Embed Size (px)
Citation preview

Effects of Treatment with Oxandrolone for 4 Years on the Frequency ofSevere Arithmetic Learning Disability in Girls with Turner Syndrome
Judith L. Ross, MD, Michele M. M. Mazzocco, PhD, Harvey Kushner, PhD, Karen Kowal, PA, Gordon B. Cutler, Jr, MD,
and David Roeltgen, MD
Objectives To study androgen treatment effects on arithmetic performance in girls with Turner syndrome.Study design Forty-four girls, ages 10 to 14 years at baseline, completed 4 years of treatment with oxandrolone(Ox) or placebo (Pl). All received growth hormone and estrogen replacement therapy. We assessed the number ofgirls with severe learning disability (LD, standard score #5th percentile) on measures of academic arithmetic andreading achievement (WRAT-3, arithmetic and reading), given yearly, and the WIAT numerical operations (NOS)and reading subtests, given at year 4.Results On the WRAT-3 arithmetic, the frequency of severe arithmetic LD was similar in the Ox and Pl groups atbaseline and at years 1 and 2. At years 3 and 4, fewer girls in the Ox than Pl group had a severe arithmetic LD (year 4:0/22 vs 5/21, P = .02). On the WIAT NOS (year 4), fewer girls in the Ox than Pl groups had a severe arithmetic LD (3/21vs 8/20, P = .09). WIAT NOS error analysis suggested that the improved performance in the Ox group was associ-ated with better performance on multiplication and division (P < .01). The frequency of severe LD for the WRAT-3reading was similar for the Ox and Pl groups (all years) and for the WIAT reading subtest (year 4).Conclusions Androgen treatment for 4 years in girls with Turner syndrome resulted in a small decrease infrequency of severe arithmetic LD, with no effect on reading LD. (J Pediatr 2009;155:714-20).
Turner syndrome (TS) occurs in approximately 1 of every 2000 female births as the result of partial or complete lack of thesecond X chromosome. The ovaries in TS involute prematurely at 4 to 5 months’ gestation,1 which results in diminishedovarian estrogen and androgen production,2 absent spontaneous pubertal maturation, and infertility. Previous studies of
hormonal influences on cognition in TS have focused primarily on the role of estrogen deficiency. However, androgen levels arealso decreased in patients with TS3,4 because the normal ovary produces 50% of circulating androgen. TS therefore representsa unique androgen-deficient female population in which to determine the effects of androgen treatment during adolescence.
The TS cognitive phenotype typically includes normal-range verbal ability5-9 and relatively impaired nonverbal ability affect-ing spatial cognition (visual-spatial, perceptual, visual motor ability), working memory, and executive function.10-17 The rel-ative risk for arithmetic learning disabilities is increased in TS, starting in the primary school years.18-22 Relatively impairedarithmetic performance in TS is associated with increased operational and procedural errors and impaired math fact retrieval,perhaps secondary to slower response time, impaired working memory, and decreased executive and visual-spatialabilities.18-21,23 However, the link between math and visual-spatial deficits in TS is not always found.20
The complex cognitive phenotype in TS appears to be related to both hormonal and genetic factors. Estrogen replacement inpatients with TS during childhood has been associated with improvement in spatially mediated motor performance and non-verbal processing speed.24 Other cognitive deficits seen in TS such as those involving spatial abilities, working memory, andmathematics are apparently not ameliorated by estrogen replacement25 and may occur secondary to androgen deficiency or ge-netic haploinsufficiency.26 Correspondingly, population-based studies of normal variation in cognition have shown that malesversus females, on average, have superior mathematics performance,27-29 perhaps related to higher androgen levels in males.
