Embed Size (px)
Citation preview

Effect of Aspirin and Ticlopidine onPlasma Tissue Factor Levels in Stable
and Unstable Angina PectorisJean Marco, MD, Robert A.S. Ariens, PhD, Jean Fajadet, MD, Irene M. Bossi, MD,
Isabelle Marco, MD, Monique Bernies, MD, Salvatore M. Romano, MD,Francesco Donatelli, MD, Gabri M. Brambilla, MD, Francesco Somalvico, PhD,
Daniela Mari, MD, and Luisa Gregorini, MD
Patients with unstable angina have an increased activa-tion of the coagulation system. Aspirin and ticlopidinegiven in combination may potentiate each other by thecombination of different action mechanisms and mayreduce the risk of coronary occlusion and clinical insta-bility. Plasma tissue factor (TF) levels collected into thestenotic coronary artery may be an index of TF expres-sion within the vasculature. In 160 patients undergoingangioplasty for a 81 6 5% coronary lesion, we mea-sured TF in blood samples collected from a vein and fromthe coronary ostium. Immediately after and 10 minutesafter the dilation procedures the samples were with-drawn also beyond the lesion. Heparin 150 U/kg wasgiven as an anticoagulant. All patients were pretreated
with 250 mg/day of aspirin. One hundred twenty pa-tients were randomly assigned to receive 24, 48, or 72hours of ticlopidine treatment (250 mg/twice daily). TFlevels did not increase during angioplasty but there wasa significantly higher TF expression in unstable than instable patients, irrespective of the invasiveness of de-bulking procedures. When ticlopidine was given for 72hours, TF levels were similar to normal laboratory valuesboth in stable and unstable patients. This combinedantiplatelet pretreatment may be of benefit in unstableangina patients, with a favorable cost/benefit ratio.Q2000 by Excerpta Medica, Inc.
(Am J Cardiol 2000;85:527–531)
Unstable angina is a dynamic clinical situation inwhich recurrence of symptoms correlates with
plaque ulceration, coagulation activation, and throm-bus formation.1–3 An angioscopic study of the plaqueshas shown that ulcerations are present in 55% andthrombus in 68% of the coronary arteries responsiblefor unstable angina.4 The lipid-rich atheroscleroticcore exposed to circulating blood by plaque rupturetriggers the coagulation activation.5,6 Coronary stent-ing7,8 and rotational atherectomy9 are revasculariza-tion techniques that extensively abrade endotheliumand plaque,10,11 thus exposing the tissue factor (TF)present within the necrotic lipid-rich core12–15 to fac-tor VII. TF may be responsible for activation of thecoagulation cascade, and accordingly could be in-volved in the pathogenesis of acute events.15–17Traceamounts of TF are also present in plasma,14 and theseplasma levels may reflect TF expression within thevasculature. We have recently shown that aspirin,heparin, and 72 hours of ticlopidine pretreatment ef-ficiently reduced both thrombin generation and plate-
let activation in patients undergoing angioplasty.18 Inthe present study we investigated whether aspirin andticlopidine pretreatment, given in combination in pa-tients with stable and unstable angina, may reduceplasma TF levels in the most unfavorable clinicalcondition of endothelium abrasion and plaque fissur-ing as during angioplasty.
METHODSWe enrolled in the study 160 consecutive patients
who represented a typical sample of our angioplastypopulation. Among them 80 had stable angina and 80had spontaneous durable recurrent episodes of chestpain and were classified as unstable.1,2 The mean agewas 63.56 11.6 (18 women) and 64.46 11.3 (12women) in patients with stable and unstable angina,respectively. The indication to angioplasty was givenin the presence of a coronary lesion that occluded thevessel by 796 4% and 836 5% (mean6 SD) inpatients with stable and unstable angina, respectively.Among the unstable patients, 18 had non–insulin-dependent diabetes. All patients signed an informedwritten consent to allow blood sampling, and the Clin-ique Pasteur ethical committee had previously ap-proved the study.
