Embed Size (px)
Citation preview

Effect of Donor JNK Signal Transduction Inhibitionon Transplant Outcome in Brain Dead Rat Model
Lu Chen,1 Danfeng Xu,1 Yi Gao,1 Xingang Cui,1 Zunguo Du,2 Qiang Ding,2 and XiangWang2,3
Abstract—Renal grafts from brain-dead donors compared to living donors have a significantlyshortened survival time due to heightened renal immunogenicity. The influence of pretreatmentwith a JNK signal transduction inhibitor on ischemia–reperfusion injury was examined in a renaltransplant model using donors from a standardized rat model of brain death. Donors were treatedimmediately after induction of brain death with a JNK signal transduction inhibitor or saline.Kidney grafts from experimental group and control groups (saline-treated brain dead or living donorgrafts) were examined serially up to 7 days post transplantation by morphology, immmunohistology,and real-time PCR. JNK inhibition reduced the intensity of ischemia–reperfusion injury and acuterejection compared to saline treated donors. Likewise, cellular infiltration, mRNA transcription ofsome representative proinflammatory mediators and MHC-II molecules in the grafts werediminished in the JNK-inhibited donors compared to saline controls. Lewis rats transplanted withkidneys from JNK inhibited, brain-dead BN donors survived significantly longer than rats transplantedwith saline treated brain-dead donors. The JNK inhibitor pretreatment of brain dead rats improveddonor kidney quality, and improved graft survival.
KEY WORDS: brain dead; kidney transplantation; JNK signal transduction; inflammation.
INTRODUCTION
Transplant outcome achieved with kidneys fromliving donors is superior when compared to kidneysobtained from brain-dead (BD) donors [1, 2], but amajority of the kidney grafts are still obtained from BDdonors. Studies have shown that the catastrophic injuryof brain death has detrimental effects on hemodynamicstability, hormone regulation, immunological activation,and renal structures [3–5].
The “autonomic storm” leads to peripheral vaso-constriction and organ hypoperfusion, followed byischemia–reperfusion (I/R) injury in the subsequent
transplanted kidney. In addition, the elevated levels ofproinflammatory cytokines and major histocompatibilitycomplex (MHC) class II are associated with an increasedrisk of acute rejection after transplantation [4, 6, 7].There is a consensus that reducing the hemodynamicinstability and immunogenicity of the donor kidney canimprove the transplant outcome.
c-Jun N-terminal kinase (JNK) is a serine threonineprotein kinase that plays a crucial role in regulating theprocess of hypoxia, ischemia–reperfusion, and T-cellactivation and differentiation. JNK belongs to themitogen-activated protein kinase family. SP600125 is apotent, cell-permeable, selective, and reversible inhibitorof JNK. It exhibits over 300-fold greater selectivity forJNK as compared to ERK1 and p38. SP600125 inhibitsthe phosphorylation of c-Jun, blocks the expression ofIL-2, IFN-γ, TNF-α, and cyclooxygenase (COX)-2, andprevents IL-1-induced accumulation of phosphor-c-Junand induction of c-Jun transcription [8]. SP600125treatment has reduced myocardial ischemia-reperfusioninjury and infarct size in vivo [9]. During islet isolationand transplantation, inhibition of JNK has prevented theimpairment of islet cells and improved outcomes after
1 Department of Urology, Changzheng Hospital, The Second MilitaryMedical University, 415 Fengyang Road, Shanghai, 200003, People’sRepublic of China
2 Department of Urology, Huashan Hospital, Fudan University, 12Wulumuqi Zhong Road, Shanghai, 200040, People’s Republic ofChina
3 To whom correspondence should be addressed at Department ofUrology, Huashan Hospital, Fudan University, 12 Wulumuqi ZhongRoad, Shanghai, 200040, People’s Republic of China. E-mail:[email protected]
0360-3997/12/0100-0122/0 # 2011 Springer Science+Business Media, LLC
Inflammation, Vol. 35, No. 1, February 2012 (# 2011)DOI: 10.1007/s10753-011-9296-6
122

pancreatic islet transplantation [10]. Additionally, someinvestigators demonstrated that the SP600125 inhibitsboth T-lymphocyte expansion in vitro and T-cell-medi-ated alloimmune responses in vivo during heterotopicheart transplantation [11]. Thus, we hypothesized thattherapeutic inhibition of JNK phosphorylation hassignificant potential in improving the quality of kidneygrafts from brain-dead donors. We have comparedSP600125 pretreated or saline pretreated BD donorkidneys to living donor grafts on renal transplantsurvival as well as downstream events in the JNKpathways.
