Embed Size (px)
Citation preview
Educational Design (Pre Conferences) Safe Patient Handling and Mobility Conference, Glendale Arizona, April 11-15, 2016
Title Safe Patient Handling and Mobility: Hands On with the Newest SPHM Technologies with Limited Participant Specialty in Rehabilitation
Presenters name and credentials Kay Steadman, Margaret Arnold, Brad Dugan, et al. Description (1 paragraph) This pre-conference provides a tutorial and opportunities to gain competencies in the newest patient handling equipment as it
relates to the patient’s level of independence. This program will be most helpful for direct care providers as well as educators and safety peer leaders responsible for assessments of staff. Participants will rotate through 3 unique stations over the course of this workshop. In addition to the Hands On stations we are providing a limited participation for those of you wanting a focus on 3 stations specific Rehabilitation’s influence on patient goals. You must confirm participation for the rehabilitation special offering at the time of registration to attend as it is a separate offering internal of the Hands On.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. To incorporate best practices for the use of SPHM technologies in to clinical use strategies to reduce adverse events. 2. To incorporate best practices for the use of SPHM technologies into rehabilitation strategies to improve patient function and reduce adverse events associated with immobility. 3. Evaluate technological solutions for safe patient handling and falls management. 4. To incorporate a competency model for participants. 5. To identify basic biomechanical principles which assist the participant in the identification of ergonomic hazards across patient care settings covered in the session. 6. Apply best practices for reducing patient handling risks to caregivers.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. To more effectively identify SPHM, SPHM technologies and adverse events to target and reduce at-risk behaviors in caregivers: a. Will create lists of at risk behaviors b. Will carry on table and panel discussions on key elements of risk. 2. To incorporate best practices for the use of SPHM technologies into rehabilitation strategies to improve patient function and reduce adverse events associated with immobility. a. Will engage in Rehabilitation station exercises to demonstrate best practices and tenants of patient mobility. b. Will identify multiple levels of mobility and the impact of managing each level. 3. To evaluate technological solutions for safe patient handling and falls management. a. Will identify 7 categories of SPHM technologies. b. Will engage in group station participation and discussion about each technology category to improve use, competency methods and identify gaps for safe use and application. c. Identify technology role in falls management in stations, technology choice and panel discussion. 4. To incorporate a competency model for participants. a. Will cover a competency model in presentation for participants to follow in station experiential. b. Panel discussion covers competency and training for facility implementation. 5. To identify basic biomechanical principles which assist the participant in the identification of ergonomic hazards across patient care settings covered in the session. a. Presentation of anatomy and biomechanical limitations as it relates to the injury and disease process. b. Coaching on technique in stations during technology use. 6. Apply best practices for reducing patient handling risks to caregivers. a. Technology station participation with clinical leaders on practices. b. Individual identification of at least one best practice the participant will implement and discuss impact the participant is anticipating from that implementation. c. Update on SPHM regulation in panel presentation.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Interactive group in technology stations, highly participatory activities , PPT and panel discussions.
References (3-5 evidence-based publications)
1. Nelson, A., Motacki, K., & Menzel, N. (2009). The Illustrated Guide to Safe Patient Handling and Movement. New York: Springer Publishing. 2. The Working Back: A Systems Review by William Marras. 3. W. S. Marras, G. G. Knapik, & S. Ferguson, "Lumbar spine forces during maneuvering of ceiling-based and floor-based patient transfer devices." Ergonomics 52, no. 3 (2009): 384-97. 2. 4. VISN 8 Patient Safety Center Technology Resource Guide. http://www.visn8.va.gov/VISN8/PatientSafetyCenter/default.asp. 5. J. Lloyd & A Baptiste, "Friction-reducing devices for lateral patient transfers: a biomechanical evaluation," American Association of Occupational Health Nurses 54, no. 3 (March 2006): 113-19. 6. Waters, T. R. (2006). Using the NIOSH lifting equation to determine the maximum recommended weight limits for manual patient handling tasks. Presentation at the 2006 Safe Patient Handling and Movement Conference, march 2006, St. Pete Beach, FL. 7. Institute of Medicine (US). 2001. Crossing the quality chasm: a new health care system for the 21st century. Committee on Quality of Health Care in America, Washington DC. National Academies Press.
Title Ergonomics and Biomechanics 101 Presenters name and credentials Guy Fragala Ph.D., PE, CSP, CSPHP Description (1 paragraph) Appropriate for newcomers and attendees who have a rudimentary understanding of ergonomics and want to develop their skills
and understanding in this area in more depth. Basic concepts of ergonomics will be discussed including how primary risk factors such as force, repetition and posture contribute to occupational risks to health care workers. Safe patient handling problems will be defined from an ergonomic perspective and solution strategies suggested. Participants will learn the basics to begin an ergonomic risk assessment. An overview of current solutions available will be presented demonstrating how ergonomics is applied to reduce risk. This workshop will prepare attendees to investigate solutions in more depth at the main conference.
Objectives (Learner Outcomes in 1. Understand how basic concepts of ergonomics are applied to better match job demands to worker capabilities. 2. Understand
Behavioral Terms). Upon completion learner will be able to:
how to begin a basic ergonomic risk assessment related to safe patient handling and mobility in a healthcare facility. 3. Discuss application all of basic safe patient handling and mobility technology to address problems identified related to occupational risk from patient handling activities. 4. Understand how to reduce exposure to ergonomic risk factors force, repetition and posture for caregivers and healthcare.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. What is the science or discipline of ergonomics, 2. Understanding the job demands related to patient handling activities, 3. Does application of ergonomics make sense in healthcare, 4. Risk identification and assessment in the environment of care, 5. Risk analysis in the environment of care, 6. Formulating recommendations applying appropriate safe patient handling and mobility technology, 7. Understanding risk factors and minimizing occupational risk.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Lecture, Discussion and Interactive Activities References (3-5 evidence-based publications)
1. Fragala, G. “Creating Safer Environments for Long-Term Care Staff and Patients”, Annals of Long-Term Care, February 2012 pp. 2-6. 2. Fragala, G. “Facilitating Repositioning in Bed”, American Association Occupational Health Nurses Journal (AAOHN),February 2011, Vol. 59, pp. 63-68. 3. Nelson, A., Fragala, G. “Development and Evaluation of a Multifaceted Ergonomics Program to Prevent Injuries Associated with Patient Handling Tasks”, International Journal of Nursing Studies, 2005. 4. Fragala, G. Ergonomics: How to Contain on-the-Job Injury, Joint Commission on Accreditation of Healthcare Organizations, Chicago, IL, 1996
Title It Takes a Village to Implement a SPHM Program Part I Presenters name and credentials Margaret Arnold, BSN, PR, CEES, CSPHP; Jennifer Binkley, DPT, OCS, CSPHA, CEAS II; Teresa Boynton, MS, OTR, CSPHP; Debbie
Coughlin, PT, CSPHP; Lena Deter, RN, MPH, CSPHP, LTC-SSC; Dee Kumpar, RN, BSN, MBA, CSPHP; Laurel Helfen-Lardent, OTR/L, MHA, CEAS, CSPHP; Renee Kielich, RN, CSPHP; Charlotte Lynch, MS, CNS, CSPHP; Elizabeth Potts, BSN, RN-BC, CEASII; Carys Price, PT, MS, CSPHP, CEAS II; Linda Stevens, DNP, RN-BC, CPHQ, CSPHP; Sandy Swan, RN, BSN, MS, COHN-S/CM; CEAS, CSPHP; Patty Wawyziecki, MS, CSPHP; Wendy Weaver, MEd; Kent Wilson, CIE, CSPHP
Description (1 paragraph) This 2 day/13 hour workshop provides SPHM novices working in the acute care, long-term care and/or a community setting with the basic knowledge and skills required to implement a SPHM program at his/her facility. Day 1 is a seven-hour pre-conference. Day 2 is a six-hour post-conference. A bridge between the two workshops is created throughout the conference by the use of luncheon meetings. A workbook will be provided to each participant. Part 1 provides a brief description of SPHM, introduces the novice to program implementation, provides an introduction to the "best practices" important to program development including the development of laundering and inspection processes, and provides the novice with the necessary tools to successfully navigate the conference.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Describe the method of program implementation that you will use for your facility. 2. Explain the best practices you will use to pilot, choose and purchase equipment including friction reducing devices and slings. 3. Describe the laundering and inspection process your facility will use to ensure the safety of slings and FRDs.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Various implementation models available; Barriers and solutions to implementation; Pros and cons of various implementation programs that have been used in case study facilities. 2. Pros and cons of various types of equipment, slings and FRDs; reusable versus disposable; determining amount of equipment, FRDs and slings for your facility. 3. Writing SOP for laundering.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Novice
Method of Presentation PowerPoint presentations, Interactive learner activities, learner workbook.
References (3-5 evidence-based publications)
1. American Nurses Association. (2013). Safe patient handling and mobility: interprofessional national standards. Silver Spring, MD: NursesBooks.org. 2. Occupational Safety and Health Administration. (2009). Guidelines for Nursing Homes, Ergonomics for the Prevention of Musculoskeletal Disorders (OSHA 3193 2003; rev. 3/09). US Department of Labor, Occupational Safety and Health Administration. 3. Matz, M. (2010). Facilitating Acceptance of a PHAMP and PHAM Technology. C Borden (Ed.), Patient Handling and Movement Assessments: A White Paper. Dallas, TX: The Facilities Guidelines Institute. 4. Matz, M. (2013). Safe Patient Handling Unit Binder: peer leader. Retrieved 1/21/15 froM: http://www.tampavaref.org/safe-patient-handling/UPLUnitSPHBinder.pdf. 5. Nelson, A. (2006). Safe patient handling and movement. New York: Springer Publishing, Inc. 6. Nelson, A., Motacki, K., & Menzel, N. (2009). Patient Safety Center of Inquiry. (2006). Patient care ergonomics resource guide: safe patient handling and movement. Tampa, FL: VISN 8 Patient Safety Center of Inquiry.
Title Post Fall Management Presenters name and credentials Patricia A. Quigley, PhD, ARNP, CRRN, FAAN, FAANP Description (1 paragraph) This session will provide clinicians with review of the evidence, core practices for falls management and relevant clinical skills at the
point of care. Tools and strategies for falls management will be provided. Participants also will be challenged to redesign patient education strategies to maximize patient engagement in fall management plans. Afternoon break will be provided
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Summarize evidence of current fall management practices and clinical expertise. 2. Demonstrate core skills in fall management. 3. Examine tools to reduce preventable falls.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Evidence: Multifactorial interventions, single interventions from multisite vs. single hospital studies, summary of fall management interventions for hospitals from AHRQ toolkit. 2. Core Skills: Fall risk screening vs. fall risk assessment; Population-based fall management; 3. Clinical skills
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation PowerPoint presentation, Discussion, Q&A References (3-5 evidence-based publications)
Agency for Healthcare Research and Quality, (2008). The U.S. Preventive Services Task Force Procedure Manual. AHRQ Publication No. 08-05118-EF. Retrieved January 5, 2009 from http://www.ahrq.gov/clinic/uspstf08/methods/procmanual.htm. Wright, A.D., & Laing, A.C. (2012). The influence of head for orientation and flooring systems on impact dynamics during simulated fall-related head impacts. Medical Engineering & Physics, 34, 1071–8. Wu, S., Keeler, E., Rubenstein, L., Maglione, M. A., & Shekelle, P. G. (2010). A cost- effectiveness analysis of a proposed national falls prevention program. Clinics in Geriatric Medicine, 26, 751–66. Yates, K. M. & Tart, R. C. (2010). Acute care patient falls: Evaluation of a revised fall prevention program following comparative analysis of psychiatric and medical patient falls. Applied Nursing Research, 25, 68–74.
Educational Design (Day One) Safe Patient Handling and Mobility Conference, Glendale Arizona, April 11-15, 2016 Title Just Culture and Safety in Health Care Presenters name and credentials
John Westphal, BS
Description (1 paragraph)
A just culture organization, like many others, has a mission. Its pursuits and reason for being are grounded in certain values it has determined are most important to it. Now imagine every employee protects those values by the choices they make and how they accomplish their duties.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. List the five skills of a just culture. 2. Define the skills of a just culture.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. List the skills: a. Values, b. System, c. Behavioral Choices, d. Learning Systems, e. Justice. 2. Define the skills: a. Defining and understanding competing values. b. Managing the quality of the system desdign. c. Managing the quality of the behavioral choice. d. Use of learning system principles to encourage reporting and leraning from errors, while using investigative rules and concepts to analyze errors and events. e. Establishment of fair and consistent guidelines to affect accountability.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation
Oral presentation with powerpoint slides.
References (3-5 evidence-based publications)
1. Marx, D. (2007). Patient safety and the "just culture." Albany, NY: State of New York. Available at http://www.health.ny.gov/professionals/patients/patient_safety/conference/2007/docs/patient_safety_and_the_just_culture.pdf. 2. Bishop, A. C., & Cregan, B. R. (2015). Patient safety culture: finding meaning in patient experiences. J Health Care Qual Assur, 28(6), 595-610. 3. Brunt, B. A. (2010). Developing a just culture. Brentwood, TN: HealthLeaders Media. May 18. Available at: http://healthleadersmedia.com/content.cfm?content_id=251182&page=1&topic=NRS##.
Title The Art of Story Telling to Drive Behavior Presenters Nelson, Dick
name and credentials Description (1 paragraph)
People do things for their own reasons, NOT yours. Stories are a powerful tool to relay a message, get people to think and ultimately drive behavior. But story telling is a skill and has a methodology to do it well. Join us for a story telling adventure and craft your own powerful story to use at your facility.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Participants will learn the 5 “gotta be’s” to telling an effective story. 2. Participants will learn the 4 types of stories that drive behavior change. 3. Participants will craft their own story to use at their facility
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
All
Method of Presentation
Heavy facilitation, participant involvement, hands on.
