Embed Size (px)
Citation preview
Original article
Effects of deflazacort immunosuppression on long-term growthand growth factors after renal transplantation
Jorge R. Ferraris1, Patricia Pennisi3, Titania Pasqualini2, and Hector Jasper3
1 Servicio de Nefrologia Pediatrica and2 Seccion de Endocrinologia, Creciminiento y Desarrollo, Hospital Italiano de Buenos Aires,Buenos Aires, Argentina3 Division Endocrinologı´a, Hospital de Nin˜os Ricardo Gutierrez, Buenos Aires, Argentina
Received May 13, 1996; received in revised form and accepted November 20, 1996
Abstract. Deflazacort is an oxazoline compound derivedfrom prednisolone. We studied changes in kidney function,growth velocity, weight/height ratio, insulin-like growthfactor (IGF-I), and IGF binding proteins before and aftersubstitution of deflazacort for methylprednisone in 27transplanted patients aged 3.1–20 years. Methylprednisone(mean+SEM 0.17+0.01 mg/kg per day) was replaced bydeflazacort (0.29+0.01 mg/kg per day) for a period of 1–5years. Calculated creatinine clearance did not change sig-nificantly during deflazacort treatment. Growth velocityincreased from 2.6+0.5 cm/year to 5.2+0.7 cm/year (1styear) in 14 prepubertal patients. After 4 years of deflazacorttreatment, height standard deviation score for chronologicalage did not change in 7 prepubertal patients. Mean weight/height ratio decreased by 50% (1st year) and remainedreduced during follow-up. Serum IGF-I, IGF binding pro-tein -3 (IGFBP3), IGF/IGFBP3 molar ratio, and IGF-I and-II binding capacities showed no significant change; how-ever in 5 of 6 patients IGFBP2 decreased during deflazacorttherapy. Our findings suggest that immunosuppressivetreatment with deflazacort is as effective as methylpredni-sone and may lead to an improvement in the growthprognosis of children with renal transplantation.
Key words:mGrowth – Insulin-like growth factor-I –Insulin-like growth factor binding proteins – Renalfailure – Renal transplantation – Deflazacort
Introduction
Deflazacort is an oxazoline analogue of prednisolone [1, 2]with fewer effects on calcium, phosphate, and glucosemetabolism at doses equally effective for antiinflammatoryand immunosuppressive responses [3]. In a recent study of
nine children who underwent successful renal transplanta-tion, a shift from maintenance dosage of methylprednisoneto an equivalent dosage of deflazacort resulted in an in-crease in serum growth hormone (GH) and linear growthvelocity, and a decrease in weight/height ratio and cush-ingoid appearance. Moreover, renal function remainedstable and no rejection episodes could be documentedduring 15 months of deflazacort therapy [4].
This report represents an update of our earlier paper [4],including a larger cohort of patients followed for a muchlonger period. We have also evaluated the insulin-likegrowth factor-I (IGF-I)/IGF binding proteins axis aftersubstitution of deflazacort for methylprednisone.
Patients and methods
Twenty seven patients, 21 boys and 6 girls, were studied (9 have beenreported previously [4]). Mean age at transplantation was 10.4 years(range 1.6–18.8 years); mean age at the start of the study was13.9 years (range 3.1–20.4 years). Fourteen were at Tanner pubertalstage I, 6 at Tanner stage III/IV, and 7 at Tanner stage V. Elevenchildren completed 5 years of deflazacort therapy. Long-term growthwas evaluated in 7 of those who remained at Tanner stage I. All hadstable renal function for at least 1 year before the study. Im-munosuppressive treatment of 6 patients included azathioprine andmethylprednisone, whereas the remaining 21 received triple therapywhich also included cyclosporine.
