Embed Size (px)
Citation preview

Eur Respir J, 1993, 6, 1371-1377 Ptinted in UK • all rights reserved
Copyright ©ERS Journals ltd 1993 European Respiratory Journal
SERIES 'HIGHLIGHTS ON PULMONARY HYPERTENSION' Edited by T. Higenbottam and R. Rodriguez-Roisin
ISSN 0903 • ;~ '; )
~ Effect of pulmonary hypertension on gas exchange
A.G.N. Agustl*, R: Rodriguez-Roisin**
Effect of pulmonary hypertension on gas exchange. A.G.N. Agustf, R. Rodriguez-Roisin. ©ERS Journals I..Jd. ABSJ'RACT: This paper revie~'S the effects of pulmonary anery bypertei\Sion on gas excbant,>e by e..'J>Ioring tbree different ~ namely: 1) bow dOt!S gas exchange behave in diseases characterized by increased vascular tone (primary pulmonary hypertension (PPH), chronic o~1ructive pulmonary di<;ease (COPD) and interstitial pulmonary fibrosis (IPF)) or decrea'ied vascular tone ("hepatopulmonary syndrome"); 2) bow does exercise, as a 0()1)-pharmacological tool of increasing pulmonary blood Oow, modiiY gas e..Xl'hange in these diseases; and 3) how do several drugs that lower (vasodil.ators) or increase (almitrine) the active component of pulmonary hypertension interact with gas exchange.
Available data show tha.t: J) in PPH a high pulmonary vascular tone enhances gas exchange and wb.cn it is lowered, either by oxygen or vasodilators, ventilation perfusion (V A/0) distributions deteriorate; 2) in COPD a lowered (vasodilat.ors) or augmented (almitrine) active vascular lone is almost invariably paralleled by a deterioration or enhanl-ernent of ventilation-perfusion matching, respectively; 3) in IPF an adequate active response of the pulmoJUlry vasculature is essential to maintain gas exchange, both at rest and during exerci-;c; and 4) in patients with liver cirrhosis a low pulmonary vascular tone induces an abnonnaJ ~ A/Q distribution.
In SUI1l.DllUy, these data show that any situation and/or therapeutic intervention that lowers the active va'ICUiar tone deteriorates V A/0 relationships and vice ven;a. 1be final effect of pulmonary vascular tone on ru1.erial oxygen tension (PaoJ is less predictable. Tbe reason for f.hi.; li1'1Certainty is that the ac:tua1 ~ value depends on the interplay of the intraand extrap.~onary factors that control gaq exchange in huiJlJlllS, and not only on l.he degree of V A/Q mi!>nwtchlllg. Eur Respir J., 1993. 6, 1371-1377.
*Servicio de Neumologfa, Hospital Un.iv. Son Dureta, Palma de Mallorca, Spain. **Servei de Pneumologia i All~rgia Respiratoria, Hospital Clinic, Barcelona, Spain.
Correspondence: A.G.N. Aguslf Servicio Neumologfa Hospital Son Dureta Cl Andrea Doria 55 07014 Pal.ma de Mallorca Espana
Keywords: Exercise gas exchange hypoxemia inert gases pulmonary circulation V AIQ distributions
Received: March 31 1993 Accepted for publication May 23 1993
Pulmonary hypertension is a common and severe complication of lung disease. It~ deleterious effects on right ventricular mechanics and performance have been well described. However, the effects of pulmonary hypertension on gas exchange are less well understood The purpose of this paper is to show that gas exchange in pulmonary hypertension, as a result of high vascular tone, is much better than in lung diseases characterized by low pulmonary vascular tone.
disease (COPD) and cryptogenic fibrosing alveolitis, compared with diseases where pulmonary vascular tone is decreased, e.g. hepatopulmonary syndrome [1, 2]; 2) the way in which exercise, as a nonpharmacological mean of increasing pulmonary blood flow, modifies gas exchange in these diseases; and 3) the effects of drugs lowering (vasodilators), or increasing (almitrine), pulmonary vasomotor tone on gas exchange.
It is important to differentiate structural and functional changes of the pulmonary vasculature which cause pulmonary hypertension. Functional change is characterized by the contractile response to hypoxia (hypoxic pulmonary vasoconstriction), where vascular tone is increased. Its main physiological characteristic is that of reversibility when nonnoxia is restored. Structural change is where there is a fixed component from anatomical derangement or loss of pulmonary capillary surface area. Such pulmonary hypertension is caused by the lung disease itself. By definition, this fixed form is not reversible by oxygen or drugs.
