Embed Size (px)
Citation preview
Education for Clerical Staff and Charge Nurse
Medication Reconciliation Patient Safety InitiativeLast updated: May 2015

Agenda• MedRec Basics
• What is MedRec?
• Why do we need MedRec?
• MedRec Project Overview• MedRec Champions
• Implementation/Dates
• MedRec Information• Admission & Responsibilities
• Transfer & Responsibilities
• Discharge & Responsibilities
• MedRec Resources
What is Medication Reconciliation?
• Patient Safety Initiative
• Goal: • Develop a structured process to ensure that
comprehensive and accurate medication information is collected and follows the patient’s journey during key transitions of care (admission, transfer and discharge).
• Accreditation Canada ROP Requirement

Patient Safety AwarenessCommunication
and Collaboration
Why do we need MedRec?
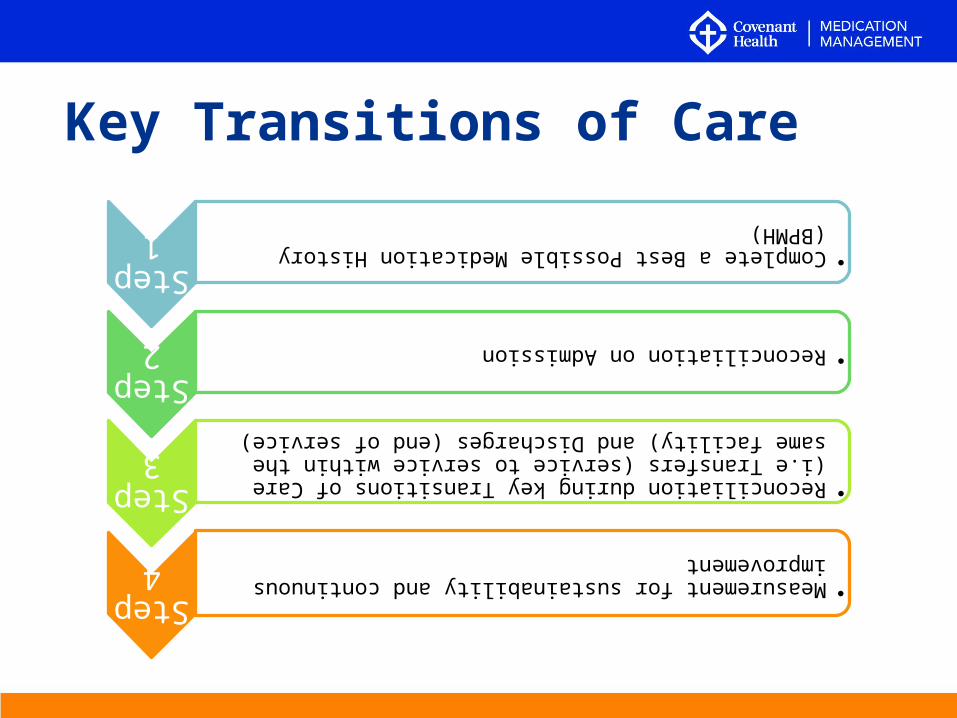
Key Transitions of Care
Step1
•Complete a Best Possible Medication History (BPMH)
Step 2
•Reconciliation on Admission
Step 3
•Reconciliation during key Transitions of Care (i.e Transfers (service to service within the same facility) and Discharges (end of service)
Step 4
•Measurement for sustainability and continuous improvement
• MedRec Leader and “Super-User”
• They have provided the MedRec Project Team with their expertise and knowledge of the program area/unit for implementation
• Will provide you (their colleagues) with support and awareness of MedRec
• Sustainability once MedRec team has finished implementation
• Liaison between the MedRec Project Team and frontline staff
What is a MedRec Champion?
Local Implementation• Begin with “Kick-Off Event”
• Implementation:
• Week One: Project Team is physically present on the local unit/site for first week Support ChampionsCoaching & guidance for local staff on the use of MedRec
tools/processes
• Week Two: Project Team available remotely via pagers• Two weeks in: auditing commences
• End with “Celebration Event”
(See dates on next slide)

Important Dates:
GNCH MCH
Implementation Dates June 15 – 26, 2015 TBD
Kick-Off Event June 15, 2015 TBD
Celebration Event June 26, 2015 TBD

Admission MedRec
• Best Possible Medication History (BPMH) is the cornerstone of the MedRec admission process.
• BPMH is:• a medication history• a reference point for decisions to continue,
discontinue or modify the medication regimen during key transitions of care
• acts as the one “source of truth”• serves as medication orders on admission
(once reconciled and signed by prescriber)
Admission
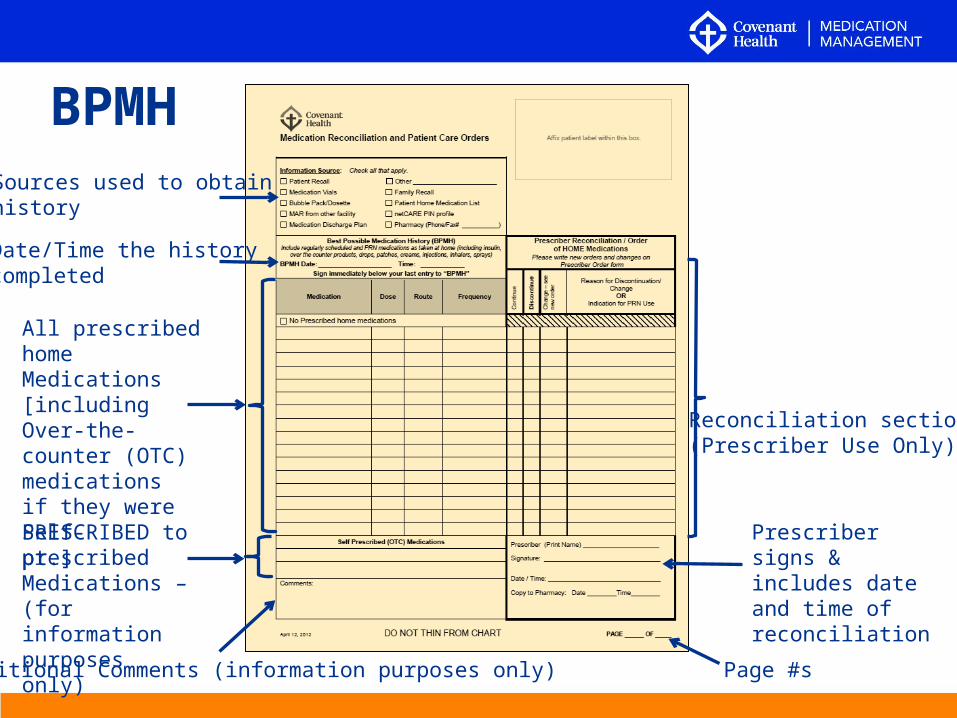
Sources used to obtainhistory
Date/Time the historycompleted
All prescribed homeMedications [including Over-the-counter (OTC) medicationsif they were PRESCRIBED to pt.]
