Embed Size (px)
Citation preview

Review article
Effects of postnatal interventions for the reduction of vertical
HIV transmission on infant growth and non-HIV infections:
a systematic review
Moleen Zunza§,1, Gareth D Mercer2, Lehana Thabane3,4, Monika Esser5 and Mark F Cotton1
§Corresponding author: Moleen Zunza, Francie van Zijl Drive, Tygerberg 7505, South Africa. Tel: �27 73 376 4624. ([email protected])
Abstract
Introduction: Guidelines in resource-poor settings have progressively included interventions to reduce postnatal HIV
transmission through breast milk. In addition to HIV-free survival, infant growth and non-HIV infections should be considered.
Determining the effect of these interventions on infant growth and non-HIV infections will inform healthcare decisions about
feeding HIV-exposed infants. We synthesize findings from studies comparing breast to formula feeding, early weaning to
standard-duration breastfeeding, breastfeeding with extended antiretroviral (ARV) to short-course ARV prophylaxis, and
alternative preparations of infant formula to standard formula in HIV-exposed infants, focusing on infant growth and non-HIV
infectious morbidity outcomes. The review objectives were to collate and appraise evidence of interventions to reduce postnatal
vertical HIV transmission, and to estimate their effect on growth and non-HIV infections from birth to two years of age among
HIV-exposed infants.
Methods: We searched PubMed, SCOPUS, and Cochrane CENTRAL Controlled Trials Register. We included randomized trials
and prospective cohort studies. Two authors independently extracted data and evaluated risk of bias. Rate ratios and mean
differences were used as effect measures for dichotomous and continuous outcomes, respectively. Where pooling was possible,
we used fixed-effects meta-analysis to pool results across studies. Quality of evidence was assessed using the GRADE approach.
Results and discussion: Prospective cohort studies comparing breast- versus formula-fed HIV-exposed infants found
breastfeeding to be protective against diarrhoea in early life [risk ratio (RR)�0.31; 95% confidence interval (CI)�0.13 to
0.74]. The effect of breastfeeding against diarrhoea [hazard ratio (HR)�0.74; 95% CI�0.57 to 0.97] and respiratory infections
(HR�0.65; 95% CI�0.41 to 1.00) was significant through two years of age. The only randomized controlled trial (RCT) available
showed that breastfeeding tended to be protective against malnutrition (RR�0.63; 95% CI�0.36 to 1.12). We found no
statistically significant differences in the rates of non-HIV infections or malnutrition between breast-fed infants in the extended
and short-course ARV prophylaxis groups.
Conclusions: Low to moderate quality evidence suggests breastfeeding may improve growth and non-HIV infection outcomes of
HIV-exposed infants. Extended ARV prophylaxis does not appear to increase the risk for HIV-exposed infants for adverse growth
or non-HIV infections compared to short-course ARV prophylaxis.
Keywords: postnatal interventions; HIV; children; growth; non-HIV infections; breast milk.
To access the supplementary material to this article please see Supplementary Files under Article Tools online.
Received 8 September 2013; Revised 2 November 2013; Accepted 27 November 2013; Published 20 December 2013
Copyright:– 2013 Zunza M et al; licensee International AIDS Society. This is an Open Access article distributed under the terms of the Creative Commons Attribution
3.0 Unported (CC BY 3.0) License (http://creativecommons.org/licenses/by/3.0/), which permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
IntroductionHIV infection among children is a public health concern
especially in poorly resourced countries [1]. Most children
acquire HIV infection through mother-to-child transmission
(MTCT) [2]. Approximately 2.5 million children are living
with HIV/AIDS worldwide [3]. Although the proportion of
HIV-attributable death among children less than five years of
age is declining worldwide, HIV/AIDS is still a leading cause
of premature death in Southern African children [4]. In the
absence of antiretroviral (ARV) treatment, one third of HIV-
infected children die by one year of age and about 50%
by two years of age [4]. Infectious diseases and nutritional
complications are the predominant underlying causes of
mortality in these children [4].
HIV may be vertically transmitted in pregnancy, labour,
delivery, or through breast milk. Without interventions, 15�30% of infants are vertically infected; breastfeeding increases
the risk to 20�45% [5]. Strategies to reduce postnatal vertical
transmission of HIV focus on reducing transmission through
breast milk. HIV-positive mothers in high-income countries
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
1

are recommended to completely avoid breastfeeding [6].
However, in poorly resourced countries where formula feed-
ing does not generally meet AFASS criteria (Acceptable,
Feasible, Affordable, Sustainable, and Safe), avoiding breast-
feeding increases the risks of infant mortality and infectious
morbidity [7].
Description of the intervention
The efficacy of ARV regimens in reducing HIV vertical
transmission through breast milk has been demonstrated
in several randomized controlled trials (RCTs) [8�11], theseinterventions have since been incorporated into the World
Health Organization (WHO) guidelines on infant feeding by
HIV-positive mothers [12].
WHO 2013 prevention of MTCT (PMTCT) guidelines re-
commend that all HIV-positive pregnant women receive
highly active ARV treatment (HAART), until at least one week
after cessation of breastfeeding or after delivery when formula
feeding, but should preferably be continued as lifelong
therapy regardless of CD4 count [12]. Mothers with CD4
count 5500cells/mm3 orWHO clinical stage 3 or 4 disease are
recommended to continue lifelong ARVs. HIV-exposed in-
fants on breast milk are recommended to receive once-daily
nevirapine (NVP) prophylaxis until they are fully weaned.
Formula-fed infants should receive 4�6 weeks of daily NVP ortwice-daily zidovudine (ZDV) [12].
Effect of postnatal MTCT interventions on infant growth
and non-HIV infections
Compared to infant formula, breast milk protects against
gastrointestinal and respiratory tract infections and improves
overall survival [13]. Breastfeeding also promotes optimal
child growth until two years of age [14].
ARVs drugs minimize postnatal HIV transmission through
breast milk by reducing breast milk viral load. As ARVs have
clinical and laboratory adverse effects, their safety in HIV-
exposed children should be considered. Baroncelli et al.
reported a high risk of anaemia in HIV-exposed infants
exposed to HAART with ZDV alone compared to HAART
without ZDV, which disappeared at one month of life [15].
Grade 3�4 hepatoxicity was reported in infants exposed to
NVP for at least five days [16]. Neonatal exposure to lopinavir/
ritonavir (LPV/r) has been associated with cardiac toxicity
and adrenal dysfunction [17]. Lamivudine exposure is safe in
HIV-exposed infants [18]. While side effects would not negate
the benefits of ARVs in preventing HIV transmission, it is
important for health policy makers to have accurate estimates
of the anticipated risks of such effects when introducing these
interventions into clinical practice.