MATERIALS AND METHODS
Animals and Operative Technique
Inbred adult (250–300 g) male Brown–Norway rats(BN) and Lewis rats (Chinese Academy of Sciences,China) acted as kidney donors and recipients, respec-tively. All animal care and surgical procedures wereperformed in accordance with the guidelines of theanimal care and use committee at Fudan University. Thegrafts were flushed with 3 ml of cold lactated Ringerssolution before removal and stored transiently in the coldsolution. The donor kidneys were transplanted heterotopi-cally to the recipient abdominal great vessels and ureterby end-to-end anastomoses using modified microsurgicaltechniques [12–17]. The bilateral native kidneys of therecipients were removed after transplantation.
Brain-Dead Model
Brain death was induced in anesthetized BN rats aspreviously described [18–21]. Briefly, a No. 3 Fogartycatheter balloon (Fogarty Arterial Embolectomy Cathe-ter: 3F, Edwards Lifesciences Co., USA) was introducedinto the intra-cranial cavity through a 1-mm burr hole.BD was induced by slow progressive inflation of theballoon which gradually raised intra-cranial BP. BN ratswere under continuous BP and electroencephalographicmonitoring. BD was confirmed by flat-line tracings,physical signs of apnea, areflexia, and maximally dilatedand fixed pupils. All rats were connected to a rodentrespirator and mechanically ventilated at a rate of85 breaths/min with a tidal volume of 2.0 ml for 6 h(Rodent ventilator, model DHX-150, Chengdu Instru-ments Co., China). BD rats that maintained a stablemean arterial blood pressure (MAP>80 mmHg) wereaccepted as donors in the study to avoid peripheral
ischemia secondary to hypotension. After 6 h, the leftkidney was removed for transplantation. Sham-operatedrats in which a burr hole was drilled but no catheter wasinserted served as living donor controls.
SP600125 Administration
SP600125 (Sigma-Aldrich Co., USA) was prepareddaily by dissolving in PPCES vehicle (30% polyethyleneglycol 400, 20% propylene glycol, 15% Cremophor EL,5% ethanol, 30% saline) [11]. The drug solution (2.5 mlper kg body weight which equals to 15 mg/kg SP600125)was administered subcutaneously (s.c.) to a rat.
Experimental Groups
Three groups were studied (n=30/group). One hourafter BD induction, group 1 BD donors were administeredSP600125 solution s.c. and Group 2 BD donors receivedphysiological saline subcutaneously for 5 h. Group 3 wereliving donors which were treated with physiological salines.c. for 5 h. The left kidneys of each group were removedand transplanted. Engrafted organs (n=6 animals/timeinterval/group) were removed and analyzed at 8 h, 24 h,3 days, and 7 days post-transplantation. The right kidneysof the donors were removed at the time of left kidneydonor acquisition and analyzed immediately (0 h, n=6). Inaddition, another six recipients were used for survivalestimates in each group. The graft survival time wasdefined from the date of transplantation to the time ofrenal failure secondary to complete and irreversiblerejection of allografts. Postoperative complications wereruled out by autopsy. The graft function was assessed byserum creatinine level. The creatinine level was measuredon serum samples taken everyday by use of the creatinineassay kit from Sigma Chemical Co. (St. Louis, MO). Therenal graft failure was determined when the serumcreatinine level reaches the reference value.
Histology
The grafts were removed 7 days post transplanta-tion and fixed by 10% neutral formalin. Paraffinembedding sections were stained with hematoxylin–eosin and examined by light microscope. Twentyconsecutive high power fields (×400 magnification)from six kidneys per group were evaluated. Morpho-metric analysis of leukocyte infiltration, tubular epithe-litis, and vasculitis were performed according to Banff97 classification [22]. The grade was scored on the basisof semi-quantitative assessment which had a scale of 0
123JNK Signal Transduction Inhibition in Brain Dead Rat Model

to 3 arbitrary units: 0 (none), 1 (mild change), 2(moderate change), 3 (intense change).
Immunohistology
Immunohistochemical studies were performed onparaffin-embedded sections using the avidin–biotincomplex (ABC) horseradish–peroxidase method. Pri-mary antibodies against the following antigens wereapplied according to the manufacturer’s guidelines(Dako, Glostrup, Denmark): Monoclonal antibodies(mAb; AbD Serotec), were directed against monocytes/macrophages, MHC class II antigens and phospho-c-Jun.The sections were then interacted with rabbit anti-mouseIgG after specific mAb staining.