Self-prescribed Medications – (for information purposes only)
Additional Comments (information purposes only)
Reconciliation section(Prescriber Use Only)
Prescriber signs & includes date and time of reconciliation
Page #s
BPMH
• A BPMH may be completed prior to, or alongside, all other admission orders being written (Proactive/Prospective Model)
or
• After initial admission orders have been written (Retroactive/Retrospective Model).
• In either case, a BPMH should ideally be completed within 24h of admission.
25
8.6
Admission
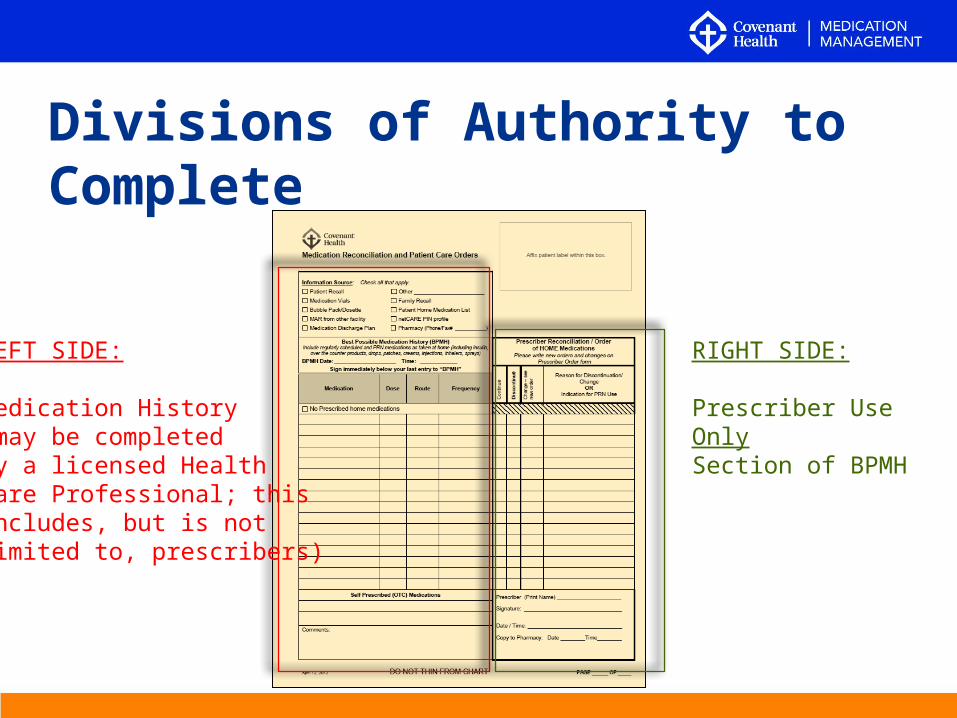
Divisions of Authority to Complete
LEFT SIDE:
Medication History(may be completedby a licensed Health Care Professional; this includes, but is not limited to, prescribers)
RIGHT SIDE:
Prescriber Use OnlySection of BPMH
• The Prescriber Reconciliation Section can be completed either:• Pre-op
or• Post-op
• This will be decided by the Admitting Prescriber on a patient by patient basis
Prescriber Reconciliation
Ensure you are checking the chart for BPMH orders Pre-op and Post-op, but note that the BPMH can only be used as an order and scanned to pharmacy once
NOT BOTH
Implementation
Starting Monday, June 15, all Surgical inpatients will require a BPMH to be completed within 24h of admission, including non-elective admissions (direct admits, ER admits).
Patients admitted prior to this and are without a BPMH do not have to have a BPMH completed retrospectively.
Direct admit from another facility
• Patients who already have a completed admission BPMH from another site (copy faxed to your site).
In this case:
• The BPMH will not serve as inpatient orders, but as a history/reference only.
• A new BPMH is not to be completed.
Who will be completing BPMHs?
For Surgery implementation, the admitting prescriber (Resident/Surgeon) is to complete the BPMH on admission.
If missed or unable to be completed at time of admission, the attending physician/team is responsible for completion the following day.
• Ideally, a BPMH should be completed and reconciled within 24h of admission. It is completed either before/with admission orders, or shortly after.
• If the patient is new to your unit, please check that a BPMH has been completed. If not, flag this to the attending prescriber/team.
When is the BPMH completed?
