Embed Size (px)
Citation preview

Kidney International, Vol. 56 (1999), pp. 1934–1943
Effects of an amino acid dialysate on leucine metabolism incontinuous ambulatory peritoneal dialysis patients
JACQUES DELARUE, CLAUDE MAINGOURD, MARTINE OBJOIS, MICHELE PINAULT, RICHARD
COHEN, CHARLES COUET, and FERNAND LAMISSE
Laboratoire de Nutrition de Tours, Association Regionale d’Aide aux Uremiques du Center Ouest, CHRU de Tours, andService de Radiopharmacie et Radioanalyse, Hopital Neuro-cardiologique, Lyon, France
Effects of an amino acid dialysate on leucine metabolism in neal absorption [3]. Conversely, glucose has some ad-continuous ambulatory peritoneal dialysis patients. verse effects in CAPD patients. The repetition of
Background. Protein-energy malnutrition is frequent in con- peritoneal glucose loads in patients with insulin resis-tinuous ambulatory peritoneal dialysis (CAPD) patients. Thetance [4, 5] entertains chronic hyperinsulinemia, whichuse of amino acids in the dialysate could improve the proteinmay induce dyslipidemia [6]. In addition, peritoneal dial-balance, especially if associated to a concomitant energy intake.
Methods. A 1.1% amino acid solution for peritoneal dialysis ysis with glucose could aggravate anorexia [7], and itwas administered to CAPD patients over 30 minutes during induces losses of amino acids and protein into dialysateconcomitant absorption of 600 ml water (control study) or of [8]. These effects of dialysis, associated with superim-a 600 kcal meal/600 ml. Leucine metabolism was studied using
posed catabolic illnesses and/or metabolic alterations re-the combination of intravenous [2H3] and intraperitoneal [13C]lated to end-stage renal failure itself, lead to malnutritionleucine.
Results. The rate of leucine appearance was stimulated by [9]. Indeed, protein-energy malnutrition is observed in56 and 53% (control and meal) at 45 minutes. The rates of 40% of patients undergoing CAPD [10]. An approachleucine appearance and disappearance were lower from 180 to improving protein balance in CAPD patients has beento 300 minutes during the meal versus control study (P , 0.05).
the use of amino acids in place of glucose in the dialysateProteolysis was unaffected during the control study and was[11]. To obtain such a beneficial effect, these amino acidsinhibited by 25% during the meal study (P , 0.05). During
the five-hour cycle dialysis with or without a meal, 80% of the must contribute to protein synthesis and/or must induceleucine administered into the peritoneum was absorbed. Forty- a decrease in protein catabolism. In addition, it is knownone percent was retained in the splanchnic bed. Forty-three that the administration of energy substrates (carbohy-percent was used for protein synthesis, and 16% was oxidized.
drates and/or lipids) decreases nitrogen output and in-Conclusions. This amino acids solution is efficaciously uti-hibits endogenous protein breakdown, which reinforceslized for protein synthesis in CAPD patients with no effect on
protein breakdown. The concomitant ingestion of a carbohy- the positive effect of protein or amino acid load on pro-drate-lipid meal inhibits protein breakdown and reinforces a tein balance [12, 13]. Thus, the absorption of a carbohy-positive effect of the amino acids solution on protein balance. drate-lipid meal during a cycle of peritoneal dialysis with
an amino acid solution could enhance its potential bene-ficial effect on protein metabolism in CAPD patients.
Continuous ambulatory peritoneal dialysis (CAPD) To more directly address the effects of the peritonealis a chronic renal replacement therapy based on the delivery of amino acids on protein metabolism in associa-exchanges between the blood and a peritoneal glucose tion with or without an oral energy intake, we used thesolution that is replaced many times a day through an technique of a dual tracer of leucine: (a) [1-13C]-leucine,implanted catheter [1]. The main advantages of glucose to quantitate the metabolic fate of leucine contained inas an osmotic agent are its low toxicity [2] and its contri- the dialysis solution delivered into the peritoneal cavity;bution to energy metabolism via oxidation after perito- and (b) [5,5,5-2H3] leucine, to estimate whole body pro-
tein turnover and endogenous protein breakdown.Key words: protein balance, malnutrition, CAPD, diet and dialysis,carbohydrates.
METHODSReceived for publication February 2, 1999 Patientsand in revised form May 20, 1999Accepted for publication June 17, 1999 Six clinically stable, nondiabetic, chronically uremic
patients (2 women and 4 men, 53 6 13 years old, 61 6 1999 by the International Society of Nephrology
1934

Delarue et al: Peritoneal amino acids and protein metabolism 1935
Table 1. Plasma albumin and anthropometric data in CAPD patients on entry in the study
Brachial Triceps Biceps Supra-iliac Sub-scapularcircumference skinfold skinfold skinfold skinfold
Age Albuminyears g/liter mm
Patient #1 60 39 24.5 3.8 2.4 6.6 7.2Patient #2 51 39 26 4 1.8 5.6 5.1Patient #3 56 36 35 34.6 15.2 36.4 39.3Patient #4 51 40 25.9 6.9 1.6 6.8 11.2Patient #5 30 34 22.5 4.4 3 5.4 5.9Patient #6 71 34 30 20 7.8 16.4 17
13 kg, body mass index 23.9 6 6.8 kg/m2) gave theirwritten consent for participation in the study. Three pa-tients were anuric. All of the subjects underwent CAPDfor at least six months (6 to 70 months). None had sufferedfrom peritonitis for at least six months. The mean dailyenergy and protein intakes were, 40 6 19 kcal · kg · day21
and 1.39 6 0.6 kcal · kg · day21, respectively. The meanserum albumin was 38 6 2 g/liter. Individual values for
Fig. 1. Protocol design.albumin and anthropometric data are reported in Table 1.The protocol was approved by the Ethical Committeeof Tours.
