Embed Size (px)
Citation preview

Original research article
Effect of Implanon� and Norplant� subdermal contraceptive implantson serum lipids—a randomized comparative study
Arijit Biswas*, Osborne A.C. Viegas, Asim C. RoyDepartment of Obstetrics and Gynaecology, National University Hospital, National University of Singapore, 5 Lower Kent Ridge Road, Singapore
Received 23 April 2003; received in revised form 29 May 2003; accepted 12 June 2003
Abstract
The objective of this study was to assess the possible differences in effects of Implanon� (etonogestrel 68 mg, single-rod) and Norplant�(levonorgestrel 36 mg, six capsules) implants on serum lipids over 2 years of use. In this 2-year open randomized study of 80 implantacceptors, selected serum lipids were tested before implant insertion and at 6, 12 and 24 months after implant insertion. The lipid parametersevaluated were: total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C),triglycerides, apolipoprotein A-I and apolipoprotein B. During the 2 years, the serum lipid pattern in the Implanon users was not significantlydifferent from that of the Norplant users. There was slight decrease in HDL-C levels in both the groups but there were no significant changesin the HDL/TC ratio and the HDL/LDL ratio. Although it was statistically significant, the magnitude of decrease in HDL-C from preinsertionlevels in Implanon users was only 5.8% at the end of 2 years. © 2003 Elsevier Inc. All rights reserved.
Keywords: Implanon; Etonogestrel; 3-Ketodesogestrel; Implants; Progestins; Lipid metabolism
1. Introduction
Implanon� (NV Organon, Oss, The Netherlands) is anew single-rod subdermal contraceptive implant that re-leases etonogestrel, the biologically active metabolite ofdesogestrel. It provides contraceptive protection for 3 yearsand has been approved for use in many countries around theworld. Implanon, being a single-rod system, has a simplerinsertion and removal procedure. Prior to Implanon, theonly other widely marketed implants were the levonorg-estrel-releasing six-capsule system, Norplant, and the 2-rodsystem, Jadelle. The safety and efficacy of the levonorg-estrel-releasing implants are well established.
We have previously reported on the effects of the Impl-anon implant on carbohydrate metabolism, thyroid and ad-renal function [1,2]. The objective of the present paper wasto assess the possible differences in effects of this newimplant system, Implanon, as compared to Norplant onselected serum lipid parameters.
2. Materials and methods
Eighty volunteers were recruited for the study. The vol-unteers were randomized to receive either Implanon orNorplant implants, with 40 subjects in each arm of thestudy. The study period was 24 months. The sizes of thestudy and control groups are based upon the recommenda-tions made by the World Health Organization for metabolicstudies, viz., 40 subjects per group [3].
The women included in the study were aged between 18and 40 years, were sexually active and of childbearingpotential. They had normal menstrual cycles with a meanlength of between 24 and 35 days and an intra-individualvariation of �3 days. They were deemed to have goodphysical and mental health, without contraindications to theuse of contraceptive steroids.
Fasting blood samples were drawn prior to the insertionof the implant and after 6, 12 and 24 months of use. Thesamples were obtained from the antecubital vein contralat-eral to the arm in which the implant or implants wereinserted. The sera obtained were stored frozen in aliquotsfor the biochemical tests. The lipid parameters evaluatedwere: total cholesterol (TC), high-density lipoprotein cho-lesterol (HDL-C), low-density lipoprotein cholesterol(LDL-C), triglycerides (TG), apolipoprotein A-I (Apo A-I)
* Corresponding author. Tel.:�65-772-4261; fax:�65-779-4753.E-mail address: [email protected] (A. Biswas).
Contraception 68 (2003) 189–193
0010-7824/03/$ – see front matter © 2003 Elsevier Inc. All rights reserved.doi:10.1016/S0010-7824(03)00145-8
and apolipoprotein B (Apo B). These were estimated in eachsample of blood.
Total cholesterol, HDL-C and triglycerides were mea-sured by spectrophotometric analysis using a multipurposeautoanalyzer, Cobas Mira Plus (Roche Diagnostic Systems,Basel, Switzerland). The kits used were from BoehringerMannheim. LDL-C was calculated using the formula:LDL-C � TC � (HDL-C � TG/2.19) mmol/L [4]. Theapolipoproteins (Apo A-I and Apo B) were measured by animmunoturbidimetric method using Cobas Mira Plus auto-analyzer. The kits used were from Boehringer Mannheim.The ratios HDL-C/LDL-C, HDL-C/TC and Apo A-I/Apo Bwere calculated.