Where will the BPMH be kept?• The BPMH will be kept in the Patient Care Orders Section (pink
sheets) of the chart
• It will be the top page of the section and be placed opposite the pink sheets
•This is so the BPMH is easily accessible for review when the prescriber writes their orders
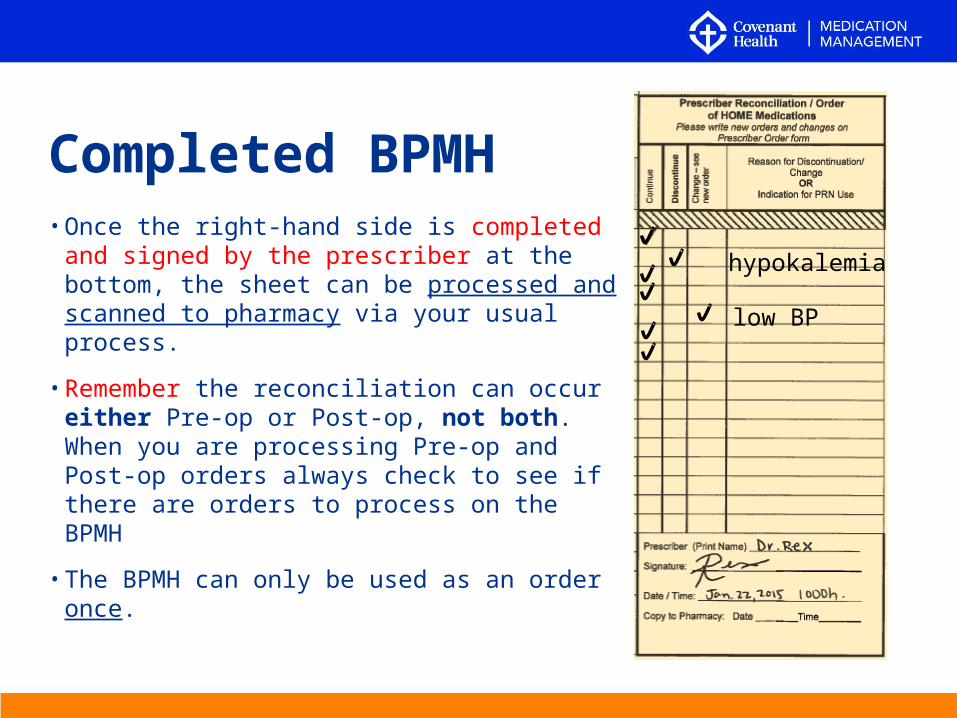
Completed BPMH• Once the right-hand side is completed and
signed by the prescriber at the bottom, the sheet can be processed and scanned to pharmacy via your usual process.
• Remember the reconciliation can occur either Pre-op or Post-op, not both. When you are processing Pre-op and Post-op orders always check to see if there are orders to process on the BPMH
• The BPMH can only be used as an order once.
hypokalemia
low BP
How to interpret columns
The following slides help explain how to interpret the various columns on the BPMH tool
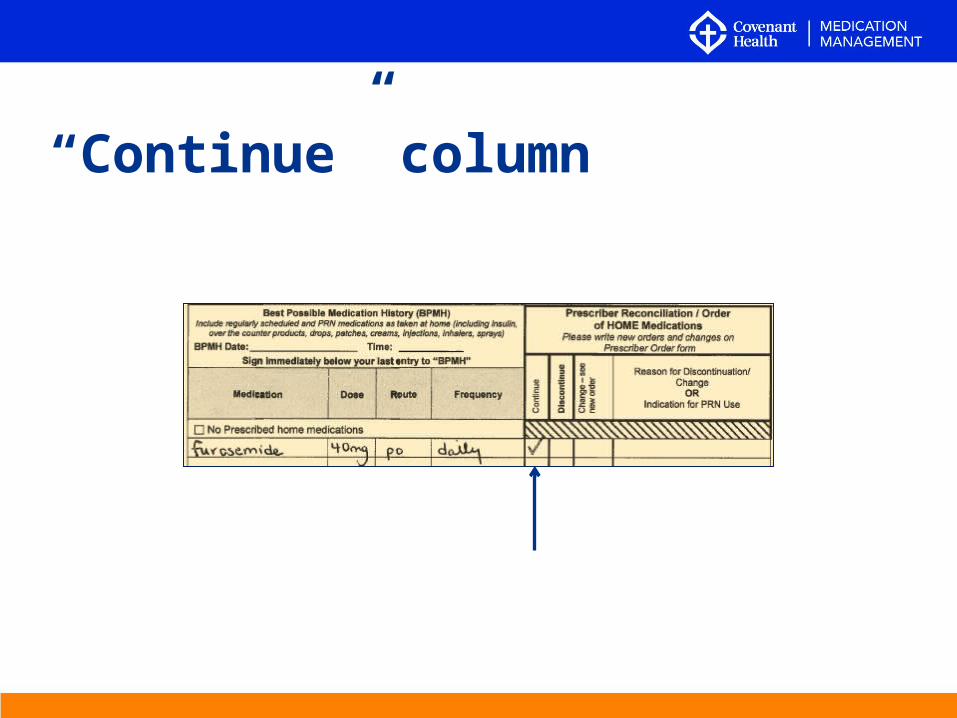
“Continue” column
“Continue” column
This means the prescriber would like the medication to continue in hospital exactly as written. This serves as a Prescriber’s Order.
What if this medication is already ordered?
If the prescriber selects “continue” and there is a previous order for this medication, the BPMH order will replace the older order (just as any new Prescriber’s Order would). The older order is then “discontinued” and replaced with the new order.
FYI Safety Alert:
• If the previously active order was identical to it, do not duplicate entries on the MAR! Only one is to be active.
