Embed Size (px)
Citation preview

2072 BOWEL AND SPLENIC INJURY DURING RENAL SURGERY
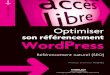
FIG. 2. Nephrostogram demonstrates opacification of small bowel.
FIG. 3. Contrast study via tube in small bowel opacifies colon as well. Foley catheter is in perinephric space and Double-J stent is placed.
and a Double-J stent was placed at the conclusion of surgery. Unfortunately significant postoperative bleeding required transfusion of 1 unit of blood on day 1 postoperatively. An- giography on day 2 postoperatively failed to reveal any source of the bleeding and hemaglobin stabilized transiently. Bleeding recurred 1 week later and the patient underwent
nephrectomy, at which a crossing arterial vessel was noted anterior to the ureteropelvic junction.
DISCUSSION
Injury to adjacent organs is a potential complication of percutaneous renal surgery. Patients with a lean body hab- itus are more at risk for colonic injury due to the paucity of retroperitoneal fat and the possibility of a retrorenal colon. Our patient was 65 inches tall and weighed 110 pounds for a body mass index of 18 kg./m.'. Also problematic was the puncture site for percutaneous access, which was clearly too lateral. The needle passed anterior to the colon, injuring the spleen and small bowel, which are intraperitoneal struc- tures. In thin patients the puncture site for percutaneous access should be more medial and superior.
Injuries to retroperitoneal organs, such as the colon and duodenum, have been successfully managed conservatively.' Our patient sustained a slight bowel injury that was con- verted into a fistula through drain placement. Small bowel fistulas are most often due to surgical trauma. Complications include sepsis, fluid and electrolyte imbalance, malnutrition and skin breakdown. Although mortality from small bowel fistulas may exceed 20% even with nutritional support, ap- proximately 30% close spontaneously.2 A fistula should be managed with bowel rest, total parenteral nutrition, ade- quate fistula drainage and appropriate skin protection. Fac- tors that prevent spontaneous closure include distal obstruc- tion, a short tract less than 2.5 cm., radiation enteritis, cancer, foreign body in the tract and inflammation, such as an undrained abscess or granulomatous disease.
Postoperatively abdominal and pelvic fluid collections are well-known complications. In patients with an easily visual- ized collection on CT percutaneous drainage is indicated and appropriate. Gram's staining and aspirate culture may then guide antibiotic treatment. Rarely does an intra-abdominal fluid collection require open surgery. Initially it was thought that this patient was a good candidate for conservative man- agement. However, after sepsis developed the consulting general surgeons believed that the most appropriate course was open surgery to repair the small bowel enterotomy and evacuate the pelvic abscess.
CONCLUSIONS
We report on a patient who sustained a small bowel and splenic injury after percutaneous renal surgery. The percu- taneous site in patients with a low body mass index should be more medial and superior to avoid bowel injury. Although we have had favorable results managing colonic injuries conser- vatively, we advocate a surgical approach in patients with small bowel injuries.
REFERENCES
1. Gerspach, J. M., Bellman, G. C., Stoller, M. L. and Fugelso, P.: Conservative management of colon injury following percuta- neous renal surgery. Urology, 49 831,1997.
2. Townsend, C. M., Jr. and Thompson, J. C.: Small intestine. In: Principles of Surgery, 6th ed. Edited by S. I. Schwartz. New York McGraw Hill, chapt. 25, 1994.
EDITORIAL COMMENT
These authors bring out several important points that I believe should be stressed. This case nicely demonstrates the problem that may occur if the nephrostomy tube is placed too far medially. Gen- erally the skin incision for the nephrostomy tube should lie between the posterior axillary line and spine, which should protect any adja- cent renal organs, such as the spleen, colon or small bowel, from injury.
The authors correctly note that the usual treatment of a pelvic abscess is percutaneous drainage. This therapy may well have re-

BOWEL AND SPLENIC INJURY DURING RENAL SURGERY 2073 solved the problem in this case, since radiograms before exploration actually showed that the puncture site in the bowel had sealed. I believe that drainage may have been an effective and much less invasive solution to the problem.
Before performing endopyelotomy in an individual with secondary versus primary ureteropelvic junction obstruction I believe that en- doluminal ultrasound or spiral CT is helpful. In a patient with secondary ureteropelvic junction obstruction these studies may re- veal that the safest site of incision is in an unconventional plane, such as posteromedial or even directly medial. In many of these patients secondary ureteropelvic junction obstruction may result from scarring of the newly constructed ureteropelvic junction di- rectly to the medial surface of the kidney. Thus, a lateral or postero- lateral incision may possibly result in significant hemorrhage, which may have occurred in this case because exploration at surgery showed only anterior crossing vessels. It would also explain why the angiogram did not show a discrete vessel, since the source of bleeding would have been diffise due to parenchymal injury. In addition, in
retrospect this patient also had significant risk factors against a successll outcome, given the relatively poor 27% function of the left kidney before initial endopyelotomy and only 20% function after repeat endopyelotomy. Recent articles have provided some prelimi- nary data relating poor renal function to a poor outcome.l.2
Ralph V. Clayman Division of Urology Washington University School of Medicine Washington University Medical Center St. Louis, Missouri
1. Gupta, M., Tuncay, 0. L. and Smith, k D.: Open surgical explo- ration aRer failed endopyelotomy: a 12-year perspective. J. Urol., 167: 1613, 1997.
2. Danuser, H., Ackermann, D. K, Bohlen, D. and Studer, U. E.: Endopyelotomy for primary ureteropelvic junction obstruction: risk factors determine success rate. J. Urol., 169: 56, 1998.