Embed Size (px)
Citation preview

Effect of stove intervention on household air pollutionand the respiratory health of women and children in ruralNigeria
Oluwafemi Oluwole & Godson R. Ana & Ganiyu O. Arinola &
Tess Wiskel & Adeyinka G. Falusi & Dezheng Huo &
Olufunmilayo I. Olopade & Christopher O. Olopade
Received: 8 September 2012 /Accepted: 13 March 2013# Springer Science+Business Media Dordrecht 2013
Abstract Domestic cooking with biomass fuels exposeswomen and children to pollutants that impair health. Theobjective of the study was to investigate the extent ofhousehold air pollution from biomass fuels and the effec-tiveness of stove intervention to improve indoor air quality,exposure-related health problems, and lung function. Weconducted a community-based pilot study in three ruralcommunities in southwest Nigeria. Indoor levels of particu-late matter (PM2.5) and carbon monoxide (CO) were mea-sured, and exposure-related health complaints were assessedin 59 households that used firewood exclusively for
cooking. Fifty-nine mother–child pairs from these house-holds were evaluated pre-intervention and 1 year after dis-tribution and monitored use of low-emission stoves. Meanage (± SD; years) of mothers and children were 43.0±11.7and 13.0±2.5, respectively. Median indoor PM2.5 level was1414.4 μg/m3 [interquartile range (IQR) 831.2–3437.0] pre-intervention and was significantly reduced to 130.3 μg/m3
(IQR 49.6–277.1; p<0.0001) post-intervention. Similarly,the median CO level was reduced from 170.3 ppm (IQR116.3–236.2) to 14.0 ppm (IQR 7.0–21.0; p<0.0001). Therewere also significant reductions in frequency of respiratorysymptoms (dry cough, chest tightness, difficult breathing,and runny nose) in mothers and children. Over 25 % ofmothers and children had moderate airway obstruction onspirometry pre-intervention that did not improve 1 year afterintervention period. Cooking with firewood causes house-hold air pollution and compromised lung health. Introduc-tion of low-emission stoves was effective at improvingindoor air quality and reducing exposure-related symptoms.
Keywords Household air pollution . Biomass fuels .
Exposure . Rural communities . Health . Intervention
Introduction
Household air pollution (HAP) from burning biomass is amajor public health hazard that affects over three billionpeople in developing countries (Salvi and Barnes 2010).Additionally, HAP accounts for two million yearly deathsfrom acute respiratory infections (ARI) in children and isassociated with increased frequency of non-smoking-relatedchronic bronchitis and lung cancer in women (Smith and
O. Oluwole :O. I. OlopadeCenter for Clinical Cancer Genetics and the Center for GlobalHealth, University of Chicago, Chicago, IL, USA
G. R. Ana :G. O. Arinola :A. G. FalusiCollege of Medicine, University of Ibadan, Ibadan, Oyo State,Nigeria
T. WiskelPritzker School of Medicine, University of Chicago, Chicago, IL,USA
D. HuoDepartment of Health Studies, University of Chicago, Chicago, IL,USA
C. O. OlopadeDepartment of Medicine and Family Medicine and the Center forGlobal Health, University of Chicago, Chicago, IL, USA
C. O. Olopade (*)Section of Pulmonary and Critical Care, Department of Medicineand the Center for Global Health, University of Chicago,5841 S. Maryland Avenue, MC 6076,Chicago, IL 60637, USAe-mail: [email protected]
Air Qual Atmos HealthDOI 10.1007/s11869-013-0196-9

Mehta 2003; Emmelin and Wall 2007). A recent WorldHealth Organization (WHO) report identified Nigeria asone of 11 African countries where HAP causes an estimated1.2 million deaths annually (WHO 2007).
Most women in rural areas of Nigeria cook with driedwoods combined with processed palm kernel skin, collec-tively called biomass fuels, that generate high levels of toxicpollutants, such as particulate matter (PM), carbon monox-ide (CO), volatile organic compounds, polycyclic aromatichydrocarbons, and oxides of nitrogen, sulfur, and fluorine(Zhang and Smith 2003). PM2.5 is the respirable fraction(less than or equal to 2.5 μm in aerodynamic diameter PM2.5)that can reach the alveoli easily. Both PM10 and PM2.5 and COexposure experienced by women and young children, themost vulnerable populations in many developing countries,have been estimated to be about 20 to 100 times above WHOguidelines and national guideline limits (Bruce et al. 2000;WHO 2004; McCracken et al. 2007).
In Nigeria, over 70 % of households still use biomassfuels for cooking, where women, who are traditionally theprimary cooks, and their children are highly exposed to theemitted smoke in poorly ventilated kitchens (Obueh 2006).As a result, HAP associated with biomass fuel is estimatedto be a major factor in up to 3.8 % of the national burden ofdisease (WHO 2007). While assessments have been made ofthe effectiveness of improved cooking stoves in reducingindoor air pollution (Naeher et al. 2007; McCracken et al.2007), few studies have systematically evaluated theirhealth impacts (Diaz et al. 2007; Smith et al. 2007; Romieuet al. 2009), and there are no data on the extent of HAP andrelated exposure to pollutants in Nigerian women and chil-dren. We conducted a pilot study to show the impact ofbiomass fuel use during cooking and to evaluate the poten-tial benefits of improved cooking stoves on the health ofrural women and children. The manuscript demonstrates theimpact of a 1-year intervention program on the health of thewomen and children participating in the study as well as theindoor air quality (IAQ).