Treatment protocol.The mean (+SEM) maintenance dosage of orallyadministered methylprednisone before the start of the study was0.17+0.01 mg/kg per day (range 0.1–0.28 mg/kg per day). This wasreplaced by a mean dosage of 0.29+0.01 mg/kg per day (range0.18–0.4 mg/kg per day) of deflazacort (Azacortid, Lepetit, BuenosAires, Argentina). The replacement dosage was calculated by assum-ing the equivalence of 1 mg methylprednisone to 1.5 mg deflazacort[2]. The deflazacort treatment protocol was approved by the ethicscommittee of the Hospital Italiano. Assent was obtained from thechildren studied and informed consent was signed by the parents.Pubertal status, weight, and height were evaluated as described pre-viously, by the same trained observer at 3-month intervals [4].
Laboratory studies.We performed laboratory studies before and after6 months of deflazacort therapy in 12 patients. At the start of the study,
Correspondence to:J. R. Ferraris, Avenida Santa Fe 2664/1 “A”,1425 Buenos Aires, Argentina
Pediatr Nephrol (1997) 11: 322–324 IPNA 1997
the mean age was 14.5 years [range 3.1–20.3 years, Tanner stage I(n = 5), III–V (n = 7)]. The following serum determinations wereperformed: IGF-I, IGF binding protein 3 (IGFBP3), total IGF bindingcapacities, and western ligand blots of the IGF binding proteins. Serumcreatinine concentrations and calculated creatinine clearances(Schwartz formula) were determined monthly during the follow-upperiod.
IGF-I was determined by radioimmunoassay after C18 Sep Pak(Waters, Mass., USA) acid extraction of the serum IGF bindingproteins. Human recombinant IGF-I (Bachem, Calif., USA) was usedfor standard and tracer. The UBK 487 IGF-I antibody was kindlyprovided by Dr. L. E. Underwood. IGFBP3 was measured by im-munoradiometric assay (DSL, Webster, Tex., USA). Total IGF bindingcapacities were determined according to Cailleau et al. [5]. Thewestern ligand blots were performed according to Hossenlopp et al.[6]. Local normal ranges according to chronological age are as follows:IGF-I: 3–7 years, 46–225µg/l; 7–11 years, 61–409µg/l; 11–15years, 119–483µg/l; 18–30 years, 107–371µg/l; IGFBP3: 3–7years, 1.3–3.7 mg/l; 7–11 years, 1.6–5.0 mg/l; 11–15 years,2.1–7.4 mg/l; 18–30 years, 1.3–3.9 mg/l; IGF-I/IGFBP3 molarratio: 1–7 years, 0.05–0.28; 7–11 years, 0.09–0.35; 11–15 years,0.19–0.40; 18–30 years, 0.16–0.72; IGF-I binding capacity: prepu-bertal, 2.16%–9.32%/5µl; pubertal, 5.39%–10.74%/5µl; IGF-IIbinding capacity: prepubertal 1.87%–6.15%/0.5µl; pubertal,5.27%–9.77%/0.5µl.
Statistical analysis.Results were analyzed by paired and unpairedStudent’st-tests and linear regression, as appropriate. Values are re-ported as mean and ranges or as mean+SEM; P50.05 was consid-ered statistically significant.
Results
Graft function
The mean total duration of deflazacort substitution was2.7 years (range 1–5 years). The serum creatinine andcalculated creatinine clearance did not change significantlyduring the 1st year of deflazacort therapy: 1.3+0.1 mg/dland 72.0+5.5 ml/min per 1.73 m2, versus 1.2+0.1 mg/dland 72.2+4.9 ml/min per 1.73 m2 with conventional glu-cocorticoid treatment (n = 27). Moreover, calculated crea-tinine clearance in 11 children before and after 5 years of
deflazacort therapy did not change significantly:72.0+6.6 ml/min per 1.73 m2 versus 65.0+7.5 ml/min per1.73 m2, respectively. In addition, no acute rejection epi-sodes could be documented in the 27 patients throughoutthe 2.7+0.4 years of deflazacort therapy.