2.1. Statistical methods
In each treatment group, comparison of changes frombaseline was performed for each assessment and for the lastmeasurement using the Wilcoxon matched-pairs signed-rank test. Mann-Whitney U-test was used for between-group comparisons of means.
3. Results
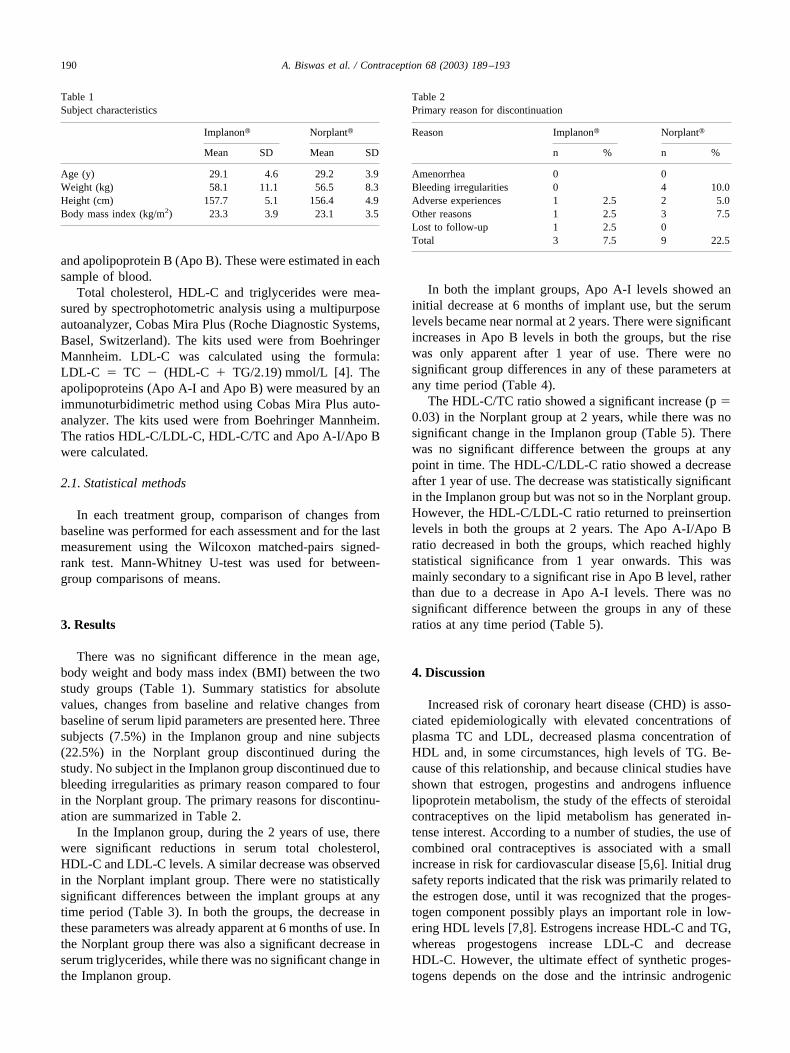
There was no significant difference in the mean age,body weight and body mass index (BMI) between the twostudy groups (Table 1). Summary statistics for absolutevalues, changes from baseline and relative changes frombaseline of serum lipid parameters are presented here. Threesubjects (7.5%) in the Implanon group and nine subjects(22.5%) in the Norplant group discontinued during thestudy. No subject in the Implanon group discontinued due tobleeding irregularities as primary reason compared to fourin the Norplant group. The primary reasons for discontinu-ation are summarized in Table 2.