Pharmacologic treatment: All patients were pre-treated with 250 mg/day of aspirin. Twenty of 80patients who had stable angina and an apparentlyregular, short, and smooth lesion were pretreated onlywith aspirin and the lesion was dilated by conven-tional percutaneous transluminal coronary angioplasty(PTCA). Twenty of 80 patients who had unstable
From Clinique Pasteur, Toulouse, France; and Cardiovascular Scienceand Internal Medicine Department, Ospedale Maggiore-IRCCS, Uni-versity of Milan, Milan, Italy. This study was supported in part byinstitutional funds from the University of Milan (MURST 60%), Milan,Italy, and by the research funds from Clinic Pasteur, Toulouse, France.Manuscript received April 26, 1999; revised manuscript received andaccepted September 29, 1999.
Address for reprints: Luisa V. Gregorini, MD, Cardiovascular Sci-ence Department, Ospedale Maggiore IRCCS, Universita di Milano,Via Francesco Sforza 35, 20122 Milano, Italy. E-mail:[email protected].
527©2000 by Excerpta Medica, Inc. All rights reserved. 0002-9149/00/$–see front matterThe American Journal of Cardiology Vol. 85 March 1, 2000 PII S0002-9149(99)00805-X

angina were pretreated only with aspirin, but to pre-vent possible complications they were given low mo-lecular weight heparin in a weight–adjusted dose(enoxaparin 120 IU/kg) before PTCA. After coronarystenting they were treated with ticlopidine and aspirinfor 1 month. All other patients received ticlopidine250 mg twice daily in addition to aspirin.18 Ticlopi-dine pretreatment was randomly given to patients afterdiagnostic coronary angiography (1 of 4 patients in thestable or unstable angina group) for 24, 48, or 72hours to find the time course of antiplatelet treatment.Antianginal treatment such as nitrates and calciumantagonists (diltiazem 180 to 360 mg/day) orb-adren-ergic blockers (atenolol 50 mg/day) were given indoses able to reduce recurrent ischemic episodes.
Angioplasty procedure: To dilate the lesion, con-ventional PTCA was performed in 40 patients withstable angina, coronary stenting in 110 cases, androtational atherectomy in 10 patients (Rotablator,Heart Technology, Bellevue, Washington). Thechoice of technique to perform for dilating the stenosiswas left to the clinician after the anatomy of theplaque to treat and the presence of calcium was es-tablished.7–9 Ninety patients had left anterior descend-ing, 20 left circumflex, and 44 right coronary arterylesions, and 6 of them had a left main trunk lesion.Either the radial (90 patients) or the femoral (70patients) artery approach was used to perform angio-plasty. Heparin (150 U/kg) was given intravenously asanticoagulant after obtaining the basal venous andcoronary ostium blood samples. Isosorbide dinitrate (3mg) was administered intracoronarily as vasodilator.One or multiple stents were implanted in vessels witha reference diameter$3.0 mm. High-pressure infla-tions were performed to overextend the struts of thestents. No acute or subacute closure was observedafter coronary stenting. After coronary stenting ticlo-pidine, 250 mg once daily was given for 1 month.Aspirin was given for life.
Blood sampling: To collect blood samples from thedistal dilated coronary artery and from the coronaryostium, a probing catheter with an internal lumen of0.018 inch was inserted immediately after the lastballoon inflation through the monorail side. As soonas collected blood samples were added to ice-chilledplastic tubes containing sodium citrate (9:1 vol.:vol.).The blood samples were again withdrawn 10 minutesafter the dilation procedures. The blood samples werecentrifuged at 2,000g for 15 minutes at 4°C. Thesupernatant platelet-poor plasma was stored at280°Cuntil analysis. TF was measured in duplicate by en-zyme-linked immunosorbent assay (ELISA) usingcommercially available kits (ImmuBind tissue factorELISA Kit, American Diagnostica Inc., Greenwich,Connecticut). Thrombin-antithrombin (TAT) wasmeasured by enzyme immunoassay using commer-cially available kits (Behring Enzygnost DiagnosticInc.: ELISA-TAT Micro, Marburg, Germany). Allplasma assessments were performed in a blinded man-ner and in duplicate.
