Embed Size (px)
Citation preview

EFFECT OF THE BOBATH CONCEPT ON UPPER LIMB
AND HAND FUNCTION IN STROKE INDIVIDUALS
WITH MODERATE TO SEVERE ARM DEFICIT
BY
MISS THANCHANOK PUMPRASART
A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF
THE REQUIREMENTS FOR THE DEGREE OF MASTER OF
SCIENCE (PHYSICAL THERAPY)
FACULTY OF ALLIED HEALTH SCIENCES
THAMMASAT UNIVERSITY
ACADEMIC YEAR 2017
COPYRIGHT OF THAMMASAT UNIVERSITY
Ref. code: 25605812030533ARL

EFFECT OF THE BOBATH CONCEPT ON UPPER LIMB
AND HAND FUNCTION IN STROKE INDIVIDUALS
WITH MODERATE TO SEVERE ARM DEFICIT
BY
MISS THANCHANOK PUMPRASART
A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF
THE REQUIREMENTS FOR THE DEGREE OF MASTER OF
SCIENCE (PHYSICAL THERAPY)
FACULTY OF ALLIED HEALTH SCIENCES
THAMMASAT UNIVERSITY
ACADEMIC YEAR 2017
COPYRIGHT OF THAMMASAT UNIVERSITY
Ref. code: 25605812030533ARL

Thesis Title EFFECT OF THE BOBATH
CONCEPT ON UPPER LIMB AND
HAND FUNCTION IN STROKE
INDIVIDUALS WITH MODERATE
TO SEVERE ARM DEFICIT
Author Miss Thanchanok Pumprasart
Degree Master of Science
Major Field/Faculty/University Physical Therapy
Faculty of Allied Health Sciences
Thammasat University
Thesis Advisor
Thesis Co-Advisor
Academic Year
Asst. Prof. Noppol Pramodhyakul,
Ph.D, PT.
Pagamas Piriyaprasarth, Ph.D, PT.
2017
Ref. code: 25605812030533ARL

(1)
ABSTRACT
Background/Aims:
Many chronic stroke individuals still have neurological deficits with
impairments and activity limitations. Most are unable to use their affected upper limb.
The therapy based on the Bobath concept could improve upper limb and hand function
in chronic stroke, yet its effect has not been clearly demonstrated in patients with
different degrees of deficit severity. Therefore, the aim of this study was to compare
the effectiveness of the Bobath therapy program on upper limb and hand function,
muscle tone, and sensation in chronic stroke with moderate to severe arm deficits.
Methods:
The current study was the quasi-experimental study. The intervention program
consisted of the preparation phase 15 minutes (passive stretching and muscle
mobilization), movement facilitation (shoulder flexion, scapular protraction, elbow
extension, wrist extension, finger extension and opposition), and task specific training
with and without objects (target location, reaching, and skilled grasp). The treatment
frequency was 3 days/ week for 6 weeks. In each session, participants practiced 20
repetitions per set, 3 sets per task. The Wolf Motor Function Test was used to evaluate
upper limb function. The Fugl-Meyer Assessment of upper extremity (FMA-UE), the
Modified Ashworth Scale (MAS), and the Revised Nottingham Sensory Assessment
(RNSA) was used to evaluate impairments.
Results:
The participants were chronic stroke individuals in community with moderate
arm deficits (n=13) and severe arm deficits (n=13). Almost all items of the WMFT
(functional ability scale and movement time) and the FMA-UE demonstrated
statistically significant improvements (p < 0.05) between pre and post interventions.
The MAS of shoulder adductors, wrist flexors, and finger flexors demonstrated
statistically significantly decrease post the intervention (p < 0.05). For sensory
assessment, only stereognosis demonstrated statistically significantly difference post
intervention
Ref. code: 25605812030533ARL

(2)
Conclusions:
The findings supported the use of the Bobath therapy program in 6 weeks for
enhancing upper limb and hand function as well as impairment minimization in chronic
stroke with moderate to severe arm deficits. Further investigation on the retention effect
such as at 3, 6 months, and one year post intervention is warrant.
Keyword Bobath therapy, chronic stroke, upper limb and hand function, arm deficits
Ref. code: 25605812030533ARL

(3)
ACKNOWLEDGEMENTS
I would like to express my sincere gratitude to my advisor Asst. Prof. Noppol
Pramodhyakul and Pagamas Piriyaprasarth for their excellent academic support, good
advice and continuous supervision during entire process of dissertation.
I would like to thank all participants of this study. The thesis could not have
been completed without their participation. I am extremely thankful to the research
assistants for their great effort and valuable time. I am grateful to village health
volunteers and all authority who participated in Khlongluang municipality, Thaklong
municipality and Rangsit city municipality for contacting participants.
I would like to thank Thammasat University for research fund. It would not be
possible for me without their support. Finally, I would like to thank my family and my
friends for their assistance.
Miss Thanchanok Pumprasart
Ref. code: 25605812030533ARL

(4)
TABLE OF CONTENTS
Page
ABSTRACT (1)
ACKNOWLEDGEMENTS (3)
LIST OF FIGURES (9)
LIST OF TABLES (10)
CHAPTER 1 INTRODUCTION 1
1.1 Background and rationale 1
1.2 Research question 3
1.3 Objective 3
1.4 Research hypothesis 3
1.5 The variables used in the study 5
1.6 Potential benefits of the study 5
CHAPTER 2 LITERATURE REVIEW 6
2.1 Stroke 6
2.1.1 Definition 6
2.1.2 Incidence of stroke 6
2.1.3 Impairments post stroke 7
2.1.4 Problems of arm deficits post stroke 7
2.1.5 Recovery after a stroke 8
2.1.6 Factors affecting recovery of stroke 9
2.1.7 The prognosis of arm recovery post stroke 9
Ref. code: 25605812030533ARL

(5)
2.2 Interventions for improving upper limb
and hand function in patients with stroke 10
2.3 Bobath therapy 12
2.3.1 Bobath concept 12
2.3.2 Theoretical underpinning the Bobath concept 13
2.3.3 Bobath approach for upper limb
and hand function improvement 14
2.3.4 Clinical applications of Bobath therapy 14
2.4. Measurements of impairments and function of upper limb and hand 15
CHAPTER 3 MATERIAL AND METHOD
3.1 Intra- and Inter-rater reliability test of the Wolf Motor Function Test and
Fugl-Meyer assessment of the upper extremity 18
3.1.1 Participants (Patients with stroke) 19
3.1.1.1 Sample size 19
3.1.1.2 Inclusion criteria 21
3.1.1.3 Exclusion criteria 21
3.1.2 Assessors 22
3.1.3 Assessment tools and equipment 22
3.1.4 Method 23
3.2 Effect of the Bobath therapy on upper limb and hand function in stroke
individuals with moderate to severe arm deficit 23
3.2.1 Participants (patients with stroke) 23
3.2.1.1 Sample size 23
3.2.1.2 Sampling 25
3.2.1.3 Discontinuous criteria 25
3.2.2 Trainer 25
3.2.3 Assessors 25
Ref. code: 25605812030533ARL

(6)
3.2.4 Assessment tools and equipment 25
3.2.5 Research design and setting 27
3.2.6 Method 27
3.2.7 Assessment 27
3.2.8 Variables 27
3.2.9 Interventions 28
3.2.9.1 Intervention Program 29
3.2.9.2 Bobath therapy 31
3.3 Data Analysis 41
CHAPTER 4 RESULTS
4.1 Intra- and inter-rater reliability test of the Wolf Motor Function
Test and the Fugl-Meyer Assessment of the upper extremity 42
4.1.1 Intra- and inter-rater reliability test of
the Wolf Motor Function Test 42
4.1.2 Intra- and inter-rater reliability test of
the Fugl-Meyer assessment of the upper extremity 47
4.2 Effect of the Bobath therapy on upper limb and hand function in
stroke individuals with moderate to severe arm deficits 48
4.2.1 Characteristics of the participants in the reliability study 49
4.2.2 Wolf Motor Function Test (movement time) of the affected side 51
4.2.3 Wolf Motor Function Test (functional ability scale)
of the affected side 52
4.2.4 Fugl-Meyer assessment of the upper extremity 53
4.2.5 Modified Ashworth Scale 57
Ref. code: 25605812030533ARL

(7)
4.2.6 Revised Nottingham Sensory assessment 58
CHAPTER 5 DISCUSSION
5.1 Intra- and inter-rater reliability test of the Wolf Motor Function Test
and the Fugl-Meyer assessment of the upper extremity 59
5.2 Effect of the Bobath therapy on upper limb and hand function
in stroke individuals with moderate to severe arm deficits 59
5.2.1 The characteristics of participants 61
5.2.2 The effect of the Bobath therapy on upper limb
and hand function 61
5.2.3 The effect of the Bobath therapy on upper limb
and hand impairments 65
5.2.3.1 Muscle tone 66
5.2.3.2 Sensation 69
CHAPTER 6 CONCLUSION 73
REFERENCES 74
APPENDICES
APPENDIX A Ethical approval 91
APPENDIX B Information sheet 94
APPENDIX C Informed consent form 110
APPENDIX D General data form 116
APPENDIX E Thai version - The Mini–Mental State Examination 117
Ref. code: 25605812030533ARL

(8)
APPENDIX F Visual Analog Scale 121
APPENDIX G Wolf Motor Function test 122
APPENDIX H Fugl - Meyer Assessment (upper extremity) 124
APPENDIX I Modified Ashworth Scale 128
APPENDIX J Revised Nottingham Sensory Assessment 129
APPENDIX K Raw data
Intra- rater and inter-rater reliability test of the Wolf Motor Function
Test and the Fugl-Meyer assessment of the upper extremity 134
APPENDIX L Raw data
Effect of the Bobath therapy on upper limb and hand function in
stroke individuals with moderate to severe arm deficits 145
APPENDIX M Result
Comparison between moderate and severe level of severity 174
Ref. code: 25605812030533ARL

(9)
LIST OF FIGURES
Page
Figure 1.1 Conceptual framework 4
Figure 2.1 Recovery after a stroke 8
Figure 3.1 Experimental flowchart 40
Figure 4.1 Participant flowchart 48
Ref. code: 25605812030533ARL

(10)
LIST OF TABLES
Tables Page
Table 3.1 Assessment (pre-intervention) 28
Table 3.2 Detail of intervention 29
Table 3.3 Preparation for treatment 30
Table 3.4 Bobath therapy 31
Table 4.1.1 Characteristics of the participants 43
Table 4.1.2 Intra and inter-rater reliability of the
Wolf Motor Function Test (movement time) of the affected side 44
Table 4.1.3 Intra- and inter-rater reliability of the Wolf Motor Function Test
(movement time) of the less-affected side 45
Table 4.1.4 Intra- and inter-rater reliability of the
Wolf Motor Function Test (functional ability scale)
of the affected side 45
Table 4.1.5 Intra- and inter-rater reliability of the
Wolf Motor Function Test (FAS) of the less-affected side 46
Table 4.1.6 Intra- and inter-rater reliability of the
Fugl-Meyer assessment of the upper extremity 47
Table 4.2.1 Characteristics of the participants 50
Table 4.2.2 Pre- and post-assessment of the Wolf Motor Function Test
(movement time) of the affected side 51
Ref. code: 25605812030533ARL

(11)
Table 4.2.3 Pre- and post-assessment of the Wolf Motor Function Test
(functional ability scale) of the affected side 52
Table 4.2.4 Pre-assessment and post-assessment of the
Fugl-Meyer assessment of the upper extremity 53
Table 4.2.5 Pre-assessment and post-assessment of the
Modified Ashworth Scale 57
Table 4.2.6 Pre-assessment and Post-assessment of the
Revised Nottingham Sensory assessment 58
Ref. code: 25605812030533ARL

1
Chapter 1
Introduction
1.1 Background and rationale
Stroke or cerebrovascular accident is a global public health problem. The incidence
of stroke is almost 17 million each year worldwide (1) . In Thailand, the incidence of
stroke is estimated to be more than 250,000 new stroke cases each year (2). The situation
worldwide and in Thailand demonstrated that stroke is the common non-communicable
disease of the global population.
Stroke could lead to disabilities. Chronic stroke individuals could still have
neurological deficits with impairments and activity limitations. Most patients with
stroke are unable to use their affected upper limb. Only fourteen percent of stroke
survivors with severe arm deficits have full recovery of upper limb and hand function
(3). Problems of those with moderate to severe arm deficits are reach and grasp
incoordination, delay in time to maximal grip aperture (TMA), prolong movement time
(reach to grasp), and lack of accuracy (4, 5). Physical therapy is essential for the stroke
individuals with moderate to severe motor deficits to improve their functional ability
(3).
Interventions for improving upper limb and hand function are various. Bobath
therapy, task- specific training (6), sensorimotor training (7), mental practice (8), orthosis
(9), constraint- induced movement therapy (10), EMG/ Biofeedback (11), functional
electrical stimulation ( FES) (12), mirror therapy (13), robot- assisted therapy (14), virtual
reality (15) are the examples of interventions for improving upper limb and hand function
post stroke. Nevertheless, handling technique is applicable for stroke survivors in
community given no specific tools are required. The rehabilitation at patient’ s home
could also reduce cost and benefit for patients (16). Most interventions of upper
extremity have been reported for improving function in the stroke patients with mild to
moderate arm paresis. Interventions for improving severe arm deficits are less available
and details were unclear. The patients with mild paresis have ability to do activity of
Ref. code: 25605812030533ARL
2
daily living more than those with other levels of deficits. They may increase in their
upper limb and hand function as a result of activities performing in daily life. In
addition, the evidence of therapy based on the Bobath concept in chronic stroke very
few. All in all, interventions for improving upper limb and hand function in stroke
patients with moderate and severe paresis should be further investigated.
The Bobath concept is one of the first neurological physical therapy approaches
used in the management of patients following neurological deficits. The Bobath concept
is one of most commonly uses for rehabilitation in patients with central nervous system
disorders (17). The Bobath therapy focuses on postural control, selective movement,
and sensorimotor integration (18). Studies have been shown that when a person started
moving their upper extremities, postural tone has been adapted earlier ( anticipatory
postural adjustment ( APA) ) (19). In a previous study, therapy based on the Bobath
concept showed improvement of upper limb and hand function in chronic stroke (20).
However, the implementation of the Bobath concept on upper limb and hand function
in stroke individuals are limited due to the lack of specific details of treatment as well
as flaws in research methodology. The details of the Bobath intervention programs were
unclear regarding therapeutic doses in previous studies (21, 22). The arguments and
summary that the Bobath therapy is not better than other approaches are bias- hidden.
For example, having non-equivalent doses of treatments was aiming to verify the
effectiveness of another treatment as compared to the Bobath therapy (22, 23). In addition,
there was no study regarding chronic stroke with different degrees of deficit severity in
terms of community based rehabilitation. Together with few effective interventions to
improve upper limb and hand function in those with severe deficits, the aim of this
study was to investigate the effect of the Bobath therapy for improving upper limb and
hand function in chronic stroke with moderate to severe arm deficits.
As the presented in figure 1.1, the conceptual framework consisted of the activity
limitation, problem in moderate and severe arm deficits impairments, the Bobath
therapy and the recovery.
Ref. code: 25605812030533ARL

3
1.2 Research question
Could the Bobath therapy improve arm and hand functions in chronic stroke with
moderate to severe arm deficits?
1.3 Objectives
Primary objectives
1.3.1 To compare pre- post intervention effectiveness of the Bobath
therapy on upper limb and hand functions in chronic stroke with
moderate to severe arm deficits.
Secondary objectives
1.3.2 To compare pre- post intervention effectiveness of the Bobath
therapy on motor impairments, muscle tone, and sensation of upper
limb and hand in chronic stroke with moderate to severe arm
deficits.
1.4 Research hypotheses
1.4.1 There will be a difference of upper limb and hand functions
between pre- and post-intervention.
1.4.2 There will be differences in motor impairments, muscle tone, and
sensation of upper limb and hand between pre- and post-
intervention.
Ref. code: 25605812030533ARL

4
Chronic stroke
Problems in moderate and severe arm deficits
Impairment
o Muscle weakness
o Decrease ability to control movement
o Slow movement and less accuracy
o Reach/grasp incoordination
o Minimal grip aperture
o Delay in movement time
Bobath therapy
- Addressed on anticipatory postural adjustment (APA)
- Selective movement for co-ordinated sequences of
movement
- Sensorimotor integration through specific handlings
Recovery
Primary outcome measure
Wolf Motor Function Test
Secondary outcome measures
Fugl Meyer Assessment - UE
Modified Ashworth Scale
Revised Nottingham Sensory Assessment
Figure 1.1 Conceptual framework
Activity limitation
- Reaching
- Grasping
- Holding
- Releasing
Ref. code: 25605812030533ARL

5
1.5 The variables used in the study
1.5.1 Independent variables: time period: pre and post intervention of the
Bobath therapy for improving upper limb and hand functions.
1.5.2 Dependent variables: upper limb and hand function as assessed by
using the Wolf Motor Function Test, and impairments by using the
Fugl-Meyer assessment of the upper extremity (FMA-UE), the
Modified Ashworth Scale, and the revised Nottingham Sensory
Assessment.
1.6 Potential benefits of the study
1.6.1 To provide the effectiveness of the Bobath therapy on upper limb and
hand functions in chronic stroke individuals with moderate to severe
deficits.
1.6.2 To provide the insights of clinical applications in stroke individuals
with moderate to severe arm and hand functions for physical
therapists.
Ref. code: 25605812030533ARL

6
Chapter 2
Literature review
This chapter detailed the literature review related to the topic of research
proposal on stroke, Bobath Concept, and interventions for improving upper limb and
hand function post stroke.
2.1 Stroke
2.1.1 Definition
By the definition of WHO, stroke or cerebrovascular accident (CVA) is a
disorder within specific arteries in the brain. The neurological symptoms
persisted at least 24 hours leading to disabilities or could lead to death (1). Causes
of stroke are arterial occlusion, stenosis or hemorrhage (24). Symptoms and
severity of stroke depend on the lesion. Stroke is accounted for a period of time
after having a stroke one month to six months. Finally, chronic stroke is
accounted for a period of time after having a stroke longer than six months (2 5 ,
2 6 ) . Stroke is classified by 2 types according to pathology of stroke which are
ischemic and hemorhagic stroke. Hemorhagic stroke cause from rupture of the
cerebral vessels, due to high blood pressure excessive on arterial walls. Ischemic
strokes or cerebral infarcts (CI) are the result of development of thrombosis,
embolus leading block and affect to deficiency of oxygen pass to brain tissues
(27).
2.1.2 Incidence of stroke
Stroke is one of the most common non-communicable diseases. The
incidence of stroke worldwide has been occures almost 17 millions per year so
the campaign stroke awareness was developed for pleple. The incidence of
stroke is increasing every year in Thailand (2) and evidenced in 2552-2557 BE
(28). More than 250,000 new cases with stroke is estimated each year (2). The
female has been incidence of stroke (1 in 5 people) higher the male (1 in 6
people) was reported from world stroke organization (WSO) (29). Age at onset
of most patients with stroke worldwide is older than 65 years (30). The average
Ref. code: 25605812030533ARL
7
age is 45 - 64 years (31). Similary in Thailand, patients with stroke are 45 - 64
years and most are older than 65 years (32).
2.1.3 Impairments post stroke
Impairments of stroke are varied across individuals. The impairments
include deficits in motor function, cranial nerve function (speech, swallowing),
muscle weakness, altered reflexes, postural instability, coordination problems
and apraxia. Impairments of the sensory system included loss or impaired
sensation, and perceptual disorders (33). Patients may feel numbness, tingling
and hyper-sensitivity. Moreover, they could have more complex sensory
deficits such as astereognosis, agraphia and loss of double stimultaneous
stimuli. Impairments of the visual system included monocular blindness and
cortical blindness. In addition, some patients may have deficits in cognition and
emotion. They may have problems of memory, attention and mood disorders
such as depression. The important one is motor impairment including deficits
in motor function and functional limitation of the upper limb and hand function
is the major problem of activity daily living in stroke patients (34).
2.1.4 Problems of arm deficits post stroke
Most patients with stroke were unable to use their affected upper limb. It
has been reported that around eighty percent of patients with arm deficits post
stroke had incomplete recovery after six months (35). The severity of arm deficits
ranged from mild to severe. The severity of arm deficits has been defined based
on Fugl-Meyer score as mild > 50/66, moderate 26-50/66, and severe < 26/66
(36). Another criteria that have been used to identify those with mild to moderate
arm deficits is active range of wrist extension of at least twenty degrees and
finger extension ten degree. Previous study showed that most chronic stroke in
community are mild paresis (36 percent), followed by severe (14 percent) and
moderate paresis (10 percent) (37). One study showed that most patients with
Ref. code: 25605812030533ARL

8
mild arm paresis have full recovery (78 percent) and only few of those with
severe arm paresis have full recovery (18 percent) at 11 weeks post stroke (3).
Problems of those with severe arm deficits are incoordination of arm and
hand during reach to grasp, delay in time to maximal grip aperture (TMA),
minimal grip aperture (aperture scaling during reach to grasp), prolong
movement time in reach to grasp, lack of accuracy, and muscle weakness (4, 5).
2.1.5 Recovery after a stroke
Following a stroke, motor recovery is rapid within 30 days and gradually
continued to 90 days. Recovery reaches the plateau after 90 days to six months
(38).
Figure 2.1 Recovery post stroke in patients with different levels of severity (A)
mild level, (B) moderate level, (C) severe level, and (D) very severe level (38).
In Figure 2.1, neurologic means the neurological examination such as
muscle strength, reflex, sensation, conscious (39) and functional means the
ability to perform function such as ADL (40).
Ref. code: 25605812030533ARL

9
2.1.6 Factors affecting recovery of stroke
There are several factors affecting effective interventions. First, the patient
with recurrence stroke mostly presented with severe activity limitations than
patients with first stroke, and especially if the recurrence occurred in the other
side of first stroke (41). Second is the severity of weakness (42). Patients with
severe weakness of contralateral arm (active wrist extension less than 20° and
finger extension at less than 10°) have shown slow recovery (10). Third, control
of dominant arm and non-dominant arm movements are different in chronic
stroke patients (43). In addition, cognitive impairments have been shown to have
a negative effect on the patient’s functional independence (44).
2.1.7 The prognosis of arm recovery post stroke
The initial severity of muscle weakness is the major prognosis of arm
recovery post stroke (45). Nevertheless, 14 percent of stroke survivors with
severe arm deficits have full recovery of upper limb and hand function within
11 weeks (3). The recovery does not depend on genders, ages, and types of stroke
(46) but depend on neuroplasticity and physical rehabilitation. Physical
rehabilitation could make permanent change of neural function through motor
learning. In which, neuroplasticity is the process of neuronal changes of neurons
such as connection between neurons. These resulted in the recovery of function
post stroke (47). Ability to move the affected arm within 23 days post stroke
indicated a good prognosis (48) and if arm cannot move and grasp cannot be
made at four weeks post stroke indicated poor prognosis (49).
One study investigated arm function recovery after stroke over a period of
four years. Even after sixteen weeks, improvement still occurred in some stroke
patients. Nevertheless, effective treatments could improve arm functions and
decrease disabilities (50). Physical therapy addressing upper limb and hand
function training is important for improving patient’ s ability to perform daily
living activities independently (51) or with minimal assistance, social
participation, and quality of life (52). In addition, one previous study has shown
that chronic stroke patients with severe arm paresis (FMA-UE score 0-25) had
Ref. code: 25605812030533ARL

10
some improvements after upper limb training half an hour per day for 30 days
(FMA score increased 0 – 6 points) (37).
In addition, the repetition of training is a current focus as a factor of
recovery. In chronic stroke patients with moderate paresis, the typical number
of home- based functional muscle strengthening repetitions in a single session
was 12 per task in 30 minutes and three sessions per week. This amount of
training resulted in good outcomes for the upper-extremity level of activity (53).
Another observational study reported the average number of 32 repetitions per
session consisting of task- specific, functional upper extremity movements in
upper limb rehabilitation for stroke. The average session duration was 36
minutes (54). It is may be not adequate to recovery neural reorganization
poststroke. In one study, 300 repetitions of various tasks, 60 minutes per day, 4
days per week of high- repetition upper- extremity task- specific training in 19
sessions demonstrated improvement in impairments and activities (55).
2.2 Interventions for improving upper limb and hand function in patients with
stroke
Interventions for improving upper limb and hand function are various (56). Bobath
therapy is one of the pioneer interventions originally addressed on the use of the
affected side. Through the development of intervention and the updated knowledge on
neurosciences, currently the Bobath therapy is focused on anticipatory postural
adjustment (APA), selective movement, and sensorimotor integration (18). Task-specific
training is focused on motor learning and experience influencing neural plasticity (6).
Sensorimotor training used the principle of sensory information to stimulate motor
output (7). Mental practice is the intervention focused on motor imagery and improved
performance ( 8 ) . Orthoses have the purpose to reduce spasticity and pain, prevent
contracture and edema, and assist in the improvement of function ( 9 ) . Constraint-
Induced Movement Therapy (CIMT) is the intervention limiting the movement of the
less-affected side while shaping the movements of the affected side (57). EMG/
Biofeedback is the intervention focused on audio or visual feedback on eliciting
movements (11) and Functional Electrical Stimulation (FES) assisted movement via
Ref. code: 25605812030533ARL

11
electrical stimulation (12). Mirror therapy is the intervention focused on visual imagery
to convey visual stimuli (1 3 ) . Music Upper Limb Therapy- Integrated (MLT-I) is the
intervention focused on physical, psychological and social domains of rehabilitation
(58). Arm Weight Support training is using the ArmeoSpring for recovery arm and hand
(59).
Some other interventions addressed on minimizing impairments such as strength
training, stretching. Complementary interventions are robotics training (13), bilateral
arm training (60), Virtual Reality training (61), Transcranial magnetic stimulation (TMS)
(6 2 ) and rehabilitation program in community. After discharging from acute hospital,
patients with stroke are either referred back to another hospital or their own homes
depending on their medical conditions and health care needed. In Thailand, most
patients with stroke are discharged to their own homes in community and may are
unable to access health care as needed due to limitation in access or other personal
issues. Without rehabilitation, they may have been left with activity limitation and
disabilities. Rehabilitation at home has many advantages for the patients, especially for
those who have trouble accessing health care sectors (63).
A study on stroke rehabilitation in UK community addressing reach to grasp
training showed that the patients have the improvement of reaching. Training in this
study consisted of active movement of shoulder flexion, with and without gravity effect
and reaching training in various directions. The total treatment time was 14 hours in six
weeks.
One previous study investigated the effectiveness of standardized rehabilitation
program consisting of active exercise, resisted exercise, and ADL training in patients
with stroke in a local hospital setting in Thailand. The results showed that the
rehabilitation program could improve function and quality of life for patients
(64). Physical therapy interventions addressing on improving, endurance, strength
balance, flexibility, strength and upper- limb function has been reported to improve
daily living activities (65). The home- based program has also been reported for its
effectiveness in subacute and chronic stroke in improving recovery and maintaining
their functional ability (66).
Ref. code: 25605812030533ARL

12
In previous study, the effect of interventions of moderate to severe arm deficits have
similar efficiencies that increasing the performance and the speed of movement. The
most of study have no significant between groups.
2.3 Bobath therapy
2.3.1 Bobath concept
This approach was invented by Berta Bobath, a physiotherapist
and pediatrician Dr. Karel Bobath who believed that appropriate treatment for
patients with paralyzed body parts is to stimulate the movement of those parts
by means of movement facilitation through sensory stimulation (1 7 ) .
Neuroscience knowledge has been applied to explain the efficacy
of therapy based on the Bobath Concept.
The important aim of the therapy followed the Bobath concept is to
improve quality of movement. Quality of movement is the characteristic of
behavior movement which is important for effective neuro - rehabilitation
strategies (17, 67). The Bobath concept focuses on postural control for stabilizing
the trunk while moving limbs, maintain alignment and preparation of a joint
movement. Selective movement is the other main focus of this concept to
control specific movement and limit abnormal movement pattern. Last is the
address on sensorimotor integration to improve effective movement. Sensory
inputs contribute on motor learning and shaping motor output (68). The sensory
information is the essential in the specification and regulation of activation
thresholds of movement (69).
For motor relearning, therapists can use sensory inputs in the form of
tactile information from the hands to shape movement and gradually removing
manual guidance when the capable of self- generated movement has been
achieved. Proper placing of the therapist’s hands is thought to guide a patient to
move their limbs in the target movement. The cutaneous and other sensory
signals can adapt motor output (70).
Ref. code: 25605812030533ARL

13
Sensory receptors included those in joints (stimulated through
compression and distraction), Golgi tendon organs, cutaneous receptors, muscle
spindles are involved in movement facilitation. Sensory and proprioceptive
information through handling at key points of control are used as feedback and
facilitation strategy (17, 19). Thus, sensory guidance is the principles of movement
production.
2.3.2 Theoretical underpinning the Bobath concept
The Bobath therapy is based on system model of motor control, theory of
plasticity and motor learning. Motor control is the control of movement in the
interaction with various tasks and environment. Within individual person,
movement is contributed by the coordination between perception, cognition and
action. Many systems are involved in the integration and response to the
succession of motor goals (17).
Motor control is the current theoretical underpinning of the Bobath
concept. It was important to have understanding the movement system. The
control of integrated movement to interacting systems cooperative work (71).
The emphasis of the Bobath concept is on motor control based upon a
continuous interaction of individuals. This is based on a nervous system
working with theory of motor control and multilevel processing (19).
The plasticity of nervous structures is the modification or changes from
motor learning and the practice (72, 73). The nervous system and neuromuscular
system can adapt or change the structure based on experiences and effective
functional goals in a variety of environments.
Motor learning refers to permanent change in motor performance (72). The
motor learning requires active participant, practice and meaningful goals. There
are essential for learning (74).
Ref. code: 25605812030533ARL

14
2.3.3 Bobath approach for upper limb and hand function improvement
The Bobath approach could be applied to any body parts including trunk
and limbs. Approaches for upper limb and hand function have been designed to
tailor individual’ s problems. This included reaching, joint realignment, hand
shaping, and fine movement (18). Treatment addressed selective movement
while concerning postural control through specific handlings. After facilitation
of individual joint movement, functional training is advice for patients to learn
movement in function. Target location and skilled grasp are the example of
training together with movement facilitation.
2.3.4 Clinical applications of the Bobath therapy
Studies on the effectiveness of the Bobath therapy showed improved
upper limb and hand function (22, 23, 75). There were assessed by the Fugl-Meyer
for upper extremity, Wolf Motor Function Test, Action Research Arm Test
(ARA), joint motion/ pain scores, Motor Evaluation Scale, functional ability,
speed of movement, quality of movement, hand functions and ADL in the
affected arm (22, 76).
The Bobath therapy in the literature review of arm activity training has
been performed in various situations such as reaching the object on the floor,
side lateral and various other positions. The physical therapist provided training
for the patients with or without objects. The duration of a treatment session
varied from 30 to 60 minutes, with the most frequent report of 45 minutes. The
frequency of treatment varied from five days or less per weeks and the total
period of treatment varied from two weeks to six months (22, 75).
The Bobath therapy has been compared with CIMT, arm basis training,
and motor relearning program. In which, there were no significant difference
between groups, but significant differences were found pre and post
intervention within each group (22, 75, 77). However, when the Bobath therapy
study was compared with orthopedic approach there was a significant difference
Ref. code: 25605812030533ARL

15
between groups. That is, the Bobath therapy improved the function of upper
limb and hand post intervention better than the orthopedic approach (20).
2.4. Measurements of function and impairments of upper limb and hand
There are several existing measures for assessing upper limb and hand function in
patients with stroke. For example, Action Research Arm Test (ARAT) has been
designed to assess upper limb and hand dexterity (78), Box and Block Test is used for
assessing performance of gross dexterity (79). The Chedoke - McMaster Stroke
Assessment Scale (CMSA) is used for assessing physical impairment inventory and a
disability inventory (80), Wolf Motor Function Test (WMFT) is designed for assessing
upper extremity motor function (81).
The aim of the Wolf Motor Function Test (WMFT) is to assess upper extremity
motor function for patients with stroke. The WMFT is an assessment tool with high
inter-rater reliability, internal consistency, test-retest reliability, and adequate stability.
Next, Minimal detectable change (MDC) for timed items has been reported of 0.7
seconds and for WMFT functional ability scale is 0.1 points (81, 82).
The widely used version of the WMFT consists of 17 items; 15 function-based
task and two strength-based tasks. Both performance time and functional ability of
upper limb and hand function are assessed. Items 1-6 are timed functional tasks, items
7-14 are measures of strength and the remaining 9 items also analyzing movement
quality. The test focused on the less affected side upper limb. The assessment tool is 6-
point ordinal scale; scale 0 for no attempt and scale 6 for normal performed movement
(scale 6). The equipment used in WMFT consisted of a standardized table (54 inches
long, 30 inches wide, and 29 inches high) and chair, standardized test item template,
height-adjustable bedside table, box (one that does not require patient to flex or abduct
shoulder more than 90 degrees), individual wrist weights, 1-20 pounds, 12-oz beverage
can, unopened, 7 inches pencil with 6 flat sides, 2 inches paper clip, 3 checkers, 3
inches x 5 inches note cards, standardized lock and key board at 45 degree angles,
standardized face towel, standardized basket, dynamometer, talcum powder to reduce
friction as needed, stopwatch, and video camera (optional) (81).
Ref. code: 25605812030533ARL

16
Impairments of upper limb and hand post stroke could be seen as paresis, impaired
sensation, and abnormal muscle tone. The Stroke Impairment Assessment Set (SIAS)
(83), Chedoke- McMaster Stroke Assessment (84) have been used to assess motor
recovery. Accelerometer assess acceleration of movement (85). Goniometer or
inclinometer have been used to assess the range of motion (86). Virtual Peg Insertion
Test have been used to assess the virtual reality and haptic feedback for sensorimotor
functions assessment (87). The Fugl-Meyer Assessment has long been used for assessing
motor and sensory impairments and joint range of motion is usually assessed by using
goniometry in clinical settings. The Fugl-Meyer Assessment: Upper Extremity (FMA-
UE) is the section of the Fugl- Meyer Assessment and has been used to measure motor
and sensory recovery of the upper limb in patients with stroke. This assessment is the
one of most widely measures for motor impairment with excellent inter-rater and intra-
rater reliability (r = 0.995-0.996) and construct validity (36). The responsiveness of FMA
is proper to detect change for patients after stroke rehabilitation (88). Minimal clinically
important difference of 10 points-change in FMA Upper extremity is comparable to 1.5
changes in the Functional Independence Measure (FIM). The Item are 3 point score
ordinal scale (89).
Voluntary movement assessed by measuring active range of motion has also been
used to indicate the severity of hand movement (90). Range of motion is clinically
measured by using goniometry. One study reported excellent intra- rater reliability of
goniometry (ICC- 3, k = 0.94) and digital inclinometry (ICC- 3, k = 0.95) for measuring
active shoulder flexion, abduction, internal and external rotation mobility measurement.
In addition, the concurrent validity between both measures was good. This study
supported the use goniometry or digital inclinometer for measuring range of motion of
shoulder joint (91).
Muscle spasticity could be assessed by using the Ashworth Scale (92) and
Modified Ashworth Scale. The purpose of the Modified Ashworth Scale is to grade
muscle spasticity in patients with lesions of the central nervous system ( CNS) . The
reliability has been reported of very good (Kappa = 0.84 for inter-rater reliability and
0. 83 for intra- rater reliability) (93). Convergent validity has been demonstrated
Ref. code: 25605812030533ARL

17
as excellent correlations between the Modified Ashworth Scale and motor performance
tests (94).
Sensory assessment is also necessary for the upper limb and hand function. This
is the indicator the effectiveness of an intervention. The Fugl-Meyer (FM) assessment,
the Nottingham Sensory Assessment, and the Revised Nottingham Sensory Assessment
could be used to assess sensory function post stroke. The Fugl-Meyer (FM) assessment
has been reported of adequate inter- rater reliability for the section of sensory
assessment.
The Revised Nottingham Sensory assessment has been developed from the
Nottingham Sensory Assessment (95) with good to excellent inter- rater reliability has
been reported (96). This is a suitable assessment for the use in patients with stroke (97).
From the literature review, only few studies are available on improving upper
limb and hand function in stroke individuals with moderate to severe arm weakness.
Most studies are conducted in those with ability to move their arms and hands. In
addition, studies in communities did not include those with severe arm weakness. Next
chapter will detail the methodology of the current study.
Ref. code: 25605812030533ARL

18
Chapter 3
Material and method
In this chapter, inclusion and exclusion criteria, material and method, statistical
analysis were described.
Prior to the main study investigating the effect of the Bobath therapy on upper
limb and hand function, the reliability of the Wolf Motor Function Test and the Fugl-
Meyer assessment of the upper extremity (FMA-UE) was evaluated.
3.1 Intra- and inter-rater reliability test of the Wolf Motor Function Test and
Fugl-Meyer assessment of the upper extremity
Two major outcome measures of the current study were the WMFT and FMA-UE.
The Wolf Motor Function test (WMFT) assessment consisted of 17 items. However,
only 15 items not involving in direct measure of muscle strength were chosen in this
study. Both movement time and functional ability was tested. The functional ability
scale is the 6-point ordinal scale (0-5). Each item has specific detail for scoring the
functional ability.
The Fugl-Meyer assessment of upper extremity (FMA-UE) - motor impairment
consisted of upper extremity, wrist, hand and coordination sections. There are 33 sub
items. Scoring is based on the 3-point ordinal scale (0-2). The maximum score is 66
points.
3.1.1 Participants (Patients with stroke)
3.1.1.1 Sample size
1) Intra-rater reliability of the Wolf Motor Function Test
Sample size in this study was calculated from the data
reported in the study by Morris and colleagues (2012) (81)
investigating hand function using the Wolf Motor Function Test
Ref. code: 25605812030533ARL

