-
1
中山醫學大學附設醫院
神 經 外 科
陳偉健
1. Infarction(73.5%)• Thrombosis• Embolism•Venous
thrombosis(0.1%)
2 H h
1. Infarction(73.5%)• Thrombosis• Embolism•Venous
thrombosis(0.1%)
2 H h
CVA (Stroke):1. Infarction 2. Hemorrhage
SAH
2. Hemorrhage• Spontaneous ICH (16.2%)
•Hypertension[83.1]•AVMs•Others ( tumours, vasculitis,
coagulopathy )
•SAH (2.9%)•Aneurysms [69.5%]
3.TIA (6.7%)
2. Hemorrhage• Spontaneous ICH (16.2%)
•Hypertension[83.1]•AVMs•Others ( tumours, vasculitis,
coagulopathy )
•SAH (2.9%)•Aneurysms [69.5%]
3.TIA (6.7%)ICH
主要原因: rupture of small vessel (microaneurysm)長期的高血壓(50-70
yrs)Amyloid angiopathy(>70yrs)
發生率:發生率:東方人及黑人>白種人目前35歲以上每10萬人口每年約有73人(22%)
死亡率:發病一個月內的死亡率約26‐30%
臨床症狀:
a.突發的局部神經症狀
b.頭痛(40﹪)、噁心嘔吐(35﹪)、血壓偏高(87﹪)、意識障礙(50﹪),少數會有癲癇發作現象(6.1%)
c.約35﹪早期症狀會有惡化(6小時內持續出血)
致病原因:
a.高血壓病史,可能伴隨頭部外傷之症狀
b.用抗凝血劑、抗血栓藥物
c.酒精或藥物成癮
d.血液疾病
e.其他原因如顱內動脈瘤,腦瘤,動靜脈畸型或類澱粉樣血管病變等。
列為常規檢查。
Dx: PE or NE很難準確區分出ICH或infarction
use CT
( level of evidence I, grade A recommendation )
DSA: (可做) 年青、無高血壓病史或無其他腦出血危險因素之患者可做。(可做) 年青
無高血壓病史或無其他腦出血危險因素之患者可做(不需做)年長病患,腦出血位於基底核、視丘、小腦或橋腦
MRI:海綿狀血管瘤(cavernous malformation) or tumor
Routine:CBC 、一般生化、PT及APTT、electrolyte、EKG、chest x-ray
Indicating of angiography :
Unusual location of ICH
Young stroke, without bleeding tendency
-
2
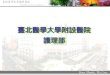
Putamen (A) 50 %Lobar
(B) 16 %Thalamus
(C) 12 %Cerebellum
(D) 10 %Cerebellum
(D) 10 %Pons
(E) 8 %Caudate
(F) 4 %
Putaminal ICH
A B
Thalamic ICH Basal ganglia ICH +Thalamic ICH + IVH+SAH
IVHSAH SAH
PT
P: putamen T: thalamus Uncal/transtentorial herniations
Pontine ICH
3V
LV
4V
LV: lateral ventricle
Cerebellar ICH
-
3
M/74, CVA due to cerebellar hemorrhage, with IVH, and
compressing the 4th ventricle, causing obstructive
hydrocephalus
Subcortex ICH of left occipital lobes
Multiple hemorrhages in the cerebral cortex.Repeat attack.Aged patients.
Female, 72 y/oCortical hemorrhage, possible is due to amyloid
microangiopathy
CT MRI, T1WI MRI, T2WI
-
4
Tumor bleeding
M/73Lung ca. with brain metastasis with tumor bleeding
ACA
ACA
AVM
F/44A. 89,3,5 CT: An ICH in Rt. Frontal lobe.B,C. 89,3,6 DSA: A
small AVM, feeded from Rt. ACA, with drainage veins to sagittal
sinus.
Aneurysm
M/34yAneurysm in the M1 portion ofleft MCA, causing a big ICH in
the left basal ganglia and frontal lobe, and with IVH.
