Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Int J Clin Oncol (2009) 14:332–336 © The Japan Society of Clinical Oncology 2009DOI 10.1007/s10147-008-0871-2
S. Arai · H. Mitsufuji · Y. Nishii · S. Onoda · S. Ryuge · M. Wada · K. Katono · M. Iwasaki · A. Takakura · S. Otani · M. Yamamoto · T. Yanaihara · M. Yokoba · M. Kubota · M. Katagiri · T. Fukui · H. Kobayashi · N. Yanase · R. Hataishi · N. Masuda (*)Department of Respiratory Medicine, Kitasato University School of Medicine, 1-15-1 Kitasato, Sagamihara, Kanagawa 228-0022, JapanTel. +81-42-778-8111; Fax +81-42-778-6412e-mail: [email protected]
S. AraiDepartment of Respiratory Medicine, Kitasato Institute Medical Center Hospital, Kitamoto, Saitama, Japan
Susumu Arai · Hisashi Mitsufuji · Yasuto Nishii Sayaka Onoda · Shinichiro Ryuge · Mayuko Wada Ken Katono · Maiko Iwasaki · Akira Takakura Sakiko Otani · Michiko Yamamoto · Tomoko Yanaihara Masanori Yokoba · Masaru Kubota · Masato Katagiri Tomoya Fukui · Hirosuke Kobayashi · Nobuo Yanase Ryuji Hataishi · Noriyuki Masuda
Effect of gefi tinib on warfarin antithrombotic activity
Key words Gefi tinib · Warfarin · Drug interaction · Pro-thrombin time-international normalized ratio · Non-small cell lung cancer
Introduction
Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) represent a new treatment option for patients with advanced non-small cell lung cancer (NSCLC). Gefi -tinib is an orally active selective EGFR-TKI with the most extensive clinical experience, particularly in Japan.1 Gefi -tinib has shown excellent activity in heavily pretreated patients with NSCLC, with median survival times of 6.5–7.6 months and 1-year survival rates of 29%–35%.2,3 Although a large confi rmatory phase III trial of gefi tinib (IRESSA Survival Evaluation in Lung Cancer [ISEL]) in patients with pretreated NSCLC failed to show a signifi cant survival benefi t, a pre-planned subgroup analysis demonstrated a signifi cant survival advantage for gefi tinib compared with placebo in an Asian patient population.4 A second, larger, phase III trial (IRESSA NSCLC Trial Evaluating Response and Survival against Taxotere [INTEREST]) comparing gefi tinib with docetaxel in pretreated patients with advanced NSCLC has recently demonstrated that gefi tinib had statis-tically non-inferior survival compared to docetaxel.5
Many cancer patients have a hypercoagulable state, with recurrent thrombosis due to the impact of cancer cells and chemotherapy on the coagulation cascade; it is also known that the incidence of both atrial fi brillation and lung cancer increases with age.6,7 Warfarin is the treatment of choice for long-term oral anticoagulation in patients with these dis-eases, because other coumarins are poorly absorbed. Many drugs are known to alter the pharmacodynamic response to warfarin; these interactions place patients at risk for throm-botic or hemorrhagic events.8,9 However, there are few reports describing the interaction between cytotoxic anti-cancer agents and warfarin.10–13 Furthermore, it is not known whether there is an interaction between warfarin and the molecular target-based agent gefi tinib.