19
(performance time). The sample size determination was
computed using the following formula (98):
N = + 3 when Z = 0.5 × In
N = Sample size
Zα = Z-value for the type І error; One-tailed = 1.645
Zβ = Z-value for the type ІІ error; Zβ = Z0.8 = 0.84
Z = 2.526
r = Correlation coefficient (0.92)
α = 0.05
Power = 0.8
Sample size = 4
2) Inter-rater reliability of the Wolf Motor Function Test
Sample size in this study was calculated from the data
reported in the study by Morris and colleagues (2012) ( 8 1 )
investigating hand function using the Wolf Motor Function Test
(performance time). The sample size determination was
computed using the following formula (98):
N = + 3 when Z = 0.5 × In
N = Sample size
Zα = Z-value for the type І error; One-tailed = 1.645
Zβ = Z-value for the type ІІ error; Zβ = Z0.8 = 0.84
r = Correlation coefficient (0.92)
Z = 2.526
α = 0.05
Power = 0.8
Sample size = 4
Zα + Zβ
Z
2
1 - r
1 + r
Z 1 - r
Zα + Zβ
1 + r 2
Ref. code: 25605812030533ARL

20
3) Intra-rater reliability of the Fugl- Meyer assessment of
the upper extremity
Sample size in this study was calculated from the data
reported in the study by Sullivan and colleagues (2011) (89) using
the Fugl-Meyer assessment of the upper extremity (FMA-UE) .
The sample size determination was computed using the
following formula (98):
N = + 3 when Z = 0.5 × In
N = Sample size Zα = Z-value for the type І error; One-tailed = 1.645
Zβ = Z-value for the type ІІ error; Zβ = Z0.8 = 0.84
r = Correlation coefficient (0.92)
Z = 2.526
α = 0.05
Power = 0.8
Sample size = 4
4) Intra-rater reliability of the Fugl- Meyer assessment of
the upper extremity
Sample size in this study was calculated from the data
reported in the study by Sullivan and colleagues (2011) (89) using
the Fugl-Meyer assessment of the upper extremity (FMA-UE) .
The sample size determination was computed using the
following formula (98):
N = + 3 when Z = 0.5 × In
N = Sample size Zα = Z-value for the type І error; One-tailed = 1.645
Zβ = Z-value for the type ІІ error; Zβ = Z0.8 = 0.84
r = Correlation coefficient (0.92)
Z = 2.526
α = 0.05
Power = 0.8
Sample size = 4
1 + r Z 1 - r
Zα + Zβ
Z 1 - r
Zα + Zβ
1 + r
2
2
Ref. code: 25605812030533ARL

21
3.1.1.2 Inclusion criteria
1) Having first stroke confirmed by medical diagnosis
2) Chronic stroke (onset more than six months) caused by
ischemic and hemorrhagic
3) Age 45 years or older
4) Fugl-Meyer Assessment of the Upper Extremity: motor
Assessment scores for moderate level (26-50/66) to
severe level (< 26/66)
5) Live in community
6) Thai nationality
7) Able to sit independently for at least 30 minutes
8) Able to understand and follow one-step command
9) Stable medical condition
3.1.1.3 Exclusion criteria
1) Having other neurological conditions apart from stroke
2) Having musculoskeletal pain affecting reaching
3) Severe shoulder pain
(visual analog scale = 75 – 100 mm) (99)
4) Limited passive range of motion of shoulder flexion less
than 90 degree
5) Modified Ashworth Scale (grade) more than 2
6) Cognitive impairment considered by using the Thai
Mini Mental State Examination based on educational
criteria (score for people education less than primary
school ≥ 14, primary school ≥ 17, and higher than
primary school ≥ 22)
7) Having unilateral neglect
8) Participated in other interventions
Ref. code: 25605812030533ARL

22
3.1.2 Assessors
Assessors were two physiotherapists with clinical experience in stroke
rehabilitation and have been trained to assess upper limb and hand function
using the Wolf Motor Function Test, and the Fugl-Meyer Assessment of the
upper extremity.
3.1.3 Assessment tools and equipment
3.1.3.1 Thai-MMSE
3.1.3.2 Fugl-Meyer Assessment of the upper extremity
1) Tennis ball
2) Small can
3) Pencil
4) Paper
5) Hammer jerk
3.1.3.3 Wolf Motor Function test
1) Box
2) Sand bag
3) 12-oz beverage can, unopened
4) 7ʺ pencil with 6 flat side
5) 2ʺ paper clip
6) 3ʺ checkers
7) Three 3ʺ x 5ʺ note cards
8) Standardized lock and key board at 45 degree angle
9) Standardized face towel
10) Standardized basket
11) Stopwatch
3.1.3.4 Modified Ashworth scale (MAS)
Ref. code: 25605812030533ARL

23
3.1.4 Method
Firstly, the researcher recorded the WMFT and FMA-UE assessments
of healthy volunteers using the video for training the assessors. Then, the
researcher appointed assessors for training the assessments by using the
video recording. During the training session, the researcher explained
scoring system and demonstrated the assessments to assessors. The
researcher recorded the WMFT and FMA-UE assessments of another four
volunteers with stroke using the video. After that, the researcher appointed
assessors for watching and rating the video recording of four patients with
stroke (each file was displayed no more than twice). Assessors assessed the
WMFT (movement time) assessment by using a stopwatch and rated the
WMFT (FA) and FMA by ordinal scoring. Re-assessment via the video
recording was taken again seven days later. The researcher calculated data
by using the SPSS program, Version 22. Finally, the researcher evaluated
reliability of the assessments using the criteria of acceptable reliability (ICC
greater than 0.8). If the reliability was less than acceptance, the reliability
protocol was repeated.
3.2 Effect of the Bobath therapy on upper limb and hand function in stroke
individuals with moderate to severe arm deficits
3.2.1 Participants (patients with stroke)
3.2.1.1 Sample size
Sample size in this study was calculated from the data reported in
the study by Huseyinsinoglu and colleagues (2012) (22) investigating
hand function using the Wolf Motor Function Test (performance time)
after the Bobath therapy in patients with stroke. The sample size
determination was computed using the following formula (98):
n =
2 (Zα + Zβ) 2 𝜎2
∆2
Ref. code: 25605812030533ARL

24
n = sample size
∆ = mean difference
= mean (pre-intervention) – mean (post-intervention)
Mean group pre-intervention = 31.5
Mean group post-intervention = 20.5
∆ = 31.5 - 20.5 = 11
𝜎 = 18
Effect size = 0.513
α = 0.05
Power = 0.7
Zα
Zβ = Z-value for the type II error;
Zβ = Z0.3 = 0.524
n =
n = 2 (1.645 + 0.524)2 182
n = 25.19
Sample size = 25
With the additional number of 20% drop out, the number of participants in this
study were 30 cases.
= Z-value for the type I error;
One–tailed = 1.645
2 (Zα + Zβ) 2 𝜎2
∆2
112
Ref. code: 25605812030533ARL

25
3.2.1.2 Sampling
Purposive sampling or judgement sampling was used to sampling
participants. The researcher recruited participants with stroke in Pathum
Thani, Thailand using the following criteria.
3.2.1.3 Discontinuous criteria
1) Having other health conditions requiring hospitalization
2) No longer required to participate in this study
3.2.2 Trainer
A physiotherapist with clinical experience in stroke rehabilitation who has
been trained with the Bobath therapy for at least 30 hours.
3.2.3 Assessors
Assessors were two physiotherapists who have clinical experience in
stroke rehabilitation and have been trained to assess upper limb and hand
function using the Wolf Motor Function Test, the Fugl- Meyer Assessment of
the upper Extremity, Modified Ashworth Scale ( MAS) and the revised
Nottingham Sensory Assessment. Each assessor was assigned by the researcher
with the same assessor did the baseline assessment and post intervention
assessment for the same participant.
Intra-rater and inter-rater reliability were tested before starting baseline
assessment as described in section 3.1.
3.2.4 Assessment tools and equipment
3.2.4.1 Thai-MMSE
3.2.4.2 Fugl-Meyer Assessment of the upper extremity
Ref. code: 25605812030533ARL

26
1) Tennis ball
2) Small can
3) Pencil
4) Paper
5) Hammer jerk
3.2.4.3 Wolf Motor Function test
1) Box
2) Sand bag
3) 12-oz beverage can, unopened
4) 7ʺ pencil with 6 flat side
5) 2ʺ paper clip
6) 3ʺ checkers
7) Three 3ʺ x 5ʺ note card
8) Standardized lock and key board at 45 degree angle
9) Standardized face towel
10) Standardized basket
11) Stopwatch
3.2.4.4 Modified Ashworth scale (MAS)
3.2.4.5 Goniometer for assessing AROM
3.2.4.6 Revised Nottingham Sensory Assessment
1) 10 Coin
2) 2 Coin
3) 50 Coin
4) Brio
5) Pencil
6) Comb
7) Scissors
8) Sponge
9) Flannel
10) Cup
11) Glass
Ref. code: 25605812030533ARL

27
3.2.5 Research design and setting
Quasi-experimental study was implemented in this study. This study
investigated effect of the Bobath therapy on upper limb and hand functions in
chronic stroke with severe arm deficits. The settings were communities in
Pathum Thani, Thailand.
3.2.6 Method
All stroke participants were voluntarily provided a written consent prior
to their participation in this study. General characteristics were obtained using
the interview on age, sex, stroke onset, affected side, dominant arm, and highest
education. Screening tests were performed in the sitting position to identify
eligible participants using the criteria of the Fugl- Meyer Assessment of upper
extremity scores less than 50 (moderate level: 26- 50/66 and severe level:
<26/66) (Figure 3.1 Experimental flowchart).
3.2.7 Assessment
Impairments and functions of upper limb and hand were assessed using
following tools:
3.4.1.1 Fugl-Meyer Assessment of upper extremity (motor function)
3.4.1.2 Wolf Motor Function Test (performance and movement time)
3.4.1.3 Modified Ashworth Scale
3.4.1.4 The Revised Nottingham Sensory Assessment (body part;
shoulder, elbow, wrist and hand).
3.2.8 Variables
3.4.2.1 Independent variables: intervention (the Bobath therapy)
3.4.2.2 Dependent variables: Wolf Motor Function Test, Fugl- Meyer
assessment of the upper extremity, Modified Ashworth Scale,
and the Revised Nottingham Sensory Assessment.
3.2.9 Interventions
The intervention program has been designed based on individual’s
ability as assessed by using the Wolf motor function test (Table 3.1).
Ref. code: 25605812030533ARL

28
Table 3.1 Intervention program details based on pre-intervention Wolf motor
function test
Upper limb function
limitation
Hand function limitation Upper limb and hand
function limitation
Assessed by WMFT
Item 1-8
Scapula, shoulder
and elbow
movement
(movement facilitation or
active assisted training)
Upper limb
function training
(reaching)
Assessed by WMFT
Item 12, 13, 15
Wrist and hand
movement
(movement
facilitation or
active assisted
training)
Hand function
training (grasping)
Assessed by WMFT
Item 9, 10, 11, 16, 17
Scapula, shoulder
and elbow
movement
(movement facilitation or
active assisted training)
Upper limb and
hand function
training
(reaching, grasping)
Ref. code: 25605812030533ARL

29
3.2.9.1 Intervention Program
All participants received same training preparation consisting of
muscle stretching. The repetitions of movement training in the actual
training session in the program depended on the ability of individual
participants and noted by the physical therapy. Shapes of the object used
in training and re-assessments were similar, for example, a glass and a
can.
The overall details of therapy in the Bobath group are outlined
in Table 3.2 and through details of treatment preparation are illustrated
in Table 3.3.
Table 3.2 Details of interventions used in this study Bobath therapy
Preparation phase 15 minutes
(passive stretching and muscle mobilization)
Muscle mobilization: scapular, shoulder, elbow, wrist, and finger muscles
Treatment:
Frequency: three days/ week for six weeks
During each session, participants practiced 20 repetitions per set, 3 sets of each task. Rest
time 1-2 minutes as needed between sets.
Movement facilitation;
shoulder flexion, scapular protraction, elbow extension, wrist extension, and finger
extension.
Functional training with and without object
(target location, reaching, skilled grasp)
If participants could do movement independently, the trainer withdrew the
facilitation for improving of movement.
If participants could perform selective movement of upper limb and hand without
facilitation, the trainer stopped the practice of selective movement.
Ref. code: 25605812030533ARL
30
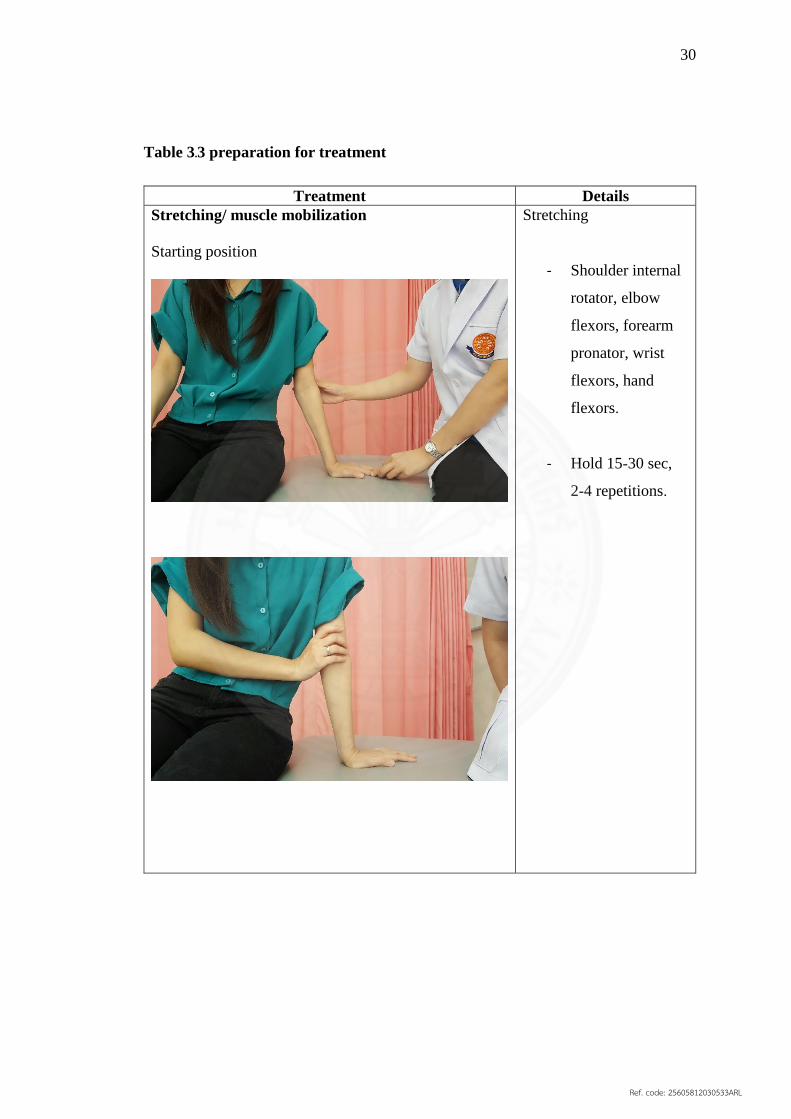
Table 3.3 preparation for treatment
Treatment Details
Stretching/ muscle mobilization
Starting position
Stretching
- Shoulder internal
rotator, elbow
flexors, forearm
pronator, wrist
flexors, hand
flexors.
- Hold 15-30 sec,
2-4 repetitions.
Ref. code: 25605812030533ARL

31
3.2.9.2 Bobath therapy
Therapy based on the Bobath concept was implemented in
accordance with impairments and limitation of upper limb and hand
functions of individual participants. The trainer withdrew the facilitation
as movement improved.
The trainer observed and corrected the posture and body
alignment of individual participants before and during practice. The
trainer evaluated participant’s ability and made the decision to change
the training program next practice. The details are as follows (Table 3.4):
Facilitation of shoulder, elbow, wrist and finger movements
Upper limb and hand function training
If the participants presented with sensory impairments, they
were also received the sensory facilitation.
Table 3.4 Bobath therapy intervention
Treatment Details
Scapular protraction
Starting position
Lateral view
Starting position; sitting position
- One hand placed on the
lateral side of thenar
muscles.
- Another hand placed under
inferior angle of scapular.
- Facilitation of scapular
protraction through full
range of motion.
- Relaxation to the starting
position.
Ref. code: 25605812030533ARL

32
Treatment Details
Posterior view
Lateral view
Posterior view
Ref. code: 25605812030533ARL

33
Treatment Details
Elbow extension
Starting position
starting position; sitting position
- One hand placed on thenar
muscles on the lateral surface.
- Another hand placed on
triceps brachii tendon.
- Facilitation of elbow
extension through full range
of movement.
- Relaxation to the starting
position.
Ref. code: 25605812030533ARL

34
Treatment Details
Wrist extension
Pattern I
Starting position
Starting position; sitting position
Sitting position
- Hand and wrist joint rest on the
table.
- Compression toward wrist
joint and facilitation through
full range of wrist extension.
- Relaxation to the starting
position.
Ref. code: 25605812030533ARL

35
Treatment Details
Pattern II
Starting position
If the participant presented with
severe spasticity of muscle or
severe tightness of muscle, the
trainer would use pattern II for
treatment.
Starting position; sitting position
- Hand and wrist joint rest on the
table.
- Compression toward wrist
joint and facilitation through
full range of wrist extension.
- Relaxation to the starting
position.
Ref. code: 25605812030533ARL

36
Treatment Details
Finger opposition
Thumb to little finger
Starting position
Starting position; Sitting position
- Placed the affected forearm
and hand in supination on the
table.
- Compression on
metacarpophalangeal joint and
facilitation through full range
of finger opposition.
- Relaxation to the starting
position.
Ref. code: 25605812030533ARL

37
Treatment Details
Thumb to index finger
Starting position
Starting position; sitting position
- The hand rest on the table
in the supination position.
- Compression on
metacarpophalangeal joint and
facilitation through full range
of finger opposition.
- Relaxation to the starting
position.
Ref. code: 25605812030533ARL

38
Treatment Details
Supination with object
Starting position
Starting position; sitting position
- Forearm rest on the table
(mid position).
- Compression through the wrist
to the elbow joint.
- Facilitation of forearm
supination.
- Relaxation to the starting
position.
Ref. code: 25605812030533ARL

39
Treatment Details
Grasping an object/Releasing an object
Starting position
Starting position; sitting position
- Assisted grasping.
- Compression on
metacarpophalangeal joint and
facilitation full range of
grasping.
- Distraction of
metacarpophalangeal joint to
full range of releasing.
- Relaxation to the starting
position.
Ref. code: 25605812030533ARL

40
\ฃฃ
Screening for eligibility
Inclusion criteria
1) First stroke confirmed by medical diagnosis
2) Chronic stroke (stroke onset more than six months)
3) Age 45 years or older
4) Fugl-Meyer Assessment of the Upper Extremity
: Motor assessment scores for moderate level
(26-50/66) to severe level (<26/66)
5) Thai nationality
6) Live in community
7) Able to sit independently for at least 30 minutes
8) Able to understand and follow one-step command
9) Stable medical condition
Exclusion criteria
1. Having other neurological conditions apart from stroke
2. Having musculoskeletal pain affecting reaching
3. Severe shoulder pain (visual analog scale = 75 – 100 mm) 4. Limited passive range of motion of shoulder flexion less than 90 degree
5. Modified Ashworth Scale (grade) more than 2
6. Cognitive impairment
7. Having unilateral neglect
8. Participated in other interventions
Baseline assessment
- Wolf Motor Function Test
- Fugl-Meyer Assessment of the upper extremity
- Muscle tone (Modified Ashworth Scale)
- The Revised Nottingham Sensory Assessment
- Treatment preparation; 15 minutes
- Movement facilitation; shoulder flexion, protraction,
elbow extension, wrist extension, finger extension
Functional training with and without object
(Target location, reaching and skilled grasp)
Three days/ week for six weeks
6 week Post assessment as same as at baseline
Figure 3.1 Experimental flowchart
30 patients
Purposive sampling
Ref. code: 25605812030533ARL

41
3.3 Data Analysis
Descriptive statistics was used to analyze baseline characteristic data. Intra-Class
Correlation (ICC) (3,1) was used to determine intra- rater reliability and ICC (2,1) was
used to determine inter-rater reliability of the Wolf Motor Function Test and Fugl-
Meyer assessment of the upper extremity.
Data distribution was analyzed using skewness and the Kolmogorov- Smirnov test
(K- S test). Descriptive statistics was used to analyze baseline characteristic data.
Wilcoxon Signed rank test was used to compare non- normal distributed data and
ordinal data. In this study, the significant level was set at 0. 05. SPSS Version 22 was
used to analyze all data.
Ref. code: 25605812030533ARL
42
Chapter 4
Results
4.1 Intra- and Inter-rater reliability test of the Wolf Motor Function Test and
Fugl-Meyer assessment of the upper extremity
The characteristic of four patients with stroke patients were those with moderate
upper limb and hand deficits (n = 2) and severe deficit (n = 2). The average age was
62.25 ± 11.76 years (Table 4.1.1).
4.1.1 Intra- and Inter-rater reliability test of the Wolf Motor Function Test
Intra and inter-rater reliability of the Wolf Motor Function Test
(movement time) of the affected side are presented in Table 4.1.2. Intra-rater
reliability ranged from 0.829 to 1.00 for assessor ‘1’ and 0.946 to 1.00 for
assessor ‘2’, respectively. Furthermore, inter-rater reliability of the Wolf Motor
Function Test (movement time) of the affected side ranged from 0.883 to 1.00.
Intra and inter-rater reliability of the Wolf Motor Function Test
(movement time) of the less-affected side are presented in Table 4.1.3. Intra-
rater reliability ranged from 0.806 to 1.00 for assessor ‘1’ and 0.836 to 1.00 for
assessor ‘2’, respectively. Furthermore, inter-rater reliability of Wolf Motor
Function Test (movement time) of less-affected side ranged from 0.875 to 1.00.
Intra- and inter-rater reliability of the Wolf Motor Function Test (FAS) of
the affected side are presented in Table 4.4. Intra-rater reliability ranged from
0.923 to 1.00 for assessor ‘1’ and 0.941 to 1.00 for assessor ‘2’, respectively.
Furthermore, inter-rater reliability of the Wolf Motor Function Test (FAS) of
the affected side ranged from 0.818 to 1.00.
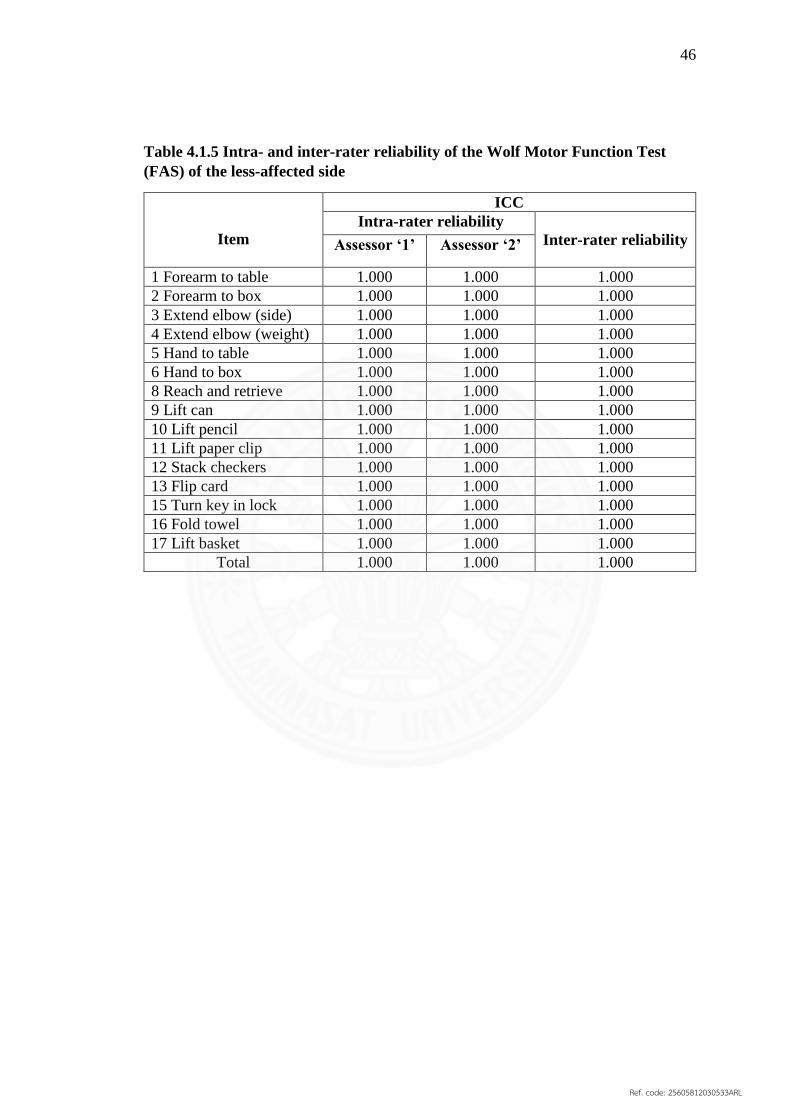
Intra- and inter-rater reliability of the Wolf Motor Function Test (FAS) of
the less-affected side are presented in Table 4.5. Intra- and inter-rater reliability
of the Wolf Motor Function Test (FAS) of the less-affected side were all 1.00.
Ref. code: 25605812030533ARL

43
Table 4.1.1 Characteristics of the participants in the reliability study
Characteristics Participants (n= 4)
Sex
- Female (n (%))
- Male (n (%))
1 (25%)
3 (75%)
Age (years) (Mean ± SD) 62.25 ± 11.76
Onset of stroke (months) 42.00 ± 52.00
Upper limb and hand deficits
- Moderate level (n (%))
- Severe level (n (%))
2 (50%)
2 (50%)
Affected side
- Left side (n (%))
- Right side (n (%))
2 (50%)
2 (50%)
Dominant-hand
- Left side (n (%))
- Right side (n (%))
-
4 (100%)
Education
- Primary School (n (%))
- Secondary School (n (%))
- Bachelor Degree (n (%))
-
2 (50%)
2 (50%)
Mini – Mental State Examination:
Thai version 2002
(scores)
(Mean ± SD)
29 ± 2.00
Ref. code: 25605812030533ARL

44
Table 4.1.2 Intra and inter-rater reliability of the Wolf Motor Function Test
(movement time) of the affected side
Item
ICC
Intra-rater reliability Inter-rater
reliability
Assessor ‘1’ Assessor ‘2’
1 Forearm to table 0.963 0.948 0.947
2 Forearm to box 0.926 0.946 0.941
3 Extend elbow (side) 0.912 0.953 1.000
4 Extend elbow (weight) 0.829 0.946 0.883
5 Hand to table 0.902 0.995 0.953
6 Hand to box 1.000 1.000 1.000
8 Reach and retrieve 1.000 1.000 1.000
9 Lift can 1.000 1.000 1.000
10 Lift pencil 1.000 1.000 1.000
11 Lift paper clip 1.000 1.000 1.000
12 Stack checkers 1.000 1.000 1.000
13 Flip card 1.000 1.000 1.000
15 Turn key in lock 1.000 1.000 1.000
16 Fold towel 1.000 1.000 1.000
17 Lift basket 1.000 1.000 1.000
Average time 1.000 1.000 1.000
Ref. code: 25605812030533ARL

45
Table 4.1.3 Intra- and inter-rater reliability of the Wolf Motor Function Test
(movement time) of the less-affected side
Item
ICC
Intra-rater reliability Inter-rater
reliability Assessor ‘1’ Assessor ‘2’
1 Forearm to table 0.890 0.970 0.925
2 Forearm to box 0.823 0.838 0.890
3 Extend elbow (side) 0.932 0.990 0.885
4 Extend elbow (weight) 0.831 0.836 0.898
5 Hand to table 0.968 0.978 0.875
6 Hand to box 0.900 0.878 0.879
8 Reach and retrieve 0.921 0.960 0.933
9 Lift can 0.958 0.990 0.961
10 Lift pencil 0.856 0.996 0.957
11 Lift paper clip 0.806 0.997 0.911
12 Stack checkers 0.836 0.959 0.931
13 Flip card 0.957 0.998 0.931
15 Turn key in lock 0.975 0.977 0.960
16 Fold towel 0.964 0.959 0.892
17 Lift basket 0.993 0.994 0.989
Average time 0.979 0.981 0.972
Table 4.1.4 Intra- and inter-rater reliability of the Wolf Motor Function Test
(FAS) of the affected side
Item
ICC
Intra-rater reliability Inter-rater
reliability Assessor ‘1’ Assessor ‘2’
1 Forearm to table 1.000 1.000 0.895
2 Forearm to box 0.930 1.000 0.879
3 Extend elbow (side) 1.000 1.000 1.000
4 Extend elbow (weight) 1.000 1.000 1.000
5 Hand to table 1.000 1.000 0.818
6 Hand to box 0.958 0.941 0.920
8 Reach and retrieve 1.000 1.000 1.000
9 Lift can 1.000 1.000 1.000
10 Lift pencil 0.923 1.000 0.952
11 Lift paper clip 0.923 1.000 0.952
12 Stack checkers 0.923 1.000 0.952
13 Flip card 1.000 1.000 1.000
15 Turn key in lock 1.000 1.000 1.000
16 Fold towel 1.000 1.000 1.000
17 Lift basket 1.000 1.000 1.000
Total 0.984 0.999 0.978
Ref. code: 25605812030533ARL
46
Table 4.1.5 Intra- and inter-rater reliability of the Wolf Motor Function Test
(FAS) of the less-affected side
Item
ICC
Intra-rater reliability
Inter-rater reliability
Assessor ‘1’ Assessor ‘2’
1 Forearm to table 1.000 1.000 1.000
2 Forearm to box 1.000 1.000 1.000
3 Extend elbow (side) 1.000 1.000 1.000
4 Extend elbow (weight) 1.000 1.000 1.000
5 Hand to table 1.000 1.000 1.000
6 Hand to box 1.000 1.000 1.000
8 Reach and retrieve 1.000 1.000 1.000
9 Lift can 1.000 1.000 1.000
10 Lift pencil 1.000 1.000 1.000
11 Lift paper clip 1.000 1.000 1.000
12 Stack checkers 1.000 1.000 1.000
13 Flip card 1.000 1.000 1.000
15 Turn key in lock 1.000 1.000 1.000
16 Fold towel 1.000 1.000 1.000
17 Lift basket 1.000 1.000 1.000
Total 1.000 1.000 1.000
Ref. code: 25605812030533ARL

47
4.1.2 Intra- and inter-rater reliability test of the Fugl-Meyer assessment of
the upper extremity
Intra- and inter- rater reliability of the Fugl- Meyer assessment of the upper
extremity of the affected side are presented in Table 4.6. Intra- rater reliability ranged
from 0.800 to 1.000 for assessor ‘1’ and 0.836 to 1.00 for assessor ‘2’ , respectively.
Furthermore, inter-rater reliability of the Fugl-Meyer assessment of the upper extremity
of the affected side ranged from 0.805 to 1.000.
Table 4.1.6 Intra- and inter-rater reliability of the Fugl-Meyer assessment
of the upper extremity
Item
ICC
Intra-rater reliability Inter-rater reliability
Assessor ‘1’ Assessor ‘2’
A1 1.000 1.000 1.000
A2 0.888 0.874 0.805
A3 1.000 1.000 1.000
A4 0.936 0.941 0.862
A5 1.000 1.000 1.000
B 0.800 1.000 0.939
C 0.872 0.836 0.858
D 0.835 0.945 0.862
Total 0.980 0.969 0.910
Ref. code: 25605812030533ARL

48
4.2 Effect of the Bobath therapy on upper limb and hand function in stroke
individuals with moderate to severe arm deficits
Screening test
(n = 46)
Excluded (n=20)
- Mild level of upper limb
and hand function
- (n = 9)
- Severe level of spasticity
(n = 7)
- Cognitive impairment
(n = 2)
- Recurrent stroke (n = 2)
Included
(n = 26)
Pre-assessment
Bobath therapy
3 days/week
6 weeks
(n = 26)
Post-assessment
Figure 4.1 Participant flowchart
Ref. code: 25605812030533ARL
49
This study included only 26 participants because the sample size calculation of
the study was 25 and there was no drop out in this study. Forty-six patients with stroke
were screened and only 26 patients met the inclusion criteria. However, the calculation
of power of the test from the data of 26 participants demonstrated 80 percent. This
power of test showed that amount of sample size was sufficient for detecting the
changes between pre- and post- assessment.
4.2.1 Characteristics of the participants
Participants in this study (n = 26) were chronic stroke with moderate level
( n = 13) and severe level ( n = 13) of upper limb and hand deficits. The
characteristics are shown in Table 4.7. The average age of the participants was
59. 69 ± 8. 69 years. The average score of the FMA-UE was 24. 77 ± 11. 39.
Moreover, the onset of stroke was 69.65 ± 65.13 months.
Ref. code: 25605812030533ARL

50
Table 4.2.1 Characteristics of the participants
a assessed by using the Fugl-Meyer assessment of the upper extremity
Characteristics Participants (n=26)
Moderate levela
(n=13)
Severe levela
(n=13)
Total
(n=26)
Sex
- Female (n (%))
- Male (n (%))
3 (23.08)
10 (76.92)
5 (38.46)
8 (61.54)
10
16
Age (years) 61.23 ± 10.64 58.15 ± 6.24 59.69 ± 8.69
Onset of stroke (months) 67.77 ± 69.11 71.54 ± 63.67 69.65 ± 65.13
Affected side
- Left side (n (%))
- Right side (n (%))
5 (38.46%)
8 (61.54%)
5 (38.46%)
8 (61.54%)
10 (38.46%)
16 (61.54%)
Dominant-hand
- Left side (n (%))
- Right side (n (%))
0 (0%)
13 (100%)
1 (7.69%)
12 (92.31%)
1 (3.85%)
25 (96.15%)
Education
- Primary (n (%))
- Secondary (n (%))
- Bachelor (n (%))
7 (53.85%)
5 (38.46%)
1 (7.69%)
5(38.46%)
7(53.85%)
1 (7.69%)
12 (46.15%)
12 (46.15%)
2 (7.69%)
Mini – Mental State
Examination: Thai
version 2002 (scores)
(mean ± SD)
23.69 ± 4.73
24.23 ± 3.37
23.96 ± 4.03
Fugl-Meyer assessment
of the upper extremity
(scores) (mean ± SD)
34.46 ± 6.78
15.08 ± 4.57
24.77 ± 11.39
Ref. code: 25605812030533ARL

51
4.2.2 Wolf Motor Function Test (movement time) of the affected side
Time used in forearm to box, extend elbow ( weight) , hand to box, reach
and retrieve, lift can, lift pencil, lift paper clip, flip card, turn key in lock, fold
towel, lift basket and total movement time demonstrated statistically significant
difference (p < 0.05) between pre and post assessment of movement time of the
Wolf Motor Function Test (movement time) of the affected side. However, time
spent in stack checkers did not show a significant difference (Table 4.2.2).
Table 4.2.2 Pre- and post-assessment of the Wolf Motor Function Test (movement
time) of the affected side
Item Pre – assessment
(n=26)
(seconds)
(mean ± SD)
Post – assessment
(n=26)
(seconds)
(mean ± SD)
P-value
1 Forearm to table 7.26 ± 23.04 2.73 ± 5.11 ≤ 0.001*
2 Forearm to box 13.17 ± 31.76 11.23 ± 32.05 0.007*
3 Extend elbow (side) 66.36 ± 59.10 48.79 ± 57.57 0.031*
4 Extend elbow (weight) 63.41 ± 57.85 44.99 ± 55.89 0.001*
5 Hand to table 8.12 ± 23.29 2.82 ± 5.24 0.005*
6 Hand to box 30.00 ± 50.33 10.87 ± 32.14 0.001*
8 Reach and retrieve 30.34 ± 50.21 2.85 ± 2.11 0.006*
9 Lift can 98.93 ± 44.18 76.99 ± 55.63 0.009*
10 Lift pencil 80.38 ± 55.56 56.87 ± 56.04 0.011*
11 Lift paper clip 100.05 ± 42.28 71.93 ± 57.27 0.006*
12 Stack checkers 101.91 ± 38.78 93.56 ± 44.99 0.176
13 Flip card 101.66 ± 38.75 83.91 ± 44.63 0.019*
15 Turn key in lock 96.63 ± 44.03 79.25 ± 48.63 0.015*
16 Fold towel 96.03 ± 44.66 58.00 ± 46.12 ≤ 0.001*
17 Lift basket 74.30 ± 56.41 43.64 ± 49.66 0.005*
Average time 64.51 ± 28.10 45.98 ± 30.50 0.000*
*P-value < 0.05
Calculated by the Wilcoxon signed rank in SPSS program
Ref. code: 25605812030533ARL
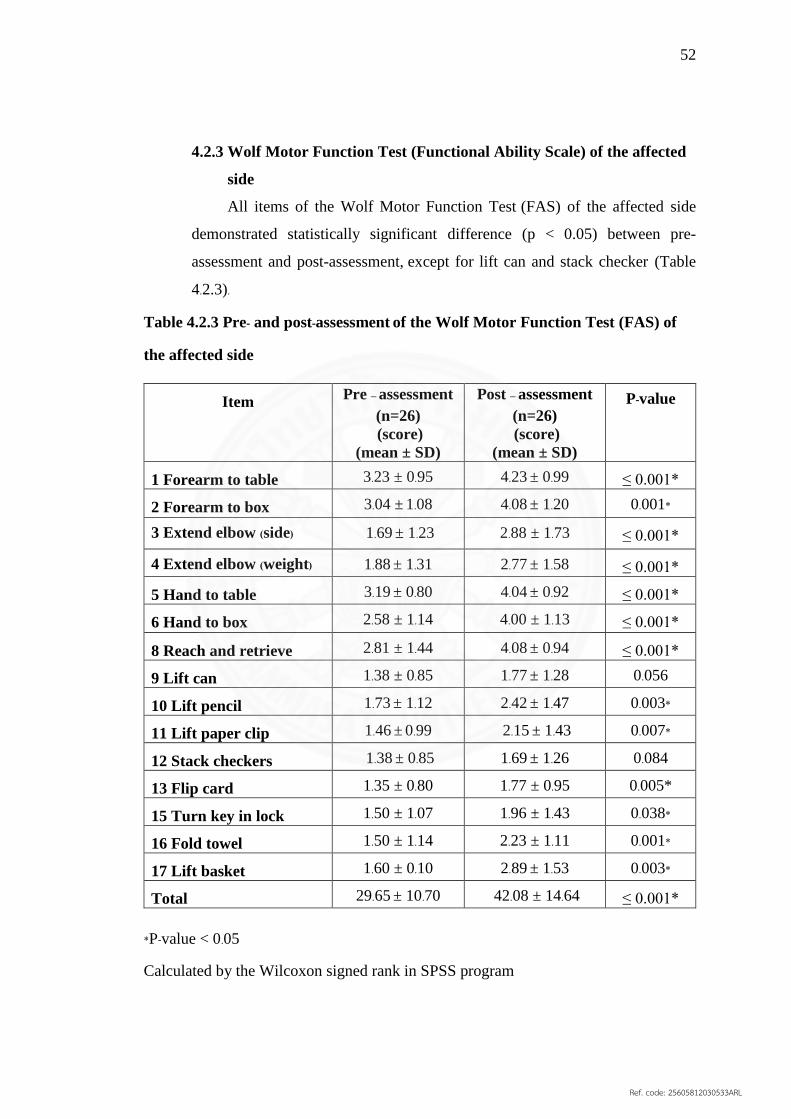
52
4.2.3 Wolf Motor Function Test (Functional Ability Scale) of the affected
side
All items of the Wolf Motor Function Test (FAS) of the affected side
demonstrated statistically significant difference (p < 0.05) between pre-
assessment and post-assessment, except for lift can and stack checker (Table
4.2.3).
Table 4.2.3 Pre- and post-assessment of the Wolf Motor Function Test (FAS) of
the affected side
Item Pre – assessment
(n=26)
(score)
(mean ± SD)
Post – assessment
(n=26)
(score)
(mean ± SD)
P-value
1 Forearm to table 3.23 ± 0.95 4.23 ± 0.99 ≤ 0.001*
2 Forearm to box 3.04 ± 1.08 4.08 ± 1.20 0.001*
3 Extend elbow (side) 1.69 ± 1.23 2.88 ± 1.73 ≤ 0.001*
4 Extend elbow (weight) 1.88 ± 1.31 2.77 ± 1.58 ≤ 0.001*
5 Hand to table 3.19 ± 0.80 4.04 ± 0.92 ≤ 0.001*
6 Hand to box 2.58 ± 1.14 4.00 ± 1.13 ≤ 0.001*
8 Reach and retrieve 2.81 ± 1.44 4.08 ± 0.94 ≤ 0.001*
9 Lift can 1.38 ± 0.85 1.77 ± 1.28 0.056
10 Lift pencil 1.73 ± 1.12 2.42 ± 1.47 0.003*
11 Lift paper clip 1.46 ± 0.99 2.15 ± 1.43 0.007*
12 Stack checkers 1.38 ± 0.85 1.69 ± 1.26 0.084
13 Flip card 1.35 ± 0.80 1.77 ± 0.95 0.005*
15 Turn key in lock 1.50 ± 1.07 1.96 ± 1.43 0.038*
16 Fold towel 1.50 ± 1.14 2.23 ± 1.11 0.001*
17 Lift basket 1.60 ± 0.10 2.89 ± 1.53 0.003*
Total 29.65 ± 10.70 42.08 ± 14.64 ≤ 0.001*
*P-value < 0.05
Calculated by the Wilcoxon signed rank in SPSS program
Ref. code: 25605812030533ARL