Materials and methods
Study area and participants
The study settings were three similar rural communities,Ajibade, Eruwa, and Olorisaoko, near Ibadan, southwestNigeria. A two-stage random sampling method was usedto select 59 households from the communities for question-naire administration. Following listing of the homes in thestudy areas, the first stage identified households using bio-mass fuels exclusively for cooking indoors while the secondstage identified households that had at least one mother–child pair with the mother’s age between 20 and 60 years
and the child’s age between 6 and 17 years. The lower agelimit for children was set above 5 years to ensure successfulperformance of spirometry, which requires subject cooperation.Also, to be eligible, households expressed willingness toparticipate in the study.
Data collection methods
Data were collected in two phases: Phase I involved admin-istering questionnaires for health and biomass fuel exposureinformation. Indoor air sampling for PM2.5 and CO, andspirometry were performed in mother–child pairs in the 59households that use firewood exclusively for cooking. PhaseII involved education on the dangers of exposure to biomasssmoke and distribution and monitored use of low-emissionstoves with firewood.
Phase I data collection
Questionnaire survey
Detailed information was obtained from the mothers using astructured questionnaire. The questionnaires were adminis-tered in the local language to ensure that the women had agood understanding of the questions related to symptomsreporting. Additional information was collected from select-ed mother–child pairs on demographics, socioeconomic sta-tus, house construction types, fuel consumption patterns,cooking behaviors, and self-reported frequency of healthcomplaints.
Indoor air sampling during cooking
We conducted a pilot assessment of the indoor air quality inthe selected 59 households. Real-time measurement of PM2.5
was conducted in cooking areas before and during cookingusing the Thermo Scientific pDR 1500 personal aerosol mon-itor and data logger (Thermo Scientific, Franklin, MA, USA)in active mode, which uses gravimetric and optically basedmethods and compensates for many environmental variablesduring sampling. After calibration and equilibration, the in-strument was set to cycle every minute for an hour during thecooking of evening meals. At the start of the study, werandomly selected ten representative households from therecruited 59 households and monitored concentrations ofPM2.5 for 3 and 1 h in each of the ten households. Average3- and 1-h concentrations of PM2.5 were found to be similarand not different from each other during the sampling dura-tions; thus, we settled on the 1-h sampling duration. Sincedaily cooking episodes in each household were also similar,we monitored each household for PM2.5 concentrations for20 min before the start of cooking and during peak cookingperiod, which usually was 60 min from the start of cooking.
Air Qual Atmos Health

During the 1-h monitoring period, readings were obtained at15-min intervals and automatically recorded by the sampler.The average PM2.5 values for the 1-h duration were automat-ically logged into the sampler. Also, a digital CO10 carbonmonoxide meter (Cole-Parmer Instrument, Vernon Hills, IL,USA) similarly measured CO levels in each household. Sam-plers were positioned at the center of the kitchen and placedapproximately 0.5 m from the ground and within 1-m radiusof the plume arising from the pollution source to capture theemissions the women and children were exposed to duringcooking, as previously described (Ana et al. 2012). Allbaseline procedures were repeated 1 year later.
Pulmonary function tests
Pulmonary function testing was performed with the PC-basedKoKo spirometer (nSpire Health, Inc. Longmont, CO, USA) inaccordance with American Thoracic Society (ATS) recommen-dations (ATS 1994), with subjects in a sitting position andwearing nose clips. Spirometry was performed at similar timesof the day to minimize diurnal variation. Predicted normalvalues for lung function variables were obtained from theATS/ERS recommendations using NHANES reference equa-tion which adjusts for sex, age, and height and serves as themost appropriate reference value for African populations(Hankinson et al. 2010). The spirometer was calibrated dailyand operated within the ambient temperature. Technicians hadstandardized training before starting the study. Also spirometrytests were reviewed for quality control and assurance by anexpert pulmonologist, and if judged inadequate, spirometrywas repeated. Spirometry was interpreted as normal (forcedexpiratory volume in 1 s (FEV1)>80% predicted, FEV1/forcedvital capacity (FVC)>70 %), mild (FEV1≥80 % predicted,FEV1/FVC<70 %), moderate (30 %≤FEV1<80 % predicted,FEV1/FVC<70 %), and severe (FEV1<30 % predicted,FEV1/FVC<70 %) obstructions using the GOLD criteria foradults (Pauwels et al. 2001) and the ATS/ERS criteria forchildren (Celli and MacNee 2004). We measured FVC,FEV1, and peak expiratory flow rate (PEFR).
Phase II: distribution of improved cooking stovesand education awareness program
We distributed low-emission cooking stoves (Stovetec, Eugene,OR, USA) to all 59 homes. Instruction on how to operate thestoves was provided, and compliance visits were conductedevery 2 weeks over the 1-year period. After a year of monitoreduse, with home visits, inquiries about exclusive use of thedistributed stoves, and other questions, we repeated the surveyquestionnaire, monitored indoor air levels of PM2.5 and CO,and performed spirometry. The 1-year timeframe between base-line information and post-intervention for this study was select-ed to ensure we are able to compare our results with earlier
studies that have used the same timeframe to evaluate theeffectiveness of stove interventions on HAP and health insimilar rural settings in developing countries (Ezzati et al.2000; Romieu et al. 2009; Smith-Severtsen et al. 2009).
Data analysis
Descriptive analyses were conducted using mean, standarddeviation (SD), median, interquartile range (IQR), andcounts, based on distribution. Only the data obtained fromthe 59 households that were selected in the second stagesampling were included in the analysis. To investigate theeffects of intervention, a comparison of the pre- and post-intervention data was conducted using Wilcoxon sign ranktest for air pollutants, paired t test for respiratory functions,and McNemar test for exposure-related respiratory symp-toms. Differences were considered statistically significant atp<0.05. All statistical analyses were performed usingSTATA statistical software (Version 12.0).