Statistical analysis: Results are expressed asmean6 SD. One- or 2-way analysis of variance was
performed with the SPSS 6.1 package, (SPSS Inc.,Chicago, Illinois). To assess statistical significancebetween groups and times of treatment, the Tukey testfor multiple comparisons was applied, with a p value,0.05 considered significant. The plot of the differ-ences between the 2 plasma sample assays against themean differences was evaluated by estimating theconsistent bias between measurements (mean6 2SDs), as described by Bland and Altman.19 The sig-nificance of the mean differences was evaluated usinga paired 2-tailed Student’st test.
RESULTSNo difference was found between TF levels ob-
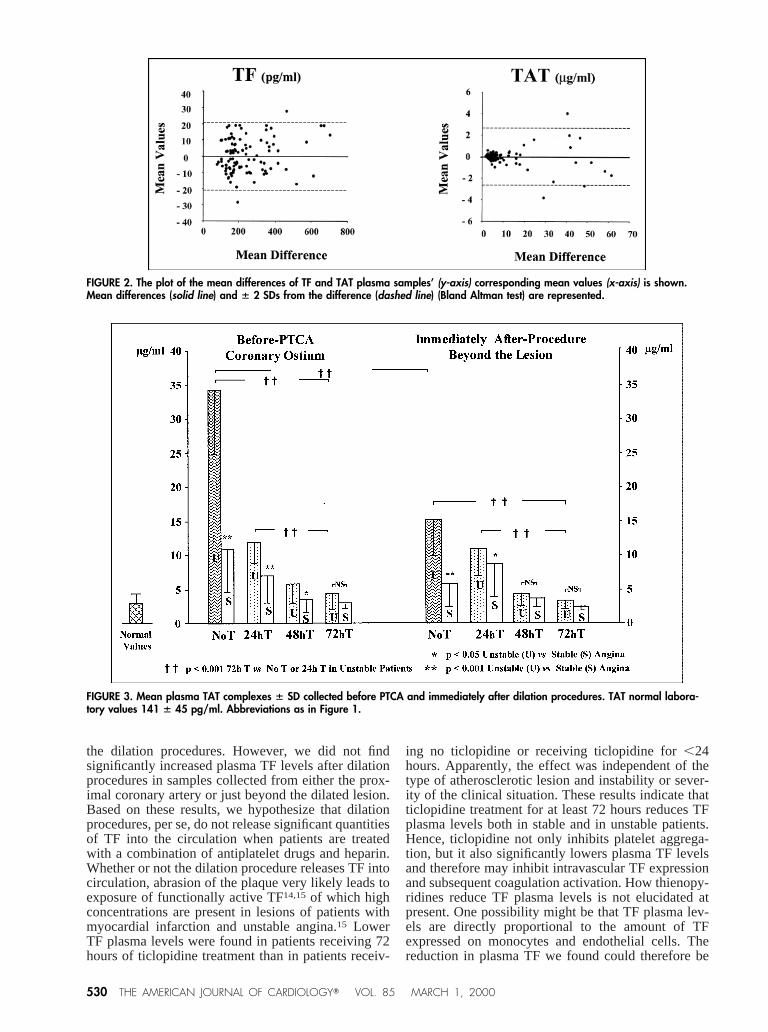
tained in blood samples collected from the coronaryostium before the procedure and those obtained fromthe coronary ostium or from the dilated coronarysegment beyond the lesion immediately after or 10minutes after angioplasty (Figure 1 and Table I). Inaddition, the samples obtained from a peripheral veinwere not different from those obtained from the guid-ing catheter. No differences were observed in plasmaTF antigen levels among patients undergoing the dif-ferent dilation or debulking procedures. Accordingly,data reported in Figure 1 and in Table I were pooled.A significant difference in TF levels was found onlywhen patients were divided by angina status, stable, orunstable. This difference was no longer significantwhen ticlopidine pretreatment was administered for$72 hours. In our patients, the revascularization pro-cedure did not, per se, increase TF levels. The plot ofthe differences between the values from 2 TF samplesversus the mean of the 2 measurements showed amean difference of 0.5656 10.755 pg/ml, with goodagreement because all points but 2 were within6 2SDs (Figure 2) (r5 0.994; p5 0.60).