Growth evaluation
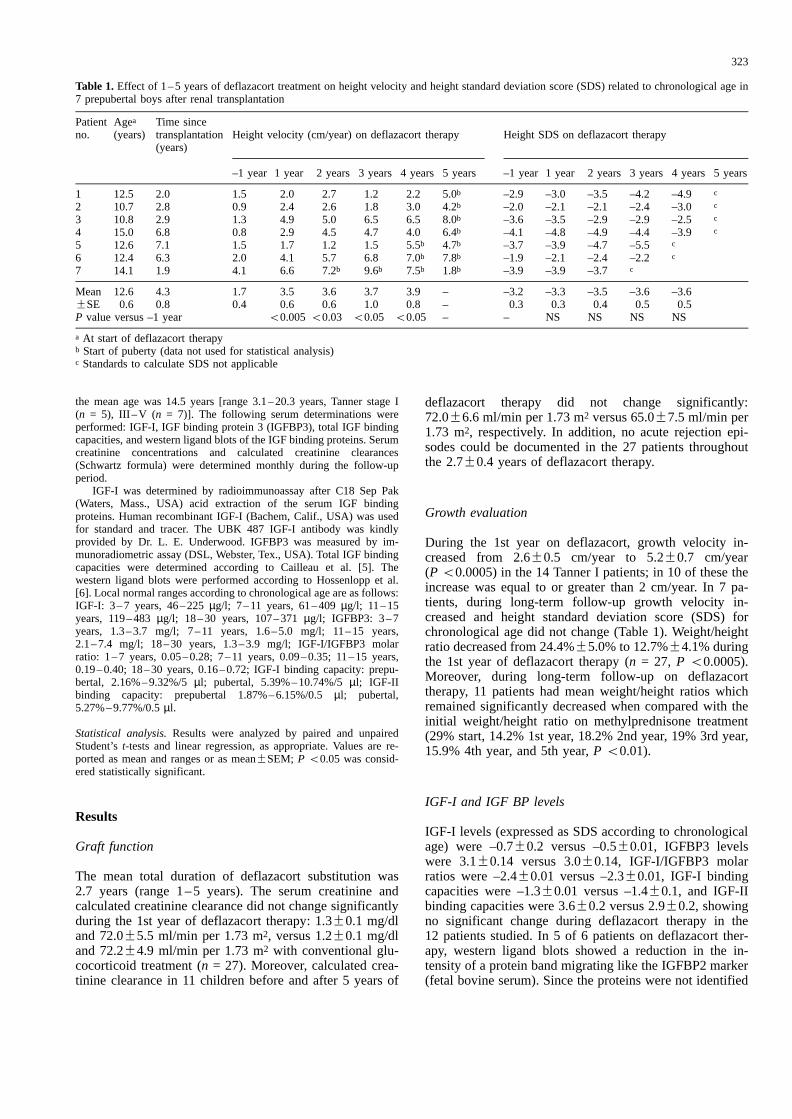
During the 1st year on deflazacort, growth velocity in-creased from 2.6+0.5 cm/year to 5.2+0.7 cm/year(P50.0005) in the 14 Tanner I patients; in 10 of these theincrease was equal to or greater than 2 cm/year. In 7 pa-tients, during long-term follow-up growth velocity in-creased and height standard deviation score (SDS) forchronological age did not change (Table 1). Weight/heightratio decreased from 24.4%+5.0% to 12.7%+4.1% duringthe 1st year of deflazacort therapy (n = 27, P 50.0005).Moreover, during long-term follow-up on deflazacorttherapy, 11 patients had mean weight/height ratios whichremained significantly decreased when compared with theinitial weight/height ratio on methylprednisone treatment(29% start, 14.2% 1st year, 18.2% 2nd year, 19% 3rd year,15.9% 4th year, and 5th year,P50.01).