The percentage and intensity of staining cellswithin 20 consecutive high power fields (×400 magni-fication) were evaluated in six kidneys/group andreported semi-quantitatively as 1 (percentage <30%), 2(percentage between 30% and 60%) or 3 (percentage>60%) and 1 (weak staining), 2 (moderate staining) or 3(strong staining), respectively. A score was calculated asfollows: score=sum of (1×the corresponding score ofpercentage of weak, 2×the corresponding score ofpercentage of moderate, and 3×the corresponding scoreof percentage of strong staining).
Real-Time PCR
Kidney grafts were removed, snap-frozen andstored at −80°C. Expression of IL-6, TNF-α and TGF-β mRNA in the grafts was determined by real-time PCRusing the ABI PRISM 7700 Sequence Detection System(Applied Biosystems, Foster City, CA, USA). TotalRNAwas extracted from kidney samples with Trizol andreverse transcribed into cDNA at 37°C for 15 min and at98°C for 5 min using the ReverTra Ace qPCR RT Kit(TOYOBO, Osaka, Japan) with 1 μg RNA [23].
Primers were designed by primer5.0 software andthe sequences were:
GAPDH, 5′-GCCTTCCGTGTTCCTACC-3′ and 5-GCCCCTCCTGTTGTTATG-3′;
IL-6, 5′-A41GCCACTGCCTTCCCTAC-3′ and 5′-TTGCCATTGCACAACTCTT-3′;
TNF-α, 5′-CCACGCTCTTCTGTCTACTG-3′ and 5′-GCTACGGGCTTGTCACTC-3′;
TGF-β, 5′-GCAACAACGCAATCTATGAC-3′ and 5′-CCCTGTATTCCGTCTCCTT-3′.
QPCR was performed in a two-step RT-PCR usingSYBR Green PCR Master Mix (TOYOBO) with 2 μl
cDNA and 0.3 μM of primers in a total reaction volumeof 50 μL. The PCR thermal cycle consisted of a 5-minincubation at 95°C and 40 amplification cycles (15 s at94°C, 15 s at 63°C, and 45 s at 72°C). The amplificationand data acquisition were run on the real-time PCRsystem (ABI Prism 7700, Applied Biosystems, FosterCity, CA, USA). All samples were normalized toexpression of GAPDH. The relative quantification valueis calculated by the formula 2−ΔCt.
Statistical Analysis
Numerical data are expressed as mean±standarddeviation (SD). For immunohistological parameters andreal-time PCR analysis, statistical analysis was per-formed using the Kruskal–Wallis test with option formultiple comparisons (stata 10.0). For light microscopyanalysis, Fisher’s exact test was used. For survivalanalysis, log-rank test were applied. A p value of lessthan 0.05 was considered significant.
RESULTS
Histology
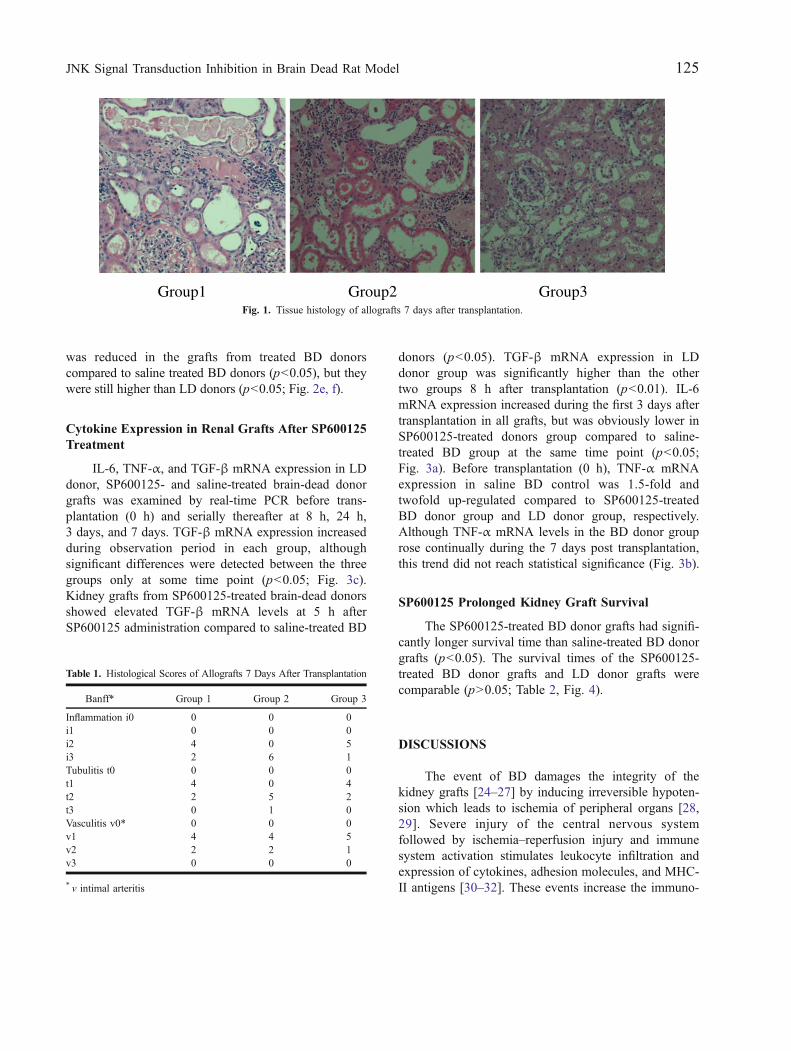
Saline-infused brain-dead donor grafts (group 2)showed significantly elevated interstitial inflammationand tubulitis (p<0.05), compared to grafts obtained fromSP600125-treated brain-dead donors (group 1) andliving donors (group 3). All the grafts in the threegroups displayed vasculitis and no statistical significance(p>0.05) was detected between treatments (Fig. 1,Table 1).