These observations led us to hypothesize that androgen replacement in adolescent girls with TS would improve arithmeticperformance, as measured by arithmetic achievement tests. To test this hypothesis, we conducted a 4-year clinical trial (2-year
From Thomas Jefferson University (J.L.R., K.K.),Philadelphia, PA; the Department of Pediatrics and theduPont Hospital for Children (J.L.R.), Wilmington, DE;Kennedy Krieger Institute (M.M.M.M.), Johns HopkinsUniversity, Baltimore, MD; Biomedical ComputerResearch Institute (H.K.), Philadelphia, PA; theDevelopmental Endocrinology Branch (G.B.C.), NICHD,NIH, Bethesda, MD; and the Department of Neurologyand Center for Aphasia Research and Rehabilitation(D.R.), Georgetown University, Washington, DC
Supported by NIH NS32531. The authors declare noconflicts of interest.
0022-3476/$ - see front matter. Copyright � 2009 Mosby Inc.
All rights reserved. 10.1016/j.jpeds.2009.05.031
LD Learning disability
MRS Mathematics reasoning
NOS Numerical operations
Ox Oxandrolone
Pl Placebo
TS Turner syndrome
VIQ/PIQ Verbal IQ/performance IQ
WIAT Wechsler Individual Achievement Test
WISC Wechsler Intelligence Scale for Children
WRAT Wide Range Achievement Test
714

Vol. 155, No. 5 � November 2009
initial study plus 2-year extension) of 10- to 14 year-old girlswith TS treated with either androgen (oxandrolone, Ox) orplacebo (Pl).30 Oxandrolone was chosen as the androgenfor this study because of its overall safety record duringmore than 20 years in which it has been used to stimulategrowth in girls with TS.31,32
Methods
This 2-year extension study, to 4 years’ total duration, ofan ongoing double-blinded, randomized, placebo-con-trolled trial was conducted from 1993 to 2006 at ThomasJefferson University and at the Development EndocrinologyBranch of the National Institute of Child Health and Hu-man Development. The study was approved by humanstudies committees at both institutions, and informed con-sent and assent were obtained in all cases. The clinical trialwas registered with the National Institutes of Health (NIH,NCT00029159). A data and safety monitoring board re-viewed the extension study yearly from 1995 to 2003 andrecommended study continuation until all subjects hadcompleted the trial.
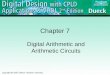
Subjects were randomly assigned (by the NIH ClinicalCenter Research Pharmacy) at baseline (before year 1 of theoriginal clinical trial) to receive daily treatment for 2 yearswith either (1) the oral nonaromatizable androgen Oxandro-lone (Ox, 0.06 mg/kg PO daily) or (2) placebo (Pl), both sup-plied by Bio-Technology General Corporation, Iselin, NewJersey (Figure 1). All study participants also received growthhormone (Humatrope, supplied by Eli Lilly and Company,Indianapolis, Indiana, 0.05 mg/kg SQ daily). Growth hor-mone treatment is FDA-approved for TS and is consideredstandard medical care. Study drug compliance was assessedby patient diaries and pill counts.
Inclusion criteria included karyotype diagnosis of TS,chronologic age 10 to 14 years at study entry, and no previoustreatment with androgen or estrogen. Study exclusion studycriteria were verbal IQ (VIQ) <2 SD (SS = 70; n = 5) or per-formance IQ (PIQ) >2 SD (SS = 130, n = 2), according to theDixon Gap Rule (testing for potential statistical outliers)33
Figure 1. Schematic representation of the study.
and the statistical analysis plan. At baseline, 41 and 35 subjects(n = 76) were randomly assigned into the Ox and Pl groups,respectively.
At the end of year 2 of the initial study, all participants wereinvited to continue in the extension study (Figure 1). All hadmet the study inclusion and exclusion criteria and continuedthe double-blinded study ([Ox or Pl] and growth hormone).A total of 26 subjects treated with Ox and 25 receiving Plchose to continue (15 subject treated with Ox and 10 receiv-ing Pl did not continue). The reasons for not continuing theextension were study disinterest, that is, satisfied with theirheight or the families no longer wanted to travel for the study.According to the extension protocol (Figure 1), all subjectsalso received estrogen replacement as 50 ng/kg/d ethinyl es-tradiol during year 3 and 100 ng/kg/d during year 4. At year3, 2 subjects treated with Ox and 1 receiving Pl, and at year4, 1 patient treated with Ox and 1 receiving Pl had dose reduc-tions of estrogen because of rapid onset of breast developmentor bone age advancement.