53
4.2.4 Fugl-Meyer assessment of the upper extremity
All items of the Fugl- Meyer assessment of the upper extremity
demonstrated statistically significant difference between pre- and post-
assessment (p < 0.05), except for reflex activity and normal reflex activity
(Table 4.2.4).
Table 4.2.4 Pre-assessment and post-assessment of the Fugl-Meyer assessment of
the upper extremity
Item
Pre –
assessment
(n=26)
(score)
(mean ± SD)
Post –
assessment
(n=26)
(score)
(mean ± SD)
P-value
Upper extremity
- Reflex activity
Flexors: Biceps and finger flexors
Extensors: triceps
2.00 ± 0.00
1.92 ± 0.39
2.00 ± 0.00
1.92 ± 0.39
1.000
1.000
- Volitional movement within
synergies
Shoulder retraction
elevation
abduction (90°)
external rotation
Elbow flexion
Forearm supination
Shoulder adduction/internal
rotation
Elbow extension
Forearm pronation
0.88 ± 0.65
1.08 ± 0.56
1.04 ± 0.59
0.81 ± 0.69
1.23 ± 0.58
0.23 ± 0.43
1.08 ± 0.79
0.92 ± 0.68
0.31 ± 0.47
1.42 ± 0.57
1.50 ± 0.58
1.35 ± 0.74
1.15 ± 0.78
1.58 ± 0.70
0.88 ± 0.76
1.46 ± 0.58
1.23 ± 0.65
0.81 ± 0.74
0.003*
0.002*
0.059
0.039*
0.007*
0.001*
0.032*
0.033*
0.002*
Subtotal II (max 18) 7.38 ± 3.68 11.38 ± 4.67 ≤ 0.001*
*P-value < 0.05
Calculated by the Wilcoxon signed rank in SPSS program
Ref. code: 25605812030533ARL

54
Table 4.2.4 Pre-assessment and post-assessment of the Fugl-Meyer assessment of
the upper extremity (continued)
*P-value < 0.05
Calculated by the Wilcoxon signed rank in SPSS program
Item
Pre –
assessment
(n=26)
(score)
(mean ± SD)
Post –
assessment
(n=26)
(score)
(mean ± SD)
P-value
- Volitional movement
mixing synergies
Hand to lumbar spine
Shoulder flexion 0°-90°
Elbow at 0°
Pronation-supination 0°
Pronation-supination
Elbow at 90°
Shoulder at 0°
0.85 ± 0.73
0.54 ± 0.70
0.65 ± 0.62
1.27 ± 0.72
1.04 ± 0.91
1.12 ± 0.65
0.002*
0.005*
0.007*
Subtotal III (max 6) 1.96 ± 1.66 3.46 ± 1.75 ≤ 0.001*
- Volition movement with
little or no synergy
Shoulder abduction 0 - 90°
Elbow at 0°
Forearm pronated
Shoulder flexion 90 - 180°
Elbow at 0°
Pronation-supination 0°
Pronation/supination
Elbow at 0°
Shoulder at 30° - 90° flexion
0.54 ± 0.58
0.35 ± 0.65
0.46 ± 0.58
0.85 ± 0.88
0.69 ± 0.78
0.96 ± 0.77
0.033*
0.058
0.002*
Subtotal IV (max 6) 1.35 ± 1.26 2.65 ± 1.83 ≤ 0.001*
Ref. code: 25605812030533ARL

55
Table 4.2.4 Pre-assessment and post-assessment of the Fugl-Meyer assessment of
the upper extremity (continued)
Item
Pre – assessment
(n=26)
(score)
(mean ± SD)
Post – assessment
(n=26)
(score)
(mean ± SD)
P-value
- Normal reflex activity
Biceps, triceps, finger
flexors
1.31 ± 0.78
1.54 ± 0.64
0.177
- Wrist
Stability at 15° dorsiflexion
Elbow at 90°, forearm
pronated
Shoulder at 0
Repeated dorsiflexion /
volar flexion
Elbow at 90°, forearm
pronated
Shoulder at 0°, slight finger
flexion
Stability at 15° dorsiflexion
Elbow at 0°, forearm
pronated
Slight shoulder
flexion/abduction
Repeated dorsiflexion /
volar flexion
Elbow at 0°, forearm
pronated
Slight shoulder
flexion/abduction
Circumduction
0.46 ± 0.64
0.46 ± 0.70
0.35 ± 0.56
0.38 ± 0.57
0.35 ± 0.62
1.00 ± 0.84
0.96 ± 0.82
0.85 ± 0.78
0.96 ± 0.77
0.77 ± 0.71
0.003*
0.003*
0.002*
0.001*
0.002*
Total B (max 10) 1.85 ± 2.54 4.54 ± 3.58 ≤ 0.001*
*P-value < 0.05
Calculated by the Wilcoxon signed rank in SPSS program
Ref. code: 25605812030533ARL

56
Table 4.2.4 Pre-assessment and post-assessment of the Fugl-Meyer assessment of
the upper extremity (continued)
Item
Pre – assessment
(n=26)
(score)
(mean ± SD)
Post – assessment
(n=26)
(score)
(mean ± SD)
P-value
- Hand
Mass flexion
Mass extension
- Grasp
A- flexion in PIP and DIP
(digit II-V) extension in
MCP II-V
B- thumb adduction
1-st CMC, MCP, IP at 0,
scrap of paper between
thumb and 2-nd MCP joint
C – opposition pulpa of the
thumb against the pulpa of
2-nd finger, pencil, tug
upward
D - cylinder grip
Cylinder shaped object
(small can) tug upward,
opposition in digits I and II
E – spherical grip
Fingers in
abduction/flexion, thumb
opposed, tennis ball
1.12 ± 0.81
0.54 ± 0.76
1.31 ± 0.83
0.65 ± 0.89
0.73 ± 0.87
0.88 ± 0.86
0.77 ± 0.81
1.58 ± 0.57
0.88 ± 0.86
1.50 ± 0.64
1.27 ± 0.77
1.19 ± 0.89
1.58 ± 0.70
1.35 ± 0.74
0.012*
0.073
0.293
0.001*
0.015*
0.001*
0.001*
Total C (max 14) 6.00 ± 4.49 9.12 ± 4.41 ≤ 0.001*
*P-value < 0.05
Calculated by the Wilcoxon signed rank in SPSS program
Ref. code: 25605812030533ARL
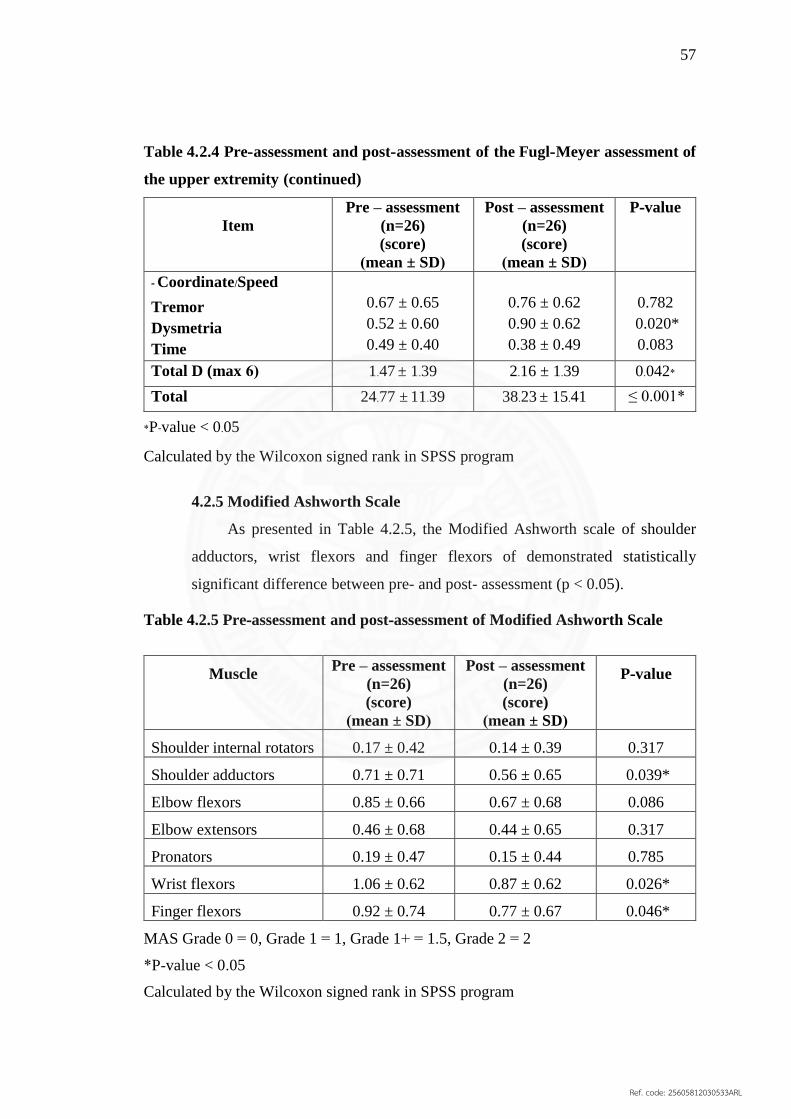
57
Table 4.2.4 Pre-assessment and post-assessment of the Fugl-Meyer assessment of
the upper extremity (continued)
Item
Pre – assessment
(n=26)
(score)
(mean ± SD)
Post – assessment
(n=26)
(score)
(mean ± SD)
P-value
- Coordinate/Speed
Tremor
Dysmetria
Time
0.67 ± 0.65
0.52 ± 0.60
0.49 ± 0.40
0.76 ± 0.62
0.90 ± 0.62
0.38 ± 0.49
0.782
0.020*
0.083
Total D (max 6) 1.47 ± 1.39 2.16 ± 1.39 0.042*
Total 24.77 ± 11.39 38.23 ± 15.41 ≤ 0.001*
*P-value < 0.05
Calculated by the Wilcoxon signed rank in SPSS program
4.2.5 Modified Ashworth Scale
As presented in Table 4.2.5, the Modified Ashworth scale of shoulder
adductors, wrist flexors and finger flexors of demonstrated statistically
significant difference between pre- and post- assessment (p < 0.05).
Table 4.2.5 Pre-assessment and post-assessment of Modified Ashworth Scale
Muscle Pre – assessment
(n=26)
(score)
(mean ± SD)
Post – assessment
(n=26)
(score)
(mean ± SD)
P-value
Shoulder internal rotators 0.17 ± 0.42 0.14 ± 0.39 0.317
Shoulder adductors 0.71 ± 0.71 0.56 ± 0.65 0.039*
Elbow flexors 0.85 ± 0.66 0.67 ± 0.68 0.086
Elbow extensors 0.46 ± 0.68 0.44 ± 0.65 0.317
Pronators 0.19 ± 0.47 0.15 ± 0.44 0.785
Wrist flexors 1.06 ± 0.62 0.87 ± 0.62 0.026*
Finger flexors 0.92 ± 0.74 0.77 ± 0.67 0.046*
MAS Grade 0 = 0, Grade 1 = 1, Grade 1+ = 1.5, Grade 2 = 2
*P-value < 0.05
Calculated by the Wilcoxon signed rank in SPSS program
Ref. code: 25605812030533ARL

58
4.2.6 Revised Nottingham Sensation assessment
As presented in Table 4.2.6, only stereognosis demonstrated statistically
significant difference (p = 0.028) between pre- and post-assessment of the
revised Nottingham Sensory assessment.
Table 4.2.6 Pre-assessment and Post-assessment of the Revised Nottingham
Sensory assessment
Item
Pre – assessment
(n=26)
(score)
(mean ± SD)
Post – assessment
(n=26)
(score)
(mean ± SD)
P-value
Tactile sensation
Light touch
15.50 ± 3.40
15.42 ± 1.33
0.343
Temperature 13.92 ± 3.20 14.46 ± 3.04 0.059
Pinprick 14.77 ± 2.32 15.27 ± 1.76 0.109
Tactile
localization
15.00 ± 1.69 15.26 ± 1.3 0.059
Bilateral
Simultaneous
touch
7.15 ± 1.80 7.19 ± 1.98 0.783
All 103.08 ± 16.57 104.08 ± 14.83 0.645
Proprioception 8.50 ± 3.52 9.92 ± 8.21 0.067
Stereognosis 9.80 ± 2.65 12.31 ± 8.85 0.028*
*P-value < 0.05
Calculated by the Wilcoxon signed rank in SPSS program
Ref. code: 25605812030533ARL

59
Chapter 5
Discussion
This chapter explained the significant results of this study based on current
principles and comparison with previous studies.
5.1 Intra- and inter-rater reliability test of the Wolf Motor Function Test and the
Fugl-Meyer assessment of the upper extremity
The purpose was to evaluate the intra-rater and inter-rater reliability of the Wolf
Motor Function Test (movement time and functional ability scale and the Fugl-Meyer
assessment of the upper extremity of two assessors. The participants with stroke in this
study were four patients with moderate (n=2) to severe deficits (n=2) of upper limb and
hand. All of them were chronic stroke.
5.1.1 Reliability of the Wolf Motor Function Test
The intra-rater and inter- rater reliability of the Wolf Motor Function Test
(movement time and functional ability scale) was excellent. This is in line with
previous studies regarding high intra-rater and inter-rater reliability of the Wolf
Motor Function Test in chronic stroke (ICC ranged from 0.88-0.97) (81, 100). The
Wolf Motor Function Test has standardized particularity which is the important
reason for good psychometric properties (81). Moreover, brief training for two
assessors in the current study enhanced acceptable reliability. Excellent
reliability of the WMFT ensured the rating consistency of the raters and
demonstrated actual changes from the intervention used in the current study.
5.1.2 Reliability of the Fugl-Meyer Assessment of the upper extremity
The intra-rater and inter-rater reliability of individual items and total score
of the Fugl-Meyer assessment of the upper extremity was good to excellent (ICC
Ref. code: 25605812030533ARL

60
˃ 0.8). Brief training of the test for new assessors could enhance the reliability
of assessment (101). In addition, rating the assessment via video recording (102) or
via direct observation (101, 103) did not affect the reliability of the Fugl-Meyer
Assessment. In previous studies, intra-rater and inter-rater reliability ranged
from 0.95-0.99 (ICC) (101-103). High intra-rater and inter-rater reliability ensured
the consistency of re-assessments by the same rater and across raters.
5.2 Effect of the Bobath therapy on upper limb and hand function in stroke
individuals with moderate to severe arm deficits
The effectiveness of the Bobath therapy on upper limb and hand function was
shown in Study 2. Motor impairments, muscle tone and sensation of upper limb and
hand were also assessed in chronic stroke individuals with moderate to severe arm
deficits.
The Bobath therapy implemented problem solving approach for assessment and
treatment (104). The details of the Bobath therapy program in this study featured the
preparation of muscle length, selective movement training, and functional training.
Therefore, the Bobath therapy could improve the function and minimize impairments
of the upper limb and hand in stroke individuals.
This concept is based on motor control and motor learning theory. Active
participation of individual participants is the main ingredient of motor control in the
intervention program (18). Sufficient repetitions of practiced movements also
contributed to motor learning (105). According to the neuronal plasticity, the neuronal
structures and function changed and modified as motor learning occurred (106, 107).
Repeated movements using movement facilitation enhanced sensory stimulation to the
sensorimotor cortex through the stimulation of exteroceptors and proprioreceptors (108).
These sensory inputs are then enhanced the activation of motor cortex as well as motor
pathway, resulting in better control of movement (109).
Ref. code: 25605812030533ARL

61
5.2.1 The characteristics of participants
All participants in this study were included according to the inclusion
criteria. They were chronic stroke without cognitive deficits. The proportion of
those with moderate deficits and those with severe deficits of upper limb and
hand functions as assessed by using the Fugl-Meyer Assessment of the upper
extremity was equivalent. As demonstrated in several studies, patients with mild
to moderate deficits could achieve completely recovery more than patients with
severe deficits (110, 111). The current study emphasized the therapy to improve
upper limb and hand function in those with severe deficits as well as those with
moderate deficits.
Chronicity also has strong impact on recovery post stroke. The progress
of recovery in chronic stroke are slower than subacute and acute stroke (112, 113)
The valid prognostication of upper extremity (UE) functions recovery was
difficult over 11 weeks post stroke for those with severe deficits (114). However,
the study by Broeks and colleagues (1999) showed that some subacute stroke
individuals still improved in their upper limb and hand functions after four
months post stroke (50). For chronic stroke, improvement in their movements has
been evidenced regardless the onset of stroke (115).
In the current study, all participants were not involved in any
rehabilitation programs. The results in this study were mainly from the effect of
training using the Bobath therapy.
5.2.2 The effect of the Bobath therapy on upper limb and hand functions
The Bobath therapy was effective in improving upper limb and hand
functions as presented in the results. Improvement of upper limb and hand
functions in stroke with moderate to severe deficits in the current study could
be explained by task specific training. The practice of specific repetitive tasks
would result in motor learning and improvement in upper limb and hand
functions (116, 117). The features of the Bobath therapy program used in the
Ref. code: 25605812030533ARL

62
current study were facilitation technique of hand orientation movement
(CHOR) and hand function. CHOR is the basic movement of various hand
functions such as grasping, picking up an object, and release the object from the
hand (18).
Another explanation is sufficient number of movement repetitions for
motor learning. The patients with stroke whom received the sufficient number
of movement repetitions could improve their upper limb and hand functions
(118). In the current study, almost all items of the WMFT demonstrated
significant improvement after the interventions compared to the baseline.
Various items in the WMFT were similar to tasks practices in the intervention.
Therefore, the functional training with and without objects and movement
facilitation training in the Bobath program could improve functions of upper
limb and hand. The Bobath therapy used in the current study consisted of
selective movement training of individual upper limb joints, for example,
shoulder flexion and wrist flexion. Once the participants had better control of
movement, facilitation was decreased and functional training with and without
objects were administered. As the facilitation decreased, the participants had to
gain more control in executing movements. This self-control promoted motor
learning (119).
The postural control in the Bobath therapy program is also related to upper
limb and hand movements (120). In the previous study, the external trunk support
improved upper limb and hand function as assessed by using the Wolf Motor
Function test in chronic stroke patients. The appropriate degrees of freedom in
trunk (upper and lower part) had positive effect on the reorganization of motor
system and coordination of reaching task. The trunk stabilization supported the
movement of proximal and distal segment in chronic stroke (121). Moreover, the
trunk stability was a base of torque generation for upper limb movement (122).
The Bobath concept emphasized on the posture and movement through the
alignment of body (19). During practice, correct trunk posture was in concern.
Postural control is essential in improving upper limb and hand function (123).
Ref. code: 25605812030533ARL
63
The address of postural control before and during practice in the Bobath
therapy program in the current study enhanced body orientation and
stabilization. The trainer gave feedback on postural control for individual
patients. In addition, proximal and central and key point of control have a
dynamic interrelationship for motor control (68). Appropriate postural tone and
postural control are related to functional movement (19).
Moreover, selective movement improved joint movements control and
normal patterns of movement through specialized handling. These handling
techniques also improved sensorimotor integration (18). In the Bobath therapy
program used in the current study, the therapist assisted in correcting
movement and joint orientation during movement facilitation. Sensory
information (joint position sense, light touch, joint compression and
distraction) and optimal joint alignment from the handling technique could
also promote the reorganization of the central nervous system (CNS) through
sensorimotor integration and resulting in motor output (124, 125).
Total number of movements used in the current study was 60 repetitions
per task and 300 – 600 repetitions per session. This is considered a sufficient
dose to improve the control of upper limb and hand movement. From the
literature review, optimal training program was indicated by total treatment
time. For example, the modified CIMT program effectively improved upper
limb and hand functions used three hours for a training session and altogether
10 sessions (22). This dose is comparable to the amount of practice used in the
current study. Nevertheless, the participants in the current study were patients
with chronic stroke who no longer received rehabilitation program prior to their
participation in this study. Improvements gained were therefore mainly the
effect from the intervention program.
All in all, the Bobath therapy could improve function, minimize
impairments of the upper limb and hand in chronic stroke. Minimization of
impairments will be discussed in the following section. Although the training
frequency per week for individual participants was not equal. Some participants
Ref. code: 25605812030533ARL

64
were ill and had medical appointments during the intervention schedule.
However, total times of interventions delivered for participants were equivalent.
Stack checker (item 12) and can lifting (item 9) did not show significant
improvements post interventions as compared to baseline in the current study.
This could be due to the tasks are the most difficult items and complex (126, 127).
For the stack checker, there was no change of both the movement time and
functional ability scale. This task is a complex activity and involving multiple
joints during movement (127). Coordination and holding ability are essential for
task achievement (128). For the participants in the current study, their
coordination as assessed by using the FMA-UE showed moderate deficits at
baseline. However, there was a significant improvement in dysmetria.
Therefore, the finding of no significant improvement in the complex task may
mainly cause by insufficient ability to control movement rather than
incoordination. Movement components of stack checker are shoulder flexion,
scapular protraction, elbow extension, wrist extension, finger extension,
opposition of thumb and index finger. For the can lifting, there was a change in
movement time but not in the functional ability scale of the WMFT. Movement
components in the training program such as wrist extension and hand opening
were similar to the movement components in can lifting. In addition, this task
is required muscle strength in order to lift an unopened can. The practice in this
study might be not enough for improving muscle strength for manipulating an
object with weight. However, changing in functional ability scale required
specific amount of training (129). Movement repetitions used in previous studies
are similar to the current study, but different in participants’ characteristics (6,
118, 130). In the current study, participants were chronic stroke with moderate to
severe deficits of upper limb and hand while the participants in other three
previous studies were acute to subacute stroke. This could imply that sufficient
number of movement repetitions in practice is also efficient in chronic stroke
with severe deficits.
In the current study, the functional ability scale of other items changed
1-2 scale. However, movement change was not yet comparable to the normal
Ref. code: 25605812030533ARL

65
movement. The practice components of the Bobath therapy used in the current
study were related to upper limb and hand function such as reaching, grasping,
hand opening, and fine movements. These movement components are involved
in various activities (131, 132). The recovery of upper limb and hand functions are
essential for the quality of life of stroke individuals (18, 67, 133). The current study
had various tasks of the training, for example, hand function training with and
without objects. The participants received the appropriately functional training
for improving upper limb and hand performance. Therefore, they had
improvement in the functional ability scale and movement time in the WMFT.
Additional comparison between moderate and severe deficits has been made
and the findings showed more improvement of the complex task ability in stroke
with moderate deficits than those with severe deficits. The progression of
recovery and performance of task in stroke individuals with moderate deficits
was better than those with severe deficits.
5.2.3 The Effect of the Bobath therapy on upper limb and hand
impairments
The Bobath therapy was effective in minimizing impairments of the upper
limb and hand in individuals with chronic stroke. As presented in the results,
almost all items of the Fugl- Meyer assessment of the upper extremity
demonstrated statistically significant improvement post interventions. As thumb
adduction, spherical grip, cylinder grip and opposition showed good
improvement, these were in accordance with the improvement of hand function.
In addition, the Bobath program consisted of the facilitation of selective upper
limb and hand movement. This was effective in improving the impairments in
terms of the control of individual joint movements. The selective movement and
task specific training promoted neuroplasticity (synapse changing, synaptic
transmission), muscular plasticity (fiber length, sarcomeres numbers), and
cortical plasticity (motor and sensory cortical area activation) (134, 135). One
Ref. code: 25605812030533ARL

66
previous study showed that the task specific training program could improve
the cortical area activation (primary motor, sensorimotor cortex, primary
sensory and premotor cortex) in patients with stroke (136).
Handling scapula in the program used in the current study enhanced
upper limb and hand movement. Handling proximal key point at scapular
provided stability, alignment and movement guidance for normal movement
pattern (19). It has been shown that appropriate scapular position increased the
activation of the muscles surrounding the shoulder joint and improved the
function of the upper extremity (137). This is in accordance with another previous
study that the scapular stabilization program could improve upper limb and
hand function in the patients with chronic stroke (138).
Huseyinsinoglu and colleagues (2012) studied the effectiveness of the
Bobath therapy compared with the constraint-induced movement therapy. Their
results showed improvements in impairments between pre and post intervention
in subacute and chronic stroke participants with high level function of arm
(active wrist extension more than twenty degrees and active extension of the
metacarpophalangeal joints and interphalangeal joint of all digits more than ten
degrees). In their study, the intervention program based on the Bobath concept
consisted of muscle tone normalization, postural stability, and upper limb and
hand activities during unilateral or bilateral tasks. The treatment time was one
hour per session, last for 10 weeks (22). Although participants in the current study
were chronic stoke individuals with moderate to severe impairments,
improvements in impairments were demonstrated.
5.2.3.1 Muscle tone
Hypertone was manifested in almost all of the stroke participants
in the current study at baseline. Based on the Bobath concept, hypertone
occurred from the loss of inhibitory control (18). Spasticity limited joint
range of motion and induced the deviation of normal functional pattern
of upper limb and hand (139, 140). From the findings, the MAS of shoulder
Ref. code: 25605812030533ARL

67
adductors, wrist flexors and finger flexors decreased significantly post-
interventions as compared to pre-interventions. In the current study, the
patients showed improvement in motor impairment and involuntary
movement. The results were in accordance with one previous study
demonstrated the relation of spasticity with motor units and involuntary
control of spastic muscles activation (141). As a result, as motor control
improve, spasticity reduced.
Passive stretching implemented during the preparation phase
results in muscle tone normalization in the current study. In addition,
movement facilitation addressed elbow extension in reaching, and wrist
extension in hand opening and grasping. The selective movement of
wrist and hand movement helped the relaxation of the wrist and hand
flexor muscles. In addition, the number of hand manipulation in
practices was greater than the number of movement repetitions for
reaching. As a result, muscle tone decreased in only wrist and finger
flexors. In addition, shoulder abduction was the movement component
in several tasks being practiced in the current study. This could explain
the finding that muscle tone of shoulder adductor muscles decreased.
A number of studies supported the effect of a combination of
electrical stimulation on the dorsiflexor muscles and inhibitory Bobath
techniques Bobath therapy on the decrease of hypertone. For example,
the study by Bakhtiary and colleagues (2008) demonstrated that the
intervention could decrease the spasticity of plantarflexor muscle as
assessed by MAS in patients with stroke (142). The intervention program
consisted of the Bobath inhibitory techniques for fifteen minutes,
passive movement of hip abduction, hip external rotation, knee
extension, ankle dorsiflexion (inhibitory movement pattern) and nine
minutes electrical stimulation. Furthermore, the Bobath therapy
program of guide line by the physical therapy 10 sessions demonstrated
decreased spasticity of elbow flexors muscle or elbow extensors muscle
in subacute and chronic stroke patients (21). Different muscles being
Ref. code: 25605812030533ARL

68
decreased in muscle tone across studies may be due to the difference in
movements being practiced and the characteristics of participants. The
participants in previous studies were subacute and chronic stroke and
the movement being practiced focused recovery the muscle tone.
While there were significant changes in shoulder adductors,
wrist and finger flexors, there was no significant changes in shoulder
flexors, elbow extensors, elbow flexors and pronators post-interventions
as compared to pre-interventions. The participants had spasticity in these
muscle groups as well as moderate to severe deficits of upper limb and
hand at baseline. Minimal changes in the score of MAS in severe
spasticity muscles has been reported (85, 143). In current study, only some
participants had the spasticity of shoulder internal rotator. For elbow
flexor muscles and elbow extensor muscles, there was no change in
MAS as the spasticity of these muscles was in greater degree than other
muscles.
Sustained stretching from 1 to 2 minutes, 12 times per session 4
times a week, 8 weeks decreased spasticity of upper limb muscle (144).
Stretching and muscle mobilization in preparation phase are 15 minutes.
Stretching in the preparation phase in the current study addressed elbow
flexor, wrist and finger flexor. Although no significant improvement,
elbow flexor muscles and elbow extensor muscles showed a trend to
improve in muscle tone.
The characteristics of training in the current study, for example,
hand function training and reaching might also affect muscle tone of
forearm pronator muscles. Most of task practices were in the position
of forearm pronation. Therefore, there were less occasions that forearm
pronator was stretched. Nevertheless, muscle contraction and relaxation
is one possible mechanism to normalize muscle tone. As agonist muscle
is contracting, the antagonist muscles are being lengthened (145). For
example, lower limb pattern practice with the rhythmic initiation of a
repeated stretch and a combination of isotonic technique in
Ref. code: 25605812030533ARL

69
Proprioceptive Neuromuscular Facilitation (PNF) treatment led to tone
normalization of lower extremity muscles (146). For the PNF
intervention, they applied a lower extremity hip extension-abduction-
internal rotation with knee extension pattern, together with the rhythmic
initiation of a repeated stretch and a combination of isotonic techniques.
Among the many important muscles used in walking and balancing, this
pattern simultaneously stimulates the semitendinosus, the lateral
gastrocnemius, the medial gastrocnemius, the rectus femoris, and the
biceps femoris semitendinosus. The PNF decrease abnormally increased
muscle tone. The intervention increased the muscle activity of lower
extremities muscles.
Overall, muscle tone of the upper limb and hand in chronic
stroke improved post the specified Bobath program. These is in
accordance to the previous study that muscle tone impairment and
functions are associated (147). The improvement of spasticity may change
the task being performed of stroke individuals (148). The baseline
impairment was the important predictor of the neuroplastic changing in
response to treatment program (149).
5.2.3.2 Sensation
In the current study, only stereognosis was found to be different
post intervention comparing to the baseline. Movement facilitation
technique based on the Bobath concept provided sensory input such as
proprioception and tactile for the patients (18). This technique helped
enhancing positive changes to the sensory system (150). The sensorimotor
integration induced the cortical reorganization (151, 152). The cortical area
could be modified through cortical reorganization by sensory input,
experience and learning (18, 153). The stereognosis is cortical sensation
(154). Therefore, changes in stereognosis post the Bobath therapy
program in the current study could be explained by the improvement of
Ref. code: 25605812030533ARL

70
somatosensory integration. In the current study, many patients with
stereognosis improvement were intact in other sensations. Activation of
cortex area (primary sensory area) might affect object recognition.
One role of the somatosensory association cortex is sensory information
integration from the primary somatosensory cortex to recognition (155).
Task oriented arm practice has been demonstrated to improve the
cortical area (primary sensory area (S1) activation in patients with stroke
(156). In accordance to the study by Rich and colleagues (2017), changing
in stereognosis was demonstrated post CIMT (task specific training) in
chronic stroke with hemiparesis (157). As the components of the Bobath
therapy used in the current study was task specific training. This could
enhance stereognosis.
Moreover, learning and memory is the essential factor for
emphasizing stereognosis (158). In the current study, intervention
program showed improvement in motor learning as demonstrated by
improved upper limb and hand function. As motor control improved,
patients could explore environments themselves and these also had
positive effect on the stereognosis. The ability of hand, for example,
grasping, releasing and finger movement could influence sensory input
via the hand. In the current study, the decrease in muscle tone, and the
increase of hand ability (the result of hand impairments and function
improvement) may also improve hand sensation through the touching
area in the palm. The association of stereognosis and hand ability has
been demonstrated in children with hemiparetic CP ( 1 5 6 ) . Hand
manipulation improved recognition of the objects such as surface and
shape of the object. Stereognosis improvement has been shown to be
related with improvement in motor deficits (159).
Meyer and colleagues (2016) demonstrated a moderate
relationship between somatosensory (stereognosis) and motor deficits
(r = 0.51-0.60) in patients with subacute stroke (159). Likewise, in the
current study, both motor deficits and stereognosis showed
Ref. code: 25605812030533ARL

71
improvement. A review summarized that treatments minimizing
impairments could enhance the recovery of function post stroke (160).
All other sensory modalities did not show a statistically
significant difference between pre and post assessment. At baseline,
many participants had no deficits in sensation. Therefore, intervention
may not further improve sensory for these participants. This result was
supported by the study by Platz and colleagues (2005) that arm sensation
such as the light touch and joint position sense of arm were not affected
by the Bobath therapy in subacute stroke with severe arm paresis (161).
The practices in their study consisted of muscle tone normalization,
upper limb and hand activities in various positions with and without the
objects, both unilateral and bilateral task in four weeks. Their Bobath
therapy program also considered perception, balance, and movement.
These components of practice are similar to the current study but
practice period and the characteristics of patients are different. The
characteristics of participants were chronic stroke with moderate to
severe deficits in the current study while the participants in their study
were subacute stroke with severe arm paresis.
Limitations of the study
1. Improvement in participation level and quality of life as a result of improvement
in impairments and activities was not explored in the current study.
2. The trainer in the Bobath therapy program must have skill professional or
receive training from an expert.
Ref. code: 25605812030533ARL

72
Clinical implications
1. In this study, the frequency of the Bobath intervention program for improving
upper limb and hand function was three times per week and continued for six
weeks.
2. The Bobath therapy is one appropriate intervention for stroke individuals with
moderate to severe level of deficits. In clinical practice, the Bobath therapy is
applicable in the conjunction with the other appropriate interventions in chronic
stroke with moderate to severe level of deficits.
3. The Bobath intervention program is one appropriate approach to be used for
stroke individuals in communities.
Further study
1. Further exploration shall also address the assessment of the quality of life as
well as the participation restriction of individuals with stroke as a result of
improvement of impairments and activities of upper limb and hand.
2. Further investigation on the retention effect 3, 6 months and one year post
intervention is warrant. If the retention effect is demonstrated, it will be the
indicator for sufficient practice. If there is no retention effect, it will be the
indicator for additional training required.
Ref. code: 25605812030533ARL

73
Chapter 6
Conclusion
6.1 Intra- and inter-rater reliability test of the Wolf Motor Function Test and
Fugl-Meyer assessment of the upper extremity
Overall items of WMFT and FMA presented acceptable to excellent reliability
(ICC ˃ 0.8) for both intra-rater and inter-rater reliability. This ensured that the finding
in this study could demonstrate true effect of the intervention program and not from the
measurement error.
6.2 Effect of the Bobath therapy on upper limb and hand function in stroke
individuals with moderate to severe arm deficits
The findings demonstrated the benefit of the Bobath intervention program in
chronic stroke individuals with moderate to severe deficits. Task specific training with
repetitions, together with specific handling and preparation phase used in the program
improved selective movement and sensorimotor integration which resulted in the
improvement of upper limb and hand functions. All components in the program
promoted wrist and finger extension essential for grasping as well as reaching.
After the intervention, muscle tone of involved muscles in the training program
became more normalized. These are wrist and finger flexors. Among sensory
modalities, only stereognosis showed improvement after the Bobath intervention.
In summary, the findings supported the use of the Bobath therapy within 6 weeks
for enhancing upper limb and hand function as well as impairment minimization in
chronic stroke with moderate to severe arm deficits.
Ref. code: 25605812030533ARL

