Embed Size (px)
Citation preview

Effect of whole grains on markers of subclinical inflammation
Michael Lefevre and Satya Jonnalagadda
The reduction of subclinical inflammation has been suggested as a potentialmechanism to explain the favorable association between whole-grain consumptionand reduced risk for cardiovascular disease, diabetes, and certain cancers. Thisreview examines evidence for the effects of whole-grain consumption on markers ofsubclinical inflammation derived from 13 epidemiological and 5 interventionalstudies retrieved from a search of the PubMed database. Epidemiological studiesprovide reasonable support for an association between diets high in whole grainsand lower C-reactive protein (CRP) concentrations. After adjusting for other dietaryfactors, each serving of whole grains is estimated to reduce CRP concentrations byapproximately 7%. In contrast to epidemiological studies, interventional studies donot demonstrate a clear effect of increased whole-grain consumption on CRP orother markers of inflammation. Issues related to insufficient length of intervention,extent of dietary control, population selection, types of whole grains, and lack of adirect anti-inflammatory effect may underlie these discrepant findings. Additionalcarefully controlled interventional studies are needed to clarify the effects of wholegrains on subclinical inflammation.© 2012 International Life Sciences Institute
INTRODUCTION
There is a substantial body of evidence supporting theassociation between higher whole-grain consumptionand reduced risk for the development of major chronicdiseases. Prospective population studies show that indi-viduals who consume diets higher in whole grains have areduced risk of developing cardiovascular disease,1–9 type2 diabetes,10–14 and certain types of cancer.15–17 Based inpart on these favorable epidemiological findings, the USDepartment of Agriculture,18 the American Heart Asso-ciation,19 and the American Diabetes Association20 haverecommended increased consumption of whole-grainfoods.
The mechanisms by which whole grains exert theirbeneficial effects are not fully elucidated. However, therecognition that subclinical inflammation is associatedwith cardiovascular disease21 and type 2 diabetes22,23 hasprompted investigations into the direct relationshipbetween whole-grain intake and markers of subclinical
inflammation. Below, the evidence linking whole-grainconsumption and subclinical inflammation is reviewed.
SELECTION OF STUDIES FOR REVIEW
The PubMed database was searched (last search, May2011) using the search string “(whole OR unrefined ORbrown) AND (grain* OR cereal* OR wheat OR oat* ORrye OR corn OR rice) AND (inflammat* OR CRP ORC-reactive protein OR interleukin-6 OR IL-6) ANDhuman*.” The search yielded a total of 98 references. Theretrieved articles were downloaded into a reference man-agement database and the abstracts were reviewed forrelevance. Only those studies that specifically examinedwhole grains in either epidemiological surveys (cross-sectional or prospective) or in dietary interventions wereselected. Studies that primarily focused on whole-grainfractions such as fiber and/or bran products wereexcluded. Relevant papers were retrieved and their
Affiliations: M Lefevre is with the Department of Nutrition, Dietetics and Food Science, Utah State University, 9815 Old Main Hill, Logan,Utah, USA. S Jonnalagadda is with the General Mills Bell Institute of Health and Nutrition, Golden Valley, Minnesota, USA.
Correspondence: M Lefevre, Department of Nutrition, Dietetics and Food Science, Utah State University, 9815 Old Main Hill, Logan, UT84322-9815, USA. E-mail: [email protected], Phone: +1-435-797-3821, Fax: +1-435-797-8117.
Key words: C-reactive protein, inflammation, interleukin-6, whole grains
bs_bs_banner
Special Article
doi:10.1111/j.1753-4887.2012.00487.xNutrition Reviews® Vol. 70(7):387–396 387

bibliographies were scanned to identify additional articlesthat may have been missed in the initial search. A total of13 epidemiological studies24–36 and 5 interventionalstudies were reviewed.37–41 Within the epidemiologicalstudies, a number of papers represented different analy-tical approaches or subpopulations using the samestudy population, including the Health ProfessionalsFollow-Up Study,24,28 the Nurses’ Health Study,25,33 andthe Multi-Ethnic Study of Atherosclerosis.29,32,34
MARKERS OF SUBCLINICAL INFLAMMATION
Epidemiological and interventional studies have used anumber of circulating proteins as markers of subclinicalinflammation, including C-reactive protein (CRP),interleukin-6 (IL-6), fibrinogen, tumor necrosis factor-a(TNF-a), and TNF-a receptor-1 and receptor-2. Of these,CRP is most commonly measured, followed by IL-6. CRPis an acute-phase protein secreted by the liver in responseto IL-6.42 Elevated concentrations of CRP are associatedwith increased risk for cardiovascular disease,43,44 insulinresistance and type 2 diabetes,45 and some cancers.44
Similarly, elevated IL-6 concentrations are associatedwith increased risk for both cardiovascular disease46
and type 2 diabetes.23 A substantial amount of IL-6 is
produced by abdominal adipose tissue, which, in part,explains the relationship between obesity and subclinicalinflammation.23,47
DEFINING WHOLE-GRAIN FOODS
The FDA states that “cereal grains that consist of theintact, ground, cracked or flaked caryopsis [kernel],whose principal anatomical components – the starchyendosperm, germ, and bran – are present in the samerelative proportions as they exist in the intact caryopsis –should be considered a whole grain.”48 This definitionallows for the grain to undergo processing, including thetemporary separation of the individual components, aslong as the final product contains the germ, endosperm,and bran in virtually the same proportion as the originalgrain. This definition differs from the operational defini-tion of whole-grain foods used in epidemiological studiesto estimate population intakes (Table 1). Because of thelimitations associated with the range and description offood items contained within a food frequency question-naire, items that do not meet the definition of a wholegrain (e.g., wheat germ, wheat bran) or that may have verylow or no whole-grain content (e.g., high-fiber breads andcereals) may be included in estimates of whole-grainintake. Conversely, other whole-grain items that may be
Table 1 Definitions used to quantify whole-grain foods and serving sizes.Study Serving definition Whole-grain foods
definitionIRAS36 One serving defined as a
participant-identified, medium-sizedserving of FFQ line items comparable toservings consumed by men or women ofthe same age
Dark bread (including whole-wheat, rye, pumpernickel,and other high-fiber bread); high-fiber bran orgranola cereals, shredded wheat; cooked cereal(including oatmeal, Cream of Wheat®, and grits)weighted by a factor of 0.5
MESA32 Patterned after the IRAS study Cold cereal containing � 3 g dietary fiber per 100 g dryweight; oatmeal; dark, whole-grain breads or rolls;bran muffins; brown or wild rice
BioCycle35 A whole-grain serving defined as a 16 g or½ cup of a 100% whole-grain food
A food product in which a whole-grain ingredient wasthe first ingredient on the food label; productscontaining only some whole grains were notincluded
IWHS9 Commonly used serving size Dark bread; cold breakfast cereal with � 25% wholegrain or bran by weight; brown rice; popcorn; wheatgerm; bran; cooked oatmeal, and other grains(bulgur, kasha, and couscous)
NHS25,33/HPFS24,28 Whole-grain intake reported in g/day,based on commonly used portion sizeand estimated percent whole-graincontent derived from analysis of recipesand ingredient data
All foods that, based on analysis of average recipes andingredient labels, contained any of the following:whole wheat and whole-wheat flour, whole oats andwhole-oat flour, whole cornmeal and corn flour,brown rice and brown rice flour, whole barley, wholerye and rye flour, bulgur, buckwheat, popcorn,amaranth, and psyllium
Abbreviations: FFQ, food frequency questionnaire; HPFS, Health Professionals Follow-Up Study; IRAS, Insulin Resistance AtherosclerosisStudy; IWHS, Iowa Women’s Health Study; MESA, Multi-Ethnic Study of Atherosclerosis; NHS, Nurses’ Health Study.
