Embed Size (px)
Citation preview

Vol.39 Issue No.3, Nov 2010
The Grasp
1
EDITORIAL BOARD EDITOR
Dr. Mukesh Gupta
CO-EDITORSDr. Pradeep BaligaDr. Manoj Gandhi
Advisory BoardDr. Lalit M. Kapoor
Dr. Arshad Gulam Moh’d.Dr. Sujata Rao
BOARD OF TRUSTEESManaging TrusteeDr. Lalit M. Kapoor
TrusteesDr. S. S. Rao
Dr. S. N. AgarwalDr. Anil SuchakDr. Dilip S. NaikDr. Bipin V. ShahDr. Bipin Pandit
WEBSITEwww.amcmumbai.com
WEB EDITORSDr. Arshad Gulam Moh’d.
Dr. Sujata RaoDr. Veena Pandit
DISCLAIMERUnless otherwise stated, the opinions expressed by the writers are their personal opinions. The AMC reserves the right to use material published in ‘The Grasp’ for its Website or for any other purpose deemed necessary.
The appearance of advertisement in ‘The Grasp’ is not guarantee or endorsement of the product or the claims made by the manufacturer / advertiser.
ASSOCIATION OF MEDICAL CONSULTANTS, MUMBAI4, Ganpati Niwas, Old Police Lines, Opp. Andheri Station,
Andheri (East), Mumbai - 400 069.Tel.: 2684 4639 / 2683 6019 (10 a.m. to 6 p.m.)
Telefax : 2682 1109E-mail : [email protected]
MANAGING COMMITTEE (2010 - 2011)President Dr. Walavalkar RajeevPresident Elect Dr. Agarwal NiranjanImm. Past President Dr. Kate SuhasVice President Dr. Rao SujataVice President Dr. Hariani Ajay R.Hon.Secretary Dr. Naik SudhirHon.Treasurer Dr. Kulkarni Gurudas B.Hon. Jt. Treasurer Dr. Das DebashishHon. Jt. Secretary Dr. Pandit VeenaHon. Jt. Secretary Dr. Pikale Sangeeta Prog. Committee Chairperson Dr. Adyanthaya Kishore Office Secretary Dr. Rao Nitin Editor Grasp Dr. Gupta Mukesh
ZONAL DIRECTORSDr. Badwe Shrikant Dr. Dave RajeshDr. Khambay S.S. Dr. Nayak Achyut Dr. Oza Umesh Dr. Parikh Ketan
COMMITTEE MEMBERSDr. Bahekar Pramod Dr. Balasubramaniam Ramnarayan. Dr. Bal Inamdar Dr. Baliga PradeepDr. Borges Eric Dr. Chawan RajendraDr. Checker Vipin Dr. Desai AjitDr. Gandhi Manoj Dr. Hegde DineshDr. Pai Hrishikesh Dr. Parikh HiteshDr. Patel Manoj Dr. Pattiwar SanjayDr. Ruke Milind Dr. Shah Jayesh Dr. Sharma Smita Dr. Shenoy GopinathDr. Sheth Rajen Dr. Shukla AshokkumarDr. Vazzifdar Khurshed Dr. Wankhade RajendraDr. Worlikar Umesh
CHAIRPERSON OF CELLSEnvironmental Protection Cell Dr. Rao P. N.Consultants Benevolent Scheme Dr. Shah Bipin V.EMS Cell Dr. Pandit BipinH & A Dr. Rao Suresh S.Hon. Doctors Welfare Cell Dr. Desai AjitInfrastructure Cell Dr. Parihar AnandMedical Council Reforms Cell Dr. Arshad Gulam Moh’dMedicolegal Cell Dr. Datar NikhilNursing Home Cell Dr. Sheth SudhaTPA Cell Dr. Badwe Shrikant
Edited by : Dr. MUKESH GUPTACo-ordinated at JAI GRAPHICS, Kandivali (East), Mumbai - 400 101
Telefax : 2885 1832 • E-mail : [email protected] Association of Medical Consultants, Mumbai. (For Private Circulation Only)

