Embed Size (px)
Citation preview
Effects of Fixed-Dose Isosorbide Dinitrate/Hydralazine onDiastolic Function and Exercise Capacity in
Hypertension-Induced Diastolic Heart FailureRichard M. Wilson, Deepa S. De Silva, Kaori Sato, Yasuhiro Izumiya, Flora Sam
Abstract—Hypertension-induced diastolic heart failure accounts for a large proportion of all heart failure presentations.Hypertension also induces left ventricular (LV) hypertrophy. Fixed-dose isosorbide dinitrate/hydralazine (HISDN)decreased mortality in human systolic heart failure but it is unknown whether it improves maladaptive myocardialremodeling. We sought to test the hypothesis that chronic HISDN modulates LV hypertrophy and myocardialremodeling in hypertension-induced diastolic heart failure. FVB mice underwent either saline (n�18) or aldosterone(n�28) infusion. All underwent uninephrectomy and drank 1% salt water for 4 weeks. Mice were randomized aftersurgery to regular chow or chow containing HISDN (isosorbide dinitrate: 26 mg/kg per day; hydralazine: 50 mg/kg perday) for 4 weeks. Aldosterone infusion increased tail-cuff blood pressure (161�3 mm Hg) versus saline-infused mice(129�2 mm Hg). Aldosterone induced LV hypertrophy versus saline-infused mice (LV:body weight ratio: 4.2�0.1versus 3.6�0.1 mg/g). HISDN attenuated the aldosterone-induced increased in systolic blood pressure (137�5 mm Hg)and also lowered blood pressure in saline-infused mice (114�2 mm Hg). However, HISDN did not cause LVhypertrophy regression in aldosterone-infused mice. Aldosterone increased LV end-diastolic dimensions that were notattenuated by HISDN. Similarly, neither aldosterone infusion nor HISDN affected LV end-systolic dimensions. LVejection fraction and wet:dry lung ratio were not different between aldosterone-untreated and aldosterone-HISDN mice.However, mitral Doppler E/A ratio (a measure of diastolic function), exercise capacity, and plasma soluble vascular celladhesion molecule 1 levels were improved in aldosterone-HISDN hearts. In conclusion, fixed-dose HISDN improvedhypertension, diastolic function, and exercise capacity and reduced soluble vascular cell adhesion molecule 1 levels.There were no reductions in LV hypertrophy, cardiac fibrosis, or pulmonary congestion. These functional improvementsare likely related to extracardiac effects, such as effects on the vasculature. (Hypertension. 2009;54:583-590.)
Key Words: diastolic heart failure � hydralazine � nitrates � hypertension � exercise capacity
Hypertension induces left ventricular (LV) hypertrophy(LVH) and is a major cause of both diastolic and
systolic heart failures (HF).1 Diastolic HF accounts for up to�50% of all HF presentations2 and is associated withincreasing morbidity and mortality.3 Diastolic HF refers tothe clinical syndrome of pulmonary congestion in the pres-ence of a normal LV ejection fraction, whereas diastolicdysfunction denotes an abnormality of mechanical propertiesthat exist during LV relaxation and filling.4,5 Diastolic dys-function may be an intermediary between hypertension andHF.6 In the setting of hypertension, diastolic HF represents adiverse clinical syndrome with various associated comorbidi-ties (eg, age and sex) and manifests a spectrum of symptomsranging from exercise intolerance to acute pulmonary edema.In addition to LVH, cardiac fibrosis, altered myocyte calciumhandling,7 and ventricular-vascular stiffening plays a signif-icant role in the pathophysiology of diastolic HF.7
In the African-American Heart Failure Trial (AHeFT),fixed-dose isosorbide dinitrate and hydralazine (HISDN)reduced mortality in black patients with advanced systolicHF.8,9 The predominant cause of HF in AHeFT was hyper-tension.9 Benefits of HISDN are partially derived from nitricoxide (NO),10 which results in vasorelaxation, inhibition ofcardiac hypertrophy,11 and improved cardiac remodeling.11–13
Unfortunately the use of NO donors is limited by thedevelopment of tolerance. With HISDN, the component ofhydralazine (a potent antioxidant) is thought to diminish NOconsumption by reactive oxygen species14,15 and reactivenitrogen species.16 The survival benefits seen in AHeFT werereported to be attributed to myocardial effects, because LVejection fraction improved, and LV mass was reduced.17
However, there are no experimental studies thus far that testthis hypothesis. We, therefore, sought to test the hypothesisthat chronic fixed-dose HISDN modulates LVH and adversemyocardial remodeling in hypertension-induced diastolic HF.
Received April 20, 2009; first decision May 12, 2009; revision accepted June 17, 2009.From the Whitaker Cardiovascular Institute (R.M.W., D.S.D.S., K.S., Y.I., F.S.), Cardiovascular Section (F.S.), and Evans Department of Medicine
(F.S.), Boston University School of Medicine, Boston, Mass.Correspondence to Flora Sam, Whitaker Cardiovascular Institute, Boston University School of Medicine, Evans Department of Medicine and
Cardiovascular Section, 715 Albany St, Room W507, Boston, MA 02118. E-mail [email protected]© 2009 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.109.134932
583
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
Methods and MaterialsAn expanded Materials and Methods section is available in theonline Data Supplement at http://hyper.ahajournals.org. Ten-week–old male FVB mice (Charles River) were maintained on a 12-hourlight/dark cycle in a temperature-controlled (19°C to 21°C) room.Mice were fed standard rodent chow ad libitum. The BostonUniversity School of Medicine Institutional Animal Care and UseCommittee approved all of the study procedures related to handlingand surgery of the mice.
ResultsHISDN Improved Hypertension But Had NoEffect on Cardiac HypertrophyAll of the mice survived (Table 1). HISDN prevented thealdosterone-induced increase in systolic blood pressure (SBP;137�5 versus 161�3 mm Hg; P�0.001). Heart rate tendedto be lower with aldosterone infusion but was unaffected byHISDN. The body weight (BW) of all of the HISDN-treatedmice was increased; therefore, morphological measurementswere normalized to BW. This was attributed to the HISDN-chow being made with lactose. Aldosterone caused LVH, asshown by an increase in the LV weight:BW ratio (4.2�0.1).However, despite the reduction in SBP in aldosterone-HISDNmice, there was no decrease in the LV weight:BW ratio.Cardiomyocyte cross-sectional area was increased in re-sponse to aldosterone infusion. Similar to the LV weight:BWratio, cardiomyocyte hypertrophy was no different betweenaldosterone-untreated and aldosterone-HISDN hearts. Aldo-sterone infusion induced pulmonary congestion that wasunaffected by HISDN.
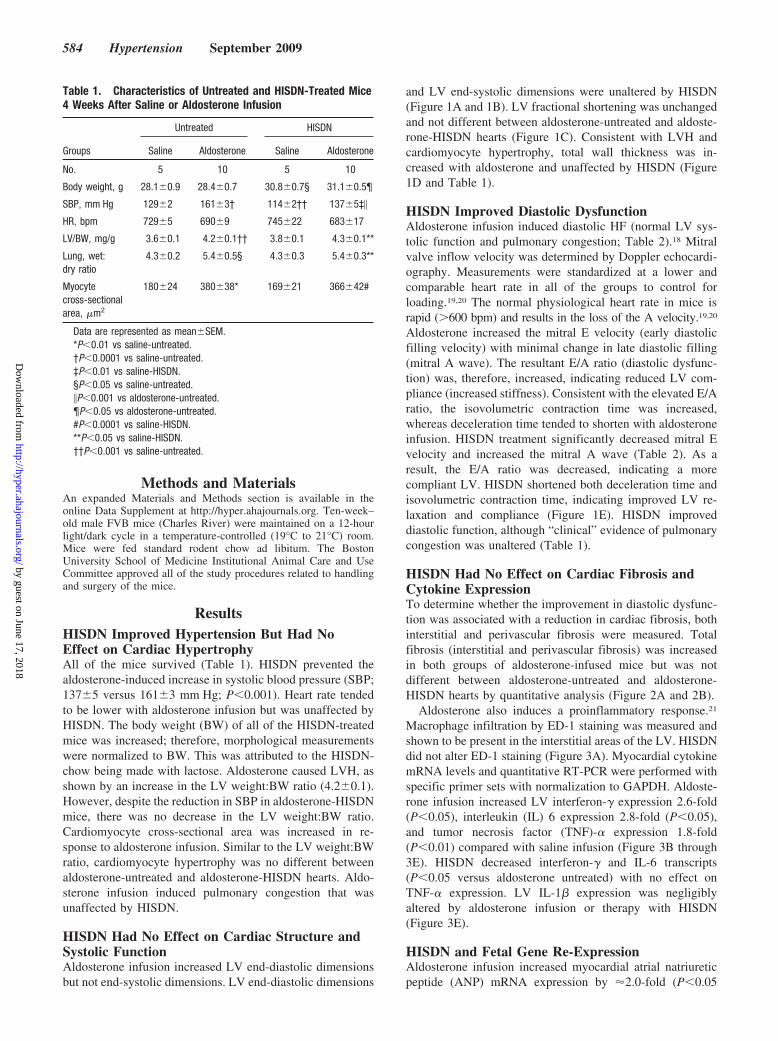
HISDN Had No Effect on Cardiac Structure andSystolic FunctionAldosterone infusion increased LV end-diastolic dimensionsbut not end-systolic dimensions. LV end-diastolic dimensions
and LV end-systolic dimensions were unaltered by HISDN(Figure 1A and 1B). LV fractional shortening was unchangedand not different between aldosterone-untreated and aldoste-rone-HISDN hearts (Figure 1C). Consistent with LVH andcardiomyocyte hypertrophy, total wall thickness was in-creased with aldosterone and unaffected by HISDN (Figure1D and Table 1).