Immunohistology
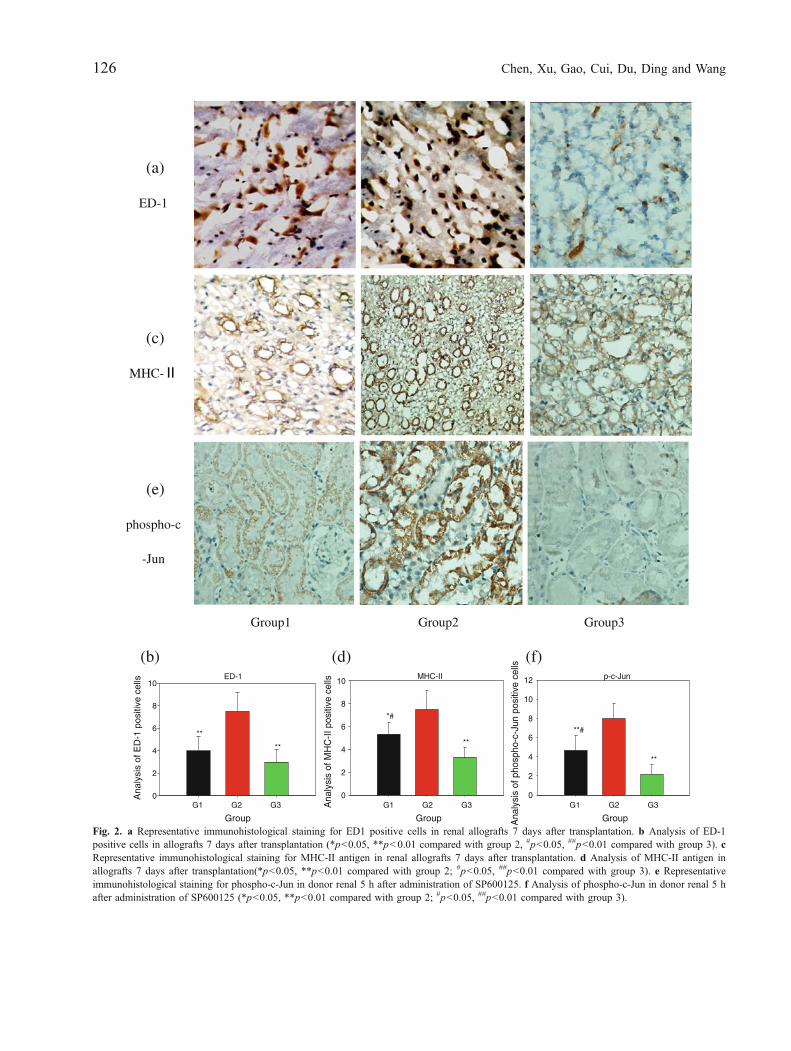
Reduced monocyte infiltration and MHC-II antigenexpression in renal grafts were observed from SP600125treated brain-dead donors. In agreement with thehistology, renal grafts of SP600125 treated BD donors(group 1) had significantly less ED-1 positive monocytesand MHC-II positive cells than saline-infused BDdonors (group 2; p<0.05).
SP600125 Inhibited JNK Signal TransductionEffectively
Donor kidneys were removed 5 h after adminis-tration of SP600125 subcutaneously. The extent of c-Junphosphorylation was examined with phospho-c-Junantibody. The number and intensity of labeled cells
124 Chen, Xu, Gao, Cui, Du, Ding and Wang
was reduced in the grafts from treated BD donorscompared to saline treated BD donors (p<0.05), but theywere still higher than LD donors (p<0.05; Fig. 2e, f).