Why it is important to do this review
A Cochrane review appraised evidence for the efficacy of
postnatal HIV PMTCT interventions in preventing HIV trans-
mission, and improving HIV-free survival [19]. However, in
addition to their efficacy in preventing HIV transmission, policy
makers should consider the effects of these interventions on
infant growth and susceptibility to non-HIV infections.
Contradictory findings of the effects of different postnatal
PMTCT interventions on infant growth and non-HIV infec-
tious morbidity were reported in clinical trials and observa-
tional studies; therefore the true effects of the interventions
on these outcomes are uncertain. To inform decision-making
about HIV PMTCT recommendations, this review aims to
synthesize findings from studies comparing the effects of
different postnatal interventions for PMTCT of HIV on infant
growth and non-HIV infections, with follow-up periods of
between 3 and 24 months of age.
Objectives
To collate and appraise evidence of interventions to re-
duce postnatal vertical HIV transmission in HIV-exposed
infants, and estimate their effect on (1) growth from birth to
two years of age (primary objective) and (2) non-HIV infections
from birth to two years of age (secondary objective).
MethodsCriteria for considering studies for this review
Studies
. RCTs of postnatal interventions to prevent vertical
transmission of HIV, which included the assessment of
infant growth or non-HIV infections.
. RCTs assessing the effect of established postnatal
interventions for prevention of vertical transmission
of HIV on infant growth or on HIV infections.
. Cohort studies were also included if the interven-
tion (e.g. mode of feeding) could not be ethically
randomized.
Participants
HIV-positive mothers and their infants.
Interventions
Intervention aimed at reducing HIV vertical transmission.
Primary outcomes
. Weight-for-age (WAZ), weight-for-length (WLZ), length-
for-age (LAZ), and head circumference-for-age (HCA)
z-scores and malnutrition.
. Non-HIV infections, e.g. respiratory tract infections,
gastrointestinal infections.
Search methods for identification of studies
Electronic searches
Search strategies developed by The Cochrane Collaboration
HIV/AIDS Review group were used to search for studies [19].
PubMed (24 April 2013), SCOPUS (24 April 2013), and
Cochrane CENTRAL Controlled Trials Register (11 March
2013) were searched without language, time or publication
status restrictions (Supplementary file). Dates indicate the
timewhen searches were last performed in each database.The
reference lists of included studies were searched for studies.
Data collection and analysis
Selection of studies
Two reviewers (MZ and GM) independently reviewed ab-
stracts of electronic search results. Full texts of potentially
relevant articles were retrieved and independently examined
for eligibility.
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
2

Data extraction
The following data were independently extracted in dupli-
cate: study design, study duration, methodological quality,
study interventions, and outcomes. Discrepancies were
resolved through discussion.
Assessment of risk of bias in included studies
The Cochrane Collaboration’s risk of bias tool was used to
assess the methodological quality of each selected study [20].
Two authors (MZ and GM) independently assessed the risk
of bias. The following domains were assessed: sequence
generation; allocation concealment; blinding of participants,
personnel, and outcome assessors; whether incomplete out-
comes data were adequately addressed; selective reporting;
and other bias.
ClinicalTrial.gov and Current Controlled trial registries
were searched for protocols of included studies. If the
protocol was unavailable, the methods and results sections
were compared to assess the potential for selective report-
ing bias.
Measures of treatment effect
When included publications presented summary data sepa-
rately for each intervention group, we calculated risk ratios
(RR) for binary outcomes and mean differences (MD) for
continuous outcomes, and associated 95% confidence inter-
vals (CI). Otherwise we have directly presented the effect
estimates [RR, hazard ratio (HR), and odds ratios (OR)]
reported in the publications.
For infectious morbidity events, we assumed that the
occurrence of each outcome per participant is a random
variable following a Poisson distribution. The normal approx-
imation to the Poisson distribution was used to calculate CI
for MD in the incidence of infectious morbidity outcomes.
The 95% CI for MD was calculated as:
k1 � k2
� �� 1:96�
ffiffiffiffiffiffiffiffiffiffiffiffiffik1
n1þ k2
n2
q, where k1 and k2 are esti-
mated average counts of a specific infection in Groups 1 and
2, and n1 and n2 are the numbers of infants with complete
follow-up data in each group [21]. Included studies did not
report results disaggregated by sex separately for each study
randomisation arm. Therefore, we could not extract study
results disaggregated by sex in this review.
Unit of analysis issues
Repeated observations on participants. When results
were presented for more than one time point, the following
approaches were used to obtain single effect measures:
For infectious events, we computed the total number
of events experienced during the entire follow-up period for
each intervention group. For growth outcomes, summary
data were extracted at the longest follow-up time point.
Multiple intervention groups. Experimental intervention
groups deemed sufficiently comparable were combined for
pairwise comparison with the control group. For dichotomous
outcomes, sample size and outcome events were summed
across combined groups. For continuous outcomes, means
and standard deviations (SD) were combined using the
following formulas [20]:
where N1, M1 and SD1 are sample size, mean and standard
deviation of Group 1, N2, M2, SD2 are the corresponding
values of Group 2.
Studies using a factorial design. One report was from a
trial that used a factorial design [11]. We only report on
the effect of ARV interventions in this review. Reports of the
study did not suggest an important interaction between the
two interventions.
Dealing with missing data
Authors of 12 studies were contacted for missing infor-
mation; the requested information being obtained for six
studies. The potential impact of missing data was considered
during risk of bias assessment. Meta-analysis was repeated,
excluding studies with attrition rates �20% to assess the
robustness of the results to missing data, and both estimates
are presented.
Assessment of heterogeneity
Substantial statistical heterogeneity was defined as an I2
statistic �50% [20].
Assessment of publication bias
Too few studies were included in each comparison to enable
an investigation of publication bias.
Data synthesis
Fixed-effects meta-analysis using the Mantel-Haenszel method
for dichotomous outcomes and the inverse-variance
method for continuous outcomes were used to pool results
across studies [20]. Where meta-analysis was inappropriate,
individual study results were reported separately. Review
Manager 5.1 was used for analysis.