CTA
DSA
Mycotic aneurysm
M/4, CVA, due to rupture of an mycotic aneurysmCT: Acute
hematoma and edema in right parietal lobe.DSA: an aneurysm (mycotic
aneurysm) in the right Sylvian branch
Moya Moya disease
F/21MoyaMoya disease with thalamic hemorrhage
and IVHA. CT: Rt. Thalamic hemorrhage with IVHB. Rt. Carotid
angiographyC. Lt. Carotid angiographyD. Vertebral angiographyE. The
angiographies showing total occlusions of the bilateral
internal carotid arteries with numerous fine
collateralcirculations, with “moyo-moya appearance,煙霧狀”.
Moyamoya disease 事實上引起ischemic infarction 比較多
All patients
should be monitored in a dedicated ICU for at least 24 hours
afterthe clinical event.
( A I Qureshi et al. Spontaneous intracerebral
haemorrhage.N Engl J Med 2001;344:1450‐1461 )
-
5
急診室: ‧ ABC。
注意呼吸道:‧ 昏迷的病人‧ 腦幹功能障礙
雖然目前尚無足夠的臨床試驗佐證,可證明內科或外科治療對病人較有幫助,但下列的處理仍為大家所認可的基本原則:
腦幹功能障礙
On Endo: ‧ 缺氧現象PO250mmHg)‧ 吸入性肺炎
Tracheostomy:‧ 氣管插管2星期左右仍無法能拔除。
Keep plasma
Na+ > 140m mol/l. (a decrease produces an osmotic gradient across the BBB & aggravates cerebral edema)
Avoid hyperglycemia and hypoglycemia
(=120mg/dl) (an increase aggravates brain ischemia
by increasing (an increase aggravates brain ischemia
by increasing cerebral lactic acidosis)
N‐G tube feeding
(gastric motility drugs can be given)
15‐30º head up tilt
with the head kept in a
neutral positionmay improve CPP
Aim(高血壓病史的病人): SBP
-
6
EVD:Ind:腦出血後阻塞腦脊髓液通路而造成續發性水腦症;一般引流最好不要超過7天,且需給予預防性抗生素以免感染。
Osmotic:glycerol或manitol(易產生反彈)Mannitol 20 %, 0.25-0.5 g/Kg,
Q4h; Furosemide 10 mg,Q4h,
Steroids:建議儘量不使用類固醇,因其副作用太大,且降顱內壓效果不會比高滲透壓藥物效果好。
Hyperventilation:PaCO2降至30-35mmHg約可降低顱內壓25-30﹪。突然停止過度換氣,可能造成顱內壓反彈而突然升高,因此需在1、2天內慢慢將PaCO2恢復正常。將PaCO2恢復正常
Barbiturate
coma治療為最後的選擇,它可降低腦細胞代謝,減少腦血流而降低顱內壓,但會使血壓降低,亦容易造成感染,導致敗血症而死亡。Multiple
small boluses ( Thiopental ): 0.3-0.6 mg/Kg
預防癲癇腦出血病患視病情需要可給Dilantin或其他抗癲癇葯物做預防性治療使用一個月後若無發作,才慢慢停藥。
( Class III,level C)
( Class IIb,level C)
輸液治療(fluid management)EuvolemiaCVP:5-12mmHg,pulmonary wedge
pressure:10-14mmHg電解質及酸鹼平衡都需做監測調整
每天的intake and output亦需視尿量做調整(尿量加500cc,若有發燒,每度加300cc)。
體溫控制體溫應儘量維持在正常範圍
高於38.5℃時,可給予acetaminophen,或降溫毯將體溫降低。
需注意探討及預防各種感染的可能性,及使用預防性抗生素以避免感染染。
其他內科療法對於譫妄(delirium)或躁動不安的病人,可使用短效的Benzodiazepines或propofol,
其他如止痛、鎮靜劑亦可視各種情況使用。
其他亦需注意深部靜脈阻塞、肺栓塞之預防,以及早期做復健治療。
( Class I,level b)
SjO2 monitoringTCD
Those techniques hasyet to be tested in a randomised study forpatients with
TCDPBrO2EEG monitoring
Spontaneous ICH.