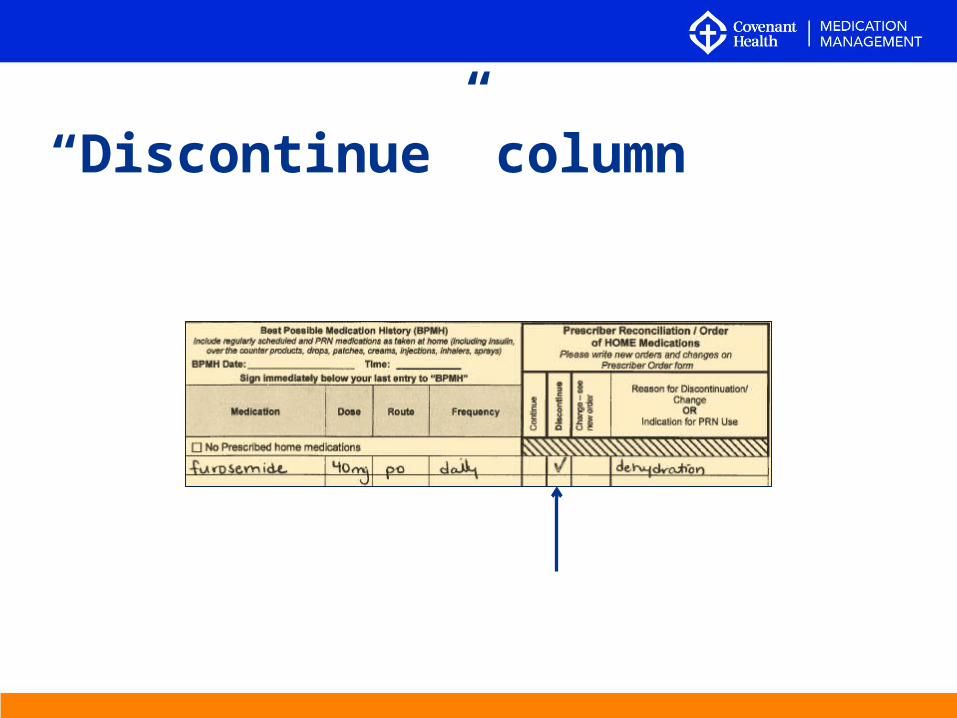
“Discontinue” column
“Discontinue” column
If this column is selected, the medication as written will be stopped.
If there is an identical existing order previously active in the chart, then discontinue it.
If the medication has never been ordered yet since admission, this is for information and communication purposes only.
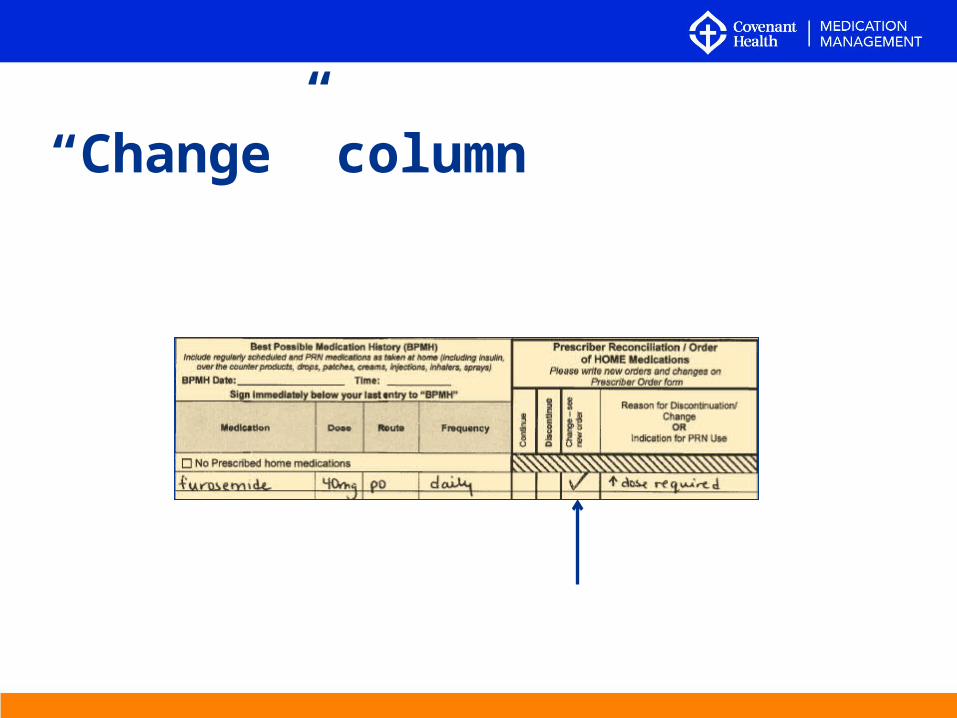
“Change” column
“Change” column
This means the prescriber has determined that the medication will still be prescribed, but in a different way (change to dose, route and/or frequency).
In this case, do not process the order as it reads on the BPMH. The new replacement order will be written separately in the Patient Care Orders section – this is the order to process.
When in doubt…
If you are unsure of the intent or how to process any of the BPMH orders, or they appear to conflict with previous orders, please confirm with the prescriber.
• New information may be learned about the patient’s HOME medications after the initial BPMH is processed.