Vol.39 Issue No.3, Nov 2010Vol.39 Issue No.2, Aug 2010
The
Grasp
16

Vol.39 Issue No.3, Nov 2010
The Grasp
9
A General Physician was busy attending a case of acute MI in an ICCU in the suburbs. In the middle of this, he
received a call on his mobile phone from a Gynec nursing home in which he was one of the visiting Physicians. The nurse on the other end of the line was frantic and reported that there was a case of a 30-year old male who had come with acute chest pain and could he please come immediately to see the patient. Of course, the Physician expressed his inability to see the patient since he was busy with an emergency. The nurse, however, persisted and requested him to come as soon as possible as the gynecologist owner of the nursing home was not contactable though she was expected shortly. The other Physicians were either not reachable or busy elsewhere. The Physician explained that it would be quite a while before he could reach the nursing home and asked the nurse to contact again some other Physician. The nurse agreed to this but asked what she could give the patient meanwhile. The Physician advised her to give the patient Inj. Fortwyn 1 ml. by the intramuscular route. He then continued attending the emergency on hand.
An hour or so later, the Gynecologist called him up to inform that the patient had expired a little while after the suggested injection had been administered. It transpired that thereafter a large mob of
relatives and friends of the deceased patient had gathered and become unruly. They made several allegations including doctor not being available and wrong injection having been given. The Gynecologist called the Police who controlled the mob and, of course, the body was sent for PM.
The following day, the Physician was horrified to receive a call from the PM Doctor ostensibly to get information about the case but at the same time to enquire as to how the physician had advised on phone some injection to be given to a patient whom he had not even examined. He said this was a serious matter that amounted to medical negligence and further enquiry in the matter was necessary.
Following this , the police called the Physician for recording his statement in which he said he had advised the injection to be given for symptomatic relief since no other doctor was available. Several questions were posed to him and he had to give a number of explanations. It was quite a harrowing experience. Other issues subsequently diverted the focus of attention, and with appropriate advice, the physician managed to disengage himself from the case.
The physician had not imagined in a long shot that an innocuous advice on phone could lead to so much harassment. He
DO’S AND DON’Ts TELEPHONE CONSULTATIONS – BEWARE!Dr. Lalit Kapoor
Vol.39 Issue No.3, Nov 2010
The Grasp
Vol.39 Issue No.3, Nov 2010
knows better now and is a wiser man.
A lot many consultants will identify themselves with this physician and find the situation where advice is asked on the phone familiar. Most of them would have acted similarly.
What then is the right thing to do? Should one refuse all advice on phone? Should one give advice in selected cases or situations? What are the various implications of telephone advice?
The fact of the matter is that we do not have definite answers to any of these questions for the simple reason that these have, to the best of my knowledge, hardly ever been put to a judicial test in our country. The above case should provide us food for thought and stimulate us to seek guidelines, perhaps from MCI.
Undoubtedly, in the times ahead, with the increasing litigation-mania and the Americanisation of our medico-legal system, such issues are more likely to surface and we need to crystallize our concepts. This gains more importance in light of emergence of telemedicine / teleconsultations / distance treatment and so on.
Going back to the above case, hindsight (which is always 6 / 6) would have dictated that the physician should have insisted on some doctor seeing the patient and report to him before he could give any advice. In other words, it is my opinion that had a doctor, say an RMO or the Gynecologist-owner of the nursing home, asked for advice after examining the patient; the situation might have been more comfortable.
What about a patient trying to consult a doctor on phone? Most of you might
have noticed that there is an increasing tendency on the part of patients to consult doctors on phone, especially so after the era of mobile phones. This leads us to other questions: Should you give your cell number to all your patients, some of your patients or none of your patients. I have noticed that some consultants are more than willing to give their cell numbers to all patients whereas there are many who do so reluctantly.
My personal take in the matter of telephone consultations would be somewhat like this: (a) don’t give advice to a new patient whom you have never examined before. Ask him or her to take an appointment to see you in person. Refuse to give medical advice. In an emergency situation, there is all the more reason to insist that the patient be brought to you or taken to a Casualty room or ER as the Americans would say.
(b) In the case of a patient currently under your care, the situation is different and telephonic advice may be easier to justify. However, it should be made a practice to document the tele-conversation in the appropriate record of the patient, not of course forgetting to date and time the call and recording the name of the person on the other end of the line. Needless to add, even your old patients need not be given advice in situations where you think he / she needs to be examined before giving advice.
The next question that will crop up is: Should you charge for telephone consultations? In the USA telephone consultations are accepted in a big way. It is estimated that 25 % of interactions between patients in the USA take place on the telephone. Proper charges are taken for the same and regular bills are sent.
10

Vol.39 Issue No.3, Nov 2010
The Grasp
11
I recall a joke I read sometime back wherein an American patient who was solving a crossword, called up his doctor and asked him the medical word for “windpipe” since this was one of the clues. The doctor informed him that it was “trachea”. The patient thanked the doctor and hung up. The doctor promptly sent a bill for $ 10 under the heading “Telephone Consultation”!! In our country, of course, patients don’t even pay the regular bills, so recovering bills for telephone consultations might be a pipe dream.
To the question, which patient should be given your cell number, personally I give my number to selected patients depending on the condition for which I am treating the patient.
I know a consultant who refuses to give his cell number to any patient. In fact, there must be many such consultants. But I have also heard patients holding it against the doctor for not giving his cell number and labeling such doctors as uncaring. “I feel secure if I know I can contact my doctor instantly in case of an emergency situation “say many patients.
I suppose there can be no thumb rule in this matter and each one of us must customize our practice on this issue.
In the USA, the branch of medicine called “Telephone Medicine” is growing rapidly and several advantages have been claimed for the same. However, the downside of this is also stressed by them. It is interesting to note some of them:
Adverse outcomes resulting from communication errors in telephone medicine may range from inconvenience to anxiety to serious risks to patient safety. History taking may be inadequate in more
than half of phone calls and management decisions may be inappropriate in more than one-third.
Problems of confidentiality whilst giving test reports on telephone if these are given to family members.
Lack of visual cues prevents the physician from gauging the patient’s emotional response.
Patients calling at inappropriate times for perceived emergencies.
Another big question that is waiting to emerge from the shadows is medical consultations on-line or e-consultations . Communication by patients with their doctors, I understand, even in our country, is gaining currency. The same issues pertaining to telephone consultations will apply to these viz. malpractice liabilities, provision for reimbursement, establishment of doctor-patient relationship, and so on. We need to understand these issues at length.
I also know a number of our Consultants communicating with their patients by SMS. Methods and need for recording these may be required to be thought of.
Be that as it may,, it is better to be Safe than Sorry as far as telephone consultations or e-communications incl. SMSes are concerned. You may even land yourself in a soup as the physician in the above story realized. Hence do not give telephone or e-advice indiscriminately.
Also the fact that you will not be paid for it is an additional reason to avoid it!!
email: [email protected]