Protocol designMaterials The design of the study is reported in Figure 1. The
The peritoneal dialysis solution used for these experi- subjects were studied twice, two weeks apart, in a ran-ments contained 1.1% amino acids (Nutrinealt PD4; dom order. The subjects were instructed to drain any
dialysate from the peritoneum 12 hours before the begin-Baxter, Maurepas, France). The dialysis solutions bagsning of each experiment. After voiding, the subjects werewere from the same batch and were sampled for determi-placed at rest in a bed and maintained in the supinenation of actual leucine concentration and isotopic en-position throughout the experiments. Any residual dialy-richment (IE) before and after introduction of L-[1-13C]-sate was drained from their peritoneum. One intrave-leucine. L-[1-13C]-leucine [99 mol percent excess (MPE)]nous catheter was inserted into a wrist vein for collectionand L-[5,5,5-2H3]-leucine (99 MPE) were obtained fromof blood samples. This hand was maintained in a heatedCambridge Isotopes Laboratories (Andover, MA, USA).box (608C) to achieve partial arterialization of venousIsotopic and chemical purity were checked by gas chro-blood. Another catheter was inserted into an antecubitalmatography-mass spectrometry (GC-MS; Hewlett-Pack-vein of the controlateral arm for tracer infusion. At 7:30ard 5971, series II; Hewlett-Packard, Les Ulis, France).a.m. (T2180), a primed (60 3 infusion rate/min) constantTracers of leucine were prepared as sterile pyrogen-free(0.04 mmol · kg · min21) infusion of [5,5,52H3]-leucine wassolutions in normal saline. The solutions were filteredstarted and maintained for the next eight hours. The
through a 0.22 mm Millipore filter (Millipore Corp., Bed- dialysis solution enriched with L-[1-13C]-leucine (3.43 6ford, MA, USA) during introduction into the dialysis 0.25 MPE) was delivered into the peritoneal cavity oversolution bag (L-[1-13C]-leucine) or during priming and 30 minutes (T0 to T30). The volume of the solution infusedintravenous infusion (L-[5,5,52H3]-leucine). The actual was obtained from the weighing to the nearest gram ofdeuterated leucine concentration was determined in each the dialysis bag before and after its emptying into theinfusion solution. The meal absorbed by the patients peritoneal cavity. In control study, the patients ingestedwas composed of 30 g of wheat glucose (3.66 kcal/g; 600 ml tap water over 30 minutes (T0 to T30), that is,IE:1.08815 atom percent) plus 88 g of potato maltodex- over the same time as the administration of the dialysistrin (Glucidex 9t, 3.84 kcal/g, IE:1.08396 atom percent- solution. In meal study, over 30 minutes (T0 to T30) theage) equivalent to a carbohydrate energy load of 448 patients ingested a 600 kcal carbohydrate-lipid meal di-kcal and of 16.8 g of sunflower oil (IE:1.07917 atom luted in 600 ml of tap water and homogenized with apercentage) equivalent to a lipid energy load of 152 kcal. mixer. The study was then pursued until 300 minutes,Glucose and maltodextrin were kindly provided by Ro- that is, a five-hour cycle dialysis. Oxygen consumption and
carbon dioxide production were measured continuouslyquette Freres (Lestrem, France).

Delarue et al: Peritoneal amino acids and protein metabolism1936
from T260 to T300 minutes using indirect calorimetry with before injection in GC-MS. The gas chromatograph wasa ventilated hood, as previously described [3]. equipped with a 25 m fused silica capillary column (CP
Blood samples were sequentially collected in the basal SIL 19 CB, 25 m, 0.25 m ID, phase 0.20 mm Chrompack,state and every 15 minutes during the five-hour cycle France). The operating conditions were as follows: injec-dialysis for the determination of glucose, nonesterified tor temperature, 2508C; oven temperature, 1828C; andfatty acids, and insulin concentrations, and for the deter- source temperature, 2708C. Fragmentation of the mole-mination of IE in 13C and in deuterium of leucine. Sam- cules was performed by electron impact ionization andples for plasma bicarbonates and urea levels determina- selective monitoring of ions 305 and 302 for determina-tion were obtained at T0 and T300. The dialysate was tion of IE of [2H3] leucine and of ions 303 and 302 foralso sampled every 30 minutes for the determination of determination of IE of [13C] leucine. The molar ratiosleucine concentrations and IE in 13C. At the end of each of [2H3] leucine and [13C] leucine were then calculatedstudy, the peritoneal cavity was drained. The volume of from standard curves of [2H3] leucine in natural leucinethe drained dialysate was obtained from weighing the and of [13C] leucine in natural leucine. In the calculationdialysis bag to the nearest gram. Samples of expired air of the [2H3] leucine molar ratio, we corrected the peakwere obtained in basal state and every 15 minutes during area ratio at m/z 305/302 for the contribution of [13C]the cycle dialysis for the determination of IE in 13C of leucine to the peak area of ion 302 [16]. Leucine concen-expired CO2. Urine was collected at the end of the con- trations in plasma, in dialysis solution, and in dialysatetrol study in the three nonanuric patients. were determined by GC-MS using norleucine as an inter-
nal standard. We calculated the molar ratios from a stan-Analytical procedures
dard curve of norleucine in natural leucine with selectiveBlood samples were immediately spun at 48C. Plasma monitoring of ion 200 of leucine and norleucine.