• Any licensed health care professional may document the new information so the home medication history is as accurate as possible
• If there is no room, start a new admission BPMH page and renumber all associated pages
BPMH Tool: Late Entries
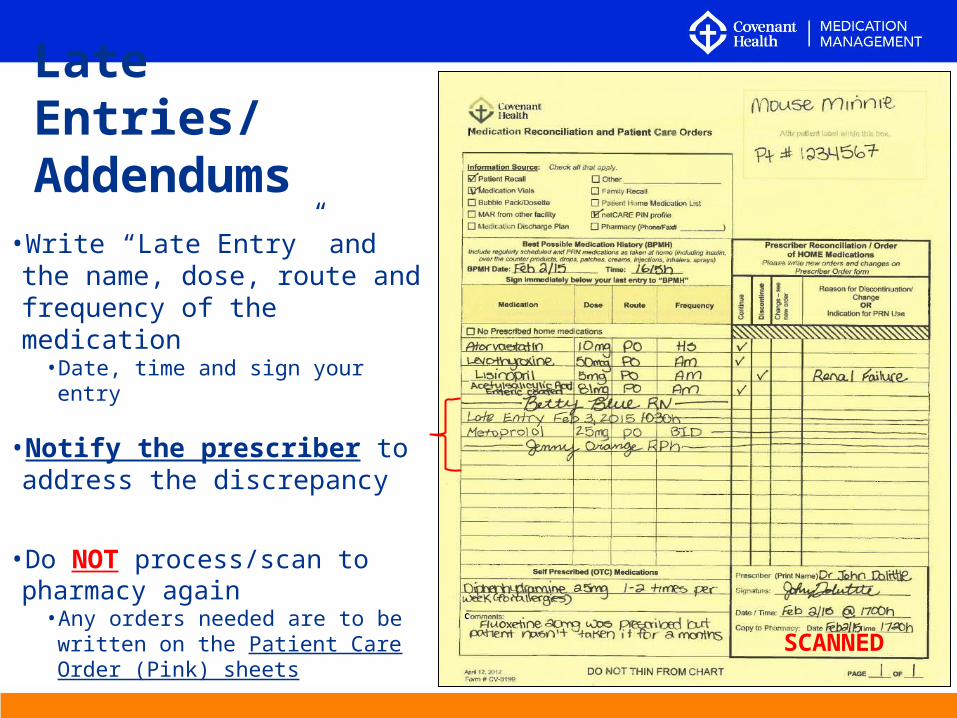
•Write “Late Entry” and the name, dose, route and frequency of the medication
• Date, time and sign your entry
•Notify the prescriber to address the discrepancy
•Do NOT process/scan to pharmacy again
• Any orders needed are to be written on the Patient Care Order (Pink) sheets
Late Entries/Addendums
SCANNEDC
What is my role in Admission MedRec?
• Printing a Netcare Medication Profile (ED only)
• Ensuring a BPMH sheet (Best Possible Medication History) is in the chart of all new admissions
• Exception: Direct admits from another facility; the sending facility’s BPMH will be used as reference and a new BPMH is not to be completed.
• Once BPMH is complete, it is to be processed and scanned to pharmacy.
• It is to be stored in a clear sleeve in the Patient Care Orders (pink sheets) section of the chart.
• Any documents used to obtain this history (Netcare printout, lists) should also go in this folder, behind the BPMH.
• If BPMH contains active diabetic orders, a photocopy is to be made and placed into the diabetic orders section.
• Remove sleeve upon patient discharge
• Flag to Prescribers any patient who has been admitted for more than 24h that does not yet have a BPMH completed
What is my role in Admission MedRec?

Transfer MedRec
Transfer
A change in service, and/or level of care within the facility
• ex. Grey Nuns Surgery to Grey Nuns Internal Medicine
• If the attending physician changes/rotates but the patient remains cared for by the same service, this is not considered a transfer
• Within-service bed changes are not considered transfers
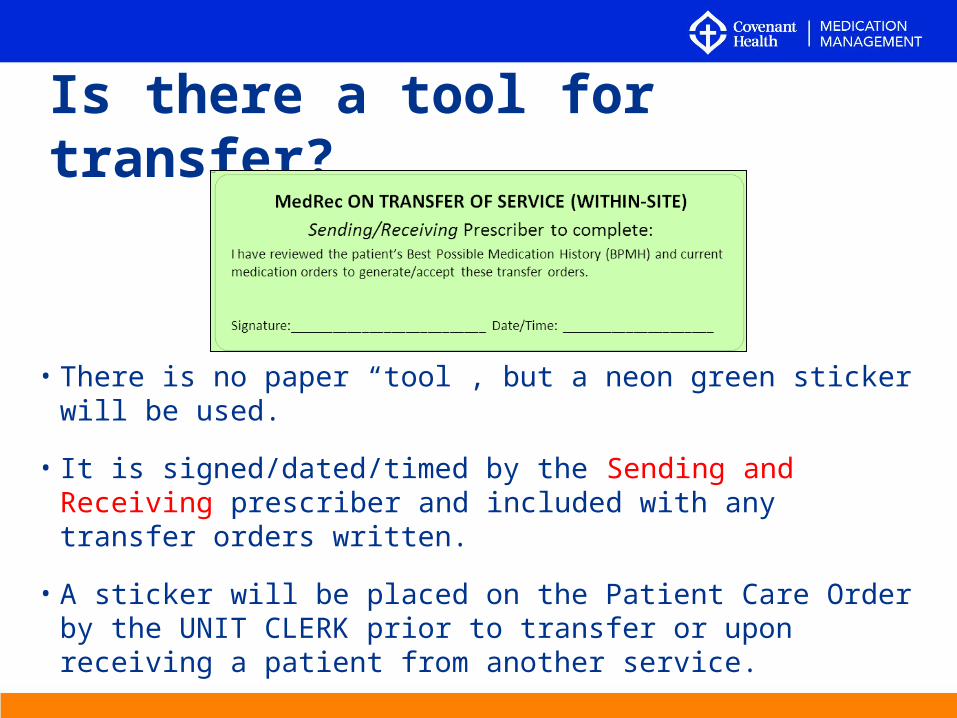
Is there a tool for transfer?
• There is no paper “tool”, but a neon green sticker will be used.
• It is signed/dated/timed by the Sending and Receiving prescriber and included with any transfer orders written.
• A sticker will be placed on the Patient Care Order by the UNIT CLERK prior to transfer or upon receiving a patient from another service.