To demonstrate that a high pulmonary vascular tone enhances and preserves a more homogeneous ventilationperfusion cV AJQ) matching, three different issues will be explored: l) the contrasting effects on gas exchange in those diseases where vascular tone is increased, e.g. primary pulmonary hypertension, chronic obstructive pulmonary
The majority of studies used the multiple inert gases elimination technique (MIGET) [3-5] to estimate the distribution of V A/Q relationships, this being the most suitable technique to determine pulmonary gas exchange in patients and to study it~ relationship to pulmonary vascular resistance [6, 7]. The methods used in MIGET will not be described in detail; we refer the reader to recent reviews on this subject [6, 7].
Gas exchange in diseases associated with high vascular tone
Primary pulmonary hypertension (PPH)
PPH can be considered the model of diseases characterised by increased pulmonary vascular tone. DANIZXER and

1372 A.G.N. AGUSTI, R. RODRIGUEZ-ROISIN
BOWER [8] were the first to use the MIGET in a group of patients with PPH. They showed that, at rest breathing room air, V AIQ relationships were essentially well-preserved, with most of the ventilation and perfusion being distributed to alveolar units with normal V AIQ ratios; most patients also showed a small second mode characterised by perfusion of units with a very low V AIQ ratio ( <0.1 excluding shunt), or even with a V AIQ ratio of zero ( <0.005, shunt) [8].
To study the relationship of V AIQ distribution to pulmonary hemodynamics in these patients, hypoxic pulmonary vasoconl>triction wa~ reversed with high fractional inspired oxygen levels. The cardiac output increased and pulmonary vascular resistance decreased. It can be concluded that restoration of norrnoxia reduced pulmonary vasoconstriction, so diminishing resistance to flow and enabling an increase in cardiac output. Norrnoxia appears, therefore, to have a beneficial effect on pulmonary haemodynamics. However, at the same time, the physiological shunt increased (from 2 to 7% of cardiac output) and the second mode in the perfusion distribution described above, that is the amount of blood flow perfusing poorly-ventilated areas, also increased significantly. Thus, despite the improved pulmonary haemodynamics with oxygen, V AIQ relationships clearly deteriorated (8]. The investigators interpreted these findings as evidence of the deleterious effects of releasing hypoxic pulmonary vasoconstriction (active tone) on gas exchange in patients with PPH. Therefore, the increased pulmonary vascular tone of these patients under baseline conditions (breathing room air) was, in fact, contributing to preserve gas exchange [8].
DANTZKER and BoWER [8] also tested the effec.ts of several vasodilator drugs on V AIQ relationships in these patients. They observed that after infusing either isoproterenol or nitroprusside, V AIQ relationships again deteriorated markedly, with a significant increase in both shunt and petfusion to poorly-ventilated alveolar units with low V AIQ ratios ( <0.1) [8]. Two ye~ later, MELoT et al. [9] reported similar results on V AIQ relationships in patients with PPH after nifedipine, a calcium channel blocker.
In summary, studies in patients with PPH have shown that a high pulmonary vascular tone enhances gas exchange, and that when it is lowered, either by oxygen or with vasodilators, V AIQ distributions deteriorate.
Chronic obstructive pulmonary disease (COPD)
Abnormal pulmonary gas exchange with hypoxaemia and hypercapnia is characteristic of COPD. These patients often develop pulmonary hypertension. Both structural and functional factors contribute to the development of pulmonary hypertension in COPD. The structural changes are associated with a loss of capillary surface area, particularly in patients with pulmonary emphysema. There is also increased pulmonary vascular tone, because of the presence of poorly-ventilated lung units, due to hypoxic pulmonary vasoconstriction. It is not clear how these two components of pulmonary hypertension interact with gas exchange, and more specifically V AIQ relationships.
In 1990, Aousn et al. [10] investigated the effect~ of exercise and the vasodilator nifedipine on V AIQ relationships in a group of patients with advanced, but otherwise clinically
stable, COPD with mild to moderate pulmonary hypertension. The rationale behind their study wa~ that exercise is a non-pharmacological method of increasing pulmonary blood flow, whilst nifedipine increases pulmonary blood flow by relaxing vascular smooth muscle. At the same time, nifedipine "reverses" the hypoxic pulmonary vasoconstriction component of pulmonary hypertension [10]. The authors choose to include patients with only moderate pulmonary hypertension on the assumption that these patient~ would probably have both increased active tone and anatomical derangement of the pulmonary vasculature, whilst patients with more advanced COPD and severe pulmonary hypertension may have a greater anatomical destruction of the capillary bed, and hence be less responsive to manipulations of the vascular tone [10]. This assumption has recently been stressed by other authors on the basis of physiological deterrninations [11], morphometric studies [12, 13] and, very recently, in vitro investigations of the functionality of the pulmonary endothelial cells of patients with COPD submitted to lung transplant [14, 15].