was separated into aliquots. Plasma aliquots and dialy- Isotopic enrichment in 13C of expired CO2 was deter-sate samples were immediately frozen at 2808C. Urine mined using an Isotope Ratio Mass Spectrometersamples were frozen at 2808C for a further determina- (IRMS; Isochrom, Micromass, Villeurbanne, France).tion of total urinary nitrogen.
Plasma glucose concentrations were measured by the Calculationsglucose oxidase method using a Beckman glucose ana- Nomenclature. The total rate of plasma leucine ap-lyzer 2 (Beckman Instruments, Fullerton, CA, USA). pearance (Ra) is the sum of the infused tracer (Fiv), theNonesterified fatty acid concentrations were measured entry rate in plasma of leucine absorbed through theby an enzymatic colorimetric method with the use of a peritoneum (exogenous; Raexo), and the entry rate ofcommercial kit (NEFA C; Wako Chemicals, Freiburg, leucine released from endogenous protein breakdownGermany). Plasma insulin was measured by radioimmu- (Raendo). Exogenous leucine oxidation (Exo Leuox) is thenoassay (INS-IRMA; Biosource Europe S.A., Nivelles, rate of oxidation of exogenous leucine. Exogenous leu-Belgium). Plasma urea was determined by a kinetic ultra-
cine nonoxidized (Exo Leunon-ox) is the rate of exogenousviolet method on an automatized apparatus (Abbott
leucine utilized for protein synthesis.Spectrum, Rungis, France). Total urinary nitrogen wasRa, Raexo, Raendo. Total Ra, Raexo, and Raendo were calcu-determined with the use of Kjeldahl’s method.
lated in non-steady state using Steele’s equation [17],The enrichment in 13C and in deuterium of plasmaadapted by Proietto et al [18] and used as previouslyleucine was determined by GC-MS on the t-butyldimeth-described by Boirie et al [19].ylsilyl (TBDMS) derivative of leucine [14, 15]. The sam-
Ra was calculated as follows:ples were deproteinized with ice-cold perchloric acid(6% vol/vol) and neutralized with 3.2 m K2CO3 before
Ra 5Fiv 2 [pV 3 C(t) 3 dEIiv/dt]
EI(t)centrifugation at 2000 g. The supernatant was acidified(pH 1 to 1.5) with HCl 3N and deposed on a cation
where Fiv is the rate of tracer infusion (mmol/kg · min21),exchange resin (Bio-Rad Cation AG 50 W-X8 hydrogenand p is the correction factor of the pool size for instantform resin 200–400 mesh, Ivry-sur-Seine, France). Themixing (P 5 0.25). V is the volume of distribution (V 5resin was rinsed with HCl 0.01 N. Leucine was then0.5 liter/kg body wt) so that pV 5 0.125 liter/kg [19].eluted with NH4
1 4N. The effluent was first evaporatedC(t) is the mean plasma leucine concentration includingunder nitrogen at an ambient temperature to eliminatelabeled and unlabeled leucine between two time pointsammoniac and was then dried with a Speed Vac Concen-(in mmol/liter); dEIiv/dt is the variation of enrichment oftrator (Jouan, France). The dried sample was then deriv-plasma deuterated leucine from infused tracer (in MPE)atized with 50 ml of a 1:1 mixture of N methyl-N-(t-as a function of time, and EI(t) is the mean plasmabutyldimethylsylil) trifluoroacetamide (MTBSTFA; Pierce,leucine enrichment for the intravenous tracer betweenRockford, IL, USA) and acetonitrile. The derivatized
sample was then kept 12 hours at ambient temperature two sample points.

Delarue et al: Peritoneal amino acids and protein metabolism 1937
Raexo was calculated according to the transposition of gen from urea in dialysate corrected from the variationof body urea pool [22].Steele’s equation by Proietto:
Statistical analysisRaexo 5RaT 3 EI13C(t) 1 [pV 3 C(t) 3 dEI13C/dt]
13C dial Leu EI All data are expressed as mean 6 se. A comparisonof kinetics of the different parameters over time duringwhere EI13C is the isotopic enrichment (IE) of plasmaone study was performed using one-way analysis of vari-leucine appearing from the dialysate and 13C dial Leu EIance with repeated measures. A comparison of kineticsis the enrichment in 13C of leucine contained in dialysate.of the different parameters over time between the twoThen Raendo, an estimate of whole body protein break-studies was performed using factorial analysis of variancedown, was calculated as follows:and Student’s paired t-test.