Received: August 13, 2008 / Accepted: December 17, 2008
AbstractBackground. Despite the literature indicating adverse inter-actions between warfarin and cytotoxic agents, whether such an interaction occurs when warfarin and gefi tinib are used concomitantly is unknown. We analyzed the preva-lence of the concomitant use of warfarin and gefi tinib, and the incidence of prothrombin time-international normal-ized ratio (PT-INR) alterations or adverse interactions in concomitant users of warfarin and gefi tinib.Methods. We conducted a retrospective study of patients with non-small cell lung cancer treated at the Kitasato University Hospital who received concomitant warfarin and gefi tinib between September 2002 and January 2007. Medical information, including the indication for warfarin use, warfarin dosing and dosing changes, and exposure to gefi tinib were collected from computerized databases and medical records.Results. Twelve (4.1%) of 296 patients treated with gefi -tinib received warfarin. PT-INR elevation occurred in 6 patients (50.0%). Two (16.7%) of the 12 patients had liver metastases. Liver dysfunction was associated with PT-INR elevation (P = 0.0100).Conclusion. As there is a possibility of PT-INR abnormali-ties occurring during the concomitant use of gefi tinib and warfarin, clinicians should be aware of this interaction. Because of the potentially severe consequences of this interaction, close monitoring of PT-INR and warfarin dose adjustment are recommended for patients receiving warfa-rin and gefi tinib, especially during the fi rst 2 weeks in the beginning of warfarin therapy.

333
In this study, we retrospectively analyzed the prevalence of the concomitant use of warfarin and gefi tinib, and the incidence of prothrombin time-international normalized ratio (PT-INR) alterations or adverse interactions, includ-ing bleeding, in patients with NSCLC. We also evaluated potential predictive factors to determine the effect on the PT-INR alteration in these patients. Here, we report the drug interaction between warfarin and gefi tinib that resulted in two patterns of response to warfarin.
Patients and methods
Study population
Using automated inpatient and outpatient pharmacy data-bases, we identifi ed all patients with NSCLC who had received at least one prescription for gefi tinib between Sep-tember 1, 2002, and January 31, 2007, at the Kitasato Uni-versity Hospital. The study population was limited to those individuals who received a prescription for gefi tinib along with a prescription for warfarin (regardless of which pre-scription came fi rst). In the medical records, information was obtained on the indication for warfarin use, warfarin dosing and dosing changes, exposure to gefi tinib, and all thrombotic or bleeding events. Information including age, sex, performance status (on the Eastern Cooperative Oncol-ogy Group [ECOG] scale), histologic subtype, clinical stage, site of metastases, biochemical data, and response to gefi -tinib was also obtained from the medical records. For each patient, an “index date” was identifi ed as the fi rst date at which gefi tinib and warfarin were co-prescribed, according to medical record abstraction.
Statistical analysis
The unpaired t-test or Fisher’s exact test was used to examine whether alterations in the prothrombin time-international normalized ratio (PT-INR) were associated with age, sex, smoking status, liver metastasis, performance status, liver dysfunction, and response to treatment, and P < 0.05 was considered to indicate statistical signifi cance.
Results
Two hundred and ninety-six patients who received a gefi -tinib prescription during the study period were identifi ed. According to medical record review, 12 patients were true concurrent users of warfarin and gefi tinib, of whom 2 patients have been reported previously.14
The characteristics of these 12 patients are shown in Table 1. Almost 75% of the patients were 60 years or older. Most patients were diagnosed with adenocarcinoma. All patients had stage IV disease. Two patients (17%) had liver metastases. Five (42%) patients had received warfarin for
deep vein thrombosis and 5 (42%) had received the drug for atrial fi brillation.