The Institutional Review Boards on Human Research atthe University of Ibadan, Nigeria and the University ofChicago, USA gave ethical approval for the conduct of thestudy with approval number UI/EC/10/0045 and 10-263-B,respectively. All adult participants gave verbal and writtenconsent, while parents provided written informed consentfor children. Approval to conduct the study was alsoobtained from local community leaders.
Results
Household and cooking characteristics
Participants’ sociodemographic data are presented inTable 1. The mean age (± SD; years) of mothers and chil-dren were 43.0±11.7 and 13.0±2.5, respectively. Fifty per-cent of the mothers had no formal education. Firewood andcharcoal were the common sources of cooking energy with81 and 36 % households using them, respectively, while nohousehold used liquefied petroleum gas (LPG) and electricity.Households were poorly ventilated, with more than 60 %having one or no windows in the kitchen. None of the selectedhouseholds had access to electricity or LPG for cooking, areflection of the low socioeconomic status (SES) in thesefarming communities. In 58 % of households, averagecooking time was over 2 h daily.
Exposure-related symptoms
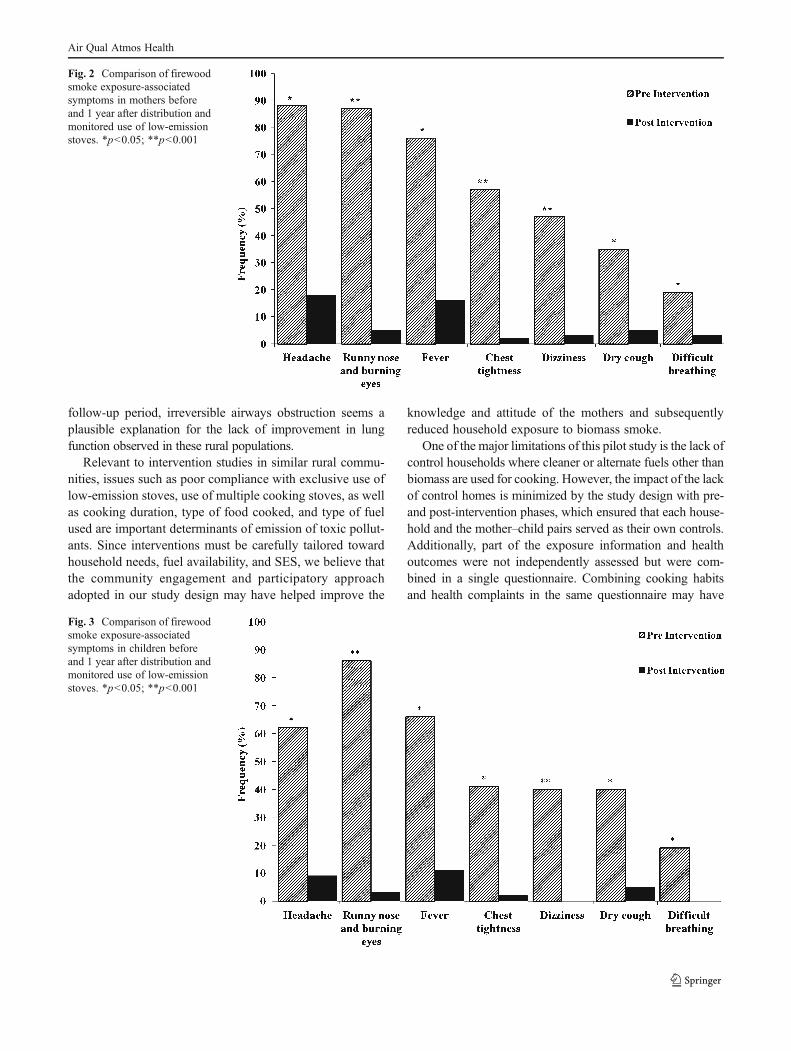
In the households surveyed, mothers and children reportedexposure-related symptoms. Headaches and burning eyeswere the most common symptoms in mothers (88 and87 %) and children (62 and 86 %), respectively. Also, chest
Air Qual Atmos Health
tightness and fever were reported in over 40 % of mothersand children.
Indoor air quality measurements
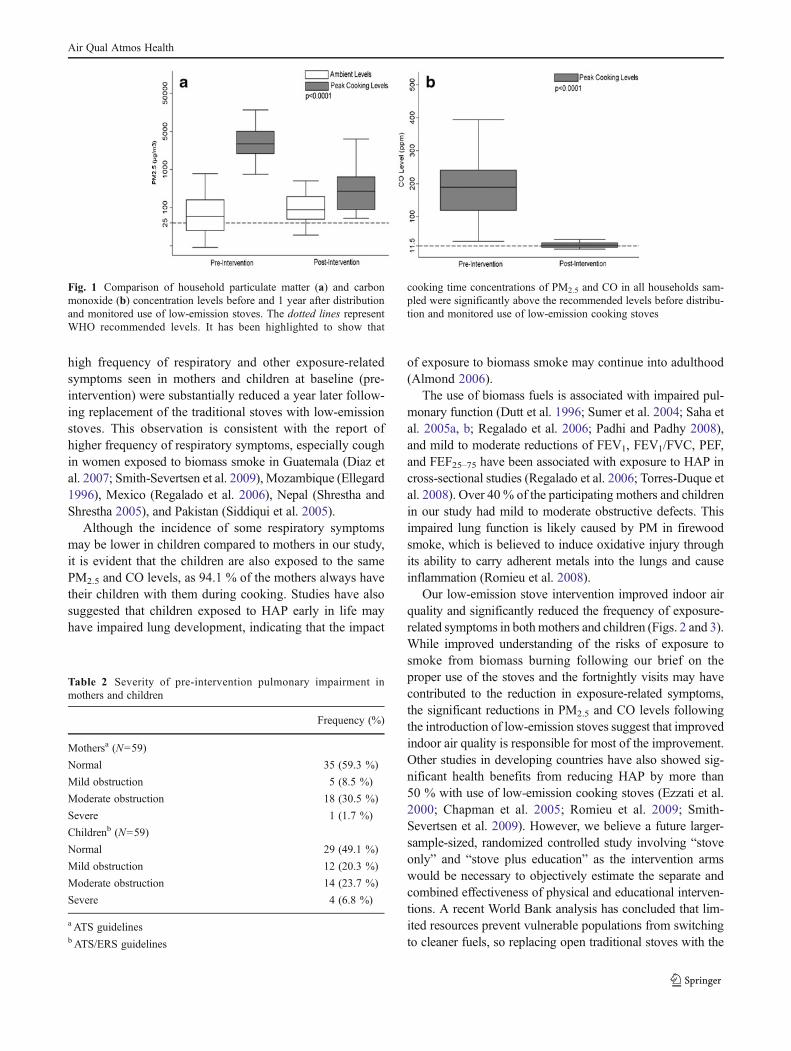
Data on PM2.5 and CO concentration levels are presented inFig. 1. Pre-intervention median concentrations of PM2.5 andCO during cooking were 1,414.4 μg/m3 (IQR 831.2–3,437.0)
and 170.3 ppm (IQR 116.3–236.2), respectively. Compared topre-intervention values, the PM2.5 concentration after 1 yearof monitored use of low-emission stoves was significantlyreduced to a median concentration of 130.3 μg/m3 (IQR 49.6–277.1; p<0.0001) while the CO concentration level wasalso reduced to a median value of 14.0 ppm (IQR 17.0–21.0; p<0.0001).