Quality of evidence
The Grades of Recommendation Assessment, Development
and Evaluation (GRADE) approach was used to rate quality
SD ¼
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiN1 � 1ð ÞSD2
1 þ N2 � 1ð ÞSD22 þ N1N2
N1þN2M2
1 þM22 � 2M1M2ð Þ
N1 þN2 � 1
vuut
Mean ¼ N1M1 þN2M2
N1 þN2
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
3

of evidence [22]. In evaluating the quality of RCT evidence,
we considered the following in whether to downgrade the
quality of evidence: methodological limitations, inconsistency
in study results, indirectness, imprecision and publication
bias. For observational studies, we considered the following
factors in determining whether to upgrade the quality of
evidence: large observed effect and whether plausible
confounding would change the intervention effect. Our
ratings for the breastfeeding versus formula feeding and
the breastfeeding with extended versus short-course ARV
prophylaxis comparisons are presented in Tables 1 and 2,
respectively.
ResultsIncluded studies
We identified 14 reports from seven RCTs and three prospec-
tive cohort studies (Figure 1) conducted in: South Africa (3),
Zambia (1), Malawi (1), USA and Brazil (1), Cote d’lvoire (1),
Tanzania (1), Kenya (1), Burkina Faso, Kenya and South Africa
(1) and South Africa, Tanzania, Uganda and Zimbabwe (1)
(Supplementary file). Ten studies were excluded on review
of full articles (Supplementary file).
Types of interventions
Table 3 summarizes the studies included and outcomes
assessed under each comparison.
Risk of bias in included studies
The risk of bias summary presents authors’ judgments on risk
of bias in each domain for each study separately (Figure 2),
while the risk of bias graph presents the risk of bias in each
domain as a percentage across all included studies (Figure 3).
A summary of our findings on study methodological quality
for each domain follows below.
Allocation (selection bias)
Random sequence generation was adequate in 10 studies
[9,11,23�30]. The method of sequence generation was not
reported in one study [31]. Risk of bias was high for three
observational studies because participants self-selected into
comparison groups [32�34].Methods of allocation concealment were adequate in
10 studies [9,11,23�27,29�31]. One study did not report how
treatment allocation was concealed [28]. The risk of bias
in this domain was high for the three observational studies
[32�34].
Blinding (performance bias and detection bias)
Participants and personnel (performance bias). Seven
studies were assessed as having low risk of participant
performance bias [9,11,24,26,27,30,31]. Five studies were at
high risk because participants were unblinded and it was felt
that knowledge of their intervention allocation, rather than
the intervention itself, could have affected participants’ out-
comes [23,25,28,33,34]. Two studies were unclear on whether
participants were blinded [29,32]. Risk of personnel perfor-
mance bias was low in eight studies [9,11,23,24,26,27,30,31].
Two studies were at high risk because personnel may have
treated participants differently through knowing their inter-
vention allocation, thereby influencing the outcomes [25,33].
It was unclear in four studies whether personnel were blinded
[28,29,32,34].
Outcome assessment (detection bias). Risk of detec-
tion bias was judged to be low in 10 studies [9,11,23�27,31,33,34]. One study was at high risk because outcomes were
ascertained through participants’ verbal reports and outcome
definitions were relatively subjective [28]. It was unclear
whether outcome assessors were blinded in three studies
[29,30,32].
Incomplete outcome data (attrition bias)
Seven reports with an attrition rate below 20% were judged to
have low risk of attrition bias [9,11,27�30,33]. Five reports
were judged high risk [23,26,31,32,34], and two studies were
unclear [24,25].
Selective reporting (reporting bias)
Protocols were available for five studies [9,11,23,27,30].
Nine reports were at low risk of reporting bias [11,25�30,32,34]. Three reports were at high risk, because either
not all study results were reported at pre-specified time
points or the reported outcome was not pre-specified in the
protocol [9,23,24]. Risk of bias due to selective reporting was
unclear in two studies [31,33].
Table 1. Breastfeeding compared to formula feeding for HIV-exposed infants
Outcomes Relative effect (95% CI) Number of participants (studies) Quality of the evidence (GRADE)
Malnutrition RCT RR 0.63 (0.36 to 1.12) 371 (1) ���� lowa,b
Diarrhoea ‘‘Cohort study, effect
up to two years of age’’
HR 0.74 (0.57 to 0.97) 557 (1) ���� moderatea,c
Diarrhoea ‘‘Cohort study, effect
up to three months of age’’
RR 0.31 (0.13 to 0.74) 127 (1) ���� lowc,d
Respiratory infections RCT HR 1 (0.9 to 1.11) 371 (1) ���� lowa,b
Respiratory infections Cohort HR 0.60 (0.36 to 0.98) 557 (1) ���� moderatec
Diarrhoea RCT HR 1.11 (0.91 to 1.43) 371 (1) ���� lowa,b
aStudy had some methodological limitations, bwide confidence interval and fails to exclude the null effect, cobserved breastfeeding effect was
considered clinically important, dsample size was too small. RR: Risk ratio; HR: Hazard ratio.
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
4

Other sources of bias
Nine studies were judged low risk of other bias [9,25�30,32,33]. One study was at high risk; the Data Safety
Monitoring Board recommended enrolment of controls be
stopped early because of an apparent intervention benefit
[11]. Risk of other bias was unclear in four studies; either
baseline characteristics were not compared between study
arms, there was a potential for misclassification of expo-
sure status or the role of the funder was not described
[23,24,31,34].
Effects of interventions
Except where specified, results are from combined data from
HIV-infected and HIV-uninfected infants. Wherever publica-
tions presented findings separately for HIV-uninfected infants
we report these. For characteristics of included studies, see
Supplementary file.
1. Breastfeeding versus formula feeding
One RCT [28] and three prospective cohort studies [32�34]compared growth and non-HIV infections outcomes between
breast- and formula-fed HIV-exposed infants. We report the
RCT and cohort studies separately.
Mbori-Ngacha et al. randomly assigned mother-infant pairs
to breast or formula-feeding groups [28]. Cumulative HIV-
infection rates by two years of age were 37% and 21%,
respectively.
Becquet et al. compared infants whose mother chose
breastfeeding with rapid transition to formula feeding after
four months of age to infants whosemothers chose exclusively
formula feeding [32]. HIV transmission rates at 18 months
were 5% and 1% among breast- and formula-fed infants,
respectively.
Kindra et al. compared outcomes of infants whose
mothers elected to either breastfeed or formula feed. By
six weeks of age, HIV transmission rates were 7.9% and
4% among breast- and formula-fed infants, respectively
[33].
Venkatesh et al. compared rates of infant hospitalizations
associated with infectious morbidity among infants whose
mothers elected to breastfeed or formula feed [34]. They
documented HIV transmission rates of 18.4% and 13.2%
among breast- and formula-fed infants, respectively by three
months.
Outcomes
Growth
Kindra et al. found no difference in z-scores between breast-
and formula-fed infants at nine months of age [33].