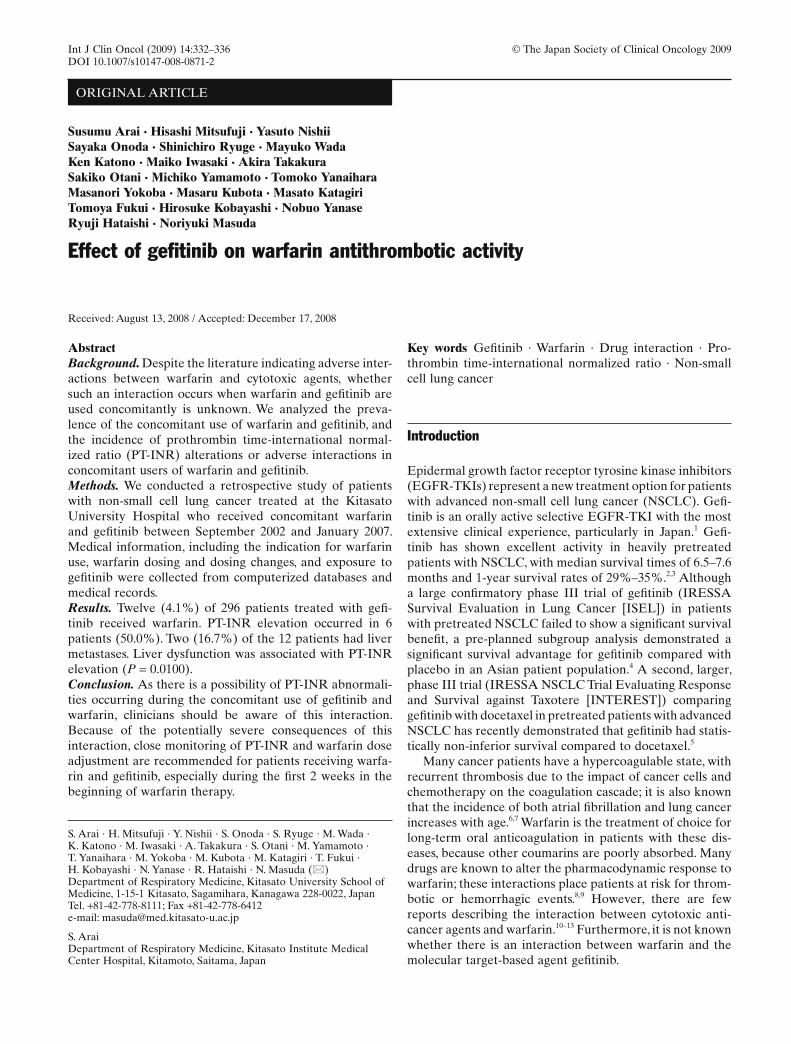
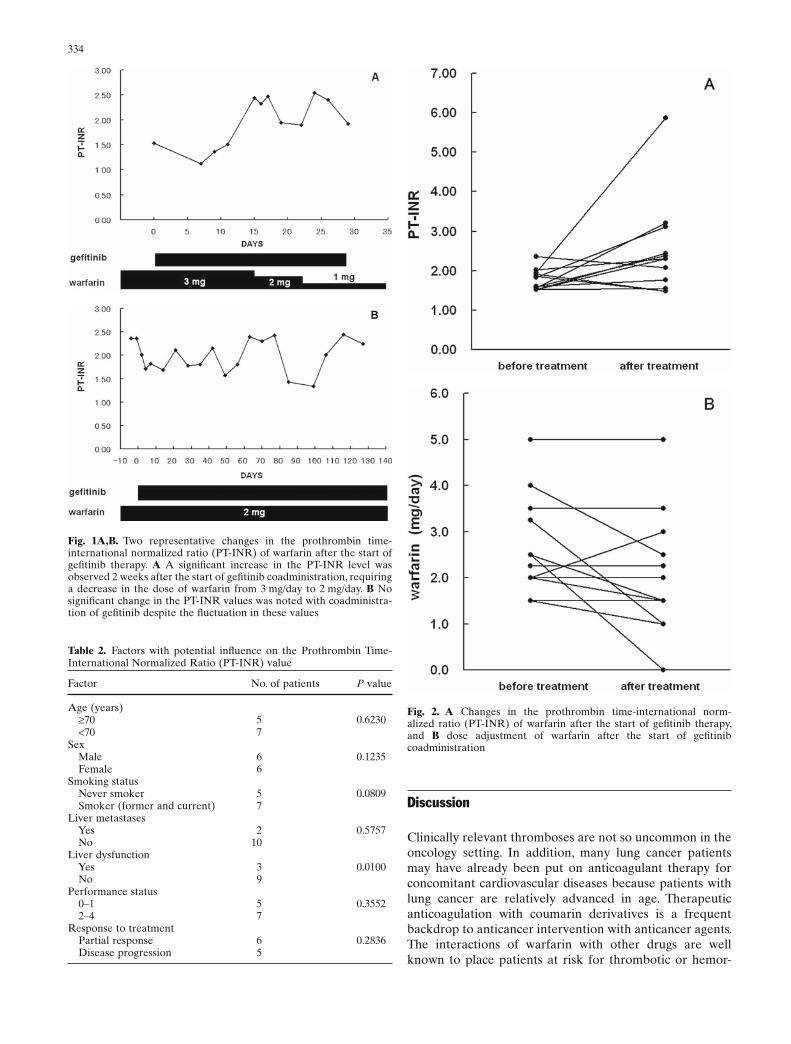
There were two patterns of change in the PT-INR values in the presence of combined gefi tinib and warfarin (Fig. 1). A signifi cant increase in PT-INR levels was observed in six patients (50%) within 2 weeks after the start of warfarin coadministration, requiring a decrease in the dose of war-farin (Figs. 1A and 2). However, neither epistaxis, hematu-ria, nor overt bleeding events occurred in these patients. We could not fi nd any prognostic factor associated with the PT-INR elevation. No relation was observed between liver metastases and the PT-INR elevation. Also, no signifi cant correlation of PT-INR elevation with diarrhea or mucositis was observed for these patients. No elevation in the PT-INR values was noted in six patients (50%; Figs. 1B and 2).
As shown in Table 2, of the seven factors examined for a potential infl uence on PT-INR values: age, sex, smoking status, liver metastasis, performance status, liver dysfunc-tion, and response to treatment, liver dysfunction was the only factor that was correlated with an increase in the PT-INR values (P = 0.0100).
Table 1. Characteristics of patients with non-small cell lung cancer
Age at beginning of gefi tinib therapy Mean, 67.0 years (range, 53–76 years)
Sex Male 6 Female 6Smoking status Never smoker 5 Former smoker 5 Current smoker 2Pathological type Adenocarcinoma 10 Squamous cell carcinoma 1 Large cell carcinoma 0 Others 1Stage IV 12Metastasis Lung 6 Bone 5 Brain 4 Liver 2 Adrenal gland 0Performance status 0 0 1 5 2 3 3 3 4 1Prior treatments Yes 7 Platinum-based 6 Non-platinum-based 1 No 5Underlying disease necessitating treatment with warfarin Deep vein thrombosis 5 Atrial fi brillation 5 Old myocardial infarction 1 Pulmonary embolism 1
334
Fig. 1A,B. Two representative changes in the prothrombin time-international normalized ratio (PT-INR) of warfarin after the start of gefi tinib therapy. A A signifi cant increase in the PT-INR level was observed 2 weeks after the start of gefi tinib coadministration, requiring a decrease in the dose of warfarin from 3 mg/day to 2 mg/day. B No signifi cant change in the PT-INR values was noted with coadministra-tion of gefi tinib despite the fl uctuation in these values