IGF-I and IGF BP levels
IGF-I levels (expressed as SDS according to chronologicalage) were –0.7+0.2 versus –0.5+0.01, IGFBP3 levelswere 3.1+0.14 versus 3.0+0.14, IGF-I/IGFBP3 molarratios were –2.4+0.01 versus –2.3+0.01, IGF-I bindingcapacities were –1.3+0.01 versus –1.4+0.1, and IGF-IIbinding capacities were 3.6+0.2 versus 2.9+0.2, showingno significant change during deflazacort therapy in the12 patients studied. In 5 of 6 patients on deflazacort ther-apy, western ligand blots showed a reduction in the in-tensity of a protein band migrating like the IGFBP2 marker(fetal bovine serum). Since the proteins were not identified
323
Table 1. Effect of 1–5 years of deflazacort treatment on height velocity and height standard deviation score (SDS) related to chronological age in7 prepubertal boys after renal transplantation
Patientno.
Agea
(years)Time sincetransplantation(years)
Height velocity (cm/year) on deflazacort therapy Height SDS on deflazacort therapy
–1 year 1 year 2 years 3 years 4 years 5 years –1 year 1 year 2 years 3 years 4 years 5 years
1 12.5 2.0 1.5 2.0 2.7 1.2 2.2 5.0b –2.9 –3.0 –3.5 –4.2 –4.9 c
2 10.7 2.8 0.9 2.4 2.6 1.8 3.0 4.2b –2.0 –2.1 –2.1 –2.4 –3.0 c
3 10.8 2.9 1.3 4.9 5.0 6.5 6.5 8.0b –3.6 –3.5 –2.9 –2.9 –2.5 c
4 15.0 6.8 0.8 2.9 4.5 4.7 4.0 6.4b –4.1 –4.8 –4.9 –4.4 –3.9 c
5 12.6 7.1 1.5 1.7 1.2 1.5 5.5b 4.7b –3.7 –3.9 –4.7 –5.5 c
6 12.4 6.3 2.0 4.1 5.7 6.8 7.0b 7.8b –1.9 –2.1 –2.4 –2.2 c
7 14.1 1.9 4.1 6.6 7.2b 9.6b 7.5b 1.8b –3.9 –3.9 –3.7 c
Mean 12.6 4.3 1.7 3.5 3.6 3.7 3.9 – –3.2 –3.3 –3.5 –3.6 –3.6+SE 0.6 0.8 0.4 0.6 0.6 1.0 0.8 – 0.3 0.3 0.4 0.5 0.5P value versus –1 year 50.00550.03 50.05 50.05 – – NS NS NS NS
a At start of deflazacort therapyb Start of puberty (data not used for statistical analysis)c Standards to calculate SDS not applicable

by immunoblots, we can only infer this band corresponds toIGFBP2.
Discussion
We have previously reported [4] that in prepubertal chil-dren who underwent renal transplantation the change frommethylprednisone to deflazacort increased height velocity,decreased weight/height ratios, and cushingoid appearance,with no change in the renal function during the first15 months of follow-up. We now report that in a largercohort these advantages persist during a 5-year follow-up.Switching from methylprednisone to deflazacort was notassociated with the appearance of any signs of rejection.Moreover, the serum creatinine concentration did notchange significantly during the 1st year of deflazacorttherapy, and calculated creatinine clearance remainedstable after 5 years of treatment.
In the short term, the change from methylprednisone todeflazacort increased height velocity more than 2 cm/year(growth acceleration). During 4 years of deflazacort treat-ment, height SDS for chronological age did not change inprepubertal patients. Therefore, these patients did not losestature, which did occur in patients treated with methyl-prednisone [7]. After 1 year of deflazacort treatment, theweight/height ratio decreased by a mean of 50% and re-mained significantly reduced during 5 years of long-termfollow-up. The patients also showed a decrease in theircushingoid appearance.