Vol.39 Issue No.3, Nov 2010
The Grasp
13
The total number of doctors in the country is estimated to be 6,70,000 to 7,00,000, the doctor : population
ratio being 6.7 per 10,000 population, against a desirable 10. But the distribution is skewed and the rural population has only 2 doctors per 10,000. The government, therefore, wants to increase the number of doctors by increasing the number of students in existing medical colleges, by a whopping 50% without increasing the bed strength. There will be 250 students where earlier there were 150, and 3 post graduate students per unit instead of 2 as at present. Quality will be sacrificed for quantity in the hope that flooding will send doctors to rural areas. More likely, they will flood urban areas even more. Mumbai is already having 22 doctors per 10,000 population, equal to the ratio in U.K. It has 20 beds against the national average of 9, and has most number of specialists, super-specialists and the most advanced technology. Yet a Mumbaikar lives an average life of 56.8 years 11 years less than a Maharashtrian, who lives 68 years. Too much commercialization or too much incompetence? Obviously doctors sell health-products, not health-services. The same picture is seen internationally. Despite poor infrastructure a Sri-Lankan
has a much better average life span than a Russian who has one of the highest medical manpower in the world.
And who are the buyers? 40% people below poverty line or poor have to depend on public sector and 30% upper class plus those who are well covered for their health needs prefer high-tech major hospitals. So, we sell our product mainly to the middle 30% people only. But the income of 50% people is shrinking while the number of specialists is increasing.
WHAT IS THE STRUGGLE AHEAD?
1) Increasing over crowding of specialists in cities has to be reduced.
2) The expenses are becoming unmanageable even to upper middle class, while the quality is declining. This results in shrinkage of the medical field.
3) There is no referral system, no functional demarcation-compartmentalization, if I may call it. The resulting insecurity and confusion explains the morbidly increasing heart attacks among young doctors.
4) We are totally neglecting primary health care and the public sector at our own peril. It is in our own interest that
STRUGGLE AHEAD Dr. S.V. Nadkarni
Vol.39 Issue No.3, Nov 2010
The Grasp
Vol.39 Issue No.3, Nov 2010
primary care improves and public sector expands. That will absorb more G.P.s and specialists, that will help expand the medical field, and that will reduce assaults on doctors, if public unrest is subdued.
5) The concept of free treatment for the poor is creating havoc not only for doctors but also for the very poor who are supposed to benefit by free treatment.
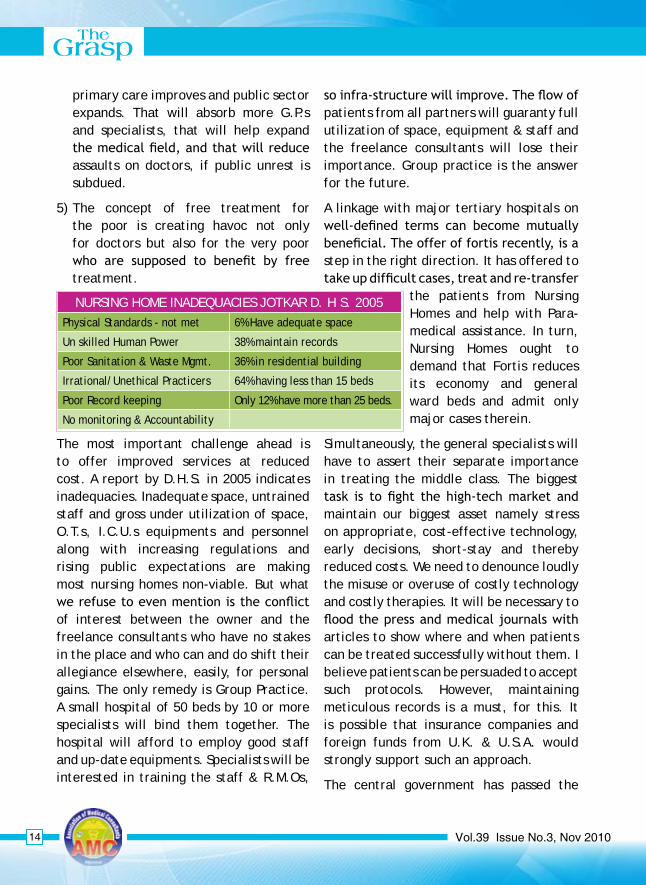
The most important challenge ahead is to offer improved services at reduced cost. A report by D.H.S. in 2005 indicates inadequacies. Inadequate space, untrained staff and gross under utilization of space, O.T.s, I.C.U.s equipments and personnel along with increasing regulations and rising public expectations are making most nursing homes non-viable. But what we refuse to even mention is the conflict of interest between the owner and the freelance consultants who have no stakes in the place and who can and do shift their allegiance elsewhere, easily, for personal gains. The only remedy is Group Practice. A small hospital of 50 beds by 10 or more specialists will bind them together. The hospital will afford to employ good staff and up-date equipments. Specialists will be interested in training the staff & R.M.Os,
so infra-structure will improve. The flow of patients from all partners will guaranty full utilization of space, equipment & staff and the freelance consultants will lose their importance. Group practice is the answer for the future.
A linkage with major tertiary hospitals on well-defined terms can become mutually beneficial. The offer of fortis recently, is a step in the right direction. It has offered to take up difficult cases, treat and re-transfer
the patients from Nursing Homes and help with Para-medical assistance. In turn, Nursing Homes ought to demand that Fortis reduces its economy and general ward beds and admit only major cases therein.
Simultaneously, the general specialists will have to assert their separate importance in treating the middle class. The biggest task is to fight the high-tech market and maintain our biggest asset namely stress on appropriate, cost-effective technology, early decisions, short-stay and thereby reduced costs. We need to denounce loudly the misuse or overuse of costly technology and costly therapies. It will be necessary to flood the press and medical journals with articles to show where and when patients can be treated successfully without them. I believe patients can be persuaded to accept such protocols. However, maintaining meticulous records is a must, for this. It is possible that insurance companies and foreign funds from U.K. & U.S.A. would strongly support such an approach.
The central government has passed the
NURSING HOME INADEqUACIES JOTKAR D. H S. 2005Physical Standards - not met 6% Have adequate space
Un skilled Human Power 38% maintain records
Poor Sanitation & Waste Mgmt. 36% in residential building
Irrational/Unethical Practicers 64% having less than 15 beds
Poor Record keeping Only 12% have more than 25 beds.
No monitoring & Accountability
14