References (3-5 evidence-based publications)
1. Stanford University Story Telling Project. 2. The Science of Story Telling: How narrative cuts through distraction like nothing else by Jonathon Gottschall. 3. Why your Brain Loves Good Story Telling by Paul J Zak in Harvard Business Review
Title The One Safety Program: Using High Reliability to Integrate Patient and Employee Safety in One Program Presenters name and credentials
Tom Peterson, MD, FAAP, VP, Chief Safety Officer, SCL Health; Nancy McGann PT, CSPHP, Ergonomic Injury Prevention Coordinator, SCL Health
Description (1 paragraph)
The basic concepts and strategies implemented on the journey to become a high reliability organization will generate groundbreaking knowledge to enhance, sustain, evaluate and create permanent culture change for safe patient handling and
mobility. Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Upon completion, participant will understand basic concepts of HRO’s as they relate to Healthcare and SPHM. 2. Upon completion, participants will understand the need for a new way of thinking about safety in healthcare that other industries have already successfully conquered. 3. Upon completion, participant will learn strategies to instill HRO principles into their SPHM programs.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1 Basic Concepts HRO. a. HRO Concepts and Strategies as it relates to patient and associate safety. b. Increasing reporting of near miss events is critical to long term success. 2. Industrial Examples a. Nuclear power, airlines and construction outcomes after becoming HRO’s, b. Basic tenants and systems work for any organization. 3. HRO strategies to use in SPHM program. aUsing near miss reporting and leading indicators to effectively guide and enhance a SPHM programs. b. Accountability through reporting, huddles and rounding will be reviewed through clinical campaigns, rewards and information sharing, c. Specific examples of benefits will be explained.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation
Powerpoint and Handouts including sample tools to facilitate objectives
References (3-5 evidence-based publications)
1. Mark R. Chassin, M.D., FACP, M.P.P., M.P.H. President and Chief Executive Officer, “Zero patients harmed: The promising future of healthcare: Commitment to zero patient harm and preventable death is the first step towards achieving it.” http://www.patientsafetyupdates.com/industry-news/getting-healthcare-to-zero-patients-harmed#.U04KqSlOWdH. 2. High Reliability Organization Learning Network Operational Advice From the Exempla Healthcare Site Visit: Becoming a High Reliability Organization: Operational Advice for Hospital Leaders. April 2008. Agency for Healthcare Research and Quality, Rockville,MD.http://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/hroadvice/hroadviceapb.html. 3. Dekker, S; The Field Guide to Understanding Human Error, June 30, 2006. 4. Safety Culture & Behaviors of Error Prevention Training: SCL Health System, February 2014. 5. Reason, James. Managing the Risks of Organizational Accidents. Burlington: Ashgate,2001.
Title Exploring Organizational Dimensions of Culture and Their Impact on SPHM Programming and Behavior Change Presenters name and credentials
Renée Kielich, RN, CSPHP; Gail Powell-Cope, PhD, ARNP, FAAN
Description (1 paragraph)
This presentation looks at the research on organizational culture and the cultural dimensions necessary for sustaining healthy organizational culture. Ten cultural dimensions will be explored as a foundation for evaluating the necessary elements in successful
safe patient handling and mobility programming. The presentation will focus on the inclusion of safe patient handling and mobility programming in hospital quality initiatives and outcome management for both patients and their caregivers to emphasize a culture of safety within the healthcare environment. Behavioral change management will be addressed to show the importance for sustaining the necessary practice change at the bedside.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Examine the theoretical elements of organizational culture change in current SPHM literature. 2. Understand the importance of a "culture of safety" to ensure successful safe patient handling and mobility programming. 3. Review organizational culture dimensions necessary for sustaining change. 4. Relate culture change to safe patient handling and mobility programming. Learning outcome: Based on organizational culture dimensions the learner will formulate at least one strategy to use for implementing SPHM within their facility and one strategy for sustaining SPHM within their facility.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Examine the theoretical elements of organizational culture change in current SPHM literature. a. Review of the culture references found in current publications and literature. b. Define culture and irs importance to organizations. 2. Understand the importance of a "culture of safety" to ensure successful safe patient handling and mobility programming. a. Discuss caregiver outcomes realized through SPHM practices, b. Discuss patient outcomes realized through SPHM practices. 3. Review organizational culture dimensions necessary for sustaining change. a. Ten dimensions will be reviewed: leadership, structure, planning, innovation, environment, job performance, communication, humanistic workplace, development of the individual and socialization on entry. b. These dimensions will be discussed in detail on why they are necessary for healthy organizations. 3. Relate culture change to SPHM programming. a. Behavioral change management model will be utilized to discuss how to influence change on a personal, social and environmental level. b. The 10 dimensions of culture will be analyzed side-by-side with the necessary elements described in SPHM literature as necessary for successful and sustained SPHM programming.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation
PowerPoint
References (3-5 evidence-based publications)
1. Handbook of Organizational Culture & Climate, Neal M. Ashkanasy, Celeste P. M. Wilderom, Mark F. Peterson. 2. Questionnaire Measures of Organizational Culture, Neal M. Ashkanasy, Lyndelle E. Broadfoot, Sarah Falkus. 3. How to 10X Your Influence, Joseph Grenny. Vital Smarts. 4. The Advisory Board Company; Managing Disruptive Change, Best Practices for Overcoming Employee Resistance 2009. 5. Switch: How to change things when change is hard, Chip and Dan Heath.
1/26/2016 1:27 PM | 1
Educational Design (Day Two) Safe Patient Handling and Mobility Conference, Glendale Arizona, April 11-15, 2016
Title 9 Years On and Still Going Strong--Tips to Keep SPH Relevant and Successful Presenters name and credentials
Margaret Arnold, BSc, CEES, CSPHP, Rehabilitation Services Coordinator; Kay Steadman, MA, OTR, CHSP, Ergonomist
Description (1 paragraph) This session will identify the steps in program development and when and where to include plans for sustainability and how to incorporate these methods into your practice.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Identify the steps in program development and when and where to include plans for sustainability. 2. Describe best practices in program sustainability. 3. Understand how to incorporate these methods into your practice.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Program Development: Assess current program; choose applicable best practices. 2. Program Sustainability: Teamwork; Communication Strategies; Regular Analysis/Follow Up
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation PowerPoint presentation, Discussion, Q&A References (3-5 evidence-based publications)
1. Durable Medical Equipment (DME) Coverage. http://www.medicare.gov/coverage/durable-medical-equipment-coverage.html. 2. Matz M. Patient Handling (Lifting) Equipment Coverage & Space Recommendations. 2007 http://www.visn8.va.gov/patientsafetycenter/safepthandling/coveragespacerecs.doc. 3. Campo M., Shiyko M. P., Margulis H., & Darragh A. R. (2013). Effect of a safe patient handling programs on rehabilitation outcomes. Archives of Physical Medicine and Rehabilitation, 94, 17-22. 4. Darragh A.R., Campo M. A., Frost L., Miller M., Pentico M., & Margulis H. (2013). Safe-patient-handling equipment in therapy practice: Implications for Rehabilitation. American Journal of Occupational Therapy, 67, 45-53. 5. Arnold, M., Combs, J., Gach, R., & Lecreche, M. (2015). Overcoming barriers to mobilizing bariatric patients: three case studies. Am J SPHM, 5(2), 47-54.
Title Safe Patient Handling Along the Continuum of Care
Presenters name and credentials
Kent Wilson CIE, Debra Slack Katz RN, Anthony Donaldson CSPHP, Vicki Missar MS CPE SSBB CSPHP CHSP. Moderator: Guy Fragala PhD PE CSP CSPHP
Description (1 paragraph) Safe patient handling is an important consideration across the continuum of care which includes acute care, long term care, ambulatory care and home care. Although there are common risks and problems across the continuum of care there are also specific differences which must be considered when doing assessments and determining solutions. This session will present a panel of experts with specific knowledge in each of the areas of care. Common areas of risk will be considered and risk specific to each area of care will be discussed. Methods for assessment and appropriate solutions for each area of care will be explored.
1/26/2016 1:27 PM | 2
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Discuss the common safe patient handling risks across the continuum of care. 2. Understand the different safe patient handling problems specific to each area of care. 3. Gain knowledge of solutions for safe patient handling problems specific to each area of care.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Safe Patient Handling Risks Across the Continuum of Care 1a. Are there safe patient handling risks common to all healthcare settings. 1b. Are there safe patient handling risks specific to acute care, long term care, home care and ambulatory care. 2. Safe Patient Handling Problems Specific to Individual Care Settings. 2a. What are the safe patient handling problems specific to acute are, long term care, home care and ambulatory care. 2b. What are the obstacles to solving safe patient handling problems for an organization with a variety of care settings. 2c. What are the specific obstacles to solving problems in each individual care setting. 3. Finding the Proper Solution for Problems Identified. 3a. What are the technology needs for the different care settings. 3b. What are the organizational and program needs necessary to develop and implement solutions.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Panel Presentation, Discussion
References (3-5 evidence-based publications)
1.Macdonald, C., (2010). Brief: Importance of Accessible Examination Tables and Weight Scales, Center for Disabilities Issues and the Health Professions, Western University of the Health Sciences, Pomona CA, Edition 5. 2.T. Lagu et al., (2013). Access to Subspecialty Care for Patients With Mobility Impairment: A Survey, Ann Intern Med. 158(6):441-446. 3.Pharr, J. R. (2013). Accommodations for patients with disabilities in primary care: a mixed methods study of practice administrators. Global Journal of Health Science, 6(1), 23-32. 4 Fragala, G., Fragala, M. “Repositioning Patients in Chairs-An Improved Method”, Workplace Health & Safety. April 2013 Vol.61 No. 4 pp.141-144. 5. Fragala, G. “Lifting Up, Implementing the Right Safe Patient Handling Program and Equipment Can Help Reduce Risks”, Environment of Care News, Joint Commission Publication, July 2012, Vol. 15, No.7 pp. 7-10. 6. Fragala, G., Perry, B., Fragala, M. “Examining Bed Width as a Contributor to Risk of Falls from Bed in Long-Term Care”, Annals of Long-Term Care, June 2012 pp. 35-7. 7. Fragala, G. “Creating Safer Environments for Long-Term Care Staff and Patients”, Annals of Long-Term Care, February 2012 pp. 2-6.
Title New and Improved VA Algorithms/New SPHM App!
Presenters name and credentials
Rogers, Matz, Martin
Description (1 paragraph) The VA and other healthcare organizations developed, tested, and released "Safe Patient Handling Assessment, Algorithms, and Care Plan" in 2001. They were the first assessment strictly for use in determining the most appropriate patient handling equipment, technique, and number of caregivers needed. The revised algorithms incorporate lessons learned over the years. In addition to being an important tool for technology selection, they are a great educational tool. They are included in the new VA SPHM App which will be unveiled during this presentation!
1/26/2016 1:27 PM | 3
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Determine appropriate patient handling equipment for each unique patient using the VA Assessment/Algorithms. (2) Replay contents of the VA SPHM App.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Determine appropriate equipment (ceiling lift, floor lift, etc). 2. App. A. Contents of the App, b. How to use the app: Pictures and video clips of a variety of patient handling and mobility technologies, Comprehensive patient assessments and algorithms, scoring and algorithms for specific patient handling tasks, Information about the Assoc. of Orthopaedic Nurses and the Assoc. of periOperative Registered Nurses, SPHM resources.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Interactive presentation/PowerPoint/Internet Link
References (3-5 evidence-based publications)
1. OSHA. (2003). Ergonomic guidelines for nursing homes. Washington: US Department of Labor. 2. Nelson, A. L., Matz, M., Chen, F., Siddharthan, K., Lloyd, J., & Fragala, G. (2006). Development and evaluation of a multifaceted ergonomics program to prevent injuries associated with patient handling tasks. International Journal of Nursing Studies, 43(6), 717-733. 3. VISN 8 Patient Safety Center of Inquiry. (2006). Patient Care Ergonomics Resource Guide: Safe Patient Handling and Movement. Tampa, FL: Department of Veterans Affairs VISN 8 Patient Safety Center of Inquiry.
Title Prevention of Pressure Ulcers by Optimizing Transfer and Repositioning Techniques
Presenters name and credentials
Hanneke Knibbe
Description (1 paragraph) This session will provide reliable and practical insights in the risks of certain repositioning techniques for the patient (pressure ulcer risks) and the occupational health risks for the nurses. These practical principles that apply to any transfer or repositioning technique with or without equipment and aids will enable him/her to reduce the risk of developing or increasing pressure ulcers without compromising the nurse's health (back, neck and shoulder).
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Identify repositioning technique risks; 2. Explain the occupational health risks for caregivers. 3. Apply these techniques in their own facility to increase patient and caregiver safety.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1a. Increased or new pressure ulcers that can go unnoticed with a sling in place. 1b. How to examine the patient once in the sling to assure that the material is smooth and not bunched or torn. 1c. Know when and what types of slings can be left on the patient and in what circumstances. 2a. Back injuries, 2b. Muscular injuries due to turning in limited space environments. 3a. Knowing statistics on caregiver injuries to justify program development and sustenance. 3b Knowing statistics on patient outcomes in environments where equipment is or is not used.
1/26/2016 1:27 PM | 4
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation PowerPoint presentation plus discussion question and answer.