Thrombin-antithrombin complexes: The TAT levelswere not different in venous and in arterial baselinesamples (Figure 3 and Table II), indicating that thecatheter did not activate the coagulation in the pres-ence of the combined anticoagulant and antiplatelettreatment given. During the revascularization proce-dures, the degree of coagulation activation did notchange significantly, with no differences found be-tween basal venous and arterial levels of TAT com-pared with immediately after and 10 minutes afterPTCA levels. Significantly higher TAT levels werefound in patients not treated or pretreated with ticlo-pidine for#24 hours than in patients given$72 hoursof ticlopidine pretreatment. No difference was ob-served between the samples obtained in duplicate (p50.477). The variability between the 2 measurementsestimated in 100 cases showed a mean difference of0.606 0.834mg/ml (Figure 2), with all values but 3within 6 2 SDs.
DISCUSSIONOur findings show that combined antiplatelet pre-
treatment with aspirin and ticlopidine and intravenousheparin reduced plasma TF levels and thrombin gen-eration in patients with unstable angina, irrespectiveof plaque abrasion or dissections or of metal struts.
528 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 85 MARCH 1, 2000
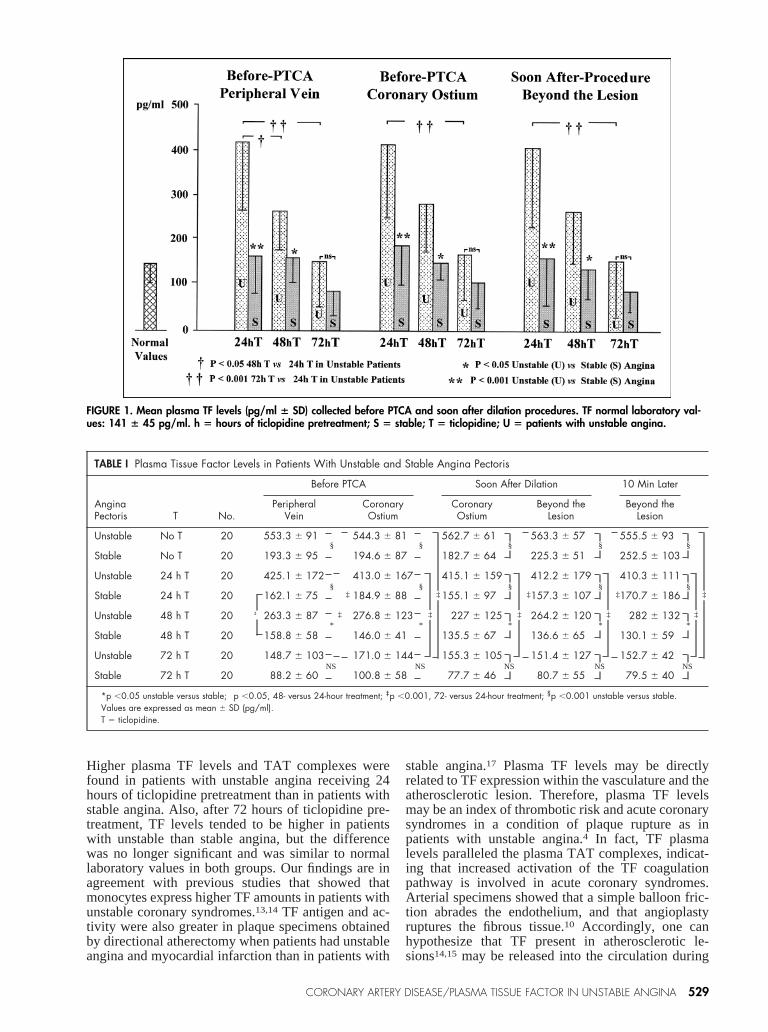
Higher plasma TF levels and TAT complexes werefound in patients with unstable angina receiving 24hours of ticlopidine pretreatment than in patients withstable angina. Also, after 72 hours of ticlopidine pre-treatment, TF levels tended to be higher in patientswith unstable than stable angina, but the differencewas no longer significant and was similar to normallaboratory values in both groups. Our findings are inagreement with previous studies that showed thatmonocytes express higher TF amounts in patients withunstable coronary syndromes.13,14 TF antigen and ac-tivity were also greater in plaque specimens obtainedby directional atherectomy when patients had unstableangina and myocardial infarction than in patients with
stable angina.17 Plasma TF levels may be directlyrelated to TF expression within the vasculature and theatherosclerotic lesion. Therefore, plasma TF levelsmay be an index of thrombotic risk and acute coronarysyndromes in a condition of plaque rupture as inpatients with unstable angina.4 In fact, TF plasmalevels paralleled the plasma TAT complexes, indicat-ing that increased activation of the TF coagulationpathway is involved in acute coronary syndromes.Arterial specimens showed that a simple balloon fric-tion abrades the endothelium, and that angioplastyruptures the fibrous tissue.10 Accordingly, one canhypothesize that TF present in atherosclerotic le-sions14,15 may be released into the circulation during
TABLE I Plasma Tissue Factor Levels in Patients With Unstable and Stable Angina Pectoris
AnginaPectoris T No.