Nutrition Reviews® Vol. 70(7):387–396388

frequently (popcorn) or infrequently (bulgur/crackedwheat, kasha/buckwheat, barley) consumed are notincluded in other estimates. This poses challenges in iden-tifying and quantifying the true effects of whole-grainintake on measured outcomes.
COHORT STUDIES WITH DIETARY PATTERNS HIGHIN WHOLE GRAINS
The study of dietary patterns provides a comprehensiveapproach to the examination of the effects of diet onindices of health and disease. These dietary patterns caneither be derived de novo from the diet intake data usingprincipal components factor analysis (PCA) and reduced-ranked regression or be specified a priori on the basis of apre-established dietary pattern (e.g., Dietary Approachesto Stop Hypertension [DASH] diet or Mediterraneandiet). Of the five studies that derived dietary patterns denovo from the diet intake data, four showed reductions inCRP with increasing intake of a dietary pattern containingwhole grains (Table 2). A study conducted in a subset of732 women in the Nurses’ Health Study25 demonstrated asignificant (P = 0.02) inverse association between plasmaconcentrations of CRP and adherence to a dietary patternderived by PCA and characterized by higher intakes ofwhole grains, fruits, vegetables, legumes, fish, and poultry.Similarly, a study of 5,089 participants in the Multi-EthnicStudy of Atherosclerosis29 identified a dietary pattern byPCA that was characterized by higher intakes of whole-grain bread, rice and pasta, fruit, seeds, nuts and peanutbutter, green leafy vegetables, and low-fat milk. Those inthe upper quintile for consumption of this dietary patternhad a mean CRP concentration 21% lower than those inthe lowest quintile of intake (P < 0.001 for trend).A studyconducted in 486 Iranian women31 found that those whowere in the highest quintile for consumption of a dietarypattern identified by PCA and characterized by increasedintake of whole grains, fruits, vegetables, tomatoes,poultry, legumes, cruciferous and green leafy vegetables,tea, and fruit juices had a mean CRP concentration 29%lower (P < 0.01 for trend) than those in the lowest quintileof consumption.
Using a somewhat different approach, Hoffmannet al.26 derived a dietary pattern by reduced-rankedregression using 49 food groups on a food frequencyquestionnaire as potential predictor variables andlow-density lipoprotein cholesterol, high-density lipopro-tein cholesterol, lipoprotein(a), CRP, and C-peptide asresponse variables. The data were derived from a popula-tion of 200 women with incident coronary artery diseaseand 255 age-matched controls. In the derived dietarypattern score, meat, poultry, margarine, vegetable fats andoils (except olive oil), and sauces were positively weighted,while vegetarian dishes, wine, cooked and raw vegetables,
and whole-grain cereals and muesli were negativelyweighted. With increasing quintiles of the dietaryscore, whole-grain cereal and muesli consumption signifi-cantly (P < 0.0001) decreased from 12 g/day to 4 g/day(1st versus 5th quintile), and CRP concentrations signifi-cantly (P < 0.0001) increased from 7 mg/L to 32 mg/L.
Similarly favorable effects of prespecified dietary pat-terns containing whole grains have been demonstrated(Table 2). Thus, individuals consuming diets with thegreatest characteristics of the DASH diet (increasedwhole grains, fruits, vegetables, nuts, legumes, low-fatdairy),33 Mediterranean diet (increased nonrefinedcereals and products, fruit, vegetables, olive oil, potatoes,fish),30 a “Comprehensive Healthy Dietary Pattern”(higher in whole-grain bread, rice, cereal or pasta, fruit,seeds and nuts),34 or who had a higher “RecommendedFood Score” (higher in low-fat whole grains, low-fat dairy,lean meats, poultry, fish)27 had plasma CRP concentra-tions that were approximately 10–20% lower in thehighest versus the lowest quantile.
A number of these studies also examined effects onother markers of inflammation, including IL-6 andfibrinogen. Effects of increased consumption of diets richin whole grains on these endpoints were slightly less con-sistent than the effects on CRP; for IL-6 concentrations,three studies29,33,34 showed significant reductions and twostudies25,31 showed no effect, while for fibrinogen, onestudy30 showed a favorable effect of dietary patterns richin whole grains and another study34 showed no effect.
Four studies examined the strength of the associationbetween dietary patterns and CRP concentrations beforeand after covariate adjustments for indices of adiposity,with three studies29,31,34 showing a weakened associationand the other25 a strengthened association. A weakeningin the association between a dietary pattern and CRPconcentrations would be consistent with at least part ofthe effects of the dietary pattern being mediated throughchanges in adiposity and/or adipose tissue metabolism.