Raendo 5 RaT 2 Raexo 2 Fiv
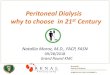
Leucine oxidation. Total leucine oxidation was not RESULTSdetermined in this study because it would have required Metabolites and hormonesa third test with infusion of 1-13C-leucine as a tracer. Kinetics of plasma glucose, nonesterified fatty acids,Such a third test was ethically difficult in our patients. and insulin are reported in Figure 2. Glycemia decreasedOxidation of leucine contained in dialysate was calcu- from 120 to 300 minutes as compared with time 0 (P 5lated as previously described [19]: 0.0001) during the control study. During the meal study,
glycemia increased from 30 to 120 minutes as comparedExo Leuox 5
EICO2
dial 13C Leu EI3 VCO2 3
10.81 with time 0 (P , 0.05). Glycemia was higher during the
meal study as compared with the control study (P 5where EICO2/dial 13C Leu EI represents the fraction of 0.001). Insulinemia increased from 30 to 90 minutes dur-leucine contained in the dialysate being oxidized. VCO2 ing the control study (P 5 0.0001). During the mealis the rate of production of CO2, and 0.81 is the recovery study, insulinemia increased from 30 to 150 minutes asfactor [20]. The background IE in 13C of expired CO2 compared with time 0 (P , 0.05). Insulinemia was higherover the five-hour cycle dialysis was not affected by the during the meal study as compared with the control study
(P , 0.01). Nonesterified fatty acids were lower from 60ingestion of the meal, as assessed in two additionalto 150 minutes as compared with time 0 (P , 0.001)CAPD patients (data not shown).during the control study. During the meal study, NEFAThe contribution of leucine from dialysate to proteinconcentrations were lower from 60 to 300 minutes assynthesis (Leunon-ox) was calculated from the differencecompared with time 0 (P , 0.001). Nonesterified fattybetween rate of disappearance of exogenous leucineacid concentrations were lower during the meal study as(Rdexo) and leucine oxidation was as follows:compared with the control study (P , 0.001). Blood pH
Exo Leunon-ox 5 Rdexo 2 Exo Leuox and plasma urea and bicarbonates concentrations arereported in Table 2.where
Respiratory quotient and substrates oxidationRdexo 5 Raexo 2
pV 3 C(t) 3 dEI13C/dtdial 13C Leu EI Kinetics of respiratory quotient (RQ) and of carbohy-
drate and lipid oxidations are reported in Figure 3. TheLeucine absorbed. The amount of leucine absorbed RQ was lower from 180 to 300 minutes than at time 0
through the peritoneum during each test was calculated (P , 0.05) during the control study. During the mealas the difference between the amount of leucine in the study, RQ increased from 150 minutes to 300 minutesdialysis bag minus the amount of leucine recovered in than at time 0 (P , 0.001). The RQ was higher duringthe dialysate at the end of the study. the meal study than during the control study (P , 0.001).
Splanchnic leucine extraction. Splanchnic leucine ex- Basal carbohydrate oxidation was similar during thetraction, that is, the amount of leucine retained in liver control study and meal study (1.93 6 0.10 vs. 2.04 6 0.23and/or peritoneum was calculated as follows: mg · kg21 · min21). Cumulated CHO oxidation was higher
during the meal study than during the control studySplanch extr 5 Leucine absorbed 2 Raexo(52.8 6 10.3 vs. 30.4 6 5 g · 5 hr21, P , 0.001). Basal
Substrates oxidation. Substrates oxidation was calcu- lipid oxidation was similar during the control study andlated from VO2, VCO2, and the caloric equivalent of the the meal study (0.53 6 0.26 vs. 0.53 6 0.25 mg · kg21 ·energy substrates given [21]. Total nitrogen excretion min21). Cumulated lipid oxidation was lower during thewas calculated as previously described [3] from the sum meal study than during the control study (5.5 6 3.7 vs.
13.3 6 4.4 mg · kg21 · min21, P , 0.01).of urinary nitrogen excretion (when available) plus nitro-

Delarue et al: Peritoneal amino acids and protein metabolism1938
Dialysate and plasma leucine concentrations
Kinetics of dialysate and plasma leucine concentra-tions are reported in Figure 4.
The amount of leucine that disappeared from the dial-ysate, that is, that which was absorbed through the peri-toneum, was similar in the control study and in the mealstudy (12.5 6 0.6 vs. 13 6 0.5 mmol, respectively) andaccounted for 80 and 84% of the amount of leucinecontained in the dialysate. Dialysate leucine concentra-tions decreased from 6.6 6 0.3 at baseline to 1.3 6 0.2mmol/liter at 300 minutes in the control study and from6.5 6 0.2 to 1.1 6 0.3 mmol/liter in the meal study. Thesekinetics were similar between the two studies.