HISDN Improved Diastolic DysfunctionAldosterone infusion induced diastolic HF (normal LV sys-tolic function and pulmonary congestion; Table 2).18 Mitralvalve inflow velocity was determined by Doppler echocardi-ography. Measurements were standardized at a lower andcomparable heart rate in all of the groups to control forloading.19,20 The normal physiological heart rate in mice israpid (�600 bpm) and results in the loss of the A velocity.19,20
Aldosterone increased the mitral E velocity (early diastolicfilling velocity) with minimal change in late diastolic filling(mitral A wave). The resultant E/A ratio (diastolic dysfunc-tion) was, therefore, increased, indicating reduced LV com-pliance (increased stiffness). Consistent with the elevated E/Aratio, the isovolumetric contraction time was increased,whereas deceleration time tended to shorten with aldosteroneinfusion. HISDN treatment significantly decreased mitral Evelocity and increased the mitral A wave (Table 2). As aresult, the E/A ratio was decreased, indicating a morecompliant LV. HISDN shortened both deceleration time andisovolumetric contraction time, indicating improved LV re-laxation and compliance (Figure 1E). HISDN improveddiastolic function, although “clinical” evidence of pulmonarycongestion was unaltered (Table 1).
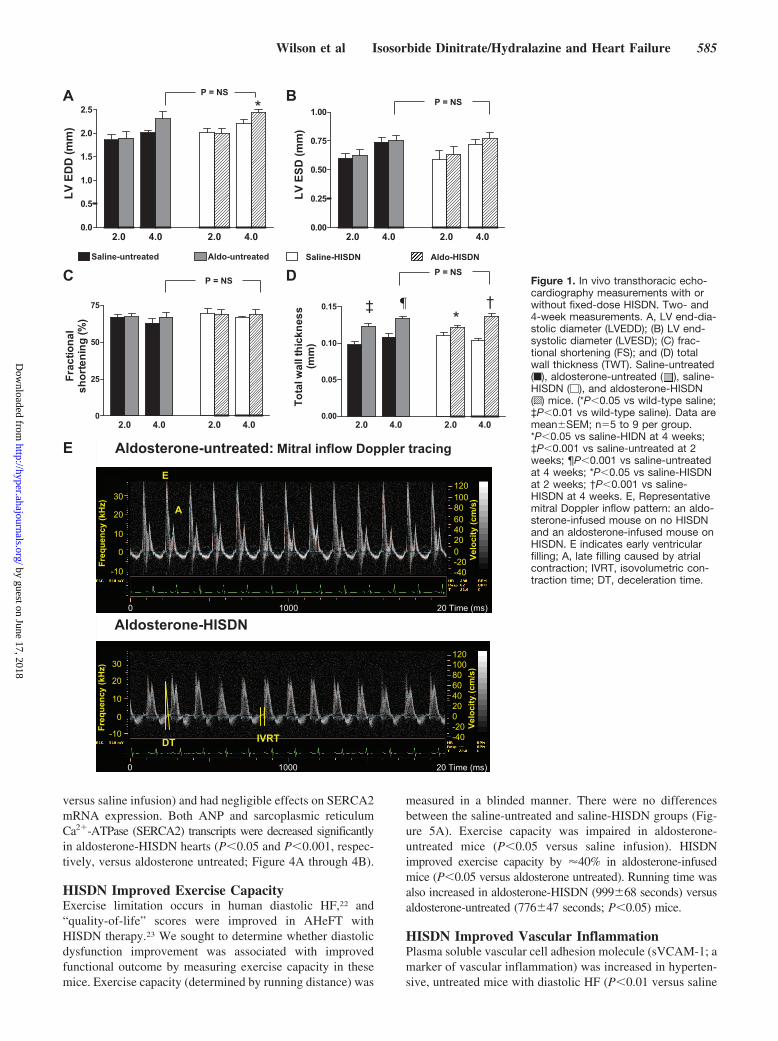
HISDN Had No Effect on Cardiac Fibrosis andCytokine ExpressionTo determine whether the improvement in diastolic dysfunc-tion was associated with a reduction in cardiac fibrosis, bothinterstitial and perivascular fibrosis were measured. Totalfibrosis (interstitial and perivascular fibrosis) was increasedin both groups of aldosterone-infused mice but was notdifferent between aldosterone-untreated and aldosterone-HISDN hearts by quantitative analysis (Figure 2A and 2B).
Aldosterone also induces a proinflammatory response.21
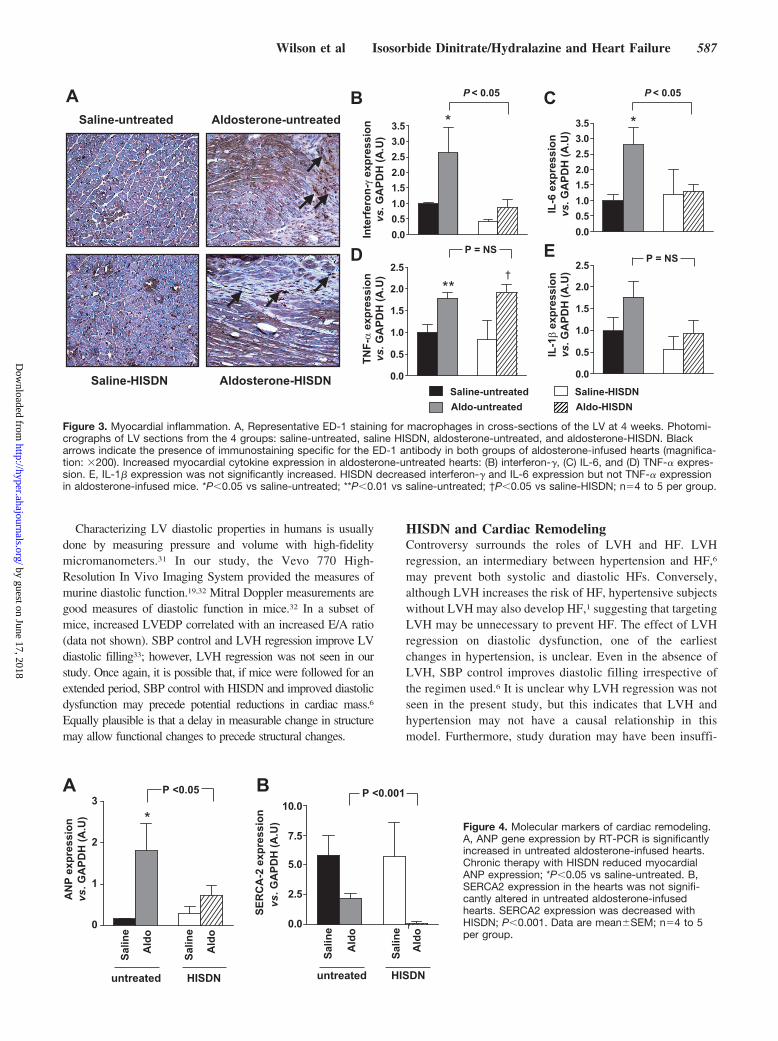
Macrophage infiltration by ED-1 staining was measured andshown to be present in the interstitial areas of the LV. HISDNdid not alter ED-1 staining (Figure 3A). Myocardial cytokinemRNA levels and quantitative RT-PCR were performed withspecific primer sets with normalization to GAPDH. Aldoste-rone infusion increased LV interferon-� expression 2.6-fold(P�0.05), interleukin (IL) 6 expression 2.8-fold (P�0.05),and tumor necrosis factor (TNF)-� expression 1.8-fold(P�0.01) compared with saline infusion (Figure 3B through3E). HISDN decreased interferon-� and IL-6 transcripts(P�0.05 versus aldosterone untreated) with no effect onTNF-� expression. LV IL-1� expression was negligiblyaltered by aldosterone infusion or therapy with HISDN(Figure 3E).