References (3-5 evidence-based publications)
1. Knibbe, JJ et al. Flying through the hospital: efficiency and safety of an ergonomic solution. Work. 2012; 41: 5642-3. 2. Koppelaar E., J.J. Knibbe, H.S. Miedema, A. Burdorf, The influence of individual and organisational factors on nurses’ behaviour to use lifting devices in healthcare, Applied Ergonomics 44, (2013) 532-537. 3. Knibbe JJ, Friele RD. (1996) Prevalence of back pain and characteristics of the physical workload of community nurses. Ergonomics; 39: 186–98. 4. Knibbe JJ, Friele RD. (1999) The use of logs to assess exposure to manual handling of patients, illustrated in an intervention study in home care nursing. Int J Ind Ergon; 24: 445–54. 5. Knibbe HJ, Knibbe NE, Klaassen AJ. (2007) Safe patient handling program in critical care using peer leaders: lessons learned in the Netherlands. Crit Care Nurs Clin North Am; 19: 205–11. 6. Koppelaar E, Knibbe JJ, Miedema HS et al. (2009) Determinants of implementation of primary preventive interventions on patient handling in healthcare: a systematic review. Occup Environ Med; 66: 353–60. 7. Koppelaar E, Knibbe JJ, Miedema HS et al. (2011) Individual and organisational determinants of use of ergonomic devices in healthcare. Occup Environ Med; 68: 659–65. 8. Koppelaar, E, HJJ Knibbe, HS Miedema, A,Burdorf, The Influence of Ergonomic Devices on Mechanical Load during Patient Handling Activities in Nursing Homes, Ann. Occup. Hyg., Vol. 56, No. 6, pp. 708–718, 2012. 9. Knibbe, JJ, NE Knibbe, CC Heitink, Fifth National Monitoring of the Implementation of the Dutch Ergonomic Guidelines for Practice in Health Care, IEA 2015,Melbourne. 10. Hignett, S., Fray M., Battevi, N., Occhipinti, E., Menoni, O., Tamminen-Peter, L., Waaijer, E., Knibbe, H.J.J., Jäger, M. (2014). “International consensus on manual handling of people in the healthcare sector: Technical report ISO/TR 12296”; 44(1):191–195. 11. Knibbe, H.J.J. (2013). “Decubitusrisico’s en transfers: dat kan en dat moet beter” (in Dutch), Gezond en Zeker Magazine, RegioPlus. pp. 12-15. 12. Knibbe, H.J.J. (2014). “Glijzeilen, wel of niet” (in Dutch), Gezond en Zeker Magazine, Regioplus, in press. 13. Knibbe, H.J.J., Panhuys, W. van, Vught, W. van (2008). “Handboek Transfers”, (published in Dutch, English and German), Corpus, Tiel. 14. Oomens, C.W., Zenhorst, W., Broek, M., Hemmes, B., Poeze, M., Brink, P.R., Bader, D.L., (2013). “A numerical study to analyse the risk for pressure ulcer development on a spine board”, Clin Biomech, 28(7):pp 736-42
Title Safe Patient Handling Common Cause Analysis Reveals Compliance Barriers and Solutions to Overcoming the Obstacles: Lessons Learned from Taking a Deep Dive Into Practice and Barriers with Special Patient Populations and Why the Same Problems Recur
Presenters name and credentials
Nancy McGann PT, CSPHP, Ergonomic Injury Prevention Coordinator, SCL Health
Description (1 paragraph) Compliance with the use of safe patient handling technologies is an ongoing problem in many healthcare institutions. We already understand many barriers such as equipment availability, perceived time constraints, and lack of knowledge of personal and patient risk factors. However, even when those barriers have been overcome, we still see compliance issues that affect caregiver and patient safety. A common cause analysis was performed to take a deep dive into practice to determine less understood obstacles that effect clinical practice.
1/26/2016 1:27 PM | 5
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
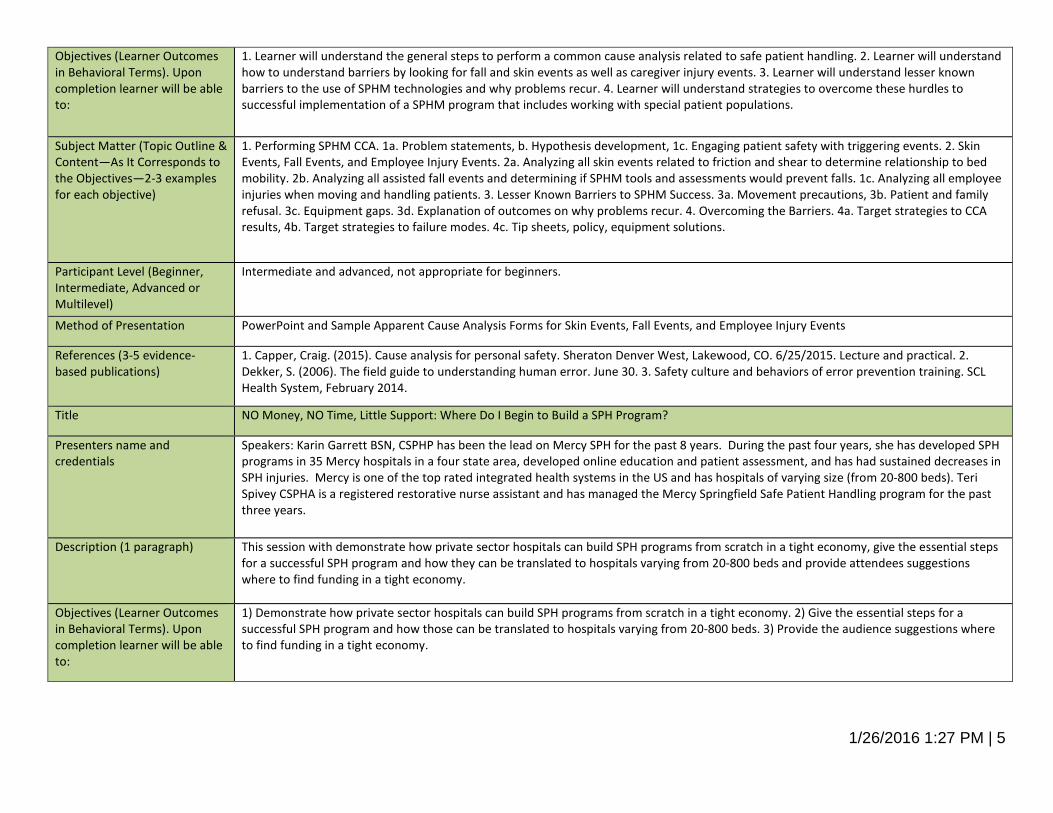
1. Learner will understand the general steps to perform a common cause analysis related to safe patient handling. 2. Learner will understand how to understand barriers by looking for fall and skin events as well as caregiver injury events. 3. Learner will understand lesser known barriers to the use of SPHM technologies and why problems recur. 4. Learner will understand strategies to overcome these hurdles to successful implementation of a SPHM program that includes working with special patient populations.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Performing SPHM CCA. 1a. Problem statements, b. Hypothesis development, 1c. Engaging patient safety with triggering events. 2. Skin Events, Fall Events, and Employee Injury Events. 2a. Analyzing all skin events related to friction and shear to determine relationship to bed mobility. 2b. Analyzing all assisted fall events and determining if SPHM tools and assessments would prevent falls. 1c. Analyzing all employee injuries when moving and handling patients. 3. Lesser Known Barriers to SPHM Success. 3a. Movement precautions, 3b. Patient and family refusal. 3c. Equipment gaps. 3d. Explanation of outcomes on why problems recur. 4. Overcoming the Barriers. 4a. Target strategies to CCA results, 4b. Target strategies to failure modes. 4c. Tip sheets, policy, equipment solutions.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Intermediate and advanced, not appropriate for beginners.
Method of Presentation PowerPoint and Sample Apparent Cause Analysis Forms for Skin Events, Fall Events, and Employee Injury Events
References (3-5 evidence-based publications)
1. Capper, Craig. (2015). Cause analysis for personal safety. Sheraton Denver West, Lakewood, CO. 6/25/2015. Lecture and practical. 2. Dekker, S. (2006). The field guide to understanding human error. June 30. 3. Safety culture and behaviors of error prevention training. SCL Health System, February 2014.
Title NO Money, NO Time, Little Support: Where Do I Begin to Build a SPH Program?
Presenters name and credentials
Speakers: Karin Garrett BSN, CSPHP has been the lead on Mercy SPH for the past 8 years. During the past four years, she has developed SPH programs in 35 Mercy hospitals in a four state area, developed online education and patient assessment, and has had sustained decreases in SPH injuries. Mercy is one of the top rated integrated health systems in the US and has hospitals of varying size (from 20-800 beds). Teri Spivey CSPHA is a registered restorative nurse assistant and has managed the Mercy Springfield Safe Patient Handling program for the past three years.
Description (1 paragraph) This session with demonstrate how private sector hospitals can build SPH programs from scratch in a tight economy, give the essential steps for a successful SPH program and how they can be translated to hospitals varying from 20-800 beds and provide attendees suggestions where to find funding in a tight economy.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1) Demonstrate how private sector hospitals can build SPH programs from scratch in a tight economy. 2) Give the essential steps for a successful SPH program and how those can be translated to hospitals varying from 20-800 beds. 3) Provide the audience suggestions where to find funding in a tight economy.
1/26/2016 1:27 PM | 6
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
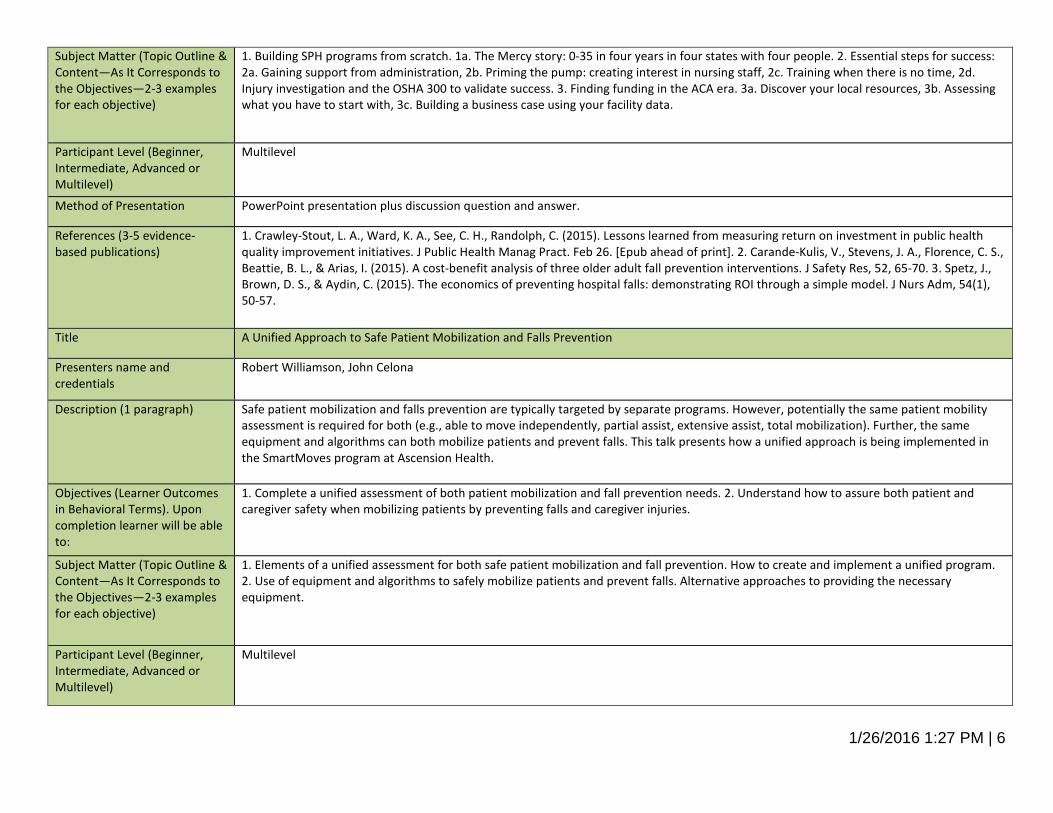
1. Building SPH programs from scratch. 1a. The Mercy story: 0-35 in four years in four states with four people. 2. Essential steps for success: 2a. Gaining support from administration, 2b. Priming the pump: creating interest in nursing staff, 2c. Training when there is no time, 2d. Injury investigation and the OSHA 300 to validate success. 3. Finding funding in the ACA era. 3a. Discover your local resources, 3b. Assessing what you have to start with, 3c. Building a business case using your facility data.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation PowerPoint presentation plus discussion question and answer.
References (3-5 evidence-based publications)
1. Crawley-Stout, L. A., Ward, K. A., See, C. H., Randolph, C. (2015). Lessons learned from measuring return on investment in public health quality improvement initiatives. J Public Health Manag Pract. Feb 26. [Epub ahead of print]. 2. Carande-Kulis, V., Stevens, J. A., Florence, C. S., Beattie, B. L., & Arias, I. (2015). A cost-benefit analysis of three older adult fall prevention interventions. J Safety Res, 52, 65-70. 3. Spetz, J., Brown, D. S., & Aydin, C. (2015). The economics of preventing hospital falls: demonstrating ROI through a simple model. J Nurs Adm, 54(1), 50-57.