The protocol included achievement tests at baseline andyearly for 4 years. The auxologic treatment results will be re-ported separately. All study participants were monitored ev-ery 6 months for adverse effects related to androgen therapy.The evaluation included a physical examination for clitoralenlargement, acne or hirsutism, and a laboratory measure-ment of liver function. According to the protocol, the dosageof Ox or Pl was reduced by 50% if adverse effects on any ofthe measures were observed.
Compliance was estimated at each patient visit from bothpatient diaries and counts of dispensed versus returned cap-sules. The percent compliance was calculated as [number ofcapsules dispensed minus number of capsules returned]/[number of days from last visit to current visit]. By year 4 ofthe study, the Ox and Pl groups were prescribed, on average,81%� 24% and 97%� 10% of the protocol-specified dose, re-spectively, reflecting dosage reductions in some subjects. Com-pliance during the 2-year extension study (years 3 and 4) wassimilar in the Ox and Pl groups: 85% � 21% vs 85% � 18%.
A total of 44 subjects with TS, ages 10.0 to 14.9 years atentry, completed the 2-year extension study and were evalu-ated at the end of year 4 (23 Ox and 21 Pl) (Figure 1). Thediagnosis of TS was confirmed by karyotype; 50% were45,X and the remainder were mosaic (41%: 45,X/46,XX,45,X/46,X isochromosome X, or 45,X/46,X ring X) or hada nonmosaic partial deletion of one X chromosome (9%:Xp or Xq deletion). No subjects had a Y component to theirkaryotype. None had been treated previously with oxandro-lone, estrogen, or growth hormone.
SES levels were derived from the Hollingshead 2-FactorIndex of Social Status,34 based on parent education and occu-pation.
The achievement tests were administered in a standardizedmanner by trained psychometricians who were blinded totreatment assignment. All testing was conducted at ThomasJefferson University Hospital and the NIH by the same psy-chometricians. A certified school psychologist reviewed allresults.
715

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 155, No. 5
Intelligence was assessed at baseline with the Wechsler In-telligence Scale for Children-Revised (WISC-R).35
Mathematics performance was assessed with 2 widely usedstandardized achievement tests. The Wide Range Achieve-ment Test-3 arithmetic (WRAT-3) (15-minute time limit)36
was administered at baseline and yearly for 4 years. TheWRAT-3 arithmetic test, which has ‘‘blue’’ and ‘‘tan’’ formsto reduce learning effects by alternating forms yearly, evalu-ates ability to count, read symbols, solve oral problems, andperform computations. Correlation of results for the alter-nate color arithmetic forms was 0.93. Internal consistencyand reliability of the test, as measured by coefficient a, rangedfrom 0.92 to 0.95. The stability coefficients (test-retest reli-ability) for arithmetic ranged from 0.91 to 0.98.36 There isno formal schematic for error analysis among the differentnumeric operations (addition, subtraction, multiplication,and division) for the WRAT-3 arithmetic subtest.