Lung function test
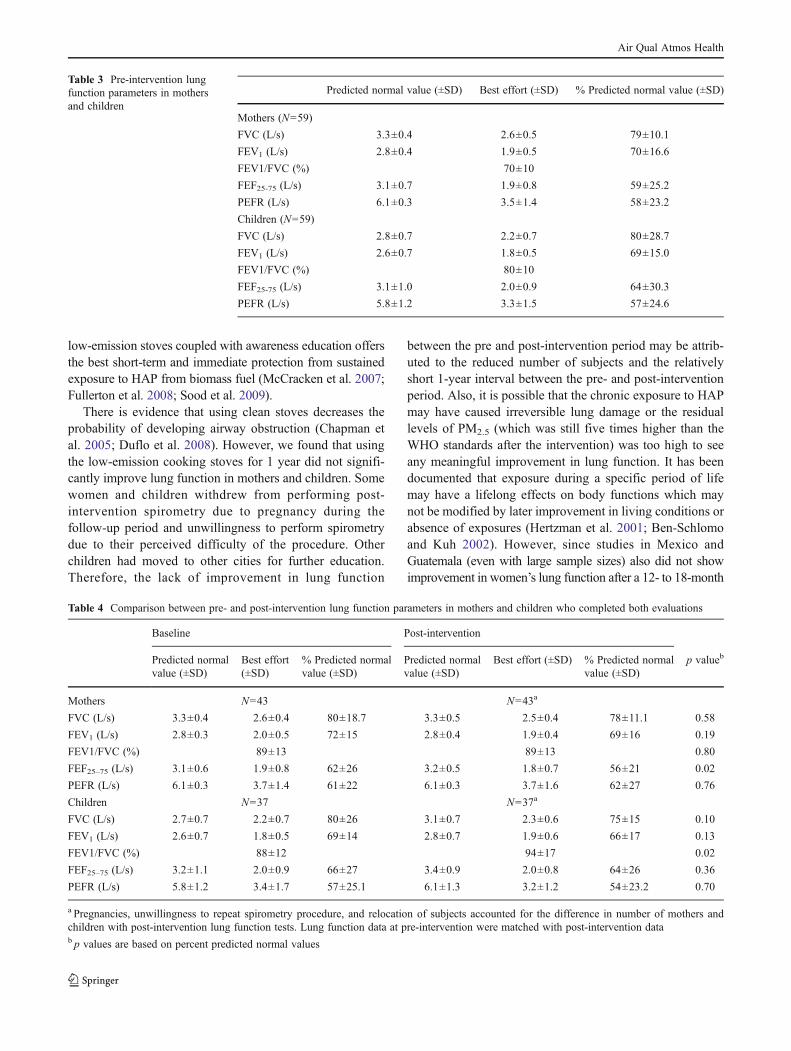
Table 2 shows details of participant’s pre-intervention lungfunction impairment. Over 30 % of mothers and childrenhad mild to moderate obstruction; 2 and 7 %, respectively,had severe obstruction (Table 3). However, no significantimprovement in lung function was observed after the 1-yearintervention period in mothers and children who completedpre- and post-intervention spirometry (Table 4).
Discussion
To our knowledge, this is the first study in Nigeria designed todetermine how much HAP is related to the widespread use ofbiomass fuel for cooking, its ultimate impact on the health ofmothers and children, and the effectiveness of low-emissioncooking stoves in improving indoor air quality, exposure-related symptoms, and lung function. WHO guidelines for 24-hmean levels of PMwith aerodynamic diameter 2.5 μg/m3 or lessis 25 μg/m3 (WHR 2005; Kurmi et al. 2008; Fullerton et al.2009), but we observed indoor levels of PM2.5 that were morethan 60-fold higher than WHO standards. Additionally, ambientconcentration levels of PM2.5 were also higher than WHO stan-dards (Fig. 1). While exposure levels may not be directly com-parable due to inconsistencies in timing and duration of samplingprocedures in earlier studies, our findings are relatively worsethan those reported in households using biomass fuel for cookinginGuatemala andMalawi, where 24-h average levels of PM2.5 ashigh as 528 and 226 μg/m3, respectively, were observed (Naeheret al. 2000; Fullerton et al. 2009).