Vol.39 Issue No.3, Nov 2010
The Grasp
15
clinical establishment Bill-2010 and accreditation is on the card soon. The association along with F.E.q.H of Mr. Gadgil is already on the job. Accrediation will be good for us, but it can spell disaster if we remain careless and ignore the aggressive high-tech high-cost market. The insistence of costly equipments with unproven merits can result in many nursing-homes being d e c l a r e d “inadequate” for major cases. Planum ven t i l a t i on , HEPA; 6 channel monitor etc. are but a few examples. We will have to insist that well m a i n t a i n e d r e c o r d s s h o w i n g a d e q u a t e results for the patients treated at the centre should be an equally important criterion of adequacy.
Compartmentalization and frontal attack on the concept of free Treatment are the other important struggles ahead. Strict compartmentalization between private and public sector is as much our need as that of the government.
Senior service doctors are quite well off-could be much better off than many of us. We must not only strongly advocate a total ban on private practice by all full-time doctors/specialists but also actively assist the authorities to implement the ban.
Similarly, we must continuously attack the concept of Free Treatment. The first step would be to denounce Free Medical Camps as an unethical practice and an insult to our brethren in service, except in disasters. Also, working as an Honarary, without per case minimum payment or free health check-ups ought to be condemned outright.
Even in public sector p r o f e s s i o n a l services must be charged. Even for the common man, these work out to be only 5% to 12% of the charges in private. But evaders must be fully charged. That will widen the net, and
expand the public sector and offer work-based incentive payment to service doctors. For example, government and municipal servants treated in public sector do not pay at all, if they are treated in their respective hospitals. If they were to be treated in approved hospitals, the govt. pays even if the patient does not. But here nobody pays. Collectively, the medical fraternity is the looser. Please realize, these families make upto 15% of the total population. Other evaders are
1) Accident victims-despite third party insurance. The public hospital fails to collect the money; the insurance company
INCOME
Private Sector Public Sector
1,00,000 Income / Salary 1,00,000
-10,000Perks - CL/PL/SL/
TA/Edu/H.R.A.25,000
-25,000PF/ Gratuity/Pension Fund
25,000
-5,000 Posturing -1,000
-5,000 C.A./Law/Media -1,000
55,000 TOTAL 1,48,000
>2,00,000 Purchasing Power Parity 1,00,000