HISDN and Fetal Gene Re-ExpressionAldosterone infusion increased myocardial atrial natriureticpeptide (ANP) mRNA expression by �2.0-fold (P�0.05
Table 1. Characteristics of Untreated and HISDN-Treated Mice4 Weeks After Saline or Aldosterone Infusion
Groups
Untreated HISDN
Saline Aldosterone Saline Aldosterone
No. 5 10 5 10
Body weight, g 28.1�0.9 28.4�0.7 30.8�0.7§ 31.1�0.5¶
SBP, mm Hg 129�2 161�3† 114�2†† 137�5‡�
HR, bpm 729�5 690�9 745�22 683�17
LV/BW, mg/g 3.6�0.1 4.2�0.1†† 3.8�0.1 4.3�0.1**
Lung, wet:dry ratio
4.3�0.2 5.4�0.5§ 4.3�0.3 5.4�0.3**
Myocytecross-sectionalarea, �m2
180�24 380�38* 169�21 366�42#
Data are represented as mean�SEM.*P�0.01 vs saline-untreated.†P�0.0001 vs saline-untreated.‡P�0.01 vs saline-HISDN.§P�0.05 vs saline-untreated.�P�0.001 vs aldosterone-untreated.¶P�0.05 vs aldosterone-untreated.#P�0.0001 vs saline-HISDN.**P�0.05 vs saline-HISDN.††P�0.001 vs saline-untreated.
584 Hypertension September 2009
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
versus saline infusion) and had negligible effects on SERCA2mRNA expression. Both ANP and sarcoplasmic reticulumCa2�-ATPase (SERCA2) transcripts were decreased significantlyin aldosterone-HISDN hearts (P�0.05 and P�0.001, respec-tively, versus aldosterone untreated; Figure 4A through 4B).
HISDN Improved Exercise CapacityExercise limitation occurs in human diastolic HF,22 and“quality-of-life” scores were improved in AHeFT withHISDN therapy.23 We sought to determine whether diastolicdysfunction improvement was associated with improvedfunctional outcome by measuring exercise capacity in thesemice. Exercise capacity (determined by running distance) was
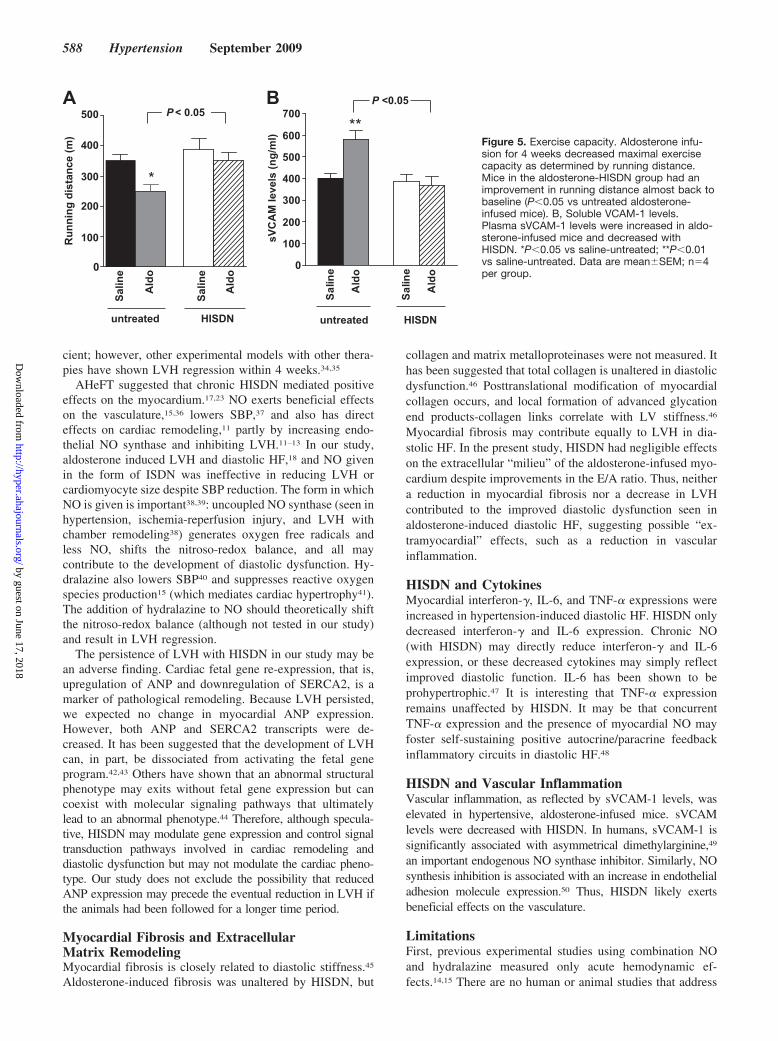
measured in a blinded manner. There were no differencesbetween the saline-untreated and saline-HISDN groups (Fig-ure 5A). Exercise capacity was impaired in aldosterone-untreated mice (P�0.05 versus saline infusion). HISDNimproved exercise capacity by �40% in aldosterone-infusedmice (P�0.05 versus aldosterone untreated). Running time wasalso increased in aldosterone-HISDN (999�68 seconds) versusaldosterone-untreated (776�47 seconds; P�0.05) mice.
HISDN Improved Vascular InflammationPlasma soluble vascular cell adhesion molecule (sVCAM-1; amarker of vascular inflammation) was increased in hyperten-sive, untreated mice with diastolic HF (P�0.01 versus saline
2.0 4.0 2.0 4.00.0
0.5
1.0
1.5
2.0
2.5
LV E
DD
(mm
)
2.0 4.0 2.0 4.00.00
0.25
0.50
0.75
1.00
LV E
SD (m
m)
2.0 4.0 2.0 4.00
25
50
75
Frac
tiona
lsh
orte
ning
(%)
2.0 4.0 2.0 4.00.00
0.05
0.10
0.15To
tal w
all t
hick
ness
(mm
)
P = NS
*‡ ¶ †
P = NS
P = NS
Saline-untreated Aldo-untreated Saline-HISDN Aldo-HISDN
BA
DC
*P = NS
Aldosterone-HISDN
E Aldosterone-untreated: Mitral inflow Doppler tracing
E
A
DT IVRT
120100806040200-20-40
Velo
city
(cm
/s)
120100806040200-20-40
Velo
city
(cm
/s)
30
20
10
0
-10
Freq
uenc
y (k
Hz)
30
20
10
0
-10Freq
uenc
y (k
Hz)
0 1000 20 Time (ms)
0 1000 20 Time (ms)
Figure 1. In vivo transthoracic echo-cardiography measurements with orwithout fixed-dose HISDN. Two- and4-week measurements. A, LV end-dia-stolic diameter (LVEDD); (B) LV end-systolic diameter (LVESD); (C) frac-tional shortening (FS); and (D) totalwall thickness (TWT). Saline-untreated(f), aldosterone-untreated ( ), saline-HISDN (�), and aldosterone-HISDN(o) mice. (*P�0.05 vs wild-type saline;‡P�0.01 vs wild-type saline). Data aremean�SEM; n�5 to 9 per group.*P�0.05 vs saline-HIDN at 4 weeks;‡P�0.001 vs saline-untreated at 2weeks; ¶P�0.001 vs saline-untreatedat 4 weeks; *P�0.05 vs saline-HISDNat 2 weeks; †P�0.001 vs saline-HISDN at 4 weeks. E, Representativemitral Doppler inflow pattern: an aldo-sterone-infused mouse on no HISDNand an aldosterone-infused mouse onHISDN. E indicates early ventricularfilling; A, late filling caused by atrialcontraction; IVRT, isovolumetric con-traction time; DT, deceleration time.