Receiving a Patient within the Facility
If the Surgery Program is receiving a patient from another service, the Receiving Prescriber will sign the MedRec Transfer sticker acknowledging the BPMH medications and current medications have been reviewed
Sending a Patient within the Facility
If the Surgery Program is sending a patient to another service, the Sending Prescriber will sign the MedRec Transfer sticker acknowledging the BPMH medications and current medications have been reviewed
• Exception: “Vascular IMCU Transfer Orders” PPCO will have a check box on the last page to indicate when this task is completed. (see next slide)
The PPCO reads: The above orders were created upon review of the patient’s current medications and Best Possible Medication History (BPMH)
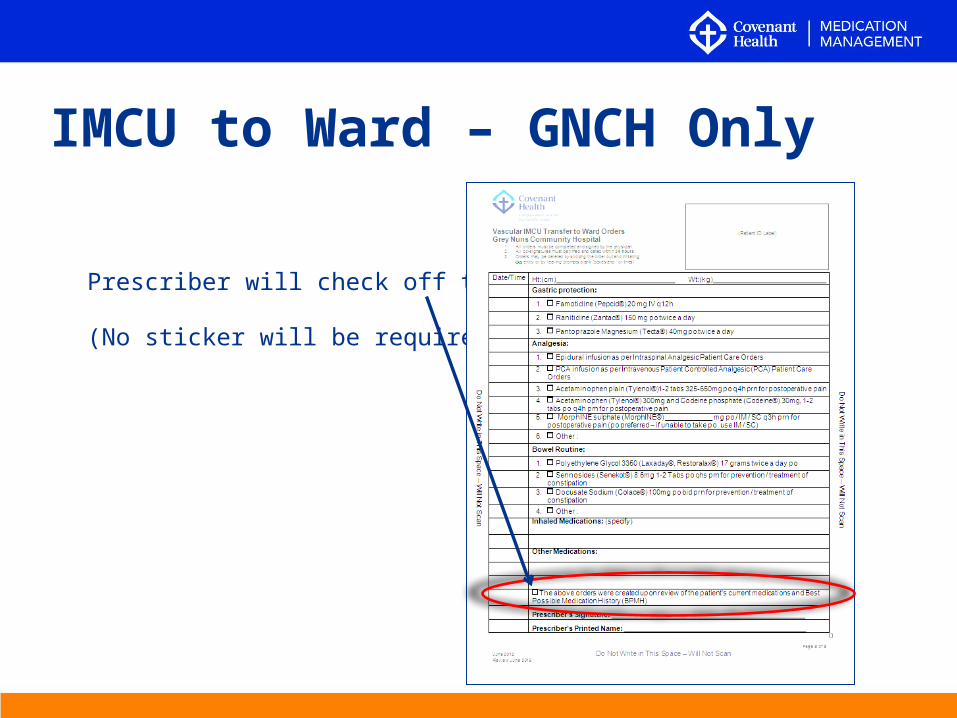
IMCU to Ward – GNCH Only
Prescriber will check off this box
(No sticker will be required)
What is my role in Transfer MedRec?
• Be aware that when a patient is transferring within hospital to another service from your unit or when receiving a patient from another service, the MedRec transfer sticker is to be included on the pink sheets with any transfer orders written/accepted.
• Exception: When an IMCU transfer to ward PPCO is used
• Ensure the stickers are readily available for prescribers.
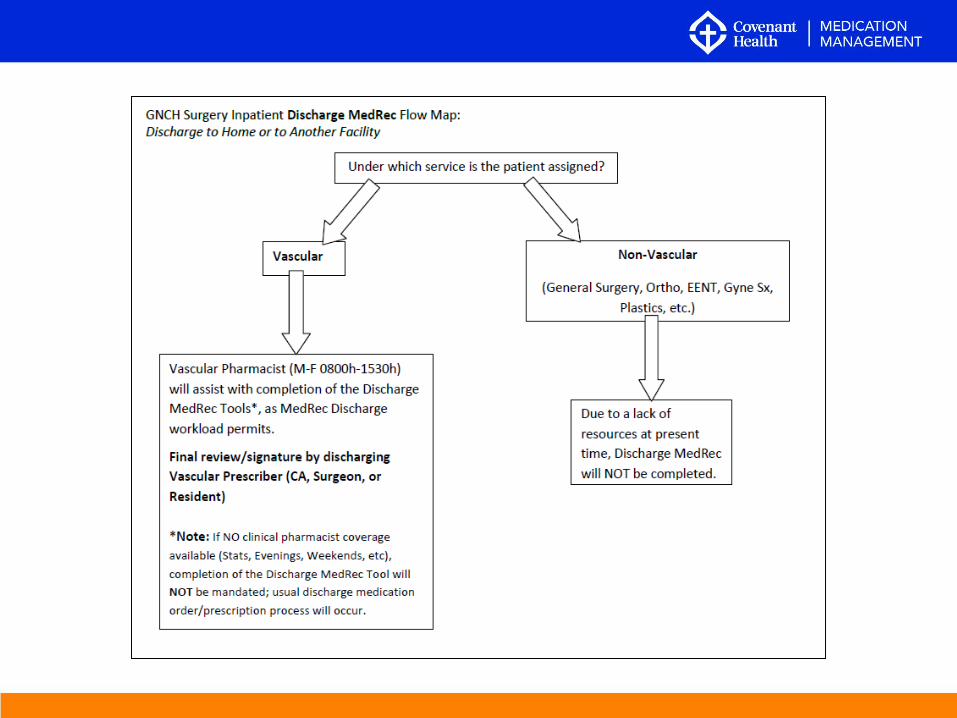
Discharge MedRecGNCH - Vascular Service Patients Only
Note: For all Non-Vascular Surgery Patients (i.e General Surgery, Ortho Surgery, Gyne Surgery etc), Discharge MedRec will not be completed. Please continue with your current Discharge Process.