Basal plasma leucine concentrations were similar be-tween the control study and the meal study (70 6 5 vs.77 6 3 mmol/liter). The delivery of the dialysis solutioninto the peritoneum induced a sharp increase in plasmaleucine concentrations that reached a similar peak at 45minutes (152 6 14 vs. 166 6 13 mmol/liter). As from thistime, kinetics were different between the two studies.During the control study, plasma leucine concentrationsdecreased progressively but remained higher at 300 min-utes (124 6 10 mmol/liter, P , 0.05) than at 0 minutes.Conversely, during the meal study, plasma leucine con-centrations decreased more rapidly and returned to basalvalue at 150 minutes. As from 210 to 300 minutes, plasmaleucine was higher in the control study than in the mealstudy (P , 0.001).
Leucine kinetics
Total rate of leucine appearance. The delivery of dial-ysis amino acid solution into the peritoneal cavity in-duced a rapid increase in the total rate of plasma leucineappearance (Fig. 5A) from 1.67 6 0.15 mmol · kg · min21
at baseline to a peak of 2.61 6 0.26 mmol · kg · min21
at 45 minutes during the control study and from 1.71 60.10 mmol · kg · min21 at baseline to a peak of 2.62 60.25 mmol · kg · min21 at 45 minutes during the mealstudy. From this time point, the kinetics were differentbetween the two studies. During the control study, Radecreased progressively but remained higher at 300 min-utes (1.89 6 0.20 mmol · kg · min21, P , 0.05) than atbaseline. During the meal study, Ra returned to baselineat 150 minutes. Ra in meal study was lower than in thecontrol study as from 180 to 300 minutes (P , 0.05).
Exogenous leucine rate of appearance, oxidation, andnonoxidative disposal. The kinetics of Raexo, Exo Leuox,and Exo Leunon-ox were similar between the control studyand the meal study. The rate of entry of exogenous(dialysate) leucine in plasma (Fig. 5B) achieved a peak
Fig. 2. Kinetics of plasma glucose (A), nonesterified fatty acids (B),at 0.86 6 0.21 mmol · kg · min21 at 45 minutes in theand insulin (C) concentrations after peritoneal delivery of an 1.1%
amino acid solution with (j) or without (h) meal ingestion. control study and at 0.80 6 0.12 mmol · kg · min21 at 60minutes in the meal study. Cumulated Raexo was 7.5 61.2 (control study) vs. 7.6 6 1 mol/5 hr21 (meal study),

Delarue et al: Peritoneal amino acids and protein metabolism 1939
Table 2. pH, plasma bicarbonate and serum urea during a five-hour cycle dialysis with a 1.1% amino acid solution
Control Meal
T0 T150 T300 T0 T150 T300
pH 7.38 6 0.01 7.39 6 0.01 7.38 6 0.01 7.39 6 0.01 7.39 6 0.02 7.40 6 0.02Bicarbonate mmol /liter 23.6 6 0.6 23.2 6 0.3 23.2 6 0.6 23.2 6 0.9 23.5 6 0.8 23.6 6 0.7Urea mmol /liter 21.5 6 2.2 22.1 6 2.5 23.2 6 3.2 23.1 6 3.1
accounting for 59 and 58% of the amount of leucine to protein synthesis. In addition, the ingestion of a carbo-hydrate-lipid meal inhibits proteolysis.absorbed through the peritoneum. Exogenous leucine
oxidation (Fig. 5C) increased abruptly and achieved a Following the intraperitoneal administration of thedialysis solution, leucine concentrations in dialysate de-peak at 0.18 6 0.05 and at 0.21 6 0.04 mmol · kg · min21
at 120 minutes in the control study and the meal study, creased rapidly to tend toward a plateau after five hours.At this time, 80% of the amount of leucine brought byrespectively. Cumulated exogenous leucine oxidationthe solution had been absorbed through the peritoneum,amounted to 2 6 0.4 (control study) versus 2.4 6 0.3which is in accordance with previous data [11]. The basalmol · 5 hr21 (meal study, P 5 NS), accounting for 16 andtotal rate of leucine appearance was similar to this re-18%, respectively, of the amount of leucine absorbed.ported in normal subjects [19] and in CAPD patientsExogenous nonoxidative leucine disposal (Fig. 5D)[23]. The peritoneal absorption of amino acids stimulatedachieved a peak at 0.74 6 0.14 mmol · kg · min21 at 60whole body protein turnover, as indicated by the sharpminutes in the control study and at 0.67 6 0.10 mmol ·increase in the total rate of leucine appearance. Thiskg · min21 at 45 minutes in the meal study. Cumulativestimulation of Ra leucine was mainly explained by theExo Leunon-ox amounted to 5.4 6 1 (control study) versusdramatic increase in rate of entry of leucine from dialy-5.2 6 0.9 mol·5 hr21 (meal study, P 5 NS), accountingsate. In fact, Raexo described the same kinetics as Ra,for 43 and 40%, respectively, of the amount of leucineincreasing abruptly to reach a peak at 90 minutes beforeabsorbed.decreasing progressively. The initial abrupt rise can beEndogenous leucine Ra (proteolysis). Endogenousexplained by a rapid absorption of leucine driven by theleucine Ra increased shortly from 1.63 6 0.15 mmol · kg ·high concentration gradient between dialysis solutionmin21 at baseline to 1.91 6 0.18 mmol · kg · min21 at 15and blood during this period. Cumulative Raexo over theminutes before returning to baseline in the control study.five hours of the cycle dialysis accounted for 59% of theIn the meal study Raendo increased from 1.67 6 0.09 mmol ·amount of leucine absorbed through the peritoneum.kg · min21 at baseline to 1.76 6 0.14 mmol · kg · min21