Malnutrition
Mbori-Ngacha et al. defined malnutrition as a weight-for-
height z-score value 2 SD below the mean. Becquet et al.
defined malnutrition as an observation of either no change or
a decrease in anthropometric measurements between study
visits. Neither study found a statistically significant difference
in malnutrition risk between breast- and formula-fed infants
Table 2. Breastfeeding with extended ARV compared to breastfeeding with short-course ARV prophylaxis for HIV-exposed infants
Illustrative comparative risksa (95% CI)
Assumed risk Corresponding risk
Outcomes
Breastfeeding with
short-course ARVs
Breastfeeding with
extended ARVs
Relative effect
(95% CI)
Number of
participants (studies)
Quality of the
evidence (GRADE)
Study population
Growth faltering 32 per 1000 36 per 1000 (27 to 48) RR 1.12
(0.83 to 1.5)
5719 (3) ����
moderateb,c
Pneumonia The average incidence of
pneumonia ranged across
control groups from 0.03
to 0.11
The average incidence of
pneumonia in the intervention
groups was 0.01 lower (0.02
lower to 0.00 higher)
6437 (4) ����
moderateb,d
Meningitis The average incidence of
meningitis ranged across
control groups from 0.0089
to 0.0147
The average incidence of
meningitis in the intervention
groups was 0 higher (0.01 lower
to 0.00 higher)
4914 (2) ���� lowb,e
Gastroenteritis The average incidence of
gastroenteritis ranged across
control groups from 0.02 to
0.07
The average incidence of
gastroenteritis in the
intervention groups was 0.01
higher (0.01 lower to 0.02
higher)
6437 (4) ����
moderateb,c
The assumed risk was based on the mean control group risk if there was one study included or otherwise, on mean range in control group risk
across studies. aThe corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the
intervention (and its 95% CI). bThere were too few studies to assess publication bias, cCI failures to exclude appreciable harm, dpoint estimates
vary widely, ethere were very few events. CI: Confidence interval; RR: Risk ratio.
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
5

(RR�0.63; 95% CI�0.36 to 1.12) and (HR�1.35; 95%
CI�0.93 to 2.0) [28,32].
Respiratory tract infections
Mbori-Ngacha et al. do not describe how upper respiratory
tract infections were defined [28].The trial found no difference
in rates of respiratory infections between breast- and formula-
fed infants (HR�1.00; 95% CI�0.90 to 1.11) [28].
Becquet et al. defined acute respiratory infection as cough,
fever, and focal pulmonary findings [32]. Venkatesh et al. used
WHO International Classification of Disease (ICD-10) criteria
to classify respiratory infections associated with hospitali-
zations [34]. The pooled estimate from these observational
studies suggests a lower incidence of respiratory infections in
breast than formula fed infants (HR�0.65; 95% CI�0.41
to 1.00) [32,34]. After adjusting for HIV status, breast-fed
infants were 40% less likely to develop respiratory infections
(HR�0.60; 95% CI�0.36 to 0.98) [32].
Diarrhoea
Diarrhoea was defined as the passage of three or more
watery stools per 24-hour period for at least two days.
Mbori-Ngacha et al. found no difference over two years
between breast- and formula-fed infants either when includ-
ing both HIV-infected and HIV-uninfected infants (HR�1.11;
95% CI�0.91 to 1.43) or in HIV-uninfected infants alone
(HR�1.11; 95% CI�0.83 to 1.43) [28]. Venkatesh et al.
reported similar findings (HR�0.50; 95% CI�0.15 to 1.70)
as Mbori-Ngacha et al. Becquet et al. and Kindra et al. differ
from Mbori-Ngacha et al. and Venkatesh et al. Both studies
found that breast-fed infants were at lower risk for diarrhoea
(RR�0.31; 95% CI�0.13 to 0.74) [33], the risk was signi-
ficantly lower for breast-fed infants after adjusting for HIV
status (HR�0.74; 95% CI�0.57 to 0.97) [32].
2. Breastfeeding with extended ARV prophylaxis versus
short-course ARV prophylaxis
A clinical adverse event is defined as any health-related
reaction or effect experienced by a study participant. Serious
clinical adverse events (SAEs) in infants were assessed as
safety endpoints in studies comparing differing postnatal
ARV prophylaxis. Five studies compared the incidence of
SAEs between infants exposed to different combinations of
extended and short-course ARV prophylaxes during breast-
feeding [9,11,26,27,30]. We use the term ‘‘extended ARV
prophylaxis’’ to refer to interventions involving ARVs given for
longer duration than the (short-course) peri-partum prophy-
laxes that were standard of care at the time the studies were
conducted. Important assumptions were made for interven-
tions in this comparison. First, Jamieson et al. and the Kesho
Bora Study included maternal ARV interventions in their
studies. Since mothers were breastfeeding while receiving
the intervention, infants would be ingesting ARVs in breast
milk. On this basis, we felt these interventions could reason-
ably be compared with ARV interventions administered
directly to infants. This assumption is supported by findings
of Shapiro et al., that concentrations of NVP, lamivudine and
ZDV in breast milk of HIV-positive women receiving HAART
are similar to or higher than their serum concentrations,
and that infant serum NVP concentrations were sufficient to
inhibit HIV-1 replication [35]. Second, the studies by Jamieson
et al. and Kumwenda et al. each tested two extended ARV
regimens against a standard short-course regimen. We felt
that the two extended ARV interventions in each study were
sufficiently similar to combine the results for comparison with
the short-course ARV group.
Four studies [9,11,27,30] used standard Division of AIDS
toxicity tables to grade the severity of SAEs. One study [26]
used the WHO ICD-10 criteria. All five studies reported rates
of SAEs without stratifying by infants’ HIV status.
Figure 1. Flow diagram of screening process.
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
6

Coovadia et al. randomly assigned infants who had
received six weeks of once-daily NVP to continue a once-
daily NVP prophylaxis or placebo until six months of age [30].
Infants were followed-up until 18 months of age. At 12
months of age HIV transmission rates were 3.6% in the
placebo group and 2.8% in the NVP group.
Gray et al. compared ZDV given to infants for the first
six weeks of life to single dose (sd) NVP at delivery [26].
Cumulative HIV transmission rates at 12 weeks were 14.3%
in the sd NVP group and 18.1% in the ZDV group.
Jamieson et al. compared a control group of mothers given
sd NVP during labour or at delivery, and mothers and infants
receiving ZDV and lamivudine for one week, to two extended
ARV groups: postnatal either the mothers received HAART
or infants received daily NVP until 28 weeks of age [11].
At 48 weeks of follow-up, HIV transmission rates were 7%
in the control group and 4% in both extended ARV groups.