Combined, these studies suggest that dietary patternsthat include whole grains are associated with significantreductions in CRP concentrations and other markers ofinflammation. Further, when comparing extremes inintakes of dietary patterns rich in whole grains, the extentof reduction in CRP is on the order of 10–29%. However,because these are complex dietary patterns containingmany foods that have the potential to exert anti-inflammatory effects, the extent to which the observedreductions can be specifically attributable to whole-grainconsumption cannot be stated with certainty.
COHORT STUDIES OF WHOLE GRAINS
Four studies have specifically examined the associationbetween whole-grain intake and markers of subclinical
Nutrition Reviews® Vol. 70(7):387–396 389

Tabl
e2
Sum
mar
yof
coho
rtst
udie
sex
amin
ing
the
effec
tsof
diet
ary
patt
erns
high
inw
hole
grai
nson
CRP
conc
entr
atio
ns.
Refe
renc
eCo
untr
yCo
hort
Sex
and
no.
ofsu
bjec
tsD
ieta
rypa
tter
nw
ithw
hole
grai
nsa
Mod
elad
just
men
tsCR
Pou
tcom
eac
ross
leve
lsof
diet
ary
patt
erns
d
Base
mod
elb
Adip
osity
c
Fung
etal
.(20
01)24
USA
HPF
SM
=46
6Pr
uden
tdie
tfac
tore
XX
NS
tren
dac
ross
quin
tiles
;NS
regr
essi
onco
effici
ent
Lope
z-G
arci
aet
al.(
2004
)25U
SAN
HS
F=
732
Prud
entd
ietf
acto
reX
P=
0.05
forn
egat
ive
tren
dac
ross
quin
tiles
;N
Sre
gres
sion
coeffi
cien
tX
XP
=0.
02fo
rreg
ress
ion
coeffi
cien
t(b
=-0
.10)
Hoff
man
net
al.
(200
4)26
Ger
man
yCO
RAF
=45
5CA
Ddi
etfa
ctor
fX
P<
0.00
01fo
rpos
itive
tren
dac
ross
quin
tiles
Net
tleto
net
al.
(200
6)29
USA
MES
AM
=2,
407
Who
legr
ains
and
frui
tfac
tore
XP
<0.
001
forn
egat
ive
tren
dac
ross
quin
tiles
;P<
0.05
forr
egre
ssio
nco
effici
ent(
b=
-0.0
89)
F=
2,68
2X
XP
<0.
05fo
rreg
ress
ion
coeffi
cien
t(b
=-0
.060
)Es
mai
llzad
ehet
al.
(200
7)31
Iran
F=
486
Hea
lthy
patt
ern
fact
ore
XP
<0.
01fo
rneg
ativ
etr
end
acro
ssqu
intil
es;P
<0.
001
forr
egre
ssio
nco
effici
ent(
b=
-0.0
90)
XX
P<
0.05
forn
egat
ive
tren
dac
ross
quin
tiles
;P=
0.01
1fo
rreg
ress
ion
coeffi
cien
t(b
=-0
.050
)Ka
ntet
al.(
2005
)27U
SAN
HAN
ESIII
M=
4,30
2F
=4,
358
Reco
mm
ende
dfo
odsc
oree
XX
P=
0.02
forn
egat
ive
tren
dac
ross
quar
tiles
Pana
giot
akos
etal
.(2
006)
30G
reec
eAT
TICA
M=
1,51
4M
edite
rran
ean
scor
eeX
P<
0.00
1fo
rreg
ress
ion
coeffi
cien
t(b
=-0
.27)
F=
1,52
8N
ettle
ton
etal
.(2
008)
34U
SAM
ESA
M+
F=
5,04
2H
ealth
ypa
tter
nsc
oree
XP
<0.
001
forn
egat
ive
tren
dac
ross
quin
tiles
XX
P=
0.04
forn
egat
ive
tren
dac
ross
quin
tiles
Fung
etal
.(20
08)33
USA
NH
SF
=1,
176
DAS
Hsc
oree
XP
=0.
008
forn
egat
ive
tren
dac
ross
quin
tiles
a“F
acto
r”de
sign
ates
anal
yses
empl
oyin
gpr
inci
palc
ompo
nent
sor
redu
ced-
rank
edre
gres
sion
tode
rive
diet
ary
patt
erns
;“sc
ore”
desi
gnat
esan
alys
esem
ploy
ing
pres
peci
fied
diet
ary
fact
ors.
bIn
clud
esad
just
men
tsfo
rany
ofth
efo
llow
ing:
age,
sex,
race
,edu
catio
n,sm
okin
gst
atus
,ene
rgy
inta
ke,p
hysi
cala
ctiv
ity,a
lcoh
olco
nsum
ptio
n,bl
ood
pres
sure
,cho
lest
erol
conc
entr
atio
ns,
supp
lem
entu
se.
cIn
clud
esad
just
men
tsfo
rany
ofth
efo
llow
ing:
body
mas
sin
dex,
wai
stci
rcum
fere
nce.
dN
S,no
nsig
nific
ant.
eW
hole
-gra
inin
take
incr
ease
sw
ithin
crea
sing
quan
tile
ofsc
ore
orfa
ctor
.fW
hole
-gra
inin
take
decr
ease
sw
ithin
crea
sing
quan
tile
ofsc
ore
orfa
ctor
.Ab
brev
iatio
ns:C
ORA
,Cor
onar
yRi
skFa
ctor
forA
ther
oscl
eros
isin
Wom
en;C
AD,c
oron
ary
arte
rydi
seas
e;CR
P,C-
reac
tive
prot
ein;
HPF
S,H
ealth
Prof
essi
onal
sFo
llow
-Up
Stud
y;M
ESA,
Mul
ti-Et
hnic
Stud
yof
Athe
rosc
lero
sis.
NH
ANES
,Nat
iona
lHea
lthan
dN
utrit
ion
Exam
inat
ion
Surv
ey;N
HS,
Nur
ses’
Hea
lthSt
udy.