Before PTCA Soon After Dilation 10 Min Later
PeripheralVein
CoronaryOstium
CoronaryOstium
Beyond theLesion
Beyond theLesion
Unstable No T 20 553.3 6 91 544.3 6 81 562.7 6 61 563.3 6 57 555.5 6 93
Stable No T 20 193.3 6 95 194.6 6 87 182.7 6 64 225.3 6 51 252.5 6 103
Unstable 24 h T 20 425.1 6 172 413.0 6 167 415.1 6 159 412.2 6 179 410.3 6 111
Stable 24 h T 20 162.1 6 75 184.9 6 88 155.1 6 97 157.3 6 107 170.7 6 186
Unstable 48 h T 20 263.3 6 87 276.8 6 123 227 6 125 264.2 6 120 282 6 132
Stable 48 h T 20 158.8 6 58 146.0 6 41 135.5 6 67 136.6 6 65 130.1 6 59
Unstable 72 h T 20 148.7 6 103 171.0 6 144 155.3 6 105 151.4 6 127 152.7 6 42
Stable 72 h T 20 88.2 6 60 100.8 6 58 77.7 6 46 80.7 6 55 79.5 6 40
*p ,0.05 unstable versus stable; †p ,0.05, 48- versus 24-hour treatment; ‡p ,0.001, 72- versus 24-hour treatment; §p ,0.001 unstable versus stable.Values are expressed as mean 6 SD (pg/ml).T 5 ticlopidine.
§
§
*
NS
§
§
*
NS
§
§
*
NS
§
§
*
NS
§
§
*
NS
† ‡ ‡ ‡ ‡ ‡
‡ ‡ ‡ ‡ ‡
FIGURE 1. Mean plasma TF levels (pg/ml 6 SD) collected before PTCA and soon after dilation procedures. TF normal laboratory val-ues: 141 6 45 pg/ml. h 5 hours of ticlopidine pretreatment; S 5 stable; T 5 ticlopidine; U 5 patients with unstable angina.
CORONARY ARTERY DISEASE/PLASMA TISSUE FACTOR IN UNSTABLE ANGINA 529
the dilation procedures. However, we did not findsignificantly increased plasma TF levels after dilationprocedures in samples collected from either the prox-imal coronary artery or just beyond the dilated lesion.Based on these results, we hypothesize that dilationprocedures, per se, do not release significant quantitiesof TF into the circulation when patients are treatedwith a combination of antiplatelet drugs and heparin.Whether or not the dilation procedure releases TF intocirculation, abrasion of the plaque very likely leads toexposure of functionally active TF14,15 of which highconcentrations are present in lesions of patients withmyocardial infarction and unstable angina.15 LowerTF plasma levels were found in patients receiving 72hours of ticlopidine treatment than in patients receiv-
ing no ticlopidine or receiving ticlopidine for,24hours. Apparently, the effect was independent of thetype of atherosclerotic lesion and instability or sever-ity of the clinical situation. These results indicate thatticlopidine treatment for at least 72 hours reduces TFplasma levels both in stable and in unstable patients.Hence, ticlopidine not only inhibits platelet aggrega-tion, but it also significantly lowers plasma TF levelsand therefore may inhibit intravascular TF expressionand subsequent coagulation activation. How thienopy-ridines reduce TF plasma levels is not elucidated atpresent. One possibility might be that TF plasma lev-els are directly proportional to the amount of TFexpressed on monocytes and endothelial cells. Thereduction in plasma TF we found could therefore be
FIGURE 2. The plot of the mean differences of TF and TAT plasma samples’ (y-axis) corresponding mean values (x-axis) is shown.Mean differences (solid line) and 6 2 SDs from the difference (dashed line) (Bland Altman test) are represented.