We combined the extended ARV groups to allow pairwise
comparison with the control group.
In the Kesho Bora Study [27] mothers received HAART
until weaning or a maximum of 6.5 months post-partum
(extended ARV group) or ZDV during pregnancy plus sd
NVP at onset of labour (short-course ARV group) [27]. By one
year of age 5.4% of infants in the extended ARV group
became HIV-infected compared to 9.5% in short-course
ARV group.
Kumwenda et al. compared sd NVP and ZDV given to
infants for the first week of life (control group) to 14 weeks
of NVP (extended NVP group) or 14 weeks of NVP plus ZDV
(extended NVP plus ZDV group) [9]. At nine months of
Table 3. Summary of included studies and outcomes assessed for each comparison
Comparisons Studies (Sample size) Outcomes assessed Studies
Breastfeeding vs. Infant formula feeding 4 (1741) Malnutrition
Growth
Respiratory tract infections
Diarrhoea
Becquet et al. 2007
Mbori-Ngacha et al. 2001
Kindra et al. 2012
Mbori-Ngacha et al. 2001
Venkatesh et al. 2011
Mbori-Ngacha et al. 2001
Becquet et al. 2007
Venkatesh et al. 2011
Kindra et al. 2012
Breastfeeding with extended ARV prophylaxis vs.
breastfeeding with short-course ARV prophylaxis
5 (7956) Growth faltering
Pneumonia
Gastroenteritis
Meningitis
Sepsis
Jamieson et al. 2012
Kesho Bora 2011
Kumwenda et al. 2008
Coovadia et al. 2012
Kesho Bora, 2011
Gray et al. 2005
Kumwenda et al. 2008
Kesho Bora, 2011
Jamieson et al. 2012
Coovadia et al. 2012
Kesho Bora, 2011
Gray et al. 2005
Kumwenda et al. 2008
Jamieson et al. 2012
Kumwenda et al. 2008
Jamieson et al. 2012
Kumwenda et al. 2008
Early cessation of breastfeeding vs. standard duration 2 (451) Growth
Prolonged diarrhoea
Arpadi et al. 2008
Fawzy et al. 2011
Chemically or biologically acidified infant formula vs.
standard infant formula
1 (132) Growth
Bronchopneumonia
Gastroenteritis
Velaphi et al. 2008
Concentrated infant formula vs. standard infant
formula
1 (1686) Growth Winter et al. 2009
Chemical acidified infant formula milk with or without
prebiotics and nucleotides
1 (84) Growth Cooper et al. 2010
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
7

age HIV transmission rates were 10.6%, 5.2% and 6.4% in the
control, the extended NVP and the extended NVP plus ZDV
groups, respectively. We combined the two extended ARV
groups for pairwise comparison with the control group.
Outcomes
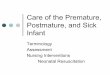
Growth faltering
The risk of growth faltering was 12% higher in infants on
extended ARV prophylaxis than short-course ARV prophylaxis
(RR�1.12; 95% CI�0.83 to 1.50) [9,11,27] (Figure 4).
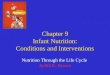
Pneumonia
The MD in incidence of pneumonia in the extended ARV
prophylaxis group was �0.01 (95% CI��0.02 to �0.00)
[9,11,26,27] (Figure 5).TheMDwas �0.02 (95% CI��0.03 to
�0.00) when we excluded the study with a high attrition rate.
Risk of pneumonia was similar between the groups in the
Coovadia study [30].
Meningitis
There was no difference in meningitis incidence between
extended and short-course ARV prophylaxis groups [9,11].
Gastroenteritis
There was no difference in rates of gastroenteritis between
extended and short-course ARV prophylaxis (MD�0.01; 95%
CI��0.01 to 0.02) [9,11,26,27] (Figure 6). Coovadia et al.
found no difference in risk of gastroenteritis between the two
groups (RR�0.90; 95% CI�0.61 to 1.33) [30].
Sepsis
Incidence of sepsis was similar between intervention groups
[9].
3. Early breastfeeding cessation versus standard duration
of breastfeeding
Two reports from a single RCT presented growth and diar-
rhoeal morbidity outcomes in HIV-exposed uninfected infants
whose mothers were randomly assigned to stop breastfeeding
at four months (intervention group) or to continue breastfeed-
ing for as long as they wished, with the median duration being
16.2 months (control group) [23,25]. HIV transmission rates
were 21.4% and 25.8% in the intervention and control groups,
respectively.
Outcomes
Growth
Weight-for-age z-scores at two years of age were similar
between infants stopping breastfeeding early compared to
continuing for a longer duration (MD�0.12; 95% CI��0.10
to 0.34) [23].
Prolonged diarrhoea
Diarrhoea lasting for at least seven days was defined as
prolonged [25]. During the 7�24 months age period, the
odds of having an episode of prolonged diarrhoea when
breastfeeding was stopped early were almost twice that of
breastfeeding for a longer duration (OR�1.70; 95% CI�1.28
to 2.26).
4. Chemically or biologically acidified formula versus
standard formula
Velaphi et al. compared infectious morbidity and growth
between HIV-exposed uninfected infants receiving chemically
or biologically acidified formula and those receiving standard
formula for the first four months [31].
Infants were randomly assigned to four groups:
1) Non-acidified (standard) whey-adapted starter formula
2) Chemically acidified standard formula, where acidifica-
tion was achieved through addition of L(�) lactic acid
3) Chemically acidified standard formula with Bifidobac-
terium lactis CNCM I-3446 added
4) Biologically acidified standard formula, where acidifica-
tion was achieved through bacterial fermentation
We combined the two chemically acidified formula groups
and the biologically acidified formula group for pairwise
comparison with the standard formula group.
Figure 2. Risk of bias for each domain per study.
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
8

Outcomes
Growth
Z-scores were calculated based on growth charts from the
Centre for Disease Control and Prevention (CDC) and were
presented up to four months of age. Head circumference-for-
age z-scores were significantly higher in infants who received
acidified formulas compared to infants who received stan-
dard formula (MD�0.31; 95% CI�0.15 to 0.48). The study
found no significant differences in WLZ-scores (MD�0.09;
95% CI��0.16 to 0.34), LAZ-scores (MD�0.08; 95%
CI��0.15 to 0.30) and WAZ-scores (MD�0.18; 95%
CI��0.05 to 0.41) between study groups.
Bronchopneumonia and gastroenteritis
The authors do not describe how infectious outcomes were
defined. Incidence of bronchopneumonia (MD 0.12; 95%
CI��0.03 to 0.27) and gastroenteritis (MD �0.07; 95%
CI��0.17 to 0.02) between birth and six months of age were
similar between infants on acidified formula and those on
standard formula.