Cytokine Expression in Renal Grafts After SP600125Treatment
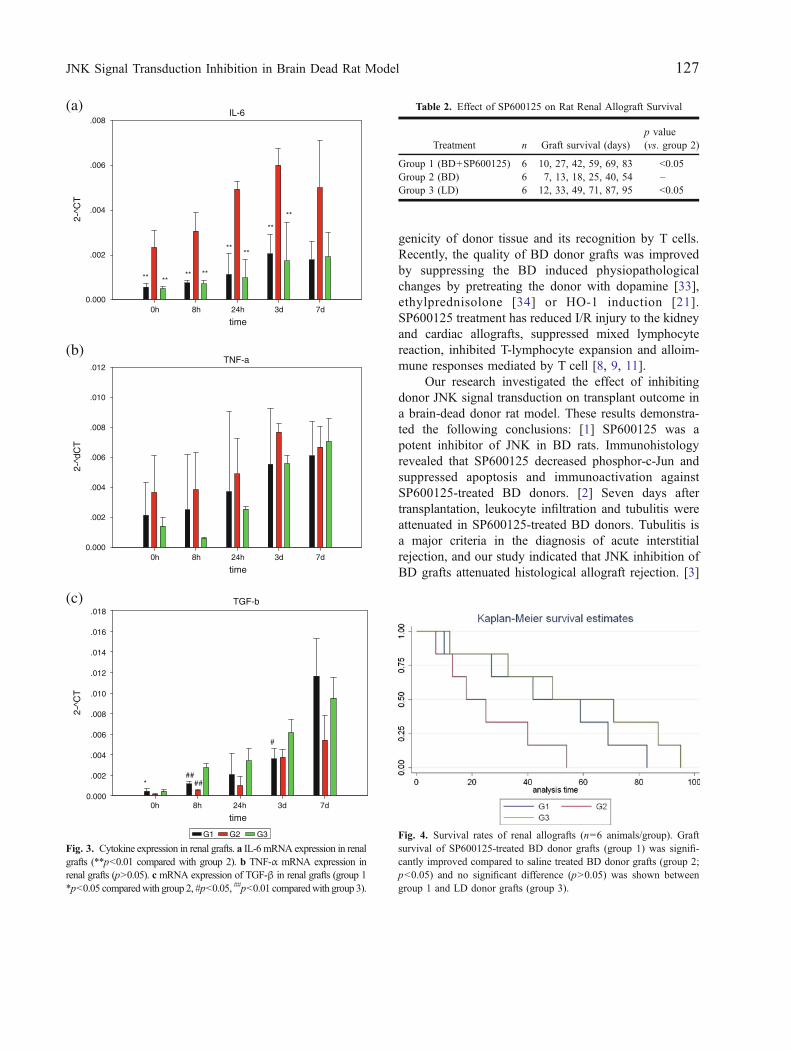
IL-6, TNF-α, and TGF-β mRNA expression in LDdonor, SP600125- and saline-treated brain-dead donorgrafts was examined by real-time PCR before trans-plantation (0 h) and serially thereafter at 8 h, 24 h,3 days, and 7 days. TGF-β mRNA expression increasedduring observation period in each group, althoughsignificant differences were detected between the threegroups only at some time point (p<0.05; Fig. 3c).Kidney grafts from SP600125-treated brain-dead donorsshowed elevated TGF-β mRNA levels at 5 h afterSP600125 administration compared to saline-treated BD
donors (p<0.05). TGF-β mRNA expression in LDdonor group was significantly higher than the othertwo groups 8 h after transplantation (p<0.01). IL-6mRNA expression increased during the first 3 days aftertransplantation in all grafts, but was obviously lower inSP600125-treated donors group compared to saline-treated BD group at the same time point (p<0.05;Fig. 3a). Before transplantation (0 h), TNF-α mRNAexpression in saline BD control was 1.5-fold andtwofold up-regulated compared to SP600125-treatedBD donor group and LD donor group, respectively.Although TNF-α mRNA levels in the BD donor grouprose continually during the 7 days post transplantation,this trend did not reach statistical significance (Fig. 3b).
SP600125 Prolonged Kidney Graft Survival
The SP600125-treated BD donor grafts had signifi-cantly longer survival time than saline-treated BD donorgrafts (p<0.05). The survival times of the SP600125-treated BD donor grafts and LD donor grafts werecomparable (p>0.05; Table 2, Fig. 4).
DISCUSSIONS
The event of BD damages the integrity of thekidney grafts [24–27] by inducing irreversible hypoten-sion which leads to ischemia of peripheral organs [28,29]. Severe injury of the central nervous systemfollowed by ischemia–reperfusion injury and immunesystem activation stimulates leukocyte infiltration andexpression of cytokines, adhesion molecules, and MHC-II antigens [30–32]. These events increase the immuno-
Group1 Group2 Group3Fig. 1. Tissue histology of allografts 7 days after transplantation.