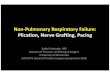
Figure 1 shows the haemodynamic profile (at rest and during exercise, with and without nifedipine) of the patients studied by AauSTI et al. (10]. Without nifedipine (continuous line), submaximal exercise (at 60% maximal 0 2 consumption) induced a marked increase both in cardiac output and mean pulmonary artery pressure. After nifedipine, at rest, mean pulmonary artery pressure did not change, but cardiac output increased. When these patients exercised after nifedipine (dashed line), cardiac output also increased (with respect to resting conditions with nifedipine). In absolute terms, cardiac output was higher than that measured during exercise without the drug. However, despite this higher cardiac output, pulmonary hypertension during exercise was lower with than without nifedipine. Overall, these data were interpreted as evidence of the vasodilator effect of nifedipine upon the pulmonary circulation.
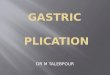
Figure 2 shows tl1e V AIQ ratio distributions obtained in a representative patient of the series JIOJ. At rest, before nifedipine, U1ere is a clearly abnonual V AIQ distribution, with
50
40 Cl
~ 30 E [ 20
10...
10
0 +---------r--------.---------, 0 5 10 15
Or l·min-1
Fig. I. - Plot of cardiac output (Qr) ven.us mean pulmona!y arte1y pressure (Ppa) obtained at rest and during submaximal exercise (60% of 'V<¥nax) in a group of patient~ with advanced COPD, before (continuous line) and after (dashed tine) the administration of nifedipine. Results are presented as mean:tso. V¥l3X: maximal 0 1 coosumplion: COPO: chronic OOitm:tive pliIOOilal)' disease. F<r ti.utD!r explanalion. see leXl (From (10] reprOOuced with permission of Ch£~1).

PULMONARY HYPERTENSION AND GAS EXCHANGE 1373
Before N Rest Exercise 1.0 1.0
";" c 0.5 0.5 ·e ...:. c:: .2 "' .g 0 0 2i 100 100 -o
After N c «! c:: 1.0 1.0 0
; ~ E ~
0.5 0.5
0 0.1 1 10 100 0 0.1 1 10 100 Ventilation-perfusion ratio
Fig. 2. - Ventilation-perfusion distribution obtained in a representative COPD patient studied at rest and during exelcise, before and after lhe ad.ministnuion of nifedipine (N). COPD: chronic obstructive pulmonary disease;
0 - : ventilation: - .--- : perfusiort For furtOOr expl!lrlalion. see text (From [I 0 l reproduced wih pcnnission of Chest).
perfusion distributed to low V AIQ units ( <0.1 excluding shw1t). and also ventilation to units with high V tJQ ratios (I 0 excluding de-dd space). Tlus type of V AIQ distribution is characteristic of COPD [6, 7]. Exercise (before nifedipine) induced a marked improvement in gas exchange, as shown by the narrowing of bolh the ventilation and blood flow dislributions. 1his improvement paralleled the marlced increase in the pulmonary artery pressure (fig. l). By contrast, at rest nifedipine induced both pulmonary vasodilation (fig. I) and a significant deterioration of V AIQ relationships (fig. 2). lt should be noted lhar aller nifedipine (at rest) there is more blood flow distributed to alveolar units with a low V tJQ ratio. Therefore, !he effects of nifedipine at rest upon pulmonary gas exchange in patients with COPD were very similar to those previously described for patients with PPH. That is, by lowering the active component of pulmonary hypertension. the mechanisms that tend to preserve V AIQ relationships became less effective. However, the study by Aousn et at. [10] extended previous observations to exercLc;e conditions. The lower right panel of figure 2 shows that despite this deleterious effect of nifedipine on V AIQ distributions. exercise had an intense influence on gao; exchange, and was still capable of improving V AIQ matching in these patients. Observe that with respect to resting conditions after nifcdipine, V AIQ distributions obtained dwing exercise with nifedipine were narrower and less heterogeneous (fig. 2). Nevertheless. the effects or nifedipine (i.e. the effects or interfering with the active component of pulmonary hypertension) were sti.U apparent during exercire, as shown by the broader V AIQ distributions shown during exercise with than without nifedipine.
Figure 3 summarizes all this infonnation by presenting a plot of oxygen uptake (Vo2, ml·min-•). i.e., intensity of exercise, versus: a) Log50 perfusion (a variable that informs
1.2 a)
c 1.0 ~~ 0 ·oo :::l 't:: 0.6 Q) a.