5. Concentrated formula versus standard formula
Winter et al. assessed growth in HIV-exposed uninfected
infants randomly assigned to receive either 87 kcal/100mL
concentrated infant formula or 67 kcal/100mL standard
formula [29].
Outcomes
Growth
Z-scores were calculated using the 2000 National Centre
for Health Statistics paediatric growth references. Mean
WAZ-scores were significantly higher for infants on concen-
trated formula than standard formula (MD�0.12; 95%
CI�0.04 to 0.20). We found no significant differences in
WLZ-scores (MD�0.11; 95% CI��0.01 to 0.23), LAZ-
scores (MD�0.03; 95% CI��0.06 to 0.12), and head-
circumference-for-age z-scores (MD��0.03; 95% CI��0.11
to 0.05).
6. Chemically acidified formula with or without prebiotics
and nucleotides
Growth and infectious morbidity were compared in HIV-
exposed, uninfected infants on chemically acidified formula
alone and with prebiotics and nucleotides [24]. Infants were
randomly assigned to three study groups and followed-up
until six months of age:
1) Chemically acidified formula (control)
2) Chemically acidified formula with prebiotics (a blend of
short-chain and long chain fructo-oligosaccharides)
3) Chemically acidified formula with prebiotics and nu-
cleotides (a blend of cytidine, uridine, adenosine and
guanosine monophosphates)
Chemical acidification was achieved as in [31]. We combined
outcomes from infants in Groups 2 and 3 to allow pairwise
comparisons with Group 1.
Outcomes
Growth
Z-scores were calculated using the 2000 CDC growth charts.
The primary study report presented summary data and
Figure 4. Forest plot of breastfeeding with extended ARV prophylaxis vs. short-course ARV prophylaxis: Growth faltering.
Figure 3. Risk of bias graph for each domain across all studies.
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
9

corresponding 95% CIs in graph format. We estimated mean
z-scores and SDs from the graphs.
Mean WAZ-scores (MD�0.08; 95% CI��0.15 to 0.31)
and LAZ-scores (MD��0.14; 95% CI��0.39 to 0.1) were
similar in all groups.
DiscussionSummary of main findings
We reviewed findings from seven RCTs and three cohort
studies evaluating the effects of various postnatal interven-
tions for PMTCT of HIV.
From our meta-analysis, breastfeeding appears to decrease
the risk of respiratory infections by 35%, when infant feeding
mode is self-selected and when not considering infant HIV
status. However, this finding was not supported by the only
RCT reporting on this comparison. There is moderate quality
evidence that the risk of respiratory infection remains lower
(by 40%) in breast-fed infants through to two years of age,
after adjusting for infant HIV status [32].
The evidence from this review is inconsistent on the effect
of breast versus formula feeding on diarrhoeal morbidity.
In three observational studies, breastfeeding significantly
reduced the risk of diarrhoeal morbidity in early life [33,34],
and, of diminished magnitude until the second birthday [32].
We graded this evidence of moderate quality. A randomized
trial found no significant difference in diarrhoeal morbidity
between breast- and formula-fed infants up to two years
of age [28]. This trial was not powered to test equivalence of
diarrhoeal morbidity in the two arms. Therefore, it is impor-
tant to avoid interpreting the lack of statistical significance
as evidence of equivalent risk. Breastfeeding is expected to
reduce diarrhoea incidence. There are a few possible explana-
tions why this was not observed in this trial. HIV transmis-
sion was higher among breast-fed than formula-fed infants,
probably obscuring the protective effect of breastfeeding.
However, even when results from HIV-uninfected infants
were analysed separately, no significant difference was found.
A limitation of performing this type of sub-analysis is that the
comparison groups are no longer ‘‘as randomized,’’ therefore
not necessarily comparable in baseline characteristics, thus
possibly obscuring the true effect of breastfeeding. In our
opinion, the most likely explanation is that as 30% of mothers
assigned to the formula group had breastfed their infants [28],
some protective effect of breast milk occurred in the formula
group.
In the only RCT comparing breastfeeding versus formula
feeding, the risk of malnutrition was 37% lower in breast-fed
infants. Though not statistically significant, the reduction in
risk may be clinically important because the 95% CI includes
strongly protective values at the lower limit and excludes
values indicating appreciable harm from breastfeeding at the
upper limit. Also, high HIV transmission rates in breast-fed
infants would be expected to attenuate any protective effect
of breastfeeding, pulling the estimate towards the null.
On the other hand, high rates of non-compliance in the
formula-feeding group could be confounding this result. This
evidence is judged of low quality. Further research comparing
the nutritional outcomes of breast- versus formula-fed
infants of HIV-positive mothers is warranted.
We found moderate quality evidence that breastfeeding
with extended ARV prophylaxis is associated with fewer
pneumonia episodes compared to breastfeeding with short-
course ARV prophylaxis in HIV-exposed infants. The causal
explanation remains unclear. If evidence of this association
continues to accumulate, further investigation to explain the
underlying biological mechanisms should be prioritized.
However, high HIV transmission rates in infants on short-
course ARV prophylaxis, especially in studies contributing
substantial sample size to our meta-analysis [9,27], could
explain the higher incidence of pneumonia experienced by
infants in this group.
Our meta-analysis shows a modestly increased risk for
growth faltering among infants in the extended ARV group.
This estimate has a wide CI, which includes the null effect.
Figure 5. Forest plot of breastfeeding with extended ARV prophylaxis vs. short-course ARV prophylaxis: Pneumonia.
Figure 6. Forest plot of breastfeeding with extended ARV prophylaxis vs. short-course ARV prophylaxis: Gastroenteritis.
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
10

However, there is some evidence that infants exposed to ARV
therapy in utero, compared to postnatal ZDV, have reduced
growth up to two years of age [36]. Therefore, growth of
infants exposed to postnatal ARVs should be studied further.
We did not find the rates of any other SAEs to differ
significantly between infants in the extended and short-course
ARV prophylaxis groups. We do not believe that inadequate
follow-up explains the lackof observed differences. In addition,
with sample sizes of between 1898 and 5719 for different
outcomes, it seems reasonable to conclude that extended
ARV prophylaxis does not increase the risk for HIV-exposed
infants to experience non-HIV infections outcomes compared
to short-course ARV prophylaxis.
ConclusionsImplications for practice
Breastfeeding may reduce the risk of diarrhoeal morbidity,
respiratory tract infections and malnutrition compared to
formula feeding in HIV-exposed infants. Extended ARV
prophylaxis and formula feeding can effectively reduce or
prevent late postnatal transmission of HIV infection (19).