Title A Unified Approach to Safe Patient Mobilization and Falls Prevention
Presenters name and credentials
Robert Williamson, John Celona
Description (1 paragraph) Safe patient mobilization and falls prevention are typically targeted by separate programs. However, potentially the same patient mobility assessment is required for both (e.g., able to move independently, partial assist, extensive assist, total mobilization). Further, the same equipment and algorithms can both mobilize patients and prevent falls. This talk presents how a unified approach is being implemented in the SmartMoves program at Ascension Health.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Complete a unified assessment of both patient mobilization and fall prevention needs. 2. Understand how to assure both patient and caregiver safety when mobilizing patients by preventing falls and caregiver injuries.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Elements of a unified assessment for both safe patient mobilization and fall prevention. How to create and implement a unified program. 2. Use of equipment and algorithms to safely mobilize patients and prevent falls. Alternative approaches to providing the necessary equipment.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
1/26/2016 1:27 PM | 7
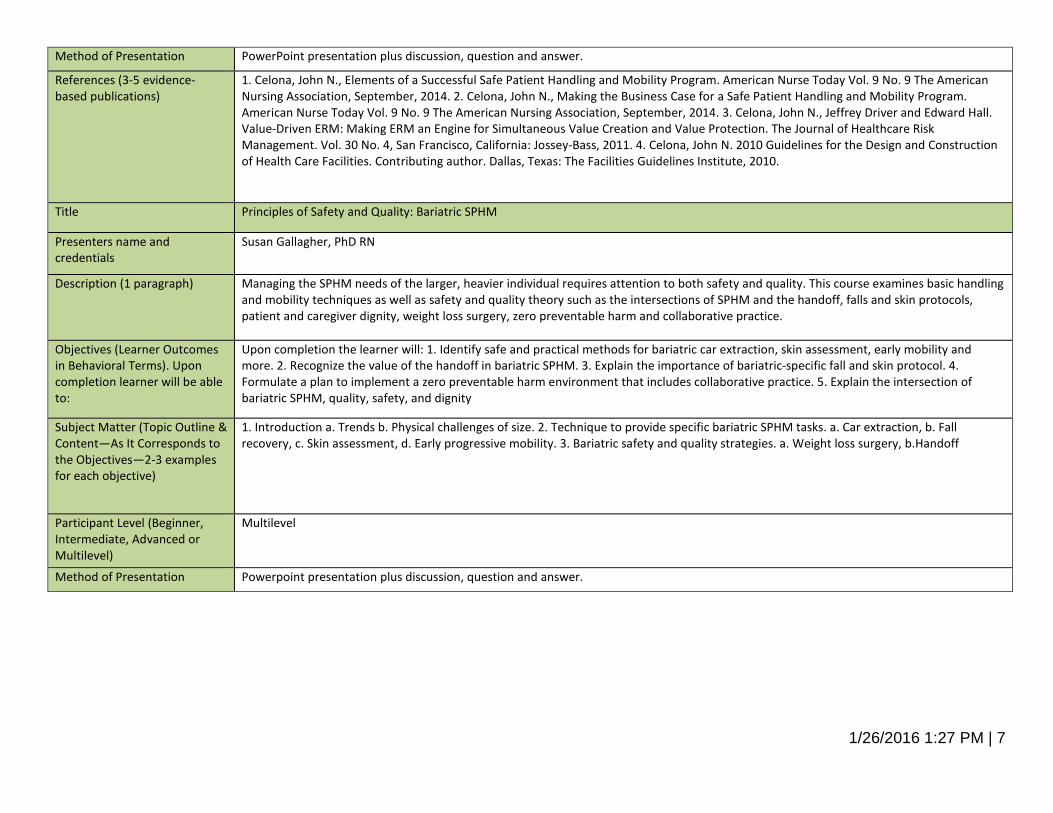
Method of Presentation PowerPoint presentation plus discussion, question and answer.
References (3-5 evidence-based publications)
1. Celona, John N., Elements of a Successful Safe Patient Handling and Mobility Program. American Nurse Today Vol. 9 No. 9 The American Nursing Association, September, 2014. 2. Celona, John N., Making the Business Case for a Safe Patient Handling and Mobility Program. American Nurse Today Vol. 9 No. 9 The American Nursing Association, September, 2014. 3. Celona, John N., Jeffrey Driver and Edward Hall. Value-Driven ERM: Making ERM an Engine for Simultaneous Value Creation and Value Protection. The Journal of Healthcare Risk Management. Vol. 30 No. 4, San Francisco, California: Jossey-Bass, 2011. 4. Celona, John N. 2010 Guidelines for the Design and Construction of Health Care Facilities. Contributing author. Dallas, Texas: The Facilities Guidelines Institute, 2010.
Title Principles of Safety and Quality: Bariatric SPHM
Presenters name and credentials
Susan Gallagher, PhD RN
Description (1 paragraph) Managing the SPHM needs of the larger, heavier individual requires attention to both safety and quality. This course examines basic handling and mobility techniques as well as safety and quality theory such as the intersections of SPHM and the handoff, falls and skin protocols, patient and caregiver dignity, weight loss surgery, zero preventable harm and collaborative practice.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
Upon completion the learner will: 1. Identify safe and practical methods for bariatric car extraction, skin assessment, early mobility and more. 2. Recognize the value of the handoff in bariatric SPHM. 3. Explain the importance of bariatric-specific fall and skin protocol. 4. Formulate a plan to implement a zero preventable harm environment that includes collaborative practice. 5. Explain the intersection of bariatric SPHM, quality, safety, and dignity
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Introduction a. Trends b. Physical challenges of size. 2. Technique to provide specific bariatric SPHM tasks. a. Car extraction, b. Fall recovery, c. Skin assessment, d. Early progressive mobility. 3. Bariatric safety and quality strategies. a. Weight loss surgery, b.Handoff
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Powerpoint presentation plus discussion, question and answer.
1/26/2016 1:27 PM | 8
References (3-5 evidence-based publications)
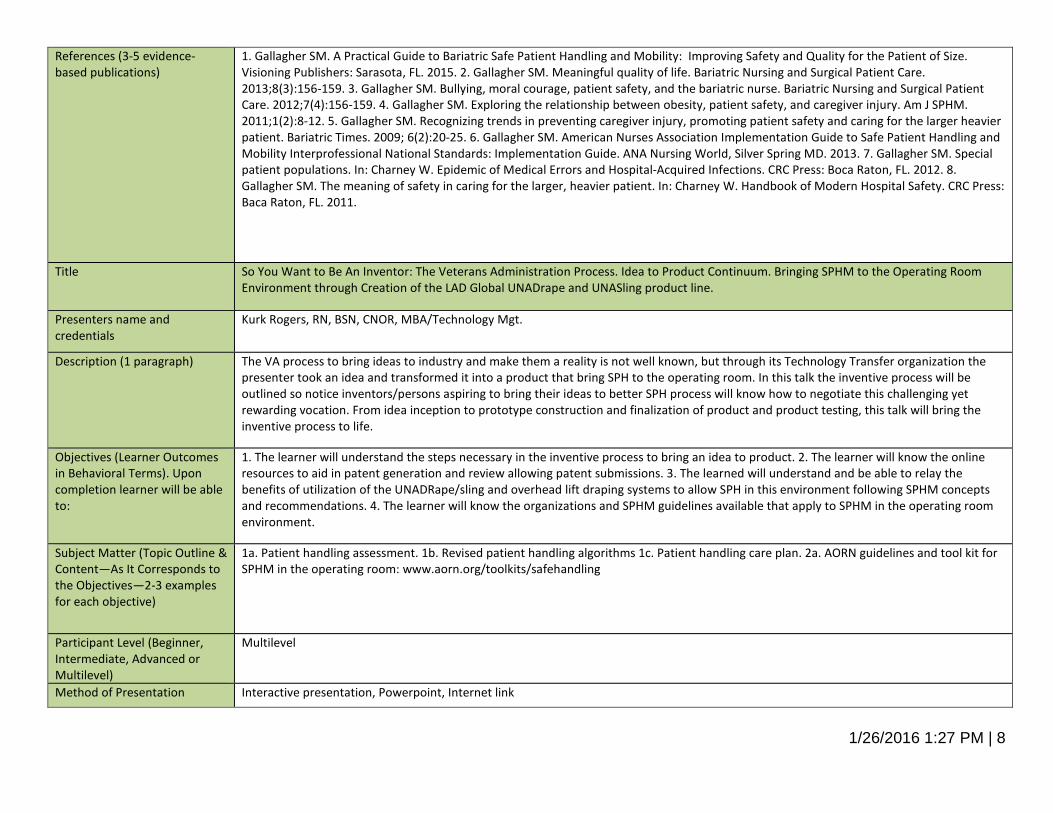
1. Gallagher SM. A Practical Guide to Bariatric Safe Patient Handling and Mobility: Improving Safety and Quality for the Patient of Size. Visioning Publishers: Sarasota, FL. 2015. 2. Gallagher SM. Meaningful quality of life. Bariatric Nursing and Surgical Patient Care. 2013;8(3):156-159. 3. Gallagher SM. Bullying, moral courage, patient safety, and the bariatric nurse. Bariatric Nursing and Surgical Patient Care. 2012;7(4):156-159. 4. Gallagher SM. Exploring the relationship between obesity, patient safety, and caregiver injury. Am J SPHM. 2011;1(2):8-12. 5. Gallagher SM. Recognizing trends in preventing caregiver injury, promoting patient safety and caring for the larger heavier patient. Bariatric Times. 2009; 6(2):20-25. 6. Gallagher SM. American Nurses Association Implementation Guide to Safe Patient Handling and Mobility Interprofessional National Standards: Implementation Guide. ANA Nursing World, Silver Spring MD. 2013. 7. Gallagher SM. Special patient populations. In: Charney W. Epidemic of Medical Errors and Hospital-Acquired Infections. CRC Press: Boca Raton, FL. 2012. 8. Gallagher SM. The meaning of safety in caring for the larger, heavier patient. In: Charney W. Handbook of Modern Hospital Safety. CRC Press: Baca Raton, FL. 2011.
Title So You Want to Be An Inventor: The Veterans Administration Process. Idea to Product Continuum. Bringing SPHM to the Operating Room Environment through Creation of the LAD Global UNADrape and UNASling product line.
Presenters name and credentials
Kurk Rogers, RN, BSN, CNOR, MBA/Technology Mgt.
Description (1 paragraph) The VA process to bring ideas to industry and make them a reality is not well known, but through its Technology Transfer organization the presenter took an idea and transformed it into a product that bring SPH to the operating room. In this talk the inventive process will be outlined so notice inventors/persons aspiring to bring their ideas to better SPH process will know how to negotiate this challenging yet rewarding vocation. From idea inception to prototype construction and finalization of product and product testing, this talk will bring the inventive process to life.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. The learner will understand the steps necessary in the inventive process to bring an idea to product. 2. The learner will know the online resources to aid in patent generation and review allowing patent submissions. 3. The learned will understand and be able to relay the benefits of utilization of the UNADRape/sling and overhead lift draping systems to allow SPH in this environment following SPHM concepts and recommendations. 4. The learner will know the organizations and SPHM guidelines available that apply to SPHM in the operating room environment.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1a. Patient handling assessment. 1b. Revised patient handling algorithms 1c. Patient handling care plan. 2a. AORN guidelines and tool kit for SPHM in the operating room: www.aorn.org/toolkits/safehandling
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Interactive presentation, Powerpoint, Internet link
1/26/2016 1:27 PM | 9
References (3-5 evidence-based publications)
1. OSHA. (2003). Ergonomic guidelines for nursing homes. US Department of Labor. 2. Nelson, A. L., Matz, M., Chen, F., Siddharthan, K., Lloyd, J., & Fragala, G. (2006). Development and evaluation of a multifaceted ergonomics program to prevent injuries associated with patient handling tasks. International Journal of Nursing Studies, 43(6), 717-733. 3. Patient Care Ergonomics Resource Guide: Safe Patient Handling and Movement. (2006). VISN 8 Patient Safety Center of Inquiry, Tampa, FL. 4. AORN. www.aorn.org/toolkits/safehandling
Title What You Don’t Know CAN Hurt You!: Using Both LEADING and Lagging Indicators to Guide your Safe Patient Handling and Mobility Program
Presenters name and credentials
Nancy McGann PT, CSPHP, Ergonomic Injury Prevention Coordinator, SCL Health
Description (1 paragraph) Using a matrix with both leading and lagging indicators will allow you to best determine needs and locations for patient handling technologies. Metrics will allow you to more successfully get investment from executives and buy-in from clinical leaders. Learn how using a variety of metrics in a grid that will guide you to make the best decisions for the future.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Upon completion, learner will understand the difference between leading and lagging indicators related to patient and employee safety. 2. Upon completion, learner will understand how to rank various metrics to create a priority matrix that allows a quantifiable basis to discuss investments and training with stakeholders. 3. Upon completion, learner will understand the benefits to quantifying near miss events, injury events, rounding outcomes, caregiver feedback and severity to guide equipment investment. 4. Upon completion, learner will understand how indicators can lead to more meaningful educational initiatives.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Leading and Lagging Indicators. a. Definition and Samples of Leading Indicators related to both caregiver and patient safety. b. Definition and Samples of Lagging Indicators. 2. Priority Matrix. a. How to use your organizations strategic plan and priorities to breakdown metrics into categories that have meaning, b. Examples of metric priority change: Falls, Pressure Ulcers, Employee Injury Costs, Lost Time and Turnover may all have varying priorities in your organization. Create matrix based on current focus and initiative. 3. Benefits of various types of event reports. a. Near Miss reports guide risk better than injury reports – learn the difference between being lucky or good? b. Executive rounding, safety rounds, casual communication or employee questionnaires will uncover hazards that may not be found in OSHA logs and need to be used to determine genuine risk. c. Equipment investment is easier to justify when risk is assessed at a deeper level and can be quantified through a matrix or spreadsheet. 4. Training and Culture Work Needs. a. Equipment is only as good as the culture and training of your organization, b. Analyzing gaps through leading and lagging indicators help to understand gaps in culture and training that enhance equipment outcomes.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Powerpoint and Handouts with actual sample grids/matrix
1/26/2016 1:27 PM | 10
References (3-5 evidence-based publications)
1. Blair L. Sadler, Leonard L. Berry, Robin Guenther, D. Kirk Hamilton, Frederick A. Hessler, Clayton Merritt, and Derek Parker, "Fable Hospital 2.0: The Business Case for Building Better Health Care Facilities," Hastings Center Report 41, no. 1 (2011): 13-23. 2. Matz,M: Patient Handling (Lifting) Equipment :Coverage and Space Requirements. http://www.publichealth.va.gov. 3. Collins, J., Nelson, A., and Sublet, V. (2006) Safe Lifting and Movement of Nursing Home Residents. DHHS (NIOSH) Publication Number 2006-117. 4. Safety Culture & Behaviors of Error Prevention Training: SCL Health System, February 2014. 5. Reason, James; “Managing the Risks of Organizational Accidents”-December 1, 1977. 6. Merrick, J.R.W., M. Grabowski, P. Ayyalasomayajula, J.R. Harrald. 2005. Understanding Organizational Safety Using Value Focused Thinking. Risk.
Title Fall Risk Screening Tools: Compare and Contrast--What Works? What's Missing?