Wilson et al Isosorbide Dinitrate/Hydralazine and Heart Failure 585
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
infusion). Therapy with HISDN decreased sVCAM-1 levelsin aldosterone-infused mice (P�0.05 versus aldosterone un-treated; Figure 5B).
DiscussionIn this study, aldosterone-induced hypertension resulted inLVH, diastolic dysfunction, and diastolic HF. Fixed-doseHISDN lowered SBP and improved diastolic dysfunction andexercise capacity. It also decreased plasma sVCAM-1 (amarker of vascular inflammation) and myocardial interferon-�and IL-6 expression. HISDN did not ameliorate LVH or cardio-myocyte size. Similarly pulmonary congestion and cardiacfibrosis remained unaffected.
HISDN and ExerciseExercise intolerance is seen in diastolic HF,22; therefore,exercise capacity was determined in the mice. The improved
exercise capacity seen in our study may be because of thefollowing: (1) a reduction in SBP despite the presence ofLVH; (2) an improvement in diastolic dysfunction24; and (3)a decrease in vascular inflammation/stiffness. Although notdirectly addressed in our study, the effect of HISDN was notlimited to the myocardium. Vascular-ventricular stiffeningduring exercise (or other stressors) may lead to an exagger-ated hypertensive response and further load-dependent dia-stolic dysfunction.25 Therefore, it is possible that HISDNenhanced vascular and ventricular interactions (that affect LVfilling and ejection) and, thus, improved diastolic dysfunctionand exercise capacity.
HISDN and Diastolic DysfunctionDiastolic dysfunction is an independent risk factor for HF andcardiovascular death.26,27 If diastolic dysfunction is consid-ered a “preclinical” diagnosis, its early recognition mayrepresent an important way to reduce the incidence ofcongestive HF.28 Conversely, diastolic dysfunction may alsobe an early marker of cardiac end-organ damage in hyperten-sion that precedes the development of LVH.6
The presence of hypertension also increases afterload anddecreases early diastolic filling and myocardial lengthening.29,30
Increased preload and afterload affect the LV relaxation rate, andthese become more pronounced during neurohormonal stimula-tion (eg, aldosterone infusion or during exercise), which thenfurther exacerbates diastolic dysfunction. In our study, SBPreduction improved diastolic dysfunction and exercise capacity.In humans, diastolic dysfunction need not be present to meet thedefinition of diastolic HF.31 Similarly, diastolic dysfunction mayherald the development of diastolic HF26,27 or systolic HF.28 Wecannot exclude the possibility that, if mice were followed for alonger period, improvement in diastolic dysfunction may pre-cede potential decreases in pulmonary congestion (ie, diastolicHF) with HISDN therapy. Thus, recognition of the beneficialeffects of HISDN on Doppler diastolic indices and exercisecapacity may potentially translate into relief of pulmonarycongestion because of vasodilatory effects of HISDN on thevasculature.14,15
Table 2. Measurements of Diastolic Function by MitralDoppler Imaging in Untreated and HISDN-Treated Mice After 4Weeks of Saline- or Aldosterone Infusion
Groups
Untreated HISDN
Saline Aldosterone Saline Aldosterone
No. 5 7 5 7
Mitral Evelocity, mm/s
623�29 1026�44** 545�25 768�77†*
Mitral Avelocity, mm/s
400�20 456�20 374�12 553�35¶*
E/A ratio 1.6�0.1 2.3�0.1** 1.5�0.1 1.4�0.1‡
IVRT, ms 20�0.9 28�1.9** 20�1.1 13.5�0.8§‡
DT, ms 23�1 21�0.5 22�1 15.5�1.1#¶
Data are represented as mean�SEM.*P�0.01 vs aldosterone-untreated.†P�0.05 vs saline-HISDN.‡P�0.0001 vs aldosterone-untreated.§P�0.001 vs saline-HISDN.¶P�0.01 vs saline-HISDN.#P�0.001 vs aldosterone-untreated.**P�0.001 vs saline-untreated.
ASaline-untreated
Saline-HISDN
Aldosterone-untreated
Aldosterone-HISDN
B
Salin
e
Ald
o
untreated
Salin
e
Ald
o
HISDN
% T
otal
fibr
osis
0
5
10
15
20
25
P = NS
*†
Figure 2. Representative Masson’s trichrome-stained cross-sections. A, Interstitial and perivascular areas in LV sections from the myo-cardium from saline- and aldosterone-infused mice with or without HISDN. Scale bar�20 �m. B, Quantitatively, there is more cardiacfibrosis in aldosterone-untreated (*P�0.05 vs saline-untreated) and aldosterone-HISDN hearts (†P�0.01 vs saline-untreated hearts).Data reflect 10 measurements from the 3 sections on the slide from each animal; n�2 to 3 per group.
586 Hypertension September 2009
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
Characterizing LV diastolic properties in humans is usuallydone by measuring pressure and volume with high-fidelitymicromanometers.31 In our study, the Vevo 770 High-Resolution In Vivo Imaging System provided the measures ofmurine diastolic function.19,32 Mitral Doppler measurements aregood measures of diastolic function in mice.32 In a subset ofmice, increased LVEDP correlated with an increased E/A ratio(data not shown). SBP control and LVH regression improve LVdiastolic filling33; however, LVH regression was not seen in ourstudy. Once again, it is possible that, if mice were followed for anextended period, SBP control with HISDN and improved diastolicdysfunction may precede potential reductions in cardiac mass.6
Equally plausible is that a delay in measurable change in structuremay allow functional changes to precede structural changes.
HISDN and Cardiac RemodelingControversy surrounds the roles of LVH and HF. LVHregression, an intermediary between hypertension and HF,6
may prevent both systolic and diastolic HFs. Conversely,although LVH increases the risk of HF, hypertensive subjectswithout LVH may also develop HF,1 suggesting that targetingLVH may be unnecessary to prevent HF. The effect of LVHregression on diastolic dysfunction, one of the earliestchanges in hypertension, is unclear. Even in the absence ofLVH, SBP control improves diastolic filling irrespective ofthe regimen used.6 It is unclear why LVH regression was notseen in the present study, but this indicates that LVH andhypertension may not have a causal relationship in thismodel. Furthermore, study duration may have been insuffi-
Saline-HISDN
Aldosterone-untreated
Aldosterone-HISDN
Saline-untreated
A
0.00.51.01.52.02.53.03.5
0.00.51.01.52.02.53.03.5
0.0
0.5
1.0
1.5
2.0
2.5
0.0
0.5
1.0
1.5
2.0
2.5
Inte
rfer
on-γ
expr
essi
onvs
. GA
PDH
(A.U
)
IL-6
expr
essi
onvs
. GA
PDH
(A.U
)
TNF-α
expr
essi
onvs
. GA
PDH
(A.U
)
IL-1β
expr
essi
onvs
. GA
PDH
(A.U
)
CB
D E
Saline-untreatedAldo-untreated
Saline-HISDNAldo-HISDN
*
P < 0.05
*
P < 0.05
**†
P = NSP = NS
Figure 3. Myocardial inflammation. A, Representative ED-1 staining for macrophages in cross-sections of the LV at 4 weeks. Photomi-crographs of LV sections from the 4 groups: saline-untreated, saline HISDN, aldosterone-untreated, and aldosterone-HISDN. Blackarrows indicate the presence of immunostaining specific for the ED-1 antibody in both groups of aldosterone-infused hearts (magnifica-tion: �200). Increased myocardial cytokine expression in aldosterone-untreated hearts: (B) interferon-�, (C) IL-6, and (D) TNF-� expres-sion. E, IL-1� expression was not significantly increased. HISDN decreased interferon-� and IL-6 expression but not TNF-� expressionin aldosterone-infused mice. *P�0.05 vs saline-untreated; **P�0.01 vs saline-untreated; †P�0.05 vs saline-HISDN; n�4 to 5 per group.
BA
AN
P ex
pres
sion
vs. G
APD
H (A
.U)
Salin
e
Ald
o
Salin
e
Ald
o
untreated HISDN
Salin
e
Ald
o
Salin
e
Ald
o
untreated HISDN
0
1
2
3
0.0
2.5
5.0
7.5
10.0
SER
CA
-2 e
xpre
ssio
nvs
. GA
PDH
(A.U
)
P <0.05
*P <0.001
Figure 4. Molecular markers of cardiac remodeling.A, ANP gene expression by RT-PCR is significantlyincreased in untreated aldosterone-infused hearts.Chronic therapy with HISDN reduced myocardialANP expression; *P�0.05 vs saline-untreated. B,SERCA2 expression in the hearts was not signifi-cantly altered in untreated aldosterone-infusedhearts. SERCA2 expression was decreased withHISDN; P�0.001. Data are mean�SEM; n�4 to 5per group.