Table 1. Histological Scores of Allografts 7 Days After Transplantation
Banff* Group 1 Group 2 Group 3
Inflammation i0 0 0 0i1 0 0 0i2 4 0 5i3 2 6 1Tubulitis t0 0 0 0t1 4 0 4t2 2 5 2t3 0 1 0Vasculitis v0* 0 0 0v1 4 4 5v2 2 2 1v3 0 0 0
* v intimal arteritis
125JNK Signal Transduction Inhibition in Brain Dead Rat Model
(a)
ED-1
(c)
MHC-
(e)
phospho-c
-Jun
Group1 Group2 Group3
(b) (d) (f)ED-1
Group
G1 G2 G3
Group
G1 G2 G3
Group
G1 G2 G3
Ana
lysi
s of
ED
-1 p
ositi
ve c
ells
0
2
4
6
8
10
**
**
MHC-II
Ana
lysi
s of
MH
C-I
I pos
itive
cel
ls
0
2
4
6
8
10
*#
**
p-c-Jun
Ana
lysi
s of
pho
spho
-c-J
un p
ositi
ve c
ells
0
2
4
6
8
10
12
**#
**
Fig. 2. a Representative immunohistological staining for ED1 positive cells in renal allografts 7 days after transplantation. b Analysis of ED-1positive cells in allografts 7 days after transplantation (*p<0.05, **p<0.01 compared with group 2, #p<0.05, ##p<0.01 compared with group 3). cRepresentative immunohistological staining for MHC-II antigen in renal allografts 7 days after transplantation. d Analysis of MHC-II antigen inallografts 7 days after transplantation(*p<0.05, **p<0.01 compared with group 2; #p<0.05, ##p<0.01 compared with group 3). e Representativeimmunohistological staining for phospho-c-Jun in donor renal 5 h after administration of SP600125. f Analysis of phospho-c-Jun in donor renal 5 hafter administration of SP600125 (*p<0.05, **p<0.01 compared with group 2; #p<0.05, ##p<0.01 compared with group 3).
126 Chen, Xu, Gao, Cui, Du, Ding and Wang
genicity of donor tissue and its recognition by T cells.Recently, the quality of BD donor grafts was improvedby suppressing the BD induced physiopathologicalchanges by pretreating the donor with dopamine [33],ethylprednisolone [34] or HO-1 induction [21].SP600125 treatment has reduced I/R injury to the kidneyand cardiac allografts, suppressed mixed lymphocytereaction, inhibited T-lymphocyte expansion and alloim-mune responses mediated by T cell [8, 9, 11].
Our research investigated the effect of inhibitingdonor JNK signal transduction on transplant outcome ina brain-dead donor rat model. These results demonstra-ted the following conclusions: [1] SP600125 was apotent inhibitor of JNK in BD rats. Immunohistologyrevealed that SP600125 decreased phosphor-c-Jun andsuppressed apoptosis and immunoactivation againstSP600125-treated BD donors. [2] Seven days aftertransplantation, leukocyte infiltration and tubulitis wereattenuated in SP600125-treated BD donors. Tubulitis isa major criteria in the diagnosis of acute interstitialrejection, and our study indicated that JNK inhibition ofBD grafts attenuated histological allograft rejection. [3]
(a)
(b)
(c)
IL-6
time0h 8h 24h 3d 7d
time0h 8h 24h 3d 7d
time0h 8h 24h 3d 7d
2-^C
T
0.000
.002
.004
.006
.008
G1 G2 G3
****** **
****
**
**
TNF-a
2-^d
CT
0.000
.002
.004
.006
.008
.010
.012
*##
##
#
TGF-b
2-^C
T
0.000
.002
.004
.006
.008
.010
.012
.014
.016
.018
Fig. 3. Cytokine expression in renal grafts. a IL-6 mRNA expression in renalgrafts (**p<0.01 compared with group 2). b TNF-α mRNA expression inrenal grafts (p>0.05). c mRNA expression of TGF-β in renal grafts (group 1*p<0.05 comparedwith group 2, #p<0.05, ##p<0.01 comparedwith group 3).
Table 2. Effect of SP600125 on Rat Renal Allograft Survival
Treatment n Graft survival (days)p value(vs. group 2)
Group 1 (BD+SP600125) 6 10, 27, 42, 59, 69, 83 <0.05Group 2 (BD) 6 7, 13, 18, 25, 40, 54 –Group 3 (LD) 6 12, 33, 49, 71, 87, 95 <0.05
Fig. 4. Survival rates of renal allografts (n=6 animals/group). Graftsurvival of SP600125-treated BD donor grafts (group 1) was signifi-cantly improved compared to saline treated BD donor grafts (group 2;p<0.05) and no significant difference (p>0.05) was shown betweengroup 1 and LD donor grafts (group 3).