Vol.39 Issue No.3, Nov 2010
The Grasp
17
gains and both the hospital and the doctors lose.
2) Foreigners- sometimes they do get admitted to public hospital; yet they are treated free of charge. An Australian lady was charged Rs. 300/- for fracture radius, ulna treated with Elizarov method.
3) My study in Goa indicated that atleast 40% of the patients who attend public hospitals for emergencies belong to be affording class. Infact, they don’t mind paying but there is no provision to collect the charges.
4) Politicians, MLA’s, Corporators etc.-less said about them the better.
Despite poverty, 80% of the people are reported to utilize private services for their primary health needs. It is a pity, we have donated this field to AYUSH doctors. This is mainly because everyone who wants to specialize gets training and experience in the teaching hospitals. But there is not a single day’s training for someone who wishes to become a general practitioner. We must demand that there should be a two year diploma course in general practice in every medical college and atleast 20% of the M.B.B.S graduates be absorbed therein. Similarly there is need to define the roles of G.P.s and consultants. In my opinion, G.P.s should be prohibited from prescribing very costly antibiotics and other drugs or advise very costly investigations. Such cases must be referred to the specialists. F.D.A. can easily prepare a schedule of such drugs and investigations. Specialists, in turn, must not see any patient unless he is referred by or was atleast treated first by a general
practitioner. Compartmentalization will make clinical practice more peaceful.
I believe we have a strong case to make C.P.A. non applicable to health services, because it is contract based on faith-and not just a contract. (Visit my website for the full high-court judgement) Suffice it to say we should anticipate problems and advise the policy makers or the authorities to correct their policies before rules are framed. If we do not do it-others do-mostly the envious elements or the market. We ought to talk both to masses as well as authorities a lot more.
On my part, I have written a book, in which I have analyzed the present scenario and given my blue-print for action. It is priced Rs.100/-.
I have also created a website and a forum within it. We need to discuss a lot on these issues, I request you to buy my book and discuss or add your comments on the website and forum.
MANAGEMENT OF THE SICK HELTH-CARE SYSTEM
(What is Wrong - What Can the Done) By Dr. S.V.Nadkarni,
Former Dean, L.T. Med.College, Sion. Tel :- 9320044525
Available with: Vora Medical Publication Near J.J.Hospital, Signal Trafic
Byculla, Tel. 23754161, Telfax-23704073. e-mail : [email protected] website : www.healthandsociety.in
FORUM: Social Need for
Cost Effective CLinical PracticeSONCELP -
email : [email protected]
Vol.39 Issue No.3, Nov 2010
The Grasp
Vol.39 Issue No.3, Nov 2010
As I Started my practice in 1982. I was clueless about various rules and regulations regarding private practice in Mumbai. I promptly joined AMC to get keyed in. As I interacted with fallow consultants at various events arranged by AMC. I gained knowledge and medical expertise. I also got practical tips. Be it consumer Acts, State and BMC rules and regulations like pollution control Act or fighting for doctors rights. Recently when certain rules threatened to lose down over 1200 Nursing homes in MUMBAI AMC was at the forefront to get rules amended so that we continued earning our daily bread. AMC has also
AMC is a luminous associate but can exude much more luminosity. We must improve/train consultants to introduce Guest Speaker. Also, thorough scrutiny of lectures to be delivered by Guest Speaker.
Introducing new faces will bring in novelty and break monotony.
AMC is not just Nursing homes and their owners Grievances of all consultants
WHAT I LIKE ABOUT AMCDr. Umesh Worlikar
WHAT YOU EXPECT FROM AMCDr. Lara B. Daue
arranged family get togethers at Essel world etc. as well as international tours. AMC has started its own benevolence scheme, group insurance, doctors indemnity scheme.
As I think about my journey and AMC over last thirty years – All I can say is you’re come a long way AMC you have become an internal part of every consultant life. What started as an association has ended up as one BIGFAMILY.
Recently introduced ‘Dream car project’ by AMC may make my dream (of owning a BMW) come true!
should be attended.
All this can be achieved by De-Centralising AMC activities. LONG LIVE AMC.
AMC is not just Nursing homes and their owners Grievances of all consultants should be attended.
20

Vol.39 Issue No.3, Nov 2010
The Grasp
21
With Best Compliments From:
SvessCare PharmaMaker’s of
Tab. Augcare 625 Tab.Vitonia –Z(Amoxycillin 500 Mg + Clavulanic Acid 125 Mg) (multivitamin+multimineral + lycopene)
Tab. C xim – O 200 Mg(Cefixime 200 Mg)
Tab.Gesiflam(Seratiopeptidase 15 Mg + Diclofenac Potassium 50 Mg+ Paracetamol 500 Mg)
Get the Most Out of Imaging : Advantage Innovision• The Innovision Advantage :
– Subspeciality radiology interpretations in breast and orthopaedic imaging. – Multimodality correlated interpretations: X-Ray, CT, MRI, US and Nuclear Medicine. – Radiologists who understand and cater to clinical needs.
• Personalised communication and reporting :– Rapid turn around times
– Electronic delivery of reports to patients and clinicians – Easy access for discussing cases.
• Reliable expertise :– US trained and board certifi ed* radiologists.
– Affi liated with major US medical centres.* – Now working with leading consultants in Mumbai.
• Going the extra mile :– Image guided injections & biopsies.
- Clinical research ideation & development. – Contracting with imaging centres nationwide (already in Mumbai & Nasik).
• For more information :– Call 022-2353 8599 (8:30 AM to 3:30 PM, M-F & 8:30 AM to 2.00 PM SAT).
– www.innovisionimaging.com
Vol.39 Issue No.3, Nov 2010
Sai Snehdeep hoSpitalSector 20, Koperkhairane, Navi Mumbai
125 bedded Multi-Speciality Hospital.
Expected date of launch: January 2011
Invites Specialists / Super-specialists to join as Consultants
Contact: Dr. ThaDani
Mobile: 98196-54088 • e-mail: [email protected]