While many earlier studies concerning particulate matter inhomes that use biomass fuels for cooking used total suspendedparticulate matter less than or equal to 10 μg/m3 (PM10) tomark exposure, our study focused on PM2.5, which is morereadily inhaled and deposited in the lower airways and alveoli,where they can induce more damage (Choi et al. 2004).Similarly, we observed indoor levels of CO during cookingin these households to be 20 times higher than WHOstandards (Fig. 1), and we believe this may have contributed tothe increased frequency of headaches and dizziness observedin exposed women and children.
We also demonstrated an association between cookingwith biomass fuel, increased prevalence of respiratorysymptoms, and presence of obstructive lung disease. The
Table 1 Sociodemographic variables of households surveyed
Characteristics Distribution, n (%) (N=59)
Age, years±SD
Mothers 43.0±11.7
Children 13.0±2.5
Education of mothers
No formal education 23 (38.9)
Primary school 20 (33.9)
Middle school 15 (25.4)
Higher education 1 (1.7)
Types of cooking fuela
Animal residue 2 (3.4)
Firewood 48 (81.4)
Charcoal 21 (35.6)
Kerosene 15 (25.4)
Liquefied 0
Electricity 0
Kitchen characteristics
Separate kitchen
Yes 45 (76.3)
No 14 (23.7)
Average cooking time per meal
1–2 h 20 (33.9)
3–4 h 22 (37.3)
5–6 h 14 (23.7)
>6 h 3 (5.1)
Cooking times per day
1 2 (3.4)
2 23 (39.0)
>2 34 (57.6)
Number of windows in kitchen
0 17 (28.8)
1 29 (49.2)
2 6 (10.2)
3 2 (3.4)
>3 3 (5.1)
Not available 2 (3.4)
Presence of children while cooking
Yes 56 (94.9)
No 3 (5.1)
a Households used combination of biomass fuels for cooking
Air Qual Atmos Health
high frequency of respiratory and other exposure-relatedsymptoms seen in mothers and children at baseline (pre-intervention) were substantially reduced a year later follow-ing replacement of the traditional stoves with low-emissionstoves. This observation is consistent with the report ofhigher frequency of respiratory symptoms, especially coughin women exposed to biomass smoke in Guatemala (Diaz etal. 2007; Smith-Severtsen et al. 2009), Mozambique (Ellegard1996), Mexico (Regalado et al. 2006), Nepal (Shrestha andShrestha 2005), and Pakistan (Siddiqui et al. 2005).
Although the incidence of some respiratory symptomsmay be lower in children compared to mothers in our study,it is evident that the children are also exposed to the samePM2.5 and CO levels, as 94.1 % of the mothers always havetheir children with them during cooking. Studies have alsosuggested that children exposed to HAP early in life mayhave impaired lung development, indicating that the impact
of exposure to biomass smoke may continue into adulthood(Almond 2006).
The use of biomass fuels is associated with impaired pul-monary function (Dutt et al. 1996; Sumer et al. 2004; Saha etal. 2005a, b; Regalado et al. 2006; Padhi and Padhy 2008),and mild to moderate reductions of FEV1, FEV1/FVC, PEF,and FEF25–75 have been associated with exposure to HAP incross-sectional studies (Regalado et al. 2006; Torres-Duque etal. 2008). Over 40 % of the participating mothers and childrenin our study had mild to moderate obstructive defects. Thisimpaired lung function is likely caused by PM in firewoodsmoke, which is believed to induce oxidative injury throughits ability to carry adherent metals into the lungs and causeinflammation (Romieu et al. 2008).
Our low-emission stove intervention improved indoor airquality and significantly reduced the frequency of exposure-related symptoms in bothmothers and children (Figs. 2 and 3).While improved understanding of the risks of exposure tosmoke from biomass burning following our brief on theproper use of the stoves and the fortnightly visits may havecontributed to the reduction in exposure-related symptoms,the significant reductions in PM2.5 and CO levels followingthe introduction of low-emission stoves suggest that improvedindoor air quality is responsible for most of the improvement.Other studies in developing countries have also showed sig-nificant health benefits from reducing HAP by more than50 % with use of low-emission cooking stoves (Ezzati et al.2000; Chapman et al. 2005; Romieu et al. 2009; Smith-Severtsen et al. 2009). However, we believe a future larger-sample-sized, randomized controlled study involving “stoveonly” and “stove plus education” as the intervention armswould be necessary to objectively estimate the separate andcombined effectiveness of physical and educational interven-tions. A recent World Bank analysis has concluded that lim-ited resources prevent vulnerable populations from switchingto cleaner fuels, so replacing open traditional stoves with the
Fig. 1 Comparison of household particulate matter (a) and carbonmonoxide (b) concentration levels before and 1 year after distributionand monitored use of low-emission stoves. The dotted lines representWHO recommended levels. It has been highlighted to show that
cooking time concentrations of PM2.5 and CO in all households sam-pled were significantly above the recommended levels before distribu-tion and monitored use of low-emission cooking stoves
Table 2 Severity of pre-intervention pulmonary impairment inmothers and children
Frequency (%)
Mothersa (N=59)
Normal 35 (59.3 %)
Mild obstruction 5 (8.5 %)
Moderate obstruction 18 (30.5 %)
Severe 1 (1.7 %)
Childrenb (N=59)
Normal 29 (49.1 %)
Mild obstruction 12 (20.3 %)
Moderate obstruction 14 (23.7 %)
Severe 4 (6.8 %)
a ATS guidelinesb ATS/ERS guidelines
Air Qual Atmos Health
low-emission stoves coupled with awareness education offersthe best short-term and immediate protection from sustainedexposure to HAP from biomass fuel (McCracken et al. 2007;Fullerton et al. 2008; Sood et al. 2009).
