Embed Size (px)
Citation preview

ELSEVIER Diabetes Research and Clinical Practice 30 (1995) 37-42
Effect of eicosapentaenoic acid and docosahexaenoic acid on diabetic osteopenia
Yuya Yamada*a, Hisako Fushimi”, Toru Inouea, Yukiko Matsuyamaa, Masakuni Kameyamaa, Takeshi Minamib, Yuko Okazakib, Yasuhisa Noguchi”,
Toshio Kasamac ‘Department of Internal Medicine, Sumitomo Hospital, 5-2-2. Nakanoshima, Kita-ku. Osaka 530, Japan
bSchool of Pharmacology, Kinki University, Osaka, Japan ‘NOF Corporation, Tokyo, Japan
Received 13 March 1995; revision received 1 August 1995; accepted 24 August 1995
Abstract
To evaluate the effect of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), which are polyunsaturated fatty acids, on diabetic osteopenia, we measured the bone fragility in streptozotocin-induced diabetic rats. The fragility of femur was increased in diabetic rats, which was prevented in part by EPA or DHA. Moreover, EPA prevented osteopenia even in diabetic rats fed a low zinc feed, which was a potent accelerator of diabetic osteopenia. Plasma alka- line phosphatase activity and parathyroid hormone level showed no difference between the two groups of diabetic rats with or without EPA. Urinary excretion of calcium and phosphate was increased and plasma inorganic phosphate level was high in diabetic rats, suggesting severe mineral loss. In diabetic rats fed EPA, although urinary and plasma calcium levels did not change significantly, urinary phosphate excretion and plasma inorganic phosphate concentration were slightly lowered, which suggested that EPA may have an effect in suppressing phosphate release from bones in diabetic rats. These data suggest that EPA and DHA could be effective on diabetic osteopenia, but to elucidate the precise mechanisms, further examinations will be needed.
Keyworris: Eicosapentaenoic acid; Docosahexaenoic acid; Diabetic osteopenia; Bone fragility; Diabetic rat
1. Introduction
It has been reported that osteopenia is observed in humans and animals with diabetes mellitus [l-4]. We previously described that streptozo- to&-induced diabetic rats showed decreases in
l Corresponding author.
bone weight and length, and an increase in bone fragility, which resulted from osteopenia confirm- ed by microscopic examination [4]. The bone fragility was normalized by insulin treatment, and mild zinc deficiency exaggerated diabetic osteo- penia [4].
On the other hand, prostaglandins are reported to modulate bone metabolism [5-lo]. However,
0168-8227/95/!$.09.50 0 1995 Elsevier Science Ireland Ltd. All rights reserved SSDI 0168-8227(95)01139-5

38 Y. Yamadn et al. /Diabetes Research and Clinical Practice 30 (1995) 37-42
the mechanisms have not been understood clearly and the effects of prostaglandins on bone cells are still controversial. Earlier reports showed that pro- staglandins accelerated bone resorption [5,6] and recent reports showed that prostaglandins in- hibited osteoclastic bone resorption [7] and stimu- lated bone formation [8,9]. Thus, prostaglandins are reported to be a multifunctional regulator of bone function [lo].
Eicosapentaenoic acid (EPA, 205) and docosa- hexaenoic acid (DHA, 22:6) which belong in the class polyunsaturated fatty acids, o-3, may influ- ence prostaglandin metabolism and may have ef- fects on bone cells. It has been reported that EPA prevented the loss of bone osteoporotic changes in ovariectomized rats fed with a low calcium diet [l 11. Therefore, in this study, we evaluated the effect of EPA and DHA on bone fragility as an in- dicator of osteopenia in streptozotocin-induced diabetic rats with or without zinc deficiency.
2. MaterIaIa and methods
Male Wistar rats were used. Diabetes was in- duced by injections of 80 mgikg of streptozotocin into the tail vein of dweek-old rats. Control and diabetic rats were fed either a standard laboratory feed (5.2 mg zinc/100 g) or a zinc-deficient feed (0.16 mg zinc/100 g). Each group was further divided into three subgroups: with EPA (soybean oil, 5.4 g + EPA, 0.6 g/100 g); with DHA (soybean oil, 5.4 g + DHA, 0.6 g/100 g); and without EPA and DHA (soybean oil, 6 g/100 g). Finally, the rats were divided into 12 subgroups. Seven weeks after streptozotocin injection, the rats fed ad libitum were sacrificed and femur, plasma and urine were collected.