74
References
1. World Health Organization. Stroke, cerebrovascular [cited 2016 september 20].
Available from: http://www.who.int/topics/cerebrovascular_accident/en/.
2. Suwanwela NC. Stroke Epidemiology in Thailand. Journal of Stroke.
2014;16(1):1-7.
3. Nakayama H, Jorgensen HS, Raaschou HO, Olsen TS. Recovery of upper
extremity function in stroke patients: the Copenhagen Stroke Study. Archives of
Physical Medicine and Rehabilitation. 1994;75(4):394-8.
4. Ramos-MA, Garcia-CE, Walter A, Cho W, Broetz D, Bogdan M, et al.
Decoding upper limb residual muscle activity in severe chronic stroke. Annals of
Clinical and Translational Neurology. 2015;2(1):1-11.
5. Michaelsen SM, Magdalon EC, Levin MF. Grip aperture scaling to object size
in chronic stroke. Motor Control. 2009;13(2):197-217.
6. Waddell KJ, Birkenmeier RL, Moore JL, Hornby TG, Lang CE. Feasibility of
High-Repetition, Task-Specific Training for Individuals With Upper-Extremity
Paresis. The American Journal of Occupational Therapy. 2014;68(4):444-53.
7. Bird T, Choi S, Goodman L, Schmalbrock P, Nichols-Larsen DS. Sensorimotor
training induced neural reorganization after stroke: a case series. Journal of neurologic
physical therapy. 2013;37(1):27-36.
8. Nilsen DM, Gillen G, Gordon AM. Use of mental practice to improve upper-
limb recovery after stroke: a systematic review. The American journal of occupational
therapy. 2010;64(5):695-708.
9. Nadler M, Pauls M. Shoulder orthoses for the prevention and reduction of
hemiplegic shoulder pain and subluxation: Systematic review. Clinical Rehabilitation.
2016.
10. Ploughman M, Shears J, Hutchings L, Osmond M. Constraint-induced
movement therapy for severe upper-extremity impairment after stroke in an outpatient
rehabilitation setting: a case report. Physiotherapy Canada. 2008;60(2):161-70.
11. Glanz M, Klawansky S, Chalmers T. Biofeedback therapy in stroke
rehabilitation: a review. Journal of the Royal Society of Medicine. 1997;90(1):33-9.
Ref. code: 25605812030533ARL

75
12. Kawashima N, Popovic MR, Zivanovic V. Effect of intensive functional
electrical stimulation therapy on upper-limb motor recovery after stroke: case study of
a patient with chronic stroke. Physiotherapy Canada. 2013;65(1):20-8.
13. Park JY, Chang M, Kim KM, Kim HJ. The effect of mirror therapy on upper-
extremity function and activities of daily living in stroke patients. Journal of Physical
Therapy Science. 2015;27(6):1681-3.
14. Chang WH, Kim YH. Robot-assisted therapy in stroke rehabilitation. Journal of
stroke. 2013;15(3):174-81.
15. Saposnik G, Levin M. Virtual reality in stroke rehabilitation: a meta-analysis
and implications for clinicians. Stroke. 2011;42.
16. Hillier S, Inglis-JG. Rehabilitation for community-dwelling people with stroke:
home or centre based? a systematic review. International Journal of Stroke.
2010;5(3):178-86.
17. Lennon S. The Bobath concept: a critical review of the theoretical assumptions
that guide physiotherapy practice in stroke rehabilitation. Physical Therapy Reviews.
1996;1(1):35-45.
18. Sue Raine LM, Mary Lynch-Ellerington. Bobath concept theory and clinical
practice in neurological rehabilitation. United kingdom: Blackwell Publishing; 2009.
19. Raine S. The current theoretical assumptions of the Bobath concept as
determined by the members of BBTA. Physiotherapy Theory and Practice.
2007;23(3):137-52.
20. Wang RY, Chen HI, Chen CY, Yang YR. Efficacy of Bobath versus
orthopaedic approach on impairment and function at different motor recovery stages
after stroke: a randomized controlled study. Clinical Rehabilitation. 2005;19(2):155-
64.
21. Mikolajewska E. NDT-Bobath method in normalization of muscle tone in post-
stroke patients. Advances in Clinical and Experimental Medicine. 2012;21(4):513-7.
22. Huseyinsinoglu BE, Ozdincler AR, Krespi Y. Bobath Concept versus
constraint-induced movement therapy to improve arm functional recovery in stroke
patients: a randomized controlled trial. Clinical Rehabilitation. 2012;26(8):705-15.
Ref. code: 25605812030533ARL

76
23. Platz T, Eickhof E, Van KS, Engel U, Pinkowski C, Kalok S, Pause M.
Impairment-oriented training or Bobath therapy for severe arm paresis after stroke: a
single-blind, multicentre randomized controlled trial. Clinical Rehabilitation.
2005:714-24.
24. Sacco RL, Kasner SE, Broderick JP, Caplan LR, Connors JJ, Culebras A, et al.
An Updated Definition of Stroke for the 21st Century. A Statement for Healthcare
Professionals From the American Heart Association/American Stroke Association.
2013;44(7):2064-89.
25. Al-Dughmi M, Al-Sharman A, Stevens S, Siengsukon CF. Sleep characteristics
of individuals with chronic stroke: a pilot study. Dove Medical Press; 2015 10/21. 139-
45 p.
26. Stein J, Harvey RL, Winstein CJ, Zorowitz RD, Wittenber GF. Stroke recovery
and rehabilitation. 2nd ed. Springer Publishing Company; 2014.
27. Perna R, Temple J. Rehabilitation outcomes: ischemic versus hemorrhagic
strokes. Behavioural Neurology. 2015;2015:891651.
28. Disease BoNC. Mortalrity ratio amout of non-communicable disease in the
budget 2557 BE 2558 [cited 2559 september 20]. Available from:
http://www.thaincd.com/information-statistic/non-communicable-disease-data.php.
29. World Stroke Organization. World stroke campaign 2558 [cited 2559 september
20]. Available from: http://www.worldstrokecampaign.org.
30. Di Carlo A. Human and economic burden of stroke. Age and Ageing.
2009;38(1):4-5.
31. Rosamond WD, Folsom AR, Chambless LE, Wang C-H, McGovern PG,
Howard G, et al. Stroke Incidence and Survival Among Middle-Aged Adults. Stroke.
1999;30(4):736.
32. Pripwai N, Phongpattanawoot U, Katsomboon K, Injai R, Lacomme N.
Incidence of new case ischemic stroke patients at Phrae Hospital. Journal of The Phrae
Hospital. 2014;21(1):7-18.
33. Kelly-Hayes M, Robertson JT, Broderick JP, Duncan PW, Hershey LA, Roth
EJ, et al. The American Heart Association Stroke Outcome Classification: executive
summary. Circulation. 1998;97(24):2474-8.
Ref. code: 25605812030533ARL

77
34. Shim S, Kim H, Jung J. Comparison of upper extremity motor recovery of
stroke patients with actual physical activity in their daily lives measured with
accelerometers. Journal of Physical Therapy Science. 2014;26(7):1009-11.
35. Kwakkel G, Kollen BJ, van der Grond J, Prevo AJ. Probability of regaining
dexterity in the flaccid upper limb: impact of severity of paresis and time since onset in
acute stroke. Stroke. 2003;34(9):2181-6.
36. Gladstone DJ, Danells CJ, Black SE. The fugl-meyer assessment of motor
recovery after stroke: a critical review of its measurement properties.
Neurorehabilitation and Neural Repair. 2002;16(3):232-40.
37. Dobkin, B. H. Motor rehabilitation after stroke, traumatic brain, and spinal cord
injury: common denominators within recent clinical trials. Current Opinion in
Neurology. 2009;22.
38. Duncan PW, Goldstein LB, Matchar D, Divine GW, Feussner J. Measurement
of motor recovery after stroke. Outcome assessment and sample size requirements.
Stroke. 1992;23(8):1084-9.
39. University of California SD. A Practical Guide to Clinical Medicine [internet].
[cited 2559 september 20]. Available from: https://meded.ucsd.edu/clinicalmed
/neuro2.htm.
40. Jehkonen M, Laihosalo M, Kettunen JE. Impact of neglect on functional
outcome after stroke: a review of methodological issues and recent research findings.
Restorative Neurology and Neuroscience. 2006;24(4-6):209-15.
41. Jorgensen HS, Nakayama H, Reith J, Raaschou HO, Olsen TS. Stroke
recurrence: predictors, severity, and prognosis. The Copenhagen Stroke Study.
Neurology. 1997;48(4):891-5.
42. Parry RH, Lincoln NB, Vass CD. Effect of severity of arm impairment on
response to additional physiotherapy early after stroke. Clinical Rehabilitation.
1999;13(3):187-98
43. Sainburg RL, Duff SV. Does motor lateralization have implications for stroke
rehabilitation?. Journal of Rehabilitation Research & Development. 2006;43(3):311-
22.
44. Nair RD, Lincoln NB. Cognitive rehabilitation for memory deficits following
stroke. The Cochrane Database of Systematic Reviews. 2007(3):Cd002293.
Ref. code: 25605812030533ARL

78
45. Gebruers N, Truijen S, Engelborghs S, De Deyn PP. Prediction of upper limb
recovery, general disability, and rehabilitation status by activity measurements assessed
by accelerometers or the Fugl-Meyer score in acute stroke. American Journal of
Physical Medicine & Rehabilitation. 2014;93(3):245-52.
46. Nakayma H, Jørgensen HS, Raaschou HO, Olsen TS. Compensation in recovery
of upper extremity function after stroke: The Copenhagen Stroke Study. Archives of
Physical Medicine and Rehabilitation.75(8):852-7.
47. Kleim JA, Jones TA. Principles of experience-dependent neural plasticity:
implications for rehabilitation after brain damage. Journal of Speech Language and
Hearing Research. 2008;51(1):S225-39.
48. Katrak PH. Shoulder shrug--a prognostic sign for recovery of hand movement
after stroke. The Medical Journal of Australia. 1990;152(6):297-301.
49. Katrak P, Bowring G, Conroy P, Chilvers M, Poulos R, McNeil D. Predicting
upper limb recovery after stroke: the place of early shoulder and hand movement.
Archives of Physical Medicine and Rehabilitation. 1998;79(7):758-61.
50. G. Broeks J, Lankhorst GJ, Rumping K, Prevo AJH. The long-term outcome of
arm function after stroke: results of a follow-up study. Disability and Rehabilitation.
1999;21(8):357-64.
51. Yoo C, Park J. Impact of task-oriented training on hand function and activities
of daily living after stroke. Journal of Physical Therapy Science. 2015;27(8):2529-31.
52. Logsdon RG, McCurry SM, Teri L. Evidence-Based Interventions to Improve
Quality of Life for Individuals with Dementia. Alzheimers care today. 2007;8(4):309-
18.
53. Graef P, Michaelsen SM, Dadalt ML, Rodrigues DA, Pereira F, Pagnussat AS.
Effects of functional and analytical strength training on upper-extremity activity after
stroke: a randomized controlled trial. Brazilian Journal of Physical Therapy. 2016:0.
54. Lang CE, Macdonald JR, Reisman DS, Boyd L, Jacobson Kimberley T,
Schindler-Ivens SM, et al. Observation of amounts of movement practice provided
during stroke rehabilitation. Archives of Physical Medicine and Rehabilitation
. 2009;90(10):1692-8.
Ref. code: 25605812030533ARL

79
55. Waddell KJ, Birkenmeier RL, Moore JL, Hornby TG, Lang CE. Feasibility of
high-repetition, task-specific training for individuals with upper-extremity paresis.
American Journal of Occupational Therapy. 2014;68(4):444-53.
56. Sousa Nanji L, Torres Cardoso A, Costa J, Vaz-Carneiro A. [Analysis of the
Cochrane Review: Interventions for Improving Upper Limb Function after Stroke.
Cochrane Database Syst Rev. 2014,11:CD010820]. Acta Medica Portuguesa.
2015;28(5):551-3.
57. Kwakkel G, Veerbeek JM, van Wegen EEH, Wolf SL. Constraint-Induced
Movement Therapy after Stroke. The Lancet Neurology. 2015;14(2):224-34.
58. Raghavan P, Geller D, Guerrero N, Aluru V, Eimicke JP, Teresi JA, et al. Music
upper limb therapy-integrated: an enriched collaborative approach for stroke
rehabilitation. Frontiers in Human Neuroscience. 2016;10:498.
59. Chan IH, Fong KN. Effects of arm weight support training to promote recovery
of upper limb function for subacute patients after stroke with different levels of arm
impairments. BioMed Research International. 2016:9346374.
60. Lin KC, Chen YA, Chen CL, Wu CY, Chang YF. The effects of bilateral arm
training on motor control and functional performance in chronic stroke: a randomized
controlled study. Neurorehabilitation and Neural Repair. 2010;24(1):42-51.
61. Brunner I, Skouen JS, Hofstad H, Strand LI, Becker F, Sanders A-M, et al.
Virtual reality training for upper extremity in subacute stroke (VIRTUES): study
protocol for a randomized controlled multicenter trial. BMC Neurology.
2014;14(1):186.
62. Graef P, Dadalt ML, Rodrigues DA, Stein C, Pagnussat Ade S. Transcranial
magnetic stimulation combined with upper-limb training for improving function after
stroke: A systematic review and meta-analysis. Journal of the Neurological Sciences.
2016;369:149-58.
63. Walker MF, Sunnerhagen KS, Fisher RJ. Evidence-Based Community Stroke
Rehabilitation. Stroke. 2012;44(1):293.
64. Chaiyawat P, Kulkantrakorn K, Sritipsukho P. Effectiveness of home
rehabilitation for ischemic stroke. Neurology International. 2009;1(1):e10.
Ref. code: 25605812030533ARL

80
65. Koc A. Exercise in patients with subacute stroke: A randomized, controlled
pilot study of home-based exercise in subacute stroke. Stroke. 2015;52(3):541-7.
66. Bernocchi P, Vanoglio F, Baratti D, Morini R, Rocchi S, Luisa A, et al. Home-
based telesurveillance and rehabilitation after stroke: a real-life study. Topics in Stroke
Rehabilitation. 2016;23(2):106-15.
67. Muratori LM, Lamberg EM, Quinn L, Duff SV. Applying principles of motor
learning and control to upper extremity rehabilitation. Journal of hand therapy.
2013;26(2):94-103.
68. Bassoe Gjelsvik BE. The Bobath Concept in Adult Neurology; 2008. 238 p.
69. Feldman AG, Levin MF. The equilibrium-point hypothesis-past, present and
future. Advances in Experimental Medicine and Biology. 2009;629:699-726.
70. Chandran AP, Maini BK, Marya RK. Long latency inhibition of H-reflex
recovery by cutaneous tactile stimulation in man: a cutaneous transcortical reflex.
Neuroscience. 1988;27(3):1037-48.
71. Bernshtein NA. The co-ordination and regulation of movements: Oxford, New
York, Pergamon Press [1967]; 1967.
72. Wishart LR, Lee, T.D.,Ezekiel, H.J., Marley, T.L.& Lehto, N.K. Application of
motor learning principles: The physiotherapy client as a problem-solver. I.
Physiotherapy Canada. 2000:229-32
73. Lehto NK, Marley, T.L., Ezekiel, H.J., et al. Application of motor learning
principles: The physiotherapy client as a problem-solver. IV. Physiotherapy Canada ;
2001.
74. Schmidt RA, Wrisberg CA. Motor Learning and Performance. Book News, Inc.,
Portland, 2000.
75. Langhammer B, Stanghelle JK. Can physiotherapy after stroke based on the
Bobath concept result in improved quality of movement compared to the motor
relearning programme. Physiotherapy Research International. 2011;16(2):69-80.
76. Ayla Fil KA. The effect of electrical stimulation in combination with Bobath
techniques in the prevention of shoulder subluxation in acute stroke patients. Clinical
Rehabilitation. 2011:51-9.
Ref. code: 25605812030533ARL

81
77. Platz T, Pinkowski C, van WF, Kim IH, di Bella P, Johnson G. Reliability and
validity of arm function assessment with standardized guidelines for the Fugl-Meyer
Test, Action Research Arm Test and Box and Block Test: a multicentre study. Clinical
Rehabilitation. 2005;19.
78. Lin JH, Hsu MJ, Sheu CF, Wu TS, Lin RT, Chen CH, et al. Psychometric
comparisons of 4 measures for assessing upper-extremity function in people with
stroke. Physical Therapy. 2009;89(8):840-50.
79. Cho S, Kim WS, Paik NJ, Bang H. Upper-Limb Function Assessment Using
VBBTs for Stroke Patients. IEEE International Conference on Rehabilitation Robotics.
2016;36(1):70-8.
80. Gowland C, Stratford P, Ward M, Moreland J, Torresin W, Van Hullenaar S, et
al. Measuring physical impairment and disability with the Chedoke-McMaster Stroke
Assessment. Stroke. 1993;24(1):58.
81. Morris DM, Uswatte G, Crago JE, Cook EW, 3rd, Taub E. The reliability of the
wolf motor function test for assessing upper extremity function after stroke. Archives
of Physical Medicine and Rehabilitation. 2001;82(6):750-5.
82. Lin KC, Hsieh YW, Wu CY, Chen CL, Jang Y, Liu JS. Minimal detectable
change and clinically important difference of the Wolf Motor Function Test in stroke
patients. Neurorehabilitation and Neural Repair. 2009;23(5):429-34.
83. Tsuji T, Liu M, Sonoda S, Domen K, Chino N. The stroke impairment
assessment set: its internal consistency and predictive validity. Archives of Physical
Medicine and Rehabilitation. 2000;81(7):863-8.
84. Gowland C, Stratford P, Ward M, Moreland J, Torresin W, Van Hullenaar S, et
al. Measuring physical impairment and disability with the Chedoke-McMaster Stroke
Assessment. Stroke. 1993;24(1):58-63.
85. Lang CE, Bland MD, Bailey RR, Schaefer SY, Birkenmeier RL. Assessment of
upper extremity impairment, function, and activity following stroke: foundations for
clinical decision making. Journal of Hand Therapy. 2013;26(2):104-15.
86. Roach S, San Juan JG, Suprak DN, Lyda M. Concurrent Validity of digital
inclinometer and universal goniometer in assessing passive hip mobility in health
subject. International Journal of Sports Physical Therapy. 2013;8(5):680-8.
Ref. code: 25605812030533ARL

82
87. Fluet MC, Lambercy O, Gassert R. Upper limb assessment using a Virtual Peg
Insertion Test. The IEEE International Conference on Rehabilitation Robotics.
2011;2011:5975348.
88. Hsieh Y-w, Wu C-y, Lin K-c, Chang Y-f, Chen C-l, Liu J-s. Responsiveness
and Validity of Three Outcome Measures of Motor Function After Stroke
Rehabilitation. Stroke. 2009;40(4):1386-91.
89. Sullivan KJ, Tilson JK, Cen SY, Rose DK, Hershberg J, Correa A, et al. Fugl-
Meyer assessment of sensorimotor function after stroke. Stroke. 2011;42(2):427.
90. Varoqui D, Niu X, Mirbagheri MM. Ankle voluntary movement enhancement
following robotic-assisted locomotor training in spinal cord injury. Journal of
NeuroEngineering and Rehabilitation. 2014;11:46.
91. Kolber MJ, Hanney WJ. The reliability and concurrent validity of shoulder
mobility measurements using a digital inclinometer and goniometer: a technical report.
International Journal of Sports Physical Therapy. 2012;7(3):306-13.
92. Damiano DL, Quinlivan JM, Owen BF, Payne P, Nelson KC, Abel MF. What
does the Ashworth scale really measure and are instrumented measures more valid and
precise?. Developmental Medicine and Child Neurology. 2002;44(2):112-8.
93. Gregson JM, Leathley M, Moore AP, Sharma AK, Smith TL, Watkins CL.
Reliability of the Tone Assessment Scale and the modified Ashworth scale as clinical
tools for assessing poststroke spasticity. Archives of Physical Medicine and
Rehabilitation. 1999;80(9):1013-6.
94. Lin FM, Sabbahi M. Correlation of spasticity with hyperactive stretch reflexes
and motor dysfunction in hemiplegia. Archives of Physical Medicine and
Rehabilitation. 1999;80(5):526-30.
95. Lincoln NB, Jackson JM, Adams SA. Reliability and Revision of the
Nottingham Sensory Assessment for Stroke Patients. Physiotherapy. 1998;84(8):358-
65.
Ref. code: 25605812030533ARL

83
96. Stolk HF, Crow JL, Hendriks EP, Van der BR, Harmeling-van der Wel BC. The
Erasmus MC modifications to the (revised) Nottingham Sensory Assessment: a reliable
somatosensory assessment measure for patients with intracranial disorders. Clinical
Rehabilitation. 2006;20(2):160-72.
97. Wu CY, Chuang IC, Ma HI, Lin KC, Chen CL. Validity and Responsiveness of
the Revised Nottingham Sensation Assessment for Outcome Evaluation in Stroke
Rehabilitation. The American Journal of Occupational Therapy.
2016;70(2):7002290040p1-8.
98. Patumanond J. Medical Epidemiology. Chaingmai: A PHRCG Publication;
1998.
99. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual
Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill
Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ),
Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and
Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis
Care & Research. 2011;63 Suppl 11:S240-52.
100. Nijland R, van Wegen E, Verbunt J, van Wijk R, van Kordelaar J, Kwakkel G.
A comparison of two validated tests for upper limb function after stroke: The Wolf
Motor Function Test and the Action Research Arm Test. Journal of Rehabilitation
Medicine. 2010;42(7):694-6.
101. Sullivan KJ, Tilson JK, Cen SY, Rose DK, Hershberg J, Correa A, et al. Fugl-
Meyer assessment of sensorimotor function after stroke: standardized training
procedure for clinical practice and clinical trials. Stroke. 2011;42(2):427-32.
102. Kim H, Her J, Ko J, Park D-s, Woo J-H, You Y, et al. Reliability, Concurrent
Validity, and Responsiveness of the Fugl-Meyer Assessment (FMA) for Hemiplegic
Patients. Journal of Physical Therapy Science. 2012;24(9):893-9.
103. Sanford J, Moreland J, Swanson LR, Stratford PW, Gowland C. Reliability of
the Fugl-Meyer assessment for testing motor performance in patients following stroke.
Physical Therapy. 1993;73(7):447-54.
104. Kollen BJ, Lennon S, Lyons B, Wheatley-Smith L, Scheper M, Buurke JH, et
al. The effectiveness of the Bobath concept in stroke rehabilitation: what is the
evidence?. Stroke. 2009;40(4):e89-97.
Ref. code: 25605812030533ARL

84
105. Richard Harvey MD (Editor) JSME, Carolee Winstein Phd PT (Editor), George
Wittenberg MD PhD (Editor), Richard Zorowitz MD (Editor). Stroke Recovery and
Rehabilitation, 2nd Edition ed: 2014; 2014. 888 p.
106. Ezekiel H, R. Wishart L, D. Lee T, L. Marley T, K. Lehto N. Application of
motor learning principles: the physiotherapy client as a problem-solver. 1. Concepts. ;
2000. 229 p.
107. Ezekiel H, L. Lehto N, L. Marley T, R. Wishart L, D. Lee T, Jarus T.
Application of motor learning principles: The physiotherapy client as a problem-solver.
IV. Physiotherapy Canada; 2001. 109 p.
108. Fregnac Y, Bathellier B. Cortical Correlates of Low-Level Perception: From
Neural Circuits to Percepts. Neuron. 2015;88(1):110-26.
109. Popa T, Velayudhan B, Hubsch C, Pradeep S, Roze E, Vidailhet M, et al.
Cerebellar Processing of Sensory Inputs Primes Motor Cortex Plasticity. Cerebral
Cortex. 2013;23(2):305-14.
110. Robert Teasell Md SPM, Andreea Cotoi Msc. Evidence-Based Review of
Stroke Rehabilitation[Internet]; 2016. [cited 2018 7th March]. Available from:
www.ebrsr.com.
111. Tseng MC, Chang KC. Stroke severity and early recovery after first-ever
ischemic stroke: results of a hospital-based study in Taiwan. Health Policy.
2006;79(1):73-8.
112. Van Kuijk AA, Pasman JW, Hendricks HT, Zwarts MJ, Geurts AC. Predicting
hand motor recovery in severe stroke: the role of motor evoked potentials in relation to
early clinical assessment. Neurorehabilitation and Neural Repair. 2009;23(1):45-51.
113. Mazzoleni S, Battini E, Crecchi R, Dario P, Posteraro F. Upper limb robot-
assisted therapy in subacute and chronic stroke patients using an innovative end-
effector haptic device: A pilot study. NeuroRehabilitation. 2018;42(1):43-52.
114. Liu M, Fujiwara T, Shindo K, Kasashima Y, Otaka Y, Tsuji T, et al. Newer
challenges to restore hemiparetic upper extremity after stroke: HANDS therapy and
BMI neurorehabilitation. Hong Kong Physiotherapy Journal. 2012;30(2):83-92.
115. Llorens R, Noe E, Colomer C, Alcaniz M, Deutsch JE. Time since injury limits
but does not prevent improvement and maintenance of gains in balance in chronic
stroke. Brain Injury. 2018;32(3):303-9.
Ref. code: 25605812030533ARL

85
116. Ezekiel H, K. Lehto N, L. Marley T, R. Wishart L, D. Lee T. Application of
Motor Learning Principles: The Physiotherapy Client as a Problem-Solver. III
Augmented Feedback. Physiotherapy Canada. 2001;33 p.
117. Valkenborghs SR, Visser MM, Dunn A, Erickson KI, Nilsson M, Callister R, et
al. AExaCTT – Aerobic Exercise and Consecutive Task-specific Training for the upper
limb after stroke: Protocol for a randomised controlled pilot study. Contemporary
Clinical Trials Communications. 2017;7:179-85.
118. Abdullahia A. Effects of Number of repetitions and Number of Hours of shaping
Practice during Constraint Induced Movement Therapy: A Randomized Controlled
Trial. 2016.
119. Andrieux M, Boutin A, Thon B. Self-Control of Task Difficulty During Early
Practice Promotes Motor Skill Learning. Journal of Motor Behavior. 2016;48(1):57-65.
120. Edwards DF. An analysis of normal movement as the basis for the development
of treatment techniques. Edinburgh: Harcourt Publishers Limited; 2002.
121. Wee SK, Hughes A-M, Warner MB, Brown S, Cranny A, Mazomenos EB, et
al. Effect of Trunk Support on Upper Extremity Function in People With Chronic
Stroke and People Who Are Healthy. Physical Therapy. 2015;95(8):1163-71.
122. Behm DG, Drinkwater EJ, Willardson JM, Cowley PM. The use of instability
to train the core musculature. Applied Physiology, Nutrition, and Metabolism.
2010;35(1):91-108.
123. Luke C, Dodd KJ, Brock K. Outcomes of the Bobath concept on upper limb
recovery following stroke. Clinical Rehabilitation. 2004;18(8):888-98.
124. Levin MF, Panturin E. Sensorimotor integration for functional recovery and the
Bobath approach. Motor Control. 2011;15(2):285-301.
125. Schmidt RAL, Timothy D. Motor control and learning: A behavioral emphasis,
4th ed. Champaign, Illinois, USA: Human Kinetics; 2005.
Ref. code: 25605812030533ARL

86
126. Wolf SL, Lecraw DE, Barton LA, Jann BB. Forced use of hemiplegic upper
extremities to reverse the effect of learned nonuse among chronic stroke and head-
injured patients. Experimental Neurology. 1989;104(2):125-32.
127. Liu W, Whitall J, Kepple TM. Multi-Joint Coordination of Functional Arm
Reaching: Induced Position Analysis. Journal of Applied Biomechanics.
2013;29(2):235-40.
128. Jaric S, Uygur M. Assessment of Hand Function Through the Coordination of
Contact Forces in Manipulation Tasks. Journal of Human Kinetics. 2013;36:5-15.
129. Combs SA, Finley MA, Henss M, Himmler S, Lapota K, Stillwell D. Effects of
a repetitive gaming intervention on upper extremity impairments and function in
persons with chronic stroke: a preliminary study. Disability and Rehabilitation.
2012;34(15):1291-8.
130. Cirstea CM, Ptito A, Levin MF. Feedback and cognition in arm motor skill
reacquisition after stroke. Stroke. 2006;37(5):1237-42.
131. Kim D. The effects of hand strength on upper extremity function and activities
of daily living in stroke patients, with a focus on right hemiplegia. Journal of Physical
Therapy Science. 2016;28(9):2565-7.
132. Popovic MR, Thrasher TA, Zivanovic V, Takaki J, Hajek V. Neuroprosthesis
for retraining reaching and grasping functions in severe hemiplegic patients.
Neuromodulation. 2005;8(1):58-72.
133. Nichols-Larsen DS, Clark PC, Zeringue A, Greenspan A, Blanton S. Factors
influencing stroke survivors' quality of life during subacute recovery. Stroke.
2005;36(7):1480-4.
134. Hosp JA, Luft AR. Cortical Plasticity during Motor Learning and Recovery
after Ischemic Stroke. Neural Plasticity. 2011;2011:871296.
135. Lieber RL. Skeletal Muscle Structure, Function, and Plasticity. 2nd ed.
Baltimore: Lippincott Williams and Williams and Wilkins; 2002.
136. Carey JR KT, Lewis SM, Auerbach EJ, Dorsey L, Rundquist P, Ugurbil K.
Analysis of fMRI and finger tracking training in subjects with chronic stroke. Brain
Injury. 2002(125):773-88.
Ref. code: 25605812030533ARL

87
137. Yang J, Lee J, Lee B, Jeon S, Han B, Han D. The Effects of Active Scapular
Protraction on the Muscle Activation and Function of the Upper Extremity. Journal of
Physical Therapy Science. 2014;26(4):599-603.
138. Song C-S. Effects of Scapular Stabilization Exercise on Function of Paretic
Upper Extremity of Chronic Stroke Patients. Journal of Physical Therapy Science.
2013. 403-5 p.
139. Moon S-H, Choi J-H, Park S-E. The effects of functional electrical stimulation
on muscle tone and stiffness of stroke patients. Journal of Physical Therapy Science.
2017;29(2):238-41.
140. Marciniak C. Poststroke hypertonicity: upper limb assessment and treatment.
Topics in Stroke Rehabilitation. 2011;18(3):179-94.
141. Mottram CJ, Wallace CL, Chikando CN, Rymer WZ. Origins of spontaneous
firing of motor units in the spastic-paretic biceps brachii muscle of stroke survivors.
Journal of Neurophysiology. 2010;104(6):3168-79.
142. Bakhtiary AH, Fatemy E. Does electrical stimulation reduce spasticity after
stroke? A randomized controlled study. Clinical Rehabilitation. 2008;22(5):418-25.
143. Lee G, An S, Lee Y, Lee D, Park D-s. Predictive factors of hypertonia in the
upper extremity of chronic stroke survivors. Journal of Physical Therapy Science.
2015;27(8):2545-9.
144. Ali S, Shahzad M. The effectiveness of sustained stretching in post stroke upper
limb spasticity. Archives of Physical Medicine and Rehabilitation. 2012. 30-4 p.
145. Gorkovenko AV, Sawczyn S, Bulgakova NV, Jasczur-Nowicki J, Mishchenko
VS, Kostyukov AI. Muscle agonist–antagonist interactions in an experimental joint
model. Experimental Brain Research Experimentelle Hirnforschung Experimentation
Cerebrale. 2012;222(4):399-414.
146. Wang J-S, Lee S-B, Moon S-H. The immediate effect of PNF pattern on muscle
tone and muscle stiffness in chronic stroke patient. Journal of Physical Therapy
Science. 2016;28(3):967-70.
147. Sommerfeld DK, Eek EU, Svensson AK, Holmqvist LW, Arbin MH. Spasticity
after stroke: its occurrence and association with motor impairments and activity
limitations. Stroke. 2004;35(1):134-9.
Ref. code: 25605812030533ARL

88
148. Yelnik A, Albert T, Bonan I, Laffont I. A Clinical Guide to Assess the Role of
Lower Limb Extensor Overactivity in Hemiplegic Gait Disorders. Stroke.
1999;30(3):580.
149. Pundik S, McCabe JP, Hrovat K, Fredrickson AE, Tatsuoka C, Feng IJ, et al.
Recovery of post stroke proximal arm function, driven by complex neuroplastic
bilateral brain activation patterns and predicted by baseline motor dysfunction severity.
Frontiers in Human Neuroscience. 2015;9:394.
150. Smania N, Montagnana B, Faccioli S, Fiaschi A, Aglioti SM. Rehabilitation of
somatic sensation and related deficit of motor control in patients with pure sensory
stroke. Archives of Physical Medicine and Rehabilitation. 2003;84(11):1692-702.
151. Machado S, Cunha M, Velasques B, Minc D, Teixeira S, Domingues CA, et al.
Sensorimotor integration: basic concepts, abnormalities related to movement disorders
and sensorimotor training-induced cortical reorganization. Revista de Neurologia.
2010;51(7):427-36.
152. Monfils MH, Plautz EJ, Kleim JA. In search of the motor engram: motor map
plasticity as a mechanism for encoding motor experience. Neuroscientist.
2005;11(5):471-83.
153. Nudo RJ. Postinfarct cortical plasticity and behavioral recovery. Stroke.
2007;38:840-5.
154. Bassetti C, Bogousslavsky J, Regli F. Sensory syndromes in parietal stroke.
Neurology 1993. 1942-9 p.
155. Arslan OE. Chapter 3 - Computational Basis of Neural Elements. In: Puri M,
Pathak Y, Sutariya VK, Tipparaju S, Moreno W, editors. Artificial Neural Network for
Drug Design, Delivery and Disposition. Boston: Academic Press; 2016. p. 29-82.
156. Carlson M, Brooks C. The Effect of altered hand position and motor skills on
stereognosis. Journal Of Hand Surgery-American Volume. 2009. 896-9 p.
157. Rich T, Cassidy J, Menk J, Van Heest A, Krach L, Carey J, et al. Stability of
stereognosis after pediatric repetitive transcranial magnetic stimulation and constraint-
induced movement therapy clinical trial. Developmental Neurorehabilitation.
2017;20(3):169-72.
158. Irving, J.B. Stereognosis, Journal of the Royal Medical Society 1968, 6(2), pp.
23, 25-27
Ref. code: 25605812030533ARL

89
159. Meyer S, De Bruyn N, Lafosse C, Van Dijk M, Michielsen M, Thijs L, et al.
Somatosensory Impairments in the upper limb poststroke: Distribution and Association
With Motor Function and Visuospatial Neglect. Neurorehabilitation and Neural Repair.
2016;30(8):731-42.
160. Ward NS, Cohen LG. Mechanisms underlying recovery of motor function after
stroke. Archives of neurology. 2004;61(12):1844-8.
161. Platz T, Eickhof C, van Kaick S, Engel U, Pinkowski C, Kalok S, et al.
Impairment-oriented training or Bobath therapy for severe arm paresis after stroke: a
single-blind, multicentre randomized controlled trial. Clinical Rehabilitation.
2005;19(7):714-24.
162. Department of Mental Health, Ministry of Public Health. MMSE - Thai 2002.
Bangkok: beyond publishing; 2012.
163. Gould D. Visual Analogue Scale (VAS). Journal of Clinical Nursing.
2001;10:697-706.
164. Measurement Instrument Database for the Social Sciences (MIDSS). Wolf
Motor Function Test (WMFT) [Internet] 2011 [cited 2016 7th July ]. Available from:
http://www.midss.org/wolf-motor-function-test-wmft.
165. Canadian Partnership for Stroke Recovery Fugl-Meyer assessment of
sensorimotor recovery after stroke (FMA) (FMA) [Internet]; 2010 [cited 2016 7th July
]. Available from: https://neurophys.gu.se/digitalAssets/1520/1520603_fma-ue-
protocol-english-updated-20150311.pdf.
166. Canadian Partnership for Stroke Recovery. Modified Ashworth Scale
[Internet]; 1999 [cited 2016 7th July]. Available from:https://www.strokengine.ca/
en/assess/mashs/.
167. Nottingham University. Nottingham Sensory Assessment Revised [Internet];
2007.[cited 2016 7th July]. Available from:httpshttps://www.nottingham.ac.uk/
medicine/about/rehabilitationageing/%20publishedassessments.aspx.
Ref. code: 25605812030533ARL

90
APPENDICES
Ref. code: 25605812030533ARL

91
APPENDIX A
Ethical approval
APPENDIX A
Ethical approval
Ref. code: 25605812030533ARL
92
Ref. code: 25605812030533ARL

93
Ref. code: 25605812030533ARL

94
APPENDIX B
Participant Information Sheet
ขอมลส ำหรบอำสำสมครวจย (Participant Information Sheet)
โครงกำรวจย ชอเรอง (ไทย) : ผลของการรกษาดวยแนวคดของโบบาธตอการท างานของแขนและมอ ในผปวยโรคหลอดเลอดสมองทมปญหาการท างานของรยางคสวนบนระดบปานกลางถงรนแรง ชอเรอง (ภำษำองกฤษ) : The effect of Bobath therapy on upper limb and hand function in stroke individuals with moderate to severe arm deficit
ชอผวจย นางสาวธนยชนก พมประสาท ต าแหนง นกศกษาปรญญาโท สถานทตดตอผวจย
(สถานศกษา) ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (สถานศกษา)02-986-9213-9 โทรศพทมอถอ 082-3243681 E-mail [email protected]
อำจำรยทปรกษำวจยหลก อ.ดร. ผกามาศ พรยะประสาธน สถานทตดตอ
ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-926-9213-9 ตอ 7256 โทรศพทมอถอ 081-6152622
E-mail [email protected]
อำจำรยทปรกษำวจยรอง ผชวยศาสตราจารย ดร.นพพล ประโมทยกล
ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร
โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7237 โทรศพทมอถอ 086-6448738
E-mail [email protected]
AF 04_07
Ref. code: 25605812030533ARL