There is evidence that using clean stoves decreases theprobability of developing airway obstruction (Chapman etal. 2005; Duflo et al. 2008). However, we found that usingthe low-emission cooking stoves for 1 year did not signifi-cantly improve lung function in mothers and children. Somewomen and children withdrew from performing post-intervention spirometry due to pregnancy during thefollow-up period and unwillingness to perform spirometrydue to their perceived difficulty of the procedure. Otherchildren had moved to other cities for further education.Therefore, the lack of improvement in lung function
between the pre and post-intervention period may be attrib-uted to the reduced number of subjects and the relativelyshort 1-year interval between the pre- and post-interventionperiod. Also, it is possible that the chronic exposure to HAPmay have caused irreversible lung damage or the residuallevels of PM2.5 (which was still five times higher than theWHO standards after the intervention) was too high to seeany meaningful improvement in lung function. It has beendocumented that exposure during a specific period of lifemay have a lifelong effects on body functions which maynot be modified by later improvement in living conditions orabsence of exposures (Hertzman et al. 2001; Ben-Schlomoand Kuh 2002). However, since studies in Mexico andGuatemala (even with large sample sizes) also did not showimprovement in women’s lung function after a 12- to 18-month
Table 3 Pre-intervention lungfunction parameters in mothersand children
Predicted normal value (±SD) Best effort (±SD) % Predicted normal value (±SD)
Mothers (N=59)
FVC (L/s) 3.3±0.4 2.6±0.5 79±10.1
FEV1 (L/s) 2.8±0.4 1.9±0.5 70±16.6
FEV1/FVC (%) 70±10
FEF25-75 (L/s) 3.1±0.7 1.9±0.8 59±25.2
PEFR (L/s) 6.1±0.3 3.5±1.4 58±23.2
Children (N=59)
FVC (L/s) 2.8±0.7 2.2±0.7 80±28.7
FEV1 (L/s) 2.6±0.7 1.8±0.5 69±15.0
FEV1/FVC (%) 80±10
FEF25-75 (L/s) 3.1±1.0 2.0±0.9 64±30.3
PEFR (L/s) 5.8±1.2 3.3±1.5 57±24.6
Table 4 Comparison between pre- and post-intervention lung function parameters in mothers and children who completed both evaluations
Baseline Post-intervention
Predicted normalvalue (±SD)
Best effort(±SD)
% Predicted normalvalue (±SD)
Predicted normalvalue (±SD)
Best effort (±SD) % Predicted normalvalue (±SD)
p valueb
Mothers N=43 N=43a
FVC (L/s) 3.3±0.4 2.6±0.4 80±18.7 3.3±0.5 2.5±0.4 78±11.1 0.58
FEV1 (L/s) 2.8±0.3 2.0±0.5 72±15 2.8±0.4 1.9±0.4 69±16 0.19
FEV1/FVC (%) 89±13 89±13 0.80
FEF25–75 (L/s) 3.1±0.6 1.9±0.8 62±26 3.2±0.5 1.8±0.7 56±21 0.02
PEFR (L/s) 6.1±0.3 3.7±1.4 61±22 6.1±0.3 3.7±1.6 62±27 0.76
Children N=37 N=37a
FVC (L/s) 2.7±0.7 2.2±0.7 80±26 3.1±0.7 2.3±0.6 75±15 0.10
FEV1 (L/s) 2.6±0.7 1.8±0.5 69±14 2.8±0.7 1.9±0.6 66±17 0.13
FEV1/FVC (%) 88±12 94±17 0.02
FEF25–75 (L/s) 3.2±1.1 2.0±0.9 66±27 3.4±0.9 2.0±0.8 64±26 0.36
PEFR (L/s) 5.8±1.2 3.4±1.7 57±25.1 6.1±1.3 3.2±1.2 54±23.2 0.70
a Pregnancies, unwillingness to repeat spirometry procedure, and relocation of subjects accounted for the difference in number of mothers andchildren with post-intervention lung function tests. Lung function data at pre-intervention were matched with post-intervention datab p values are based on percent predicted normal values
Air Qual Atmos Health
follow-up period, irreversible airways obstruction seems aplausible explanation for the lack of improvement in lungfunction observed in these rural populations.
Relevant to intervention studies in similar rural commu-nities, issues such as poor compliance with exclusive use oflow-emission stoves, use of multiple cooking stoves, as wellas cooking duration, type of food cooked, and type of fuelused are important determinants of emission of toxic pollut-ants. Since interventions must be carefully tailored towardhousehold needs, fuel availability, and SES, we believe thatthe community engagement and participatory approachadopted in our study design may have helped improve the
knowledge and attitude of the mothers and subsequentlyreduced household exposure to biomass smoke.