Bone fragility was measured using a Mosant Hardness Tester (2030-2 Kayagaki, Japan) as described previously [4], which measures the pres- sure (kg/cm2) necessary to break the femur bone by continuous compression. Plasma glucose con- centration was measured by the glucose oxidase method. Plasma total cholesterol and triglyceride levels were measured enzymatically. Plasma alka- line phosphatase activity was measured by the nitrophenol phosphate method, and alkaline phos- phatase isozyme was determined by electro-
phoresis with an alkaline phosphatase extracted from bone, liver and kidney of a rat as a standard. A bone sample was extracted with Triton X-100 and was lysed by sonication. Plasma parathyroid hormone (PTH) level was measured using an im- munoradiometric assay kit (Nippon Mediphysics, Japan) with a rat PTH [l-34] as a standard.
Statistical analysis was performed using Stu- dent’s t-test.
3. Results
3.1. Plasma glucose and lipi& (Table I) Plasma glucose concentration was markedly
higher in diabetic rats than those in controls. Plas- ma total cholesterol level was significantly higher in all diabetic groups in comparison with those in the corresponding control groups, and triglyceride level was also higher in most of the diabetic groups than in controls. Plasma triglyceride concentration was decreased in control rats with EPA and with DHA, while the change did not reach a significant level in diabetic rats.
3.2. Bone fragility (Table 2) In control rats fed either a standard or low zinc
feed, bone fragility was similar among three groups with or without polyunsaturated fatty acid administration. In diabetic rats, femur bone hard- ness was decreased to nearly half of that in con- trols. In diabetic rats fed a standard laboratory feed, bone hardness was significantly higher in both EPA and DHA groups than those without EPA and DHA. In diabetic rats fed a low zinc feed, bone hardness was also higher in rats with EPA in comparison to those without EPA and DHA, while it was unchanged in rats with DHA.
3.3. Ca, P, PTH and alkaline phosphatase (Table 3)
In rats with or without EPA, plasma and urinary calcium (Ca) and inorganic phosphate (P) concentrations, plasma PTH level and alkaline phosphatase activity were measured.
In diabetic rats, urinary Ca and P excretion was 4-5-fold greater, and plasma P level was higher than in controls, which suggested that a greater amount of Ca and P were released from the bone
Y. Yamaab et al. /Diabetes Research and Clinical Practice 30 (1995) 37-42 39
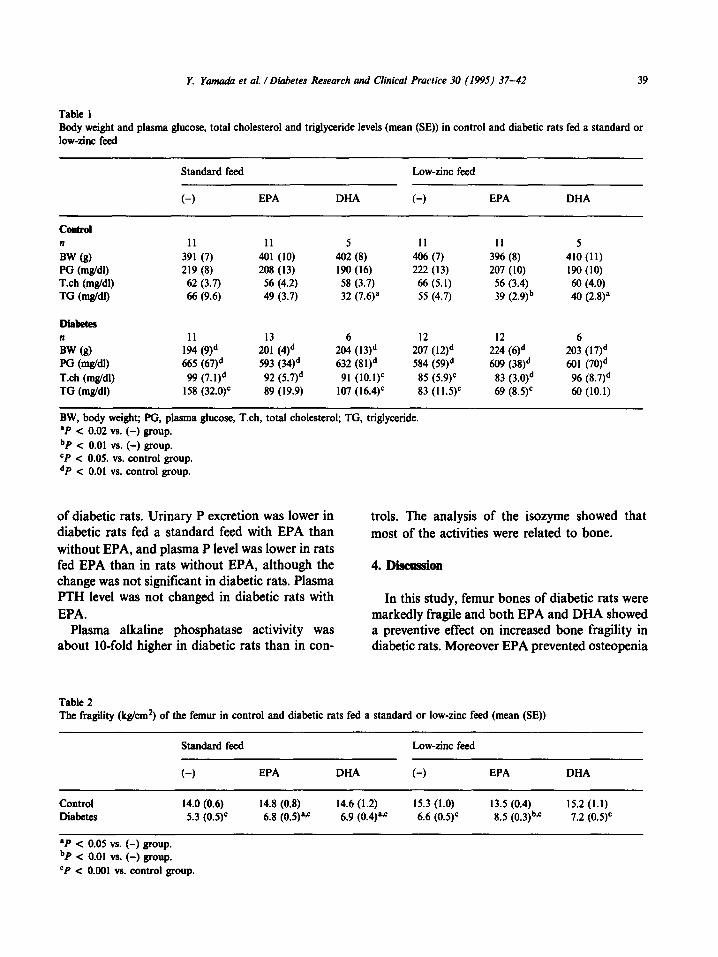