0 en
Cl 0
....J 0.6
0.4
0.2
0 200 400 600 600 1000
Oxygen uptake ml-min-1
60 b)
<?-1-
~ >
50
0 200 400 600 600 1 000
Oxygen uptake ml-min-1
Fig. 3. - Summacy plot of the effects of exercise and nifedipine on pulmonary gas exchange in patients with COPD. Results are presented as mean:±so. a) shows a plot of oxygen uptake {VoJ (i.e. intensity of exercise) vem4S 1<>&-u perfusion ( uxlicating dispasioo of blood flow dislribution). b) rresents the relationship betwen V o, and the deadspace to tidal volume ratio (Vo!VT). Shaded areas represent expected nomtal values aJ rest--: before nifcdipine; - - : nfler nifcdipine. COPD: chronic obstructive pulmonary disease. For further explan:u.ion, see texL • : represents signficance (From LJO). reproduced with permission or Chest).
of the dispersion (so) on a log scale (log) of the blood flow distribution) [3, 7]; and b) the dead space to tidal volume ratio (VoNT). The shaded areas represent the expected normal values for both variables at rest. The VoNT response to both nifedipine and exercise will not be discussed here, for the sake of brevity. For that analysis, we refer the interested reader to the original reference [lO]. With respect to log50 perfusion, note that before nifedipine (fig. 3, continuous line), exercise decreased the dispersion of pulmonary perfusion i.e. exercise improved gas exchange. The administration of nifedipine, however, increased the dispersion of blood flow. This indicates that, by lowering the pulmonary vascular tone (fig. I), nifedipine interfered with the mechanisms that try to preserve the matching between alveolar ventilation and capillary perfusion. However, even in the presence of this interference, exercise was still able to decrease (i.e. improve) the dispersion of pulmonary perfusion again (fig. 3, upper panel, continuous line). Finally, the comparison of both exercise points, with

1374 A.G.N. AGUSTI, R. RODRIGUEZ-ROISIN
and without nifedipine, reveals that there is more V AIQ mismatch following administration of the drug (fig. 3). This exemplifies the net effect of a lower pulmonary vascular tone on gas exchange during exercise in COPD patients. Taken together, these data in patients with COPD show again (as in the case of patients with PPH) that a high pulmonary vascular tone enhances and preserves gas exchange, both at rest and during exercise.
There are also data available exploring what happens to gas exchange if pulmonary vascular tone is phannacologically augmented e.g., by giving almitrine bismesylate, a drug originally designed as a ventilatory stimulant, which has been shown to enhance hypoxic pulmonary vasoconstriction [16- 18]. It has been clearly documented that, by increasing the active pulmonary vascular tone, almitrine improves ventilation-perfusion matching and, thereby, arterial oxygenation. However, this is at the expense of a slight, but significant, increase in pulmonary artery pressure, and some clinically significant neurological side-effects [16]. Therefore, at the present time, its clinical indication in patients with COPD is questioned Nevertheless, for the pwpose of this review, almitrine constitutes an excellent pharmacological example of how any increase in pulmonary vascular tone improves gas exchange.
In summary, it is clear that in patients with OOPD, as well as PPH, a lowered (vasodilators) or augmented (almitrine) active pulmonary vascular tone is almost invariably paralleled by a deterioration or enhancement of V AIQ matching,
respectively. Whether or not this statement will be altered by the use of new drugs, such as urapidil or nitric oxide [15, 19, 20], which may have a highly selective effect on the pulmonary vasculature, is still a matter of current research.
Idioparhic pulmonary fibrosis (IPF)
Patients with JPF characteristically have restrictive ventilatory impairment, decreased diffusing capacity of the lungs for carbon monoxide (OLeo), and mild arterial hypoxaemia, that generally, but not always, worsens during exercise [21]. The histopathological picture reveals a slructuralloss of alveolar-capillary units. It is not surprising, therefore, that in advanced stages of the disease, patients with IPF develop pulmonary hypertension [22]. It has been attributed largely to the physical loss of capillary surface area. However, hypoxic pulmonary vasoconstriction may also play a role in the development of pulmonary hypertension in these patients [22]. Again, the relationship between the active component of pulmonary vascular disease and gas exchange in IPF is not clear.
To clarify this question V AIQ distributions were obtained in a group of patients with IPF studied at rest breathing room air (baseline conditions), at rest breathing 100% 0 2 (to release hypoxic pulmonary vasoconstriction), and during exercise whilst breathing room air (again as a nonpharmacological tool to increase pulmonary blood flow) [23]. Figure 4 presents the V AIQ ratio distributions obtained in
a) 1.0 .---------,
b) 1.0 ,.----------,
c) 2.0 .....---------,---.
JSS JSS JSS
0.5 0.5 1.0
";"
~unt c: ·e ~ • • • c: 0 0 0 ·u; ::::1
0 ,_o,...,,~oo..--....,.----,---,---,---,.....J 0 0
"t:: Q) 0 0.01 100 0 0.01 100 0 0.01 100 c..