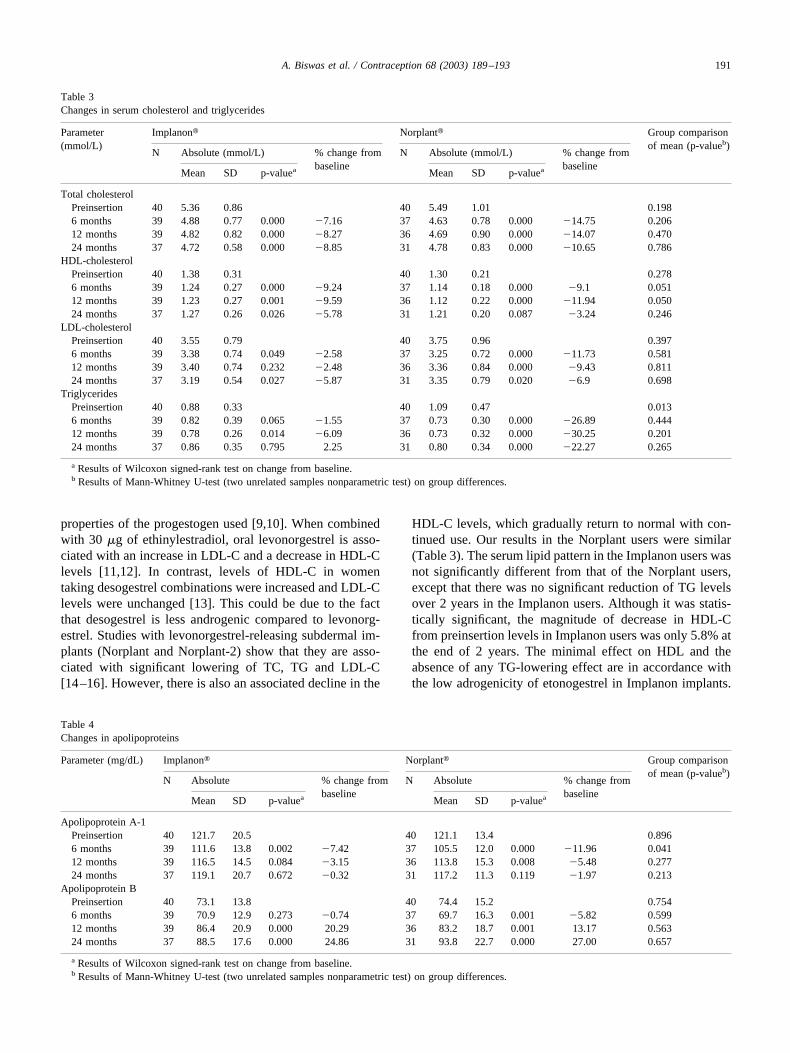
In the Implanon group, during the 2 years of use, therewere significant reductions in serum total cholesterol,HDL-C and LDL-C levels. A similar decrease was observedin the Norplant implant group. There were no statisticallysignificant differences between the implant groups at anytime period (Table 3). In both the groups, the decrease inthese parameters was already apparent at 6 months of use. Inthe Norplant group there was also a significant decrease inserum triglycerides, while there was no significant change inthe Implanon group.
In both the implant groups, Apo A-I levels showed aninitial decrease at 6 months of implant use, but the serumlevels became near normal at 2 years. There were significantincreases in Apo B levels in both the groups, but the risewas only apparent after 1 year of use. There were nosignificant group differences in any of these parameters atany time period (Table 4).
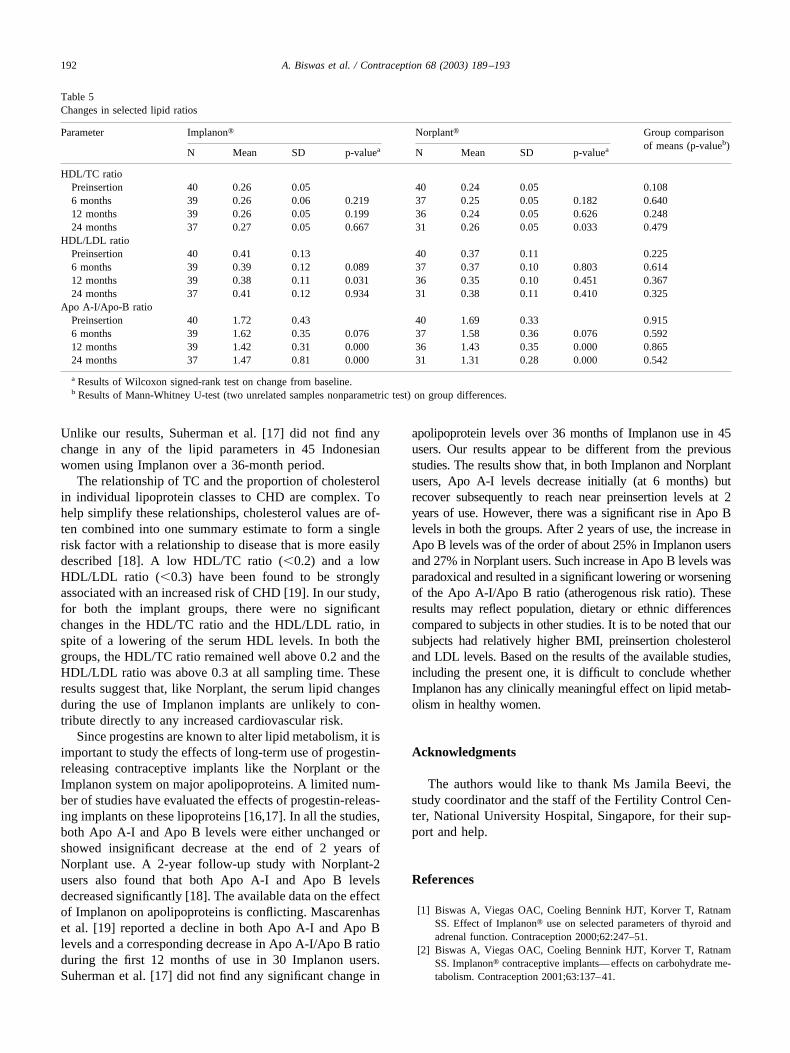
The HDL-C/TC ratio showed a significant increase (p �0.03) in the Norplant group at 2 years, while there was nosignificant change in the Implanon group (Table 5). Therewas no significant difference between the groups at anypoint in time. The HDL-C/LDL-C ratio showed a decreaseafter 1 year of use. The decrease was statistically significantin the Implanon group but was not so in the Norplant group.However, the HDL-C/LDL-C ratio returned to preinsertionlevels in both the groups at 2 years. The Apo A-I/Apo Bratio decreased in both the groups, which reached highlystatistical significance from 1 year onwards. This wasmainly secondary to a significant rise in Apo B level, ratherthan due to a decrease in Apo A-I levels. There was nosignificant difference between the groups in any of theseratios at any time period (Table 5).
4. Discussion
Increased risk of coronary heart disease (CHD) is asso-ciated epidemiologically with elevated concentrations ofplasma TC and LDL, decreased plasma concentration ofHDL and, in some circumstances, high levels of TG. Be-cause of this relationship, and because clinical studies haveshown that estrogen, progestins and androgens influencelipoprotein metabolism, the study of the effects of steroidalcontraceptives on the lipid metabolism has generated in-tense