Wilson et al Isosorbide Dinitrate/Hydralazine and Heart Failure 587
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
cient; however, other experimental models with other thera-pies have shown LVH regression within 4 weeks.34,35
AHeFT suggested that chronic HISDN mediated positiveeffects on the myocardium.17,23 NO exerts beneficial effectson the vasculature,15,36 lowers SBP,37 and also has directeffects on cardiac remodeling,11 partly by increasing endo-thelial NO synthase and inhibiting LVH.11–13 In our study,aldosterone induced LVH and diastolic HF,18 and NO givenin the form of ISDN was ineffective in reducing LVH orcardiomyocyte size despite SBP reduction. The form in whichNO is given is important38,39: uncoupled NO synthase (seen inhypertension, ischemia-reperfusion injury, and LVH withchamber remodeling38) generates oxygen free radicals andless NO, shifts the nitroso-redox balance, and all maycontribute to the development of diastolic dysfunction. Hy-dralazine also lowers SBP40 and suppresses reactive oxygenspecies production15 (which mediates cardiac hypertrophy41).The addition of hydralazine to NO should theoretically shiftthe nitroso-redox balance (although not tested in our study)and result in LVH regression.
The persistence of LVH with HISDN in our study may bean adverse finding. Cardiac fetal gene re-expression, that is,upregulation of ANP and downregulation of SERCA2, is amarker of pathological remodeling. Because LVH persisted,we expected no change in myocardial ANP expression.However, both ANP and SERCA2 transcripts were de-creased. It has been suggested that the development of LVHcan, in part, be dissociated from activating the fetal geneprogram.42,43 Others have shown that an abnormal structuralphenotype may exits without fetal gene expression but cancoexist with molecular signaling pathways that ultimatelylead to an abnormal phenotype.44 Therefore, although specula-tive, HISDN may modulate gene expression and control signaltransduction pathways involved in cardiac remodeling anddiastolic dysfunction but may not modulate the cardiac pheno-type. Our study does not exclude the possibility that reducedANP expression may precede the eventual reduction in LVH ifthe animals had been followed for a longer time period.
Myocardial Fibrosis and ExtracellularMatrix RemodelingMyocardial fibrosis is closely related to diastolic stiffness.45
Aldosterone-induced fibrosis was unaltered by HISDN, but
collagen and matrix metalloproteinases were not measured. Ithas been suggested that total collagen is unaltered in diastolicdysfunction.46 Posttranslational modification of myocardialcollagen occurs, and local formation of advanced glycationend products-collagen links correlate with LV stiffness.46
Myocardial fibrosis may contribute equally to LVH in dia-stolic HF. In the present study, HISDN had negligible effectson the extracellular “milieu” of the aldosterone-infused myo-cardium despite improvements in the E/A ratio. Thus, neithera reduction in myocardial fibrosis nor a decrease in LVHcontributed to the improved diastolic dysfunction seen inaldosterone-induced diastolic HF, suggesting possible “ex-tramyocardial” effects, such as a reduction in vascularinflammation.
HISDN and CytokinesMyocardial interferon-�, IL-6, and TNF-� expressions wereincreased in hypertension-induced diastolic HF. HISDN onlydecreased interferon-� and IL-6 expression. Chronic NO(with HISDN) may directly reduce interferon-� and IL-6expression, or these decreased cytokines may simply reflectimproved diastolic function. IL-6 has been shown to beprohypertrophic.47 It is interesting that TNF-� expressionremains unaffected by HISDN. It may be that concurrentTNF-� expression and the presence of myocardial NO mayfoster self-sustaining positive autocrine/paracrine feedbackinflammatory circuits in diastolic HF.48
HISDN and Vascular InflammationVascular inflammation, as reflected by sVCAM-1 levels, waselevated in hypertensive, aldosterone-infused mice. sVCAMlevels were decreased with HISDN. In humans, sVCAM-1 issignificantly associated with asymmetrical dimethylarginine,49
an important endogenous NO synthase inhibitor. Similarly, NOsynthesis inhibition is associated with an increase in endothelialadhesion molecule expression.50 Thus, HISDN likely exertsbeneficial effects on the vasculature.
LimitationsFirst, previous experimental studies using combination NOand hydralazine measured only acute hemodynamic ef-fects.14,15 There are no human or animal studies that address
Salin
e
Ald
o
Salin
e
Ald
o0
100
200
300
400
500
Run
ning
dis
tanc
e (m
)
*
untreated HISDN
BA
Salin
e
Ald
o
Salin
e
Ald
o0
100
200
300
400
500
600
700
sVC
AM
leve
ls (n
g/m
l)
P <0.05
**
untreated HISDN
P< 0.05
Figure 5. Exercise capacity. Aldosterone infu-sion for 4 weeks decreased maximal exercisecapacity as determined by running distance.Mice in the aldosterone-HISDN group had animprovement in running distance almost back tobaseline (P�0.05 vs untreated aldosterone-infused mice). B, Soluble VCAM-1 levels.Plasma sVCAM-1 levels were increased in aldo-sterone-infused mice and decreased withHISDN. *P�0.05 vs saline-untreated; **P�0.01vs saline-untreated. Data are mean�SEM; n�4per group.
588 Hypertension September 2009
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from

the effect of combined HISDN (which is used clinically) ondiastolic dysfunction and diastolic HF either acutely orchronically. Second, few animal models can successfullyreplicate human diastolic disease, and a single-cell study islimited in its inability to mimic diastolic disease given theimportance of the vasculature (in preload and afterload), heartrate, chamber geometry, and extracellular matrix in diastol-ogy. Therefore, this model of hypertension-induced diastolicHF is a clinically relevant model. It encompasses the myo-cardium, potential effects of the vasculature, and exerciseimpairment. Third, although Millar catheterization was notperformed in all of the mice, LVEDP correlated with the E/Aratio. Echocardiography allowed us to follow the micelongitudinally. Fourth, this study was performed exclusivelyin male mice. The prevalence of diastolic HF is greatest inelderly female mice.32 A future study proposes to study aged,female mice. Finally, although not directly addressed in thepresent study, our findings suggests that HISDN effects werenot limited exclusively to the myocardium, and the improve-ments seen were likely attributed to effects on the vasculatureand interactions of vascular and ventricular stiffness. Ourfindings represent not so much a change in diastolic functionas a change in myocardial load induced by alterations invascular inflammation and/or stiffness because of HISDN.
In conclusion, HISDN did not prevent the progression toLVH or diastolic HF. LVH regression is unnecessary for theimprovement in exercise capacity and diastolic dysfunction inhypertension. It is possible that improvement in ventricularinflammation/stiffness results in enhanced diastolic functionand will require further study.
PerspectivesDiastolic dysfunction may precede the development of LVHin hypertension and is the connection between hypertensionand diastolic HF. Although a lack of therapies continues toplague diastolic HF patients, understanding mechanisms pri-marily responsible for this clinical syndrome and its relation-ship to hypertension and diastolic dysfunction is important.Unlike human systolic HF studies,17 our findings indicate thatHISDN does not exert direct myocardial effects but ratherinfluences ventricular-vascular interactions in diastolic HF.Additional studies are warranted to determine whether LVHregression is beneficial in hypertension-mediated diastolicdysfunction and to determine causality in diastolic dysfunc-tion and cardiac remodeling.
Sources of FundingThis work was supported by funding from the National Institutes ofHealth grant HL079099 (to F.S.).
DisclosuresNone.
References1. Levy D, Larson MG, Vasan RS, Kannel WB, Ho KK. The progression
from hypertension to congestive heart failure. JAMA. 1996;275:1557–1562.
2. Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA,Rademakers FE, Marino P, Smiseth OA, De Keulenaer G, Leite-MoreiraAF, Borbely A, Edes I, Handoko ML, Heymans S, Pezzali N, Pieske B,Dickstein K, Fraser AG, Brutsaert DL. How to diagnose diastolic heart
failure: a consensus statement on the diagnosis of heart failure withnormal left ventricular ejection fraction by the Heart Failure and Echo-cardiography Associations of the European Society of Cardiology. EurHeart J. 2007;28:2539–2550.
