Embed Size (px)
Citation preview

Effectiveness of Micronutrient-rich Lipid Nutrient Supplements in
Delaying Clinical Progression of HIV in Malawian Adults
Heidi Sandige, MD

Background
• PLWHA in sub-Saharan Africa have a high risk of HIV associated malnutrition.
• progression to symptomatic disease faster

The current World Health Organization (WHO) standard of
care:
• ART limited to patients in WHO-defined Stage III or Stage II with CD4 <350
• No nutritional supplements of any kind to individuals who are HIV-infected with a body mass index (BMI) greater than 18.5.
Background
• CD4 counts are not widely available in this part of the world
• Decreasing BMI is the only clinical characteristic consistently predicting poor outcome in HIV positive patients, but this number does not reflect micronutrient deficiency
• Undernutrition = malnutrition and/or micronutrient deficiency

Background
• Various micronutrient supplement combinations have been effective in reducing HIV complications, particularly among pregnant women.
Lipid Nutrient Supplements
• RUTF designed for use in malnourished children
• Variation acceptable to malnourished HIV positive adults
• New Micronutrient rich LNS (M-LNS)

HypothesisAmong HIV-infected adults, those that receive
M-LNS compared to those not receiving supplement or micronutrients will:
1. Show less rapid progression to need for ART (stage III or stage II and CD4<350)
2. Maintain higher CD4 counts
3. Preserve their body weight and BMI more effectively
4. Experience fewer significant clinical events.
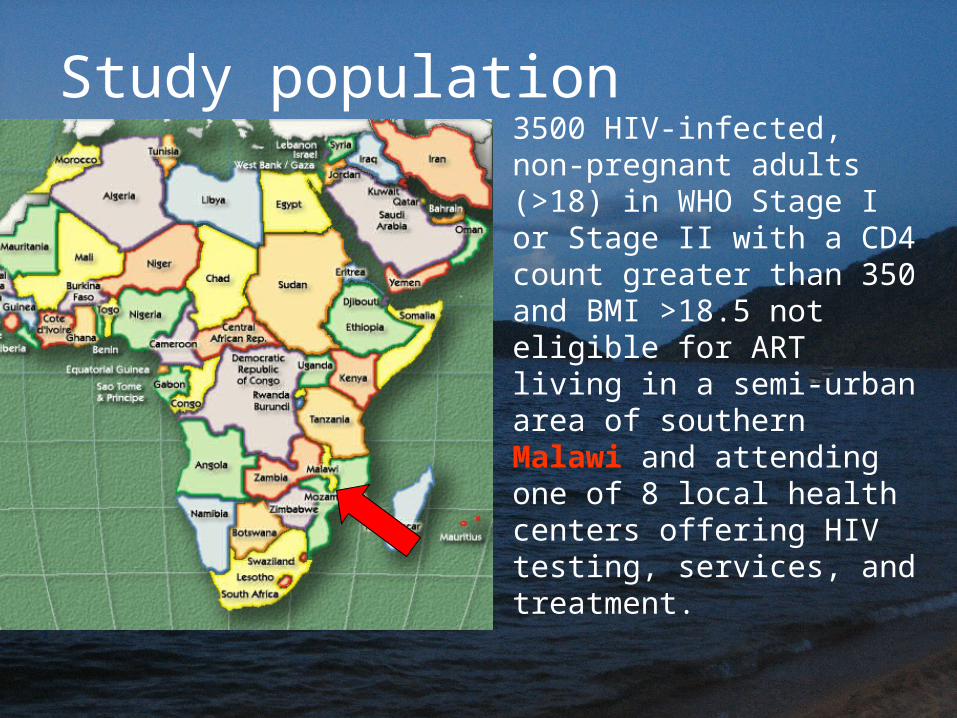
Study population3500 HIV-infected, non-pregnant adults (>18) in WHO Stage I or Stage II with a CD4 count greater than 350 and BMI >18.5 not eligible for ART living in a semi-urban area of southern Malawi and attending one of 8 local health centers offering HIV testing, services, and treatment.

MethodsProspective cluster randomized, single-blind,
controlled clinical effectiveness trial• the unit of randomization will be the health
center.

20g/day M-LNSStandard of care(no supplements)

MonitoringMonth: 0 2 4 6 8 10 12 14 16 18 20 22 24
Visit #: 0 1 2 3 4 4 6 7 8 9 10 11 12
Socio-demographic questions
Clinic visit for M-LNS supply
Questionnaire regarding clinical events
Weight, MUAC
Height, BMI
QOL and HFIAS surveys
CD4 count and HIV viral load
•Their clinical and nutritional course will be followed over a period of two years, recording anthropometric measures, and signs and symptoms of common manifestations/ complications of symptomatic AIDS.

Primary Outcomes
1. Progression to symptomatic HIV diseasewithin 2 years
Need for ARTs:• WHO stage III or higher • CD4 count <350• note: severe malnutrition increases stageDeath will be considered progression
2. Changes in CD4 count

Secondary outcomes
Within 6, 12, 18, and 24 months:– change in viral load
– change in body mass index (BMI)
– number of significant clinical events (defined as hospitalizations or deaths)
– change in quality of life assessment

Analysis• Fisher’s Exact Test for primary
outcome of progression (comparison of proportions)
• Survival analysis if there is a considerable amount of progression
• Student’s t test (or nonparametric test if not normally distributed) for continuous outcomes such as change in CD4, number of clinical events, etc.
Analysis at 6, 12, 18, and 24 months

Significance
In Sub-Saharan Africa where HIV and malnutrition are highly prevalent, if M-LNS could delay the need for ART and the complications of HIV, it could provide a useful tool in extending the asymptomatic lifetimes and improving the nutritional status and quality of life of HIV positive patients.


Thank youThank you

Sample size• 2yr progression rate:
– US/Europe 10%– in Uganda 40%
• To show 5% change (binary outcome of progression)
• 15% drop out rate
• greater power for continuous outcome changes in CD4 count and HIV viral load.
5% change # needed
10 to 15 % 686
15 to 20 % 906
20 to 25 % 1094
25 to 30 % 1251
30 to 35 % 1377
35 to 40 % 1471
α 0.05, power 80%
Effect of Cluster Randomization
?• Will depend upon baseline characteristics of patients
(generalizability)• Same set of clinicians staff clinics, different ancillary staff• Not randomizing in this way presents more logistical and
cultural problems• M-LNS may be seen as desirable OR undesirable

Additional Data collection
• In addition, associations between single clinical signs and symptoms, or constellation thereof, will be correlated with CD4 count in order to inform the development of a field assessment tool for predicting CD4 count.





