interest. According to a number of studies, the use ofcombined oral contraceptives is associated with a smallincrease in risk for cardiovascular disease [5,6]. Initial drugsafety reports indicated that the risk was primarily related tothe estrogen dose, until it was recognized that the proges-togen component possibly plays an important role in low-ering HDL levels [7,8]. Estrogens increase HDL-C and TG,whereas progestogens increase LDL-C and decreaseHDL-C. However, the ultimate effect of synthetic proges-togens depends on the dose and the intrinsic androgenic
Table 1Subject characteristics
Implanon� Norplant�
Mean SD Mean SD
Age (y) 29.1 4.6 29.2 3.9Weight (kg) 58.1 11.1 56.5 8.3Height (cm) 157.7 5.1 156.4 4.9Body mass index (kg/m2) 23.3 3.9 23.1 3.5
Table 2Primary reason for discontinuation
Reason Implanon� Norplant�
n % n %
Amenorrhea 0 0Bleeding irregularities 0 4 10.0Adverse experiences 1 2.5 2 5.0Other reasons 1 2.5 3 7.5Lost to follow-up 1 2.5 0Total 3 7.5 9 22.5
190 A. Biswas et al. / Contraception 68 (2003) 189–193
properties of the progestogen used [9,10]. When combinedwith 30 �g of ethinylestradiol, oral levonorgestrel is asso-ciated with an increase in LDL-C and a decrease in HDL-Clevels [11,12]. In contrast, levels of HDL-C in womentaking desogestrel combinations were increased and LDL-Clevels were unchanged [13]. This could be due to the factthat desogestrel is less androgenic compared to levonorg-estrel. Studies with levonorgestrel-releasing subdermal im-plants (Norplant and Norplant-2) show that they are asso-ciated with significant lowering of TC, TG and LDL-C[14–16]. However, there is also an associated decline in the
HDL-C levels, which gradually return to normal with con-tinued use. Our results in the Norplant users were similar(Table 3). The serum lipid pattern in the Implanon users wasnot significantly different from that of the Norplant users,except that there was no significant reduction of TG levelsover 2 years in the Implanon users. Although it was statis-tically significant, the magnitude of decrease in HDL-Cfrom preinsertion levels in Implanon users was only 5.8% atthe end of 2 years. The minimal effect on HDL and theabsence of any TG-lowering effect are in accordance withthe low adrogenicity of etonogestrel in Implanon implants.