Table 1 Body weight and plasma ghtcosc, total cholesterol and triglyceride levels (mean (SE)) in control and diabetic rats fed a standard or low-zinc feed
COIlhI n BW (s) PG @u&W T.ch (mg/dl) TG (mg/dl)
Standard feed Low-zinc feed
(-) EPA DHA C-1 EPA DHA
11 11 5 II 11 5 391 (7) 401 (10) 402 (8) 406 (7) 396 (8) 410 (11) 219 (8) 208 (13) 190 (16) 222 (13) 207 (10) 190 (10) 62 (3.7) 56 (4.2) 58 (3.7) 66 (5.1) 56 (3.4) 60 (4.0) 66 (9.6) 49 (3.7) 32 (7.6)a 55 (4.7) 39 (2.9)b 40 (2.8)a
Diabetes n 11 6 12 12 6 BW (g) 194 (9)d
2:: (4)d 204 (13)d 207 (12)d 224 (6)d 203 (17)d
PG (m&W 665 (67)d 593 (34)d 632 (8 l)d 584 (59)d 609 (38)d 601 (70)d T.ch (mg/dl) 99 (7. I)d 92 (5.7)d 91 (10.1)’ 85 (5.9)c 83 (3.O)d 96 (8.7)d TG (mg/dl) 158 (32.0)’ 89 (19.9) 107 (16.4)c 83 (1 1.5)c 69 (8.5)’ 60 (10.1)
BW, body weight; PG, plasma ghtcose, Tch, total cholesterol; TG, triglyceride. .P < 0.02 vs. (-1 group. bP < 0.01 vs. (-) group. cP < 0.05. vs. control group. dP < 0.01 vs. control group.
of diabetic rats. Urinary P excretion was lower in diabetic rats fed a standard feed with EPA than without EPA, and plasma P level was lower in rats fed EPA than in rats without EPA, although the change was not significant in diabetic rats. Plasma PTH level was not changed in diabetic rats with EPA.
Plasma alkaline phosphatase activivity was about IO-fold higher in diabetic rats than in con-
trols. The analysis of the isozyme showed that most of the activities were related to bone.
4. Discussion
In this study, femur bones of diabetic rats were markedly fragile and both EPA and DHA showed a preventive effect on increased bone fragility in diabetic rats. Moreover EPA prevented osteopenia
Table 2 The fragility (k&m2) of the femur in control and diabetic rats fed a standard or low-zinc feed (mean (SE))
Standard feed Low-zinc feed
t-1 EPA DHA t-1 EPA DHA
Control 14.0 (0.6) 14.8 (0.8) 14.6 (1.2) 15.3 (1.0) 13.5 (0.4) 15.2 (1.1) Diabetes 5.3 (0.5)C 6.8 (0.5)a.c 6.9 (0.4)a” 6.6 (0.5)C 8.5 (0.3)b*c 7.2 (0.5)’
aP < 0.05 vs. (-) group. bP < 0.01 vs. (-) group. cP < 0.001 vs. control group.

Tabl
e 3
Plas
ma c
alci
um, i
norg
anic
pho
spha
te, a
lkal
ine
phos
phat
ase
and
para
thyr
oid
horm
one
leve
ls, a
nd u
rinar
y ex
cret
ion
of c
alci
um a
nd p
hosp
hate
in c
ontro
l an
d di
abet
ic
rats
with
or
with
out
eico
sape
ntae
noic
aci
d (m
ean
(SE
))
EPA
Con
trol
Dia
bete
s
Stan
dard
feed
Lo
w-z
inc
feed
St
anda
rd fe
ed
Low
-zin
c fe
ed
(-)
(+I
(-)
(+)
(-)
(+)
t-1
(+I
n 6
6 6
6 5
6 6
6
Ca
bW
102 (
0.7)
10
0 (1.
5)
I05
(2.6
) I0
5 (1
.7)
97 (2
.0)
100 (
1.2)
98
(2.1
) 99
(1.4
) p
wn4
I I
8 (2
.7)
I06
(2.8
)a
124 (
4.0)
I I
O (2
.3)s
17
0 (12
.6)d
14
7 (6.