3. Vasan RS, Larson MG, Benjamin EJ, Evans JC, Reiss CK, Levy D.Congestive heart failure in subjects with normal versus reduced leftventricular ejection fraction: prevalence and mortality in apopulation-based cohort. J Am Coll Cardiol. 1999;33:1948–1955.
4. Zile MR, Brutsaert DL. New concepts in diastolic dysfunction and dia-stolic heart failure: part I–diagnosis, prognosis, and measurements ofdiastolic function. Circulation. 2002;105:1387–1393.
5. Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure–abnormalities inactive relaxation and passive stiffness of the left ventricle. N Engl J Med.2004;350:1953–1959.
6. Solomon SD, Janardhanan R, Verma A, Bourgoun M, Daley WL,Purkayastha D, Lacourciere Y, Hippler SE, Fields H, Naqvi TZ, MulvaghSL, Arnold JM, Thomas JD, Zile MR, Aurigemma GP. Effect of angio-tensin receptor blockade and antihypertensive drugs on diastolic functionin patients with hypertension and diastolic dysfunction: a randomisedtrial. Lancet. 2007;369:2079–2087.
7. Kass DA, Bronzwaer JG, Paulus WJ. What mechanisms underlie diastolicdysfunction in heart failure? Circ Res. 2004;94:1533–1542.
8. Cohn JN, Archibald DG, Ziesche S, Franciosa JA, Harston WE, TristaniFE, Dunkman WB, Jacobs W, Francis GS, Flohr KH. Effect of vaso-dilator therapy on mortality in chronic congestive heart failure: results ofa Veterans Administration Cooperative Study. N Engl J Med. 1986;314:1547–1552.
9. Taylor AL, Ziesche S, Yancy C, Carson P, D’Agostino R Jr, Ferdinand K,Taylor M, Adams K, Sabolinski M, Worcel M, Cohn JN; for the African-American Heart Failure Trial Investigators. Combination of isosorbidedinitrate and hydralazine in blacks with heart failure. N Engl J Med.2004;351:2049–2057.
10. Ignarro LJ, Napoli C, Loscalzo J. Nitric oxide donors and cardiovascularagents modulating the bioactivity of nitric oxide: an overview. Circ Res.2002;90:21–28.
11. Janssens S, Pokreisz P, Schoonjans L, Pellens M, Vermeersch P, Tjwa M,Jans P, Scherrer-Crosbie M, Picard MH, Szelid Z, Gillijns H, Van deWerf F, Collen D, Bloch KD. Cardiomyocyte-specific overexpression ofnitric oxide synthase 3 improves left ventricular performance and reducescompensatory hypertrophy after myocardial infarction. Circ Res. 2004;94:1256–1262.
12. Prabhu SD. Nitric oxide protects against pathological ventricular remod-eling: reconsideration of the role of NO in the failing heart. Circ Res.2004;94:1155–1157.
13. Scherrer-Crosbie M, Ullrich R, Bloch KD, Nakajima H, Nasseri B, AretzHT, Lindsey ML, Vancon AC, Huang PL, Lee RT, Zapol WM, PicardMH. Endothelial nitric oxide synthase limits left ventricular remodelingafter myocardial infarction in mice. Circulation. 2001;104:1286–1291.
14. Bauer JA, Fung HL. Concurrent hydralazine administration preventsnitroglycerin-induced hemodynamic tolerance in experimental heartfailure. Circulation. 1991;84:35–39.
15. Munzel T, Kurz S, Rajagopalan S, Thoenes M, Berrington WR,Thompson JA, Freeman BA, Harrison DG. Hydralazine prevents nitro-glycerin tolerance by inhibiting activation of a membrane-bound NADHoxidase: a new action for an old drug. J Clin Invest. 1996;98:1465–1470.
16. Daiber A, Oelze M, Coldewey M, Kaiser K, Huth C, Schildknecht S,Bachschmid M, Nazirisadeh Y, Ullrich V, Mulsch A, Munzel T,Tsilimingas N. Hydralazine is a powerful inhibitor of peroxynitrite for-mation as a possible explanation for its beneficial effects on prognosis inpatients with congestive heart failure. Biochem Biophys Res Commun.2005;338:1865–1874.
17. Cohn JN, Tam SW, Anand IS, Taylor AL, Sabolinski ML, Worcel M.Isosorbide dinitrate and hydralazine in a fixed-dose combination producesfurther regression of left ventricular remodeling in a well-treated blackpopulation with heart failure: results from A-HeFT. J Card Fail. 2007;13:331–339.
18. Lebrasseur NK, Duhaney TA, De Silva DS, Cui L, Ip PC, Joseph L, SamF. Effects of fenofibrate on cardiac remodeling in aldosterone-inducedhypertension. Hypertension. 2007;50:489–496.
19. Zhang Y, Takagawa J, Sievers RE, Khan MF, Viswanathan MN, SpringerML, Foster E, Yeghiazarians Y. Validation of the wall motion score andmyocardial performance indexes as novel techniques to assess cardiacfunction in mice after myocardial infarction. Am J Physiol Heart CircPhysiol. 2007;292:H1187–H1192.
Wilson et al Isosorbide Dinitrate/Hydralazine and Heart Failure 589
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from

20. Taffet GE, Hartley CJ, Wen X, Pham T, Michael LH, Entman ML.Noninvasive indexes of cardiac systolic and diastolic function in hyper-thyroid and senescent mouse. Am J Physiol. 1996;270:H2204–H2209.
21. Rocha R, Rudolph AE, Frierdich GE, Nachowiak DA, Kekec BK,Blomme EA, McMahon EG, Delyani JA. Aldosterone induces a vascularinflammatory phenotype in the rat heart. Am J Physiol Heart CircPhysiol. 2002;283:H1802–H1810.
22. Kitzman DW, Higginbotham MB, Cobb FR, Sheikh KH, Sullivan MJ.Exercise intolerance in patients with heart failure and preserved leftventricular systolic function: failure of the Frank-Starling mechanism.J Am Coll Cardiol. 1991;17:1065–1072.
23. Taylor AL, Ziesche S, Yancy CW, Carson P, Ferdinand K, Taylor M,Adams K, Olukotun AY, Ofili E, Tam SW, Sabolinski ML, Worcel M,Cohn JN; for the African-American Heart Failure Trial Investigators.Early and sustained benefit on event-free survival and heart failure hos-pitalization from fixed-dose combination of isosorbide dinitrate/hydral-azine: consistency across subgroups in the African-American HeartFailure Trial. Circulation. 2007;115:1747–1753.
24. Warner JG Jr, Metzger DC, Kitzman DW, Wesley DJ, Little WC. Lo-sartan improves exercise tolerance in patients with diastolic dysfunctionand a hypertensive response to exercise. J Am Coll Cardiol. 1999;33:1567–1572.
25. Borlaug BA, Kass DA. Mechanisms of diastolic dysfunction in heartfailure. Trends Cardiovasc Med. 2006;16:273–279.
26. Aurigemma GP, Gottdiener JS, Shemanski L, Gardin J, Kitzman D.Predictive value of systolic and diastolic function for incident congestiveheart failure in the elderly: the Cardiovascular Health Study. J Am CollCardiol. 2001;37:1042–1048.
27. Bella JN, Palmieri V, Roman MJ, Liu JE, Welty TK, Lee ET, Fabsitz RR,Howard BV, Devereux RB. Mitral ratio of peak early to late diastolicfilling velocity as a predictor of mortality in middle-aged and elderlyadults: the Strong Heart Study. Circulation. 2002;105:1928–1933.
28. Redfield MM, Jacobsen SJ, Burnett JC Jr, Mahoney DW, Bailey KR,Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction inthe community: appreciating the scope of the heart failure epidemic.JAMA. 2003;289:194–202.
29. Zile MR, Gaasch WH, Wiegner AW, Robinson KG, Bing OH.Mechanical determinants of maximum isotonic lengthening rate in rat leftventricular myocardium. Circ Res. 1987;60:815–823.
30. Zile MR, Blaustein AS, Gaasch WH. The effect of acute alterations in leftventricular afterload and beta-adrenergic tone on indices of early diastolicfilling rate. Circ Res. 1989;65:406–416.
31. Zile MR. Heart failure with preserved ejection fraction: is this diastolicheart failure? J Am Coll Cardiol. 2003;41:1519–1522.