The Wechsler Individual Achievement Test (WIAT)37 nu-merical operations (NOS), and mathematics reasoning(MRS) subtests (untimed tests) were administered once, atthe end of year 4, as additional measures of arithmetic perfor-mance. The WIAT NOS assesses ability to perform writtencalculations and basic numerical operations involving addi-tion, subtraction, multiplication, and division. There is a for-mal schematic for error analysis according to numericoperation for this subtest.37 The correlation of WIAT NOSwith WRAT-3 arithmetic is 0.79.37 The WIAT MRS measuresability to solve problems involving geometry, measurement,and statistics. The WIAT has good internal consistency anddoes not appear subject to sex or ethnic bias.37
The criterion for math learning disability (LD) in thisstudy was defined as a standard score <5th percentile (#76)for the general population, which corresponds approxi-mately to 2 grade levels behind age-matched peers.38 This isconsistent with reports of the average level of math achieve-ment reported for school-age girls with TS.21
Reading performance was assessed with (1) WRAT-3 read-ing ,36 an untimed test that measures single letter identifica-tion and single word recognition, administered at baselineand at yearly intervals; and (2) WIAT37 basic reading subtest,an untimed test that measures ability to decode letters andwords, administered once at the end of year 4. The correla-tion between performance on this subtest and on WRAT-3reading is 0.84.37 The criterion for reading LD in this studywas defined as a standard score <5th percentile (#76), corre-sponding to approximately 2 grade levels behind age-matched peers.38
StatisticsThe primary analysis was based on the continuous variable,WRAT-3 arithmetic standard score, and used a repeated-measures analysis of covariance (ANCOVA) comparing theOX and Pl groups at years 1, 2, 3, and 4, covarying for base-line WRAT-3 arithmetic and VIQ. Missing values werereplaced with last observation carried forward, and, if thebaseline level was missing, the first-year value was carriedbackward from year 1.
716
The secondary end point was comparison of the propor-tion of significant learning disability in arithmetic in theOx versus the Pl groups and was compared using Fisher exacttest. Changes from baseline were not examined. All statisticaltests were 2-tailed and were considered statistically signifi-cant at P < .05. All analyses were performed using SAS Statis-tical Analysis Software (Cary, North Carolina).
Results
The 2 TS treatment groups (23 Ox and 21 Pl) who completedthe 2-year extension (4 years of treatment) were well matchedfor baseline age, socioeconomic status, race, handedness,proportion of nonmosaic 45,X subjects, VIQ, and PIQ(Table I). As expected, both groups demonstrated lowerPIQ than VIQ. A total of 26 Ox subjects started the extensionat the end of year 2, 2 dropped out in year 3, and 1 droppedout in year 4 because of study disinterest. A total of 25 Pl sub-jects started the extension at the end of year 2, 3 dropped outin year 3, and 1 dropped out in year 4 because of study dis-interest (n = 3) and behavior issues (n = 1).
At baseline, the Ox and Pl groups were well matched formean WRAT-3 arithmetic subtest performance (Figure 2,A). At years 1, 2, 3, and 4, performance was higher in theOx vs Pl groups, but the difference was not statistically signif-icant (P = .48, ANCOVA, Figure 2, A). Effect sizes rangedfrom 29% to 46% during the 4 years of the study. At baselineand years 1 and 2, there were no differences between the Oxand Pl groups in the frequency of severe arithmetic LD fromthe WRAT-3 arithmetic subtest (Figure 2, B). At years 3 and4, however, significantly fewer subjects in the Ox versus Plgroups had severe arithmetic LD on this timed task (Figure 2,B). At year 4, the mean raw scores were slightly but not sig-nificantly higher in the Ox versus the Pl groups, respectively(35.6 � 5.2 vs 33.4 � 9.6, P = .36).
On the untimed WIAT NOS, given at year 4, fewer subjectsin the Ox than Pl groups had a score #76, although the dif-ference between the groups was not statistically significant(3/21 vs 8/20, P = .09). However, the mean raw scores forthe Ox group were significantly higher than the Pl group(34.2 � 5.0 vs 30.0 � 6.2, P = .02). In contrast, results fromthe untimed WIAT mathematical reasoning subtest, whichmeasures more heterogeneous, complex arithmetic tasksthan either the WIAT NOS or WRAT-3 arithmetic, were sim-ilar for both treatment groups (0/22 vs 2/20, P = .22).