One of the major limitations of this pilot study is the lack ofcontrol households where cleaner or alternate fuels other thanbiomass are used for cooking. However, the impact of the lackof control homes is minimized by the study design with pre-and post-intervention phases, which ensured that each house-hold and the mother–child pairs served as their own controls.Additionally, part of the exposure information and healthoutcomes were not independently assessed but were com-bined in a single questionnaire. Combining cooking habitsand health complaints in the same questionnaire may have
Fig. 2 Comparison of firewoodsmoke exposure-associatedsymptoms in mothers beforeand 1 year after distribution andmonitored use of low-emissionstoves. *p<0.05; **p<0.001
Fig. 3 Comparison of firewoodsmoke exposure-associatedsymptoms in children beforeand 1 year after distribution andmonitored use of low-emissionstoves. *p<0.05; **p<0.001
Air Qual Atmos Health

biased the health symptoms reported by the participants. Also,another possible bias could be in the reporting of symptoms.The participants in the intervention phase were not blinded tothe effects of the stove. This may have increased the tendencyof the women to report fewer symptoms because they knewwhat was expected from this new technology after the educa-tion awareness program. Such bias might have inaccuratelyincreased the estimated effect of the intervention on exposure-related symptoms experienced by the mother–child pairs.Although this is hard to assess in this study, we do not believethat this bias explains our results because we performed peri-odic assessment of stove use. In addition, the reductions inexposure-related health symptoms were so strong that we canbe confident that these reductions were likely related to theprotective effects of the improved cooking stoves because thepost-intervention reductions in exposure-related symptoms(including cough, fever, chest tightness, headache, dizziness,runny nose, and burning eyes) were substantial and occurredconcurrently with marked improvement in IAQ.
Despite these limitations, our results suggest that house-hold biomass fuel use causes significant HAP, which in-creases the likelihood of respiratory symptoms and/orobstruction in those exposed on a regular basis. We alsosuccessfully demonstrated that the distribution of low-emission stoves in combination with educating people asto its proper use is effective in improving indoor air quality,thereby protecting women and children from exposure-related respiratory symptoms. To our knowledge, this isthe first study in sub-Saharan Africa to demonstrate thatthe use of low-emission stoves and community engagementcan significantly improve indoor air quality and reduce therisk of respiratory symptoms. However, no significantimprovement in lung function was observed a year later,despite improved indoor air quality.
We hope these results lead to health policy changesaimed at mitigating the deleterious effects of exposure toHAP in mothers and children in Nigeria. This may includepolicies regarding construction of homes with better ventilatedkitchens and use of environmentally friendly, low-emission,and energy-efficient cooking stoves. These steps alone couldvastly improve the health of vulnerable women and childrenwho are the most exposed.
In conclusion, findings from our study support a scale-upmodel, which combines community engagement and partic-ipation, distribution, and monitored use of low-emissionstoves as a necessary strategy to protect vulnerable womenand children who use biomass fuel for cooking in Nigeriaand other developing countries.
Acknowledgments The Falk Medical Trust Foundation, USA andthe Chest Foundation of the American College of Chest Physiciansthrough the Humanitarian award to Christopher Olopade, MD, fundedthe project. The authors are also grateful to Healthy Life for All
Foundation (HLF), Ibadan, Nigeria, for assistance with project executionand to Rebecca Incledon for editorial assistance.
Conflict of interest None of the authors have a conflict of interest todeclare on this project.
References
Almond D (2006) Is the 1918 influenza pandemic over? Long-termeffects of in-utero influenza exposure in the post 1940 USApopulation. Journal of Political Economy 114(4):672–712
American Thoracic Society (ATS) (1994) Standardization of spirometry,1994 update. Am J Respir Crit Care Med 152(3):1107–1136
Ana G, Adeniji B, Ige O, Oluwole O, Olopade CO (2012) Exposure toemissions from firewood cooking stove and the pulmonary healthof women in Olrunda community, Ibadan, Nigeria. Air QualAtmos Health (online version). doi:10.1007/s11869-012-0183-6
Ben-Schlomo Y, Kuh D (2002) A life course approach to chronicdisease epidemiology: conceptual models, empirical challengesand interdisciplinary perspectives. Int J Epi 31:285–293
Bruce N, Perez-Padilla R, Albalak R (2000) Indoor air pollution indeveloping countries: a major environmental and public healthchallenge. Bull World Health Organ 78(9):1078–1092
Celli BR, MacNee W (2004) Standards for the diagnosis and treatmentof patients with COPD: a summary of the ATS/ERS positionpaper. Eur Respir J 23(6):932–946
Chapman RS, He X, Blair AE, Lan Q (2005) Improvement in householdstoves and risk of chronic obstructive pulmonary disease inXuanwei, China: retrospective cohort study. BMJ 331(7524):1050
Choi J, Kim J, Kim Y, Kim Y, Chung N, Cho M (2004) Comparativestudy of PM2.5- and PM10-induced oxidative stress in rat lungepithelial cells. J Vet Sci 5(1):11–18
Diaz E, Bruce N, Pope D, Lie RT, Diaz A, Arana B et al (2007) Lungfunction and symptoms among indigenous Mayan womenexposed to high levels of indoor air pollution. Int J TubercLung Dis 11(12):1372–1379
Duflo E, Greenstone M, Hanna R (2008) Cooking stoves, indoor airpollution and respiratory health in rural Orissa. Economic &Political Weekly 43(32):71–76