( NO recommendation )
是否需手術及手術的時機為何,尚無定論。
Aim: 減少腦內血塊產生的併發症(壓迫周遭正常腦組織、水腦症、或血塊導致嚴重的腦水腫)
估計血塊體積方法估計血塊體積方法以CT為主
1/2(長×寬×高)
小出血(<10cm3)或神經症狀很輕微者需注意觀察,超急性ICH(<3小時)常會有擴大情況。
昏迷指數(GCS)
-
7
病人已深度昏迷,
經加護觀察24小時以後,病情仍未好轉,醫生及家屬仍不考慮外科手術時
(Class IIb, level B)
rFVII Phase IIA的初步研究結果,3 小時內用藥可有效預防急性腦出血的擴大。
但此種治療方法是否安全有效,仍需等待未來更大型的多中心合作研究。多中心合作研究
(class IIb, level B)
CraniotomyTranscortical(subtemporal) approach (microscope or gross)Transylvian approach (microscope)
Stereotactic aspirationsStereotactic aspirationsEndoscopic surgery
Conventional surgery25% of mortality and 58.9% of poor outcomesTranssylvian approach with low technique
-
8
Most extensively studied.GCS 7‐10, surgery reduce risk of death without improving functional outcomeGCS 9‐12,lobar clot3cm,benefit of surgeryTiming: Very early surgery increase risk of rebleeding
Combined with rFVIIa
-
9
Minimally invasiveHigh efficiency: 60‐88% hematoma evacuation rateWaiting time at least 4‐6 hours after onsetUrokinase installationRebleeding rate 35%Infection rate
Case presentationCase1,87 y/o male,Rt basal ganglion ICH,
GCS:8 →12
Case2,86 y/o female,Rt basal ganglion ICH, GCS:9 →12
Case3,76 y/o male,right basal ganglion ICH, GCS:8 → 11
Case4,59 y/o left thalamus ICH, GCS:6 mortality due to central
failure
Transparent sheathProtect brain
SuctionAspiration
L
iLocationBlind techniqueSono guidedNavigator guided
Entry pointBurr hole
HemostasisSuction bipolar
-
10
Big trochar ?Traction?Hemostasis?
-
11
•Less invasive•Burr hole opening•Under local anesthesia
•Transparent sheath•Improve visualizationp•Small diameter
•Free hand surgery without fixation•3D operation
•Suction unipolar•Facillated hemostasis
•Low techniqueNewly develop endoscopic instruments for the
removal of ICH, Neurocritical care 2005
-
12
Case1,66y/o male,Lt thalamus ICH, GCS:9 →15
C 2 68 / l Rt b ll ICH GCS 7 15Case2,68 y/o male,Rt cerebellar
ICH, GCS:7 →15
Case 3,49 y/o male,Rt putamen ICH, GCS:6 →15
C 4 79 / f l Rt t ICH GCS 8 15 ( id )Case 4,79 y/o female,Rt
putamen ICH, GCS:8 →15 (video)
Case 5,57 y/o male,cerebellar ICH, GCS:6 → 12
Case 6,58 y/o male,rt basal ganglion ICH, GCS:5 → 11Case 6,58
y/o male,rt basal ganglion ICH, GCS:5 11
Our surgical procedure is indicated forSpontaneos or hypertensive ICH excluding organic disease (aneurysm,AVM etc)Putaminal,thalamic and subcortical hemorrhage >20ccCerebellar hemorrhage >15cc(or 3cm)Cerebellar hemorrhage >15cc(or 3cm)
We assume that thalamic ICH with ventricular extension with obstructive hydrocephalus is good indication.We indicate ultra‐early endoscopic surgery for ICH with a volumn of 30cc or more and for hemorrhage causing impending herniation.
-
13
1/18 conversion to standard procedure due to unable to aspirate hematoma.1/18 subdural hematomaNo motality.
Endoscopic evacuation using transparent sheath canProvide good hematoma evacuationWithin short surgical preparing timeMinimaly invasive
Our surgical procedure may show better results than Our surgical procedure may show better results than standard procedure.
ICH surgeryCT fluoro guided aspiration
Vascular surgeryEnderctomyEC
IC bEC‐IC bypassHigh flow bypass
Endoscopic surgeryTransphenoid (pituitary tumor)ETV(hydrocephalus)Brain cyst(arachnoid,pineal,supracellar,colloid)Spine surgery (PLED)