Table I. Baseline demographic and IQ information
TS-Ox TS-Pl P value
n 23 21Chronologic age 11.5 � 1.5 11.9 � 1.7 .39SES 48 � 10 49 � 10 .65% Caucasian 87% 71% .27% Right-handed 96% 91% .60% 45,X 61% 48% .54VIQ 104 � 14 102 � 14 .72PIQ 95 � 13 96 � 16 .56
Ross et al

November 2009 ORIGINAL ARTICLES
With the same criterion for severe LD (<5th percentile[# 76]), the frequency of severe reading disability, as mea-sured by the WRAT-3 reading subtest, was similar for theOx and Pl groups at baseline and all subsequent years (base-line: 0/19 vs 3/17, year 1: 0/19 vs 2/17, year 2: 0/20 vs 2/17,year 3: 0/20 vs 2/17, year 4: 0/19 vs 2/17). Likewise, no signif-icant difference between groups was observed on the WIATword reading subtest at year 4 (0/22 vs 2/15).
To define arithmetic error patterns, WIAT NOS errorrates, according to the mathematical operation required fora correct solution, were examined (Table II). The Ox groupcorrectly completed more items than the Pl group for themultiplication and division questions. Additionally, the Oxgroup had superior multiplication and division performance
Figure 2. A, Performance of subjects treated with Ox versusPl on WRAT-3 arithmetic (least-square means, ANCOVA). B,Proportion of subjects treated with Ox versus Pl with arith-metic LD.
Effects of Treatment with Oxandrolone for 4 Years on the FrequTurner Syndrome
in both the LD and the non-LD subpopulations (data notshown). For other operations, including addition, subtrac-tion, fractions, and algebraic computation, the Ox grouphad slightly more correct items than Pl, but the differencedid not reach statistical significance.
There were no treatment-related deaths or severe adverseevents. Potential androgen-associated increased liver func-tion (defined as increased SGPT [ > 100 U/L], n = 3 Ox[137, 105, 118 U/L], n = 1 Pl [117 U/L]) and hypertension(n = 1 Ox, n = 0 Pl) were slightly more frequent in the Oxgroup. The increased SPGT was mild in all subjects andhad decreased to normal at subsequent visits (data notshown). In addition to these events, 50% dose reductionsfor clitoral changes were made in 2 subjects treated withOx and 2 receiving Pl, for acne in 1 patient treated withOx, and for mild hirsutism in 3 patients receiving Ox, gener-ally within the first year of the study. In each case, the clinicalchanges resolved with dose reductions.
Discussion
The results of this randomized, double-blinded, placebo-controlled study in girls with TS, treated with Ox or PL for4 years as well as growth hormone for 4 years and pubertalestrogen replacement therapy for the 3rd and 4th years, areconsistent with our hypothesis that androgen replacementin girls with TS has a positive effect on arithmetic perfor-mance. Although the mean WRAT-3 arithmetic performancewas higher in the Ox group than the Pl group at years 1, 2, 3,and 4, the differences in the primary outcome measure werenot statistically significant in the ANCOVA analysis, reflect-ing the small sample size. However, the effect sizes were mod-erate and ranged from 29% to 46%. In the secondary analysis,significantly fewer subjects in the Ox group compared withthe Pl group had severe arithmetic LD as determined byperformance on the WRAT-3 arithmetic test by years 3 and4. A similar trend, which did not reach statistical significance,was observed for an additional measure of arithmetic perfor-mance, the WIAT NOS. Because the groups were wellmatched for age, SES and other baseline measures, as wellas for treatment with growth hormone and estrogen, thesedifferences are likely to be related to an Ox treatment effect.
The frequency of severe arithmetic LD, as measured by theWRAT-3 arithmetic subtest, increased progressively in the Plgroup but not in the Ox group over the 4 years of treatment.