127JNK Signal Transduction Inhibition in Brain Dead Rat Model

Monocyte infiltration and MHC-II antigen expressionwere significantly reduced in the SP600125-treateddonors. [4] Experiments showed a tendency for reducedIL-6 in dopamine or HO-1 induction pretreatment BDdonor grafts, but no statistical significance was detectedwhen compared to untreated donors [21, 33]. Our datashowed that SP600125-treated BD grafts reduced IL-6mRNA expression at most time points compared tosaline-treated BD group and this decline may haveplayed an important role in preventing graft rejection. Inagreement with a previous study [21], TNF-α mRNAexpression did not differ significantly between thetreated and saline treated group. [5] The Kaplan–Meiersurvival curve showed that the survival of SP600125-treated BD donor grafts was significantly longer comparedwith saline-treated BD donor grafts. Our data demonstratedthat SP600125 pretreatment prolonged BD donor renalallograft survival via inhibition of the JNK pathways.
As previously described [35], the quality of kidneygraft was improved by donor catecholamine treatment.In contrast, catecholamine treatment in liver transplanta-tion did not provide any significant benefit, and actuallyworsened the transplant outcome. Although our dataprovide evidence for the benefit of pretreatment with aJNK inhibitor on the renal BD donor graft and transplantoutcome, applicability of JNK inhibition pretreatment toother organs will require further studies.
REFERENCES
1. US Department of Health and Human Services. 2004 AnnualReport of the US Organ Procurement and Transplantation Networkand the Scientific Registry of Transplant Recipients: TransplantData 1994–2003, 2005.
2. Terasaki, P.I., J.M. Cecka, D.W. Gjertson, et al. 1995. Highsurvival rates of kidney transplants from spousal and livingunrelated donors. New Engl J Med 333: 333.
3. Herijgers, P., V. Leunens, T.B. Tjandra-Maga, et al. 1996. Changesin organ perfusion after brain death in the rat and its relation tocirculating catecholamines. Transplantation 62: 330.
4. van der Hoeven, J.A., G. Molema, G.J. Ter Horst, et al. 2003.Relationship between duration of brain death and hemodynamic(in) stability on progressive dysfunction and increased immuno-logic activation of donor kidneys. Kidney International 64:1874.
5. van den Eijnden, M.M., H.G. Leuvenink, P.J. Ottens, et al. 2003.Effect of brain death and non-heart-beating kidney donation onrenal function and injury: an assessment in the isolated perfused ratkidney. Experimental and Clinical Transplantation 1: 85.
6. Nijboer, W.N., T.A. Schuurs, J.A.B. van der Hoeven, et al. 2005.Effect of brain death on stress and inflammatory response in thehuman donor kidneys. Transplantation Proceedings 37: 367.
7. Nijboer, W.N., T.A. Schuurs, J.A. van der Hoeven, et al. 2004.Effect of brain death on gene expression and tissue activation inhuman donor kidneys. Transplantation 78: 978.
8. Bennett, B.L., D.T. Sasaki, B.W. Murray, et al. 2001. SP600125,an anthrapyrazolone inhibitor of Jun N-terminal kinase. PNAS 98:13681.
9. Milano, G., S. Morel, C. Bonny, et al. 2007. A peptide inhibitor ofc-Jun NH2-terminal kinase reduces myocardial ischemia-reperfusioninjury and infarct size in vivo. American Journal of Physiology. Heartand Circulatory Physiology 292: 1828.
10. Noguchi, H., S. Matsumoto, N. Kobayashi, et al. 2008. Effect ofJNK inhibitor during islet isolation and transplantation. Trans-plantation Proceedings 40: 379.
11. Tabata, A., M. Morikawa, M. Miyajima, et al. 2007. Suppression ofalloreactivity and allograft rejection by SP600125, a small moleculeinhibitor of c-Jun N-terminal kinase. Transplantation 83: 1358.
12. Schumacher, M., B.N. Van Vliet, and P. Ferrari. 2003. Kidneytransplantation in rats: an appraisal of surgical techniques andoutcome. Microsurgery 23: 387.
13. Lee, S. 1967. An improved technique of renal transplantation in therat. Surgery 61: 771.
14. Pahlavan, P.S., C. Smallegange, et al. 2006. Kidney transplantationprocedures in rats: assessments, complications, and management.Microsurgery 26: 404.