Vol.39 Issue No.3, Nov 2010
The Grasp
29
About 200 years ago one Hungerian doctor was born. His sir name was Simmelweis. (I guess weis means
“WISE”) His name was Ignaz. He studied medicine & worked at Vienna General Hospital. He made Following observations.
1. Most newborns born on streets of Vienna survived.
2.Many newborns born inVienna General Hospital died of illness called peurperal sepsis. Some mothers too had the same fever after delivery and many died .
They was maternity fever of women.
They could do nothing about it.
He wondered what killed them.
His male room partner doctor also died of the same illness.
HE CONCLUDED THAT IT HAD NOTHING TO DO WITH DELIVERY.
He kept thinking about it.
AND ONE DAY IT DAWNED ON HIM.
He noted following.
“They would do dissections of dead people to learn Anatomy.
Some of these were mothers who had died of puerperal sepsis.
After that they would go to delivery rooms and do PV ( per vaginum ) examination of women in the delivery room.
These there after got the same illness.
Their babies too got it. Many died.
He thought, “They did dissection, & then they did p.v.
They carried the illness of the dead to the new mothers.
Then mothers and babies got it.”
He thought that, their hands transferred the illness of the dead, to the women and babies.
He wondered if washing hands would break this transmission.
He suggested hand washing.
No one cared.
He was not head, so he could not implement it.
But once when his boss went on leave, he became the unit in charge.
He introduced hand washing.
He made it compulsory before & after seeing every patient.
They would carry a water tub on ward rounds.
This reduced the mortality in his unit to a great extend.
There after he became head of one unit.
He introduced scrupulous hand washing in his unit.
The death rate of mothers and babies went down in his unit. It became significantly less than the unit of the department head.
STORY OF OUR GURU “MAd dOCtOR” SiMMELwEiS Dr. Rajan B. Bhonsle

Vol.39 Issue No.3, Nov 2010
The Grasp
Vol.39 Issue No.3, Nov 2010
This could not be tolerated.And no body wanted to carry water tub.No body wanted to wash hands.He published his work.
However all ridiculed him.
He could not see women and babies dying every where just because people were not washing hands.
On road, He would tell all pregnant mothers, not to go to Vienna general hospital, to save their lives and lives of their babies.
He became mad.
He cut his hand by a blade, then he did a PV. of a sick woman, got infected and died of the same illness.
He was soon forgotten. Many years later when asepsis was learned people re-looked into history and found him out.
He is father of ASEPSIS.
Let us salute to him.Let us become like him.Let us think of problems of our people.Let us find solution to them.Let us not ridicule new ideas.zz.
Lessons for us.
LET US practice good practices as follows.
1.Wash hands. Before and after seeing every patient.
2.Our fore fathers were correct. They bathed 5 times. Very good custom. Keeps you clean. In hot places, it keeps you cool.
3.The women bathed then they wore freshly washed clothes.
Only then they cooked food.No one was allowed in the cooking area. not even the head of the family.
THIS IS CALLED AS “SOWALE”
We ridicule it. BUT IT IS THE CORRECT WAY OF LIVING.
4.Our fore fathers observed SOYAR and avoided SUTAK.
Soyare means relatives. Sutak is the suffering due to death of a near one.
When a new baby arrives, All relatives (Soyare) come to see the newborn. All pick up the baby.Some kiss the baby. Some of them un knowingly give infection to the baby. Then baby becomes ill. Many such babies die daily in India. Sutak, the pain of losing baby follows.
Soyar means not allowing any one to come to see the baby and the mother till the bay is 40 days old.
This is following asepsis. A good custom. Let us encourage it.
5. Recent study published in Times of India Nov. 2010 show following.
“ Swabs are taken form many spots in houses and to see presence of e coli found in human faeces. They found that even the “Clean & elite” Indian houses had high e coli count and were dirty by world standards.
q: How to eliminate e coli from our houses?
1. 1.1 One toilet per house.
1.2 One toilet for visitors in each shop/ public place/commercial place.
2. Improve toilets.
2.1 Introduce showers in all toilets to wash perenium
2.2 Keep tissue papers. Use new paper
3 3.1 Keep soaps in all toilets.
3.2 Liquid soap better than soap care every where.
30
Vol.39 Issue No.3, Nov 2010
The Grasp
31
4. Wash hands with soap after visiting toilet every time.
5. Learn & teach hyeginic use of toilet.
6. Tell every one
all good you know, especially media, the journalists make every one wiser.
This is the best service to the nation.
Dr.Hemant Joshi Dr. Archan Joshi Virar.
POEM
My school is good except bad toilets!
I will request my school to change
My office is good except bad toilets!
I will request my office to change
My public place is good
except bad toilets!
I will request my public with help of media
My trains are good except bad open toilets
I will write/sms/email to railway minister to improve toilets.
My country is good except bad toilets!
I will request my people
with help of media to change
My home,clinic & Hospital is good
except bad toilets. I will change them.
It is not too late
to improve the toilet. Unless toilets improve
Nosocomial infections will keep killing our patients and us.
We alone can change the scene.
We will change the scene.
Jai Hind
Email: [email protected]
Do you have an untreated patient with chronic Hepatitis c (Genotype 2/3)
A new oral drug by Novartis is undergoing a clinical trial.
Do you have a patient with advanced Liver cancer?A clinical trial is on with a new oral BMS drug.The drug is intended to inhibit tumor growth.
For more details regarding the drugs & studies please contact:Dr. Samir R. Shah : 9820144338, Usha : 9819563416,
Neeta: 9819056876, Mrunal: 9329421299
email: [email protected]
Vol.39 Issue No.3, Nov 2010