Table 3Changes in serum cholesterol and triglycerides
Parameter(mmol/L)
Implanon� Norplant� Group comparisonof mean (p-valueb)
N Absolute (mmol/L) % change frombaseline
N Absolute (mmol/L) % change frombaseline
Mean SD p-valuea Mean SD p-valuea
Total cholesterolPreinsertion 40 5.36 0.86 40 5.49 1.01 0.1986 months 39 4.88 0.77 0.000 �7.16 37 4.63 0.78 0.000 �14.75 0.20612 months 39 4.82 0.82 0.000 �8.27 36 4.69 0.90 0.000 �14.07 0.47024 months 37 4.72 0.58 0.000 �8.85 31 4.78 0.83 0.000 �10.65 0.786
HDL-cholesterolPreinsertion 40 1.38 0.31 40 1.30 0.21 0.2786 months 39 1.24 0.27 0.000 �9.24 37 1.14 0.18 0.000 �9.1 0.05112 months 39 1.23 0.27 0.001 �9.59 36 1.12 0.22 0.000 �11.94 0.05024 months 37 1.27 0.26 0.026 �5.78 31 1.21 0.20 0.087 �3.24 0.246
LDL-cholesterolPreinsertion 40 3.55 0.79 40 3.75 0.96 0.3976 months 39 3.38 0.74 0.049 �2.58 37 3.25 0.72 0.000 �11.73 0.58112 months 39 3.40 0.74 0.232 �2.48 36 3.36 0.84 0.000 �9.43 0.81124 months 37 3.19 0.54 0.027 �5.87 31 3.35 0.79 0.020 �6.9 0.698
TriglyceridesPreinsertion 40 0.88 0.33 40 1.09 0.47 0.0136 months 39 0.82 0.39 0.065 �1.55 37 0.73 0.30 0.000 �26.89 0.44412 months 39 0.78 0.26 0.014 �6.09 36 0.73 0.32 0.000 �30.25 0.20124 months 37 0.86 0.35 0.795 2.25 31 0.80 0.34 0.000 �22.27 0.265
a Results of Wilcoxon signed-rank test on change from baseline.b Results of Mann-Whitney U-test (two unrelated samples nonparametric test) on group differences.
Table 4Changes in apolipoproteins
Parameter (mg/dL) Implanon� Norplant� Group comparisonof mean (p-valueb)
N Absolute % change frombaseline
N Absolute % change frombaseline
Mean SD p-valuea Mean SD p-valuea
Apolipoprotein A-1Preinsertion 40 121.7 20.5 40 121.1 13.4 0.8966 months 39 111.6 13.8 0.002 �7.42 37 105.5 12.0 0.000 �11.96 0.04112 months 39 116.5 14.5 0.084 �3.15 36 113.8 15.3 0.008 �5.48 0.27724 months 37 119.1 20.7 0.672 �0.32 31 117.2 11.3 0.119 �1.97 0.213
Apolipoprotein BPreinsertion 40 73.1 13.8 40 74.4 15.2 0.7546 months 39 70.9 12.9 0.273 �0.74 37 69.7 16.3 0.001 �5.82 0.59912 months 39 86.4 20.9 0.000 20.29 36 83.2 18.7 0.001 13.17 0.56324 months 37 88.5 17.6 0.000 24.86 31 93.8 22.7 0.000 27.00 0.657
a Results of Wilcoxon signed-rank test on change from baseline.b Results of Mann-Whitney U-test (two unrelated samples nonparametric test) on group differences.
191A. Biswas et al. / Contraception 68 (2003) 189–193
Unlike our results, Suherman et al. [17] did not find anychange in any of the lipid parameters in 45 Indonesianwomen using Implanon over a 36-month period.