15. Pietsch, A.P., P.C. Nett, E. Klar, et al. 2005. A new modifiedtechnique of ureteroureterostomy in rat kidney transplantation.Transplantation Proceedings 37: 189.
16. Karatzas, T., S. Santiago, T. Xanthos, et al. 2007. An easy and safemodel of kidney transplantation in rats. Microsurgery 27: 668.
17. Martins, P.N. 2006. Kidney transplantation in the rat: A modifiedtechnique using hydrodissection. Microsurgery 26: 543.
18. Pratschke, J., P. Neuhaus, and S.G. Tullius. 2005. What can belearned from brain death models? Transplant International 18: 15.
19. Shivalkar, B., J. Van Loon, W. Wieland, et al. 1993. Variableeffects of explosive or gradual increase of intracranial pressure onmyocardial structure and function. Circulation 87: 230.
20. Pratschke, J., M.J. Wilhelm, M. Kusaka, et al. 2000. A model ofgradual onset brain death for transplant-associated studies in rats.Transplantation 69: 427.
21. Kotsch, K., M. Francuski, A. Pascher, et al. 2006. Improved long-term graft survival after HO-1 induction in brain-dead donors.American Journal of Transplantation 6: 477.
22. Solez, K., H. Benediktsson, T. Cavallo, et al. 1996. Report of theThird Banff Conference on Allograft Pathology (July 20–24, 1995)on classification and lesion scoring in renal allograft pathology.Transplantation Proceedings 28: 441.
23. Gasser, M., A.M. Waaga-Gasser, M.W. Grimm, M.R. Grimm, et al.2005. Selectin blockade plus therapy with low-dose sirolimus andcyclosporin A prevent brain death-induced renal allograft dysfunc-tion. Amer J of Transplantation 5: 662.
24. Pratschke, J., M.J. Wilhelm, M. Kusaka, et al. 2000. Acceleratedrejection of rat renal allografts from brain dead donors. Annals ofSurgery 232: 263.
25. Kusaka, M., J. Pratschke, M.J. Wilhelm, et al. 2000. Activation ofinflammatory mediators in rat renal isografts by donor brain death.Transplantation 69: 405.
26. van der Hoeven, J.A., S. Lindell, R. van Schilfgaarde, et al. 2001.Donor brain death reduces survival after transplantation in ratlivers preserved for 20 hr. Transplantation 72: 1632.
27. van der Hoeven, J.A., R.J. Ploeg, F. Postema, et al. 1999.Induction of organ dysfunction and up-regulation of inflammatorymarkers in the liver and kidneys of hypotensive brain dead rats: amodel to study marginal organ donors. Transplantation 68: 1884.
28. Mertes, P.M., K. El Abassi, Y. Jaboin, et al. 1994. Changes inhemodynamic and metabolic parameters following induced braindeath in the pig. Transplantation 58: 414.
29. Mertes, P.M., P. Burtin, J.P. Carteaux, et al. 1994. Changes inhemodynamic performance and oxygen consumption during braindeath in the pig. Transplantation Proceedings 26: 229.
128 Chen, Xu, Gao, Cui, Du, Ding and Wang

30. Toyama, H., M. Takada, Y. Suzuki, and Y. Kuroda. 2003. Braindeath-induced expression of ICAM-1 and VCAM-1 on rathepatocytes. Hepatogastroenterology 50: 1854.
31. Jassem, W., D.D. Koo, L. Cerundolo, M. Rela, N.D. Heaton, andS.V. Fuggle. 2003. Cadaveric versus living-donor livers: differ-ences in inflammatory markers after transplantation. Transplanta-tion 76: 1599.
32. Jassem, W., D.D. Koo, L. Cerundolo, M. Rela, et al. 2003.Leukocyte infiltration and inflammatory antigen expression incadaveric and living-donor livers before transplant. Transplanta-tion 75: 2001.
33. Hoeger, S., A. Reisenbuechler, U. Gottmann, et al. 2008. Donordopamine treatment in brain dead rats is associated with animprovement in renal function early after transplantation and areduction in renal inflammation. Transplant International 21: 1072.
34. Kotsch, K., F. Ulrich, A. Reutzel-Selke, et al. 2008. Methylpred-nisolone therapy in deceased donors reduces inflammation in thedonor liver and improves outcome after liver transplantation.Annals of Surgery 248: 1042.
35. Schnuelle, P., S. Berger, J. de Boer, et al. 2001. Effects ofcatecholamine application to brain-dead donors on graft survival insolid organ transplantation. Transplantation 72: 455.
129JNK Signal Transduction Inhibition in Brain Dead Rat Model



























