6 Thelow physiological CBV values in NAWM and the resulting smallsignal changes during the first pass of CA further exacerbate thisproblem. Modern imaging techniques, such as parallel imaging orview sharing,24 can be employed to address this issue on themeasurement level. On the postprocessing level, quantification al-gorithms that reduce the number of free parameters either byintroducing additional constraints25 or by compartment modeling6
facilitate quantification even at low CNRs. Once established in MS,this approach could subsequently be transferred to other disorderswith BBB disruption, for example, cerebral metastases or gliomas.
Received July 11, 2011, and accepted for publication, after revision, October 5,2011.
From the *Josef Lissner Laboratory for Biomedical Imaging, Department of ClinicalRadiology, University Hospitals Munich–Grosshadern, Ludwig Maximilian Uni-versity of Munich, Germany; †Division of Medical Physics, University of Leeds,Leeds, United Kingdom; ‡Department of Clinical Radiology, University Hospi-tals Munich–Grosshadern, Ludwig Maximilian University of Munich, Germany;and §Institut fur Klinische Neuroimmunologie, University Hospitals Munich–Grosshadern, Ludwig Maximilian University of Munich, Germany.
Conflicts of interest and sources of funding: none declared.Reprints: Michael Ingrisch, MSc, Josef Lissner Laboratory for Biomedical Imag-
ing, Institute of Clinical Radiology, Munich University Hospitals–Grosshad-ern, Ludwig Maximilian University Munich, Marchioninistr 15, 81377 Mu-nich, Germany. E-mail: [email protected].
Copyright © 2012 by Lippincott Williams & WilkinsISSN: 0020-9996/12/4704-0252
Investigative Radiology • Volume 47, Number 4, April 2012252 | www.investigativeradiology.com

Lesion (Gd3+) Detectability Invest Radiol 2013;48:55
Technological advances are providing improved tumor detection

CE-MRI plays a key role in multiple sclerosis (MS) diagnostic imaging
CE-MRI is the diagnostic ‘gold standard’ for MS w Incorporated into the McDonald evaluation criteria w CE-T1 MRI recommended for each patient in consensus
guidelines
Enhancing T1 lesions are ‘active’ – indicate acute disease
w Uniform enhancement of new lesions w Ring-like enhancement of acute lesions as they temporally
evolve, and of reactivated old lesions

Courtesy of: Alex Rovira MD Rovira A et al. Mult Scler 2009; 15: 848 – 53 Rovira A J. EJHP Practise 2009: 15(6): 33– 35
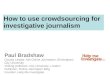
Before treatment with Betaferon®
12 months after start of treatment with Betaferon®
T2 T1 with gadobutrol
Gadovist® in Follow-up and Therapy Monitoring
Case history 33-year-old woman with previous diagnosis of relapsing-remitting multiple sclerosis
Results w No enhancing
lesions, no new T2 lesions
w Excellent clinical treatment response

Courtesy of: G. Hahn, Dresden, Germany
Gadobutrol in Pediatrics
Contrast excretion (arrows); localization and appearance suggest nephroblastoma
Courtesy of: H-J. Mentzel, Jena, Germany
CNS: Suprasellar tumor (astrocytoma) 9-year-old boy
Kidney: Solid nephroblastoma 6-year-old boy
Mild increased signal intensity within the lesion with gadobutrol (arrow)

Courtesy of: Lale Umutlu, University of Essen
Subtraction imaging
CAD analysis: malignant lesion
Non-enhanced T1w imaging
Post contrast T1w imaging
CAD Analysis

Multiparametric MR Invest Radiol 2012;47:624
Increasing the certainty of diagnosis, leading to improved patient treatment and outcomes

Improved efficacy of contrast media, leading to improved depiction of disease
Invest Radiol 2012;47:376, 2013
(on line)
Gadovist Dotarem

Compressed Sensing (for CE-MRA) Magn Reson Med
2013;69:346
This approach will have impact in many areas, initially for dynamic processes but eventually for all of clinical MR, leading to improved patient satisfaction (enabling shorter, and less invasive diagnostic exams)
Courtesy of: Mark Griswold, PhD
0.8x0.8x0.8 mm3 1 sec/volume

Cardiovascular MR Imaging … beyond Morphology
Courtesy of: Bernd J. Wintersperger, University of Toronto
@3Tesla and 1M GBCA
MRA 0.8x0.8x0.8 mm3; R=4 Dynamic MRA 0.8x0.8x0.8 mm3; R=4 3D PC GRE (300cm/s) 2.5x2.2x2.8 mm3; R=2

Myocardial Assessment … beyond Late Enhancement
%
22
24
26
28
30
32
34
36
38
40
1000
1200
400
600
800
ms
+HCT
Myocardial T1 Mapping and ECV Assessment
Courtesy of: Bernd J. Wintersperger, University of Toronto
T1-Map pre-Gd T1-Map post-Gd Extracellular Volume Map

CAIPIRINHA-DIXON-TWIST (CDT) – VIBE Invest Radiol
2013;(in press)
14 dynamic 3D frames acquired in a single breath-hold (colorectal cancer)
Courtesy of: Stefan Schoenberg, MD, and Henrik Michaely, MD
A new technique for fast time-resolved dynamic 3D imaging of the abdomen with high spatial resolution
Michaely, Morelli, Budjan, Riffel, Nickel, Kroeker, Schoenberg, Attenberger
Allowing dynamic imaging of the upper abdomen with high temporal resolution and maintained high spatial resolution

MR-PET
Courtesy of: Michael Lell MD
Pancreatic neuroendocrine tumor 68Ga DOTA-TATE
Combining the high sensitivity of PET with that of contrast enhanced MR, and its intrinsic high spatial resolution
Colorectal cancer recurrence after hemihepatectomy

Future Developments w Higher relaxivity
w Targeted agents
w Lower dose
M
M
Carbon Nanotubes, with a 4000 fold gain in sensitivity
Thrombus imaging, lymph node (metastasis) imaging
Courtesy of: Hubertus Pietsch, PhD

Conclusion
w Contrast media are an integral part of MR today, providing increased sensitivity and specificity critical to improving diagnosis, therapy, and outcome
w In the next decade we will see further advances in contrast media design and safety, playing an important role in a patient centric approach