Presenters name and credentials
Dee Kumpar, MBA, BSN, RN, CSPHP; Teresa Boynton, MS, OTR, CSPH
Description (1 paragraph) There are many fall risk screening tools currently being used, including a number of validated tools as well as "home-grown" varieties. This presentation will compare and contrast fall risk screening tools and the fall precautions and interventions recommended based on results. We will also look at the differences between screening tools and fall risk assessments. We'll also consider which tools consider mobility and links to safe patient handling.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Describe fall risk screening tools and components of a fall risk assessment. 2. Understand the limitations of screening tools and why implementing an effective fall prevention program can be so daunting. 3. Describe actions that need to be taken to be most effective.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Compared and contrast fall risk screening tools. 2. Discuss patient-specific precautions and interventions aimed at decreasing the risk of patient falls and the risk of fall-related injuries.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Powepoint, lecture, Q&A
References (3-5 evidence-based publications)
1. American Nurses Association. (2013). Special Report: Best Practices for Falls Reduction--A Practical Guide. Silver Springs, MD: ANA. 2. Oliver, D., Healey, F., & Haines, T. (2010). Preventing fall and fall-related injuries in hospitals. J Clin Geriatr Med, 26, 645-692. doi: 10.1016/j.cger.2010/06/005. 3. Gray-Miceli, D. (2014). 5 Easy Steps to Prevent Falls--The Comprehensive Guide to Keeping Patients of All Ages Safe. Silver Springs, MD: American Nurses Association. 4. Cronin, H., Kenny, R. A. (2010). Cardiac causes for falls and their treatment. J Clin Griatr Med, 26, 529-567. doi: 10.1016/j.cger.2010.06.005.
Title Evaluation of a "Best Practices" SPHM Program in an Acute Care Hospital
1/26/2016 1:27 PM | 11
Presenters name and credentials
Jim Collins, PhD, MSME
Description (1 paragraph) Dr. Collins will discuss one of his latest research studies.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Steps in program development 2. Best practices in program sustainability 3. Evaluation of how methods are incorporated into practice.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1a. Assess program, 1b. Choose applicable best practices, 1c. Where to include sustainability. 2a. Teamwork, 2b. Communication strategies, 2c. Regular analysis/follow up.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Powepoint, lecture, Q&A
References (3-5 evidence-based publications)
1. Celona, John N., Elements of a Successful Safe Patient Handling and Mobility Program. American Nurse Today Vol. 9 No. 9 The American Nursing Association, September, 2014. 2. Celona, John N., Making the Business Case for a Safe Patient Handling and Mobility Program. American Nurse Today Vol. 9 No. 9 The American Nursing Association, September, 2014. 3. Collins, J., Nelson, A., and Sublet, V. (2006) Safe Lifting and Movement of Nursing Home Residents. DHHS (NIOSH) Publication Number 2006-117.
Title Critical Thinking and Simulation Sessions for Patients with Barriers to Movement and/or Mobility: Solutions to Overcome Spinal Precautions, Sternal Precautions, Hip Precautions, and Barriers Related to Patient Fear and Anxiety, Mobilizing Patients in the ICU, and Tip Sheet Creation for all precaution Concerns
Presenters name and credentials
Nancy McGann PT, CSPHP, Ergonomic Injury Prevention Coordinator, SCL Health ; Margaret Arnold, PT, CEES, CSPHP, Owener and consultant for Inspire Outcomes LLC
Description (1 paragraph) Caregivers often have concerns about how to use mechanical lift devices and slings for various precautions. Additional barriers exist in mobility in the ICU, and in certain patient scenarios across the care continuum. These can be common reasons for lack of compliance with the use of safe patient handling equipment and policies. This interactive session will share a simulation tool used to problem solve various barriers and precautions. Training on how to develop tip sheets for end user education will be provided.
1/26/2016 1:27 PM | 12
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Upon completion learner will be able to show how to use a lift sling with various precautions including spinal, sternal and hip. 2. Upon completion, learner will be able to implement simulation training to determine best practices with their equipment for complex mobility situations. 3. Upon completion, learner will be able to create tip sheets for end user training. 4. Upon completion, learner will have tools to work with caregivers who are not using mechanical devices due to fear of movement precautions and other complex situations.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1. Precaution Concerns. a. Patient positioning in slings, b. Using pillows, towels, blankets, wedges to provide ideal positioning as needed. c. Spotters for safety during movement process. 2. Simulation Training. a. Obtaining expertise of end users, clinical educators, leaders and safe patient handling team members to create best practice, b. Trial various sling types, sizes, hanger bars and tools to create best positioning for complex patient populations. c. Vendor input for the simulation process. 3. Tip Sheet Creation. a. Sample Tip Sheets from SCL organization, b. How to adapt tip sheets specific to the tools in your organization, c. Examples of end user education with tip sheets. 4. End User Barriers. a. Real barriers to use of slings for many end users are pain, combative behaviors and movement precautions, b. Creating tip sheets to educate and overcome barriers will improve both patient and caregiver safety.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Intermediate and Advanced Level primarily but would not be inappropriate for beginners.
Method of Presentation PowerPoint with concrete examples and tip sheets
References (3-5 evidence-based publications)
1. Durable Medical Equipment (DME) Coverage. http://www.medicare.gov/coverage/durable-medical-equipment-coverage.html. 2. Matz M. Patient Handling (Lifting) Equipment Coverage & Space Recommendations. 2007 http://www.visn8.va.gov/patientsafetycenter/safepthandling/coveragespacerecs.doc. 3. Campo M., Shiyko M. P., Margulis H., & Darragh A. R. (2013). Effect of a safe patient handling programs on rehabilitation outcomes. Archives of Physical Medicine and Rehabilitation, 94, 17-22. 4. Darragh A.R., Campo M. A., Frost L., Miller M., Pentico M., & Margulis H. (2013). Safe-patient-handling equipment in therapy practice: Implications for Rehabilitation. American Journal of Occupational Therapy, 67, 45-53. 5. Arnold, M., Combs, J., Gach, R., & Lecreche, M. (2015). Overcoming barriers to mobilizing bariatric patients: three case studies. Am J SPHM, 5(2), 47-54.
Title Tools to Ensure Safety in Design and Construction of Healthcare Facilities
Presenters name and credentials
Mary Matz
Description (1 paragraph) This presentation will relay a tool for use in incorporating design criteria in the design of healthcare facilities or in renovations. The "Safety Risk Assessment" (SRA). The tool includes six areas of risk: patient falls, patient handling, medication errors, security, behavioral health, and infection control. The presentation will focus on how to use the ARA tool to reduce patient fall risk and risk from patient handling, movement, and mobility.
1/26/2016 1:27 PM | 13
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Relay how the SRA can be used as a tool ot measure safety risk before and after design development/construction. 2. List 3 questions for designers to consider when developing design specification to reduce risk of patient falls. 3. List 3 questions for designers to consider when developing design specification to reduce risk from patient handling, movement, and mobility.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1a. The Safe Design Roadmap, 1b. Use of the Safe Design Roadmap to measure improvements in safety in an organization. 2a. Navigating the SRA to locate information related to patient falls. 2b. Reducing risk for patient falls using the SRA. 3a. Navigating the SRA to locate information related to mobility. 3b. Reducing the risk from patient handling, movement, and mobility using the SRA.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Online demonstration and PowerPoint
References (3-5 evidence-based publications)
1. Facilities Guidance Institute. (2014). Guidelines for Design and Construction of Hospitals and Outpatient Facilities. American Society for Healthcare Engineering. Http://www.fgiguidelines.org. 2. Barker, A., Kamar, J., Morton, A., & Berkowitz, D. (2009). Bridging the gap between research and practice: review of a targeted hospital inpatient fall prevention programme. Quality and Safety in Health Care, 18(6), 467-472. 3. Alamgir, H., Li, O. W., Gorman, E., Fast, C., & Kidd, C. (2009). Evaluation of ceiling lifts: transfer time, patient comfort and staff perceptions. Injury, 40(9), 987-992.
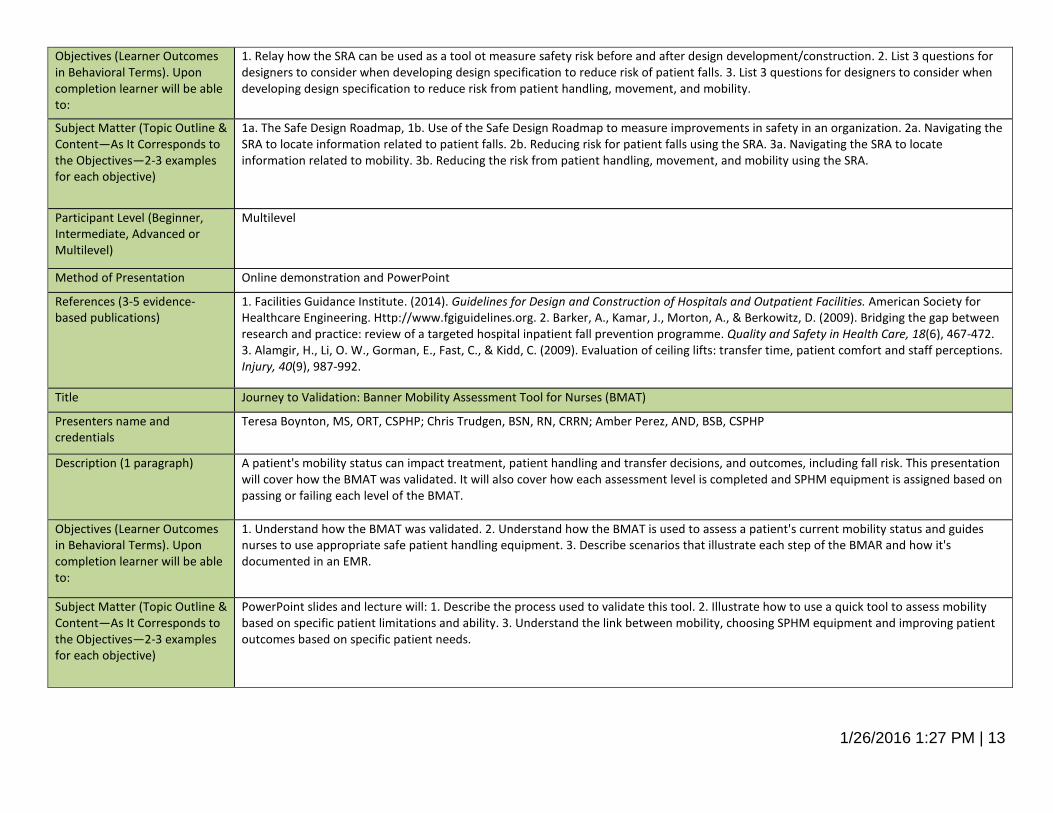
Title Journey to Validation: Banner Mobility Assessment Tool for Nurses (BMAT)
Presenters name and credentials
Teresa Boynton, MS, ORT, CSPHP; Chris Trudgen, BSN, RN, CRRN; Amber Perez, AND, BSB, CSPHP
Description (1 paragraph) A patient's mobility status can impact treatment, patient handling and transfer decisions, and outcomes, including fall risk. This presentation will cover how the BMAT was validated. It will also cover how each assessment level is completed and SPHM equipment is assigned based on passing or failing each level of the BMAT.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1. Understand how the BMAT was validated. 2. Understand how the BMAT is used to assess a patient's current mobility status and guides nurses to use appropriate safe patient handling equipment. 3. Describe scenarios that illustrate each step of the BMAR and how it's documented in an EMR.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
PowerPoint slides and lecture will: 1. Describe the process used to validate this tool. 2. Illustrate how to use a quick tool to assess mobility based on specific patient limitations and ability. 3. Understand the link between mobility, choosing SPHM equipment and improving patient outcomes based on specific patient needs.
1/26/2016 1:27 PM | 14
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation PowerPoint and Lecture
References (3-5 evidence-based publications)
1. Nelson, A. L. (2006). Safe Patient Handling and Movement: A Guide for Nurses and Other Health Care Providers. New York: Springer Publishing Co., Inc. 2. Nelson, A., Harwood, K. J., Tracey, C. A., & Dunn, K. L. (2008). Myths and facts about safe patient handling in rehabilitation. Rehabil Nurse, 33(1), 10-17. 3. Boynton, T., Kelly, L., Perez, A., Miller, M., An, Y., & Trudgen, C. (2014). Banner mobility assessment tool for nurses: instrument validation. Am J SPHM, 4(3), 86-92.