-o 1.0 c: t"O MRG c: 0
4.0 MRG
~ f E ~ "
3.0
0.5 0.5 • 2.0
• 1.0
• 0 0 ~ -- 0 L,or-""'"..--...,--.--.---,...---,.....J 0 0
0 0.01 100 0 0.01 100 0 0.01 100
Ventilation/perfusion ratio
Fig. 4. - Venlilalioo-pctfuOOII distribution obrained in two represenllllive patients (JSS and MGR) with idiopalhic pulmonaly fibrosis: a) at rest brealhing room air; b) at rest breathing 100% 0 2; and c) during exercise (brealhing room air). -o-: venlilalion;~ :perlusion. fU further explanalion, see texl (From [23), reproduced with permission of Am Rev Respir Dis).

PULMONARY HYPERTENSION AND GAS EXCHANGE 1375
two of these patients. Note that, at rest breathing room air, both patients showed relatively well-preserved V AIQ distributions, with a very small amount of shunt and/or blood flow perfusing units with low V AIQ ratios. Instead, these patients had most of their perfusion and ventilation going to alveolar units with essential normal V AIQ ratios. Despite this similarity at baseline, the two patients displayed different patterns of response, both to the administration of oxygen and to exercise. The V AIQ ratio distributions of the patient depicted in the upper panels of figure 4 (JSS) showed no noticeable change with high fractional inspiratory 0 2 (FtoJ or during exercise. By contrast, both oxygen and exercise had pronounced effects upon V AIQ distributions in the patient depicted in the lower panels (MRG). It can be observed that, compared to baseline, the inha1ation of 0 2 by this patient induced a marked increase in the amount of blood flow perfusing poorly ventilated areas (shown in the figure as a second mode in the perfusion distribution) and shunt. However, when this patient exercised, V AIQ mismatching was significantly improved with respect to baseline. These data indicate that some patients with IPF may have a pulmonary vasculature that is responsive to 0 2 (MRG), whilst others are insensitive to it (JSS), thereby suggesting a more fixed (anatomical) vascular derangement. Interestingly, the former group improved V AIQ relationships during exercise, while the latter showed no such response.
To test the hypothesis that the preservation of an active pulmonary vascular tone was desirable in terms of gas exchange (particularly during exercise), the authors tried to quantitate the degree of pulmonary vascular responsiveness to 0 2• As an "index" of pulmonary vascular reactivity, they calculated the increase in perfusion of poorly-ventilated lung units whilst breathing pure 0 2, which probably represents release of hypoxic pulmonary vasoconstriction [7, 10, 23]. This variable, i.e. percentage change from baseline in the dispersion of the perfusion distribution whilst breathing 100% oxygen (.::llog, Q), seems to be more sensitive to small changes in the pulmonary vascular tone than the standard haemodynamic measurements (pressure and flow) [7, 10, 23). Figure 5 shows this index of pulmonary vascular reactivity plotted against the values (all of them during exercise) of: a) mean pulmonary artery pressure; b) an index of the overall degree of V AIQ homogeneity, (DISP RE*); and c) P~. Ftgure 5a shows a significant relationship between "vascular reactivity" and pulmonary hypertension during exercise. Those patients having no or minimal vascular response to 0 2 (at rest) suffered severe degrees of pulmonary hypertension during exercise, whilst those exhibiting evidence of release of hypoxic vasoconstriction at rest did not develop pulmonary hypertension during exercise. These latter patients probably had a more distensible and/or recruitable pulmonary circulation than the former ones. Ftgure 5b shows an excellent relationship between vascular reactivity and overall degree of V A!Q mismatch during exercise. Those patients with more active tone at rest (i.e. those having more release of hypoxic vasoconstriction) had less V AIQ mismatch during exercise. Finally, figure 5c shows that those patients with a high pulmonary vascular active tone at rest were those who did not present arterial desaluration during exercise, whilst those having no or min-
80 a) ..
Cl :X: E
60 r=-0.67 E • p<0.05 Cl> <J)
·~ •• Q) 40 ><
Q) • Cl c
·;:: ::::J 20 .... '"0 al CL
,a_
0 0 40 80 120 160
L\log800100% 02, %baseline
14 b)
Q)
12 • <J) ·e • Cl> 10 • >< Q)
r=-0.72 p<0.0025
01 c ·;:: 8 ::::J
'"0 6 Lu • d: 4 a.. • (f) 2 0
•
0 0 40 80 120 160
L\log800 100% 02 , %baseline
120 c) Cl
~ 100 ..
E 80
40
20
•
r=0.64 p<0.01
0 '--.---.~----.~---.-~--, 0 40 80 120 160
.6.1og800 100% 02 , %baseline
Fig. 5. - On lhe abscissa. change in dispersion of lhe perlusion dislribution while breathing 100% 0 2 (%change from baseline conditions) (~<>&oQ). This variable is an expres<;ion of lhe degree of release of hypoxic pulmonaxy vasoconstiction. It is plotted against a) mean pulmonaxy artery pres<;ure (i>pa); b) a variable that indicates the overall degree of V AIQ mismatching (DIPSP R·E*); and c) ~· For further explanation, see text (Prom [23), reproduced with permission of Am Rev Respir Dis).
imal pulmonary vascular response to 0 2 (at rest) presented significant arterial hypoxaemia during exercise [23].
