Embed Size (px)
Citation preview

EFFECTIVE RESOURCE MANAGEMENT: THE OPTIMAL PROVIDER PAYMENT MIX
Cheryl CashinSenior Felllow, Results for Development InstituteNovember 4, 2013

Overview of the Presentation
2
• Defining the problem –balance between revenue and expenditure for universal health coverage
• Emerging messages from the Japan-World Bank Partnership Program for Universal Health Coverage
• Learning from experience—the role of the Joint Learning Network for Universal Health Coverage

3
Revenue and Expenditure: 2 sides of the Universal Coverage Coin
RevenueResources available to expand and sustain effective coverage
Expenditure• Benefits package (service
and medicines guaranteed)• Subsidies• Payment to providers

4
Revenue and Expenditure: 2 sides of the Universal Coverage Coin
RevenueResources available to expand and sustain effective coverage
Expenditure• Benefits package (service
and medicines guaranteed)• Subsidies• Payment to providers
Does revenue generation get more attention than expenditure management?

5
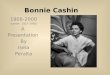
2005 2006 2007 2008 2009 2010 2011VAT SSNIT Investment Income Premiums OtherGrants
Ghana’s NHIA has achieved a growing and diversified revenue base
Raising revenue for UHC is not enough
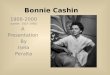
2010 2011 -
10
20
30
40
50
60
70
80
49
67
56
72
Claims/member Revenue/member
But the gap between revenue/member and claims/member is closing

6
What role does provider payment play?
Health care provider payment systems--the way providers are paid to deliver the covered package of
services—are an important strategic lever in universal health coverage
Help balance system revenues and costs and create incentives for providers to improve
quality and deliver services more efficiently
This ultimately makes it possible to expand coverage within limited funds

7
What are the options?Payment Method Definition
Line-item budget Providers receive a fixed amount to cover specific input expenses (e.g., personnel, drugs, utilities,).
Global budget Providers receive a fixed amount of funds for a certain period to cover aggregate expenditures. Budget is flexible and not tied to line items.
Per diem Hospitals are paid a fixed amount per day that an admitted patient is treated in the hospital.
Case-based (“DRG”) Hospitals are paid a fixed amount per admission depending on patient and clinical characteristics.
Fee-for-service Providers are paid for each individual service provided. Fees are fixed in advance for each service or group of services.
Per capita (“capitation”)
Providers are paid a fixed amount in advance to provide a defined set of services for each individual enrolled for a fixed period of time.

8
What are the options?Payment Method Definition
Line-item budget Providers receive a fixed amount to cover specific input expenses (e.g., personnel, drugs, utilities,).
Global budget Providers receive a fixed amount of funds for a certain period to cover aggregate expenditures. Budget is flexible and not tied to line items.
Per diem Hospitals are paid a fixed amount per day that an admitted patient is treated in the hospital.
Case-based (“DRG”) Hospitals are paid a fixed amount per admission depending on patient and clinical characteristics.
Fee-for-service (fixed fee schedule)
Providers are paid for each individual service provided. Fees are fixed in advance for each service or group of services.
Per capita (“capitation”)
Providers are paid a fixed amount in advance to provide a defined set of services for each individual enrolled for a fixed period of time.
There is no perfect payment method.
They all have strengths and weaknesses.
They all can create undesirable incentives and adverse consequences.
They all can be useful at different times depending on the objectives.

9
What is the optimal mix?
Messages emerging from the Japan-World Bank Partnership Program for Universal
Health Coverage

10
Overview of the Study
• The Japan-World Bank Program on Universal Health Coverage is a joint effort by the Government of Japan and the World Bank to support the Low and Middle Income Countries in their aspirations for UHC, following the 50th anniversary of Japan’s own achievement of UHC in 1961.

11
Countries Participating in the Study
• The countries have been selected to represent:• different stages of UHC• different geographic regions• diversity in the type of health systems
in place• willingness to explore key policy
questions in the analytical framework

12
The countries included in the study
Group 1: Early Adoption
BangladeshEthiopia
Group 2: Coverage Expansion
GhanaIndonesia
PeruVietnam
Group 3: UHC—Deepening Coverage
BrazilTurkey
Thailand
Group 4: Sustaining Coverage/Adaptive
Systems
FranceJapan

13
Coverage-enhancing vs. Coverage-eroding Expenditure Management• Expenditure management that frees up
resources to expand coverage is “coverage-enhancing.” – E.g. better negotiated medicines prices and well-
targeted subsidies “Countries that have achieved universal
population coverage and financial protection have
balanced revenue generation efforts with
coverage-enhancing expenditure management.”
• Controlling expenditure by limiting benefits, increasing cost-sharing, or under-paying providers can reduce access to necessary services and financial protection and is therefore “coverage-eroding.”

14
Countries relying on fee-for-service payment are facing coverage-eroding cost escalation and inefficiencies (except Japan)
Country Main Provider Payment System Consequences
EthiopiaFranceGhana
IndonesiaPeru
Open-ended Fee-for-Service
Sustainability concernsImplicit access and service
restrictionsImbalance between primary
and tertiary care
VietnamFee-for-Service with soft caps
based on historical expenditure
Over-use of high-cost services
Cost escalationHigh out-of-pocket payment
JapanFee-for-Service with annual
negotiation to maintain budget neutrality (“closed-ended”)
Well-functioning expenditure management

15
What is different about fee-for-service in Japan?
• Strong governance– Biennial revision of the fee schedule– Prices adjusted downward for services and medicines with large
volume increases
• Set tighter conditions for billing/payment– Example: Fee for diagnosing MRI image can only be billed once
every calendar month
• Strict enforcement of cost containment measures– On site audits to check claims with medical records
• Unified payment system across providers and insurers makes the mechanisms more effective and efficient– Only option: Play by the rules, or exit