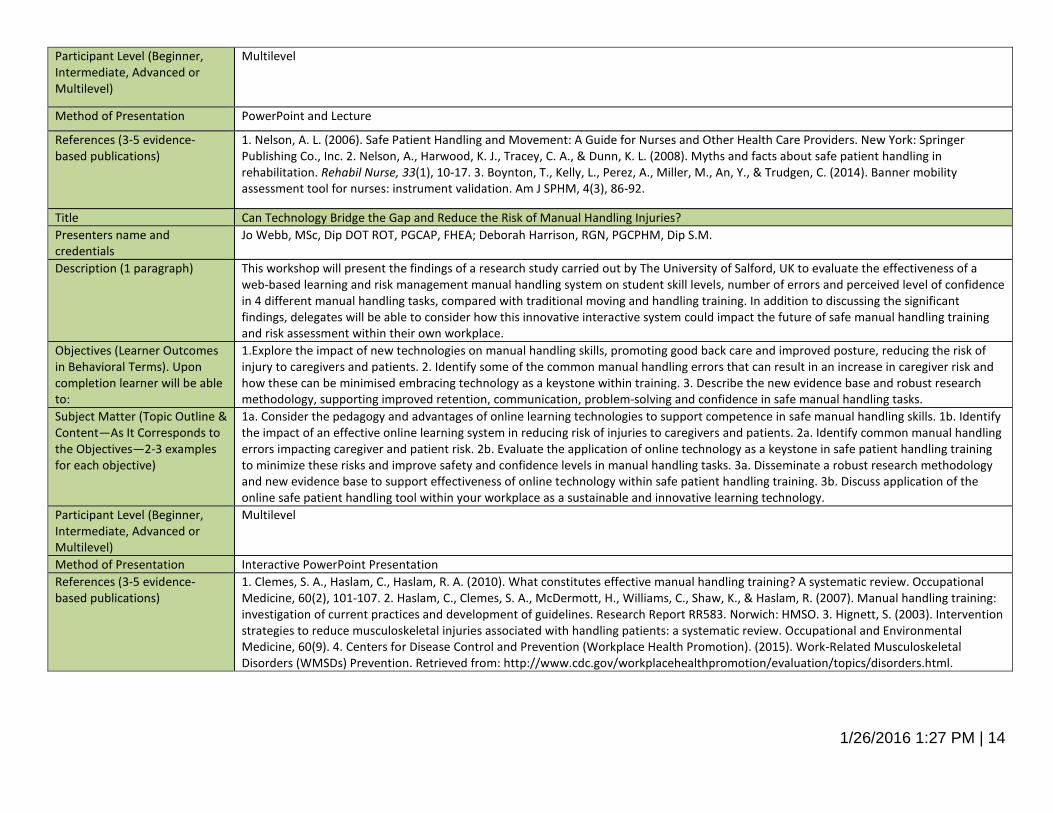
Title Can Technology Bridge the Gap and Reduce the Risk of Manual Handling Injuries? Presenters name and credentials
Jo Webb, MSc, Dip DOT ROT, PGCAP, FHEA; Deborah Harrison, RGN, PGCPHM, Dip S.M.
Description (1 paragraph) This workshop will present the findings of a research study carried out by The University of Salford, UK to evaluate the effectiveness of a web-based learning and risk management manual handling system on student skill levels, number of errors and perceived level of confidence in 4 different manual handling tasks, compared with traditional moving and handling training. In addition to discussing the significant findings, delegates will be able to consider how this innovative interactive system could impact the future of safe manual handling training and risk assessment within their own workplace.
Objectives (Learner Outcomes in Behavioral Terms). Upon completion learner will be able to:
1.Explore the impact of new technologies on manual handling skills, promoting good back care and improved posture, reducing the risk of injury to caregivers and patients. 2. Identify some of the common manual handling errors that can result in an increase in caregiver risk and how these can be minimised embracing technology as a keystone within training. 3. Describe the new evidence base and robust research methodology, supporting improved retention, communication, problem-solving and confidence in safe manual handling tasks.
Subject Matter (Topic Outline & Content—As It Corresponds to the Objectives—2-3 examples for each objective)
1a. Consider the pedagogy and advantages of online learning technologies to support competence in safe manual handling skills. 1b. Identify the impact of an effective online learning system in reducing risk of injuries to caregivers and patients. 2a. Identify common manual handling errors impacting caregiver and patient risk. 2b. Evaluate the application of online technology as a keystone in safe patient handling training to minimize these risks and improve safety and confidence levels in manual handling tasks. 3a. Disseminate a robust research methodology and new evidence base to support effectiveness of online technology within safe patient handling training. 3b. Discuss application of the online safe patient handling tool within your workplace as a sustainable and innovative learning technology.
Participant Level (Beginner, Intermediate, Advanced or Multilevel)
Multilevel
Method of Presentation Interactive PowerPoint Presentation References (3-5 evidence-based publications)
1. Clemes, S. A., Haslam, C., Haslam, R. A. (2010). What constitutes effective manual handling training? A systematic review. Occupational Medicine, 60(2), 101-107. 2. Haslam, C., Clemes, S. A., McDermott, H., Williams, C., Shaw, K., & Haslam, R. (2007). Manual handling training: investigation of current practices and development of guidelines. Research Report RR583. Norwich: HMSO. 3. Hignett, S. (2003). Intervention strategies to reduce musculoskeletal injuries associated with handling patients: a systematic review. Occupational and Environmental Medicine, 60(9). 4. Centers for Disease Control and Prevention (Workplace Health Promotion). (2015). Work-Related Musculoskeletal Disorders (WMSDs) Prevention. Retrieved from: http://www.cdc.gov/workplacehealthpromotion/evaluation/topics/disorders.html.

1/26/2016 1:27 PM | 15
Educational Design (Day Three) Safe Patient Handling and Mobility Conference, Glendale Arizona, April 11-15, 2016
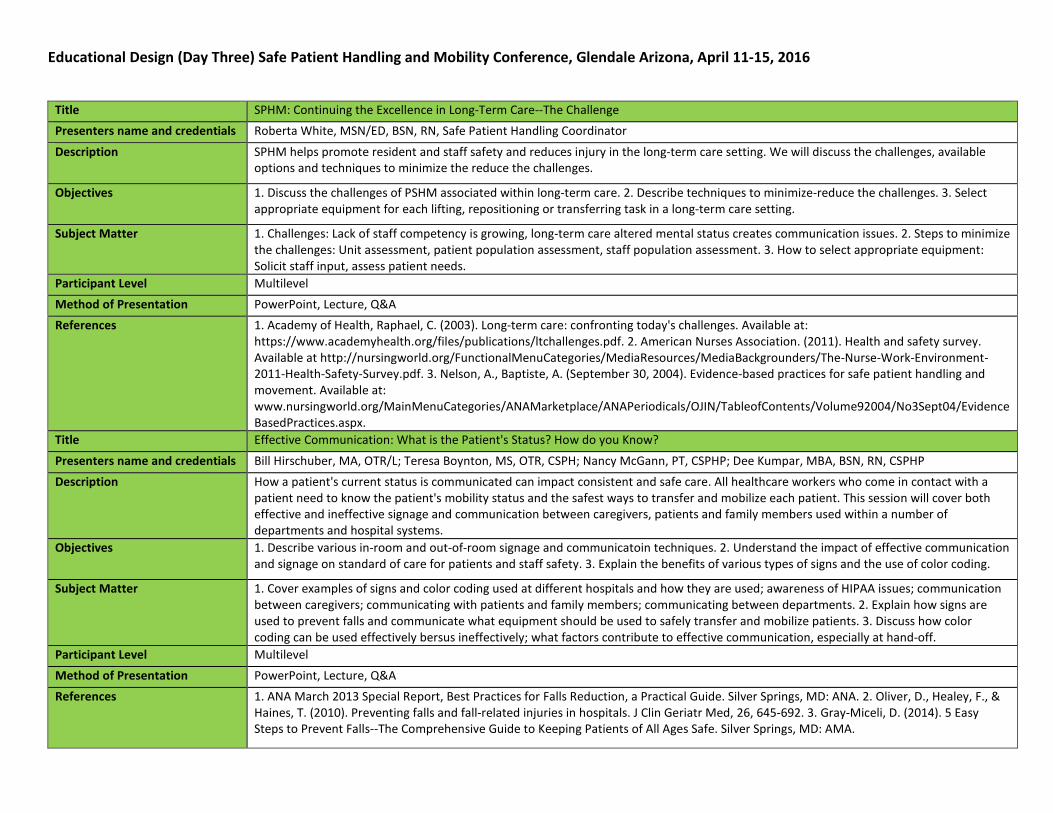
Title SPHM: Continuing the Excellence in Long-Term Care--The Challenge Presenters name and credentials Roberta White, MSN/ED, BSN, RN, Safe Patient Handling Coordinator
Description SPHM helps promote resident and staff safety and reduces injury in the long-term care setting. We will discuss the challenges, available options and techniques to minimize the reduce the challenges.
Objectives 1. Discuss the challenges of PSHM associated within long-term care. 2. Describe techniques to minimize-reduce the challenges. 3. Select appropriate equipment for each lifting, repositioning or transferring task in a long-term care setting.
Subject Matter 1. Challenges: Lack of staff competency is growing, long-term care altered mental status creates communication issues. 2. Steps to minimize the challenges: Unit assessment, patient population assessment, staff population assessment. 3. How to select appropriate equipment: Solicit staff input, assess patient needs.
Participant Level Multilevel Method of Presentation PowerPoint, Lecture, Q&A References 1. Academy of Health, Raphael, C. (2003). Long-term care: confronting today's challenges. Available at:
https://www.academyhealth.org/files/publications/ltchallenges.pdf. 2. American Nurses Association. (2011). Health and safety survey. Available at http://nursingworld.org/FunctionalMenuCategories/MediaResources/MediaBackgrounders/The-Nurse-Work-Environment-2011-Health-Safety-Survey.pdf. 3. Nelson, A., Baptiste, A. (September 30, 2004). Evidence-based practices for safe patient handling and movement. Available at: www.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/Volume92004/No3Sept04/EvidenceBasedPractices.aspx.
Title Effective Communication: What is the Patient's Status? How do you Know?
Presenters name and credentials Bill Hirschuber, MA, OTR/L; Teresa Boynton, MS, OTR, CSPH; Nancy McGann, PT, CSPHP; Dee Kumpar, MBA, BSN, RN, CSPHP Description How a patient's current status is communicated can impact consistent and safe care. All healthcare workers who come in contact with a
patient need to know the patient's mobility status and the safest ways to transfer and mobilize each patient. This session will cover both effective and ineffective signage and communication between caregivers, patients and family members used within a number of departments and hospital systems.
Objectives 1. Describe various in-room and out-of-room signage and communicatoin techniques. 2. Understand the impact of effective communication and signage on standard of care for patients and staff safety. 3. Explain the benefits of various types of signs and the use of color coding.
Subject Matter 1. Cover examples of signs and color coding used at different hospitals and how they are used; awareness of HIPAA issues; communication between caregivers; communicating with patients and family members; communicating between departments. 2. Explain how signs are used to prevent falls and communicate what equipment should be used to safely transfer and mobilize patients. 3. Discuss how color coding can be used effectively bersus ineffectively; what factors contribute to effective communication, especially at hand-off.
Participant Level Multilevel Method of Presentation PowerPoint, Lecture, Q&A References 1. ANA March 2013 Special Report, Best Practices for Falls Reduction, a Practical Guide. Silver Springs, MD: ANA. 2. Oliver, D., Healey, F., &
Haines, T. (2010). Preventing falls and fall-related injuries in hospitals. J Clin Geriatr Med, 26, 645-692. 3. Gray-Miceli, D. (2014). 5 Easy Steps to Prevent Falls--The Comprehensive Guide to Keeping Patients of All Ages Safe. Silver Springs, MD: AMA.
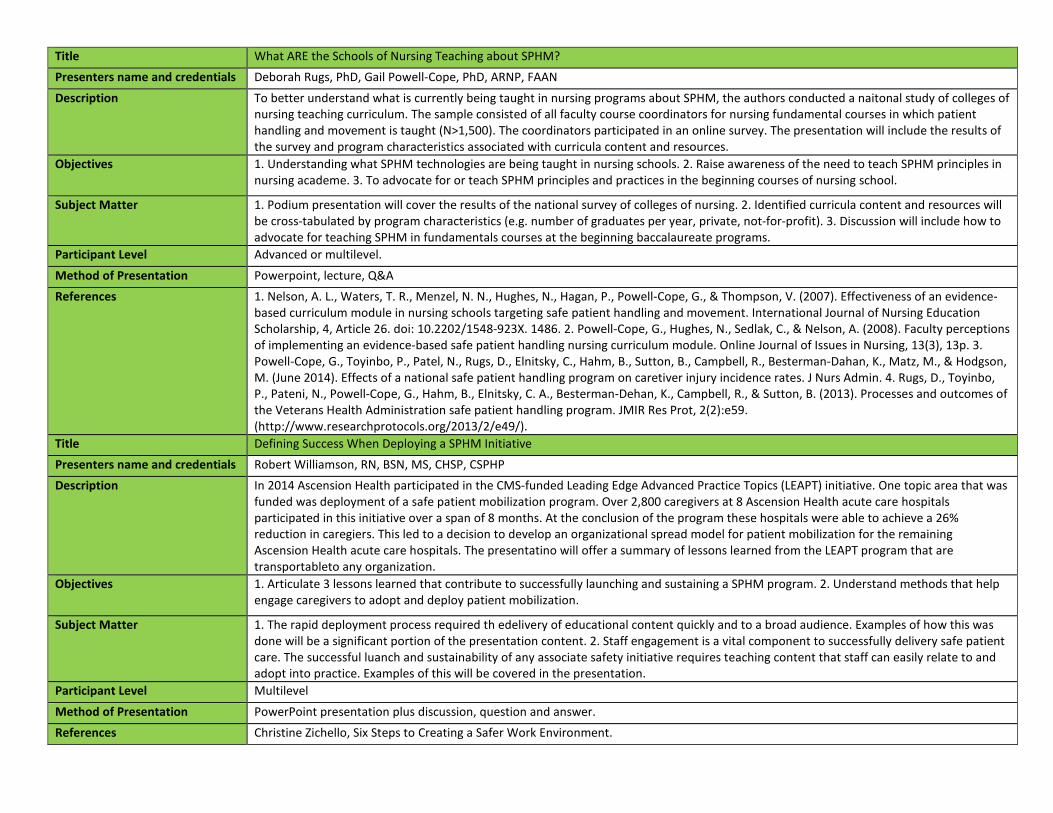
Title What ARE the Schools of Nursing Teaching about SPHM? Presenters name and credentials Deborah Rugs, PhD, Gail Powell-Cope, PhD, ARNP, FAAN
Description To better understand what is currently being taught in nursing programs about SPHM, the authors conducted a naitonal study of colleges of nursing teaching curriculum. The sample consisted of all faculty course coordinators for nursing fundamental courses in which patient handling and movement is taught (N>1,500). The coordinators participated in an online survey. The presentation will include the results of the survey and program characteristics associated with curricula content and resources.
Objectives 1. Understanding what SPHM technologies are being taught in nursing schools. 2. Raise awareness of the need to teach SPHM principles in nursing academe. 3. To advocate for or teach SPHM principles and practices in the beginning courses of nursing school.