Thus, 41% of the leucine absorbed was retained in theat 45 minutes. From 210 to 300 minutes, Raendo was lowersplanchnic bed, that is, peritoneum and/or liver duringthan at baseline (P , 0.05). Endogenous leucine Ra inthe same period. This is somewhat higher than the 25comparison to baseline (Fig. 6) was lower from 210 toto 30% splanchnic extraction usually reported for leucine300 minutes during meal study as compared with theafter a continuous or a bolus meal [24]. The differencecontrol study (P , 0.05).might be explained by an underestimation of Raexo, whichSplanchnic leucine extraction. Splanchnic leucine ex-did not return to baseline values at the end of the studies,traction, that is, liver and/or peritoneum extractions wasand/or by a sequestration of some leucine in the perito-5.0 6 0.9 (control study) versus 5.4 6 0.7 mmol · 5 hr21
neal membrane.(meal study, P 5 NS), accounting for 43 and 40%, respec-A striking result of this study is that the main portiontively, of the amount of leucine absorbed through the
(43%) of absorbed leucine was nonoxidized, that is, wasperitoneum.used for protein synthesis, whereas only 16% was oxi-The leucine balance over the five-hour cycle dialysisdized over the five hours of the cycle dialysis. Naturally,is found in Table 3.because neither Exo Leuox nor Exo Leunon-ox returned tobaseline at the end of the five hours of the cycle dialysis,
DISCUSSION this repartition could have changed if the cycle of dialysisbeen longer than five hours. However, a duration of fiveThe objectives of this study were to evaluate the acute
effects of a 1.1% amino acid dialysis solution, associated hours for a cycle dialysis appears to be reasonable froma practical point of view in CAPD patients. In fact, ator not with the ingestion of a carbohydrate-lipid meal,
on leucine metabolism in CAPD patients. Our data show the fifth hour dialysate leucine concentrations were onlyvery slightly higher than plasma leucine concentrations,that 80% of the leucine contained in the dialysis solution
was absorbed through the peritoneum and contributed so that the dialysis solution has no more osmotic effect

Delarue et al: Peritoneal amino acids and protein metabolism1940
Fig. 4. Kinetics of dialysate (A) and plasma (B) leucine concentrationsafter peritoneal delivery of an 1.1% amino acid solution with (j) orwithout (h) meal ingestion (*P , 0.001).
and should be replaced by another dialysis solution any-way. However, an effect of the amino acid dialysis solu-tion on whole body protein synthesis has not been directlyassessed. This information could have been obtained froma third study using 1-13C-leucine as the intravenoustracer. However, this was ethically difficult in our CAPD
Fig. 3. Kinetics of respiratory quotient (A), carbohydrate oxidationpatients. Boirie et al observed that after a 30 g amino(B), and lipid oxidation (C) after peritoneal delivery of an 1.1% amino
acid solution with (j) or without (h) meal ingestion. acids ingestion in healthy subjects, the increase in total

Delarue et al: Peritoneal amino acids and protein metabolism 1941
Fig. 5. Kinetics of total rate of plasma leucineappearance (Ra; A), exogenous rate of plasmaleucine appearance (B), exogenous leucine oxi-dation (C ), and nonoxidative plasma leucinedisposal (D) after peritoneal delivery of an1.1% amino acid solution with (j) or without(h) meal ingestion (*P , 0.05).
nonoxidative leucine disposal (that is, protein synthesis)was almost solely due to the stimulation of Exo Leunon-ox
[19]. Thus, it is reasonable to speculate that in our study,where Exo Leunon-ox was also strongly stimulated, theamino acid solution would have stimulated total proteinsynthesis. The long-term use of the same 1.1% aminoacid solution in CAPD patients induced a positive pro-tein balance due to an increase in protein synthesis, asassessed by [15N]-glycine excretion [25].