8)d
I55
(4.3
)d
I40
(6.0
)d
ALP
(ILV
I) 25
3 (1
5)
292
(39)
23
7 (1
3)
194
(26)
23
84 (
275)
d 25
93 (
165
)d
1682
(180
)d
1999
(209
)d
PTH
@g/
N
27.9
(3.8
) 10
.9 (3
.2)b
47
.7 (6
.4)e
39
.2 (7
.4)’
31.3
(13.
6)
25.4
(6.8
) 30
.0 (7
. I)
24.7
(5.7
)
52 (3
.4)
139 (
12.2
)b
II6 (
12.2
)’ 84
(15.
2)e
298
(76)
c 64
0 (1
78)c
50
1 (6
2)d
546
(175
)’ 2.
5 (0
.3)
2.6
(0.4
) 2.
4 (0
.5 )
1.8
(0.2
) 19
.2 (2
.4)d
II.
9 (l.
l)“*d
10
.9 (l
.8)d
*e
10.0
(l.2)
d
EPA,
eic
osap
enta
enoi
c aci
d; A
LP,
alka
line
phos
phat
ase;
PTH
, pa
rath
yroi
d ho
rmon
e; C
r. cr
eatin
ine.
aP
< 0
.05
vs. (
-) g
roup
. bP
< 0
.01
vs. (
-) g
roup
. cP
< 0
.05
vs. c
ontro
l gro
up.
dP <
0.0
1 vs
. con
trol g
roup
. ‘P
< 0
.05
vs. s
tand
ard
feed
gro
up.
‘P <
0.0
1 vs
. sta
ndar
d fe
ed g
roup
.
Y. Yamadn et al. /Diabetes Research and Clinical Practice 30 (1995) 37-42 41
even in diabetic rats fed a low zinc feed, which was range. On the other hand, urinary excretion of P a potent accelerator of diabetic osteopenia [4]. was decreased significantly in diabetic rats fed a EPA and DHA are polyunsaturated fatty acids standard feed with EPA, and plasma P level was and are natural products in some foods such as lower in groups with EPA in comparison with fish. EPA is used as an antihyperlipidemic drug in groups without EPA, although the change of plas- Japan. Although data obtained from young rats ma P level was not significant in diabetic rats. with insulin-dependent diabetes mellitus are not These data suggest that EPA may prevent P release directly applied to human diabetics, EPA and from the bone. Though the decrease in P release DHA could be viable candidates as therapeutic from the bone alone does not result in the preven- agents for diabetic osteopenia in humans as they tion of osteopenia, it may be one of the effects of do not have any harmful side effects. EPA on bone metabolism.
The details of the mechanisms of EPA on bone metabolism are not clear. There was secondary hyperparathyroidism in control rats fed a low zinc feed, but not in diabetic rats and the difference of plasma PTH level was not significant between the groups with or without EPA. Bone turnover seem- ed to be higher in diabetic groups, but there was no difference with or without EPA, suggesting that the effect of EPA on bone metabolism was not through the enhancement of bone formation.
EPA or DHA lowered plasma triglyceride con- centrations in control rats. In diabetic rats, plasma triglyceride level was increased and EPA or DHA did not overcome hypertriglyceridemia because the dose used in this study was not sufficient to lower plasma triglyceride level. However, this small dose of fatty acids showed a preventive effect on osteopenia, suggesting that the decrease of plasma triglyceride levels was unlikely to explain the effect of EPA on bone metabolism.
We previously reported that microscopic exami- nation of ground cross-section of the tibia showed markedly thinner cortical bone in diabetic rats sec- ondary to mineral loss 141, a finding which is sup- ported by another report on human diabetics [ 121. In this study, urinary excretion of Ca and P was in- creased dramatically, and plasma P levels were higher in diabetic rats than in controls, suggesting that bone mineral was released and lost through urinary excretion in diabetic rats. If EPA or DHA reduces urinary mineral excretion, it could prevent diabetic osteopenia. Buck et al. reported that 24-h urinary Ca excretion was significantly decreased by EPA in experimental animals [ 131. In our study, the change in urinary Ca excretion was not signifi- cant between diabetic groups with or without EPA, although data were scattered in a wide
EPA and DHA may have an effect on bone metabolisms through prostaglandin metabolism. This is a possible mechanism of the effect of the n- 3 type of fatty acids on bone metabolism. The anti- aggregatory action of platelets by EPA is reported to be a competitive inhibitor of cyclooxygenase [14]. If this is the case in bone, EPA could inhibit prostanoid production from arachidonic acid, in- cluding prostaglandin Ez. On the other hand, EPA is a precursor for prostaglandin Es, which is reported, by Raisz et al., to stimulate bone resorp- tion as well as prostaglandin E, [ 151. They also reported that, however, EPA was a less effective precursor for bone-resorbing prostanoids than arachidonic acid in cultured rat bone [ 151. DHA may act like EPA as an n-3 type of fatty acid. Thus, the n-3 type of fatty acids could modulate prostaglandin metabolism in bone. However the role of prostaglandins on bone metabolism is com- plicated [5-lo] and local changes in prostanoid levels in bone are not clear. Sakaguchi et al. reported that EPA inhibited bone loss in ovariec- tomized rats with a low Ca diet [ 111. They sug- gested that the effect of EPA on osteoporosis was related to prostaglandin metabolism, but the precise mechanism was not clear. Further exami- nation is required for further understanding of the mechanisms.