Discharge
• Refers to the end of service provision by the care facility• i.e. the patient physically exits the current facility
and subsequently goes home or to a different care facility
Tip: “Elvis has left the building” and is not returning (Case number is closed)
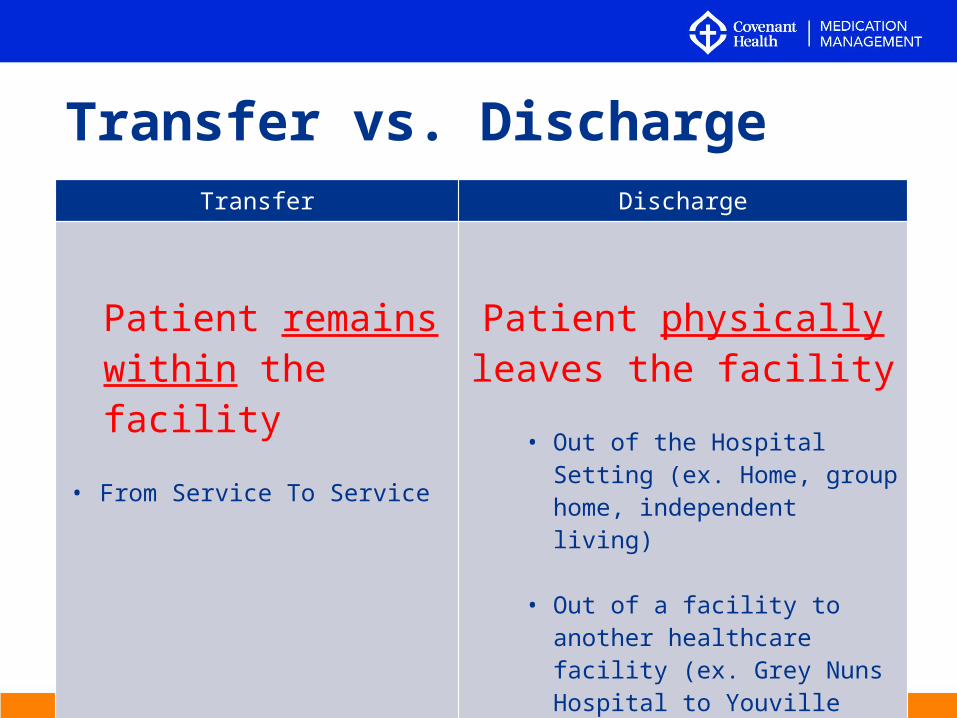
Transfer Discharge
Patient remains within the facility
• From Service To Service
Patient physically leaves the facility
• Out of the Hospital Setting (ex. Home, group home, independent living)
• Out of a facility to another healthcare facility (ex. Grey Nuns Hospital to Youville Home)
Transfer vs. Discharge
• Complete and accurate list of discharge medications
• Plus a list of discontinued home medications
• Once signed by prescriber:
• Discharge medication orders (if going to another facility) and/or
• Prescription (if a quantity specified)
• Replaces current discharge prescription process
Why a Discharge MedRec Tool?
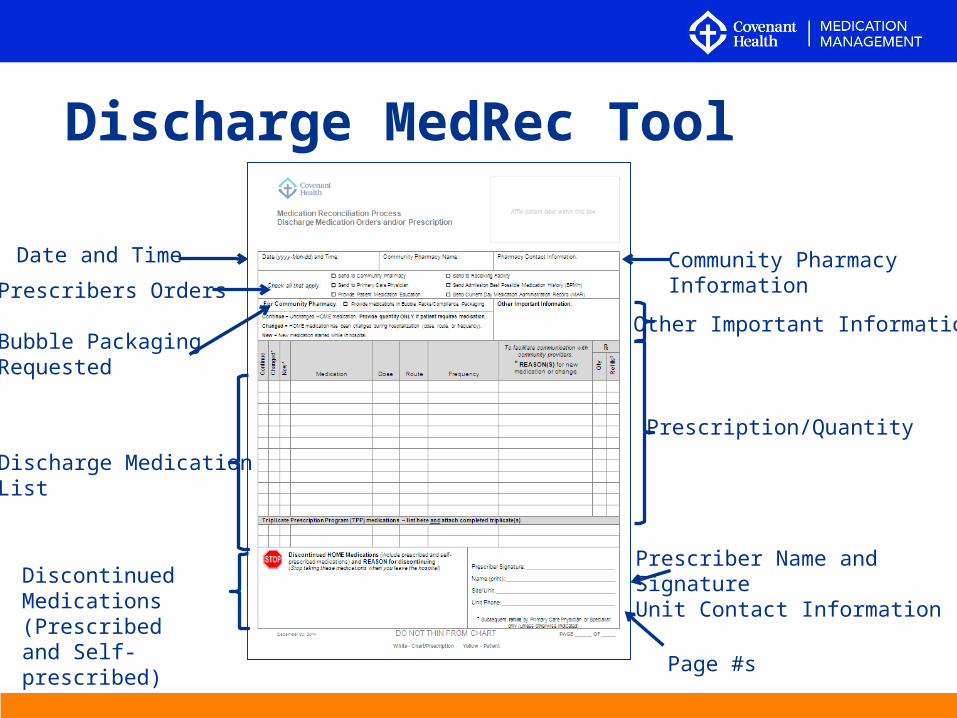
Discharge MedRec Tool
Date and Time
Prescribers Orders
Bubble Packaging Requested
Discharge MedicationList
DiscontinuedMedications (Prescribedand Self-prescribed)
Prescriber Name andSignatureUnit Contact Information
Prescription/Quantity
Page #s
Other Important Information
Community Pharmacy Information
Discharge Tool: Two-plyWhite ply:
• Chart copy. If patient would prefer to take this copy in person to his or her pharmacy, a copy of it must be made for the chart. Clearly mark the photocopy as, “CHART COPY.”
Yellow ply:
• Copy for patient/resident or caregiver for information purposes
• Provide along with yellow copy of the Short Stay Discharge Summary Form.
• Patient/caregiver will always receive this copy.
If Discharge Tool is faxed to a Community Pharmacy
• In this case, the patient will ONLY receive the Yellow copy
What if the patient does not have a BPMH?