Fig. 2. A Changes in the prothrombin time-international norm-alized ratio (PT-INR) of warfarin after the start of gefi tinib therapy, and B dose adjustment of warfarin after the start of gefi tinib coadministration
Discussion
Clinically relevant thromboses are not so uncommon in the oncology setting. In addition, many lung cancer patients may have already been put on anticoagulant therapy for concomitant cardiovascular diseases because patients with lung cancer are relatively advanced in age. Therapeutic anticoagulation with coumarin derivatives is a frequent backdrop to anticancer intervention with anticancer agents. The interactions of warfarin with other drugs are well known to place patients at risk for thrombotic or hemor-
Table 2. Factors with potential infl uence on the Prothrombin Time-International Normalized Ratio (PT-INR) value
Factor No. of patients P value
Age (years) ≥70 5 0.6230 <70 7Sex Male 6 0.1235 Female 6Smoking status Never smoker 5 0.0809 Smoker (former and current) 7Liver metastases Yes 2 0.5757 No 10Liver dysfunction Yes 3 0.0100 No 9Performance status 0–1 5 0.3552 2–4 7Response to treatment Partial response 6 0.2836 Disease progression 5

335
rhagic events.8,9 The interaction between gefi tinib and war-farin is not an exception. We previously reported two cases of coadministration of warfarin and gefi tinib, indicating that one patient showed potentiation of the effect of warfarin with the simultaneous administration of gefi tinib, whereas the other patient did not.14 While this report may be infor-mative, information on the prevalence of coadministration of warfarin in patients receiving gefi tinib was not available. In the present study, 12 of 296 patients who fi lled a prescrip-tion for gefi tinib (4.1%) fi lled a prescription for warfarin. There were two patterns of response to warfarin in patients receiving gefi tinib and warfarin concurrently. In these 12 patients with concomitant use of the two agents, the PT-INR became elevated in 6 patients (50%), and it was not elevated in the other 6 patients (50%).