Nutrition Reviews® Vol. 70(7):387–396390

inflammation (Table 3). As previously mentioned, thedefinitions for whole-grain foods for inclusion in theanalyses differed with each study. Nonetheless, in all fourstudies, in the least-adjusted statistical model, increasedconsumption of whole-grain foods was associated witha significant reduction in CRP concentrations rangingfrom 11% to 29% in a comparison of the first and lastquantiles of whole-grain intake.28,32,35,36 However, consis-tent with the dietary patterns analysis, individuals withhigher whole-grain intakes generally had a healthier life-style, variably characterized by less smoking, lower bodymass index (BMI), increased physical activity, increasedfruit and vegetable intake, and decreased alcohol, satu-rated fat, and/or meat intake – not all of which wereconsidered in the base statistical model. Consequently,after correcting for differences in BMI, waist circumfer-ence, and/or markers of insulin sensitivity or for otherdietary components, including fruit, vegetables, refinedgrains, fiber, meat, and/or dietary fatty acids, the degree ofassociation between whole-grain intake and CRP concen-trations was substantially weakened32,36 or became statis-tically nonsignificant.28,35 Further, when both measures ofadiposity/insulin resistance and confounding dietaryvariables were included in the model, no study revealed asignificant independent effect of whole grains on CRPconcentrations.
Similar results were found with other markers ofinflammation. Two studies examined the associationbetween whole-grain consumption and IL-6 concentra-tions, of which one showed no association28 and the othershowed a significant inverse association with the basemodel, but not for more fully adjusted models.32 Twostudies28,36 also examined fibrinogen concentrations, withneither showing any significant association with whole-grain intake.
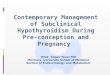
To obtain a quantitative estimate of the effect of asingle serving of whole grains on CRP concentrations,published beta coefficients relating servings of whole-grain intake to log-transformed CRP concentrations wereused. If beta coefficients were not provided, these valueswere estimated by regression analysis using quantilevalues for whole-grain intake and CRP concentrations.Whole-grain intake data expressed as grams per daywere converted to servings per day by assuming thatone whole-grain serving corresponded to 16 g of wholegrains. Beta coefficients for the minimally adjustedbase, diet-adjusted, adiposity/insulin resistance-adjusted,and/or fully adjusted models were included in a least-squares model that included whole-grain intake, study,and model adjustments as predictor variables. Data wereweighted by the inverse of variance estimated for the betacoefficients.
The results of this analysis appear in Figure 1 andshow that in the minimally adjusted model, each addi-
tional serving of whole grains reduces CRP concentra-tions by approximately 10%. As previously noted, whole-grain intake is associated with a healthier dietary pattern.Therefore, it is not surprising that after correction of anyof a number of dietary covariates, the effect of wholegrains is attenuated such that each additional serving isassociated with a 7% reduction in CRP concentrations.
Adjustment of the model for measures of adiposityand/or insulin resistance further attenuates the effect ofan additional serving of whole grains by approximately40%, whether measured from the base or the diet-adjusted model. However, unlike adjustments for dietarycovariates that serve to isolate the “true effect” of wholegrains on CRP concentrations, adjustments for measuresof adiposity in combination with insulin resistanceprovide information regarding potential mechanisms.Increased intake of whole grains is associated withreduced BMI and adiposity49 and improved insulinsensitivity,50,51 both of which have been shown to be asso-ciated with lower CRP concentrations.52–54 Thus, approxi-mately 40% of the improvement in CRP concentrationsassociated with increased whole-grain consumption maybe due to the favorable effect of whole grain on adiposityand insulin sensitivity.
INTERVENTIONAL STUDIES
In contrast to epidemiological studies, in which favorableeffects of whole-grain consumption on inflammation aregenerally observed, data from interventional studies aremuch less conclusive. Of the five studies that specificallyexamined the effects of increased whole-grain intake,only one showed a significant favorable effect on CRPconcentrations.
Andersson et al.37 studied 30 participants (22 post-menopausal women and 8 men) between the ages of 35and 70 years with at least one physiological marker ofinsulin resistance. Participants were instructed to includea fixed amount of refined-grain or whole-grain foods(112 g/day) in their habitual diet for a period of 6 weekseach, in a crossover design. The whole grains were amixture of wheat, rye, oats, and rice, with wheat predomi-nating. Relative to the end of the refined-grain period,consumption of whole grains was associated with a smallbut statistically significant increase in BMI, no change ininsulin sensitivity, and no change in either CRP or IL-6concentrations.
Similar results were observed in a smaller study ofshorter duration. Fifteen participants (3 women, 12 men)with a mean age of 55 years and a mean BMI of27.4 kg/m2 were instructed to include refined- or whole-grain wheat products into their habitual diet for a periodof 3 weeks each. No significant effects of inclusion of
Nutrition Reviews® Vol. 70(7):387–396 391

Tabl
e3
Sum
mar
yof
coho
rtst
udie
sex
amin
ing
effec
tsw
hole
grai
nson
CRP
conc
entr
atio
nsin
heal
thy
adul
ts.
Refe
renc
eCo
hort
Sex
and
no.
ofsu
bjec
tsW
hole
-gra
inin
take
(firs
tver
sus
last
quan
tile)
Mod
elad
just
men
tsO
utco
med
Base
mod
ela
Adip
osity
/insu
linre
sist
ance
bD
ietc
Jens
enet
al.
(200
6)28
HPF
S&
NH
SII
M=
468
8.2
vers
us43
.8g/
day
XP
=0.
03fo
rneg
ativ
etr
end
acro
ssqu
intil
esF
=47
0X
XN
Str
end
acro
ssqu
intil
esX
XX
NS
tren
dac
ross
quin
tiles
Luts
eyet
al.
(200
7)32
MES
AM
+F
=5,
496
0.02
vers
us1.
39se
rvin
gs/d
ayX
P<
0.00
01fo
rneg
ativ
etr
end
acro
ssqu
intil
es
XX
P=
0.00
4fo
rneg
ativ
etr
end
acro
ssqu
intil
esX
XX
NS
tren
dac
ross
quin
tiles
Mas
ters
etal
.(2
010)
36IR
ASM
+F
=94
00.
04ve
rsus
2.00
serv
ings
/day
XP
=0.