• Effective the start date of implementation, a discharge MedRec tool is to be completed for ALL VASCULAR SERVICE patients being discharged
• Even if there is no official BPMH in chart from admission.
Discharge directly to another facility
• BPMH should be faxed to the receiving facility in addition to the discharge MedRec tool.
• This provides the receiving facility with an understanding of the patient’s home medications, as a point of reference.
Where is the discharge tool kept?
Place a blank tool in the Discharge Section of the chart.
If more than one page is required by the prescriber, please be aware of where additional pages can be found.
What about if a bridge medication supply is needed?
• Continue with the current process already in place.
• This includes a prescriber order on the designated form for pass/bridge medications.
What is my role in Discharge MedRec?
• Ensuring a blank Discharge MedRec Tool is in the Discharge Section of the chart
• Once completed, process pages and fax to any requested locations
• If the patient is being sent directly to another healthcare facility the admission BPMH should be faxed to them as well
• Liaise with bedside nurse to ensure the patient/caregiver always receives the yellow carbon copy of the tool upon discharge
• If patient is also taking the white copy (prescription) in person to their pharmacy, a copy of it must be made for keeping in the chart
How are the tools ordered?Ordered from Forms (DATA Group):
• Admission BPMH: • Medication Reconciliation CV- 0199 (1-ply)*• *Note: there is also a CV-1099NCR 2-ply version – please ensure
you order the 1-ply if your unit scans orders to pharmacy!
• Discharge Tool: • Discharge Medication Reconciliation CV- 0375 (2-ply)
----------------------------------------------------------------------------------------------
Transfer Tool: is a sticker template available on CompassionNet (compatible with labels 4" x 1-1/3“ – 14 per page. (Avery 5162, 5262, 5522, 5662, 5962, 8162, 8252, 8462, and 8662)
Measurement and Evaluation
Auditing:• Auditing of admission and discharge MedRec will
occur on a monthly basis by your unit’s designated auditor.
Measure QuestionSuccess Measure Was MedRec completed?Quality Measure Was it done well?Outcome Measure Were there any discrepancies?
Measurement and Evaluation:
MedRec ResourcesCompassionNet
• Internal and External Resources
• MedRec Policy
• On Deck with MedRec Newsletters
MedRec Info Binders• Binder will be at unit clerk’s desk
MedRec Flow Sheet/Responsibilities Poster
• Will be on all units
MedRec Project Team• [email protected]
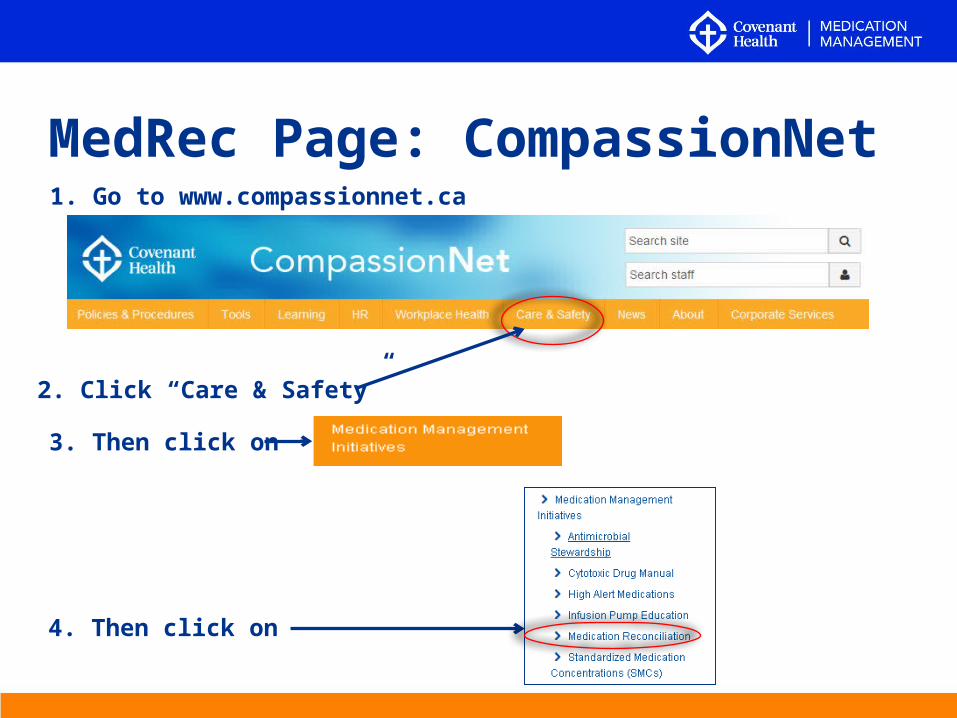
MedRec Page: CompassionNet1. Go to www.compassionnet.ca
2. Click “Care & Safety”
3. Then click on
4. Then click on
If I have questions, who do I ask?
• MedRec Champions
• MedRec Team • During implementation dates: in-person and via pagers;
• pager #1: (780) 445-5398 (Jessica)
• pager #2: (780) 969-9879 (Laura)
• After implementation dates: via email
RLS
If you discover any MedRec related incidents, please report them as you would any other incident discovered.
• Do you have proposed changes to the MedRec initiative?
• Complete a “Change Request Form” (available on CompassionNet)
• Submit to: [email protected]
• Questions? Feedback?
• Email [email protected]
Contact Us







![Medication Reconciliation and Management[1] - Care for …careforelders.org/html/Medication_Reconciliation_and_Management[1... · Medication Reconciliation and Management 1. ... •](https://img.pdfslide.net/doc/110x75/5ac9890a7f8b9a6b578d1c77/medication-reconciliation-and-management1-care-for-1medication-reconciliation.jpg)





