Table II. WIAT numerical operations subtest by number of correct operation (year 4)
n Addition/subtraction* Multiplication/division* Fractions* Algebra*
No. of items† 16 8 6 3Ox group total 21 15.1 � 1.0 7.0 � 1.0 3.9 � 2.0 2.1 � 1.3Pl group total 20 14.6 � 1.4 5.6 � 1.9 2.9 � 1.9 1.4 � 1.4P valuez .21 .006 .10 .11
*Operation for item defined in the WIAT manual.37
†Number of items for these operations.zt test: comparison of Ox and Pl groups.
ency of Severe Arithmetic Learning Disability in Girls with 717

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 155, No. 5
In contrast, the frequency of severe reading LD, as measuredby the WRAT-3 reading subtest, did not change in either theOx or the Pl groups. We interpret these results as suggestingthat androgen (Ox) improved the acquisition of arithmeticskills such that girls treated with Ox remained within 2 gradelevels for arithmetic performance, whereas girls treated withPl were more likely to fall further behind. Previous studies ofelementary school–age girls with TS reveal that they tend tofall further behind their peers during primary school41 andcontinue to be at increased risk for math LD into the middleschool years.49 This same pattern emerged in the presentstudy, but only for the Pl group.
Difficulties with mathematics are reported in approxi-mately half of girls and women with TS.18,22,39 Previously,Temple and Marriott23 noted impaired calculation abilityin TS, with predominant difficulty in multiplication and di-vision rather than addition and subtraction. In the currentstudy, error analysis by type of operation in the WIATNOS suggested that the improved performance in the Oxgroup was associated with significantly better performanceon multiplication and division problems rather than onaddition, subtraction, or improved algebra skills, in agree-ment with Temple and Marriott.23
There was an apparent inconsistency between the WIATNOS and the WIAT MRS subtest for the placebo subjects,with a 40% frequency of severe learning disability for theNOS versus a 10% frequency for the MRS. In these untimedtests, girls with TS appear to perform better on the higher-or-der tasks of the WIAT MRS than on the basic calculations ofthe NOS. There was also an apparent disparity between theWIAT NOS and the WRAT3 results in that the frequencyof severe arithmetic LD in the Ox group versus the Pl groupreached statistical significance for the WRAT-3 (P = .02) butnot for the WIAT NOS (0.09). This apparent disparity mayresult from qualitative differences in the skills tested orfrom the difference between timed (WRAT-3) and untimed(WIAT NOS) tests. Math difficulties in girls with TS aremost apparent during timed testing.40
This study provides little insight into how Ox may haveaffected the brain. Whether the androgen effect in thisstudy is due to organizational effects that appear only afteryears of treatment, or to shorter-term activation effects onmore basic spatial and temporal information processingthat ultimately improve cumulative acquisition of mathskills, is uncertain. However, a potential brain impact ofOx is suggested by the observation, from imaging studies,that adult women with TS who were treated with oxandro-lone in childhood had a larger left caudate and increasedparietal lobe neuronal density.41 The caudate has richconnections with frontal regions, an area associated withworking memory.42 Previously, we showed improved per-formance on tests of working memory in girls with TS aftercumulative Ox exposure for 2 years,30 which seems moreconsistent with changes in brain structure or organizationthan with acute changes in function or physiology. Addi-tionally, studies in animals indicate that androgen may af-fect the nervous system by increasing cell number and
718
dendritic structure.43 Similar changes, over time, mightexplain androgenic effects on cognition in TS.
Previous studies have identified specific brain structuresassociated with defined components of mathematic process-ing44-46 that are likely targets of androgen. They includestructures associated with (1) number processing (compre-hension and production of numbers), in the left frontaland temporal regions, and (2) calculation (number factsand procedural knowledge), in the right parietal cortex.44,45
Recent functional imaging studies in TS suggest that reducedgray matter in the right intraparietal sulcus is related to num-ber processing difficulties.47,48
There are several additional limitations of this study. First,only 67% of the original 76 randomly assigned subjects en-tered the 2-year extension study, and only 58% completedthe full 4-year study. Thus, there may have been bias in thechildren who chose to continue in the extension, althoughsuch a bias, if any, was not detected in any of the baselinemeasures. Second, age may be an important variable in theresponse to Ox, and, in particular, the effects of Ox in youn-ger girls (<10) may be different. Third, we defined arithmeticLD arbitrarily as performance below the 5th percentile, whichis relatively severe performance impairment (2 grade levelsbelow the child’s grade); however, this definition is consistentwith the frequency of math disability reported in typically de-veloping children (�6%).49 Fourth, all children were treatedwith estrogen during the 2-year duration of this extension,and potential interactions between estrogen and oxandrolonemay have affected the outcome.