FIGURE 3. Mean plasma TAT complexes 6 SD collected before PTCA and immediately after dilation procedures. TAT normal labora-tory values 141 6 45 pg/ml. Abbreviations as in Figure 1.
530 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 85 MARCH 1, 2000

caused by inhibition of TF expression on these cellsby ticlopidine. This effect could be similar to, butindependent of, the reduction of glycoprotein IIb-IIIaexpression induced on platelets by ticlopidine. Alter-natively, plasma levels of TF may reflect concentra-tion of the enzyme responsible for TF release into thecirculation. The inhibitory effect of ticlopidine on TFcould be through reduction of this releasing mecha-nism. Either effect may be independent of the effecton platelet biochemistry.
Ticlopidine reduces platelet aggregation by inhib-iting adenosine diphosphate–induced platelet activa-tion, serotonin release from platelets, and expressionof the fibrinogen receptor on the platelet mem-brane.20,21 TF has a structure similar to interferonreceptors, and is placed in the cytokine receptor su-perfamily.22,23 Therefore, TF functions as a cellularreceptor of factor VII,24 and because ticlopidine in-hibits expression of platelet fibrinogen receptors, itmay inhibit expression of TF in a similar fashion.
1. Braunwald E. Unstable Angina: a classification.Circulation 1989;80:410–414.2. Buja LM, Willerson JT. Clinicopathologic correlates of acute ischemic heartsyndromes.Am J Cardiol1984;54:1349–1354.3. Merlini PA, Bauer KA, Oltrona L, Ardissino D, Cattaneo M, Belli C, Man-nucci PM, Rosenberg RD. Persistent activation of coagulation mechanisms inunstable angina and myocardial infarction.Circulation 1994;90:61–68.4. de Feyter PJ, Ozaki Y, Baptista J, Escaned J, Di Mario C, de Jaegere PP,Serruys PW, Roelandt JR. Ischemia related lesion characteristics in patients withstable or unstable angina. A study with intracoronary angioscopy and ultrasound.Circulation 1995;92:1408–1413.5. Fuster V, Steele PM, Chesebro JH. Role of platelets and thrombosis incoronary atherosclerotic disease and sudden death.J Am Coll Cardiol1985;5:175B-184B.6. Bleifeld W, Hamm CW, Braunwald E, eds. Unstable Angina. New York:Springer-Verlag, 1990.7. Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G,Emanuelsson H, Marco J, Legrand V, Materne P, et al, for the Benestent StudyGroup. A comparison of balloon-expandable-stent implantation with balloonangioplasty in patients with coronary artery disease.N Engl J Med1994;331:489–495.8. Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K,
Veltri L, Ricci D, Nobuyoshi M, Cleman M, Heuser R, Almond D, Teirstein RS,Fish D, and the STRESS investigators. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary arterydisease.N Engl J Med1994;331:496–501.9. Warth DC, Leon MB, O’Neill W, Zacca N, Polissar NL, Buchbinder M.Rotational atherectomy multicenter registry: acute results, complications and6-month angiographic follow-up in 709 patients.J Am Coll Cardiol 1994;24:641–648.10. Waller BF. “Crackers, breakers, stretchers, drillers, scrapers, shavers, burn-ers, welders and melters”: the future treatment of the atherosclerotic coronaryartery disease, a clinical morphologic assessment. J Am Coll Cardiol1989;13:969–987.11. Mintz GS, Potkin BN, Karen G, Satler