95
กอนททานจะตดสนใจเขารวมการวจย ทานควรท าความเขาใจถงเหตผล และทราบวางานวจยนเกยวของกบอะไร กรณาใชเวลาในการอานขอมลตอไปนอยางละเอยดรอบคอบ และสอบถามขอมลเพมเตมหรอขอมลทไมชดเจนไดตลอดเวลา
1. เหตผลและควำมจ ำเปนทตองท ำกำรวจย โรคหลอดเลอดสมองน าไปสความพการ ผปวยโรคหลอดเลอดสมองระยะเรอรง (นานกวา 6
เดอน) ยงพบความผดปกตและบกพรองและจ ากดการท ากจกรรมตางๆ และผปวยโรคหลอดเลอด
สมองจ านวนมากทมปญหาการใชงานแขนและมอขางทออนแรง
โดยหลกการของการรกษาดวยแนวคดของโบบาธคอ เทคนคการใชมอของนกกายภาพบ าบด
ในการฝกเพอกระตนการท างานของกลามเนอโดย เนนการทรงตว การเคลอนไหวทเปนปกต และ
กระบวนการกระตนระบบประสาทสมผส โดยผานการใหแรงกดและดงผานขอตอตางๆของรยางค
สวนบนและมอ ซงมความเหมาะสมทสามารถน าไปใชในการฝกผปวยในชมชน ดวยเทคนคการรกษา
และการน าไปใชกบผปวยไดงาย ในการศกษากอนหนาทมการรกษาดวยแนวคดของโบบาธ แสดงให
เหนวามการเพมขนของการท างานของแขนและมอในผปวยโรคหลอดเลอดสมองระยะเรอรง แตยง
ขาดรายละเอยดทมความเฉพาะเจาะจงของการรกษา
2.วตถประสงคของกำรวจย
กำรศกษำควำมนำเชอถอของกำรประเมนหลกทใชในงำนวจย
1. เพอหาคาความนาเชอถอในการวดซ าของแบบประเมน Wolf Motor Function Test และ Fugl-Meyer assessment of the upper extremity โดยผวด (assessor) แตละคน
2. เพอหาคาความนาเชอถอระหวางผวดทงสองคน (assessors) ของแบบประเมน Wolf Motor Function Test และ Fugl-Meyer assessment of the upper extremity
3. รำยละเอยดของอำสำสมคร ผปวยโรคหลอดเลอดสมองในจงหวดปทมธาน
เกณฑกำรคดเขำ
1) เปนโรคหลอดเลอดครงแรก
2) มอายตงแต 45 ปขนไป
Ref. code: 25605812030533ARL
96
3) มความบกพรองการท างานของรยางคสวนบนและมอระดบปานกลางถงรนแรง ประเมนดวย
แบบประเมนความบกพรองในการเคลอนไหวรยางคสวนบน(Fugl-Meyer Upper
Extremity Motor Assessment
4) มสญญาณชพคงท ไดแก อตราการเตนของหวใจ อตราการหายใจ และความดนโลหต
5) สามารถนงไดอยางนอย 30 นาท 6) สามารถเขาใจและปฏบตตามค าสงทละขนตอนได
เกณฑกำรคดออก
1) เปนโรคทางระบบประสาทอนๆรวมดวย 2) มอาการปวดจากโรคทางกระดกและกลามเนอทสงผลกระทบตอการฝกรยางคสวนบนและ
มอ 3) มอาการปวดไหลระดบรนแรง 4) เคลอนไหวในทาทางการงอขอไหล ไดนอยกวา 90 องศา 5) มการเกรงตวของกลามเนอแขนและมอระดบรนแรง 6) มปญหาดานการเขาใจและการรบร 7) มอาการเพกเฉยและละเลยตอรางกายดานตรงขาม 8) อยในระหวางการฟนฟหรอการรกษาทเกยวของกบการเคลอนไหวของรยางคสวนบนและมอ
4. กระบวนกำรวจย และกำรใหขอมลแกอำสำสมคร
ขนตอนด ำเนนกำรวจย (Experimental protocol)
กำรศกษำควำมนำเชอถอของกำรประเมนหลกทใชในงำนวจย
การศกษาขนตอนน ท าการเกบขอมลโดยผวจยจะท าการเกบขอมลโดยใชกลองวดโอถายภาพ
เคลอนไหวของการประเมนอาสาสมครทเขารวมในขนตอนการศกษานจ านวน ทงหมด 4 คน ซงม
คณสมบตตามเกณฑการคดเลอก จะไดรบการประเมนโดยแบบประเมน Wolf Motor Function
Test และแบบประเมน Fugl-Meyer assessment of the upper extremity
Ref. code: 25605812030533ARL

97
1. ผวจยอธบายวตถประสงค ขนตอนการวจย และประโยชนของการวจยครงนแก อาสาสมคร และขอความยนยอมจากอาสาสมครเปนลายลกษณอกษร
2. ผวจยแนะน าวธการประเมนแกอาสาสมคร
3. ประเมนกอนการคดเขา (screening test)
- ประเมนการรบรดวยแบบประเมน Mini Mental State Examination (MMSE)
- ประเมนการปวดขอไหลดวย Visual Analogue Scale (VAS) ถาผปวยมอาการปวดไหล
คดเลอกอาสาสมครตามทเกณฑทระบไวในเกณฑการคดเขาและคดออก
4. ประเมนความสามารถในการใชมอและแขนในการใชงานดวยประเมนแบบประเมน Wolf Motor Function Test 5. ประเมนความบกพรองในการเคลอนไหวรยางคสวนบนดวยแบบประเมน Fugl-Meyer assessment of the upper extremity (FMA-UE) หวขอ motor function
6. บนทกวดโอขณะท าการประเมน
7. วเคราะหผลและสรปผลคาความนาเชอถอในการวดซ าของผประเมนแตละคนและคาความนาเชอถอระหวางผประเมน
5. ในกำรคดกรองอำสำสมครวจย หำกพบวำผนนไมอยในเกณฑคดเขำ และอยในสภาวะท
สมควรไดรบความชวยเหลอ/แนะน า ผวจยจะใหความชวยเหลอและค าแนะน าตามทสามารถท าไดใน
สวนของงานกายภาพบ าบด
6.ควำมเสยงหรออนตรำยทจะเกดขน และ/หรอควำมไมสะดวกสบำยของอำสำสมครท
อำจไดรบ และมำตรกำรทผวจยเตรยมไวปองกน
อาสาสมครอาจมความเสยงตอการเกดอาการเกรงของกลามเนอและเกดความเหนอยลา ระหวางการทดสอบ ผวจยจะอธบายวธการทดสอบและการฝกเพอลดความเสยงหรออนตรายทอาจเกดขน ซงกอน ระหวาง และหลง การทดสอบแตละกจกรรมทานสามารถพกไดตามตองการ โดยผวจยจะมการประเมนอตราการเตนของหวใจและคาความเหนอย และมระยะเวลาพกใหแกอาสาสมคร หากอาสาสมครรสกวาการทดสอบและการฝกไมปลอดภยหรอยากเกนไปจนอาจเสยงตอการเกดอนตรายตอตวอาสาสมครสามารถหยดการทดสอบไดตลอดเวลา ผวจยจะอยกบอาสาสมครตลอดเวลาระหวางการทดสอบและการฝก
Ref. code: 25605812030533ARL
98
กำรดแลรกษำและแกปญหำอนกรณเกดผลแทรกซอนแกอำสำสมคร การทดสอบจะหยดทนทเมออาสาสมครประสงคจะหยดหรอไมสามารถท าตอได หากเกดผล
ขางเคยงทไมพงประสงคจากการวจยครงน เชน หากอาสาสมครมอาการลา จะไดรบระยะเวลาพก
เพมขนเทาทตองการ ถามอาการหนามด จะไดรบการปฐมพยาบาลเบองตน และหากเกดผลขางเคยง
อนๆ ทไมสามารถปฐมพยาบาลเบองตนได จะไดรบการน าตวสงสถานพยาบาลทใกลเคยงทสด โดย
คณะผวจยจะเปนผรบผดชอบคาใชจายในการรกษาอาการแทรกซอนทเปนผลจากการวจย
โดยจะมการระมดระวงถงความปลอดภยและรายงานอาการไมพงประสงค ผวจยจะท าการ
สงเกต อาการผดปกตตางๆ ทเกดขนระหวางใหการประเมนกบอาสาสมคร เชน อาการเหนอย โดยใชการสอบถามและแบบประเมนความเหนอย
7. ประโยชนในกำรเขำรวมวจย ประโยชนทคาดวาจะเกดขนจากการท าวจย
1.) เพอทราบความนาเชอถอในการวดซ าของผประเมนแตละคนและคาความนาเชอถอระหวางผประเมน
2.) เพอใหการประเมนกอนและหลงการรกษาในงานวจยหลกมความนาเชอถอ
8. การเขารวมในการวจยของอาสาสมครเปนโดยสมครใจ และสามารถปฏเสธทจะเขารวมหรอถอนตวจากการวจยไดทกขณะ โดยไมตองใหเหตผลใหทราบลวงหนา และการไมเขารวมการวจยหรอถอนตวออกจากโครงการวจยนจะไมมผลกระทบตอการบรการและการรกษาทสมควรจะไดรบแตประการใด 9. การศกษานไมมคาตอบแทนในการเขารวม โดยอาสาสมครจะไดรบคาเดนทาง เปนเงนจ านวน 500 บาท
10. “หากอาสาสมครไม ได รบการปฏบตตามขอมลด งกล าวสามารถรองเรยน ไดท :
คณะอนกรรมการจรยธรรมการวจยในคน มหาวทยาลยธรรมศาสตร ชดท 3 อาคารราชสดา ชน 1
ภายในศนยสงเสรมสขภาพ คณะพยาบาลศาสตร มหาวทยาลยธรรมศาสตร ศนยรงสต โทรศพท 02-
986-9213 ตอ 7373 โทรสาร 02-5165381
Ref. code: 25605812030533ARL

99
11. ขอมลทเกยวของกบทานจะเกบเปนควำมลบ หากมการเสนอผลการวจยจะเสนอเปน
ภาพรวม ขอมลใดทสามารถระบถงตวทานไดจะไมปรากฏในรายงาน ขอมลสวนตวของทานจะถกเกบ
รกษาไว ไมเปดเผยตอสาธารณะเปนรายบคคล แตจะรายงานผลการวจยเปนขอมลสวนรวม ขอมล
ของผเขารวมเปนรายบคคลอาจมคณะบคคลบางกลมเขามาตรวจสอบได เชน ผใหทนวจย สถาบน
หรอองคกรของรฐทมหนาทตรวจสอบ คณะกรรมการจรยธรรมฯ เปนตน
Ref. code: 25605812030533ARL

100
ขอมลส ำหรบผประเมน
(Assessor Information Sheet)
โครงการวจย ชอเรอง (ไทย) : ผลของการรกษาดวยแนวคดของโบบาธตอการทางานของแขนและมอ ในผปวยโรคหลอดเลอดสมองทมปญหาการท างานของรยางคสวนบนระดบปานกลางถงรนแรง ชอเรอง (ภาษาองกฤษ) : The effect of Bobath therapy on upper limb and hand function in stroke individuals with moderate to severe arm deficit
ชอผวจย นางสาวธนยชนก พมประสาท ต าแหนง นกศกษาปรญญาโท สถานทตดตอผวจย
(สถานศกษา) ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (สถานศกษา) 02-986-9213-9 โทรศพทมอถอ 082-3243681 E-mail [email protected]
อำจำรยทปรกษำวจยหลก อ.ดร. ผกามาศ พรยะประสาธน สถานทตดตอ
ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7256 โทรศพทมอถอ 081-6152622
E-mail [email protected]
อำจำรยทปรกษำวจยรอง ผชวยศาสตราจารย ดร.นพพล ประโมทยกล
ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร
โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7237 โทรศพทมอถอ 086-6448738
E-mail [email protected]
AF 04_07
Ref. code: 25605812030533ARL

101
กอนททานจะตดสนใจเขารวมการวจย ทานควรท าความเขาใจถงเหตผล และทราบวางานวจยนเกยวของกบอะไร กรณาใชเวลาในการอานขอมลตอไปนอยางละเอยดรอบคอบ และสอบถามขอมลเพมเตมหรอขอมลทไมชดเจนไดตลอดเวลา
2. เหตผลและควำมจ ำเปนทตองท ำกำรวจย โรคหลอดเลอดสมองน าไปสความพการ ผปวยโรคหลอดเลอดสมองระยะเรอรง (นานกวา 6
เดอน) ยงพบความผดปกตและบกพรองและจ ากดการท ากจกรรมตางๆ และผปวยโรคหลอดเลอด
สมองจ านวนมากทมปญหาการใชงานแขนและมอขางทออนแรง
โดยหลกการของการรกษาดวยแนวคดของโบบาธคอ เทคนคการใชมอของนกกายภาพบ าบด
ในการฝกเพอกระตนการท างานของกลามเนอโดย เนนการทรงตว การเคลอนไหวทเปนปกต และ
กระบวนการกระตนระบบประสาทสมผส โดยผานการใหแรงกดและดงผานขอตอตางๆ ของรยางค
สวนบนและมอ ซงมความเหมาะสมทสามารถน าไปใชในการฝกผปวยในชมชน ดวยเทคนคการรกษา
และการน าไปใชกบผปวยไดงาย ในการศกษากอนหนาทมการรกษาดวยแนวคดของโบบาธ แสดงให
เหนวามการเพมขนของการท างานของแขนและมอในผปวยโรคหลอดเลอดสมองระยะเรอรง แตยง
ขาดรายละเอยดทมความเฉพาะเจาะจงของการรกษา
การศกษาครงนเปนสวนหนงของงานวจยหลกทจะท าการศกษาผลของการรกษาทาง
กายภาพบ าบดทจ าเพาะเพอการฟนฟการใชงานแขนและมอขางทออนแรงของผปวยโรคหลอดเลอด
สมองระยะเรอรง
2.วตถประสงคของกำรวจย
1) เพอหาคาความนาเชอถอในการวดซ าของแบบประเมน Wolf Motor Function Test และ Fugl-Meyer assessment of the upper extremity โดยผประเมนแตละคน
2) เพอหาคาความนาเชอถอระหวางผประเมน ของแบบประเมน Wolf Motor Function Test และ Fugl-Meyer assessment of the upper extremity
Ref. code: 25605812030533ARL

102
3.รำยละเอยดของผประเมน 1) เปนนกกายภาพบ าบดทมประสบการณการรกษาผปวยโรคหลอดเลอดสมอง
2) ไดรบการฝกการประเมนดวยแบบประเมนทใชในงานวจย ไดแก แบบประเมน Wolf Motor
Function Test และแบบประเมน Fugl-Meyer Assessment of upper extremity (FMA-
UE)
4. กระบวนกำรวจย และกำรใหขอมลแกอำสำสมคร
ขนตอนด ำเนนกำรวจย (Experimental protocol)
การศกษาขนตอนน ท าการเกบขอมลโดยมผประเมนจ านวน 2 คน ประเมนความสามารถใน
การเคลอนไหว และการท างานของรยางคสวนบนและมอของผปวยโรคหลอดเลอดสมองจากวดโอ
ถายภาพเคลอนไหวของการประเมน อาสาสมครทเขารวมในขนตอนการศกษานจ านวน ทงหมด 4
คน ซงมคณสมบตตามเกณฑการคดเลอก ไดแกการประเมนดวยแบบประเมน Wolf Motor
Function Test และแบบประเมน Fugl-Meyer assessment of the upper extremity ดงน
1) ผวจยอธบายวตถประสงค ขนตอนการวจย และประโยชนของการวจยครงนแก ผประเมน และขอความยนยอมจากอาสาสมครเปนลายลกษณอกษร
2) ผวจยแนะน าวธการประเมนทใชในงานวจยแกผประเมน ผประเมนจะไดรบการฝกการป ร ะ เ ม น แบบ ปร ะ เ ม น Wolf Motor Function Test แ ล ะประ เ ม น Fugl-Meyer assessment of the upper extremity (FMA-UE) หวขอ motor function
3) ผประเมนท าการประเมนความสามารถในการใชมอและแขนในการใช งานของผปวยโรคหอลดเลอดสมอง 4 ราย ดวยประเมนแบบประเมน Wolf Motor Function Test ซงการศกษานจะประเมนความสามารถการท างานของแขนและมอ 15 หวขอ
4) ผประเมนท าการประเมนความบกพรองในการเคลอนไหวรยางคสวนบนของผปวยโรคหลอดเลอดสมอง 4 ราย ดวยแบบประเมน Fugl-Meyer assessment of the upper extremity (FMA-UE) หวขอ motor function
5) ผวจยท าการวเคราะหผลและสรปผลคาความนาเชอถอในการวดซ าของผประเมนแตละคนและคาความนาเชอถอระหวางผประเมน
Ref. code: 25605812030533ARL

103
6.ควำมเสยงหรออนตรำยทจะเกดขนและ/หรอควำมไมสะดวกสบำยของผประเมนทอำจ
ไดรบ และมำตรกำรทผวจยเตรยมไวปองกน
งานวจยนมความเสยงนอย แตอยางไรกตาม การจดจอกบการประเมนเปนระยะเวลาตดตอกน อาจะท าใหผประเมนเกดความเหนอยลา ดงนน ระหวางการทดสอบ การทดสอบแตละกจกรรม อาสาสมครสามารถพกไดตามตองการ
กำรดแลรกษำและแกปญหำอนกรณเกดผลแทรกซอนแกผประเมน การทดสอบจะหยดทนทเมออาสาสมครประสงคจะหยดหรอไมสามารถท าตอได หากเกดผล
ขางเคยงทไมพงประสงคจากการวจยครงน เชน หากอาสาสมครมอาการลา สามารถพกเพมขนเทาท
ตองการ
7. ประโยชนในกำรเขำรวมวจย ประโยชนทคาดวาจะเกดขนจากการท าวจย
1.) ไดทราบความนาเชอถอในการวดซ าของผประเมนแตละคนและคาความนาเชอถอระหวางผประเมน
2.) เพอใหการประเมนกอนและหลงการรกษาในงานวจยหลกมความนาเชอถอ
8. การเขารวมในการวจยของผประเมนเปนโดยสมครใจ และสามารถปฏเสธทจะเขารวมหรอถอนตวจากการวจยไดทกขณะ โดยตองใหเหตผลใหทราบลวงหนา 9. มคาตอบแทน ใหแกผประเมน รายละ 500 บาทในการเขารวมการศกษาครงน
10. “หากผ ประเมน ไม ได ร บการปฏบ ต ตามขอมลด งกล าวสามารถรอ ง เร ยน ไดท :
คณะอนกรรมการจรยธรรมการวจยในคน มหาวทยาลยธรรมศาสตร ชดท 3 อาคารราชสดา ชน 1
ภายในศนยสงเสรมสขภาพ คณะพยาบาลศาสตร มหาวทยาลยธรรมศาสตร ศนยรงสต โทรศพท 02-
986-9213 ตอ 7373 โทรสาร 02-5165381
11. ขอมลทเกยวของกบทานจะเกบเปนควำมลบ หากมการเสนอผลการวจยจะเสนอเปน
ภาพรวม ขอมลใดทสามารถระบถงตวทานไดจะไมปรากฏในรายงาน ขอมลสวนตวของทานจะถกเกบ
รกษาไว ไมเปดเผยตอสาธารณะเปนรายบคคล แตจะรายงานผลการวจยเปนขอมลสวนรวม ขอมล
ของผเขารวมเปนรายบคคลอาจมคณะบคคลบางกลมเขามาตรวจสอบได เชน ผใหทนวจย สถาบน
หรอองคกรของรฐทมหนาทตรวจสอบ คณะกรรมการจรยธรรมฯ เปนตน
Ref. code: 25605812030533ARL

104
ขอมลส ำหรบอำสำสมครวจย (Participant Information Sheet)
โครงการวจย ชอเรอง (ไทย) : ผลของการรกษาดวยแนวคดของโบบาธตอการทางานของแขนและมอ ในผปวยโรคหลอดเลอดสมองทมปญหาการท างานของรยางคสวนบนระดบปานกลางถงรนแรง ชอเรอง (ภาษาองกฤษ) : The effect of Bobath therapy on upper limb and hand function in stroke individuals with moderate to severe arm deficit
ชอผวจย นางสาวธนยชนก พมประสาท ต าแหนง นกศกษาปรญญาโท สถานทตดตอผวจย
(สถานศกษา) ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (สถานศกษา) 02-986-9213 โทรศพทมอถอ 082-3243681 E-mail [email protected]
อำจำรยทปรกษำวจยหลก อ.ดร. ผกามาศ พรยะประสาธน สถานทตดตอ
ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7256 โทรศพทมอถอ 081-6152622
E-mail [email protected]
อำจำรยทปรกษำวจยรอง ผชวยศาสตราจารย ดร.นพพล ประโมทยกล
ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร
โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7237 โทรศพทมอถอ 086-6448738
E-mail [email protected]
กอนททานจะตดสนใจเขารวมการวจย ทานควรท าความเขาใจถงเหตผล และทราบวางานวจยนเกยวของกบอะไร กรณาใชเวลาในการอานขอมลตอไปนอยางละเอยดรอบคอบ และสอบถามขอมลเพมเตมหรอขอมลทไมชดเจนไดตลอดเวลา
AF 04_07
Ref. code: 25605812030533ARL

105
1. เหตผลและควำมจ ำเปนทตองท ำกำรวจย โรคหลอดเลอดสมองน าไปสความพการ ผปวยโรคหลอดเลอดสมองระยะเรอรง (นานกวา 6
เดอน) ยงพบความผดปกตและบกพรองและจ ากดการท ากจกรรมตางๆ และผปวยโรคหลอดเลอด
สมองจ านวนมากทมปญหาการใชงานแขนและมอขางทออนแรง
โดยหลกการของการรกษาดวยแนวคดของโบบาธคอ เทคนคการใชมอของนกกายภาพบ าบด
ในการฝกเพอกระตนการท างานของกลามเนอโดย เนนการทรงตว การเคลอนไหวทเปนปกต และ
กระบวนการกระตนระบบประสาทสมผส โดยผานการใหแรงกดและดงผานขอตอตางๆ ของรยางค
สวนบนและมอ ซงมความเหมาะสมทสามารถน าไปใชในการฝกผปวยในชมชน ดวยเทคนคการรกษา
และการน าไปใชกบผปวยไดงาย ในการศกษากอนหนาทมการรกษาดวยแนวคดของโบบาธ แสดงให
เหนวามการเพมขนของการท างานของแขนและมอในผปวยโรคหลอดเลอดสมองระยะเรอรง แตยง
ขาดรายละเอยดทมความเฉพาะเจาะจงของการรกษา
2. วตถประสงคของกำรวจย
วตถประสงค เพอเปรยบเทยบประสทธผลการรกษาดวยแนวคดของโบบาธตอการท างาน
ความบกพรองของแขนและมอ ความเกรงตวของกลามเนอ และการรบรความรสกในผปวย
โรคหลอดเลอดสมองระยะเรอรงทมปญหาการท างานของรยางคสวนบนและมอระดบปาน
กลางถงรนแรงกอนและหลงการรกษา
3. รำยละเอยดของอำสำสมคร ผปวยโรคหลอดเลอดสมองไทย ระยะเรอรงในจงหวดปทมธาน
เกณฑกำรคดเขำ
1) เปนโรคหลอดเลอดสมองครงแรก และมระยะเวลาทเปนโรคหลอดเลอดสมองตงแต 6
เดอน
2) มอายตงแต 45 ปขนไป
3) มความบกพรองการท างานของรยางคสวนบนและมอระดบปานกลางถงรนแรง โดยการ
ประเมนดวยแบบประเมนความบกพรองในการเคลอนไหวรยางคสวนบน (Fugl-Meyer
Upper Extremity Motor Assessment)
4) มสญญาณชพคงท (ไดแก อตราการเตนของหวใจ อตราการหายใจ และความดนโลหต)
5) สามารถนงไดอยางนอย 30 นาท
Ref. code: 25605812030533ARL

106
6) สามารถเขาใจและปฏบตตามค าสงทละขนตอนได
เกณฑกำรคดออก
1) เปนโรคทางระบบประสาทอนๆ รวมดวย 2) มอาการปวดจากโรคทางกระดกและกลามเนอทสงผลกระทบตอการฝกรยางคสวนบนและ
มอ 3) มอาการปวดไหลระดบรนแรง 4) เคลอนไหวในทาทางการงอขอไหล ไดนอยกวา 90 องศา 5) มการเกรงตวของกลามเนอแขนและมอระดบรนแรง 6) มปญหาดานการเขาใจและการรบร 7) มอาการเพกเฉยและละเลยตอรางกายดานตรงขาม 8) อยในระหวางการฟนฟหรอการรกษาทเกยวของกบการเคลอนไหวของรยางคสวนบนและมอ
4. กระบวนการวจย และการใหขอมลแกอาสาสมคร
ขนตอนการเตรยมการ; ผวจยจะอธบายวตถประสงค ขนตอนการวจย และประโยชนของการวจยครงนแกอาสาสมคร และขอความยนยอมจากอาสาสมครเปนลายลกษณอกษร โดยจะมผเขารวมเปนอาสาสมครทงหมด 30 คน
Ref. code: 25605812030533ARL

107
ขนตอนกำรเกบขอมล
พจารณาเลอกผเขารวมวจยตามเกณฑทก าหนด
อาสาสมครทจะเขารวมลงนามแสดงความยนยอมในการเขารวม
การวจย
ผวจยอธบายถงวตถประสงค ขนตอนการวจย และประโยชนของการวจยแก
อาสาสมคร
การประเมนความสามารถการเคลอนไหวของแขนและมอ โดยใชการตรวจการเคลอนไหว และประเมนความตงตวของกลามเนอ ประกอบดวย
- Wolf Motor Function Test
- Fugl Meyer Assessment - UE
- Modified Ashworth Scale
- Revised Nottingham Sensory Assessment
การรกษาดวยแนวคดของโบบาธ 3 วน / สปดาห ทงหมด 6 สปดาห
ประเมนหลงการรกษาในวนถดไปหลงจาก ใหการรกษาครงสดทาย
วนถดมา 1 วน
วนถดมา 1 วน
Ref. code: 25605812030533ARL

108
5. ในกำรคดกรองอำสำสมครวจย หำกพบวำผนนไมอยในเกณฑคดเขำ และอยในสภาวะ
ทสมควรไดรบความชวยเหลอ/แนะน า ผวจยจะใหความชวยเหลอและค าแนะน าตามทสามารถท าได
ในสวนของงานกายภาพบ าบด
6.ควำมเสยงหรออนตรำยทจะเกดขน และ/หรอควำมไมสะดวกสบำยของอำสำสมครท
อำจไดรบ และมำตรกำรทผวจยเตรยมไวปองกน
อาสาสมครอาจมความเสยงตอการเกดอาการเกรงของกลามเนอและเกดความเหนอยลา ระหวางการทดสอบหรอการฝก ผวจยจะอธบายวธการทดสอบและการฝกเพอลดความเสยงหรออนตรายทอาจเกดขน ซงกอน ระหวาง และหลง การทดสอบหรอการฝกแตละกจกรรมทานสามารถพกไดตามตองการ โดยผวจยจะมการประเมนอตราการเตนของหวใจและคาความเหนอย และมระยะเวลาพกใหแกอาสาสมคร หากอาสาสมครรสกวาการทดสอบและการฝกไมปลอดภยหรอยากเกนไปจนอาจเสยงตอการเกดอนตรายตอตวอาสาสมครสามารถหยดการทดสอบและการฝกไดตลอดเวลา ผวจยจะท าการสงเกต อาการผดปกตตางๆ ทเกดขนระหวางใหการประเมนหรอรกษากบอาสาสมคร เชน อาการเหนอย โดยใชการสอบถามและแบบประเมนความเหนอย
กำรดแลรกษำและแกปญหำอนกรณเกดผลแทรกซอนแกอำสำสมคร การทดสอบจะหยดทนทเมออาสาสมครประสงคจะหยดหรอไมสามารถท าตอได หากเกดผล
ขางเคยงทไมพงประสงคจากการวจยครงน เชน หากอาสาสมครมอาการลา จะไดรบระยะเวลาพก
เพมขนเทาทตองการ ถามอาการหนามด จะไดรบการปฐมพยาบาลเบองตน และหากเกดผลขางเคยง
อนๆ ทไมสามารถปฐมพยาบาลเบองตนได จะไดรบการน าตวสงสถานพยาบาลทใกลเคยงทสด โดย
คณะผวจยจะเปนผรบผดชอบคาใชจายในการรกษาอาการแทรกซอนทเปนผลจากการวจย
7. ประโยชนในกำรเขำรวมวจย ประโยชนทคาดวาจะเกดขนจากการท าวจย
1.) เพอทราบประสทธผลของการรกษาดวยแนวคดของโบบาธในผปวยทมปญหาการท างานของแขนและมอในผปวยโรคหลอดเลอดสมองระดบปานกลางถงรนแรง
2.) เพอเปนแนวทางในการประยกตใชการรกษาทางกายภาพบ าบดในผปวยทมปญหาการท างานของแขนและมอในผปวยโรคหลอดเลอดสมองระดบปานกลางถงรนแรง ซงจะเปนประโยชนในการใหการวางแผนรกษาผปวยโรคหลอดเลอดสมองในชมชน
Ref. code: 25605812030533ARL

109
นอกจากนอาสาสมครจะไดรบความร ขอแนะน าทางกายภาพบ าบดในการฝกการเคลอนไหว เขาใจในอาการและความบกพรองตางๆ มากขน ส าหรบน าไปปรบใชในการด าเนนชวตประจ าวน เพอสงเสรมการเคลอนไหวทดขน
8. การเขารวมในการวจยของอาสาสมครเปนโดยสมครใจ และสามารถปฏเสธทจะเขารวมหรอถอนตวจากการวจยไดทกขณะ โดยไมตองใหเหตผลใหทราบลวงหนา และการไมเขารวมการวจยหรอถอนตวออกจากโครงการวจยนจะไมมผลกระทบตอการบรการและการรกษาทสมควรจะไดรบแตประการใด 9. คาตอบแทน “การศกษานไมมคาตอบแทนในการเขารวม”
10. “หากอาสาสมคร ไม ได ร บการปฏบต ตามขอมลด งกล าวสามารถรอง เร ยนไดท :
คณะอนกรรมการจรยธรรมการวจยในคน มหาวทยาลยธรรมศาสตร ชดท 3 อาคารราชสดา ชน 1
ภายในศนยสงเสรมสขภาพ คณะพยาบาลศาสตร มหาวทยาลยธรรมศาสตร ศนยรงสต โทรศพท 02-
986-9213 ตอ 7373 โทรสาร 02-5165381
11. ขอมลทเกยวของกบทานจะเกบเปนควำมลบ หากมการเสนอผลการวจยจะเสนอเปน
ภาพรวม ขอมลใดทสามารถระบถงตวทานไดจะไมปรากฏในรายงาน ขอมลสวนตวของทานจะถกเกบ
รกษาไว ไมเปดเผยตอสาธารณะเปนรายบคคล แตจะรายงานผลการวจยเปนขอมลสวนรวม ขอมล
ของผเขารวมเปนรายบคคลอาจมคณะบคคลบางกลมเขามาตรวจสอบได เชน ผใหทนวจย สถาบน
หรอองคกรของรฐทมหนาทตรวจสอบ คณะกรรมการจรยธรรมฯ เปนตน
Ref. code: 25605812030533ARL

110
APPENDIX C
Informed Consent Form
หนงสอแสดงควำมยนยอมเขำรวมกำรวจยของอำสำสมครวจย (Informed Consent Form)
ตอนท 1
ท าท..................................................................... วนท.............เดอน.......................พ.ศ. ..............
เลขท อาสาสมครวจย…...................……
ขาพเจา ซงไดลงนามทายหนงสอน ขอแสดงความยนยอมเขารวมโครงการวจย ชอโครงการวจย ผลของการรกษาดวยแนวคดของโบบาธ ตอการท างานของแขนและมอ ในผปวยโรคหลอดเลอดสมองทมปญหาการท างานของรยางคสวนบนระดบปานกลางถงรนแรง (The effect of Bobath therapy on upper limb and hand function in stroke individuals with moderate to severe arm deficit)
ตอนท 1 การทดสอบความนาเชอถอของผประเมนในการใชแบบประเมน Wolf Motor
Function Test และ Fugl-Meyer assessment of the upper extremity
ชอผวจย นางสาวธนยชนก พมประสาท ทอยทตดตอ ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213 โทรศพทมอถอ 082-324-3681 อำจำรยทปรกษำ อำจำรยทปรกษำวจยหลก อ.ดร. ผกามาศ พรยะประสาธน ทอยทตดตอ ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-926-9213-9 ตอ 7256 โทรศพทมอถอ 081-6152622 อำจำรยทปรกษำวจยรอง ผชวยศาสตราจารย ดร.นพพล ประโมทยกล ทอยทตดตอ (ทท างาน) ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7237 โทรศพทมอถอ 086-6448738
AF 05_07
Ref. code: 25605812030533ARL

111
ขาพเจาไดรบทรำบรายละเอยดเกยวกบทมาและวตถประสงคในการท าวจย รายละเอยดขนตอนตางๆ ทจะตองปฏบตหรอไดรบการปฏบต ความเสยง/อนตราย และประโยชนซงจะเกดขนจากการวจยเรองน โดยไดอานรายละเอยดในเอกสารชแจงอาสาสมครวจยโดยตลอด และไดรบค ำอธบำยจากผวจยจนเขำใจเปนอยำงดแลว
ขาพเจาจงสมครใจเขารวมในโครงการวจยน ตามทระบไวในเอกสารชแจงอาสาสมครวจยโดยขาพเจายนยอมสละเวลาตอบแบบสอบถามขอมลทวไป รบการประเมนการท างานและกจกรรมตางๆดวยแบบประเมน Wolf Motor Function Test และรบการประเมนความบกพรองในการเคลอนไหวโดยแบบประเมน Fugl-Meyer assessment of the upper extremity (FMA-UE) เมอเสรจสนการวจยแลว ขอมลทเกยวของกบอาสาสมครวจยจะถกท าลาย
ขาพเจามสทธถอนตวออกจากการวจยเมอใดกไดตามความประสงค โดยไมตองแจงเหตผล ซงการถอนตวออกจากการวจยนน จะไมมผลกระทบตอการบรการและการรกษาทสมควรจะไดรบแตประการใด
ขาพเจาไดรบค ารบรองวา ผวจยจะปฏบตตอขาพเจาตามขอมลทระบไวในเอกสารชแจงอาสาสมครวจยและขอมลใดๆ ทเกยวของกบขาพเจา ผวจยจะเกบรกษำเปนควำมลบ โดยจะน าเสนอขอมลการวจยเปนภาพรวมเทานน ไมมขอมลใดในการรายงานทจะน าไปสการระบตวขาพเจา
หำกขำพเจำไมไดรบกำรปฏบตตรงตำมทไดระบไวในเอกสำรชแจงอำสำสมครวจย ขาพเจาสามารถรองเรยนไดท: คณะอนกรรมการจรยธรรมการวจยในคน มหาวทยาลยธรรมศาสตร ชดท 3 อาคารราชสดา ชน 1 ศนยสงเสรมสขภาพ คณะพยาบาลศาสตร มหาวทยาลยธรรมศาสตร ศนยรงสต โทรศพท 02-986-9213 ตอ 7373 โทรสาร 02-5165381
ขาพเจาไดลงลายมอชอไวเปนส าคญตอหนาพยาน ทงนขาพเจาไดรบส าเนาเอกสารขอมลส าหรบ อาสาสมครวจย และส าเนาหนงสอแสดงความยนยอมเขารวมการวจยของอาสาสมครวจยไวแลว
ลงชอ............................................................... (..................................................................)
ผวจยหลก วนท……..…/……….……./…………
ลงชอ................................................................ (.......................................................................)
อาสาสมครวจย วนท……..…/……….……./…………
ลงชอ................................................................ (.................................................................... ...)
พยาน วนท……..…/……….……./…………
ลงชอ....................................................... ......... (.......................................................................)
พยาน วนท……..…/……….……./…………
Ref. code: 25605812030533ARL

112
หนงสอแสดงควำมยนยอมเขำรวมกำรวจยของผประเมน (Informed Consent Form)
ท าท..................................................................... วนท.............เดอน.......................พ.ศ. ..............
เลขท อาสาสมครวจย…...................……
ขาพเจา ซงไดลงนามทายหนงสอน ขอแสดงความยนยอมเขารวมโครงการวจย ชอโครงการวจย ผลของการรกษาดวยแนวคดของโบบาธ ตอการท างานของแขนและมอ ในผปวยโรคหลอดเลอดสมองทมปญหาการท างานของรยางคสวนบนระดบปานกลางถงรนแรง (The effect of Bobath therapy on upper limb and hand function in stroke individuals with moderate to severe arm deficit)
ตอนท 1 การทดสอบความนาเชอถอของผประเมนในการใชแบบประเมน Wolf Motor
Function Test และ Fugl-Meyer assessment of the upper extremity
ชอผวจย นางสาวธนยชนก พมประสาท ทอยทตดตอ ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213 โทรศพทมอถอ 082-324-3681 อำจำรยทปรกษำ อำจำรยทปรกษำวจยหลก อ.ดร. ผกามาศ พรยะประสาธน ทอยทตดตอ ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7256 โทรศพทมอถอ 081-6152622 อำจำรยทปรกษำวจยรอง ผชวยศาสตราจารย ดร.นพพล ประโมทยกล ทอยทตดตอ (ทท างาน) ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7237 โทรศพทมอถอ 086-6448738
AF 05_07
Ref. code: 25605812030533ARL