Warfarin is a racemic mixture of two optical isomers, enantiomers, R (+) and S (−) warfarin. These enantiomers are differently metabolized by human CYP isozymes. The three- to fi vefold more potent S (−) enantiomer of warfarin is metabolized mainly by CYP2C9 and has a shorter half-life, whereas the less active R (+) enantiomer is metabolized by CYP1A2, CYP3A4, and other isozymes.15 Gefi tinib is also extensively metabolized predominantly by CYP3A4. Because the R (+) enantiomer of warfarin and gefi tinib are metabolized by the same CYP isoenzyme, CYP3A4, there is a theoretical possibility that gefi tinib could compete with the less active isomer of warfarin. Furthermore, gefi tinib has been reported to have a weak inhibitory effect on CYP1A2, CYP2C9, and CYP3A4 activities.16 In some patients, gefi tinib could inhibit the metabolism of warfarin, which is a substrate of CYP1A2, CYP2C9, and CYP3A4. The degree of the inhibitory effect of gefi tinib on CYP enzymes varies from patient to patient. This may in part explain the variability of the PT-INR values observed on the coadministration of gefi tinib and warfarin. In addition, gefi tinib exhibits extensive binding to human plasma protein (approximately 97%) with little difference across species,17 and warfarin is also reported to be highly but reversibly bound (97%–99%) to albumin binding site I.18 Therefore, the unbound fraction of warfarin would be increased by displacement of the binding site caused by the coadminis-tration of gefi tinib. The elevated levels of unbound warfarin may potentiate hypoprothrombinemia, resulting in a rise in the PT-INR value. Gefi tinib causes asymptomatic increases in liver transaminases in approximately 20% of Japanese patients.2 This liver dysfunction may decrease the metabolic function of the CYP enzyme system, as well as decreasing the synthesis of clotting factors. Therefore, this hepatic tox-icity could also contribute to the elevated PT-INR values. A less likely alternative could be the following: because diarrhea is one of the major dose-limiting toxicities of gefi -tinib,2 gefi tinib-induced mucositis within the gastrointesti-nal tract may limit the intake and/or the absorption of vitamin K, increasing the sensitivity of patients to the vitamin K antagonist, warfarin.
The response rate to gefi tinib of 54.5% (6 of 11; Table 2) obtained in the present study appears to be superior to that reported for the single-agent activity of gefi tinib.2,3 At least, the coadministration of warfarin does not have a
detrimental effect on the antitumor activity of gefi tinib. However, this small study does not allow a precise estimate of the degree of the anticancer activity of gefi tinib when warfarin competes with gefi tinib on CYP3A4. Therefore, further studies of this drug interaction are needed to deter-mine whether the coadministration of gefi tinib and warfarin will affect the response rate and survival signifi cantly.
In conclusion, the results shown here, that 4.1% of gefi -tinib users treated at the Kitasato University Hospital fi lled a prescription for warfarin at the same time, indicate a not-so-low prevalence of concomitant gefi tinib and warfarin use; nearly 42% of the concomitant use was for deep vein thrombosis. In our series, there were two patterns of change in the PT-INR values in combined gefi tinib and warfarin users, and there was marked interindividual variability in the interaction. Clinicians should be aware of this interac-tion and should monitor closely PT-INR values in patients receiving gefi tinib and warfarin. Appropriate adjustment of the warfarin dose should be done if an altered response to warfarin is observed.