Subject Matter 1. Podium presentation will cover the results of the national survey of colleges of nursing. 2. Identified curricula content and resources will be cross-tabulated by program characteristics (e.g. number of graduates per year, private, not-for-profit). 3. Discussion will include how to advocate for teaching SPHM in fundamentals courses at the beginning baccalaureate programs.
Participant Level Advanced or multilevel.
Method of Presentation Powerpoint, lecture, Q&A References 1. Nelson, A. L., Waters, T. R., Menzel, N. N., Hughes, N., Hagan, P., Powell-Cope, G., & Thompson, V. (2007). Effectiveness of an evidence-
based curriculum module in nursing schools targeting safe patient handling and movement. International Journal of Nursing Education Scholarship, 4, Article 26. doi: 10.2202/1548-923X. 1486. 2. Powell-Cope, G., Hughes, N., Sedlak, C., & Nelson, A. (2008). Faculty perceptions of implementing an evidence-based safe patient handling nursing curriculum module. Online Journal of Issues in Nursing, 13(3), 13p. 3. Powell-Cope, G., Toyinbo, P., Patel, N., Rugs, D., Elnitsky, C., Hahm, B., Sutton, B., Campbell, R., Besterman-Dahan, K., Matz, M., & Hodgson, M. (June 2014). Effects of a national safe patient handling program on caretiver injury incidence rates. J Nurs Admin. 4. Rugs, D., Toyinbo, P., Pateni, N., Powell-Cope, G., Hahm, B., Elnitsky, C. A., Besterman-Dehan, K., Campbell, R., & Sutton, B. (2013). Processes and outcomes of the Veterans Health Administration safe patient handling program. JMIR Res Prot, 2(2):e59. (http://www.researchprotocols.org/2013/2/e49/).
Title Defining Success When Deploying a SPHM Initiative Presenters name and credentials Robert Williamson, RN, BSN, MS, CHSP, CSPHP Description In 2014 Ascension Health participated in the CMS-funded Leading Edge Advanced Practice Topics (LEAPT) initiative. One topic area that was
funded was deployment of a safe patient mobilization program. Over 2,800 caregivers at 8 Ascension Health acute care hospitals participated in this initiative over a span of 8 months. At the conclusion of the program these hospitals were able to achieve a 26% reduction in caregiers. This led to a decision to develop an organizational spread model for patient mobilization for the remaining Ascension Health acute care hospitals. The presentatino will offer a summary of lessons learned from the LEAPT program that are transportableto any organization.
Objectives 1. Articulate 3 lessons learned that contribute to successfully launching and sustaining a SPHM program. 2. Understand methods that help engage caregivers to adopt and deploy patient mobilization.
Subject Matter 1. The rapid deployment process required th edelivery of educational content quickly and to a broad audience. Examples of how this was done will be a significant portion of the presentation content. 2. Staff engagement is a vital component to successfully delivery safe patient care. The successful luanch and sustainability of any associate safety initiative requires teaching content that staff can easily relate to and adopt into practice. Examples of this will be covered in the presentation.
Participant Level Multilevel
Method of Presentation PowerPoint presentation plus discussion, question and answer. References Christine Zichello, Six Steps to Creating a Safer Work Environment.
Title Safe Patient Handling and Falls Management for Ambulatory Care Presenters name and credentials Guy A Fragala, PhD, PE, CSP, CSPHP--Senior Advisor for Ergonomics, Patient Safety Center of Inquiry, Tampa, FL; Stephanie Hart-Hughes, PT,
MSMS, NCS, VISN 8 Patient Safety Center of Inquiry, James A Haley VA Hospital, Tampa, FL; Anthony W. Donaldson, CSPHP, Kaiser Permanente, NEH&S Senior Staff Manager, National Environmental, Health & Safety, 1800 Harrison Street, 6th Floor (Office #064R10),Oakland, CA 94612
Description When considering the risk exposure in healthcare related to safe patient handling, mobility issues and falls management we sometimes might overlook the ambulatory care environment and focus on in patient and homecare. Current trends in healthcare will drive expansion of ambulatory care and demands will increase while patients seen in ambulatory care clinics will have serious mobility issues and be at risk for experiencing falls. This session will consider the safe patient handling and fall risks present in ambulatory care settings and consider where action is required to mitigate risk. Practical solutions will be considered and discussed.
Objectives 1. Understand what safe patient handling and fall risks are present in the ambulatory care setting. 2. Discuss where action is required in attempts to reduce occupational risk to caregivers providing care in ambulatory care clinics. 3. Discuss possible solutions to consider when attempting to reduce both risk to caregivers and to patients in ambulatory care.
Subject Matter a. Determining dependency classifications for ambulatory care patients. b. Assessing safe patient handling requirements for different ambulatory care patients. c. Understanding of the population who might be at risk for falls when visiting ambulatory care clinics. d. What type of patient assessments might be required to determine safe patient handling and falls management needs for patient in ambulatory care. e. Available interventions to reduce risk in the ambulatory care setting. f. Directions for the future for developing new solutions to reduce risk.
Participant Level Multilevel Method of Presentation Lecture and Discussion References 1. Macdonald, C., (2010). Brief: Importance of Accessible Examination Tables and Weight Scales, Center for Disabilities Issues and the
Health Professions, Western University of the Health Sciences, Pomona CA, Edition 5. 2. T. Lagu et al., (2013). Access to Subspecialty Care for Patients With Mobility Impairment: A Survey, Ann Intern Med. 158(6):441-446. 3. Pharr, J. R. (2013). Accommodations for patients with disabilities in primary care: a mixed methods study of practice administrators. Global Journal of Health Science, 6(1), 23-32.
Title The Role of Safe Patient Handling in Reducing Pressure Ulcers
Presenters name and credentials Kermit Davis, PhD, CPE; Susan Kotowski, PhD, CPE Description Pressure ulcers (PUs) are a pervasive and costly problem, with 1.3 to 3 million being reported each year. This session will discuss the factors
leading to Pus (pressure, shear, friction, moisture and heat). Repositioning schedules and guidelines will be discussed as well as ways to minimize the risks using safe patient handling equipment
Objectives 1. Gain a basic understanding of the multiple factors that lead to pressure ulcers 2. Understand which patient handling procedures can be used to minimize the risk of pressure ulcers.
Subject Matter 1a. Shear, friction, pressure, moisture, heat, patient attributes. 2a Elimination of movement down in the bed, repositioning, key components and practices to minimize risk.
Participant Level Multilevel Method of Presentation Lecture, Discussion References 1. Akins, J. S., Karg, P. E., Brienza, D. M. (2011). Interface shear and pressure characteristics of wheelchair seat cushions. J Rehabil res Dev,
48(3), 225-234. 2. Lyder, C. H. (2003). Pressure ulcer prevention and management. JAMA, 289(2), 223-226. 3. Reger, S. I., Ranganathan, V. K., Orsted, H. L.., Ohura, T., & Gefen, A. (2010). Shear and friction in context. In: International Review. Pressure Ulcer Prevention: Pressure, Shear, Friction and Microclimate in Context: A Consensus Document, London, 2-10. 4. MTakahashi, M., Black, J., Dealey, C., Gefen, A. (2010). Pressure in Context. In: Internaitonal Review. Pressure Ulcer Prevention: Pressure, Shear, Friction and Microclimate in Context. A Consensus Document, London, 2-10/ 5. Webb, M. (2010). Evaluation of New Lifting Products to Promote Patient Hygiene and Reduce Risk
of Pressure Ulcers. WOCN/WCET Joint Conference, Phoenix, AZ.
Title Evaluating Differing Showering and Washing Methods on Their Ergonomic, Quality and Efficiency Aspects
Presenters name and credentials Hanneke Knibbe Description Nurses and patients make choices in washing procedures. These choices have consequences for their comfort, pleasure, physical load and
their workload. In spite of that there is little reliable information in the [scientific] literature on how strenuous, time sonsuming, or comfortable these procedures are. This session will present a way to assess these factors to attain the best method of care.
Objectives 1. List the various tasks involved. 2. Understand how to assess various methods that can be used. Subject Matter 1a. High-low profiling bed, 1b. Fixed height shower chair, 1c. High-low shower chair, 1d. Shower chair with profiling seat, 1e. High-low
shower trolley, 1f. Flexible shower trolley. 2a. Time procedure will take, 2b. Physical load (static and dynamic)., 2c. Number of caregivers required, 2d. Time caregivers spend in healthy postures, 2d. Quality of care and perceived comfort rated by patients and nurses.
Participant Level Multilevel Method of Presentation Powerpoint, lecture, Q&A References 1. Koppelaar, E., HJJ Knibbe, HS Miedema, A. Burdorf. (2012). The influence of ergonomic devices on mechanical load during patient
handling activities in nursing homes. Annals of Occupational Hygiene, 56(5), 708-718. 2. Loppelaar, E., Knibbe, J. J., Miedema, HS et al. (2011). Individual and orgaizatnal determinants of use of ergonomic devices in healthcare. Occupational and Environmental Medicine, 68, 659-665.
Title Safe at Home? Challenges to SPH in the Home Care Setting
Presenters name and credentials Esther Murray, RN, MSN, CSPHP Description Homes health represents one of the most difficult settings in which to promote safe patient handling. In the past several years there has
been an upsurge of MSD injuries in the home health area. While the home health agency may have injured employees, they are able to hire a replacement. The family caregiver is irreplaceable and often is hurt before the family looks for assistive devices. The home health worker, the client and the family caregivers are all part of a vulnerable population.
Objectives 1. Discuss the vulnerability of the home health worker and family care giver to musculoskeletal disorders. 2. identify give most dangerous patient handling and movement tasks in the home setting. 3. List types of assistive devices utilized for above tasks. 4. Discuss changes needed in the physical environment to correct difficult and awkward postures. 5. Identify barriers to implementing Safe Patient Handling in the Home Health environment.
Subject Matter 1. Vulnerability: a. Demographjics of HHW, b. Injury rates for HHW, c. Injury rates for family caregivers (AARP survey). 2. Dangerous tasks. A. Elements of a rishy home environment. B. 5 Most risky patient handling tasks. 3. List types of assistive devices utilized for above tasks. a. Friction reducing devices, b. Ceiling lifts, c. Assistive bathing devices. 4. Environment. a. Guidelines for simple changes in physical environment, b. Correcting awkward postures. 5. Barriers. a. Adequate funding, b. Time for training/role playing, c. Home assessment to identify number of attendants to safely administer care, d. Empowering home health care worker to advocate for their own safety.
Participant Level Intermediate Method of Presentation Lecture, multi-media, case studies.
References a. Cheung, K., Gillne, M., Faucett, J., Krause, N. (2005). The prevalence of and risk factors for back pain among home care nursing personnel in Hong Kong. American Journal of Industrial Medicine, 49(1), 14-22. 2. Gong, F., Baraon, S.< Stock, L., Ayala, L. (2009). Formative research in occupational health and safety intervention for diverse, underserved worker populatoins: a homecare worker intervention project. Public Health Reports, 124(1), 84-89. 3. Koppelaar, E., Knibbe, J., Miedema, H., Burdorf, A. (2013). The influence of individual and organizational factors on nurses' behavior to use lifting devices in healthcare. Applied Ergonomics, 44(4), 532-537. 4. Markkanen, P., Quinn, M., Glaligan, C., Chalupka, S., Davis, L., Laramie, A. (2007). There's no place like home: a qualitative study of the working conditions of home health care providers. JOEM, 49(3), 327-337).
Title Making Your Data Work: Effective Use of Workers' Compensation Data to Support SPHM Efforts
Presenters name and credentials Teresa Boynton, MS, OTR, CSPH; Stavey Coffman, BS, DBA, Certified Database Administrator Description Effective use of workers' comp data can drive SPHM efforts an d can impact sustainability. Data has to be presneted in a manner that is
understandable and tells a clear "story." Preseentation of data needs to be geared to the audience (i.e., what will limpacts CEOs, CNOs and CFOs to take action is often different from data that will lead Department Directors and Nurse Managers to act.
Objectives 1. Describe how to collect data, create pivot tables and clearly display data for greatest impact. 2. Understand how to effectively communicate the status of employee injuries and workers' compensation claims within your organization for appropriate action planning. 3. Understand how to use OSHA, DOL, BLS data and info for benchmarking.
Subject Matter PowerPoint slides and lecture will. 1. Cover examples of data and use of Excel spreadsheets; show to to create bar and line graphs that are easy to understand compared to examples that are difficult to understand. 2. Cover examples of charts that provide a clear picture of large amounts and types of data (e.g., all injuries compared to patient handling-related injuries; lost time and restricted itme for all injuries compared to patient handling-related injuries, TCIR and DATR). 3. Use of various data and charts for facilities compared to OSHA, DOL, BLS data.
Participant Level Multilevel Method of Presentation PowerPoint and Lecture References 1. OHSA and BLS web sites. 2. Aon Risk Solutions, Health Care Workers Compensation Barometer. (2014). Retrieved from:
http://www.aon.com/risk-services/thought-leadership/report-2014-health-care-barometer.jsp. 3. Aon Risk Solutions, Empower Results: Four Tactics to Tune Up a Safe Patient Mobility Program. (2014). Retrieved from: http://www.aon.com/attachments/risk-services/Techniques-for-Improving-a-Patient-or-Resident-%20Movement-Program.pdf. 4. Glassman, K. S., & Rosenfield, P. (2015). Data Makes the Difference: The Smart Nurse Handbook for Using Data to Improve Care. Silver Springs, MD: ANA.
Title Don’t Fall For It Presenters name and credentials Dee Kumpar, MBA, BSN, RN, CSPHP Description Are we doing everything we can to prevent falls? Using evidence-based research this session reviews prevalence of falls and contributing
factors to falls. Discuss anticipated and non-anticipated physiological falls and accidental falls. There is a review of four of the most popular fall risk tools and best practice toolkits. The need for SPHM as a fall intervention is explored.