In summary, these data indicate that IPF patients with more fixed changes of the pulmonary vasculature (probably because they also have a more advanced clinical disease) showed no evidence of hypoxic vasoconstriction being relieved by 0 2 at rest and, at the same time, showed more severe pulmonary hypertension, more V AIQ mismatch and

1376 A.G.N. AGUSTI, R. RODRIGUEZ-ROISIN
lower P~ during exercise (fig 5). Taken together, these data indicate that. an adequate active response of the pulmonary vasculature is also essential in patients with IPF to preserve gas exchange, both at rest and during exercise.
Gas exchange in diseases associated with low vascular tone
The hepatopulmcnary syndrome
The term "hepatopulmonary syndrome" was coined to describe the abnormalities of pulmonary gas exchange and lung circulation that may occur in patient~ with cirrhosis of ~e liver, in the absence of any intrinsic lung or heart disease [241. The possibility that some patients with cirrhosis may associate cyanosis, clubbing and dyspnoea has been known since 1884 [25]. However, we have only recently begun to understand the pathophysiological basis for this clinical observation [ 1, 2, 26-29). The hepatopulmonary syndrome is now thought to be a condition characterized by pulmonary vasodilation and abnormal gas exchange [1, 2, 26-29], with blunted or decreased pulmonary vascular response to hypoxia [30, 31]. It therefore seems appropriate for the purposes of this review to analyse in detail how this low active vascular tone affects pulmonary gas exchange.
The ftrst study to use the MIGEf in cirrhosis was published in 1987, by R ODRIOUEZ-R OJSIN et a[ [32). All of the patients studied were in stable clinical condition (without ascites or fluid retention), had normal spirometry, and no evidence of. cardiac disease [32]. At rest breathing room air, these pattent'i showed the characteristic hyperdynamic cardiocirculatory state of cinhosis, characterised by high cardiac output and low pulmonary vascular resistance [32]. When they were given 12% 0 2 to breathe (to investigate hypoxic pulmonary vasoreactivity), pulmonary vascular resistance increased only marginally, particularly in those patients with cutaneous spider naevi [32J. Subsequent studies during exercise confirmed this observation (blunted and/or absent hypoxic vasoconstriction) and demonstrated that patients with cinhosis usualy have an abnonnally dilated pulmonary circulation [33].
Despite the absence of airflow limitation and/or fluid retention, and the presence of normal cardiac function, patients with cirrhosis showed substantial V AIQ mismatch [32, 33]. "!hls. was characterized by the presence of perfusion to low V AIQ units and, in some patients, a moderate degree of shunt [32, 33]. These abnormalities of gas exchange were more pronounced in patients with cutaneous spider naevi (those who also depicted the more severe haemodynamic abnormalities) [32]. Studies by other groups extended these observations to patients with more severe degrees of arterial hypoxaemia, in whom pure shunt seems to acquire more physiological relevance [34-37], as well as some level of diffusion disequilibrium to oxygen transfer [35-36]. Both abnormalities of the pulmonary circulation and of gas exchange seem to be more pronounced in those patients with a severe degree of liver failure [1, 2, 31]. Also of interest is the fact that most of these gas exchange and haemodynamic abnormalities appear to resolve following normal-
ization of liver function after transplant [2, 24]. Therefore, it is now generally accepted that the "hepatopulmonary syndrome" is characterized by an abnormally low pulmo~ vascular ton~, ~ eviden~ by a blunted or absent hypoXIc vasoconstnct.ton, that mterferes with an appropriate matching of alveolar ventilation and capillary perfusion and that usually runs in parallel to liver function. Very recently, several diagnostic criteria for this syndrome have been proposed [2].
In summary, for the purpose of this review, the studies alluded to in patients with liver cirrhosis, stressed again the important interrelationships between the pulmonary vascular tone and gas exchange, by demonstrating that, in this case, a low pulmonary vascular tone interferes with the homogeneous distribution of V A!Q ratios.
Summary and conclusions
We have reviewed the interaction of pulmonary vascular tone and gas exchange in primary pulmonary hypertension, COPD, IPF and liver cirrhosis. We have shown that any situation and/or therapeutic intervention that lowers the active vascular tone deteriorates V A!Q relationships, and vice versa. Therefore, this paper has presented evidence to support the fact that, in terms of g~ e~change, a high pul~onary vasc~lar tone enhances V AIQ matching in lung dtsease and IS, therefore, desirable. However, the final e~ect of pulmonary vascular tone on arterial P~ is less predictable. The reason for this uncertainty is that the actual Pa01 valu~ depends on the interplay of the intrapulmonary factors (V AIQ relationships, intrapulmonary shunt and diffusion limitation to oxygen) and extrapulmonary factors (cardiac output, overall ventilation and oxygen consumption) that contro!s 8l!S exchange in humans, and not only on the degree of V AIQ mismatching [7]. A deep analysis of these interactions is beyond the scope of this paper. The interested reader is referred to other papers that discuss this point in more depth [6, 7, 33, 38, 39]. Finally, we have not discwsed the well-known deleterious effects of pulmonary hypertension on right ventricular mechanics and performance. Nonetheless, these latter effects should always be borne in mind when facing any given clinical decision.