Another observation is that the endogenous proteinbreakdown was not affected by the delivery of the aminoacid solution alone, except during the first 30 minuteswhen it was slightly stimulated. This lack of an inhibitingeffect of the amino acid load has previously been ob-served during the absorption of a single protein meal[19, 26] and differs from what has been reported duringfeeding studies [27]. Hyperinsulinemia and to a lowerextent hyperaminoacidemia [28] inhibit protein break-down. The lack of inhibition of endogenous proteinbreakdown during the control study can be explained bythe very low increase in insulinemia as well as an only
Fig. 6. Kinetics of the endogenous leucine rate of appearance in plasma transient increase in aminoacidemia (leucinemia has been(Raendo) relative to the basal value after peritoneal delivery of a 1.1% considered as grossly representative of aminoacidemia inamino acid solution with (j) or without (h) meal ingestion (*P ,
our study). Indeed, it has been shown that a slowly ab-0.05).sorbed protein inhibits protein breakdown, whereas a

Delarue et al: Peritoneal amino acids and protein metabolism1942
Table 3. Leucine (Leu) balance during a five hour cycle dialysis with a 1.1% amino acid solution
Leu peritdelivered Leu abs Splanch extr Raexo Exo Leuox Exo Leunon-ox
mmol /5 hr
Control 15.6 12.5 6 0.6 5.0 6 0.9 7.5 6 1.2 2.0 6 0.4 5.4 6 1.0Meal 15.6 13.0 6 0.5 5.4 6 0.7 7.6 6 1.0 2.4 6 0.3 5.2 6 0.9
Abbreviations are: Leu perit, leucine delivered into the peritoneum; Leu abs, leucine absorbed through the peritoneum; Splanch extr, splachnic extraction; Raexo,rate of appearance of exogenous leucine (from the dialysate); Exo Leuox, oxidation of exogenous leucine; Exo Leunon-ox, rate of exogenous nonoxidized leucine.
Reprint requests to Jacques Delarue, M.D., Ph.D., Laboratoire dequickly absorbed protein does not [26]. The meal absorp-Nutrition, Hopital Bretonneau 37044-TOURS Cedex, France.
tion did not affect maximal stimulation of protein turn- E-mail: [email protected], but induced its more rapid decrease after the sec-ond hour of the study with a return to baseline value at REFERENCES150 minutes. This more rapid decrease in Ra was entirely
1. Moncrieff JW, Popovich RP: Continuous ambulatory peritonealaccounted for by the inhibition of endogenous protein dialysis best treatment for end-stage renal disease. Kidney Int
28(Suppl 17):S23–S25, 1985breakdown (218%), inasmuch as Raexo was very similar2. Rubin J: Comments on dialysis solution, antibiotic transport, poi-during the two studies. The decrease in endogenous pro- sonings, and novel uses of peritoneal dialysis, in Peritoneal Dialysis,
tein breakdown is consistent with the protein-sparing edited by Nolph KD, Dordrecht, Kluwer Academic, 1988, pp199–229effect of energy substrates [13, 14]. This was probably
3. Delarue J, Maingourd C, Lamisse F, Garrigue MA, Bagros P,mediated in our study by the carbohydrate-induced hy- Couet C: Glucose oxidation after a peritoneal and an oral glucoseload in dialyzed patients. Kidney Int 45:1147–1152, 1994perinsulinemia [13]. Exogenous leucine oxidation calcu-
4. Friedman JE, Dohm GL, Elton CW, Rovira A, Chen JJ, Leggett-lation was performed using a recovery factor of 0.81 inFrazier N, Atkinson SM, Thomas FT, Long DL, Caro JF: Muscle
the two studies. The recovery factor could have de- insulin resistance in uremic humans: Glucose transport, glucosetransporters, and insulin receptors. Am J Physiol 261:E87–E94,creased because of a decrease in gluconeogenesis during1991carbohydrate ingestion. In fact, in two additional experi- 5. Delarue J, Maingourd C, Couet C, Vidal S, Bagros P, Lamisse
ments we verified that the background IE in 13C of ex- F: Effects of oral glucose on intermediary metabolism in CAPDpatients versus healthy subjects. Perit Dial Int 18:505–511, 1998pired CO2 was not affected by meal ingestion. Conse-
6. Ruderman N, Chisholm D, Pi-Sunyer X, Schneider S: Thequently, no correction was applied. The absence of metabolically obese, normal-weight individual revisited. Diabetesvariation of background enrichment may be explained 47:699–713, 1998
7. Lindholm B, Bergstrom J: Nutritional aspects on peritoneal dial-by the fact that liver glycogen stores were repleted be-ysis. Kidney Int 42(Suppl 38):S165–S171, 1992
cause of the high usual glucose intake in CAPD patient 8. Blumenkrantz MJ, Kopple JD, Moran JK, Grodstein GP, Co-burn JW: Nitrogen and urea metabolism during continuous ambu-dialyzed with glucose solutions. On the other hand, thelatory peritoneal dialysis. Kidney Int 20:78–82, 1981increase in metabolic rate caused by the meal ingestion
9. Kopple JD: Protein-energy malnutrition in maintenance dialysisshould have increased the recovery factor. However, patients. Am J Clin Nutr 65:1544–1557, 1997