The magnitude of absolute benefit of breastfeeding com-
bined with extended ARV prophylaxis may be sufficient to
improve survival of children.
The benefits of breastfeeding with extended ARV prophy-
laxis must be weighed against the risk of HIV transmission
through breast milk when making decisions about feeding
HIV-exposed infants. Baseline risks, such as maternal viral
load, safety of ARVs and sustained adherence should also
influence decisions. Uptake of exclusive breastfeeding is
reportedly poor in most African settings [37,38]. Sub-optimal
infant feeding practices are likely to modify the effectiveness
of breastfeeding with ARV prophylaxis, especially in normal
practice settings. Continuous evaluation of these interventions
to determine whether their effectiveness remains clinically
important should be a priority as these interventions are
introduced into clinical practice.
Implication for research
Large prospective cohort studies with sufficient length of
follow-up are justified to investigate the effectiveness of
postnatal interventions for PMTCT of HIV in normal practice
settings. The studies should include infectious morbidity and
infant growth as primary outcomes. Effects of specific infant
formulas on growth require further evaluation.
Authors’ affiliations1Department of Paediatrics and Child Health, Children’s Infectious Disease
Clinical Research Unit, Stellenbosch University, Tygerberg, South Africa; 2MD/
PhD Program, Faculty of Medicine, University of British Columbia, Vancouver,
British Columbia, Canada; 3Department of Clinical Epidemiology and
Biostatistics, McMaster University, Hamilton, Ontario, Canada; 4Biostatistics
Unit/FSORC, St Joseph’s Healthcare Hamilton, Hamilton, Ontario, Canada;5Department of Pathology, Immunology Unit, NHLS, Stellenbosch University,
Tygerberg, South Africa
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
MZ: Contributed in conception and design of review, screened search results,
data extraction, analysis and interpretation, and writing of the manuscript.
GDM: Assisted in designing the review protocol, screened search results,
extracted data, rated evidence, and assisted with analysis and interpretation,
and writing of the manuscript. LT: Revised manuscript, gave input on statistical
analysis and interpretation. ME: Contributed in conception of review, edited
the manuscript and gave input on interpretation. MC: Contributed in
conception and design of review, edited the manuscript and gave input on
interpretation. All authors have read and approved the final manuscript.
Acknowledgements
The review authors thank Alvina Matthee for performing the electronic
database searches and authors of primary studies who provided requested
information.
Funding
This research has been supported by: The President’s Emergency Plan for AIDS
relief (PEPFAR) through HRSA under the terms of T84HA21652, Stellenbosch
University Faculty of Medicine and Health Sciences Clinical Research Grant,
South Africa Medical Research Council Self-Initiated Grant. GM is supported by
a CFRI-CIHR-UBC MD/PhD Studentship Award and a Canadian Institutes of
Health Research (CIHR) Vanier Canada Graduate Scholarship.
The funders had no role in study design, data extraction and analysis,
decision to publish, or preparation of the manuscript.
Disclaimer
The views expressed in this article are those of the authors and do not
necessarily reflect the view of the funders.
References
1. Traore AT, Querre M, Brou H, Leroy V, Desclaux A, Du Lou AD. Couples,
PMTCT programs and infant feeding decision-making in Ivory Coast. Soc Sci
Med. 2009;69(6):830�7.2. Muko KN, Tchangwe KG, Ngwa VC, Njoya L. Preventing mother-to-child
transmission: factors affecting mothers’ choice of feeding*a case study from
Cameroon. SAHARA-J. 2004;1(3):132�8.3. UNAIDS/WHO. AIDS epidemic update. Geneva, Switzerland: UNAIDS;
2007.
4. Taha TE, Graham SM, Kumwenda NI, Broadhead RL, Hoover DR, Markakis D,
et al. Morbidity among human immunodeficiency virus-1-infected and
-uninfected African children. Pediatrics. 2000;106(6):E77.
5. De Cock KM, Fowler MG, Mercier E, de Vincenzi I, Saba J, Hoff E, et al.
Prevention of mother-to-child HIV transmission in resource-poor countries:
translating research into policy and practice. JAMA. 2000;283(9):1175�82.6. Mepham SO, Bland RM, Newell ML. Prevention of mother-to-child
transmission of HIV in resource-rich and -poor settings. BJOG. 2011;118(2):
202�18.7. Creek TL, Kim A, Lu L, Bowen A, Masunge J, Arvelo W, et al. Hospitalization
and mortality among primarily nonbreastfed children during a large outbreak
of diarrhea and malnutrition in Botswana, 2006. J Acquired Immune Defic
Syndr. 2010;53(1):14�9.8. Six Week Extended-Dose Nevirapine (SWEN) Study Team, Bedri A, Gudetta
B, Isehak A, Kumbi S, Lulseged S, et al. Extended-dose nevirapine to 6 weeks of
age for infants to prevent HIV transmission via breastfeeding in Ethiopia, India,
and Uganda: an analysis of three randomised controlled trials. Lancet.
2008;372(9635):300�13.9. Kumwenda NI, Hoover DR, Mofenson LM, Thigpen MC, Kafulafula G, Li Q,
et al. Extended antiretroviral prophylaxis to reduce breast-milk HIV-1
transmission. N Engl J Med. 2008;359(2):119�29.10. Kilewo C, Karlsson K, Ngarina M, Massawe A, Lyamuya E, Swai A, et al.
Prevention of mother-to-child transmission of HIV-1 through breastfeeding by
treating mothers with triple antiretroviral therapy in Dar es Salaam, Tanzania:
the Mitra Plus study. J Acquir Immune Defic Syndr. 2009;52(3):406�16.11. Jamieson DJ, Chasela CS, Hudgens MG, King CC, Kourtis AP, Kayira D, et al.
Maternal and infant antiretroviral regimens to prevent postnatal HIV-1
transmission: 48-week follow-up of the BAN randomised controlled trial.
Lancet. 2012;379(9835):2449�58.12. World Health Organization. Consolidated guidelines on the use of
antiretroviral drugs for treating and preventing HIV infection [Internet]. 2013
[cited 2013 Jul 26]. Available from: http://www.who.int/hiv/pub/guidelines/
arv2013/download/en/
13. Black RE, Morris SS, Bryce J. Where and why are 10 million children dying
every year? Lancet. 2003;361(9376):2226�34.14. Onyango AW, Esrey SA, Kramer MS. Continued breastfeeding and child
growth in the second year of life: a prospective cohort study in western Kenya.
Lancet. 1999;354(9195):2041�5.