LF, Pichard AD, Kent KM, Popma JJ,Leon MB. Intravascular ultrasound evaluation of the effect of rotational atherec-tomy in obstructive atherosclerotic coronary artery disease.Circulation 1992;86:1383–1393.12. Wilcox JN, Smith KM, Schwartz SM, Gordon D. Localization of tissue factorin the normal vessel wall and in the atherosclerotic plaque.Proc Natl Acad SciUSA1989;86:2839–2843.13. Fuster V, Fallon JT, Nemerson Y. Coronary thrombosis.Lancet 1996;348(suppl):S7-S10.14. Nemerson Y. Tissue factor and hemostasis.Blood 1988;71:1–8.15. Neri Serneri GG, Abbate R, Gori AM, Attansio M, Martini F, Giusti B,Dabazzi P, Poggesi L, Modesti PA, Trotta F, Rostagno C, Boddi M, Gensini GF.Transient intermittent lymphocyte activation is responsible for the instability ofangina.Circulation 1992;86:790–797.16. Marmur JD, Thiruvikraman SV, Fyfe BS, Arabinda G, Sharma SK, AmbroseJA, Fallon JT, Nemerson Y, Taubman MB. Identification of active tissue factorin human coronary atheroma.Circulation 1996;94:1226–1232.17. Ardissino D, Merlini PA, Ariens RAS, Coppola R, Bramucci E, MannucciPM. Tissue-factor antigen and activity in human atherosclerotic plaques.Lancet1997;349:769–771.18. Gregorini L, Marco J, Fajadet J, Bernies M, Cassagneau B, Brunel P, BossiIM, Mannucci PM. Ticlopidine and aspirin pretreatment reduces coagulation andplatelet activation during coronary dilation procedures.J Am Coll Cardiol1997;29:13–20.19. Bland MJ, Altman DG. Statistical method for assessing agreement betweentwo methods of clinical measurement.Lancet1986;1:307–309.20. McTavish D, Faulds D, Goa KL. Ticlopidine an up dated review of itspharmacology and therapeutic use in platelet dependent disorders.Drugs 1990;40:238–259.21. Harker LA, Bruno JJ. Ticlopidine’ s mechanism of action on human platelets.In: Hass WK, Easton JD, eds. Ticlopidine, Platelets and Vascular Disease. NewYork: Springer Verlag, 1991:41–51.22. Bazan JF. Structural design and molecular evolution of a cytokine receptorsuperfamily.Proc Natl Acad SCI USA1990;87:6934–6938.23. Edgington TS, Mackman N, Brand K, Ruff W. The structural biology ofexpression and function of tissue factor.Thromb Haemost1991;66:67–79.24. Pendurthi UR, Alok D, Rao LVM. Binding of factor VIIa to tissue factorinduces alterations in gene expression in human fibroblast cells: up-regulation ofpoly (A) polymerase.Proc Natl Acad Sci USA1997;94:12598–12603.
TABLE II Thrombin-Antithrombin Complexes
AnginaPectoris T No.
Before PTCA Soon After Dilation
Peripheral Vein Coronary Ostium Coronary Ostium Beyond Lesion
Unstable No T 20 38.63 6 10 34.3 6 9.5 15.53 6 5.3 15.11 6 7.1
Stable No T 20 7.99 6 2.7 10.9 6 6.2 5.73 6 3.1 6.56 6 3.2
Unstable 24 h T 20 11.91 6 3.2 11.9 6 7.1 7.90 6 3.1 11.52 6 3.5
Stable 24 h T 20 6.92 6 1.7 7.0 6 3.9 10.22 6 3.5 8.29 6 2.3
Unstable 48 h T 20 6.65 6 2.1 5.87 6 2.7 5.71 6 3.1 4.68 6 2.1
Stable 48 h T 20 3.91 6 0.7 3.61 6 1.7 3.51 6 1.2 3.92 6 1.7
Unstable 72 h T 20 4.40 6 1.5 4.45 6 2.3 3.35 6 1.1 3.25 6 1.5
Stable 72 h T 20 3.03 6 0.7 3.00 6 0.7 2.36 6 0.5 2.53 6 0.3
*p ,0.05 unstable versus stable; unstable versus stable; †p ,0.05; ‡p ,0.001; §p ,0.001.T 5 ticlopidine.
‡
†
§
§
§
*
‡
‡
‡
†
§
§
§
*
‡
‡
‡
‡
‡
§
§
§
NS
‡
‡
§
§
*
NS
‡
‡
‡
CORONARY ARTERY DISEASE/PLASMA TISSUE FACTOR IN UNSTABLE ANGINA 531