0181
forr
egre
ssio
nco
effici
ent(
b=
-0.1
03)
XX
P<
0.03
4fo
rreg
ress
ion
coeffi
cien
t(b
=-0
.102
)X
XX
NS
forr
egre
ssio
nco
effici
ent(
b=
-0.0
36)
Gas
kins
etal
.(2
010)
35Bi
oCyc
leF
=24
9N
one
vers
us1.
6se
rvin
gs/d
ayX
P=
0.04
com
parin
gno
neve
rsus
�1
serv
ing/
day
XX
NS
com
parin
gno
neve
rsus
�1
serv
ing/
day
aIn
clud
esad
just
men
tsfo
rany
ofth
efo
llow
ing:
age,
sex,
race
,edu
catio
n,sm
okin
gst
atus
,ene
rgy
inta
ke,p
hysi
cala
ctiv
ity,a
lcoh
olco
nsum
ptio
n,ch
oles
tero
lcon
cent
ratio
ns.
bIn
clud
esad
just
men
tsfo
rany
ofth
efo
llow
ing:
BMI,
wai
stci
rcum
fere
nce,
insu
linco
ncen
trat
ions
,ins
ulin
sens
itivi
ty(S
i),2h
-pos
tpra
ndia
lglu
cose
.c
Incl
udes
adju
stm
ents
fora
nyof
the
follo
win
gin
take
s:fr
uit,
vege
tabl
es,r
efine
dgr
ains
,fibe
r,fis
han
dpo
ultr
y,m
eat,
fatt
yac
idcl
ass.
dN
S,no
nsig
nific
ant.
Abbr
evia
tions
:HPF
S,H
ealth
Prof
essi
onal
sFo
llow
-Up
Stud
y;IR
AS,I
nsul
inRe
sist
ance
Athe
rosc
lero
sis
Stud
y;M
ESA,
Mul
ti-Et
hnic
Stud
yof
Athe
rosc
lero
sis;
NH
SII,
Nur
ses’
Hea
lthSt
udy
II.
Nutrition Reviews® Vol. 70(7):387–396392

whole-wheat products into the diet were observed oneither insulin sensitivity or CRP concentrations.40
The WHOLEheart study39 is the largest interven-tional study conducted to date to examine the effects ofwhole-grain supplementation. A total of 316 participants,with low habitual consumption of whole-grain foods andBMIs above 25 kg/m2, were randomized to one of threediet groups. The control group was asked to maintaintheir current dietary habits. The intervention groups wereprovided with a range of whole-grain products and wereinstructed to substitute the products for similar items intheir habitual diet. One group was instructed to increasetheir consumption of whole grains to 60 g/day for a totalof 16 weeks, while a second group was instructed toincrease their consumption of whole grains to 60 g/dayfor the first 8 weeks and to 120 g/day for the final 8 weeks.At the end of the 16-week study, no significant differenceswere observed in the concentrations of either CRP orIL-6.
Another large study examined the effects of wholegrains in 226 overweight (mean BMI of intervention
groups, 27.0–28.0 kg/m2) middle-aged men andwomen.41 After a 4-week run-in period in which partici-pants consumed a refined-grain (habitual) diet, they wererandomized to one of three interventions: a refined-graindiet, a prescribed diet in which regular refined-grain fooditems were replaced with three servings of whole-wheatfoods, or a prescribed diet in which refined grains werereplaced with one serving of whole-wheat foods and twoservings of oats. At the end of the 12-week intervention,changes from the run-in diet for CRP or IL-6 concentra-tions were not significantly different between diets.
A favorable effect of increased whole-grain con-sumption on subclinical inflammation was identifiedwhen subjects were provided with a hypocaloric diet.38
Fifty obese participants with a mean age of 46 years and aBMI > 30 kg/m2 received dietary advice to either avoid allwhole-grain foods or consume only whole-grain foodsfor a period of 12 weeks. Dietary advice to both groupsalso included a 500 kcal/day deficit. The whole-graingroup increased whole-grain intake to approximately fiveservings per day. At the end of the intervention, there wasno difference in weight loss between groups, although thewhole-grain group lost a significantly greater percentageof body fat in the abdominal region. Additionally, CRPconcentrations declined significantly by 38% in thewhole-grain group but were unchanged in the refined-grain group. Changes in CRP concentrations were notcorrelated with the extent of weight loss, suggesting amechanism of action independent of effects on adiposity.
Several reasons may explain why interventionalstudies have not consistently confirmed the favorableeffects of increased whole-grain consumption on sub-clinical inflammation that have been observed in epide-miological studies. First, in none of the studies was dietcompletely controlled. Systematic or random day-to-dayvariations in dietary constituents that have the potentialto impact markers of inflammation (dietary fatty acids,glycemic load, antioxidants), combined with the inap-propriate substitution of foods in the habitual diet withthe intervention foods, would make the identification ofany true effects of whole grains more problematic. As anexample, in the WHOLEheart study, the inclusion ofwhole grains in the diet was accompanied by a reductionin fruit consumption,39 which may have offset any anti-inflammatory effects of whole grains. Additionally, in theWHOLEheart study, it was noted that energy intakeincreased in the whole-grain groups, suggesting that thesupplied food items were added on top of, rather thansubstituted for, similar items in the regular diet. Asimilar incomplete substitution may have occurred inthe study by Andersson et al.,37 since it was observedthat BMI values were slightly but significantly higherafter consumption of whole-grain versus refined-grainproducts.
Figure 1 Beta coefficients relating change in log-transformed CRP [ln(CRP)] per serving of whole grains.The “Base” model is the minimally adjusted model that doesnot include adjustments for dietary factors (other thanenergy), measures of adiposity, or measures of insulin resis-tance. The “Diet” adjusted model includes adjustments forany of the following intakes: fruit, vegetables, refined grains,fiber, fish and poultry, meat, fatty acid classes. The “BMI”adjusted model includes adjustments for any of the follow-ing: BMI, waist circumference, insulin concentrations, insulinsensitivity (Si), 2h-postprandial glucose. Data from indi-vidual studies are displayed as symbols with error bars(mean � SE), with common symbols across adjustmentmodels representing the same study. Bars represent esti-mates of the beta coefficient for each model, based onanalysis of the composite study data.