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
11

15. Baroncelli S, Pinnetti C, Genovese O, Tamburrini E, Floridia M. Hemato-
logical effects of zidovudine prophylaxis in newborn infants with and without
prenatal exposure to zidovudine. J Med Virol. 2011;83(3):551�6.16. McKoy JM, Bennett CL, Scheetz MH, Differding V, Chandler KL, Scarsi KK,
et al. Hepatotoxicity associated with long-versus short-course HIV prophylactic
nevirapine use: a systematic review and meta-analysis from the research
on adverse drug events and reports (RADAR) project. Drug Saf. 2009;32(2):
147�58.17. McArthur MA, Kalu SU, Foulks AR, Aly AM, Jain SK, Patel JA. Twin preterm
neonates with cardiac toxicity related to lopinavir/ritonavir therapy. Pediatr
Infect Dis J. 2009;28(12):1127�9.18. Kenny J, Musiime V, Judd A, Gibb D. Recent advances in pharmacovigilance
of antiretroviral therapy in HIV-infected and exposed children. Curr Opin HIV
AIDS. 2012;7(4):305�16.19. Horvath T, Madi BC, Iuppa IM, Kennedy GE,Rutherford G, Read JS.
Interventions for preventing late postnatal mother-to-child transmission of HIV.
Cochrane Database Syst Rev. 2009;(1):CD006734.
20. Deeks J, Higgins J, Altman D. Analysing data and undertaking meta-
analysis. In: Higgins JPT, Green S, editors. Cochrane handbook for systematic
reviews of interventions. West Sussex, England: John Wiley & Sons; 2008. p.
243�96.21. Van Belle G, Fisher DL, Heagerty JP, Lumley T. Biostatistics a methodology
for the health sciences. 2nd ed. Hoboken, NJ: John Wiley & Sons; 2004.
22. Brozek J, Oxman A, Schunemann H. GRADEpro. [Computer program] for
Windows; 2008;3:2.
23. Arpadi S, Fawzy A, Aldrovandi GM, Kankasa C, Sinkala M, Mwiya M, et al.
Growth faltering due to breastfeeding cessation in uninfected children born to
HIV-infected mothers in Zambia. Am J Clin Nutr. 2009;90(2):344�53.24. Cooper PA, Bolton KD, Mokhachane M, Velaphi SC, Mphahlele R, Bomela
HN, et al. Growth of infants born to HIV-positive mothers fed a whey-adapted
acidified starter formula with prebiotics and nucleotides. South Afr J Clin Nutr.
2010;23(2):90�5.25. Fawzy A, Arpadi S, Kankasa C, Sinkala M, Mwiya M, Thea DM, et al. Early
weaning increases diarrhea morbidity and mortality among uninfected children
born to HIV-infected mothers in Zambia. J Infect Dis. 2011;203(9):1222�30.26. Gray GE, Urban M, Chersich MF, Bolton C, van Niekerk R, Violari A, et al.
A randomized trial of two postexposure prophylaxis regimens to reduce
mother-to-child HIV-1 transmission in infants of untreated mothers. AIDS.
2005;19(12):1289�97.27. Kesho Bora Study Group. Triple antiretroviral compared with zidovudine
and single-dose nevirapine prophylaxis during pregnancy and breastfeeding for
prevention of mother-to-child transmission of HIV-1 (Kesho Bora study): a
randomised controlled trial. Lancet Infect Dis. 2011;11(3):171�80.28. Mbori-Ngacha D, Nduati R, John G, Reilly M, Richardson B, Mwatha A,
et al. Morbidity and mortality in breastfed and formula-fed infants of HIV-1-
infected women: a randomized clinical trial. JAMA. 2001;286(19):2413�20.29. Winter HS, Oleske JM, Hughes MD, McKinney RE Jr, Elgie C, Powell C, et al.
Randomized controlled trial of feeding a concentrated formula to infants born
to women infected by human immunodeficiency virus. J Pediatr Gastroenterol
Nutr. 2009;49(2):222�32.30. Coovadia HB, Brown ER, Fowler M, Chipato T, Moodley D, Manji K,
Musoke P, et al. Efficacy and safety of an extended nevirapine regimen in infant
children of breastfeeding mothers with HIV-1 infection for prevention of
postnatal HIV-1 transmission (HPTN 046): a randomised, double-blind, placebo-
controlled trial. Lancet. 2012;379(9812):221�8.31. Velaphi SC, Cooper PA, Bolton KD, Mokhachane M, Mphahlele RM, Beckh-
Arnold E, et al. Growth and metabolism of infants born to women infected
with human immunodeficiency virus and fed acidified whey-adapted starter
formulas. Nutrition. 2008;24(3):203�11.32. Becquet R, Bequet L, Ekouevi DK, Viho I, Sakarovitch C, Fassinou P, et al.
Two-year morbidity-mortality and alternatives to prolonged breast-feeding
among children born to HIV-infected mothers in Cote d’Ivoire. PLoS Med.
2007;4(1):17.
33. Kindra G, Coutsoudis A, Esposito F, Esterhuizen T. Breastfeeding in HIV
exposed infants significantly improves child health: a prospective study.
Matern Child Health J. 2012;16(3):632�40.34. Venkatesh KK, de Bruyn G, Marinda E, Otwombe K, van Niekerk R, Urban
M, et al. Morbidity and mortality among infants born to HIV-infected women in
South Africa: implications for child health in resource-limited settings. J Trop
Pediatr. 2011;57(2):109�19.35. Shapiro RL, Holland DT, Capparelli E, Lockman S, Thior I, Wester C, et al.
Antiretroviral concentrations in breast-feeding infants of women in Botswana
receiving antiretroviral treatment. J Infect Dis. 2005;192(5):720�7.36. Clayden P. Decreased growth in ART exposed uninfected infants in
Botswana. 5th International Workshop on HIV Pediatrics; 2013 Jun 28�29;Kuala Lumpur, Malaysia: HIV Treatment Bulletin; 2013.
37. Omari AA, Luo C, Kankasa C, Bhat GJ, Bunn J. Infant-feeding practices of
mothers of known HIV status in Lusaka, Zambia. Health Policy Plan. 2003;
18(2):156�62.38. Shapiro RL, Lockman S, Thior I, Stocking L, Kebaabetswe P, Wester C, et al.
Low adherence to recommended infant feeding strategies among HIV-infected
women: results from the pilot phase of a randomized trial to prevent mother-
to-child transmission in Botswana. AIDS Educ Prev. 2003;15(3):221�30.
Zunza M et al. Journal of the International AIDS Society 2013, 16:18865
http://www.jiasociety.org/index.php/jias/article/view/18865 | http://dx.doi.org/10.7448/IAS.16.1.18865
12