Dutt D, Srinivasa DK, Rotti SB, Sahai A, Konar D et al (1996) Effectof indoor air pollution on the respiratory system of women usingdifferent fuels for cooking in an urban slum of Pondicherry. NatlMed J India 9(3):113–117
Ellegard A (1996) Cooking fuel smoke and respiratory symptomsamong women in low income areas in Maputo. Environ HealthPerspect 104(9):980–985
Emmelin A,Wall S (2007) Indoor air pollution: a poverty-related cause ofmortality among the children of the world. Chest 132(5):1615–1623
Ezzati M, Mbinda MB, Kammen DM (2000) Comparison of emissionsand residential exposure from traditional and improved cook-stoves in Kenya. Environ Sci Technol 34(4):78–583
Fullerton DG, Bruce N, Gordon SB (2008) Indoor air pollution frombiomass fuel smoke is a major health concern in the developingworld. Trans R Soc Trop Med Hyg 102(9):843–851
Fullerton DG, Semple S, Kalambo F, Suseno A, Malamba R, HendersonG et al (2009) Biomass fuel use and indoor air pollution in homes inMalawi. Occup Environ Med 66(11):777–783
Hankinson JL, Kawut SM, Shahar E, Smith LJ, Stukovsky KH, BarrRG (2010) Performance of American Thoracic Society-recommended spirometry reference values in a multiethnic sampleof adults. Chest 137(1):138–145
Hertzman C, Power C, Matthew S, Manor O (2001) Using an interac-tive framework of society and lifecourse to explain self-ratedhealth in early adulthood. Soc Sci Med 53:1575–1585
Air Qual Atmos Health

Kurmi OP, Semple S, Steiner M, Henderson GD, Ayres JG (2008)Particulate matter exposure during domestic work in Nepal. AnnOccup Hyg 52(6):509–517
McCracken JP, Smith KR, Diaz A, Mittleman MA, Schwartz J (2007)Chimney stove intervention to reduce long-term wood smokeexposure lowers blood pressure among Guatemalan women.Environ Health Perspect 115(7):996–1001
Naeher LP, Leaderer BP, Smith KR (2000) Particulate matter andcarbon monoxide in highland Guatemala: indoor and outdoorlevels from traditional and improved wood stoves and gas stoves.Indoor Air 10(3):200–205
Naeher LP, Brauer M, Lipsett M, Zelikoff JT, Simpson CD, Koenig JQet al (2007) Woodsmoke health effects: a review. Inhal Toxicol19:67–106
Obueh J (2006) Methanol stoves for indoor air pollution reduction inDelta State, Nigeria. Bioling Point 52:26–29
Padhi BK, Padhy PK (2008) Domestic fuels, indoor air pollution, andchildren's health. Ann N YAcad Sci 1140:209–217
Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS (2001)Global strategy for the diagnosis, management, and preven-tion of chronic obstructive pulmonary disease. NHLBI/WHOGlobal Initiative for Chronic Obstructive Lung Disease(GOLD) Workshop summary. Am J Respir Crit Care Med163(5):1256–1276
Regalado J, Perez-Padilla R, Sansores R, Paramo RJI, Brauer M, PareP et al (2006) The effect of biomass burning on respiratorysymptoms and lung function in rural Mexican women. Am JRespir Crit Care Med 174(8):901–905
Romieu I, Castro-Giner F, Kunzli N, Sunyer J (2008) Air pollution,oxidative stress and dietary supplementation: a review. Eur RespirJ 31(1):179–197
Romieu I, Riojas-Rodriguez H, Marron-Mares AT, Schilmann A,Perez-Padilla R, Masera O (2009) Improved biomass stoveintervention in rural Mexico: impact on the respiratory healthof women. Am J Respir Crit Care Med 180(7):649–656
Saha A, Kulkarni PK, Shah A, Patel M, Saiyed HN (2005a) Ocularmorbidity and fuel use: an experience from India. Occup EnvironMed 62(1):66–69
Saha A, Rao NM, Kulkarni PK, Majumdar PK, Saiyed HN (2005b)Pulmonary function and fuel use: a population survey. Respir Res6:127
Salvi S, Barnes P (2010) Is exposure to biomass smoke the biggest riskfactor for COPD globally? Chest 138(1):3–5
Shrestha IL, Shrestha SL (2005) Indoor air pollution from biomassfuels and respiratory health of the exposed population in Nepalesehouseholds. Int J Occup Environ Health 11(2):150–160
Siddiqui AR, Lee K, Gold EB, Bhutta ZA (2005) Eyes and respiratorysymptoms among women exposed to wood smoke emitted fromindoor cooking: a study from southern Pakistan. Energy for Sus-tainable Development 9(3):58–66
Smith KR, Mehta S (2003) The burden of disease from indoor airpollution in developing countries: comparison of estimates. Int JHyg Environ Health 206(4–5):279–289
Smith KR, Dutta K, Chengappa C, Gusain PPS, Masera O, Berrueta V(2007) Monitoring and evaluation of improved biomass cook-stove programs for indoor air quality and stove performance:conclusion from the Household Energy and Health Project. Ener-gy for Sustainable Development 11:15–18
Smith-Severtsen T, Diaz E, Pope D (2009) Effect of reducing indoor airpollution on women's respiratory symptoms and lung function:the RESPIRE Randomized Trial, Guatemala. Am J Epidemiol170(2):211–220
Sood A, Peterson H, Blanchette C, Meek P, Belinsky S, Picchi M et al(2009) Wood smoke associated chronic obstructive pulmonarydisease (COPD) underappreciated in the United States. Am JRespir Crit Care Med 179:A4742
Sumer H, Turaclar UT, Onarlioglu T, Ozdemir L, Zwahlen M (2004)The association of biomass fuel combustion on pulmonary func-tion tests in the adult population of Mid-Anatolia. SozPraventivmed 49(4):247–253
Torres-Duque C, Maldonado D, Perez-Padilla R, Ezzati M, Viegi G,(Forum of International Respiratory Studies (FIRS) Task Force onHealth Effects of Biomass Exposure (2008) Biomass fuels and respi-ratory diseases: a review of evidence. ProcAmThorac Soc 5:577–590
World Health Organisation (WHO) (2004) Comparative quantificationof health risks: global and regional burden of disease attributableto selected major risk factor. WHO, Geneva
World Health Organization (WHO) (2007) Indoor air pollution takesheavy toll on health: WHO Country by country standing. WHO,Geneva. Available at: http://www.who.int/mediacentre/news/notes/2007/np20/en/index.html
World Health Report (WHR) (2005) Make every mother and childcount. World Health Organization Reports. Available at: http://whqlibdoc.who.int/whr/2005/9241562900.pdf
Zhang J, Smith KR (2003) Indoor air pollution: a global health concern.Br Med Bull 68:209–225
Air Qual Atmos Health