32. Zhou YQ, Foster FS, Parkes R, Adamson SL. Developmental changes inleft and right ventricular diastolic filling patterns in mice. Am J PhysiolHeart Circ Physiol. 2003;285:H1563–H1575.
33. Wachtell K, Bella JN, Rokkedal J, Palmieri V, Papademetriou V, DahlofB, Aalto T, Gerdts E, Devereux RB. Change in diastolic left ventricularfilling after one year of antihypertensive treatment: the LosartanIntervention for Endpoint Reduction in Hypertension (LIFE) Study.Circulation. 2002;105:1071–1076.
34. Stansfield WE, Tang RH, Moss NC, Baldwin AS, Willis MS, SelzmanCH. Proteasome inhibition promotes regression of left ventricular hyper-trophy. Am J Physiol Heart Circ Physiol. 2008;294:H645–H650.
35. Errami M, Galindo CL, Tassa AT, DiMaio JM, Hill JA, Garner HR.Doxycycline attenuates isoproterenol- and transverse aortic banding-induced cardiac hypertrophy in mice. J Pharmacol Exp Ther. 2008;324:1196–1203.
36. Sydow K, Daiber A, Oelze M, Chen Z, August M, Wendt M, Ullrich V,Mulsch A, Schulz E, Keaney JF Jr, Stamler JS, Munzel T. Central role ofmitochondrial aldehyde dehydrogenase and reactive oxygen species innitroglycerin tolerance and cross-tolerance. J Clin Invest. 2004;113:482–489.
37. Bagnost T, Berthelot A, Bouhaddi M, Laurant P, Andre C, Guillaume Y,Demougeot C. Treatment with the arginase inhibitor N(omega)-hydroxy-nor-L-arginine improves vascular function and lowers blood pressure in adultspontaneously hypertensive rat. J Hypertens. 2008;26:1110–1118.
38. Moens AL, Takimoto E, Tocchetti CG, Chakir K, Bedja D, Cormaci G,Ketner EA, Majmudar M, Gabrielson K, Halushka MK, Mitchell JB,Biswal S, Channon KM, Wolin MS, Alp NJ, Paolocci N, Champion HC,Kass DA. Reversal of cardiac hypertrophy and fibrosis from pressureoverload by tetrahydrobiopterin: efficacy of recoupling nitric oxidesynthase as a therapeutic strategy. Circulation. 2008;117:2626–2636.
39. Tocchetti CG, Wang W, Froehlich JP, Huke S, Aon MA, Wilson GM, DiBenedetto G, O’Rourke B, Gao WD, Wink DA, Toscano JP, Zaccolo M,Bers DM, Valdivia HH, Cheng H, Kass DA, Paolocci N. Nitroxylimproves cellular heart function by directly enhancing cardiac sarco-plasmic reticulum Ca2� cycling. Circ Res. 2007;100:96–104.
40. Michael LH, Seidel CL. Hydralazine: effect on contraction mechanics ofWKY and SHR rat heart muscle. Hypertension. 1981;3:356–361.
41. Kwon SH, Pimentel DR, Remondino A, Sawyer DB, Colucci WS.H(2)O(2) regulates cardiac myocyte phenotype via concentration-dependent activation of distinct kinase pathways. J Mol Cell Cardiol.2003;35:615–621.
42. Antos CL, McKinsey TA, Frey N, Kutschke W, McAnally J, Shelton JM,Richardson JA, Hill JA, Olson EN. Activated glycogen synthase-3 betasuppresses cardiac hypertrophy in vivo. Proc Natl Acad Sci U S A. 2002;99:907–912.
43. Frey N, Olson EN. Cardiac hypertrophy: the good, the bad, and the ugly.Annu Rev Physiol. 2003;65:45–79.
44. Perrino C, Naga Prasad SV, Mao L, Noma T, Yan Z, Kim HS, SmithiesO, Rockman HA. Intermittent pressure overload triggers hypertrophy-independent cardiac dysfunction and vascular rarefaction. J Clin Invest.2006;116:1547–1560.
45. Brilla CG, Janicki JS, Weber KT. Impaired diastolic function andcoronary reserve in genetic hypertension: role of interstitial fibrosis andmedial thickening of intramyocardial coronary arteries. Circ Res. 1991;69:107–115.
46. Asif M, Egan J, Vasan S, Jyothirmayi GN, Masurekar MR, Lopez S,Williams C, Torres RL, Wagle D, Ulrich P, Cerami A, Brines M, ReganTJ. An advanced glycation endproduct cross-link breaker can reverseage-related increases in myocardial stiffness. Proc Natl Acad Sci U S A.2000;97:2809–2813.
47. Kuwahara K, Saito Y, Harada M, Ishikawa M, Ogawa E, Miyamoto Y,Hamanaka I, Kamitani S, Kajiyama N, Takahashi N, Nakagawa O,Masuda I, Nakao K. Involvement of cardiotrophin-1 in cardiac myocyte-nonmyocyte interactions during hypertrophy of rat cardiac myocytes invitro. Circulation. 1999;100:1116–1124.
48. Kalra D, Baumgarten G, Dibbs Z, Seta Y, Sivasubramanian N, Mann DL.Nitric oxide provokes tumor necrosis factor-� expression in adult felinemyocardium through a cGMP-dependent pathway. Circulation. 2000;102:1302–1307.
49. Nanayakkara PWB, Teerlink T, Stehouwer CDA, Allajar D, SpijkermanA, Schalkwijk C, ter Wee PM, van Guldener C. Plasma asymmetricdimethylarginine (ADMA) concentration is independently associatedwith carotid intima-media thickness and plasma soluble vascular celladhesion molecule-1 (sVCAM-1) concentration in patients with mild-to-moderate renal failure. Kidney Int. 2005;68:2230–2236.
50. Cooke JP. Does ADMA cause endothelial dysfunction? ArteriosclerThromb Vasc Biol. 2000;20:2032–2037.
590 Hypertension September 2009
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
Richard M. Wilson, Deepa S. De Silva, Kaori Sato, Yasuhiro Izumiya and Flora SamCapacity in Hypertension-Induced Diastolic Heart Failure
Effects of Fixed-Dose Isosorbide Dinitrate/Hydralazine on Diastolic Function and Exercise
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2009 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/HYPERTENSIONAHA.109.134932
2009;54:583-590; originally published online July 20, 2009;Hypertension.