Ackoowkdgermnts: 'The aul.hors acknowledge the secretarial help of I Chaves, and MJ. Labot
Refe.rences
I. Agustf AGN, Roca J, Bosch J, Rodriguez-Roisfn. - The lung in patienl~ with cirrllosis. J Hepatol1990; lO: 251-257 2. Rodriguez-Roisin R. Agusti' AGN, Roca J. - The hepatopulmonary syndrome: new name, old complexities. Tlwrax 1992; 47: 897-902. 3. Wagner PD, Naumann PF, Laravuso RB. - Simultaneous measurement of eight foreign gases in blood by gas chromatography. J Appl Physiol 1974; 36: 6()0...<)()5 4. West m. Wagner PD. Pulmonary gas exchange. - In: West m, ed. Bioengineering aspecL~ of the lung. New York, Marcel Dekker, 1977, pp 361-364.

PULMONARY HYPERTENSION AND GAS EXCHANGE 1377
5. Rodrigucz-Roisin R, Roca J, Guitan R, Agusti AGN, Torres A. Wagner PD. - Measurements of distributions of ventilationperfusion ratios: multiple inert gases elimination technique. Rev esp Fisiol 1986; 42: 465-482. 6. Dantzker DR. - VentiJation-perfusion inequality in lung dis-~- Chest 1987; 91: 749-754 7. Rodriguez-Roisin R, Wagncr PD. - Clinical relevance of ventilation-pelfusion inequality detennined by inert gas elimination. Eur Respir J 1989; 3: 469-482. 8. Dantzkcr DR, Bower JS. - Pulmonary vascular tone improves V AIQ matching in oblitcrative pulmonary hypertension. J Appl Physiol: Respirat Environ Exercise Physsio/ 1981; 51: 607-{)13. 9. Melot C, Naeije R, Mols P, Vandcnbossche JL, Denolin H. -Effects of nifedipine on ventilation/pert'usion matching in primary pulmonary hypertension. Chest 1983; 83: 203-207. 10. Agusti AGN, Barbera JA, Roca J, Wagner PO, Guitart R, Rodriguez-Roisin R. - Hypoxic pulmonary vasoconstriction and gas exchange during exen:ise in chronic obstructive pulmonary dis~- Chest 1990; 97: 268-275. 11. Saadjian A. Philip-Joet F. Levy S, Arnaud A. - Vascular and cardiac reactivity in pulmonary hypertension due to chronic obstructive lung disease: assessment with various oxygen concenttations. Eur Respir J 1992; 5: 525-530. 12. Barbera JA, Roca J, Rarnirez J, Wagner PO, Ussetti P, Rodriguez-Roisin R. - Gas exchange during exercise in mild chronic obstructive pulmonary disease. Am Rev Respir Dis 1991; 144: 520-525. 13. Barbera JA, Riverola A, Ram.irez J, et al. - Effects of pulmonary vascular abnormalities on hypoxic pulmonary vasoconstriction in mild chronic obstructive pulmonary disease (Absttact). Am Rev Respir Dis 1991; 143: AI78(A). 14. Dinh-Xuan AT, Higenbottarn TW, Clelland CA, et al. -Impairment of cndotheliurn-<iependent pulmonary artery relaxation in chronic obstructive lung disease. N Engl J Med 1991; 324: 1539-1547. 15. Dinh-Xuan AT. - Endothelial modulation of pulmonary vascular tone. Eur Respir J 1994; 5: 757-762. 16. Voisin C, Howard P, Ansquer JC. - Alrnitrine bismesy1ate: a long-term, placebo-controlled, double-blind study in COAD. Vectarion International Multicentre Study Group. Bull Eur Physiopathol Respir 1987; 23 (suppl. 11): 169-182. 17. Mclot C. Naeije R, Rothschild T. Mertens P, Mols P, Hallemans R. - Improvement in ventilation-pert'usion matching by alrnitrine in COPD. Chest 1983; 83: 528-533. 18. Romaldini H, Rodriguez-Roisin R, Wagner PD, West JB. -Enhancement of hypoxic pulmonary vasoconstriction by alrnitrine in the dog. Am Rev Respir Dis 1983; 128: 288-293. 19. Adnot S, Radermacher P, Andrivet P. Dubois-Rande JL, Dypeyrat A. Lernaire F. - Effects of sodium-nitroprusside and urapidil on gas exchange and ventilation-pert'usion relationships in patients with congestive heart failure. Eur Respir J 1991; 4: 69-75. 20. Rossaint R, Falke KJ, Lopez F. Slarna K. Pison U, Zapol WM. - Inhaled nitric oxide for the adult respiratory distress syndrome. N Engl J Med 1992; 340: 399-405. 21. Agusti AGN, Roca J, Rodriguez-Roisin R, Xaubet A, AgustiVidal A. - Different patterns of gas exchange response to exercise in asbestosis and idiopathic pulmonary fibrosis. Eur Respir J 1988; 1: 510-516.