Objectives 1. Understand the incidence of inpatient falls and factors that contribute to increased risk of falling. 2. Understand the patient, caregiver, and economic implications of hospital falls. 3. Recognize the purpose and role of fall risk screening tools, available best practice recommendations, and products for inpatient fall prevention. 4. Discuss a population-specific approach to fall and injury prevention and best practices for assessing outcomes of fall prevention initiative
Subject Matter 1. Population and hospital data from NDNQI. 2. Review of cost fro fall to patient, caregiver, and reimbursement issues. 3. Review Hendrich, Morse, STRATIFY, and Johns Hopkins rtoola
Participant Level Intermediate to Advanced Method of Presentation PowerPoint and Lecture
References 1. AAMC: To the Point. August 2013. Hospital acquired condition reduction program. Available at: https://www.aamc.org/download/353228/data/aamctothepointhac.pdf. 2. AGS/BGS Clinical Practice Guideline. Prevention of Falls in Older Persons. 2010. 3. Bates DW, et al. Serious falls in hospitalized patients: correlates and resource utilization. Am J Med. 1995;99(2):137-43. 4. Fischer ID, et al. Patterns and predictors of inpatient falls and fall-related injuries in a large academic hospital. Infect Control Hosp Epidemiol. 2005;26(10):822-7. 5. Fuller GF. Falls in the elderly. Am Fam Physician. 2000;61(7):2159-68, 2173-4.
Title Organization/Policy Panel: Vision and Action for Universal SPHM Presenters name and credentials Merl Miller, MS, ARC, CIE, CPE (Moderator); Panel: Lori Severson, CSP, Deanna Watkins, MSN, RN, CSPHP, Monica Zeigler, DPT, Denise
Loucks, CSP, CIH Description As advocates for SPHM practices, the goal of universal standards implemented across the continuum of care is an ideal we are striving for.
This panel will discuss a variety of effective methods to ensure organizations are moving toward that aim. Topics will include: 1. Linking to organization mission, vision and values; 2. Adopting the ANA Safe Patient Handling and Mobility Standards; 3. Mobilizing a vision into an actionable plan; and 4. Demonstrating the positive benefits of SPHM to executive decision makers.
Objectives a. Relate the aims of SPHM practices to the mission, vision and values statement of a healthcare organization, 2. Recognize how to communicate the benefits of SPHM to healthcare executive leadership, 3. Name three opportunities to integrate the ANA SPHM Standards into policy statements, 4. Formulate two action steps that translate a vision statement into organizational SPHM effort.
Subject Matter Panel members will do an overview of their area and then open to the floor for questions to be answered by the specialist(s) in that area.
Participant Level Multilevel Method of Presentation Panel presentation and Q&A References 1. Krill, C., Staffileno, B. & Raven, C. (2012). Empowering staff nurses to use research to change practice for safe patient handling. Nursing
Outlook, 60(3), 157-162. 2. Enos, L. (2011). Making the business case to initiate, sustain and evaluate safe patient handling programs (Part 1). American Journal of Safe Patient Handling and Movement, 1(3), 8-15. 3. Enos, L. (2011). Making the business case to initiate, sustain and evaluate safe patient handling programs (Part 2). American Journal of Safe Patient Handling and Movement, 1(4), 8-16. 4. Hunter, B., Branson, M., & Davenport, D. (2010). Saving costs, saving health car e providers' backs, and creating a safe patient environment. Nursing Economics, 28(2), 130-134, 5. Campo, M., & Darragh, A. R. (2012). Work-related musculosheletal disorders are associated with impaired presenteeism in allied health care professionals. Journal of Occupational and Environmental Medicine, 54, 64-70.
Title Meaningful Safe Environment: Individual, Facility and Legislative Approaches Presenters name and credentials Fritz, Gallagher, Kielich
Description This course seeks to provide evidence to drive the SPHM change along with practical ideas to sustain the change over time. It will explore the influences of individual and family values along with safety mandates and legislative actions.
Objectives 1. Identify evidence associated with existing safety mandates. 2. Recognize the threat a culture of sacrifice poses to patient and worker safety. 3. Describe practical approaches to facilitate sustained change.
Subject Matter Provide evidence to drive SPHM change along with practical ideas to sustain the change over time. Barriers to safety (ineffective leadership, culture of sacrifice "Florence Nightingale effect), business case. Stakeholder values: individual, facility, legislation. Practical approaches: Ethics, business case, modeling cultural transformation, growing leaders, empowering people, ways to challenge unhealthy cultures and promote a culture of safety.
Participant Level Multilevel Method of Presentation Lecture, hands-on, group discussion
References 1. Batti, R., & Victoria, S. (2014) Accountability in nursing practice: why it is important for patient safety. AORN Journal, 100(5), 537-541. 2. Pronovost, P., Berenholtz, S., Goeschel, C., Needham, D., Sexton, J., Thompson, D., Lubomski, L., Martseller, J., Makary, M., & Hunt, E. (2006) Creating high reliability in health care organizations. HSR: Health Services Research, 41(4), 1599-1617. American Nurses Association (2013). Safe Patient Handling and Mobility Interprofessional National Standards. Silver Spring, MD: ANA Nursing World. 4. Balas, E. A., & Boren, S. A. (2000). Managing Clinical Knowledge for Healthcare Improvement: Yearbook of Medical Informatics (pp. 65-70). Bethesda, MD: National Library of Medicine. 5. Smith, J. L., & McCarren, H. (2013). Developing servant leaders contributes to VHA's improved organizational health. Organizational Health, 19, 1-2.
Educational Design (Post Conferences) Safe Patient Handling and Mobility Conference, Glendale Arizona, April 11-15, 2016
Title Developing the Leadership Skills You Never Knew You Had Presenters name and credentials Diane Dick, Anna Kay Steadman MA, OTR, CHSP; Kathleen Nelson PT Description Leadership is Influence. What type of influence do you demonstrate to your team? Let us take you on a journey to develop your
Leadership toolbox thru a highly engaging session of self discovery. You will learn tangible techniques and engage in exercises to increase your leadership effectiveness with your teams.
Objectives Participants will be able … 1. To more effectively identify and reduce at risk behaviors in caregivers. 2. To understand the influence leaders have on caregivers. 3. To identify the 4 different motivators and characteristics of employees to gain greater influence. 4. To carry on effective safety conversations to positively influence behavior change
Subject Matter 1. To more effectively identify and reduce at-risk behaviors in caregivers: a. Will create lists of at risk behaviors. b. Will carry on table discussions to understand motivators for unsafe behaviors. 2. To understand the influence leaders have on their employees. a. Will engage in an exercise to demonstrate influence on teams. b. Will identify 5 levels of Leadership and the impact of each. 3. To identify and understand the 4 behavioral styles to increase your level of influence. a. Will take a high level behavioral style assessment. b. Will engage in group discussion about each style and how to utilize the information to improve communication and motivation. 4. To carry on effective safety conversations to positively influence behavior change. a. Will learn a simple 4 step conversation to engage employees in risk identification and behavior change. b. Will practice scenario based conversations in REAL PLAY (role play) exercises
Participant Level Multilevel Method of Presentation Interactive, highly participatory, PPT References 1. Becoming a Person of Influence- John Maxwell. 2. Levels of Leadership- John Maxwell. 3. Crucial Conversations- Kerry Patterson, Joseph
Grenny, Ron McMillan, Al Switzler. 4. Principle Centered Leadership- Dr Stephen Covey
Title It Takes a Village to Implement a SPHM Program Part II Presenters name and credentials Margaret Arnold, BSN, PR, CEES, CSPHP; Jennifer Binkley, DPT, OCS, CSPHA, CEAS II; Teresa Boynton, MS, OTR, CSPHP; Debbie Coughlin,
PT, CSPHP; Lena Deter, RN, MPH, CSPHP, LTC-SSC; Dee Kumpar, RN, BSN, MBA, CSPHP; Laurel Helfen-Lardent, OTR/L, MHA, CEAS, CSPHP; Renee Kielich, RN, CSPHP; Charlotte Lynch, MS, CNS, CSPHP; Elizabeth Potts, BSN, RN-BC, CEASII, Carys Price, PT, MS, CSPHP, CEAS II; Linda Stevens, DNP, RN-BC, CPHQ, CSPHP; Sandy Swan, RN, BSN, MS, COHN-S/CM; CEAS, CSPHP; Patty Wawyziecki, MS, CSPHP; Wendy Weaver, MEd; Kent Wilson, CIE, CSPHP
Description This 2 day/13 hour workshop provides SPHM novices working in the acute care, long-term care and/or a community setting with the basic knowledge and skills required to implement a SPHM program at his/her facility. Day 1 is a seven-hour pre-conference. Day 2 is a six-hour post-conference. A bridge between the two workshops is created throughout the conference by the use of luncheon meetings. A workbook will be provided to each participant. Part II is for novices working in the acute care, long-term care, and/or community setting. This session walks the SPHM novice through the development of the basic components of a SPHM program including, but not limited to, the development of mobility assessment and communication tools, unit peer leader and new hire training programs, additional "best practices" important to program development, creation of a preventative maintenance and repair program, and an introduction to policy development and outcome measurements. It also provides a description of the certification process. A workbook will be provided to each participant.
Objectives 1. Identify the architectural challenges at their facility. 2. Describe the preventative maintenance and repair program that will be created for your facility. 3. Initiate a draft mobility assessment tool and hand-off tool for your facility. 4. Design the basic components of your UPL training program and new hire orientation program. 5. Describe ways to measure and track healthcare worker and healthcare recipient outcomes. 6. Initiate a SPHM policy.
Subject Matter 1. Carpeting vs. flooring; thresholds; door widths, other architectural challenges. 2. Establishment of a PM and repair program. 3. Define mobility assessment and its purpose; Sample mobility assessment tools; Creation of mobility assessment tools for nursing versus rehab; Initiatio of a mobility assessment tool and a bedside communication (hand off) tool. 4. Tracking outcomes; Health care recipients and health care workers. 5. SPHM policy development; Policy content and importancae of each element; Staff roles, Sample policy; Policy implementation and possible barriers. 6. Certification.
Participant Level Novice Method of Presentation PowerPoint presentations, Interactive learner activities, learner workbook. References 1. American Nurses Association. (2013). Safe patient handling and mobility: interprofessional national standards. Silver Spring, MD:
NursesBooks.org. 2. Occupational Safety and Health Administration. (2009). Guidelines for Nursing Homes, Ergonomics for the Prevention of Musculoskeletal Disorders (OSHA 3193 2003; rev. 3/09). US Department of Labor, Occupational Safety and Health Administration. 3. Matz, M. (2010). Facilitating Acceptance of a PHAMP and PHAM Technology. C Borden (Ed.), Patient Handling and Movement Assessments: A White Paper. Dallas, TX: The Facilities Guidelines Institute. 4. Matz, M. (2013). Safe Patient Handling Unit Binder: peer leader. Retrieved 1/21/15 froM: http://www.tampavaref.org/safe-patient-handling/UPLUnitSPHBinder.pdf. 5. Nelson, A. (2006). Safe patient handling and movement. New York: Springer Publishing, Inc. 6. Nelson, A., Motacki, K., & Menzel, N. (2009). Patient Safety Center of Inquiry. (2006). Patient care ergonomics resource guide: safe patient handling and movement. Tampa, FL: VISN 8 Patient Safety Center of Inquiry.
Title Connecting the Dots! Presenters name and credentials Esther Murray, RN, MSN, CSPHP Description Conference attendees are often overwhelmed with the new information they encounter at the SPHM conference. This post-conference
workshop is intended to assist the attendee in writing a business plan draft collating information they have gleaned from conference presentations and exhibits. The approach utilizies the & Habits (and a business plan template) as a guide in evaluating potential strategies for the business plan inclusion.
Objectives 1. Apply the 7 Habits approach to plan for SPH success. 2. Identify proactive planning strategies to gain administrative buy-in. 3. Discuss unit assessment process. 4. Assimilate PSH goals into a facility specific business plan draft.
Subject Matter 1. Apply. A. Formulate a tentative vision/mission statement, b. Develop 3 S. M. A. R. T. goals, c. List tentative short term and long-term goals. 2. Identify. A. Develop business case for PSH program. b. Implementation strategies such as education and training. c. Identify strategies for unit peer leader development. 3. Discuss. a. List high risk units and assessment needs. b. Identify potential cost effective oslutions. 4. Assimilate. a. Utilizing a business plan template gather info for a tentative facility specific business plan..
Participant Level Intermediate Method of Presentation Multimedia/Group interaction and discussion References 1. AOHP (2014). Beyond getting started: a resource guide for implementing a safe patient handling program in the acute care setting. third
edition. 2. Cadmus, E., Brigley, P.,& Pearson, M. (2011). Safe Patient Handling: Is Your Facility Ready for Culture Change? Nursing Management, Nov. 2011. 3. Hinton, M. (2010). Establishing a safe patient handling/minimal lift program. Orthopaedic Nursing, 29(5), 325-332. 4. Hunter, B., Branson, M., & Davenport, D. (2010). Saving costs, saving healthcare providers' backs and creating a safe patient environment. Nursing Economic$, 28(2), 130-134. 5. Krueger, C., & Barnes, D. (2007). Glens Falls Hospital shares insights on creating a SPH program. AOHP Journal, 27(4), 13-15. 6. Waters, T. (2007). When is it safe to manually lift a patient? AJN, 107(8), 53-59.

![Educational Technology Conferences - teachonline.ca · Educational Technology and Education Conferences for January to June 2018, Prepared by Clayton R. Wright, crwr77[at] gmail.com](https://img.pdfslide.net/doc/110x75/5e1cee371d8bc746755ea599/educational-technology-conferences-educational-technology-and-education-conferences.jpg)




![Educational Technology Education Conferences January to ... · Educational Technology and Related Education Conferences for January to June 2011, Prepared by Clayton R. Wright, crwr77[at]](https://img.pdfslide.net/doc/110x75/5f08cbd37e708231d423c36a/educational-technology-education-conferences-january-to-educational-technology.jpg)






