Nutrition Reviews® Vol. 70(7):387–396 393

Participant selection may be an additional confound-ing issue. In all of the interventional studies, participantswere selected on the basis of being either overweight orobese. On the surface, this may seem like a reasonableselection criterion given that overweight and obese indi-viduals are more likely to have elevated markers of sub-clinical inflammation and thus would appear to be moreamenable to the potentially favorable anti-inflammatoryeffects of whole grains. However, in a study examining theeffects of a high-fiber DASH diet (which included wholegrains), significant reductions in CRP concentrationswere seen only in lean participants (30% drop) asopposed to obese participants (10% drop).55 This mayalso explain the favorable effects of whole grains on CRPconcentrations when combined with weight loss andabdominal fat loss.38
Additional study design elements may also underliethe lack of observed effect of whole-grain consumptionon markers of inflammation. Observational studiesexamine the effects of dietary constituents consumedover a period of several years in several hundred toseveral thousand individuals. In contrast, interventionalstudies are conducted over a period of weeks to severalmonths and involve far fewer individuals. Thus, if theeffects of whole grains take a long time to manifest them-selves and/or the effect size is relatively small, then thedesign limitations typically associated with interventionalstudies may make it difficult to detect the effects of wholegrains on inflammatory markers.
Finally, one must also concede the possibility that theeffects of whole grains on subclinical inflammationobserved in observational studies are due to residual con-founding with other lifestyle and dietary factors, and thatwhole grains do not independently contribute to reduc-tions in subclinical inflammation.
POTENTIAL IMPACT OF REDUCTION IN CRP, ACHIEVEDTHROUGH INCREASED WHOLE-GRAIN CONSUMPTION,
ON RISK OF CARDIOVASCULAR DISEASE
Estimates from epidemiological studies suggest that eachserving of whole grains is associated with approximately a7.2% reduction in CRP concentrations. Thus, CRP con-centrations would be expected to decline by 20% if onewere to consume the recommended amount of wholegrains (50% of 6 servings of grains). Meta-analysis of 31long-term prospective studies44 suggests a relative risk forcoronary heart disease of 1.37 for each 1.1 increase innatural logarithm CRP concentrations (corresponding toa 3-fold change in CRP concentrations). Translating thisrelationship to the decline in CRP associated with threeservings of whole grains predicts reductions in the risk ofcoronary heart disease of approximately 6%. In contrast,epidemiological studies3,4,8 suggest that an increase of
three servings of whole grains decreases the risk of coro-nary heart disease by 15–25%. Thus, only a fraction of thereduction in cardiovascular disease risk associated withincreased whole-grain consumption is likely to be medi-ated by changes in CRP concentrations.
CONCLUSION
Prospective epidemiological data provide a reasonablebody of evidence pointing towards a modest effect ofwhole grains to reduce markers of subclinical inflamma-tion, especially circulating concentrations of CRP.However, results from the epidemiological studies shouldbe interpreted with caution, given that definitions used todefine “whole-grain foods” differ substantially acrossstudies and can either include products that do not meetthe definition of whole grains (e.g., bran cereals) orexclude potentially important sources of whole grains(e.g., brown rice and popcorn). Thus, the true effects ofwhole-grain consumption may be either higher or lowerthan currently estimated.
Interventional studies have the potential to providethe clearest understanding of the effects of whole grainson subclinical inflammation. However, studies conductedto date have not provided clear evidence of an effect ofwhole grains on any of a number of markers of inflam-mation and thus are largely in contrast with the observa-tional studies. As has been previously addressed,56 futureinterventional studies must be robustly designed to iden-tify potential favorable effects of whole-grain consump-tion on markers of subclinical inflammation. Theinterventional studies must be adequately powered and ofsufficient length to identify potential long-term effects.Ideally, the dietary intervention should be rigorously con-trolled through the provision of all meals. The character-istics of the selected study population should be carefullyconsidered to ensure that the results are generalizable.Finally, study designs should additionally take into con-sideration the possibility that all whole grains are notequal with respect to their health-promoting characteris-tics. Given that wheat, corn, rye, rice, and oats differ sub-stantially with respect to their carbohydrate, fiber, andphytochemical composition,57–59 it is likely naive toassume that they all share the same physiological proper-ties. It is well known that wheat and oat products differsubstantially with respect to their ability to influence low-density lipoprotein cholesterol concentrations,60,61 andpreclinical studies in mice have shown that whole grainsdiffer with respect to their metabolic properties.62,63
Given the importance of subclinical inflammation asa risk factor for chronic disease and the substantial rolethat grain and cereal products play in the food supply, it isimportant to gain a better understanding of the potentialfor whole grains to reduce inflammation. Knowledge of
Nutrition Reviews® Vol. 70(7):387–396394

the relative effects of individual types of whole grains, thecomponents within whole grains that confer any anti-inflammatory properties, and the mechanism of action ofsuch components would be of value to both the foodindustry and the public in efforts to provide a morehealthful diet. Additional research, employing well-controlled dietary interventions, should be directedtowards these areas.
Acknowledgments
Funding. M. Lefevre received an honorarium from theGeneral Mills Bell Institute of Health and Nutrition tosupport the preparation of this manuscript.
Declaration of interest. S. Jonnalagadda is an employee ofthe General Mills Bell Institute of Health and Nutrition.
REFERENCES
1. Mellen PB, Liese AD, Tooze JA, et al. Whole-grain intake and carotid artery ath-erosclerosis in a multiethnic cohort: the Insulin Resistance Atherosclerosis Study.Am J Clin Nutr. 2007;85:1495–1502.
2. Erkkila AT, Herrington DM, Mozaffarian D, et al. Cereal fiber and whole-grainintake are associated with reduced progression of coronary-artery atherosclero-sis in postmenopausal women with coronary artery disease. Am Heart J.2005;150:94–101.
3. Jensen MK, Koh-Banerjee P, Hu FB, et al. Intakes of whole grains, bran, and germand the risk of coronary heart disease in men. Am J Clin Nutr. 2004;80:1492–1499.
4. Steffen LM, Jacobs DR Jr, Stevens J, et al. Associations of whole-grain, refined-grain, and fruit and vegetable consumption with risks of all-cause mortality andincident coronary artery disease and ischemic stroke: the Atherosclerosis Risk inCommunities (ARIC) Study. Am J Clin Nutr. 2003;78:383–390.