113
ขาพเจาไดรบทรำบรายละเอยดเกยวกบทมาและวตถประสงคในการท าวจย รายละเอยดขนตอนตางๆ ทจะตองปฏบตหรอไดรบการปฏบต ความเสยง/อนตราย และประโยชนซงจะเกดขนจากการวจยเรองน โดยไดอานรายละเอยดในเอกสารชแจงอาสาสมครวจยโดยตลอด และ ไดรบค ำอธบำยจากผวจยจนเขำใจเปนอยำงดแลว
ขาพเจาจงสมครใจเขารวมในโครงการวจยน ตามทระบไวในเอกสารชแจงผประเมนโดยขาพเจายนยอมสละเวลาเกบขอมลอาสาสมครผปวยโรคหลอดเลอดสมอง โดย ประเมนการท างานและกจกรรมตางๆดวยแบบประเมน Wolf Motor Function Test และประเมนความบกพรองในการเคลอนไหวโดยแบบประเมน Fugl-Meyer assessment of the upper extremity (FMA-UE) เมอเสรจสนการวจยแลว ขอมลทเกยวของกบผประเมนจะถกท าลาย
ขาพเจามสทธถอนตวออกจากการวจยเมอใดกไดตามความประสงค โดยตองแจงเหตผลใหทรำบลวงหนำ
ขาพเจาไดรบค ารบรองวา ผวจยจะปฏบตตอขาพเจาตามขอมลทระบไวในเอกสารชแจงผประเมนและขอมลใดๆ ทเกยวของกบขาพเจา ผวจยจะเกบรกษำเปนควำมลบ โดยจะน าเสนอขอมลการวจยเปนภาพรวมเทานน ไมมขอมลใดในการรายงานทจะน าไปสการระบตวขาพเจา
หำกขำพเจำไมไดรบกำรปฏบตตรงตำมทไดระบไวในเอกสำรชแจงผประเมน ขาพเจาสามารถรองเรยนไดท: คณะอนกรรมการจรยธรรมการวจยในคน มหาวทยาลยธรรมศาสตร ชดท 3 อาคารราชสดา ชน 1 ศนยสงเสรมสขภาพ คณะพยาบาลศาสตร มหาวทยาลยธรรมศาสตร ศนยรงสต โทรศพท 02-986-9213 ตอ 7373 โทรสาร 02-5165381
ขาพเจาไดลงลายมอชอไวเปนส าคญตอหนาพยาน ทงนขาพเจาไดรบส าเนาเอกสารขอมลส าหรบ อาสาสมครวจย และส าเนาหนงสอแสดงความยนยอมเขารวมการวจยของอาสาสมครวจยไวแลว
ลงชอ............................................................... (..................................................................)
ผวจยหลก วนท……..…/……….……./…………
ลงชอ................................................................ (.......................................................................)
อาสาสมครวจย วนท……..…/……….……./…………
ลงชอ................................................................ (.......................................................................)
พยาน วนท……..…/……….……./…………
ลงชอ................................................................ (.......................................................................)
พยาน วนท……..…/……….……./…………
Ref. code: 25605812030533ARL

114
หนงสอแสดงควำมยนยอมเขำรวมกำรวจยของอำสำสมครวจย (Informed Consent Form)
ท าท..................................................................... วนท.............เดอน.......................พ.ศ. ..............
เลขท อาสาสมครวจย…...................……
ขาพเจา ซงไดลงนามทายหนงสอน ขอแสดงความยนยอมเขารวมโครงการวจย ชอโครงการวจย ผลของการรกษาดวยแนวคดของโบบาธ ตอการท างานของแขนและมอ ในผปวยโรคหลอดเลอดสมองทมปญหาการท างานของรยางคสวนบนระดบปานกลางถงรนแรง (The effect of Bobath therapy on upper limb and hand function in stroke individuals with moderate to severe arm deficit) ชอผวจย นางสาวธนยชนก พมประสาท ทอยทตดตอ ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213 โทรศพทมอถอ 082-324-3681 อำจำรยทปรกษำ อำจำรยทปรกษำวจยหลก อ.ดร. ผกามาศ พรยะประสาธน ทอยทตดตอ ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7256 โทรศพทมอถอ 081-6152622 อำจำรยทปรกษำวจยรอง ผชวยศาสตราจารย ดร.นพพล ประโมทยกล ทอยทตดตอ (ทท างาน) ภาควชากายภาพบ าบด คณะสหเวชศาสตร มหาวทยาลยธรรมศาสตร โทรศพท (ทท างาน) 02-986-9213-9 ตอ 7237 โทรศพทมอถอ 086-6448738
ขาพเจาไดรบทรำบรายละเอยดเกยวกบทมาและวตถประสงคในการท าวจย รายละเอยดขนตอนตางๆ ทจะตองปฏบตหรอไดรบการปฏบต ความเสยง/อนตราย และประโยชนซงจะเกดขนจากการวจยเรองน โดยไดอานรายละเอยดในเอกสารชแจงอาสาสมครวจยโดยตลอด และ ไดรบค ำอธบำยจากผวจยจนเขำใจเปนอยำงดแลว
AF 05_07
Ref. code: 25605812030533ARL

115
ขาพเจาจงสมครใจเขารวมในโครงการวจยน ตามทระบไวในเอกสารชแจงอาสาสมครวจยโดยขาพเจายนยอมสละเวลาตอบแบบสอบถามขอมลทวไป ประเมนการท างานและกจกรรมตางๆ ดวยแบบประเมน Wolf Motor Function Test ประเมนสมรรถภาพทางกายและความบกพรองในการเคลอนไหวโดยแบบประเมนFugl-Meyer assessment of the upper extremity (FMA-UE) ประเมนการเกรงตวของกลามเนอ Modified Ashworth Scale และประเมนดานการรบรความรสก Revised Nottingham Sensory Assessment เมอเสรจสนการวจยแลว ขอมลท เกยวของกบอาสาสมครวจยจะถกท าลาย
และไดรบการรกษาตามโปรแกรม ครงละประมาณ 60 นาท 3 วนตอสปดาห เปนระยะเวลา 6 สปดาห
ขาพเจามสทธถอนตวออกจากการวจยเมอใดกไดตามความประสงค โดยไมตองแจงเหตผล ซงการถอนตวออกจากการวจยนน จะไมมผลกระทบตอการบรการและการรกษาทสมควรจะไดรบแตประการใด
ขาพเจาไดรบค ารบรองวา ผวจยจะปฏบตตอขาพเจาตามขอมลทระบไวในเอกสารชแจงอาสาสมครวจยและขอมลใดๆ ทเกยวของกบขาพเจา ผวจยจะ เกบรกษำเปนควำมลบ โดยจะน าเสนอขอมลการวจยเปนภาพรวมเทานน ไมมขอมลใดในการรายงานทจะน าไปสการระบตวขาพเจา
หำกขำพเจำไมไดรบกำรปฏบตตรงตำมทไดระบไวในเอกสำรชแจงอำสำสมครวจย ขาพเจาสามารถรองเรยนไดท: คณะอนกรรมการจรยธรรมการวจยในคน มหาวทยาลยธรรมศาสตร ชดท 3 อาคารราชสดา ชน 1 ศนยสงเสรมสขภาพ คณะพยาบาลศาสตร มหาวทยาลยธรรมศาสตร ศนยรงสต โทรศพท 02-986-9213 ตอ 7373 โทรสาร 02-5165381
ขาพเจาไดลงลายมอชอไวเปนส าคญตอหนาพยาน ทงนขาพเจาไดรบส าเนาเอกสารขอมลส าหรบ อาสาสมครวจย และส าเนาหนงสอแสดงความยนยอมเขารวมการวจยของอาสาสมครวจยไวแลว
ลงชอ............................................................... (..................................................................)
ผวจยหลก วนท……..…/……….……./…………
ลงชอ................................................................ (.......................................................................)
อาสาสมครวจย วนท……..…/……….……./…………
ลงชอ................................................................
(.......................................................................) พยาน
วนท……..…/……….……./…………
ลงชอ................................................................ (.......................................................................)
พยาน วนท……..…/……….……./…………
Ref. code: 25605812030533ARL

116
APPENDIX D
General data form
รหสผเขารวมวจย..........................................
1. อาย.......................... ป 2. เพศ ชาย หญง
3. สถานะภาพสมรส
โสด สมรส หมาย/หยา/แยกกนอย
4. ระยะเวลาทเปนโรคหลอดเลอดสมอง .....................ป .....................เดอน
5. ดานทมอาการออนแรง........................... ดานทถนด..............................
6. น าหนก.......................กโลกรม สวนสง.........................เซนตเมตร
7. โรคประจ าตว โรคเบาหวาน โรคความดนโลหตสง
โรคหวใจ
โรคอนๆ (ระบ) ................................................
8. สบบหรและดมสราหรอไม (ถาเคยใหระบความถ) สบบหร ไมสบ เคยสบแตปจจบนไมไดสบแลว ระบความถ............................. ดมสรา ไมดม เคยดมแตปจจบนไมไดดมแลว ระบความถ.............................. 9. ระดบการศกษา ต ากวาหรอเทยบเทามธยมศกษา อนปรญญา ต ากวาประถมศกษา
ปรญญาตรหรอสงกวา ประถมศกษา อนๆ 10. อาชพหรอลกษณะงานทท าอยในปจจบน (ระบลกษณะงาน)............................................. 11. ทานเคยไดรบการรกษาทางกายภาพบ าบดหลงจากการเกดโรคหลอดเลอดสมองหรอไม ไมเคย เคย
ระบการรกษา...................................
v
v
Ref. code: 25605812030533ARL

117
APPENDIX E
Thai version - The Mini–Mental State Examination
(MMSE-Thai 2002)(162)
Orientation for time (5 คะแนน) คะแนน วนนวนทเทาไร วนนวนอะไร เดอนนเดอนอะไร ปนปอะไร ฤดนฤดอะไร Orientation for place (5 คะแนน) # กรณอยสถานพยาบาล สถานทตรงนเรยกวาอะไร และ.........ชอวาอะไร ขณะนอยชนทเทาไรของของตวอาคาร ทนอยในอ าเภออะไร ทนจงหวดอะไร ทนภาคอะไร Orientation for place (ตอ) # กรณอยทบานของผถกทดสอบ สถานทตรงนเรยกวาอะไร และบานเลขทเทาไร ทนหมบาน หรอละแวก/คม/ยาน/ถนนอะไร ทนอยในอ าเภอ/เขตอะไร ทนจงหวดอะไร ทนภาคอะไร Registration (3 คะแนน) (ตอบถก 1 ค าได 1 คะแนน) บอกชอของ 3 อยางแลวใหผถกทดสอบพดตาม
ดอกไม แมน า รถไฟ ในกรณทท าแบบทดสอบซ าภายใน 2 เดอน ใหใชค าวา
ตนไม ทะเล รถยนต
Ref. code: 25605812030533ARL

118
Attention/ Calculation (5 คะแนน) (ใหเลอกขอใดขอหนง) คดเลขในใจใหเอา 100 ตง ลบออกทละ 7 ไปเรอยๆ ไดผลลพธเทาไร ……. ……. …….. ……. ……. Attention/ Calculation (ตอ) สะกดค าวามะนาวใหฟง แลวใหผถกทดสอบสะกดถอยหลงจากพยญชนะตวหลงไปตวแรก “มอมา-สระอะ-นอหน-สระอา-วอแหวน” ……. ……. …….. ……. ……. ว า น ะ ม Recall (3คะแนน)” (ตอบถก 1 ค าได 1 คะแนน) เมอสกครทใหจ าของ 3 อยาง จ าไดไหมมอะไรบาง ดอกไม แมน า รถไฟ ในกรณทท าแบบทดสอบซ าภายใน 2 เดอน ใหใชค าวา ตนไม ทะเล รถยนต Naming ( 2 คะแนน) ยนดนสอใหผถกทดสอบดและถามวา “ของสงนเรยกวาอะไร” ชนาฬกาขอมอใหผถกทดสอบดและถามวา “ของสงนเรยกวาอะไร” Repetition (1 คะแนน) พดขอความแลวใหพดตาม โดยบอกเพยงครงเดยว “ใครใครขายไกไข”
Ref. code: 25605812030533ARL

119
Verbal command (3คะแนน) # บอกผถกทดสอบวาจะสงกระดาษให แลวใหรบดวยมอขวา พบครงดวยมอ 2 ขาง แลววางไวท....................... (พน, โตะ, เตยง) # สงกระดาษเปลาขนาดประมาณ เอ-4 ไมมรอยพบ ใหผถกทดสอบ �รบดวยมอขวา �พบครง �วางไวท (พน, โตะ, เตยง) Written command (1 คะแนน) # ใหผถกทดสอบอานขอความทก าหนด แลวใหท าตาม จะอานออกเสยงหรออานในใจกได # ผทดสอบแสดงกระดาษทเขยนวา “หลบตา” หลบตาได Writing (1 คะแนน) ใหผถกทดสอบเขยนขอความอะไรกไดทอานแลวรเรอง หรอมความหมายมา 1 ประโยค …………………….……………… ประโยคมความหมาย
Ref. code: 25605812030533ARL

120
Vasoconstriction (1 คะแนน) ขอนเปนค าสง “ใหวาดภาพเหมอนภาพตวอยาง”
รวมคะแนน คะแนนเตม 30 จดตดส าหรบคะแนนทสงสยภาวะสมองเสอม ระดบการศกษา จดตด คะแนนเตม # ไมไดเรยนหนงสอ (อานไมออก-เขยนไมได) < 14 23 (ไมตองท าขอ 4, 9, 10) # เรยนระดบประถมศกษา < 17 30 # เรยนระดบสงกวาประถมศกษา < 22 30
Ref. code: 25605812030533ARL
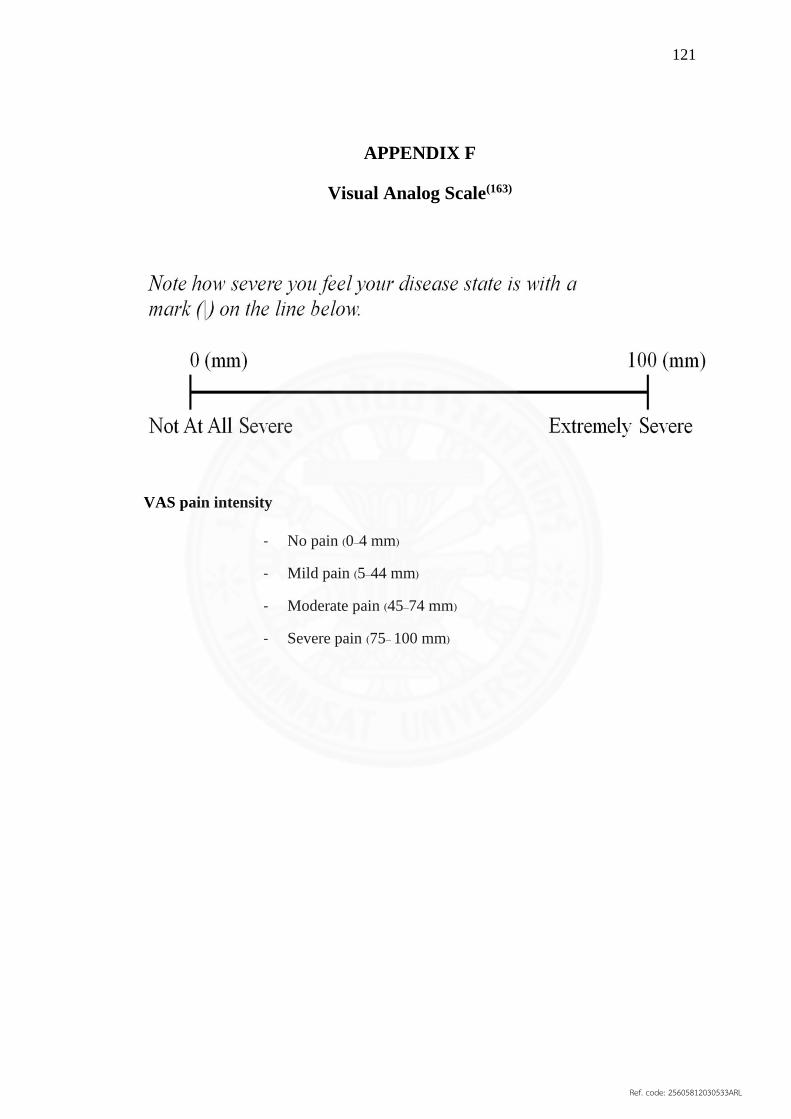
121
APPENDIX F
Visual Analog Scale(163)
VAS pain intensity
- No pain (0–4 mm)
- Mild pain (5–44 mm)
- Moderate pain (45–74 mm)
- Severe pain (75– 100 mm)
Ref. code: 25605812030533ARL

122
APPENDIX G
Wolf Motor Function test (164)
Participant’s study ID :
Evaluation date :
Evaluator’s initials : …………/…………..
Arm’s test More-affected R/L Less-affected R/L
Task Time Functional ability Time
Comment
1. Forearm to table (side) ……………………… 0 1 2 3 4 5 ………………………
2. Forearm to box (side) ……………………… 0 1 2 3 4 5 ………………………
3. Extend elbow (side) ……………………… 0 1 2 3 4 5 ………………………
4. Extend elbow (weight) ……………………… 0 1 2 3 4 5 ………………………
5. Hand to table (front) ………………………. 0 1 2 3 4 5 ………………………
6. Hand to box (front) ………………………. 0 1 2 3 4 5 ………………………
7. Weight to box ………….……………lbs. ………………………lbs.
8. Reach and retrieve ………………………. 0 1 2 3 4 5 .………………………
9. Lift can ………………………. 0 1 2 3 4 5 ………………………
10. Lift pencil ………………………. 0 1 2 3 4 5 .……………………..
11. Lift paper clip ………………………. 0 1 2 3 4 5 ………………………
12. Stack checkers ………………………. 0 1 2 3 4 5 ..……………………..
13. Flip cards ………………………. 0 1 2 3 4 5 ………………………
14. Grip strength ……………………….kgs. . .……………………kgs.
15. Turn key in lock ………………………. 0 1 2 3 4 5 .……………………..
16. Fold towel ………………………. 0 1 2 3 4 5 ……………………….
17. Lift basket ………………………. 0 1 2 3 4 5 ……………………….
รหสผเขารวมวจย......................................................................
First /Last
Ref. code: 25605812030533ARL

123
0 - Dose not attempt with upper extremity being tested
1 - UE being tested dose not participate functionally; however, attempt is made to
use the upper limb. In unilateral tasks the upper limb not being tested may be used to
move the upper limb being tested.
2 - Dose, but requires assistance of the UE not being tested for minor
readjustments or change of position, or requires more than two attempts to complete,
or accomplishes very slowly. In bilateral tasks the UE being tested may serve only as a
helper
3 - Dose, but movement is influenced to some degree by synergy or is performed
slowly or with effort.
4 - Dose; movement is close to normal*, but slightly slower; may lack precision,
fine coordination or fluidity
5 - Dose; movement appears to be normal*
(*) For the determination of normal, the less-involved UE can be utilized as an available
index for comparison, with pre-morbid UE dominance taken into consideration.
Ref. code: 25605812030533ARL

124
APPENDIX H
Fugl- Meyer Assessment: Upper Extremity (FMA-UE) (165)
A.UPPER EXTREMITY, sitting position
I. Reflex activity none can be elicited
Flexors: Biceps and finger flexors
Extensors: triceps
0 2
0 2
Subtotal I (max 4)
II. Volitional movement within synergies, without gravitational
help
none partial full
Flexor synergy: Hand
from contralateral knee to
ipsilateral ear. From
extensor synergy (shoulder
adduction/ internal
rotation, elbow extension,
forearm pronation) to
flexor synergy (shoulder
abduction/ external
rotation, elbow flexion,
forearm supination). Extensor synergy: Hand
from ipsilateral ear to the
contralateral knee
Shoulder retraction
elevation
abduction (90°)
external rotation
Elbow flexion
Forearm supination
0
0
0
0
0
0
1
1
1
1
1
1
2
2
2
2
2
2
Shoulder adduction/internal rotation
Elbow extension
Forearm pronation
0
0
0
1
1
1
2
2
2
Subtotal II (max 18)
III. Volitional movement mixing synergies, without compensation none partial full
Hand to lumbar spine cannot be performed, hand in front of
SIAS hand behind of SIAS (without
compensation) hand to lumbar spine
(without compensation)
0
1
2
Shoulder flexion 0°-90°
Elbow at 0°
Pronation-supination 0°
Immediate abduction or elbow flexion
abduction or elbow flexion during
movement complete flexion 90°, maintain
0°in elbow
0
1
2
Pronation-supination
Elbow at 90°
Shoulder at 0°
No pronation/supination, starting position
impossible limited pronation/supination,
maintains position complete
pronation/supination, maintains position
0
1
2
Subtotal III (max 6)
IV. Volitional movement with little or no synergy none partial full
Shoulder abduction 0 - 90°
Elbow at 0°
Forearm pronated
immediate supination or elbow flexion
supination or elbow flexion during
movement
abduction 90°, maintains extension and
pronation
0
1
2
Shoulder flexion 90 - 180°
Elbow at 0°
immediate abduction or elbow flexion 0
1
รหสผเขารวมวจย.............................................................
.........
Ref. code: 25605812030533ARL

125
Pronation-supination 0° abduction or elbow flexion during
movement complete flexion, maintains 0°
in elbow
2
Pronation/supination
Elbow at 0°
Shoulder at 30° - 90°
flexion
No pronation/supination, starting position
impossible Limited pronation/supination,
maintains extension
Full pronation/supination, maintain elbow
extension
0
1
2
Subtotal IV (max 6)
V. Normal reflex activity evaluated only if full score of 6 points achieved on part IV
Biceps, triceps, finger
flexors
0 points on part IV or 2 or 3 reflexes
markedly hyperactive
1 reflex markedly hyperactive or at least 2
reflexes lively
Maximum of 1 reflex lively, none
hyperactive
0
1
2
Subtotal V (max 2)
Total A (max 36)
B. Wrist support may be provided at the elbow to take or hold the
position, no support at wrist, check the passive range of motion prior
testing
none partial Full
Stability at 15° dorsiflexion
Elbow at 90°, forearm
pronated
Shoulder at 0
Less than 15° active dorsiflexion
Dorsiflexion 15° , no resistance is
taken
Maintain position against resistance
0
1
2
Repeated dorsiflexion / volar
flexion
Elbow at 90°, forearm
pronated
Shoulder at 0°, slight finger
flexion
Cannot perform volitionally
Limited active range of motion
Full active range of motion,
smoothly
0
1
2
Stability at 15° dorsiflexion
Elbow at 0°, forearm pronated
Slight shoulder
flexion/abduction
Less than 15° active dorsiflexion
Dorsiflexion 15° , no resistance is
taken
Maintain position against resistance
0
1
2
Repeated dorsiflexion / volar
flexion
Elbow at 0°, forearm pronated
Slight shoulder
flexion/abduction
Cannot perform volitionally
Limited active range of motion
Full active range of motion,
smoothly
0
1
2
Circumduction Cannot perform volitionally
Jerky movement or incomplete
Complete and smooth
circumduction
0
1
2
Total B (max 10)
C. Hand support may be provided at the elbow to keep 90 flexion, no
support at the wrist, compare with less-affected hand, the objects are
interposed, active grasp
none partial full
Mass flexion
From full active or passive
extension
0 1 2
Mass extension 0 1 2
Ref. code: 25605812030533ARL

126
From full active or passive
flexion
Grasp
A- flexion in PIP and DIP
(digit II-V) extension in MCP
II-V
Cannot be performed
Can hold position but weak
Maintains position against
resistance
0
1
2
B- thumb adduction
1-st CMC, MCP, IP at 0, scrap
of paper between thumb and 2-
nd MCP joint
Cannot be performed
Can hold paper but not against tug
Can hold paper against a tug
0
1
2
C – opposition pulpa of the
thumb against the pulpa of 2-
nd finger, pencil, tug upward
Cannot be performed
Can hold pencil but not against tug
Can hold pencil against a tug
0
1
2
D - cylinder grip
Cylinder shaped object (small
can) tug upward, opposition in
digits I and II
Cannot be performed
Can hold pencil but not against tug
Can hold pencil against a tug
0
1
2
E – spherical grip
Fingers in abduction/flexion,
thumb opposed, tennis ball
Cannot be performed
Can hold pencil but not against tug
Can hold pencil against a tug
0
1
2
Total C (max 14)
D.Coordination/Speed after one trial with both arms, blind-folded, tip
of the index finger from knee to nose, 5 times as fast as possible
marked slight None
Tremor 0 1 2
Dysmetria Pronounced or unsystematic
Slight and systematic
No dysmetria
0
1
2
˃ 5s 2 – 5s ˂ 1s
Time More than 5 seconds slower than less-affected side
2-5 seconds slower than less-affected side
maximum difference of 1 second between sides
0
1
2
Total D (max 6)
Total A - D (max 66)
A. Upper extremity /36
B. Wrist /10
C. Hand /14
D. Coordination/ Speed / 6
Total A-D (motor function) / 66
Ref. code: 25605812030533ARL

127
Each item is scored with 3 point ordinal scale;
0 = cannot perform
1= perform partially
2= perform fully maximum points
Motor function (Upper extremity maximum score=66)
Ref. code: 25605812030533ARL

128
APPENDIX I
Modified Ashworth Scale(166)
0 = No increase in muscle tone
1 = Slight increase in muscle tone, manifested by a catch and release or by minimal
resistance at the end of the range of motion when the affected part(s) is moved in flexion
or extension
1+ = Slight increase in muscle tone, manifested by a catch, followed by minimal
resistance throughout the reminder (less than half) of the ROM (range of movement)
2 = More marked increase in muscle tone through most of the ROM, but affected part(s) easily move
3 = Considerable increase in muscle tone passive, movement difficult
4 = Affected part(s) rigid in flexion or extension
Ref. code: 25605812030533ARL

129
APPENDIX J
REVISED NOTTINGHAM SENSORY ASSESSMENT(167)
Name………………………………..
Examiner……………………………………
Patient code…………………..….. Side of body affected: Right / Left / Both / Neither
Date of stroke……………………. Date of assessment………………………....
Tactile sensation Regions
of the
body
Light
touch
Temperature Pinprick Tactile
Localisation
Bilateral
Simultaneous
touch
PROPRIOCEPTION
L R L R L R L R
Shoulder
Elbow
Wrist
Hand
Stereognosis
10p Coin Brio Comb Sponge Cup
2p Coin Pencil Scissors Flannel Glass
50p Coin
COMMENTS: e.g. oedoma or bruising present, TEDS,
presence of reflexes
KEY
0 Absent
1 Impaired
2 Normal
9 Unable to test
KEY – Proprioception
0 Absent
1 Appreciation of movement (wrong direction)
2 Direction of movement (˃ 10 degree)
3 Joint Position Sense (< 10 degree)
9 Unable to test
Ref. code: 25605812030533ARL

130
NOTTINGHAM SENSORY ASSESSMENT
Instructions
The patient should be assessed in sitting and in a suitable state of undress
(ideally in shorts & underwear, without TED stockings). It should be ensured the patient
is comfortable and in a quiet area with no distractions. Each test is described and
demonstrated to the patient before he or she is blindfolded. The blindfold is removed
regularly throughout the test to avoid the patient becoming disorientated.
The body area to be tested is as marked on the body chart. Apply the test
sensation to the test area, to the left and right side in a random order. The patient is
asked to indicate, either verbally or by a body movement, whenever he or she feels the
test sensation. Each part of the body is assessed three times for each of the tests. Presence
of a reflex does not count as awareness of sensation, though this should be commented
on in the comment box.
Ref. code: 25605812030533ARL

131
Tactile Sensation
If the patient has problems communicating begin testing light touch, pressure and
pinprick sections.
Scoring criteria
0; Absent Fails to identify the test sensation on three occasions
1; Impaired Identifies the test sensation, but not on all three occasions in each region
of the body or feels duller
2; Normal Correctly identifies the test sensation on all three occasions 9 Unable to test
Light Touch Touch, not brush, the skin lightly with a cotton wool ball.
Pressure Press the skin just enough to deform the skin contour using the index
finger.
Pinprick The skin with a neurotip, maintaining even pressure.
Temperature Touch the skin with the side of one of two test tubes, one filled with
hot water, one filled with cold water (use the sides, not the bases of
the test tubes). Apply hot and cold tubes in random order.
Tactile localisation Only test those areas on which the patient has scored 2 on the
pressure section.
Record all others as 9.
Repeat the pressure test with the index fingertip coated with talcum
powder to mark the spot touched and ask the patient to point to the exact
spot that has been touched. If communication permits, the test may be
combined with the pressure test. 2cm of error are allowed.
Bilateral Simultaneous Touch
Touch corresponding sites on one or both sides of the body using
fingertip and ask the patient to indicate if both or one (and which) have
been touched. Only test those items on which patient has scored 2 on
pressure section. Record all others as 9.
Ref. code: 25605812030533ARL

132
Equipment required: Blindfold, cotton wool ball, Neurotip, two test tubes, hot and
cold water, talcum, powder
Kinaesthetic Sensations
All three aspects of movement are tested: appreciation of movement, its
direction and accurate joint position sense are assessed simultaneously. The limb on the
affected side of the body is supported and moved by the examiner in various directions
but movement is only at one joint at a time. The patient is asked to mirror the change of
movement with the other limb. Three practice movements are allowed before
blindfolding.
The upper limb is tested in sitting
Scoring
0 Absent No appreciation of movement taking place.
1 Appreciation of movement taking place
Patient indicates on each movement that a movement takes place
but the direction is incorrect.
2 Direction of movement sense
Patient is able to appreciate and mirror the direction of the test
movement taking place each time, but is inaccurate in its new
position.
3 Joint Position sense
Accurately mirrors the test movement to within 10°of the new
test position
9 Unable to test
Ref. code: 25605812030533ARL

133
Equipment required: Blindfold.
Stereognosis
The object is placed in the patient's hand for a maximum of 30 seconds.
Identification is by naming, description or by pair-matching with an identical set.
Affected side of the body is tested first. The object may be moved around the affected
hand by the examiner.
Scoring for each object
2 Normal Item is correctly named or matched.
1 Impaired Some features of object identified or attempts at descriptions of
objects.
0 Absent Unable to identify the object in any manner.
9 Unable to test
Equipment required: Blindfold, 2p coin, 10p coin, 50p coin, biro (score 2 if labelled
"pen"), pencil, comb, scissors, sponge, flannel (score 2 if labelled "cloth" or "face cloth"),
cup, glass (score 2 if labelled"beaker
Ref. code: 25605812030533ARL

134
APPENDIX K
Raw data
Intra- rater and inter-rater reliability test of the Wolf Motor Function Test and the Fugl-Meyer assessment of the upper extremity
Table K1 Characteristics of participants
ID Sex Age
(years)
Onset
(months)
Affected
side
Dominant-
hand
Weight
(kilograms)
Height
(centimeters)
Smoke Alcohol Education Underlying MMSE
(score)
Status Severity
level
1 Male 71 17 Rt. Rt. 57 169 S S B DM/HT 30 M Severe
2 Female 65 15 Rt. Rt. 58 160 N N B DLP 30 D Moderate
3 Male 45 16 Lt. Rt. 55 170 N S B DLP 30 S Moderate
4 Male 68 120 Lt. Rt. 82 165 S S S DM/HT/DLP 26 M Severe
(Education: B; Bachelor, S; secondary school) (Status: S; single, D; divorce, M; Married) (Smoke and alcohol: N; never, S; stop) (DLP; Dyslipidemia, HT;
hypertension, DM; diabetes mellitus)
Ref. code: 25605812030533ARL

135
Table K2 Wolf Motor Function Test (movement time)
(Assessor ‘1’) – affected side
Item
ID
1
1st
(seconds)
1
2nd
(seconds)
2
1st
(seconds)
2
2nd
(seconds)
3
1st
(seconds)
3
2nd
(seconds)
4
1st
(seconds)
4
2nd
(seconds)
5
1st
(seconds)
5
2nd
(seconds)
6
1st
(seconds)
6
2nd
(seconds)
8
1st
(seconds)
8
2nd
(seconds)
9
1st
(seconds)
9
2nd
(seconds)
1 3.37 3.41 3.15 3.80 120.00 120.00 120.00 120.00 2.10 1.97 2.84 2.95 3.97 3.91 120.00 120.00
2 1.26 2.57 2.00 2.38 120.00 120.00 120.00 120.00 1.25 1.51 2.08 2.10 3.62 4.56 7.56 7.74
3 1.16 1.27 1.37 1.25 3.19 2.77 2.60 3.02 1.00 0.71 0.69 1.24 1.87 1.20.00 120.00 120.00
4 6.94 6.71 120.00 120.00 120.00 120.00 120.00 120.00 6.08 8.74 120.00 120.00 120.00 120.00 120.00 120.00
(1st; first test, 2nd; second test (one week after the first test))
Table K2 Wolf Motor Function Test (movement time) (continued)
(Assessor ‘1’) – affected side
Item
ID
10
1st
(seconds)
10
2nd
(seconds)
11
1st
(seconds)
11
2nd
(seconds)
12
1st
(seconds)
12
2nd
(seconds)
13
1st
(seconds)
13
2nd
(seconds)
15
1st
(seconds)
15
2nd
(seconds)
16
1st
(seconds)
16
2nd
(seconds)
17
1st
(seconds)
17
2nd
(seconds)
1 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00
2 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 17.82 23.23 120.00 120.00
3 4.03 4.41 7.15 6.78 13.93 15.34 120.00 120.00 120.00 120.00 27.59 26.89 120.00 120.00
4 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00
(1st; first test, 2nd; second test (one week after the first test))
Ref. code: 25605812030533ARL

136
Table K3 Wolf Motor function Test (movement time)
(Assessor ‘2’) – affected side
Item
ID
1
1st
(seconds)
1
2nd
(seconds)
2
1st
(seconds)
2
2nd
(seconds)
3
1st
(seconds)
3
2nd
(seconds)
4
1st
(seconds)
4
2nd
(seconds)
5
1st
(seconds)
5
2nd
(seconds)
6
1st
(seconds)
6
2nd
(seconds)
8
1st
(seconds)
8
2nd
(seconds)
9
1st
(seconds)
9
2nd
(seconds)
1 5.06 3.64 3.28 3.23 120.00 120.00 120.00 120.00 2.20 2.09 2.38 2.67 3.95 3.33 120.00 120.00
2 2.62 2.43 2.19 1.69 120.00 120.00 120.00 120.00 1.47 2.04 2.53 2.61 3.63 3.50 7.28 7.63
3 1.25 1.25 1.29 1.40 2.38 2.52 2.60 2.43 1.35 1.15 1.31 1.41 0.97 0.77 120.00 120.00
4 6.18 6.30 120.00 120.00 120.00 120.00 120.00 120.00 9.00 8.87 120.00 120.00 120.00 120.00 120.00 120.00
(1st; first test, 2nd; second test (one week after the first test))
Table K3 Wolf Motor Function Test (movement time) (continued)
(Assessor ‘2’) – affected side
Item
ID
10
1st
(seconds)
10
2nd
(seconds)
11
1st
(seconds)
11
2nd
(seconds)
12
1st
(seconds)
12
2nd
(seconds)
13
1st
(seconds)
13
2nd
(seconds)
15
1st
(seconds)
15
2nd
(seconds)
16
1st
(seconds)
16
2nd
(seconds)
17
1st
(seconds)
17
2nd
(seconds)
1 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00
2 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 23.31 24.65 120.00 120.00
3 4.19 4.51 5.80 6.75 10.66 13.68 120.00 120.00 120.00 120.00 27.70 23.46 120.00 120.00
4 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00
(1st; first test, 2nd; second test (one week after the first test))
Ref. code: 25605812030533ARL

137
Table K4 Wolf Motor function Test (movement time)
(Average time) – affected side
Item
ID
Assessor 1
1st
(seconds)
Assessor 2
1st
(seconds)
Assessor 1
2nd
(seconds)
Assessor 2
2nd
(seconds)
1 81.03 81.07 81.12 80.10
2 66.37 66.94 66.87 66.97
3 36.31 38.83 35.96 35.96
4 104.87 105.03 105.01 105.01
(1st; first test, 2nd; second test (one week after the first test))
Table K5 Wolf Motor Function Test (functional ability scale)
(Assessor ‘1’) – affected side
Item
ID
1
1st
(score)
1
2nd
(score)
2
1st
(score)
1
2nd
(score)
3
1st
(score)
3
2nd
(score)
4
1st
(score)
4
2nd
(score)
5
1st
(score)
4
2nd
(score)
6
1st
(score)
6
2nd
(score)
8
1st
(score)
8
2nd
(score)
9
1st
(score)
9
2nd
(score)
1 3 3 1 1 1 1 3 3 3 4 4 3 1 1 1 1
2 4 4 1 1 1 1 3 3 4 4 4 4 3 3 1 1
3 5 4 4 4 4 4 3 3 4 4 5 5 1 1 4 5
4 2 2 1 1 1 1 2 2 2 2 1 1 1 1 1 1
(1st; first test, 2nd; second test (one week after the first test))
Ref. code: 25605812030533ARL

138
Table K5 Wolf Motor Function Test (functional ability scale) (continued)
(Assessor ‘1’) – affected side
Item
ID
10
1st
(score)
10
2nd
(score)
11
1st
(score)
11
2nd
(score)
12
1st
(score)
12
2nd
(score)
13
1st
(score)
13
2nd
(score)
15
1st
(score)
15
2nd
(score)
16
1st
(score)
16
2nd
(score)
17
1st
(score)
17
2nd
(score)
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
2 1 1 1 1 1 1 1 1 1 1 1 1 1 1
3 4 3 4 3 4 3 1 1 1 1 1 1 1 1
4 1 1 1 1 1 1 1 1 1 1 1 1 1 1
(1st; first test, 2nd; second test (one week after the first test))
Table K6 Wolf Motor Function Test (functional ability scale)
(Assessor ‘2’) – affected side
Item
ID
1
1st
(score)
2
2nd
(score)
2
1st
(score)
2
2nd
(score)
3
1st
(score)
3
2nd
(score)
4
1st
(score)
4
2nd
(score)
5
1st
(score)
5
2nd
(score)
6
1st
(score)
6
2nd
(score)
8
1st
(score)
8
2nd
(score)
9
1st
(score)
9
2nd
(score)
1 3 3 1 1 1 1 1 1 3 3 3 3 1 1 1 1
2 3 3 1 1 1 1 1 1 3 3 3 3 3 3 1 1
3 3 4 3 3 3 3 3 3 3 3 5 4 1 1 3 3
4 2 2 1 1 1 1 1 1 2 2 1 1 1 1 1 1
(1st; first test, 2nd; second test (one week after the first test))
Ref. code: 25605812030533ARL