The relationship of TC and the proportion of cholesterolin individual lipoprotein classes to CHD are complex. Tohelp simplify these relationships, cholesterol values are of-ten combined into one summary estimate to form a singlerisk factor with a relationship to disease that is more easilydescribed [18]. A low HDL/TC ratio (�0.2) and a lowHDL/LDL ratio (�0.3) have been found to be stronglyassociated with an increased risk of CHD [19]. In our study,for both the implant groups, there were no significantchanges in the HDL/TC ratio and the HDL/LDL ratio, inspite of a lowering of the serum HDL levels. In both thegroups, the HDL/TC ratio remained well above 0.2 and theHDL/LDL ratio was above 0.3 at all sampling time. Theseresults suggest that, like Norplant, the serum lipid changesduring the use of Implanon implants are unlikely to con-tribute directly to any increased cardiovascular risk.
Since progestins are known to alter lipid metabolism, it isimportant to study the effects of long-term use of progestin-releasing contraceptive implants like the Norplant or theImplanon system on major apolipoproteins. A limited num-ber of studies have evaluated the effects of progestin-releas-ing implants on these lipoproteins [16,17]. In all the studies,both Apo A-I and Apo B levels were either unchanged orshowed insignificant decrease at the end of 2 years ofNorplant use. A 2-year follow-up study with Norplant-2users also found that both Apo A-I and Apo B levelsdecreased significantly [18]. The available data on the effectof Implanon on apolipoproteins is conflicting. Mascarenhaset al. [19] reported a decline in both Apo A-I and Apo Blevels and a corresponding decrease in Apo A-I/Apo B ratioduring the first 12 months of use in 30 Implanon users.Suherman et al. [17] did not find any significant change in
apolipoprotein levels over 36 months of Implanon use in 45users. Our results appear to be different from the previousstudies. The results show that, in both Implanon and Norplantusers, Apo A-I levels decrease initially (at 6 months) butrecover subsequently to reach near preinsertion levels at 2years of use. However, there was a significant rise in Apo Blevels in both the groups. After 2 years of use, the increase inApo B levels was of the order of about 25% in Implanon usersand 27% in Norplant users. Such increase in Apo B levels wasparadoxical and resulted in a significant lowering or worseningof the Apo A-I/Apo B ratio (atherogenous risk ratio). Theseresults may reflect population, dietary or ethnic differencescompared to subjects in other studies. It is to be noted that oursubjects had relatively higher BMI, preinsertion cholesteroland LDL levels. Based on the results of the available studies,including the present one, it is difficult to conclude whetherImplanon has any clinically meaningful effect on lipid metab-olism in healthy women.
Acknowledgments
The authors would like to thank Ms Jamila Beevi, thestudy coordinator and the staff of the Fertility Control Cen-ter, National University Hospital, Singapore, for their sup-port and help.
References
[1] Biswas A, Viegas OAC, Coeling Bennink HJT, Korver T, RatnamSS. Effect of Implanon� use on selected parameters of thyroid andadrenal function. Contraception 2000;62:247–51.
[2] Biswas A, Viegas OAC, Coeling Bennink HJT, Korver T, RatnamSS. Implanon� contraceptive implants—effects on carbohydrate me-tabolism. Contraception 2001;63:137–41.
Table 5Changes in selected lipid ratios
Parameter Implanon� Norplant� Group comparisonof means (p-valueb)
N Mean SD p-valuea N Mean SD p-valuea
HDL/TC ratioPreinsertion 40 0.26 0.05 40 0.24 0.05 0.1086 months 39 0.26 0.06 0.219 37 0.25 0.05 0.182 0.64012 months 39 0.26 0.05 0.199 36 0.24 0.05 0.626 0.24824 months 37 0.27 0.05 0.667 31 0.26 0.05 0.033 0.479
HDL/LDL ratioPreinsertion 40 0.41 0.13 40 0.37 0.11 0.2256 months 39 0.39 0.12 0.089 37 0.37 0.10 0.803 0.61412 months 39 0.38 0.11 0.031 36 0.35 0.10 0.451 0.36724 months 37 0.41 0.12 0.934 31 0.38 0.11 0.410 0.325
Apo A-I/Apo-B ratioPreinsertion 40 1.72 0.43 40 1.69 0.33 0.9156 months 39 1.62 0.35 0.076 37 1.58 0.36 0.076 0.59212 months 39 1.42 0.31 0.000 36 1.43 0.35 0.000 0.86524 months 37 1.47 0.81 0.000 31 1.31 0.28 0.000 0.542
a Results of Wilcoxon signed-rank test on change from baseline.b Results of Mann-Whitney U-test (two unrelated samples nonparametric test) on group differences.