During deflazacort therapy the mean nocturnal GH se-cretion increased significantly [4] and the GH response toarginine and GH releasing hormone (to be published) be-came normal in most patients. In addition, the improvednocturnal GH secretion correlated with the increase inlinear growth velocity in prepubertal patients. In the presentreport the favorable anthropometric changes were recordeddespite the absence of significant variation in the circulat-ing levels of IGF-I, IGFBP3, the IGF-I/IGFBP3 molarratio, and IGF-I and -II binding capacities. Nevertheless,given the small contribution of the local production of IGFsby cartilage to serum levels [8], an increase at the targetorgan level, diluted in serum by the stable contribution ofother tissues, could not be entirely ruled out.
Since Smith et al. [9] showed elevated IGFBP2 levels inGH-deficient children, and Vicini et al. [10] showed a re-duction in IGFBP2 levels after administration of GH tocattle, the decrease we noted in the presumed IGFBP2 ofour western ligand blots is compatible with the increasedGH secretion we previously reported in these patients [4].
Our data suggest that substituting deflazacort formaintenance methylprednisone therapy may lead to a sus-tained improvement in the growth prognosis of childrenwith successful renal transplantation, but additional andlarger prospective controlled trials are necessary beforewidespread use of this corticosteroid after organ trans-plantation in children can be advocated.
Acknowledgements.We thank Daniel Flores M.D. (Lepetit, Pharma-ceutical Division of Dow Quimica Argentina) for financial support,Silvina Gonzalez for technical assistance, and Ms. Mabel Isoldi forsecretarial assistance.
References
1. Nathanson G, Winter G, Testa E (1967) Steroids possessing ni-trogen atoms. III. Synthesis of new highly active corticoids: [17-alpha, 16 alpha-d] oxazolino steroids. J Med Chem 10: 799–802
2. Assandri A, Buniva G, Martinelli E, Perazzi A, Zerelli L (1984)Pharmacokinetics and metabolism of deflazacort in the rat, dog,monkey and man. Adv Exp Med Biol 171: 9–23
3. Hahn B, Pletscher S, Muniain M (1981) Immunosuppressive ef-fects of deflazacort: a new glucocorticoid with bone-sparing andcarbohydrate-sparing properties – comparison with prednisone.J Rheumatol 8: 783–790
4. Ferraris J, Fainstein Day P, Gutman R, Granillo E, Ramirez J,Ruiz S, Pasqualini T (1992) Effect of therapy with a new gluco-corticoid, deflazacort, on linear growth and growth hormone se-cretion after renal transplantation. J Pediatr 121: 809–813
5. Cailleau J, Vermeire S, Verhoeven (1990) Independent control ofthe production of insulin-like growth factor-I and its bindingprotein by cultured testicular cells. Mol Cell Endocrinol 69:79–89
6. Hossenlopp P, Seurin D, Segovia-Quinson B, Hardovin S,Binoux M (1986) Analysis of serum insulin-like factor bindingproteins using western-ligand blotting: use of the method for ti-tration of the binding proteins and competitive binding studies.Anal Biochem 154: 138–143
7. Ferraris JR, Ramirez JA, Lejarraga H (1988) Crecimiento en pa-cientes con transplante renal. Bol Med Hosp Infant Mex 45:485–490
8. D’Ercole AJ, Stiles AD, Underwood LE (1984) Tissue con-centrations of somatomedin C: further evidence for multiple sitesof synthesis and paracrine or autocrine mechanisms of action. ProcNatl Acad Sci USA 81: 935–939
9. Smith WJ, Nam, TJ, Underwood LE, Busbee WH, Celnicker A,Clemmons DR (1993) Use of insulin-like growth factor bindingprotein-2 (IGFBP2), IGFBP3, and IGF-I for assessing growthhormone status in short children. J Clin Endocrinol Metab 77:1294–1299
10. Vicini JL, Buonomo FC, Veenhuizen JJ, Miller MA, ClemmonsDR, Collier RJ (1991) Effects of nutritional balance and stage oflactation in dairy cows on insulin, insulin-like growth factor-I and-II and insulin-like growth factor binding protein 2 responses tosematotropin administration. J Nutr 121: 1656–1664
324