Vol.39 Issue No.3, Nov 2010
The Grasp
Vol.39 Issue No.3, Nov 2010
MAll medical professionals know that practicing medicine is both art and science. It needs scientific knowledge
apart from deep understanding of human behavior. Talking about investments one is reminded about the great profession that we practice i.e. medicine. Investing is like medicine which is both art and science. The world is full of various investment theories which are both complex and difficult to understand. As potential investor you will be perpetually bombarded by various investment strategies based on charts volume and price movements.
You will be deluged with opportunities to create instant wealth. Turn your TV on 10 am to hear some of them. Twenty-twenty, khataro ke khiladi, sixer, jambazz, etc. For example, consider these enticing offers “discover a stock trading system that produces double digit profits on almost every trade! Trade right off stock market charts” Revolutionary new system …. Pays off from 50-100 percent returns in just one week” and so on and so on.
The prospectus of most mutual funds says, in small print, that past performance is no guarantee of future success. Recently, ULIPs were promised by insurance people to earn fat commissions. SEBI’s delayed intervention saved some gullible investors from falling in the hands of such agents. Medical professionals are falling prey to
mutual fund, insurance and commission agents.
Here, I want to discuss some simple and time tested methods of investing. Remember the key to investing is patience and discipline. Here we will be discussing simple investment principles especially advocated by giants Benjamin Graham, Warren Buffet, Peter Lynch and likes.
Benefit from the power of compounding
Albert Einstein actually called “compounding” as the eighth wonder of the world!
And here’s why:
vzOnce there was a king who lost a game of chess to an ordinary farmer. The king asked the farmer to choose his reward and all that the farmer asked for was 1 grain of wheat for the first square of the chess board, 2 grains for the second square, 4 grains for the third, 8 for the fourth and so on and so forth for the 64 squares. The king was very happy to be let off rather lightly and readily granted the wish. The real snag came when he tried to settle the claim.
In all required 18,446,744,073,709,551,615 grains of wheat!
All medical professionals know that practicing medicine is both art and science. It needs scientific knowledge
INVESTING - ART OR SCIENCE?Dr. N. A. Sharma
36

Vol.39 Issue No.3, Nov 2010
The Grasp
37
apart from deep understanding of human behavior. Talking about investments one is reminded about the great profession that we practice i.e. medicine. Investing is like medicine which is both art and science. The world is full of various investment theories which are both complex and difficult to understand. As potential investor you will be perpetually bombarded by various investment strategies based on charts volume and price movements.
Now, isn’t that mind boggling? What happened there was that the smart farmer used the power of compounding to his advantage. And such is the power that the king just didn’t know what had hit him. Now, would you care too whether your rate of return is 12% or 14%? The fact that if you did, it would really make a big difference to your wealth over a length of time. The benefit from compounding arises from the fact that the income keeps growing the principal gradually which result in generating higher absolute returns each year. Higher rates of return or longer investment time periods increase the principal amount in geometric proportions. And this can only be advantage to you!
Choose Simplicity over Complexity
Many people believe that investing in the stock market is complex, mysterious and risky and therefore is best left to professionals. This common mindset holds that the average person can’t be a successful investor because success in the stock market requires an advanced degree, a mastery of complicated mathematical formulas, access to sophisticated market-timing computer programs and a great deal of time to constantly monitor the market,charts,volume,economic trends, and so on. Warren Buffet has shown this
to be a myth. Remember that degree of difficulty does not count in investing. Look for long lasting companies with predictable business models. Keep it simple. Here is your goal; buy stock in a great company, run by honest and capable people. Pay less for your share of that business than that share is actually worth in terms of its future earning potential. Then hold on to the stock and wait for the market to confirm your assessment.
Make your own investment decisions
Be your own investment advisor. Beware of brokers and other sales persons who aggressively push an individual stock or mutual fund to fatten their commissions and brokerages. Obviously these people do not have your best interests at heart. Beware of people finding a new growth star, a la Infosys.
Approach financial advisors, brokers and talking heads prophets with a healthy dose of skepticism. Once you acquire the fundamental of investing, make sure that you are not taken in by financial ‘experts”. Remember that most have vested interest or agendas that don’t necessarily put your financial well being first.
To succeed in the market, says Buffet, you need only ordinary intelligence. But, in addition, you need the kind of temperament that can help you ride out of storms; and stick to your long term plans. If you can stay cool while others around you are panicking, you can prevail.
Be fearful when others are greedy and greedy when others are fearful. You can safely predict that people will be greedy, fearful or foolish. You just cannot predict when or in which order. The stock market will always be influenced by periodic

Vol.39 Issue No.3, Nov 2010
The Grasp
Vol.39 Issue No.3, Nov 2010
MAIL BAG
LETTERS
epidemics of the powerful emotions of greed and fear. Seasoned investors exploit outbreaks of these highly contagious emotions by behaving in a way opposite the prevailing sentiment!
Email: [email protected]
38
Vol.39 Issue No.3, Nov 2010