139
Table K6 Wolf Motor Function Test (functional ability scale) (continued)
(Assessor ‘2’) – affected side
(1st; first test, 2nd; second test (one week after first test))
Table K7 Wolf Motor Function Test (functional ability scale)
(total score) – affected side
Item
ID
Assessor 1
1st
(score)
Assessor 2
1st
(score)
Assessor 1
2nd
(score)
Assessor 2
2nd
(score)
1 25 23 28 23
2 29 24 31 26
3 49 38 51 38
4 17 16 18 16
(1st; first test, 2nd; second test (one week after first test))
Item
ID
10
1st
(score)
10
2nd
(score)
11
1st
(score)
11
2nd
(score)
12
1st
(score)
12
2nd
(score)
13
1st
(score)
13
2nd
(score)
15
1st
(score)
15
2nd
(score)
16
1st
(score)
16
2nd
(score)
17
1st
(score)
17
2nd
(score)
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
2 1 1 1 1 1 1 1 1 1 1 2 2 1 1
3 3 3 3 3 3 3 1 1 1 1 3 3 2 2
4 1 1 1 1 1 1 1 1 1 1 2 2 1 1
Ref. code: 25605812030533ARL

140
Table K8 Wolf Motor Function Test (movement time)
(Assessor ‘1’) – less-affected side
Item
ID
1
1st
(seconds)
1
2nd
(seconds)
2
1st
(seconds)
2
2nd
(seconds)
3
1st
(seconds)
3
2nd
(seconds)
4
1st
(seconds)
4
2nd
(seconds)
5
1st
(seconds)
5
2nd
(seconds)
6
1st
(seconds)
6
2nd
(seconds)
8
1st
(seconds)
8
2nd
(seconds)
9
1st
(seconds)
9
2nd
(seconds)
1 0.31 0.30 0.88 0.72 0.62 0.60 0.90 0.99 0.46 0.51 0.25 0.78 1.82 1.75 1.75 1.73
2 0.51 0.50 1.14 1.14 0.34 0.58 1.01 0.75 0.50 0.59 0.72 0.57 2.06 2.37 2.60 2.15
3 0.44 0.38 0.41 0.45 0.56 0.43 0.69 0.81 0.29 0.31 0.34 0.20 0.69 0.83 1.00 0.88
4 0.43 0.47 0.90 0.54 0.72 0.45 1.38 1.37 0.97 0.90 0.4 0.53 1.63 2.10 2.35 3.07
(1st; first test, 2nd; second test (one week after the first test))
Table K8 Wolf Motor Function Test (movement time) (continued)
(Assessor ‘1’) – less-affected side
Item
ID
10
1st
(seconds)
10
2nd
(seconds)
11
1st
(seconds)
11
2nd
(seconds)
12
1st
(seconds)
12
2nd
(seconds)
13
1st
(seconds)
13
2nd
(seconds)
15
1st
(seconds)
15
2nd
(seconds)
16
1st
(seconds)
16
2nd
(seconds)
17
1st
(seconds)
17
2nd
(seconds)
1 1.03 1.37 4.59 4.40 3.66 4.36 6.1 7.60 2.69 3.37 17.02 17.58 3.68 4.47
2 1.92 1.82 3.59 3.63 6.32 6.80 11.28 9.88 5.84 5.77 15.97 16.02 8.16 8.16
3 1.03 1.21 3.10 3.51 4.81 3.75 4.56 5.07 3.53 3.50 17.19 17.59 3.63 4.18
4 2.25 1.98 3.50 3.02 6.22 6.25 11.06 12.90 4.97 6.35 19.75 19.68 1.15 1.41
(1st; first test, 2nd; second test (one week after the first test))
Ref. code: 25605812030533ARL

141
Table K9 Wolf Motor Function Test (movement time)
(Assessor ‘2’) – less-affected side
(1st; first test, 2nd; second test (one week after the first test))
Table K9 Wolf Motor Function Test (movement time) (continued)
(Assessor ‘2’) – less-affected side
Item
ID
10
1st
(seconds)
10
2nd
(seconds)
11
1st
(seconds)
11
2nd
(seconds)
12
1st
(seconds)
12
2nd
(seconds)
13
1st
(seconds)
13
2nd
(seconds)
15
1st
(seconds)
15
2nd
(seconds)
16
1st
(seconds)
16
2nd
(seconds)
17
1st
(seconds)
17
2nd
(seconds)
1 1.05 1.07 4.75 4.83 3.97 4.07 6.68 6.90 2.56 3.17 15.65 15.48 4.10 3.88
2 1.90 1.89 3.72 3.77 6.28 6.40 11.37 11.12 5.63 5.34 15.59 15.01 8.50 8.13
3 1.02 1.05 3.22 3.29 4.81 4.10 5.09 5.21 3.18 3.00 16.97 17.28 3.50 3.51
4 2.14 2.06 3.00 2.95 6.81 6.61 12.81 13.11 5.25 5.47 19.25 20.00 1.90 2.18
(1st; first test, 2nd; second test (one week after the first test))
Item
ID
1
1st
(seconds)
1
2nd
(seconds)
2
1st
(seconds)
2
2nd
(seconds)
3
1st
(seconds)
3
2nd
(seconds)
4
1st
(seconds)
4
2nd
(seconds)
5
1st
(seconds)
5
2nd
(seconds)
6
1st
(seconds)
6
2nd
(seconds)
8
1st
(seconds)
8
2nd
(seconds)
9
1st
(seconds)
9
2nd
(seconds)
1 0.20 0.22 0.60 0.58 0.95 0.98 0.94 0.97 0.40 0.33 0.50 0.56 1.46 1.60 1.59 1.65
2 0.50 0.59 1.00 1.11 0.63 0.61 1.06 1.58 0.88 0.77 0.83 1.01 1.75 1.94 2.37 2.42
3 0.56 0.52 0.78 0.68 0.66 0.65 0.50 0.49 0.41 0.45 0.42 0.50 1.02 0.57 1.05 1.02
4 0.86 0.81 0.81 0.97 0.62 0.64 1.32 1.74 1.04 0.97 1.12 0.92 1.71 1.70 2.10 2.28
Ref. code: 25605812030533ARL

142
Table K10 Wolf Motor Function Test (movement time)
(Total score) – less-affected side
Item
ID
Assessor 1
1st
(seconds)
Assessor 2
1st
(seconds)
Assessor 1
2nd
(seconds)
Assessor 2
2nd
(seconds)
1 46.04 45.43 46.20 46.27
2 62.34 61.99 58.28 60.94
3 42.63 42.93 40.00 39.12
4 58.10 60.80 57.19 60.97
(1st; first test, 2nd; second test (one week after the first test))
Table K11 Wolf Motor Function Test (functional ability scale)
(Assessor ‘1’) – less-affected side
Item
ID
1
1st
(score)
2
2nd
(score)
2
1st
(score)
2
2nd
(score)
3
1st
(score)
3
2nd
(score)
4
1st
(score)
4
2nd
(score)
5
1st
(score)
5
2nd
(score)
6
1st
(score)
6
2nd
(score)
8
1st
(score)
8
2nd
(score)
9
1st
(score)
9
2nd
(score)
1 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
2 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
3 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
4 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
(1st; first test, 2nd; second test (one week after the first test))
Ref. code: 25605812030533ARL
143
Table K11 Wolf Motor Function Test (functional ability scale) (continued)
(Assessor ‘1’) – less-affected side
(1st; first test, 2nd; second test (one week after the first test))
Table K12 Wolf Motor Function Test (functional ability scale)
(Assessor ‘2’) – less-affected side
Item
ID
1
1st
(score)
2
2nd
(score)
2
1st
(score)
2
2nd
(score)
3
1st
(score)
3
2nd
(score)
4
1st
(score)
4
2nd
(score)
5
1st
(score)
5
2nd
(score)
6
1st
(score)
6
2nd
(score)
8
1st
(score)
8
2nd
(score)
9
1st
(score)
9
2nd
(score)
1 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
2 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
3 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
4 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
(1st; first test, 2nd; second test (one week after the first test))
Item
ID
10
1st
(score)
10
2nd
(score)
11
1st
(score)
11
2nd
(score)
12
1st
(score)
12
2nd
(score)
13
1st
(score)
13
2nd
(score)
15
1st
(score)
15
2nd
(score)
16
1st
(score)
16
2nd
(score)
17
1st
(score)
17
2nd
(score)
1 5 5 5 5 5 5 5 5 5 5 5 5 5 5
2 5 5 5 5 5 5 5 5 5 5 5 5 5 5
3 5 5 5 5 5 5 5 5 5 5 5 5 5 5
4 5 5 5 5 5 5 5 5 5 5 5 5 5 5
Ref. code: 25605812030533ARL

144
Table K12 Wolf Motor Function Test (functional ability scale)
(Assessor ‘2’) – less-affected side
Item
ID
10
1st
(score)
10
2nd
(score)
11
1st
(score)
11
2nd
(score)
12
1st
(score)
12
2nd
(score)
13
1st
(score)
13
2nd
(score)
15
1st
(score)
15
2nd
(score)
16
1st
(score)
16
2nd
(score)
17
1st
(score)
17
2nd
(score)
1 1.05 1.07 4.75 4.83 3.97 4.07 6.68 6.90 2.56 3.17 15.65 15.48 4.10 3.88
2 1.90 1.89 3.72 3.77 6.28 6.40 11.37 11.12 5.63 5.34 15.59 15.01 8.50 8.13
3 1.02 1.05 3.22 3.29 4.81 4.10 5.09 5.21 3.18 3.00 16.97 17.28 3.50 3.51
4 2.14 2.06 3.00 2.95 6.81 6.61 12.81 13.11 5.25 5.47 19.25 20.00 1.90 2.18
Table K13 Wolf Motor Function Test (functional ability scale)
(total score) – less-affected side
ID Assessor 1
1st
(score)
Assessor 2
1st
(score)
Assessor 1
2nd
(score)
Assessor 2
2nd
(score)
1 75 75 75 75
2 75 75 75 75
3 75 75 75 75
4 75 75 75 75
(1st; first test, 2nd; second test (one week after the first test))
Ref. code: 25605812030533ARL

145
APPENDIX L
Raw data
Effect of the Bobath therapy on upper limb and hand functions in stroke individuals with moderate to severe arm deficits
Table L1 Characteristics of participants
ID Sex Age
(years)
Onset
(months)
Affected side Dominant-hand Weight
(kilograms)
Height
(centimeters)
Smoker Alcohol
1 male 45 17 Lt. Rt. 79 173 N Y
2 female 57 25 Lt. Rt. Unknown Unknown N N
3 female 55 83 Rt. Lt. 53 155 N N
4 male 57 7 Rt. Rt. 69 171 N S
5 male 63 60 Rt. Lt. 58 160 N S
6 female 56 72 Lt. Rt. 56 165 N N
7 male 45 17 Lt. Rt. 55 170 N S
8 male 59 168 Rt. Rt. 45 145 N N
9 male 64 276 Rt. Rt. 53 160 N N
10 female 47 120 Rt. Rt. 67 160 Y Y
11 male 73 84 Rt. Rt. 54 155 Y S
12 male 60 7 Lt. Rt. 70 166 N Y
13 male 59 33 Rt. Rt. 62 158 N N
14 male 61 84 Lt. Rt. 70 170 N Y
15 male 60 204 Lt. Rt. 67 165 N S
16 female 67 48 Rt. Rt. 52 160 N N
17 female 71 84 Lt. Rt. 62 156 N N
18 male 76 24 Rt. Rt. 73 165 N N
19 male 45 48 Rt. Rt. 80 185 N N
20 male 64 36 Rt. Rt. 66 170 Y Y
21 male 56 60 Lt. Rt. 63 160 N N
22 male 68 120 Rt. Rt. 70 157 S N
Ref. code: 25605812030533ARL

146
23 male 67 24 Rt. Rt. Unknown Unknown S S
24 female 64 20 Rt. Rt. Unknown Unknown N N
25 female 47 6 Rt. Rt. 58 153 N N
26 male 66 84 Lt. Rt. 67 168 S S
(Education: B; Bachelor, S; secondary school) (Status: S; single, D; divorce, M; Married) (Smoke and alcohol: N; never, S; stop, Y; yes)
Ref. code: 25605812030533ARL

147
Table L2 Characteristics of participants
ID Education Underlying
diseases
MMSE
(Score)
VAS
(millimeter)
Status Subluxation
1 P HT 27 - D Y
2 P DM/HT 25 - S Y
3 S DM/HT 29 - M Y
4 B DM/HT 27 shoulder 40 mm M Y
5 P HT / DLP 28 shoulder 15 mm D Y
6 S DM 29 shoulder 10 mm M Y
7 B HT/DLP 30 - S Y
8 P HT 22 - M Y
9 P DLP 28 - M Y
10 S HT 22 - M Y
11 S HT 22 - M Y
12 S HT 30 - M Y
13 P HT 21 - M Y
14 S DLP 28 - M Y
15 S HT 24 - M Y
16 P HT 19 shoulder 40 mm M Y
17 S HT 24 - D Y
18 S HT 24 - M Y
19 P HT 17 - D Y
20 P HT 17 - M Y
21 S HT/DLP 24 - D Y
22 S HT 22 - M Y
23 P HT 17 - M Y
24 P HT 20 - D Y
25 S DLP 22 - M Y
26 P DLP 25
M Y
(Education: B; Bachelor, P; primary school, S; secondary school) (Status: S; single, D; divorce, M; Married)
(DLP; Dyslipidemia, HT; hypertension) (DLP; Dyslipidemia, HT; hypertension, DM; diabetes mellitus) (Y; yes)
Ref. code: 25605812030533ARL

148
Table L3 Wolf Motor Function Test (movement time) at pre-assessment
Item
ID
Item 1 (seconds)
Item 2 (seconds)
Item 3 (seconds)
Item 4 (seconds)
Item 5 (seconds)
Item 6 (seconds)
Item 8 (seconds)
Item 9 (seconds)
Item 10 (seconds)
Item 11 (seconds)
Item 12 (seconds)
Item 13 (seconds)
Item 15 (seconds)
Item 16 (seconds)
Item 17 (seconds)
Average
time (seconds)
1 1.91 1.96 120.00 120.00 2.50 1.54 1.13 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 80.60
2 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 NT 120.00
3 1.35 1.37 120.00 1.35 1.53 4.06 1.19 120.00 9.50 14.13 120.00 13.44 8.88 20.50 16.56 31.78
4 2.06 18.09 120.00 120.00 23.85 120.00 2.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 91.07
5 1.94 1.94 120.00 120.00 1.87 2.35 1.78 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 80.66
6 2.32 2.44 2.00 4.00 2.04 2.16 2.12 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 69.65
7 1.78 2.19 120.00 120.00 2.19 2.98 1.47 120.00 4.16 14.94 14.59 120.00 120.00 13.03 120.00 51.82
8 2.41 1.44 120.00 120.00 2.84 6.72 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 88.89
9 2.82 1.68 120.00 120.00 1.41 1.44 3.41 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 80.71
10 4.28 17.58 5.09 120.00 2.85 1.75 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 NT 79.40
11 2.00 3.31 3.37 3.06 2.59 3.93 2.00 8.44 8.12 120.00 62.87 34.72 17.10 20.50 5.25 19.81
12 3.50 6.21 120.00 120.00 3.31 120.00 2.56 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 89.03
13 4.78 120.00 120.00 120.00 4.18 120.00 1.91 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 96.72
14 0.78 0.91 2.19 2.34 0.94 1.12 0.70 5.79 120.00 120.00 120.00 120.00 36.93 11.09 3.72 36.43
15 4.16 3.65 120.00 120.00 2.22 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 NT 95.00
16 7.21 8.26 120.00 10.66 12.87 12.57 19.19 120.00 120.00 120.00 120.00 120.00 120.00 120.00 NT 73.63
17 2.10 5.52 3.91 18.93 2.28 120.00 1.53 120.00 3.00 120.00 26.75 120.00 120.00 120.00 NT 56.00
18 1.72 1.72 1.22 1.47 2.43 1.81 5.04 120.00 3.31 3.31 13.34 10.47 6.25 15.72 6.06 12.92
19 2.16 3.28 4.72 16.87 2.16 2.56 8.06 120.00 120.00 120.00 120.00 120.00 120.00 120.00 4.06 58.92
20 4.28 1.56 1.10 1.22 1.62 1.34 2.16 120.00 4.57 120.00 120.00 120.00 120.00 120.00 NT 52.70
21 4.00 3.75 120.00 120.00 2.63 0.72 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 NT 86.50
22 3.94 3.22 120.00 120.00 2.31 3.91 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 NT 86.67
23 1.21 1.68 3.85 9.62 1.94 1.96 3.80 25.43 10.62 45.82 120.00 43.13 38.07 120.00 70.86 33.20
24 2.09 2.44 5.20 6.10 2.85 2.97 3.42 10.59 4.47 120.00 120.00 120.00 120.00 120.00 10.70 43.39
25 2.69 7.19 6.34 5.82 4.87 3.07 3.69 120.00 120.00 120.00 120.00 120.00 120.00 120.00 16.78 59.36
26 1.38 1.09 6.37 7.16 0.97 0.94 1.58 1.93 2.13 3.09 12.04 21.28 5.19 15.94 NT 5.79
Ref. code: 25605812030533ARL

149
Table L4 Wolf Motor Function Test (movement time) at post-assessment
Item
ID
Item 1
(seconds)
Item 2
(seconds)
Item 3
(seconds)
Item 4
(seconds)
Item 5
(seconds)
Item 6
(seconds)
Item 8
(seconds)
Item 9
(seconds)
Item 10
(seconds)
Item 11
(seconds)
Item 12
(seconds)
Item 13
(seconds)
Item 15
(seconds)
Item 16
(seconds)
Item 17
(seconds)
Average
time
(seconds)
1 1.12 1.85 24.15 6.06 1.53 1.60 1.72 120.00 120.00 120.00 120.00 109.00 120.00 94.84 36.10 58.53
2 27.47 120.00 120.00 120.00 28.31 120.00 9.93 120.00 120.00 120.00 120.00 120.00 120.00 120.00 NT 98.98
3 0.97 2.00 1.00 1.03 1.75 1.10 0.90 3.84 4.13 5.41 7.07 16.06 8.12 7.71 6.28 4.49
4 2.07 2.00 120.00 120.00 1.47 1.81 2.97 120.00 120.00 120.00 120.00 120.00 120.00 120.00 26.37 74.45
5 1.16 1.06 120.00 27.91 2.88 2.25 2.81 120.00 38.43 120.00 120.00 120.00 120.00 120.00 120.00 69.10
6 1.28 1.28 1.25 0.87 1.44 0.93 1.89 2.06 46.43 120.00 120.00 120.00 15.65 97.18 4.56 35.65
7 1.44 1.41 5.31 5.36 1.65 1.81 1.60 19.53 4.46 4.97 16.25 120.00 55.62 13.25 6.34 17.27
8 1.18 1.56 7.41 4.68 1.50 1.88 1.41 120.00 120.00 120.00 120.00 120.00 70.56 25.40 120.00 55.71
9 1.78 2.56 120.00 120.00 2.88 2.12 1.39 120.00 120.00 120.00 120.00 120.00 91.68 88.84 86.66 74.52
10 4.41 6.78 120.00 120.00 1.72 0.86 4.03 120.00 13.37 120.00 120.00 120.00 120.00 25.77 NT 64.07
11 2.07 2.19 2.82 3.09 2.10 2.10 1.88 5.13 4.05 4.28 13.88 68.75 9.50 17.22 4.82 9.59
12 1.96 1.94 120.00 120.00 2.40 3.37 1.81 120.00 120.00 120.00 120.00 120.00 120.00 120.00 66.93 77.23
13 2.15 120.00 120.00 120.00 2.43 120.00 1.78 120.00 120.00 120.00 120.00 120.00 120.00 120.00 120.00 96.42
14 0.63 1.19 1.46 1.79 1.25 1.59 1.00 5.72 9.25 10.31 47.06 41.25 47.06 10.28 4.53 12.29
15 2.19 1.81 120.00 120.00 1.19 1.31 3.75 120.00 120.00 120.00 120.00 120.00 120.00 120.00 NT 77.88
16 2.28 2.10 3.50 4.25 1.56 2.97 2.32 2.97 2.32 120.00 120.00 46.47 120.00 32.31 NT 33.08
17 2.12 4.53 4.28 4.75 1.56 1.41 2.56 120.00 3.85 4.94 26.18 83.16 25.55 20.34 NT 21.80
18 1.51 3.78 0.72 1.43 2.22 1.66 2.07 14.07 2.78 4.47 8.53 10.97 5.35 8.13 3.22 4.73
19 1.26 1.31 3.08 10.50 1.36 1.49 3.50 120.00 8.07 120.00 120.00 32.04 120.00 17.23 4.68 37.63
20 2.38 1.44 3.50 3.44 1.47 1.09 1.25 120.00 4.81 7.44 120.00 24.47 120.00 19.50 15.03 29.72
21 2.10 2.22 120.00 120.00 2.00 1.84 5.59 120.00 120.00 120.00 120.00 120.00 120.00 72.00 NT 74.70
22 2.94 3.43 120.00 120.00 3.28 3.28 7.78 120.00 120.00 120.00 120.00 120.00 120.00 120.00 NT 78.62
23 1.10 2.00 5.35 6.00 2.25 2.56 3.25 18.88 11.28 12.06 120.00 33.50 27.03 48.93 NT 21.01
24 1.38 1.60 3.01 4.13 1.09 1.49 3.78 6.81 3.76 4.04 120.00 25.53 15.71 22.00 7.06 14.76
25 1.37 1.16 1.13 3.31 1.10 1.37 2.25 120.00 120.00 10.28 120.00 120.00 120.00 33.06 4.25 43.95
26 0.66 0.71 0.69 1.15 0.85 0.62 1.09 2.75 1.72 2.22 33.68 10.56 8.71 13.97 NT 5.67
Ref. code: 25605812030533ARL

150
Table L5 Wolf Motor Function Test (functional ability scale) at pre-assessment
Item
ID
Item 1
(score)
Item 2
(score)
Item 3
(score)
Item 4
(score)
Item 5
(score)
Item 6
(score)
Item 8
(score)
Item 9
(score)
Item 10
(score)
Item 11
(score)
Item 12
(score)
Item 13
(score)
Item 15
(score)
Item 16
(score)
Item 17
(score)
Total
(score)
1 3 3 1 1 3 3 1 1 1 1 1 1 1 1 1 23
2 1 1 0 0 1 1 1 1 1 1 1 1 1 1 NT 14
3 4 4 1 4 4 3 4 1 3 3 1 3 3 4 1 43
4 2 2 0 0 2 1 4 1 1 1 1 1 1 1 1 17
5 4 4 1 1 4 3 4 1 1 1 1 1 1 1 1 29
6 4 4 1 3 4 4 4 1 1 1 1 1 1 1 1 32
7 3 3 1 1 3 3 3 1 4 3 3 1 1 3 1 34
8 3 3 1 1 3 0 0 1 1 1 1 1 1 0 1 18
9 3 3 1 1 3 3 2 1 1 1 1 1 1 1 1 24
10 3 2 2 1 3 3 1 1 1 1 1 1 1 1 NT 22
11 4 4 4 4 4 4 4 3 2 1 2 2 2 4 3 47
12 3 3 0 0 2 1 4 1 1 1 1 1 1 1 1 19
13 3 1 1 1 2 1 4 1 1 1 1 1 1 0 1 20
14 5 5 3 3 4 4 5 3 1 1 1 1 2 3 4 45
15 2 2 1 1 3 1 1 1 1 1 1 1 1 1 NT 19
16 3 2 1 2 3 3 3 1 1 1 1 1 1 1 NT 25
17 2 3 3 3 4 1 5 1 2 1 4 1 1 1 NT 32
18 5 5 4 4 4 3 3 1 4 4 3 4 5 4 2 55
19 4 3 2 2 3 3 2 1 1 1 1 1 1 1 4 30
20 3 3 4 4 3 3 3 1 3 1 1 1 1 1 2 34
21 2 2 1 1 4 4 1 1 1 1 1 1 1 1 NT 23
22 4 4 1 1 4 3 1 1 1 1 1 1 1 1 NT 26
23 4 4 3 3 4 3 4 3 3 3 1 2 3 2 NT 41
24 3 3 2 2 3 3 2 2 3 1 1 1 1 1 2 27
25 3 2 2 2 3 3 3 1 1 1 1 1 1 1 2 27
26 4 4 3 3 3 3 4 4 4 4 3 3 4 2 NT 45
Ref. code: 25605812030533ARL

151
Table L6 Wolf Motor Function Test (functional ability scale) at post-assessment
Item
ID
Item 1
(score)
Item 2
(score)
Item 3
(score)
Item 4
(score)
Item 5
(score)
Item 6
(score)
Item 8
(score)
Item 9
(score)
Item 10
(score)
Item 11
(score)
Item 12
(score)
Item 13
(score)
Item 15
(score)
Item 16
(score)
Item 17
(score)
Total
(score)
1 4 3 2 2 4 4 4 1 1 1 1 2 1 2 2 34
2 2 1 1 1 1 1 2 1 1 1 1 1 1 1 NT 16
3 5 5 5 5 5 5 5 5 5 5 5 4 4 5 5 73
4 3 3 1 1 3 3 3 1 1 1 1 1 1 1 2 26
5 4 5 1 2 4 5 5 1 2 1 1 1 1 1 1 35
6 5 5 5 5 5 5 5 1 2 1 1 1 4 3 5 53
7 5 5 3 3 4 4 5 3 4 4 4 3 2 3 4 56
8 4 3 3 3 3 3 3 1 1 2 1 1 2 3 1 34
9 3 3 1 1 3 3 4 1 1 1 1 1 1 1 2 27
10 5 4 1 1 5 5 5 1 3 1 1 1 1 2 NT 36
11 5 5 5 4 5 5 5 5 5 5 4 3 5 4 5 70
12 5 5 1 1 4 3 5 1 1 1 1 1 1 1 2 33
13 2 1 1 1 3 1 4 1 3 1 1 1 1 1 1 23
14 5 5 4 4 5 5 5 3 3 3 2 2 2 3 4 55
15 3 5 1 1 4 4 3 1 1 1 1 1 1 1 NT 28
16 4 5 5 4 4 4 4 1 1 1 1 2 0 3 NT 39
17 5 4 5 5 5 5 5 1 4 4 3 2 4 3 NT 55
18 5 3 5 5 4 5 5 3 4 4 4 4 4 4 5 64
19 5 5 3 3 4 4 3 1 2 1 1 2 1 2 4 41
20 3 4 4 3 4 4 4 1 4 3 1 2 1 2 2 42
21 5 5 1 1 5 5 5 1 1 1 1 1 1 2 NT 35
22 5 4 1 1 4 4 3 1 1 1 1 1 1 1 NT 29
23 4 4 3 3 4 4 3 3 3 3 1 3 4 2 NT 44
24 4 4 3 3 4 4 3 3 3 2 1 2 2 2 3 43
25 5 5 5 4 4 4 4 1 1 3 1 1 1 2 3 44
26 5 5 5 5 5 5 4 3 5 4 3 2 4 3 NT 58
Ref. code: 25605812030533ARL

152
Table L7 Fugl – Meyer assessment (upper extremity) at pre-assessment
Item
ID
A1
Flexors
(score)
A1
Extensors
(score)
A2
Shoulder
retraction
(score)
A2
Shoulder
elevation
(score)
A2
Shoulder
abduction
(score)
A2
Shoulder
external
(score)
A2
Elbow
flexion
(score)
A2
Forearm
supination
(score)
A2
Shoulder
adduction
(score)
A2
Elbow
Extension
(score)
A2
Forearm
pronation
(score)
1 2 2 2 2 2 2 2 0 2 1 0
2 2 0 0 1 0 0 0 0 0 0 0
3 2 2 2 1 2 1 2 0 2 2 1
4 2 2 0 1 1 0 1 0 0 0 0
5 2 2 0 1 0 0 1 0 0 0 0
6 2 2 0 1 0 0 1 0 0 1 0
7 2 2 1 1 1 1 1 1 1 1 1
8 2 2 1 1 1 1 1 0 1 1 1
9 2 2 1 1 1 1 1 0 2 2 0
10 2 2 2 1 1 1 1 0 2 2 0
11 2 2 1 1 2 1 1 0 1 1 0
12 2 2 1 1 1 1 1 0 1 1 0
13 2 2 1 1 1 0 0 0 1 0 0
14 2 2 2 2 2 2 2 0 2 2 1
15 2 2 1 1 1 0 1 0 1 1 0
16 2 2 0 0 1 0 1 0 0 0 0
17 2 2 0 0 1 0 2 0 0 1 0
18 2 2 1 1 1 2 1 1 2 1 0
19 2 2 1 1 1 1 1 0 1 1 0
20 2 2 1 2 2 2 2 1 2 1 1
21 2 2 1 1 1 1 2 1 0 1 0
22 2 2 1 0 1 1 1 0 1 0 0
23 2 2 1 2 1 1 2 1 2 1 1
24 2 2 1 1 1 1 1 0 1 0 1
25 2 2 0 1 0 0 1 0 2 2 0
26 2 2 1 2 1 1 2 1 1 1 1
Ref. code: 25605812030533ARL

153
Table L8 Fugl – Meyer assessment (upper extremity) at pre-assessment (continued)
Item
ID
A3 - Hand to
lumbar
(score)
A3 – 2
(score)
A3 – 3
(score)
A4 – 1
(score)
A4 – 2
(score)
A4 – 3
(score)
A5
(score)
B1
(score)
B2
(score)
B3
(score)
B4
(score)
B5
(score)
1 1 1 0 1 1 0 0 0 0 0 0 0
2 0 1 0 0 0 0 1 0 0 0 0 0
3 1 0 1 0 0 1 2 1 1 1 1 1
4 1 0 0 1 0 0 1 0 0 0 0 0
5 1 0 0 0 0 0 2 0 0 0 0 0
6 2 0 0 0 0 0 2 1 1 0 0 0
7 1 1 1 1 1 1 0 1 1 1 1 1
8 1 0 0 1 0 0 1 0 0 0 0 0
9 1 1 1 1 1 1 1 0 0 0 0 0
10 0 0 1 0 0 0 2 0 0 0 0 0
11 2 2 2 1 0 1 2 0 0 0 0 0
12 0 0 0 0 0 0 2 0 0 0 0 0
13 1 0 0 1 0 0 0 1 0 0 0 0
14 2 1 1 2 1 1 1 0 0 1 0 1
15 0 0 0 0 0 0 2 0 0 0 0 0
16 0 0 0 0 0 1 2 0 0 0 1 0
17 2 0 1 0 0 1 2 0 0 0 0 0
18 1 0 1 0 2 2 2 2 2 2 2 2
19 0 0 0 0 0 1 2 1 0 1 1 0
20 1 2 1 1 1 0 1 0 2 0 0 0
21 0 0 1 0 0 0 2 0 0 0 0 0
22 0 0 1 0 0 0 2 1 1 0 1 0
23 2 1 2 1 0 0 0 2 2 1 1 2
24 0 1 1 1 1 0 1 1 1 1 1 1
25 1 1 1 1 0 1 1 0 0 0 0 0
26 1 2 1 1 1 1 0 1 0 1 1 1
Ref. code: 25605812030533ARL

154
Table L9 Fugl – Meyer assessment (upper extremity) at pre-assessment (continued)
Item
ID
C - Mass
flexion
(score)
C - Mass
extension
(score)
C – A
(score)
C – B
(score)
C – C
(score)
C - D
(score)
C – E
(score)
D – Tremor
(score)
D – Dysmetria
(score)
D – Time
(score)
1 1 0 2 0 0 1 0 1 1 0
2 1 1 1 0 0 0 0 NT NT NT
3 2 0 0 0 1 1 0 1 1 1
4 1 0 1 0 0 1 1 NT NT NT
5 0 0 2 0 0 0 0 0 0 0
6 0 0 2 0 0 0 0 1 0 0
7 1 1 2 0 2 2 1 2 2 0
8 1 0 0 0 0 1 1 NT NT NT
9 1 0 1 0 1 2 2 0 0 0
10 2 0 1 0 0 0 0 0 0 0
11 1 0 2 2 2 2 2 2 1 1
12 0 2 2 0 0 0 0 NT NT NT
13 0 0 1 0 0 1 0 NT NT NT
14 2 1 2 1 2 2 2 1 1 0
15 0 0 0 0 0 0 0 0 0 0
16 0 0 0 0 0 0 0 0 0 0
17 2 1 2 2 2 0 1 1 1 1
18 2 2 2 2 1 1 1 0 0 0
19 2 0 2 2 2 0 1 0 0 0
20 2 1 2 2 1 2 2 1 1 0
21 0 0 0 0 0 0 0 1 0 0
22 1 1 0 0 0 0 0 1 0 0
23 2 2 2 2 2 2 2 0 1 0
24 1 0 1 1 1 1 1 1 0 0
25 2 0 2 1 0 2 1 0 1 0
26 2 2 2 2 2 2 2 1 1 1
Ref. code: 25605812030533ARL

155
Table L10 Fugl – Meyer assessment (upper extremity) at post -assessment
Item
ID
A1
Flexors
(score)
A1
Extensors
(score)
A2
Shoulder
retraction
(score)
A2
Shoulder
elevation
(score)
A2
Shoulder
abduction
(score)
A2
Shoulder
external
(score)
A2
Elbow
flexion
(score)
A2
Forearm
supination
(score)
A2
Shoulder
adduction
(score)
A2
Elbow
extension
(score)
A2
Forearm
pronation
(score)
1 2 2 2 2 2 2 2 0 2 1 0
2 2 0 0 1 0 0 0 0 0 0 0
3 2 2 2 1 2 1 2 0 2 2 1
4 2 2 0 1 1 0 1 0 0 0 0
5 2 2 0 1 0 0 1 0 0 0 0
6 2 2 0 1 0 0 1 0 0 1 0
7 2 2 1 1 1 1 1 1 1 1 1
8 2 2 1 1 1 1 1 0 1 1 1
9 2 2 1 1 1 1 1 0 2 2 0
10 2 2 2 1 1 1 1 0 2 2 0
11 2 2 1 1 2 1 1 0 1 1 0
12 2 2 1 1 1 1 1 0 1 1 0
13 2 2 1 1 1 0 0 0 1 0 0
14 2 2 2 2 2 2 2 0 2 2 1
15 2 2 1 1 1 0 1 0 1 1 0
16 2 2 0 0 1 0 1 0 0 0 0
17 2 2 0 0 1 0 2 0 0 1 0
18 2 2 1 1 1 2 1 1 2 1 0
19 2 2 1 1 1 1 1 0 1 1 0
20 2 2 1 2 2 2 2 1 2 1 1
21 2 2 1 1 1 1 2 1 0 1 0
22 2 2 1 0 1 1 1 0 1 0 0
23 2 2 1 2 1 1 2 1 2 1 1
24 2 2 1 1 1 1 1 0 1 0 1
25 2 2 0 1 0 0 1 0 2 2 0
26 2 2 1 2 1 1 2 1 1 1 1
Ref. code: 25605812030533ARL

156
Table L11 Fugl – Meyer assessment (upper extremity) at post-assessment (continued)
Item
ID
A3 - Hand to
lumbar
(score)
A3 – 2
(score)
A3 – 3
(score)
A4 – 1
(score)
A4 – 2
(score)
A4 – 3
(score)
A5
(score)
B1
(score)
B2
(score)
B3
(score)
B4
(score)
B5
(score)
1 1 1 0 1 1 0 0 0 0 0 0 0
2 0 1 0 0 0 0 1 0 0 0 0 0
3 1 0 1 0 0 1 2 1 1 1 1 1
4 1 0 0 1 0 0 1 0 0 0 0 0
5 1 0 0 0 0 0 2 0 0 0 0 0
6 2 0 0 0 0 0 2 1 1 0 0 0
7 1 1 1 1 1 1 0 1 1 1 1 1
8 1 0 0 1 0 0 1 0 0 0 0 0
9 1 1 1 1 1 1 1 0 0 0 0 0
10 0 0 1 0 0 0 2 0 0 0 0 0
11 2 2 2 1 0 1 2 0 0 0 0 0
12 0 0 0 0 0 0 2 0 0 0 0 0
13 1 0 0 1 0 0 0 1 0 0 0 0
14 2 1 1 2 1 1 1 0 0 1 0 1
15 0 0 0 0 0 0 2 0 0 0 0 0
16 0 0 0 0 0 1 2 0 0 0 1 0
17 2 0 1 0 0 1 2 0 0 0 0 0
18 1 0 1 0 2 2 2 2 2 2 2 2
19 0 0 0 0 0 1 2 1 0 1 1 0
20 1 2 1 1 1 0 1 0 2 0 0 0
21 0 0 1 0 0 0 2 0 0 0 0 0
22 0 0 1 0 0 0 2 1 1 0 1 0
23 2 1 2 1 0 0 0 2 2 1 1 2
24 0 1 1 1 1 0 1 1 1 1 1 1
25 1 1 1 1 0 1 1 0 0 0 0 0
26 1 2 1 1 1 1 0 1 0 1 1 1
Ref. code: 25605812030533ARL