5. Liu S, Sesso HD, Manson JE, et al. Is intake of breakfast cereals related to total andcause-specific mortality in men? Am J Clin Nutr. 2003;77:594–599.
6. Jacobs DR Jr, Meyer HE, Solvoll K. Reduced mortality among whole grain breadeaters in men and women in the Norwegian County Study. Eur J Clin Nutr.2001;55:137–143.
7. Liu S, Manson JE, Stampfer MJ, et al. Whole grain consumption and riskof ischemic stroke in women: a prospective study. JAMA. 2000;284:1534–1540.
8. Liu S, Stampfer MJ, Hu FB, et al. Whole-grain consumption and risk of coronaryheart disease: results from the Nurses’ Health Study. Am J Clin Nutr. 1999;70:412–419.
9. Jacobs DR Jr, Meyer KA, Kushi LH, et al. Is whole grain intake associated withreduced total and cause-specific death rates in older women? The Iowa Women’sHealth Study. Am J Public Health. 1999;89:322–329.
10. de Munter JS, Hu FB, Spiegelman D, et al. Whole grain, bran, and germ intakeand risk of type 2 diabetes: a prospective cohort study and systematic review.PLoS Med. 2007;4:1385–1394.
11. Fung TT, Hu FB, Pereira MA, et al. Whole-grain intake and the risk of type 2diabetes: a prospective study in men. Am J Clin Nutr. 2002;76:535–540.
12. Liu S, Manson JE, Stampfer MJ, et al. A prospective study of whole-grain intakeand risk of type 2 diabetes mellitus in US women. Am J Public Health.2000;90:1409–1415.
13. Meyer KA, Kushi LH, Jacobs DR Jr, et al. Carbohydrates, dietary fiber, and incidenttype 2 diabetes in older women. Am J Clin Nutr. 2000;71:921–930.
14. Montonen J, Knekt P, Jarvinen R, et al. Whole-grain and fiber intake and theincidence of type 2 diabetes. Am J Clin Nutr. 2003;77:622–629.
15. Chan JM, Wang F, Holly EA. Whole grains and risk of pancreatic cancer in a largepopulation-based case-control study in the San Francisco Bay Area, California.Am J Epidemiol. 2007;166:1174–1185.
16. Schatzkin A, Mouw T, Park Y, et al. Dietary fiber and whole-grain consumption inrelation to colorectal cancer in the NIH-AARP Diet and Health Study. Am J ClinNutr. 2007;85:1353–1360.
17. Larsson SC, Giovannucci E, Bergkvist L, et al. Whole grain consumption and riskof colorectal cancer: a population-based cohort of 60,000 women. Br J Cancer.2005;92:1803–1807.
18. US Department of Agriculture and US Department of Health and Humans Ser-vices. Dietary Guidelines for Americans, 2010, 7th ed. Washington, DC: U.S. Gov-ernment Printing Office; 2010.
19. Lichtenstein AH, Appel LJ, Brands M, et al. Diet and Lifestyle RecommendationsRevision 2006: a scientific statement from the American Heart Association Nutri-tion Committee. Circulation. 2006;114:82–96.
20. American Diabetes Association. Nutrition Recommendations and Interventionsfor Diabetes: a position statement of the American Diabetes Association. Diabe-tes Care. 2007;30(Suppl 1):S48–S65.
21. Libby P, Ridker PM. Inflammation and atherosclerosis: role of C-reactive proteinin risk assessment. Am J Med. 2004;116(Suppl 6A):S9–S16.
22. Pradhan AD, Manson JE, Rifai N, et al. C-reactive protein, interleukin 6, and risk ofdeveloping type 2 diabetes mellitus. JAMA. 2001;286:327–334.
23. Hu FB, Meigs JB, Li TY, et al. Inflammatory markers and risk of developing type 2diabetes in women. Diabetes. 2004;53:693–700.
24. Fung TT, Rimm EB, Spiegelman D, et al. Association between dietary patternsand plasma biomarkers of obesity and cardiovascular disease risk. Am J Clin Nutr.2001;73:61–67.
25. Lopez-Garcia E, Schulze MB, Fung TT, et al. Major dietary patterns are related toplasma concentrations of markers of inflammation and endothelial dysfunction.Am J Clin Nutr. 2004;80:1029–1035.
26. Hoffmann K, Zyriax BC, Boeing H, et al. A dietary pattern derived to explainbiomarker variation is strongly associated with the risk of coronary arterydisease. Am J Clin Nutr. 2004;80:633–640.
27. Kant AK, Graubard BI. A comparison of three dietary pattern indexes for predict-ing biomarkers of diet and disease. J Am Coll Nutr. 2005;24:294–303.
28. Jensen MK, Koh-Banerjee P, Franz M, et al. Whole grains, bran, and germ inrelation to homocysteine and markers of glycemic control, lipids, and inflamma-tion. Am J Clin Nutr. 2006;83:275–283.
29. Nettleton JA, Steffen LM, Mayer-Davis EJ, et al. Dietary patterns are associatedwith biochemical markers of inflammation and endothelial activation in theMulti-Ethnic Study of Atherosclerosis (MESA). Am J Clin Nutr. 2006;83:1369–1379.
30. Panagiotakos DB, Pitsavos C, Stefanadis C. Dietary patterns: a Mediterranean dietscore and its relation to clinical and biological markers of cardiovascular diseaserisk. Nutr Metab Cardiovasc Dis. 2006;16:559–568.
31. Esmaillzadeh A, Kimiagar M, Mehrabi Y, et al. Dietary patterns and markers ofsystemic inflammation among Iranian women. J Nutr. 2007;137:992–998.
32. Lutsey PL, Jacobs DR Jr, Kori S, et al. Whole grain intake and its cross-sectionalassociation with obesity, insulin resistance, inflammation, diabetes and subclini-cal CVD: the MESA Study. Br J Nutr. 2007;98:397–405.
33. Fung TT, Chiuve SE, McCullough ML, et al. Adherence to a DASH-style diet andrisk of coronary heart disease and stroke in women. Arch Intern Med. 2008;168:713–720.