16
Some countries are using coverage-eroding expenditure management approaches
Under-paying for services Brazil; Peru; VietnamSupply-side constraints and implicit access restrictions
Bangladesh; Brazil; Indonesia; Peru
Shifting of financial risk to providers (more than they can manage)
Vietnam
Increasing cost-sharing (higher deductibles)
France
Leakage to private insurance coverage
Brazil, France
Excessive shifting of financial risk to patients (creating access barriers)
Bangladesh, Ethiopia, Indonesia, Peru, Vietnam

17
What does coverage-enhancing expenditure management look like?
Japan • Fee schedule revision as a cost containment tool• Global targets for expenditure increases
France
A set of "soft" expenditure controls• System-level spending targets• Sub-level targets (ambulatory care; hospitals; rehabilitation)• Monitoring and “early warning”
Thailand
• Closed-ended capitation contracting with DRG hospital payment
• Strong primary care gate-keeping• Tough negotiation with pharmaceutical companies• Priority-setting for expansion of benefits
Turkey
• Closed-ended payment systems with performance-based component (global budget for hospitals and capitation for primary care)
• Expenditure caps at the hospital level and on pharmaceuticals

18
What does coverage-enhancing expenditure management look like?
Japan • Fee schedule revision as a cost containment tool• Global targets for expenditure increases
France
A set of "soft" expenditure controls• System-level spending targets• Sub-level targets (ambulatory care; hospitals; rehabilitation)• Monitoring and “early warning”
Thailand
• Closed-ended capitation contracting with DRG hospital payment
• Strong primary care gate-keeping• Tough negotiation with pharmaceutical companies• Priority-setting for expansion of benefits
Turkey
• Closed-ended payment systems with performance-based component (global budget for hospitals and capitation for primary care)
• Expenditure caps at the hospital level and on pharmaceuticals
Spending targets
Closed-ended provider payment

19
Key Features of “Optimal Provider Payment Mix”?
Closed-ended
Incentives to limit high-cost services
Emphasis on Primary
Care
Negotiation of drug prices

20
Key Features of “Optimal Provider Payment Mix”?
Closed-ended
Closed-ended payment systems impose a cap at some level (usually the provider)
For example,
• Capitation• DRG with global budget—pay
for admissions until volume targets are exceeded
[e.g. Thailand] Challenge: what happens when
volume target is exceeded and cap is reached?

21
Key Features of “Optimal Provider Payment Mix”?
Incentives to limit high-cost services
For example,
• Pay providers below cost for some high-cost/low priority services (e.g. MRI)
• Limit volume
[e.g. Japan]
• Higher cost-sharing for self-referral
[e.g. France, Thailand, Turkey] Challenge: requires a high degree
of monitoring and information

22
Key Features of “Optimal Provider Payment Mix”?
Emphasis on Primary
Care
For example,
• Primary care gate-keeping
• “Ring-fencing” or setting targets for share of expenditure for primary care
• Paying relatively higher rates for primary care
[e.g. France, Thailand, Turkey] Challenge: primary care system is
still weak in some countries
Resistance to gate-keeping

23
Key Features of “Optimal Provider Payment Mix”?
Negotiation of drug prices
For example,
• Reference pricing• Budget caps [e.g. Turkey]• Mandatory rebates and discounts [e.g.
Turkey]• Health technology assessment to
expand medicines covered [e.g. Thailand] Challenge: the pharmaceutical industry is
a powerful interest group
Challenge: pushing drug prices too hard could limit market participation and innovation

Examples of Provider Payment Mix
24
Payment for primary care
Payment for inpatient services
DRG with Global Budget
Capitation
(FFS for some preventive services)
Payment for outpatient specialty services
Thailand UC Scheme
Global Budget(pay-for-
performance/FFS)
Capitation
(pay-for-performance/
salary deduction)
Turkey SSI

25
Ongoing process of analysis, revision, and response
• Ongoing process-there is no endpoint
• Good provider payment systems require a high degree of institutional capacity and information takes time to build
• Involvement and negotiation with providers is key
• Some coverage-enhancing expenditure management strategies can eventually put too much pressure on the system and begin to erode coverage—so it is an ongoing process
• Countries take steps, gain experience, do analysis, and revise

26
Role of the Joint Learning Network
• These big picture messages require detailed technical action
• Technocratic solutions have to get implemented in the real world with interest groups and politics
• Sharing experience with countries who are facing the same challenges can provide innovative ideas and help avoid some pitfalls

27
How it all fits together
27
Identification of the Need for
Reform
Step 1: Diagnostics
Step 2: Payment
System Design
Step 3: Implementatio
n Roadmap
JLN PPM Diagnostic and
Assessment Guide
Topic specific joint-learning activities (e.g. JLN Health Services Costing Collaborative)
General JLN events,
knowledge products and community interaction
PPM Reform
Proposal
Country process
Joint learning input
Stakeholder consultations and data analysis
Share country experience
with JLN members
JLN targeted country support

2828
Co-production of knowledge
Practical guidance
“Soon after the costing work is commissioned, the costing team should identify and prioritize stakeholders and develop a strategy to engage them throughout the costing exercise. “
“Adopt the least expensive and labor-intensive data collection and management plan that is necessary to get valid results.”

29
Joint learning in action

30
Final Thoughts
• Revenue generation is important, but using expenditure management and provider payment levers early on or at key junctures of system refinement is critical for coverage expansion.
• Sustaining UHC is a constant balancing act.
• Countries that have been most successful make choices that are coverage-enhancing, learn from past challenges, and continuously adjust and adapt.
• Learning from other countries can help make better technical decisions and navigate real-world implementation challenges.

31
THANK YOU