157
Table L12 Fugl – Meyer assessment (upper extremity) at post-assessment (continued)
Item
ID
C - Mass
flexion
(score)
C - Mass
extension
(score)
C – A
(score)
C – B
(score)
C – C
(score)
C - D
(score)
C – E
(score)
D – Tremor
(score)
D – Dysmetria
(score)
D – Time
(score)
1 1 0 2 0 0 1 0 1 1 0
2 1 1 1 0 0 0 0 NT NT NT
3 2 0 0 0 1 1 0 1 1 1
4 1 0 1 0 0 1 1 NT NT NT
5 0 0 2 0 0 0 0 0 0 0
6 0 0 2 0 0 0 0 1 0 0
7 1 1 2 0 2 2 1 2 2 0
8 1 0 0 0 0 1 1 NT NT NT
9 1 0 1 0 1 2 2 0 0 0
10 2 0 1 0 0 0 0 0 0 0
11 1 0 2 2 2 2 2 2 1 1
12 0 2 2 0 0 0 0 NT NT NT
13 0 0 1 0 0 1 0 NT NT NT
14 2 1 2 1 2 2 2 1 1 0
15 0 0 0 0 0 0 0 0 0 0
16 0 0 0 0 0 0 0 0 0 0
17 2 1 2 2 2 0 1 1 1 1
18 2 2 2 2 1 1 1 0 0 0
19 2 0 2 2 2 0 1 0 0 0
20 2 1 2 2 1 2 2 1 1 0
21 0 0 0 0 0 0 0 1 0 0
22 1 1 0 0 0 0 0 1 0 0
23 2 2 2 2 2 2 2 0 1 0
24 1 0 1 1 1 1 1 1 0 0
25 2 0 2 1 0 2 1 0 1 0
26 2 2 2 2 2 2 2 1 1 1
Ref. code: 25605812030533ARL

158
Table L13 Modified Ashworth Scale at pre-assessment
Item
ID
Shoulder internal rotators
(scale)
Shoulder adductors
(scale)
Elbow flexors
(scale)
Elbow extensors
(scale)
Pronators
(scale)
Wrist flexors
(scale)
Finger flexors
(scale)
1 1.00 0.00 1.00 0.00 1.00 1.00 1.50
2 0.00 1.50 0.00 0.00 0.00 0.00 0.00
3 0.00 1.00 0.00 0.00 0.00 1.00 0.00
4 0.00 0.00 1.00 2.00 0.00 1.00 1.50
5 0.00 1.00 2.00 2.00 0.00 2.00 2.00
6 0.00 0.00 1.00 2.00 0.00 1.50 1.50
7 0.00 0.00 2.00 0.00 0.00 2.00 1.50
8 0.00 0.00 1.00 2.00 0.00 1.50 1.50
9 1.00 2.00 1.00 2.00 1.50 1.50 1.00
10 0.00 1.50 2.00 0.00 1.50 2.00 2.00
11 0.00 1.00 1.00 0.00 0.00 1.00 0.00
12 0.00 1.50 1.50 1.00 0.00 1.00 1.50
13 1.50 0.00 1.00 1.00 0.00 1.50 2.00
14 0.00 0.00 1.00 0.00 0.00 1.00 1.00
15 0.00 1.50 1.00 0.00 0.00 0.00 0.00
16 0.00 1.50 0.00 0.00 0.00 1.50 1.50
17 0.00 1.00 0.00 0.00 0.00 1.00 0.00
18 0.00 0.00 0.00 0.00 0.00 0.00 0.00
19 0.00 1.50 1.00 0.00 0.00 1.00 1.00
20 1.00 0.00 1.00 1.00 1.00 1.00 1.00
21 0.00 1.00 1.50 0.00 0.00 1.50 1.00
22 0.00 1.50 1.00 1.00 0.00 1.50 1.50
23 0.00 0.00 0.00 0.00 0.00 0.00 0.00
24 0.00 1.00 0.00 0.00 0.00 1.00 0.00
25 0.00 0.00 1.00 0.00 0.00 1.00 1.00
26 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Ref. code: 25605812030533ARL

159
Table L14 Modified Ashworth Scale at post-assessment
Item
ID
Shoulder internal rotators
(scale)
Shoulder adductors
(scale)
Elbow flexors
(scale)
Elbow extensors
(scale)
Pronators
(scale)
Wrist flexors
(scale)
Finger flexors
(scale)
1 0.00 0.00 0.00 0.00 1.00 1.00 1.00
2 0.00 1.00 0.00 0.00 0.00 0.00 0.00
3 0.00 1.00 0.00 0.00 0.00 0.00 0.00
4 0.00 0.00 1.50 1.50 0.00 1.50 1.50
5 0.00 1.00 0.00 2.00 0.00 1.50 1.00
6 0.00 0.00 1.00 1.50 0.00 1.50 1.50
7 0.00 0.00 2.00 0.00 0.00 1.50 1.50
8 0.00 0.00 0.00 1.00 1.50 1.00 1.00
9 1.00 2.00 1.50 1.50 1.50 1.50 1.50
10 0.00 1.00 1.50 0.00 0.00 1.00 1.00
11 0.00 1.00 0.00 0.00 0.00 1.00 0.00
12 0.00 1.50 1.50 1.00 0.00 1.00 1.00
13 1.50 0.00 1.00 1.00 0.00 1.50 2.00
14 0.00 0.00 1.00 0.00 0.00 1.00 1.00
15 0.00 1.50 1.00 0.00 0.00 0.00 0.00
16 0.00 1.50 0.00 0.00 0.00 1.50 1.50
17 0.00 0.00 0.00 0.00 0.00 0.00 0.00
18 0.00 0.00 0.00 0.00 0.00 0.00 0.00
19 0.00 0.00 1.00 0.00 0.00 1.00 1.00
20 1.00 0.00 1.00 1.00 0.00 1.00 1.00
21 0.00 1.00 1.50 0.00 0.00 1.50 1.00
22 0.00 1.00 1.00 1.00 0.00 1.50 1.50
23 0.00 0.00 0.00 0.00 0.00 0.00 0.00
24 0.00 1.00 0.00 0.00 0.00 1.00 0.00
25 0.00 0.00 1.00 0.00 0.00 0.00 0.00
26 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Ref. code: 25605812030533ARL

160
Table L15 Revised Nottingham Sensory Assessment at pre-assessment
Item
ID
Light touch
shoulder A
(score)
Light touch
shoulder L
(score)
Light touch
elbow A
(score)
Light touch
elbow L
(score)
Light touch
wrist A
(score)
Light touch
wrist L
(score)
Light touch
hand A
(score)
Light touch
hand L
(score)
Total light
touch
(score)
1 1 2 2 2 0 2 0 2 11
2 2 2 2 2 1 2 1 2 14
3 2 2 2 2 2 2 2 2 16
4 2 2 2 2 2 2 2 2 16
5 1 2 1 2 1 2 1 2 12
6 2 2 2 2 2 2 2 2 16
7 2 2 2 2 2 2 1 2 15
8 2 2 2 2 2 2 2 2 16
9 2 2 2 2 2 2 2 2 16
10 2 2 2 2 2 2 2 2 16
11 2 2 2 2 2 2 2 2 16
12 2 2 2 2 2 2 2 2 16
13 2 2 2 2 2 2 2 2 16
14 2 2 2 2 2 2 2 2 16
15 1 2 1 2 1 2 1 2 12
16 2 2 2 2 2 2 2 2 16
17 2 2 2 2 2 2 2 2 16
18 2 2 2 2 2 2 2 2 16
19 1 2 1 2 1 2 1 2 12
20 2 2 2 2 0 2 0 2 12
21 2 2 2 2 2 2 2 2 16
22 2 2 2 2 2 2 2 2 16
23 2 2 2 2 2 2 2 2 16
24 2 2 2 2 2 2 2 2 16
25 2 2 2 2 1 2 1 2 14
26 2 2 2 2 2 2 2 2 16
A; affected side, L; less affected side
Ref. code: 25605812030533ARL
161
Table L16 Revised Nottingham Sensory Assessment at pre-assessment (continued)
Item
ID
Temperature
shoulder A
(score)
Temperature
shoulder L
(score)
Temperature
elbow A
(score)
Temperature
elbow L
(score)
Temperature
wrist A
(score)
Temperature
wrist L
(score)
Temperature
hand A
(score)
Temperature
hand L
(score)
Total
(score)
1 1 2 1 2 1 2 2 0 11
2 0 1 0 1 0 1 0 1 4
3 2 2 2 2 2 2 2 2 16
4 2 2 2 2 2 2 2 2 16
5 1 2 1 2 1 2 1 2 12
6 1 2 1 2 1 2 0 2 11
7 2 2 2 2 2 2 1 2 15
8 1 2 2 2 2 2 2 2 15
9 2 2 2 2 2 2 2 2 16
10 2 2 2 2 2 2 2 2 16
11 1 2 2 2 2 2 1 2 14
12 1 1 1 1 1 1 1 1 8
13 2 2 2 2 2 2 2 2 16
14 2 2 2 2 2 2 2 2 16
15 1 2 1 2 1 2 1 2 12
16 2 2 2 2 1 2 1 2 14
17 2 2 2 2 2 2 2 2 16
18 2 2 2 2 2 2 2 2 16
19 0 2 0 2 0 2 0 2 8
20 2 2 2 2 2 2 2 2 16
21 2 2 2 2 1 2 1 2 14
22 2 2 2 2 2 2 2 2 16
23 2 2 2 2 2 2 2 2 16
24 2 2 2 2 2 2 2 2 16
25 2 2 2 2 2 2 2 2 16
26 2 2 2 2 2 2 2 2 16
A; affected side, L; less affected side
Ref. code: 25605812030533ARL

162
Table L17 Revised Nottingham Sensory Assessment at pre-assessment (continued)
Item
ID
Pinprick
shoulder A
(score)
Pinprick
shoulder L
(score)
Pinprick
elbow A
(score)
Pinprick
elbow L
(score)
Pinprick
wrist A
(score)
Pinprick
wrist L
(score)
Pinprick
hand A
(score)
Pinprick
hand L
(score)
Total
(score)
1 2 2 0 2 0 2 0 2 10
2 1 2 1 2 0 2 0 2 10
3 2 2 2 2 2 2 2 2 16
4 2 2 2 2 2 2 2 2 16
5 2 2 1 2 2 2 2 2 15
6 2 2 2 2 2 2 2 2 16
7 2 2 2 2 2 2 1 2 15
8 2 2 2 2 2 2 2 2 16
9 2 2 2 2 2 2 2 2 16
10 2 2 2 2 2 2 2 2 16
11 2 2 2 2 2 2 2 2 16
12 2 2 2 2 2 2 2 2 16
13 2 2 2 2 2 2 2 2 16
14 2 2 2 2 2 2 2 2 16
15 0 2 0 2 0 2 0 2 8
16 2 2 2 2 2 2 2 2 16
17 2 2 2 2 2 2 2 2 16
18 2 2 2 2 2 2 2 2 16
19 1 2 1 2 1 2 1 2 12
20 2 2 2 2 1 2 1 2 14
21 2 2 2 2 1 1 1 1 12
22 2 2 2 2 2 2 2 2 16
23 2 2 2 2 2 2 2 2 16
24 2 2 2 2 2 2 2 2 16
25 2 2 2 2 2 2 2 2 16
26 2 2 2 2 2 2 2 2 16
A; affected side, L; less affected side
Ref. code: 25605812030533ARL

163
Table L18 Revised Nottingham Sensory Assessment at pre-assessment (continued)
Item
ID
Tactile
localisation
shoulder A
(score)
Tactile
localisation
shoulder L
(score)
Tactile
localisation
shoulder A
(score)
Tactile
localisation
elbow L
(score)
Tactile
localisation
wrist A
(score)
Tactile
localisation
wrist L
(score)
Tactile
localisation
hand A
(score)
Tactile
localisation
hand L
(score)
Total
(score)
1 2 2 1 2 1 2 0 2 12
2 1 2 0 2 0 2 0 2 9
3 2 2 2 2 2 2 2 2 16
4 2 2 2 2 2 2 2 2 16
5 2 2 2 2 1 2 1 2 14
6 2 2 2 2 2 2 2 2 16
7 2 2 2 2 2 2 1 2 15
8 2 2 2 2 2 2 2 2 16
9 2 2 2 2 2 2 2 2 16
10 2 2 2 2 2 2 2 2 16
11 2 2 2 2 2 2 2 2 16
12 2 2 2 2 2 2 2 2 16
13 2 2 2 2 2 2 2 2 16
14 2 2 2 2 2 2 2 2 16
15 0 2 0 2 0 2 0 2 8
16 2 2 2 2 2 2 2 2 16
17 2 2 2 2 2 2 2 2 16
18 2 2 2 2 2 2 2 2 16
19 2 2 2 2 2 2 2 2 16
20 0 2 0 2 0 2 0 2 8
21 2 2 2 2 2 2 2 2 16
22 2 2 2 2 2 2 2 2 16
23 2 2 2 2 2 2 2 2 16
24 2 2 2 2 2 2 2 2 16
25 2 2 2 2 2 2 2 2 16
26 2 2 2 2 2 2 2 2 16
A; affected side, L; less affected side
Ref. code: 25605812030533ARL

164
Table L19 Revised Nottingham Sensory Assessment at pre-assessment (continued) (score)
ID Bilateral simultaneous touch
shoulder
(score)
Bilateral simultaneous
touch elbow
(score)
Bilateral simultaneous touch
wrist
(score)
Bilateral simultaneous touch
hand
(score)
Total
(score)
Total all
(score)
1 1 1 1 1 4 48
2 1 1 0 0 2 39
3 2 2 2 2 8 72
4 2 2 2 2 8 72
5 2 2 2 2 8 61
6 2 2 2 2 8 67
7 2 2 2 2 8 68
8 2 2 2 2 8 71
9 2 2 2 2 8 72
10 2 2 2 2 8 72
11 2 2 2 2 8 70
12 2 2 2 2 8 64
13 2 2 2 2 8 72
14 2 2 2 2 8 72
15 1 1 1 1 4 44
16 2 2 2 2 8 70
17 2 2 2 2 8 72
18 2 2 2 2 8 72
19 2 2 2 2 8 56
20 2 2 0 0 4 54
21 2 2 2 2 8 66
22 2 2 2 2 8 72
23 1 1 1 1 4 67
24 2 2 2 2 8 72
25 2 2 2 2 8 72
26 2 2 2 2 8 72
Ref. code: 25605812030533ARL

165
Table L20 Revised Nottingham Sensory Assessment at pre-assessment (continued)
Item
ID
Proprioception
shoulder
(score)
Proprioception
elbow
(score)
Proprioception
wrist
(score)
Proprioception
hand
(score)
Total
(score)
1 1 1 0 0 2
2 2 1 1 0 4
3 2 2 2 2 8
4 1 2 2 2 7
5 1 1 0 1 3
6 2 2 2 2 8
7 3 3 3 3 12
8 1 2 2 2 7
9 2 2 1 1 6
10 0 0 0 0 0
11 3 3 3 3 12
12 3 3 3 3 12
13 3 3 3 3 12
14 3 3 3 3 12
15 3 3 2 2 10
16 3 3 3 3 12
17 3 3 3 3 12
18 3 3 3 3 12
19 3 3 2 2 10
20 3 3 3 3 12
21 2 2 3 1 8
22 3 3 3 2 11
23 2 1 1 1 5
24 2 2 2 2 8
25 2 2 2 2 8
26 2 2 2 2 8
Ref. code: 25605812030533ARL

166
Table L21 Revised Nottingham Sensory Assessment at pre-assessment (stereognosis) (continued)
Item
ID
10
Coins
(score)
5
Coins
(score)
1
Coins
(score)
Brio
(score)
Pencil
(score)
Comb
(score)
Scissors
(score)
Sponge
(score)
Flannel
(score)
Cup
(score)
Glass
(score)
Total
(score)
1 0 0 0 0 0 0 0 0 0 0 0 0
2 0 0 0 0 0 0 0 0 0 0 0 0
3 2 2 0 2 2 2 2 2 2 2 2 20
4 2 2 0 0 1 0 0 0 0 1 2 8
5 0 0 0 0 0 0 0 0 0 0 0 0
6 2 2 2 0 2 0 0 0 2 2 2 14
7 0 0 0 2 2 2 0 0 0 0 0 6
8 0 0 0 0 0 0 0 0 2 0 0 2
9 0 0 0 2 2 2 2 2 2 0 0 12
10 2 2 2 2 2 2 2 2 2 2 2 22
11 2 0 0 2 2 2 2 2 2 2 2 18
12 2 2 2 2 2 2 2 2 2 2 2 22
13 0 0 0 0 0 2 2 0 2 2 2 10
14 2 2 0 2 2 2 2 2 2 2 2 20
15 0 0 0 2 2 2 2 2 0 2 2 14
16 0 0 0 0 2 0 2 0 2 2 2 10
17 0 0 0 0 2 0 2 0 2 0 0 6
18 2 2 2 2 2 2 2 2 2 2 2 22
19 0 0 0 2 0 2 0 0 0 0 0 4
20 0 0 0 0 0 0 0 0 0 0 0 0
21 0 0 0 0 0 0 0 0 0 0 0 0
22 0 0 0 0 0 0 0 0 0 0 0 0
23 0 0 0 0 2 0 0 0 0 0 0 2
24 2 0 0 2 2 2 2 0 2 0 0 12
25 2 2 2 0 0 0 0 0 2 2 2 12
26 2 2 2 2 2 2 2 2 2 2 2 22
Ref. code: 25605812030533ARL

167
Table L22 Revised Nottingham Sensory Assessment at post-assessment
Item
ID
Light touch
shoulder A
(score)
Light touch
shoulder L
(score)
Light touch
elbow A
(score)
Light touch
elbow L
(score)
Light touch
wrist A
(score)
Light touch
wrist L
(score)
Light touch
hand A
(score)
Light touch
hand L
(score)
Total light
touch
(score)
1 2 2 2 2 1 1 0 2 12
2 2 2 2 2 1 2 1 2 14
3 2 2 2 2 2 2 2 2 16
4 2 2 2 2 2 2 2 2 16
5 1 2 1 2 1 2 1 2 12
6 2 2 2 2 2 2 2 2 16
7 2 2 2 2 2 2 1 2 15
8 2 2 2 2 2 2 2 2 16
9 2 2 2 2 2 2 2 2 16
10 2 2 2 2 2 2 2 2 16
11 2 2 2 2 2 2 2 2 16
12 2 2 2 2 2 2 2 2 16
13 2 2 2 2 2 2 2 2 16
14 2 2 2 2 2 2 2 2 16
15 2 2 2 2 2 2 2 2 14
16 2 2 2 2 2 2 2 2 16
17 2 2 2 2 2 2 2 2 16
18 2 2 2 2 2 2 2 2 16
19 1 2 1 2 1 2 1 2 12
20 2 2 2 2 2 2 2 2 14
21 2 2 2 2 2 2 2 2 16
22 2 2 2 2 2 2 2 2 16
23 2 2 2 2 2 2 2 2 16
24 2 2 2 2 2 2 2 2 16
25 2 2 2 2 2 2 2 2 16
26 2 2 2 2 2 2 2 2 16
A; affected side, L; less affected side
Ref. code: 25605812030533ARL

168
Table L23 Revised Nottingham Sensory Assessment at post-assessment (continued)
Item
ID
Temperature
shoulder A
(score)
Temperature
shoulder L
(score)
Temperature
elbow A
(score)
Temperature
elbow L
(score)
Temperature
wrist A
(score)
Temperature
wrist L
(score)
Temperature
hand A
(score)
Temperature
hand L
(score)
Total
(score)
1 1 2 1 2 1 2 2 0 11
2 0 1 0 1 0 1 0 1 4
3 2 2 2 2 2 2 2 2 16
4 2 2 2 2 2 2 2 2 16
5 1 2 1 2 1 2 1 2 12
6 1 2 1 2 1 2 0 2 11
7 2 2 2 2 2 2 1 2 15
8 1 2 2 2 2 2 2 2 15
9 2 2 2 2 2 2 2 2 16
10 2 2 2 2 2 2 2 2 16
11 2 2 2 2 2 2 2 2 16
12 2 2 2 2 2 2 2 2 16
13 2 2 2 2 2 2 2 2 16
14 2 2 2 2 2 2 2 2 16
15 1 2 1 2 1 2 1 2 12
16 2 2 2 2 2 2 2 2 16
17 2 2 2 2 2 2 2 2 16
18 2 2 2 2 2 2 2 2 16
19 0 2 0 2 0 2 0 2 8
20 2 2 2 2 2 2 2 2 16
21 2 2 2 2 2 2 2 2 16
22 2 2 2 2 2 2 2 2 16
23 2 2 2 2 2 2 2 2 16
24 2 2 2 2 2 2 2 2 16
25 2 2 2 2 2 2 2 2 16
26 2 2 2 2 2 2 2 2 16
A; affected side, L; less affected side
Ref. code: 25605812030533ARL
169
Table L24 Revised Nottingham Sensory Assessment at post- assessment (continued)
Item
ID
Pinprick
shoulder A
(score)
Pinprick
shoulder L
(score)
Pinprick
elbow A
(score)
Pinprick
elbow L
(score)
Pinprick
wrist A
(score)
Pinprick
wrist L
(score)
Pinprick
hand A
(score)
Pinprick
hand L
(score)
Total
(score)
1 2 2 0 2 0 2 0 2 10
2 1 2 1 2 0 2 0 2 10
3 2 2 2 2 2 2 2 2 16
4 2 2 2 2 2 2 2 2 16
5 2 2 1 2 2 2 2 2 15
6 2 2 2 2 2 2 2 2 16
7 2 2 2 2 2 2 1 2 15
8 2 2 2 2 2 2 2 2 16
9 2 2 2 2 2 2 2 2 16
10 2 2 2 2 2 2 2 2 16
11 2 2 2 2 2 2 2 2 16
12 2 2 2 2 2 2 2 2 16
13 2 2 2 2 2 2 2 2 16
14 2 2 2 2 2 2 2 2 16
15 1 2 2 2 2 2 2 2 15
16 2 2 2 2 2 2 2 2 16
17 2 2 2 2 2 2 2 2 16
18 2 2 2 2 2 2 2 2 16
19 1 2 1 2 1 2 1 2 12
20 2 2 2 2 2 2 2 2 16
21 2 2 2 2 2 2 2 2 16
22 2 2 2 2 2 2 2 2 16
23 2 2 2 2 2 2 2 2 16
24 2 2 2 2 2 2 2 2 16
25 2 2 2 2 2 2 2 2 16
26 2 2 2 2 2 2 2 2 16
A; affected side, L; less affected side
Ref. code: 25605812030533ARL

170
Table L25 Revised Nottingham Sensory Assessment at post- assessment (continued)
Item
ID
Tactile
localisation
shoulder A
(score)
Tactile
localisation
shoulder L
(score)
Tactile
localisation
shoulder A
(score)
Tactile
localisation
elbow L
(score)
Tactile
localisation
wrist A
(score)
Tactile
localisation
wrist L
(score)
Tactile
localisation
hand A
(score)
Tactile
localisation
hand L
(score)
Total
(score)
1 2 2 1 2 1 2 0 2 12
2 1 2 0 2 0 2 0 2 9
3 2 2 2 2 2 2 2 2 16
4 2 2 2 2 2 2 2 2 16
5 2 2 2 2 1 2 1 2 14
6 2 2 2 2 2 2 2 2 16
7 2 2 2 2 2 2 1 2 15
8 2 2 2 2 2 2 2 2 16
9 2 2 2 2 2 2 2 2 16
10 2 2 2 2 2 2 2 2 16
11 2 2 2 2 2 2 2 2 16
12 2 2 2 2 2 2 2 2 16
13 2 2 2 2 2 2 2 2 16
14 2 2 2 2 2 2 2 2 16
15 2 2 2 2 2 2 2 2 16
16 2 2 2 2 2 2 2 2 16
17 2 2 2 2 2 2 2 2 16
18 2 2 2 2 2 2 2 2 16
19 2 2 2 2 2 2 2 2 16
20 0 2 0 2 0 2 0 2 8
21 2 2 2 2 2 2 2 2 16
22 2 2 2 2 2 2 2 2 16
23 2 2 2 2 2 2 2 2 16
24 2 2 2 2 2 2 2 2 16
25 2 2 2 2 2 2 2 2 16
26 2 2 2 2 2 2 1 2 15
A; affected side, L; less affected side
Ref. code: 25605812030533ARL

171
Table L26 Revised Nottingham Sensory Assessment at post- assessment (continued)
Item
ID
Bilateral simultaneous
touch – shoulder
(score)
Bilateral simultaneous
touch – elbow
(score)
Bilateral simultaneous
touch – wrist
(score)
Bilateral simultaneous
touch – hand
(score)
Total
(score)
Total all
(score)
1 1 1 1 1 4 49
2 2 1 0 0 3 40
3 2 2 2 2 8 72
4 2 2 2 2 8 72
5 2 2 2 2 8 61
6 2 2 2 2 8 67
7 2 2 2 2 8 68
8 2 2 2 2 8 71
9 2 2 2 2 8 72
10 2 2 2 2 8 72
11 2 2 2 2 8 72
12 2 2 2 2 8 72
13 2 2 2 2 8 72
14 2 2 2 2 8 72
15 2 2 2 2 8 65
16 2 2 2 2 8 72
17 2 2 2 2 8 72
18 2 2 2 2 8 72
19 2 2 2 2 8 56
20 0 0 0 0 0 56
21 2 2 2 2 8 72
22 2 2 2 2 8 72
23 2 1 1 1 5 69
24 2 2 2 2 8 72
25 2 2 2 2 8 72
26 2 2 2 1 7 70
Ref. code: 25605812030533ARL
172
Table L27 Revised Nottingham Sensory Assessment at post- assessment (continued)
Item
ID
Proprioception
shoulder
(score)
Proprioception
elbow
(score)
Proprioception
wrist
(score)
Proprioception
hand
(score)
Total
(score)
1 2 1 0 0 3
2 2 2 1 0 5
3 3 3 3 3 12
4 2 2 2 2 8
5 3 3 2 1 9
6 3 3 3 3 12
7 2 2 2 2 8
8 1 2 2 2 7
9 2 2 2 1 7
10 3 3 3 3 12
11 2 2 2 2 8
12 3 3 3 3 12
13 3 3 3 3 12
14 3 3 3 3 12
15 3 3 3 3 12
16 3 3 3 3 12
17 3 3 3 3 12
18 3 3 3 3 12
19 3 3 2 2 10
20 2 2 2 2 8
21 3 3 3 3 12
22 3 3 3 3 12
23 2 2 2 2 8
24 2 2 2 2 8
25 3 3 3 3 12
26 3 3 3 3 12
Ref. code: 25605812030533ARL

173
Table L28 Revised Nottingham Sensory Assessment at post- assessment (stereognosis) (continued)
Item
ID
10 Coins
(score)
5 Coins
(score)
1 Coins
(score)
Brio
(score)
Pencil
(score)
Comb
(score)
Scissors
(score)
Sponge
(score)
Flannel
(score)
Cup
(score)
Glass
(score)
Total
(score)
1 0 0 0 0s 0 0 0 0 0 0 0 0
2 0 0 0 0 0 0 0 0 0 0 0 0
3 2 2 2 2 2 2 2 2 2 2 2 22
4 2 2 2 1 1 0 0 0 0 2 2 12
5 0 0 0 0 0 0 0 0 0 0 0 0
6 0 0 0 0 0 0 0 0 0 0 0 0
7 0 0 0 2 2 2 0 0 0 0 0 6
8 0 0 0 0 0 0 0 0 0 0 0 0
9 0 0 0 2 2 2 2 2 2 0 0 12
10 2 2 2 2 2 2 2 2 2 2 2 22
11 2 2 2 2 2 0 2 2 2 2 2 20
12 2 2 2 2 2 2 2 2 2 2 2 22
13 0 0 0 0 2 2 2 0 2 2 2 12
14 2 2 0 2 2 2 2 2 2 2 2 20
15 2 2 2 2 2 2 2 2 2 2 2 22
16 2 2 2 2 2 2 2 2 2 2 2 22
17 2 2 2 2 2 2 2 2 2 2 2 22
18 2 2 2 2 2 2 2 2 2 2 2 22
19 0 0 0 2 0 2 0 0 0 0 0 4
20 0 0 0 0 0 0 2 0 0 0 2 4
21 0 0 0 2 2 2 2 0 2 2 2 14
22 0 0 2 2 2 0 2 0 2 2 2 14
23 0 0 0 0 2 0 0 0 0 0 0 2
24 2 2 0 2 2 2 2 0 2 0 0 14
25 2 2 2 0 0 0 0 0 2 2 2 12
26 2 2 2 2 2 2 2 2 2 2 2 22
Ref. code: 25605812030533ARL

174
APPENDIX M
Results
Comparison between moderate and severe level of severity
Table M1 Comparison of the Wolf Motor Function Test (movement time) of the
affected side between moderate and severe level of severity (pre- and post-
assessment)
*P-value < 0.05
Calculated by the Mann-Whitney U test
Item
Mean ± SD
(seconds)
p-value
Moderate level
(n=13)
Severe level
(n=13)
1 Forearm to table 0.55 ± 0.54 8.51 ± 25.27 0.011*
2 Forearm to box 0.16 ± 1.03 3.72 ± 4.96 0.017*
3 Extend elbow (side) 25.88 ± 48.16 9.24 ± 56.54 0.359
4 Extend elbow (weight) 19.95 ± 42.08 16.88 ± 38.87 0.388
5 Hand to table 0.26 ± 0.77 10.35 ± 25.27 0.017*
6 Hand to box 9.69 ± 32.73 28.56 ± 50.96 0.270
8 Reach and retrieve 0.73 ± 1.57 54.22 ± 58.37 0.045*
9 Lift can 25.80 ± 46.74 18.07 ± 14.11 0.242
10 Lift pencil 17.82 ± 11.54 29.18 ± 46.73 0.729
11 Lift paper clip 47.78 ± 55.08 8.44 ± 30.43 0.009*
12 Stack checkers 16.68 ± 38.32 0.00 ± 0.00 0.221
13 Flip card 29.82 ± 44.04 5.65 ± 20.39 0.125
15 Turn key in lock 22.93 ± 38.94 11.83 ± 30.97 0.199
16 Fold towel 42.65 ± 44.19 33.40 ± 42.22 0.154
17 Lift basket 27.40 ± 42.48 34.23± 47.26 0.846
Total 10.90 ± 3.03 10.93 ± 3.03 0.689
Ref. code: 25605812030533ARL
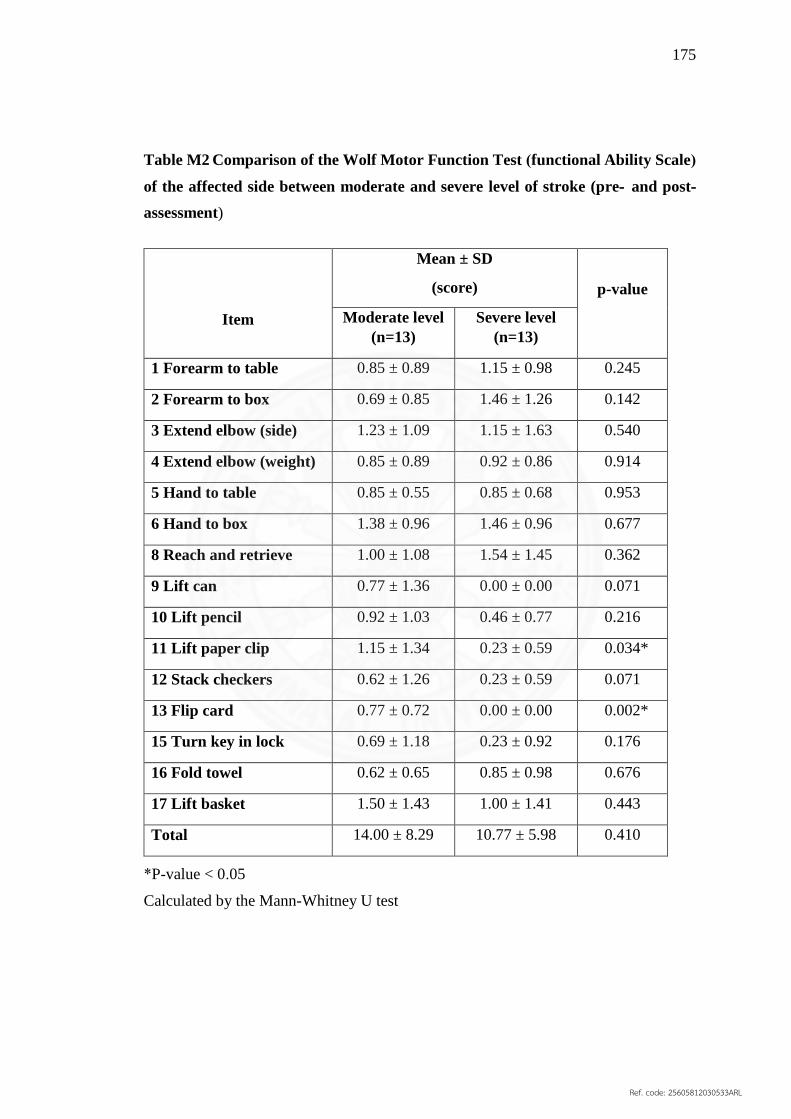
175
Table M2 Comparison of the Wolf Motor Function Test (functional Ability Scale)
of the affected side between moderate and severe level of stroke (pre- and post-
assessment)
Item
Mean ± SD
(score)
p-value
Moderate level
(n=13) Severe level
(n=13)
1 Forearm to table 0.85 ± 0.89 1.15 ± 0.98 0.245
2 Forearm to box 0.69 ± 0.85 1.46 ± 1.26 0.142
3 Extend elbow (side) 1.23 ± 1.09 1.15 ± 1.63 0.540
4 Extend elbow (weight) 0.85 ± 0.89 0.92 ± 0.86 0.914
5 Hand to table 0.85 ± 0.55 0.85 ± 0.68 0.953
6 Hand to box 1.38 ± 0.96 1.46 ± 0.96 0.677
8 Reach and retrieve 1.00 ± 1.08 1.54 ± 1.45 0.362
9 Lift can 0.77 ± 1.36 0.00 ± 0.00 0.071
10 Lift pencil 0.92 ± 1.03 0.46 ± 0.77 0.216
11 Lift paper clip 1.15 ± 1.34 0.23 ± 0.59 0.034*
12 Stack checkers 0.62 ± 1.26 0.23 ± 0.59 0.071
13 Flip card 0.77 ± 0.72 0.00 ± 0.00 0.002*
15 Turn key in lock 0.69 ± 1.18 0.23 ± 0.92 0.176
16 Fold towel 0.62 ± 0.65 0.85 ± 0.98 0.676
17 Lift basket 1.50 ± 1.43 1.00 ± 1.41 0.443
Total 14.00 ± 8.29 10.77 ± 5.98 0.410
*P-value < 0.05
Calculated by the Mann-Whitney U test
Ref. code: 25605812030533ARL

176
Table M3 Comparison of the Fugl- Meyer assessment of the upper extremity
between moderate and severe level of stroke (pre- and post-assessment)
Item
Mean ± SD
(score)
p-value
Moderate level
(n=13)
Severe level
(n=13)
Upper extremity
- A1 Reflex activity
0.00 ± 0.00 0.00 ± 0.00 1.000
- A2 Volitional movement
within synergies
4.08 ± 2.81 3.92 ± 4.71 0.757
- A3 Volitional movement
mixing synergies
1.46 ± 1.45 1.54 ± 1.05 0.496
- A4 Volition movement with
little or no synergy
1.69 ± 1.37 0.92 ± 1.15 0.113
- A5 Normal reflex activity 0.54 ± 0.87 0.00 ± 0.70 0.118
- B Wrist
Stability at 15°
dorsiflexion
Repeated
dorsiflexion/ volar
flexion
Circumduction
3.08 ± 2.78 2.15 ± 2.60 0.361
- C Hand
Mass
flexion/extension
Grasp
2.69 ± 2.59 3.54 ± 4.03 0.588
- D Coordinate/Speed 0.67 ± 1.30 0.83 ± 1.47 0.922
Total 14.23 ± 7.80 12.69 ± 11.60 0.650
*P-value < 0.05
Calculated by the Mann-Whitney U test
Ref. code: 25605812030533ARL

177
Table M4 Comparison of the Modified Ashworth Scale between moderate and
severe level of stroke (pre- and post-assessment)
Muscle
Mean ± SD
(scale)
p-value Moderate
level (n=13)
Severe level
(n=13)
Shoulder internal rotators 0.08 ± 0.28 0.00 ± 0.00 0.317
Shoulder adductors 0.19 ± 0.48 0.12 ± 0.22 0.794
Elbow flexors 0.12 ± 0.42 0.23 ± 0.63 0.693
Elbow extensors 0.04 ± 0.14 0.15 ± 0.32 0.015*
Pronators 0.08 ± 0.28 0.00 ± 0.61 0.611
Wrist flexors 0.19 ± 0.38 0.19 ± 0.43 0.945
Finger flexors 0.00 ± 0.20 0.30 ± 0.43 0.038*
*P-value < 0.05
Calculated by the Mann-Whitney U test
Ref. code: 25605812030533ARL

178
Table M5 Comparison of the Revised Nottingham Sensory assessment between
moderate and severe level of stroke (pre- and post-assessment)
Item
Mean ± SD
(score)
p-value Moderate
level (n=13)
Severe level
(n=13)
Tactile sensation
Light touch
0.46 ± 1.12
0.46 ± 1.19
0.972
Temperature 0.15 ± 0.55 0.92 ± 0.25 0.270
Pinprick 0.15 ± 0.55 0.85 ± 2.15 0.488
Tactile localization 0.24 ± 0.59 0.30 ± 0.75 0.497
Bilateral Simultaneous
touch
0.00 ± 0.40 0.38 ± 1.12 0.180
All 0.38 ± 1.12 2.92 ± 6.02 0.363
Proprioception 0.08 ± 2.75 2.69 ± 3.42 0.054
Stereognosis 1.85 ± 4.36 4.00 ± 5.88 0.762
*P-value < 0.05
Calculated by the Mann-Whitney U test
Ref. code: 25605812030533ARL

179
BIOGRAPHY
Name Miss Thanchanok Pumprasart
Date of Birth December 20, 1993
Educational Attainment 2014: Bachelor of Science
(Physical Therapy)
Thammasat University
Ref. code: 25605812030533ARL
![Constraining upper limb synergies of hemiparetic patients ... · shoulder subluxation. The compared effectiveness of Bobath and Motor Relearning approaches is still disputed [47],](https://img.pdfslide.net/doc/110x75/5e73ff5fd131a95cf01e4a13/constraining-upper-limb-synergies-of-hemiparetic-patients-shoulder-subluxation.jpg)