http://hyper.ahajournals.org/content/54/3/583World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org/content/suppl/2009/07/20/HYPERTENSIONAHA.109.134932.DC1Data Supplement (unedited) at:
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from

ONLINE SUPPLEMENT
Effects of Fixed-Dose Isosorbide Dinitrate/Hydralazine on Diastolic Function and Exercise Capacity in Hypertension-Induced Diastolic Heart Failure
Richard M. Wilson, BA*; Deepa S. De Silva, PhD*; Kaori Sato, MD, PhD*; Yasuhiro Izumiya MD PhD*, PhD; Flora Sam, MD *‡§
*Whitaker Cardiovascular Institute, ‡Cardiovascular Section and §Evans Department of Medicine;
Boston University School of Medicine, Boston, MA. Correspondence to: Flora Sam, MD Whitaker Cardiovascular Institute Boston University School of Medicine
Evans Department of Medicine and Cardiovascular Section 715 Albany Street, Room W507
Boston, MA 02118 Phone: (617) 638-8072
Fax: (617) 638-4066 E-mail: [email protected]
Expanded Materials And Methods Aldosterone infusion. Uninephrectomized mice (25-27g) received osmotic minipumps (Alzet, Durect Corporation) that delivered a continuous infusion of saline or d-aldosterone (0.15 μg/hour) (Sigma-Aldrich Co.) for 4 weeks1. All mice were maintained on 1% NaCl drinking water. Treatment. Forty-six mice were randomly assigned on the same day as the surgery to either regular chow or chow containing hydralazine: 50mg/kg/day and isosorbide dinitrate (ISDN): 26mg/kg/day, the combination known as HISDN, for 4 weeks. The dose of hydralazine and ISDN has been used by others2-4 and shown to be non-toxic. This combination maintains the same dose ratio that was used in A-HeFT5 i.e., the ISDN:hydralazine HCl ratio was 20mg:37.5mg. The 4 groups studied were: a) saline-untreated, n=9; b) saline-HISDN, n=9; c) aldosterone-untreated, n=14 and d) aldosterone-HISDN, n=14. Physiological measurements. Heart rate (HR) and tail cuff blood pressure (SBP) were determined non-invasively (BP-2000, VisiTech) as previously described1;6. Transthoracic echocardiography was performed in conscious mice biweekly after surgery using the Acuson Sequoia C-256 echocardiograph machine with a 15-MHz probe, as previously described1. Total wall thickness (TWT) was derived from an average of the interventricular septum and posterior wall thickness. Doppler echocardiography. Mitral Doppler flow study was performed using the Vevo 770 High-Resolution In Vivo Imaging System (VisualSonics,Toronto). Images were acquired using a high-resolution (30 MHz) transducer. Mice were anesthetized using isoflurane (0.5-1.5%) and titrated to achieve a HR around 350 beats/min since diastolic function measurement are sensitive to HR and loading conditions. The maximum 1.5% of isoflurane has minimal effects on diastolic function7. Images were recorded for 30–40 cardiac cycles and measurements were made from 3–5 representative cycles. The apical four-chamber view was used to record the mitral Doppler flow spectrum. Peak early (E) and late (A) mitral inflow velocities, deceleration time of early filling (DT) and isovolumetric relaxation time (IVRT) were measured as previously described8. In a subset of mice (n=5), hemodynamic measurements were performed 4 weeks after aldosterone infusion using a 1.4F catheter tip micromanometer (ARIA, Millar Instruments). Aldosterone infusion resulted in an increased LV end-diastolic pressure (EDP). Increased LVEDP correlated with the increased E/A ratio, R=0.95 (P<0.05; data not shown). Exercise Treadmill analysis. Exercise capacity was measured on a rodent motor-driven treadmill (Columbus Instruments) as previously described9. Mice were acclimated for at least 3 days (15% incline, speed of 15 m/min for 10 minutes and subsequently increased 2 m/min each 2 minutes, ending after 20 minutes). Total exercise time was recorded as the elapsed time to exhaustion and then converted to distance. Exhaustion was determined by an observer blinded to treatment groups and was defined as the point at which the animals could not keep pace with the treadmill and no longer avoided the electrical stimulus. Organ weight, tissue and blood analysis. After 4-weeks mice were sacrificed, at which time blood was obtained to determine plasma soluble vascular cell adhesion molecule (VCAM-1) levels (R&D Systems). Body weight (BW), heart weight (HW) and LV weights were also determined. Hearts were
either: (a) arrested in diastole by KCl (30mmol/l), weighed, perfused with 10% buffered formalin and sliced horizontally for histology or (b) snap-frozen in liquid nitrogen. Trichrome-stained sections (5μm) were visualized by light microscopy to measure fibrosis and the entire section was quantified using Bioquant Image analysis software. The wet-to-dry lung weight ratios were determined as an index of pulmonary congestion1. Determination of mRNA. Total RNA from 4 groups of mice hearts were extracted with PureLink™ Micro-to-Midi Total RNA purification system (Invitrogen). cDNA synthesis from total RNA was performed using a Thermoscript™ RT-PCR system (Invitrogen) according to the manufacturer’s instructions. Transcript expression levels of ANP, SERCA-2, IL-1β, IL6, INF-γ, TNF-α and GAPDH were quantified by iCycler iQ Real-Time PCR Detection Systems (BIO-RAD) using FastStart Universal SYBR Green Master Mix (Roche, IN, USA). Transcript levels were adjusted relative to the expression of GAPDH. Sequences of PCR primers are as listed. Primer sequence for mouse are as follows: ANP (F): 5'-GAG AGA CGG CAG TGC TTC TAG GC-3', ANP (R): 5'-CGT GAC ACA CCA CAA GGC CTT AGG-3'; SERCA2 (F): 5'-TAC TGA CCC TGT CCC TGA CC-3'; (R ): 5'-CAC CAC CAC TCC CAT AGC TT-3'; IL-1β (F): 5'-AGA CAC AGA TTC CAT GGT GAA GT-3', IL-1β (R): 5'-TCT CAG CTT CAA TGA AAG ACC TC-3'; IL-6 (F): CCC AAT TTC CAA TGC TCT CCT-3, IL-6 (R): TAA CGC ACT AGG TTT GCC GAG; INFγ (F): 5'-CAT GGC TGT TTC TGG CTG TTA C- 3', IFNγ (R): 5'-CCA GTT CCT CCA GAT ATC CAA GA-3'; TNF-α (F): 5'-CAT CTT CTC AAA ATT CGA GTG ACA A-3', (R): 5'-TGG GAG TAG ACA AGG TAC AAC CC-3', GAPDH (F): 5'-TCA CCA CCA TGG AGA AGG-3', GAPDH (R): 5'-GCT AAG CAG TTG GTG GTG CA-3'.
Immunohistochemistry. To visualize macrophages, ED-1 staining was used as previously described6. Sections were deparaffinized, rehydrated, and treated with 20μg proteinase K per mL of Tris-HCl (pH 8.5) for 25min at room temperature to recover antigenicity. Sections were then stained with a 1:25 dilution of rat anti-mouse cd68 primary antibody (Serotec, Raleigh, NC) in PBS with 1% BSA overnight at 4°C. Nonspecific binding was blocked by incubation with 10% horse serum in PBS (pH 7.4) for 30min before incubation with the antibody. A biotinylated anti-rat antibody (Vector) was used as secondary antibody and Vector Red alkaline phosphatase substrate (Vector) was applied. Sections were visualized under bright-field microscopy and images were recorded using an Optronics camera with Bioquant hardware and software.
Statistical analysis. Results are presented as mean±SEM. Statistical analyses of the data were carried out using the Student’s t test (2-sided). When necessary, 1- or 2-way ANOVA (followed by Student-Newman-Keuls post-hoc tests when appropriate) was applied. A value of P<0.05 was considered statistically significant.
Reference for Online Methods
1. Lebrasseur NK, Duhaney TA, De Silva DS, Cui L, Ip PC, Joseph L, Sam F. Effects of fenofibrate on cardiac remodeling in aldosterone-induced hypertension. Hypertension. 2007;50:489-496.
2. Pipili-Synetos E, Papageorgiou A, Sakkoula E, Sotiropoulou G, Fotsis T, Karakiulakis G, Maragoudakis ME. Inhibition of angiogenesis, tumour growth and metastasis by the NO-releasing vasodilators, isosorbide mononitrate and dinitrate. Br J Pharmacol. 1995;116:1829-1834.
3. Ichinose F, Bloch KD, Wu JC, Hataishi R, Aretz HT, Picard MH, Scherrer-Crosbie M. Pressure overload-induced LV hypertrophy and dysfunction in mice are exacerbated by congenital NOS3 deficiency. Am J Physiol Heart Circ Physiol. 2004;286:H1070-H1075.
4. Loufrani L, Henrion D. Vasodilator treatment with hydralazine increases blood flow in mdx mice resistance arteries without vascular wall remodelling or endothelium function improvement. J Hypertens. 2005;23:1855-1860.
5. Taylor AL, Ziesche S, Yancy C, Carson P, D'Agostino R, Jr., Ferdinand K, Taylor M, Adams K, Sabolinski M, Worcel M, Cohn JN, the African-American Heart Failure Trial Investigators. Combination of Isosorbide Dinitrate and Hydralazine in Blacks with Heart Failure. N Engl J Med. 2004;351:2049-2057.
6. Kuster GM, Kotlyar E, Rude MK, Siwik DA, Liao R, Colucci WS, Sam F. Mineralocorticoid receptor inhibition ameliorates the transition to myocardial failure and decreases oxidative stress and inflammation in mice with chronic pressure overload. Circulation. 2005;111:420-427.
7. Zhou YQ, Foster FS, Parkes R, Adamson SL. Developmental changes in left and right
ventricular diastolic filling patterns in mice. Am J Physiol Heart Circ Physiol. 2003;285:H1563-H1575.
8. Prunier F, Gaertner R, Louedec L, Michel JB, Mercadier JJ, Escoubet B. Doppler echocardiographic estimation of left ventricular end-diastolic pressure after MI in rats. Am J Physiol Heart Circ Physiol. 2002;283:H346-H352.
9. Jain M, Liao R, Podesser BK, Ngoy S, Apstein CS, Eberli FR. Influence of gender on the response to hemodynamic overload after myocardial infarction. Am J Physiol Heart Circ Physiol. 2002;283:H2544-H2550.





