Vol.39 Issue No.3, Nov 2010
The Grasp
43
REVISED ADVERTISEMENT TARIFF “The Grasp”
BackCover
SINGLE ISSUE Rs. 20,000/-
InsideCover
SINGLE ISSUERs. 15,000/-
SINGLE ISSUERs. 12,000/- each
CentreSpread
SINGLE ISSUERs. 27,000/-each
TWO SIDESAVAILABLESINGLE ISSUERs. 30000/-
SINGLE ISSUERs. 7,000/- each
10% discount for bulk booking of four issues
CLASSIFIED : Rs. 600/- for 40 words/ Rs. 750/- for 55 words maximumINSERTS : Rs. 20,000/- for each issue for Members. Rs. 30,000/- for each issue for Non-members.
It makes a good business sense to advertise in “THE GRASP” which is mailedthrough courier in the city of Mumbai ensuring an assured and timely delivery.
Cheques to be drawn in favour of “Association Of Medical Consultants, Mumbai”
Protocol for Advertisment in “the Grasp”• All advertisements to be submitted as soft copy (CD format) with a Print-out of the Advertisement.
Handwritten copy of Advertisement will not be accepted.• Advertisement charges to be paid with a post-dated cheque at the time of booking.• If the advertisement data have been changed after submitting, kindly inform the printer also about the
change in matter.technical details : Print Area 20.5 cms. x 15 cms, Printed by Offset Process.• All matter for the printed material to be supplied by the advertiser.Please note : For advertisement material other than the POSITIVE or MATTER FOR
TYPESETTING, processing charges at cost will be charged extra.
Cover Flap
Colour(One Side)
Half page Colour
Vol.39 Issue No.3, Nov 2010
The Grasp
FOR SALE / AVAILABLE
POLYCLINIC ROOMS AVAILABLE. CALL DR SAMIR VYAS 99676 33111. SANGITA POLYCLINIC 174 S.V.ROAD, GANGAVIHAR-RESIDENCY, ANDHERI-W, MUMBAI 400058.
DOCTOR R U STRESSED??.......UNWIND BY LEARNING TO SING HINDUSTANI CLASSICAL, SEMI-CLASSICAL, BHAJANS, FILM-SONGS TAUGHT BY Pt. OMPRAKASHJI RIGHT IN YOUR HOME • HURRY! CALL UP NOW TO FIx UP YOUR CLASS – 98208 21284.
A/C CONSULTING ROOMS AVAILABLE AT A PRIME LOCATION ON S.V.RD, VILE PARLE (W), CALL DR.MAYANK KHANDWALA 09820035464, KHANDWALA EYE HOSPITAL & HEM POLYCLINIC D-31, NAVMANGAL CHS, ABOVE VENILAL SAREE SHOP, S.V. ROAD, VILEPARLE(W), MUMBAI 400 056. TEL. 022-26207430.
POLYCLINIC ROOMS AVAILABLE AT POOJA MATERNITY & NURSING HOME BHATWADI, GHATKOPAR(W)DR. JAGDIP SHAH – 9821125519/25113559. e mail: [email protected].
ATTENTION: CONSULTANTS UPCOMING NEW BUILDING FOR DOCTORS ONLY ExCLUSIVELY DESIGNED CLINICS BY RENOWNED AWARD WINNING ARCHITECT ON A ‘RESERVED HOSPITAL PLOT’ AT PRIME LOCATION NEAR DIAMOND GARDEN, CHEMBUR. CONTACT DR.S. S. HANCHATE - 982187224.
RUNNING 19 BEDED HOSPITAL WITH FULLY EqUIPPED OPERATION THEATRE AND POLYCLINIC ROOMS AVAILABLE ON LEASE ON MAIN S.V. ROAD, BORIVLI (EAST). CONTACT: 9821592223 / 022-28935475.
GUJARATI DOCTOR PARENTS INVITES ALLIANCE FOR THEIR 27 YEAR OLD ATTRACTIVE DAUGHTER PURSUING DERMATOLOGY. PREFERENCE FOR POSTGRADUATE IN MEDICAL OR ENGINEERING SETTLED IN MUMBAI. PLEASE CONTACT Email: [email protected], CELL: 9869285520, 9146034743.
AVAILABLE HOSPITAL IN GHATKOPAR WEST WITH POLYCLINIC / DIAGNOSTIC CENTRE FOR USE ONVARIOUS TERMS & CONDITIONS ALSO WANTED PHYSICIANS, SURGEON, OPHTHALMOLOGIST & PEDIATRICIAN FOR POLYCLINIC. CONTACT: DR. DALAL RAJENDRA, PRABHU KRUPA, LBS MARG, NEAR SARVODAYA HOSPITAL, GHATKOPAR (WEST), MUMBAI. TEL. 9821095329, 25152721, 25152769
RUNNING HOSPITAL PREMISES FOR OUTRIGHT SALE 1500 Sq.FT.GR.FL.WELL FURNISHED/WELL MAINTAINED, LOCATED IN THICKLY POPULATED RESIDENTIAL AREA. LESS THAN 1 KM FROM DOMBIVLI WEST AND KOPER STATION. SEPERATE ENTRANCE AND WATER CONNECTION, SMALL GARDEN ON ENTRANCE. LOAN POSSIBLE. CONTACT DR.VILAS LADDHA - 98924171479
ALLIANCE INVITED FROM MEDICAL POST GRADUATE STUDENTS/CONSULTANTS FOR FAIR 5’7” OCT’1985 BORN GIRL DOING 2ND YEAR DNB IN GYNAEC/OBSTETRICS IN MUMBAI. CONTACT: DR. RAMESH PATELCALL - +91 22 9820132863. e-mail: [email protected], [email protected].
Classifieds
44
























![Untitled-1 [] · Title: Untitled-1 Author: Hrishikesh Created Date: 1/18/2014 10:21:48 AM](https://img.pdfslide.net/doc/110x75/5f24e02ad40c3c1c481cee5c/untitled-1-title-untitled-1-author-hrishikesh-created-date-1182014-102148.jpg)