34. Nettleton JA, Schulze MB, Jiang R, et al. A priori-defined dietary patterns andmarkers of cardiovascular disease risk in the Multi-Ethnic Study of Atherosclero-sis (MESA). Am J Clin Nutr. 2008;88:185–194.
35. Gaskins AJ, Mumford SL, Rovner AJ, et al. Whole grains are associated with serumconcentrations of high sensitivity C-reactive protein among premenopausalwomen. J Nutr. 2010;140:1669–1676.
36. Masters RC, Liese AD, Haffner SM, et al. Whole and refined grain intakes arerelated to inflammatory protein concentrations in human plasma. J Nutr.2010;140:587–594.
37. Andersson A, Tengblad S, Karlstrom B, et al. Whole-grain foods do not affectinsulin sensitivity or markers of lipid peroxidation and inflammation in healthy,moderately overweight subjects. J Nutr. 2007;137:1401–1407.
38. Katcher HI, Legro RS, Kunselman AR, et al. The effects of a whole grain-enrichedhypocaloric diet on cardiovascular disease risk factors in men and women withmetabolic syndrome. Am J Clin Nutr. 2008;87:79–90.
39. Brownlee IA, Moore C, Chatfield M, et al. Markers of cardiovascular risk are notchanged by increased whole-grain intake: the WHOLEheart study, a randomised,controlled dietary intervention. Br J Nutr. 2010;104:125–134.
40. Giacco R, Clemente G, Cipriano D, et al. Effects of the regular consumption ofwholemeal wheat foods on cardiovascular risk factors in healthy people. NutrMetab Cardiovasc Dis. 2010;20:186–194.
41. Tighe P, Duthie G, Vaughan N, et al. Effect of increased consumption of whole-grain foods on blood pressure and other cardiovascular risk markers in healthymiddle-aged persons: a randomized controlled trial. Am J Clin Nutr. 2010;92:733–740.
42. Rifai N, Ridker PM. Inflammatory markers and coronary heart disease. Curr OpinLipidol. 2002;13:383–389.
43. Rifai N, Ridker PM. High-sensitivity C-reactive protein: a novel and promisingmarker of coronary heart disease. Clin Chem. 2001;47:403–411.
44. Kaptoge S, Di AE, Lowe G, et al. C-reactive protein concentration and risk ofcoronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet. 2010;375:132–140.
45. Haffner SM. Insulin resistance, inflammation, and the prediabetic state. Am JCardiol. 2003;92:J18–J26.
46. Kritchevsky SB, Cesari M, Pahor M. Inflammatory markers and cardiovascularhealth in older adults. Cardiovasc Res. 2005;66:265–275.
Nutrition Reviews® Vol. 70(7):387–396 395

47. Fontana L, Eagon JC, Trujillo ME, et al. Visceral fat adipokine secretion is associ-ated with systemic inflammation in obese humans. Diabetes. 2007;56:1010–1013.
48. US Food and Drug Administration. Guidance for Industry and FDA Staff: WholeGrain Label Statements. 2006; Available at: http://www.fda.gov/Food/GuidanceComplianceRegulatoryInformation/GuidanceDocuments/FoodLabelingNutrition/ucm059088.htm [serial online]. Accessed 25 August2010.
49. McKeown NM, Yoshida M, Shea MK, et al. Whole-grain intake and cereal fiber areassociated with lower abdominal adiposity in older adults. J Nutr. 2009;139:1950–1955.
50. Liese AD, Roach AK, Sparks KC, et al. Whole-grain intake and insulin sensitivity:the Insulin Resistance Atherosclerosis Study. Am J Clin Nutr. 2003;78:965–971.
51. McKeown NM, Meigs JB, Liu S, et al. Whole-grain intake is favorably associatedwith metabolic risk factors for type 2 diabetes and cardiovascular disease in theFramingham Offspring Study. Am J Clin Nutr. 2002;76:390–398.
52. Mora S, Lee IM, Buring JE, et al. Association of physical activity and body massindex with novel and traditional cardiovascular biomarkers in women. JAMA.2006;295:1412–1419.
53. Festa A, D’Agostino R Jr, Howard G, et al. Chronic subclinical inflammation as partof the insulin resistance syndrome: the Insulin Resistance Atherosclerosis Study(IRAS). Circulation. 2000;102:42–47.
54. Festa A, Hanley AJ, Tracy RP, et al. Inflammation in the prediabetic state is relatedto increased insulin resistance rather than decreased insulin secretion. Circula-tion. 2003;108:1822–1830.
55. King DE, Egan BM, Woolson RF, et al. Effect of a high-fiber diet vs a fiber-supplemented diet on C-reactive protein level. Arch Intern Med. 2007;167:502–506.
56. Seal CJ, Brownlee IA. Whole grains and health, evidence from observational andintervention studies. Cereal Chem. 2010;87:167–174.
57. Hallfrisch J, Behall KM. Mechanisms of the effects of grains on insulin andglucose responses. J Am Coll Nutr. 2000;19:S320–S325.
58. Smeds AI, Jauhiainen L, Tuomola E, et al. Characterization of variation in thelignan content and composition of winter rye, spring wheat, and spring oat.J Agric Food Chem. 2009;57:5837–5842.
59. Okarter N, Liu RH. Health benefits of whole grain phytochemicals. Crit Rev FoodSci Nutr. 2010;50:193–208.
60. Davy BM, Davy KP, Ho RC, et al. High-fiber oat cereal compared with wheatcereal consumption favorably alters LDL-cholesterol subclass and particlenumbers in middle-aged and older men. Am J Clin Nutr. 2002;76:351–358.
61. Ripsin CM, Keenan JM, Jacobs DR Jr, et al. Oat products and lipid lowering. Ameta-analysis. JAMA. 1992;267:3317–3325.
62. Alvarez P, Alvarado C, Mathieu F, et al. Diet supplementation for 5 weeks withpolyphenol-rich cereals improves several functions and the redox state of mouseleucocytes. Eur J Nutr. 2006;45:428–438.
63. Andersson U, Rosen L, Ostman E, et al. Metabolic effects of whole grain wheatand whole grain rye in the C57BL/6J mouse. Nutrition. 2010;26:230–239.
Nutrition Reviews® Vol. 70(7):387–396396