192 A. Biswas et al. / Contraception 68 (2003) 189–193

[3] Michal F. Safety requirements for contraceptive steroids. Publishedon behalf of WHO. Cambridge: Cambridge University Press, 1989. p.439.
[4] Friedewald WI, Levy RI, Fredrickson DS. Estimation of the concen-tration of low density lipoprotein cholesterol in plasma, without theuse of the preparative ultracentrifuge. Clin Chem 1982;18:499–502.
[5] Slone D, Shapiro S, Kaufman DW, Rosenberg L, Miettinen OS,Stolley PD. Risk of myocardial infarction in relation to current anddiscontinued use of oral contraceptives. N Engl J Med 1981;305:420–4.
[6] Vessey MP, Villard-Mackintosh L, McPherson K, Yeates D. Mortal-ity among oral contraceptive users: 20-year follow-up of women in acohort study. Br Med J 1989;299:1487–91.
[7] Meade TW, Greenberg G, Thompson SG. Progestogens and cardio-vascular reactions associated with oral contraceptives and a compar-ison of the safety of 50- and 30-microgram oestrogen preparations. BrMed J 1980;280:1157–61.
[8] Wynn V, Niththyananthan R. The effect of progestins in combinedoral contraceptives on serum lipids with special reference to high-density lipoproteins. Am J Obstet Gynecol 1982;142(6 Pt 2):766–71.
[9] Oster P, Arab L, Kohlmeier M, Mordasini R, Schellenberg B, SchlierfG. Effects of estrogens and progestogens on lipid metabolism. Am JObstet Gynecol 1982;142(6 Pt 2):773–5.
[10] Wahl P, Walden C, Knopp R, et al. Effect of estrogen/progestinpotency on lipid/lipoprotein cholesterol. N Engl J Med 1983;308:862–7.
[11] Godsland IF, Crook D, Simpson R, et al. The effects of differentformulations of oral contraceptive agents on lipid and carbohydratemetabolism. N Engl J Med 1990;323:1375–81.
[12] Notelovitz M, Feldman EB, Gillespy M, Gudat J. Lipid and lipopro-tein changes in women taking low-dose, triphasic oral contraceptives:a controlled, comparative, 12-month clinical trial. Am J Obstet Gy-necol 1989;160(5 Pt 2):1269–80.
[13] Crook D, Godsland IF, Worthington M, Felton CV, Proudler AJ,Stevenson JC. A comparative metabolic study of two low-estrogen-dose oral contraceptives containing desogestrel or gestodene proges-tins. Am J Obstet Gynecol 1993;169:1183–9.
[14] Singh K, Viegas OAC, Loke DFM, Ratnam SS. Effect of Norplantimplants on liver, lipid and carbohydrate metabolism. Contraception1992;45:141–53.
[15] Singh K, Viegas OAC, Loke D, Ratnam SS. Effect of Norplant-2 rodson liver, lipid and carbohydrate metabolism. Contraception 1992;45:463–72.
[16] Singh K, Ratnam SS. A study on the effects of Norplant implantablecontraceptive on lipid, lipoprotein and apolipoprotein metabolism inSingaporean women. Contraception 1997;56:77–83.
[17] Suherman SK, Affandi B, Korver T. The effect of Implanon on lipidmetabolism in comparison with Norplant. Contraception 1999;60:281–7.
[18] Rabe T, Thuro HC, Goebel K, Borchardt C, Grunwald K, RunnebaumB. Lipid metabolism in Norplant-2 users—a two-year follow-upstudy. Total cholesterol, triglycerides, lipoproteins and apolipopro-teins. Contraception 1992;45:21–37.
[19] Mascarenhas L, van Beek A, Bennink HC, Newton J. Twenty-fourmonths comparison of apolipoproteins A-I, A-II and B in contracep-tive implant users (Norplant and Implanon) in Birmingham, UnitedKingdom [Published erratum appears in Contraception 1998;58:389].Contraception 1998;58:215–9.
193A. Biswas et al. / Contraception 68 (2003) 189–193





