22. Jackson LK, Fu1mer JD. - Structural-functional features of the interstitial lung diseases. In: Fishrnan AP, ed. Pulmonary Diseases and Disorders. Vol l. New York, McGraw-Hill 1988; pp. 739-754 23. Agust£ AGN, Roca J, Gea J, Wagner PD, Xaubet A, Rodrfguez- Roisin R. - Mechanisms of gas-exchange impairment in idiopathic pulmonary fibrosis. Am Rev Respir Dis 1991; 143: 219-225. 24. Eriksson LS, Si:iderman C, Wahren J, Ericzon BF, Eleborg L, Hedenstierna G. - ls hypoxaemia of cirrhotic patients due to a functional "hepato-pulrnonal" syndrome? (Abstract). J Hepatol 1988; 7: S29. 25. Fliickinger M. - Vorkommen von trommelschlagelforrnigen Fingerend phalangen ohne chronische Veranderungen an der Lungen oder am Herzen. Wien Med Wschnschr 1884; 34: 1457-1458. 26. Krowka MJ, Cortese DA. - Pulmonary aspect~ of chronic liver disease and liver transplantation. Mayo C/in Proc 1985; 60: 407-418. 27. Rodriguez-Roisfn R, Agustf AGN, Roca J. - Pulmonary function and liver disease. Curr Opin in Gastroemerol 1988; 4: 609-614. 28. Krowka MJ, Cortese DA. - Pulmonary aspects of liver dis~and liver transplantation. Clin Chest Med 1989; 10: 593-<i16. 29. Krowka MJ, Cortese DA. - Hepa!Opulmonary syndrome: an evolving perspective in the era of liver transplantation. Heparology 1990; 11: 138-142. 30. Daoud FS, Reeves IT, Schaeffer JW. - Failure of hypoxic pulmonary vasoconstriction in patients with liver cirrllosis. J C/in Invest 1972; 51: 1076-1080. 31. Naeije R, Hallemans R, Mols P, Melot C. - Hypoxic pulmonary vasoconstriction in liver cirrllosis. Chest 1981; 80: 570-574. 32. Roclrfguez-Roisin R, Roca J, Agustf AGN, Ma<;tai R, Wagner PD. Bosch J. - Ga~ exchange and pulmonary vascular reaCtivity in patients with liver cinilosis. Am Rev Re~pir Dis 1987; 135: 1085-1092. 33. Agusti AGN, Roca J, Rodrfguez-Roisin R, Mastai R, Wagrx!r PD. Bosch J. - Pulmonary haemodynamics and gas exchange during exercise in liver cirrhosis. Am Rev Respir Dis 1989; 139: 485-491. 34. Melot C, Naeije R, Decharnps P, Hallernans R, Lejeune P. -Pulmonary and extrapulrnonary contributors to hypoxaemia in liver cirrhosis. Am Rev Respir Dis 1989; 139: 632-Q40. 35. Edell ES, Cortese DA, Krowka JM, Rehder K. - Severe hypoxaemia and liver dis~. Am Rev Respir Dis 1989: 140: 1631-1635. 36. Castaing Y, Manier G. Haemodynamic disturbances and V AIQ matching in hypoxemic cirrhotic patients. Chest 1989; 96: 1064-1069. 37. Agusti AGN, Roca J, Bosch J, Garcfa-Pagan JC, Wagner PD, Rodriguez-Roisin R. - Effects of propranolol on arterial oxygenation and 0, ttansport to tissues in patients with cirrhosis. Am Rev Respir Dis 1990; 142: 306-310. 38. Torres A. Reyes A. Roca J, Wagner PD, Rodriguez-Roisin R. - Ventilation-pert'usion mismatching in chronic obstructive pulmonary disease during ventilator weaning. Am Rev Respir Dis 1989; 140: 1246-1250. 39. Dantzker OR, Lynch JP, Wegg JG. - Depression of cardiac output is a mechanism of shunt reduction in the therapy of acute respiratory failure. Chest 1980; 77: 636-Q42.