Confl ict of interest statement
No author has any confl ict of interest.
Acknowledgments We thank Mr. Yuichi Yonei for his help in the preparation of this manuscript.
References
1. Brown MC (1999) An adverse interaction between warfarin and 5-fl uorouracil: a case report and review of the literature. Chemo-therapy 45:392–395
2. Cohen MH, Williams GA, Sridhara R, et al. (2004) United States Food and Drug Administration Drug Approval summary: Gefi tinib (ZD1839; Iressa) tablets. Clin Cancer Res 10:1212–1218
3. Cropp JS, Bussey HI (1997) A review of enzyme induction of warfarin metabolism with recommendations for patient manage-ment. Pharmacotherapy 17:917–928
4. Douillard J-Y, Kim ES, Hirsh V, et al. (2007) Phase III, random-ized, open-label, parallel-group study of oral gefi tinib (IRESSA) versus intravenous docetaxel in patients with locally advanced or metastatic non small cell lung cancer who have previously received platinum-based chemotherapy (INTEREST). Eur J Cancer 43(Suppl 5):2
5. Fukuoka M, Yano S, Giaccone G, et al. (2003) Multi-institutional randomized phase II trial of gefi tinib for previously treated patients with advanced non-small-cell lung cancer (The IDEAL 1 Trial) [corrected]. J Clin Oncol 21:2237–2246
6. Hall G, Lind MJ, Huang M, et al. (1990) Intravenous infusions of ifosfamide/mesna and perturbation of warfarin anticoagulant control. Postgrad Med J 66:860–861
7. Kris MG, Natale RB, Herbst RS, et al. (2003) Effi cacy of gefi tinib, an inhibitor of the epidermal growth factor receptor tyrosine kinase, in symptomatic patients with non-small cell lung cancer: a randomized trial. JAMA 290:2149–2158
8. Le AT, Hasson NK, Lum BL (1997) Enhancement of warfarin response in a patient receiving etoposide and carboplatin chemo-therapy. Ann Pharmacother 31:1006–1008
9. Li J, Brahmer J, Messersmith W, et al. (2006) Binding of gefi tinib, an inhibitor of epidermal growth factor receptor-tyrosine kinase, to plasma proteins and blood cells: in vitro and in cancer patients. Invest New Drugs 24:291–297

336
10. Marshall J (2006) Clinical implications of the mechanism of epi-dermal growth factor receptor inhibitors. Cancer 107:1207–1218
11. Michalets EL (1998) Update: clinically signifi cant cytochrome P-450 drug interactions. Pharmacotherapy 18:84–112
12. Mousa SA (2006) Role of current and emerging antithrombotics in thrombosis and cancer. Drugs Today (Barc) 42:331–350
13. O’Reilly RA, Aggeler PM, Leong LS (1963) Studies on the cou-marin anticoagulant drugs: the pharmacodynamics of warfarin in man. J Clin Invest 42:1542–1551
14. Onoda S, Mitsufuji H, Yanase N, et al. (2005) Drug interaction between gefi tinib and warfarin. Jpn J Clin Oncol 35:478–482
15. Sallah S, Wan JY, Nguyen NP (2002) Venous thrombosis in patients with solid tumors: determination of frequency and char-acteristics. Thromb Haemost 87:575–579
16. Scarfe MA, Israel MK (1994) Possible drug interaction between warfarin and combination of levamisole and fl uorouracil. Ann Pharmacother 28:464–467
17. Serlin MJ, Breckenridge AM (1983) Drug interactions with warfa-rin. Drugs 25:610–620
18. Thatcher N, Chang A, Parikh P, et al. (2005) Gefi tinib plus best supportive care in previously treated patients with refractory advanced non-small-cell lung cancer: results from a randomised, placebo-controlled, multicentre study (Iressa Survival Evaluation in Lung Cancer). Lancet 366:1527–1537





