References
[l] Levin, M.E., Boisseau, V.C. and Avioli, L.V. (1976) Ef- fects of diabetes mellitus on bone mass in juvenile and adult-onset diabetes. N. Engl. J. Med. 294, 241-245.
[2] McNair, P., Madsbad, S., Christiansen, C., Faber, O.K., Trasbol, I. and Binder, C. (1978) Oesteopenia in insulin- treated diabetes mellitus. Diabetologia 15, 87-90.
[3] Ho@, S., Avioli, L.V., Bergfeld, M. A., Fallon, M.D.,
42 Y. Yamada et al. /Diabetes Research and Clinical Practice 30 (1995) 37-42
Slatopolsky, E. and Teitelbaum, S.L. (1981) Correction of abnormal bone and mineral metabolism in chronic streptozotocin-induced diabetes mellitus in the rat by in- sulin therapy. Endocrinology 108, 2228-2234.
[4] Fushimi, H., Inoue, T., Yamada, Y., Horie, H., Kameyama, M., Inoue, K., Minami, T. et al. (1993) Zinc deficiency exaggerates diabetic osteoporosis. Diabetes Res. Clin. Prac. 20, 191-196.
[S] Klein, D.C. and Raisx, L.G. (1970) Prostaglandins: stim- ulation of bone resorption in tissue culture. Endocrin- ology 86, 1436-1440.
[6] Dietrich, J.W., Goodson, J.M. and Raisx, L.G. (1975) Stimulation of bone resorption by various prostagiandins in organ culture. Prostaglandins IO, 231-240.
[7] Chambers, T.J., McSheehy, P.M.J., Thompson, B.M. and Fuller, K. (1985) The effect of calcium-regulating hormones and prostaglandins on bone resorption by osteoclasts disaggregated from neonatal rabbit bones. Endocrinology 60, 234-239.
[8] Jee, W.S.S., Ueno, K., Kimmel, D.B. Woodbury, D.M., Price, P. and Woodbury, L.A. (1987) The role of bone cells in increasing metaphyseal hard tissue in rapidly growing rats treated with prostaglandin Ep Bone 8, 171-178.
[9] Marks, S.C. Jr. and Miller, S. (1988) Local infusion of prostaglandin Et stimulates mandibular bone formation in vivo. J. Oral Pathol. 17, 500-505.
[IO] Nagai, M. (1989) The effect of prostaglandin E, on DNA and collagen synthesis in osteoblasts in vitro. Calcif. Tissue Int. 44, 41 I-420.
[Ill Sakaguchi, K., Morita, I. and Murota, S. (1994) Eicosapentaenoic acid inhibits bone loss due to ovariec- tomy in rats. Prostaglandins Leukotriene Essential Fatty Acids 50, 81-84.
[I21 McNair, P., Madsbad, S., Christensen, M.S. et al. (1979) Bone mineral loss in insulin-treated diabetes mellitus: studies on pathogenesis. Acta Endocrinol. 90, 463-472.
[13] Buck, A.C., Davies, R.L. and Harrison, T. (1991) The protective role of eicosapentaenoic acid (EPA) in the pathogenesis of nephrolithiasis. J. Ural. 146, 188-194.
[14] Culp, B.R., Titus, B.G. and Lands, W.E.M. (1979) In- hibition of prostaglandin biosynthesis by eicosapen- taenoic acid. Prostaglandins Med. 3, 269-278.
[15] Raisx, L.G., Alander, C.B. and Simmons, H.A. (1989) Effects of prostaglandin E3 and eicosapentaenoic acid on rat bone in organ culture. Prostaglandins 37, 615-625.