10. Young GA, Kopple JD, Lindholm B, Vonesh EF, De Vecchi A,when an extreme value of recovery factor of 0.90 wasScalamogna A, Castelnova C, Oreopoulos DG, Anderson GH,used, exogenous leucine oxidation was decreased by Bergstrom J, Dichiro J, Gentle D, Nissenson A, Sakhrani L,
11%, and NOLDexo was increased by 6%. This would Brownjohn AM, Nolph KD, Prowant BF, Algrim CE, MartisL, Serkes KD: Nutritional assessment of continuous ambulatorylead to the superposition of Leuox kinetics and NOLDexoperitoneal dialysis patients: An international study. Am J Kidneybetween the two studies so that the conclusions are not Dis 17:462–471, 1991
affected. 11. Jones MR, Martis L, Algrim CE, Bernard D, Swartz R, Mes-sana J, Bergstrom J, Lindholm B, Lim V, Srkes KD, Vonesh E,In conclusion, we showed that a 1.1% amino acid solu-Kopple JD: Amino acid solutions for CAPD: Rationale and clinical
tion for peritoneal dialysis is efficaciously utilized for experience. Miner Electrolyte Metab 18:309–315, 199212. Richardson DP, Wayler AH, Scrimshaw NS, Young VR: Quan-protein synthesis in CAPD patients with no effect on
titative effect of an isoenergetic exchange of fat for carbohydrateprotein breakdown. The ingestion of a carbohydrate-on dietary protein utilization in healthy young men. Am J Clin
lipid meal during a cycle dialysis with that solution inhib- Nutr 32:2217–2226, 197913. Krempf M, Hoerr RA, Pelletier VA, Marks LM, Gleason R,its protein breakdown and reinforces a positive effect of
Young VR: An isotopic study of the effect of dietary carbohydratethe amino acid solution on protein balance. on the metabolic fate of dietary leucine and phenylalanine. Am JClin Nur 57:161–169, 1993
14. Nissen SL, Van Huysen C, Haymond MW: Measurement ofACKNOWLEDGMENTSbranched chain amino acids and branched chain a-ketoacids in
This work was supported by a grant from Baxter, France. The plasma by high-performance liquid chromatography. J Chromatogrinvaluable technical help of Mrs. Catherine Girard was deeply appreci- 232:170–175, 1982ated. We thank Professor Bernard Beaufrere for helpful discussion of 15. Schwenk WF, Berg PJ, Beaufrere B, Miles JM, Haymond MW:
Use of t-butyldimethylsilylation in the gas chromatographic/massthis manuscript.

Delarue et al: Peritoneal amino acids and protein metabolism 1943
spectrometric analysis of physiologic compounds found in plasma 22. Jequier E, Acheson K, Schutz Y: Assessment of energy expendi-ture and fuel utilization in man. Ann Rev Nutr 7:187–208, 1987using electron-impact ionization. Anal Biochem 141:101–109, 1984
23. Goodship THJ, Lloyd S, Clague MB, Bartlett K, Ward MK,16. Biolo G, Tessari P, Inchiostro S, Bruttomesso D, Fongher C,Wilkinson R: Whole body leucine turnover and nutritional statusSabadin L, Fratton MG, Valerio A, Tiengo A: Leucine andin continuous ambulatory peritoneal dialysis. Clin Sci 73:463–469,phenylalanine kinetics during mixed meal ingestion: A multiple1987tracer approach. Am J Physiol 262:E455–E463, 1992
24. Tessari P, Biolo G, Barazzoni R, Zanetti M: The role of the17. Steele R, Wall JS, De Bodo RC, Altszuler N: Measurement splanchnic bed in the regulation of amino acid and protein metabo-of size and turn over rate of body glucose pool by the isotope lism. Endocrinol Metab 2:77–91, 1995dilution method. Am J Physiol 187:15–24, 1956 25. Kopple JD, Bernard D, Messana J, Swartz R, Bergstrom J,
18. Proietto J, Rohner-Jeanrenaud F, Ionescu E, Terretaz J: Non Lindholm B, Lim V, Brunori G, Leiserowitz M, Bier DM, Steg-steady state measurement of glucose turnover in rats by a one- ink LD, Martis L, Boyle CA, Serkes KD, Vonesh E, Jones MR:compartment model. Am J Physiol 252:E77–E84, 1987 Treatment of malnourished CAPD patients with an amino acid
based dialysate. Kidney Int 47:1148–1157, 199519. Boirie Y, Gachon P, Corny S, Fauquant J, Maubois JL, Beau-26. Boirie Y, Dangin M, Gachon P, Vasson MP, Maubois JL, Beau-frere B: Acute post-prandial changes in leucine metabolism as
frere B: Slow and fast dietary proteins differently modulate post-assessed with an intrinsically labeled milk protein. Am J Physiolprandial protein accretion. Proc Natl Acad Sci USA 94:14930–271:E1083–E1091, 199614935, 199720. Hoerr RA, Yu YM, Wagner DA, Burke JF, Young VR: Recov-
27. Waterlow JC: Whole-body protein turnover in humans: Past,ery of 13C in breath from NaH13CO3 infused by gut and vein: Effect present, and future. Annu Rev Nutr 15:57–92, 1995of feeding. Am J Physiol 257:E426–E438, 1989 28. Castellino P, Luzi L, Simonson D, Haymond MW, DeFronzo
21. Livesey G, Elia M: Estimation of energy expenditure, net carbohy- RA: Effect of insulin and plasma amino acid concentrations ondrate utilization, and net fat oxidation and synthesis by indirect leucine metabolism in man: Role of substrate availability on esti-calorimetry: Evaluation of errors with special reference to the mates of whole body protein synthesis. J Clin Invest 80:1784–1793,
1987detailed composition of fuels. Am J Clin Nutr 47:608–628, 1988