Last, in this study, we used the oral androgen Ox. BecauseOx levels in blood cannot be measured directly and do notcross-react with testosterone, it was not possible to determineif the treatment doses were physiological and match whata 10- to 14-year-old girl’s ovary would produce. Althoughthe frequency of side effects related to virilization was lowand study participants were closely monitored, these side ef-fects could occur with Ox treatment. Also, the effects of tes-tosterone, the major circulating androgen in males andfemales, some of which is aromatized to estradiol, may differfrom Ox, which is nonaromatizable. Thus, we could not de-termine whether Ox treatment is an exact model for treatingthe androgen (testosterone) deficiency in TS and whether Oxtreatment reflects the difference in testosterone levels relatedto the development of mathematics abilities in men versuswomen or in girls with TS versus girls with 46,XX goingthrough puberty.
In conclusion, low-dose androgen treatment in adolescentgirls with TS was associated with a decreased frequency of se-vere arithmetic learning disability after 3 and 4 years of treat-ment. Because mathematics learning disabilities are animportant and persistent problem in TS,50 an effective andsafe pharmacological intervention, such as replacing deficientlevels of androgen, would provide an important benefit forthis population in addition to standard cognitive remedia-tion. However, at the current time, treatment of girls withTS with androgen to improve cognitive function should stillbe regarded with caution. The optimal dose and duration of
Ross et al

November 2009 ORIGINAL ARTICLES
treatment, and the optimal age of treatment initiation forneural and cognitive development, are unknown. n
Submitted for publication Nov 13, 2008; last revision received April 14, 2009;
accepted May 21, 2009.
Reprint requests: Dr Judith L. Ross, Thomas Jefferson University, Department
of Pediatrics, Suite 726, 1025 Walnut Street, Philadelphia, PA 19107. E-mail:
References
1. Singh R, Carr D. The anatomy and histology of XO human embryos and
fetuses. Anat Rec 1966;155:369-84.
2. Palmer CG, Reichmann A. Chromosomal and clinical findings in 110
females with Turner syndrome. Hum Genet 1976;35:35-49.
3. Gravholt CH, Svenstrup B, Bennett P, Sandahl Christiansen J. Reduced
androgen levels in adult Turner syndrome: influence of female sex ste-
roids and growth hormone status. Clin Endocrinol (Oxf) 1999;50:
791-800.
4. Apter D, Lenko HL, Perheentupa J, Soderholm A, Vihko R. Subnormal
pubertal increases of serum androgens in Turner’s syndrome. Horm Res
1982;16:164-73.
5. Hall JG, Gilchrist DM. Turner syndrome and its variants. Pediatr Clin
North Am 1990;37:1421-40.
6. Rovet JF. The cognitive and neuropsychological characteristics of fe-
males with Turner syndrome. In: Bender B, Berch D, editors. Sex Chro-
mosome Abnormalities and Behavior. Psychological Studies. Boulder,
CO; Westview Press; 1991. p. 39-77.
7. Robinson A, Bender BG, Linden MG, Salbenblatt JA. Sex chromosome
aneuploidy: the Denver Prospective Study. Birth Defects 1990;26:
59-115.
8. Ratcliffe SG, Butler GE, Jones M. Edinburgh study of growth and devel-
opment of children with sex chromosome abnormalities, IV. Birth
Defects 1991;26:1-44.
9. Stewart DA, Bailey JD, Netley CT, Park E. Growth, development, and be-
havioral outcome from mid-adolescence to adulthood in subjects with
chromosome aneuploidy: the Toronto Study. Birth Defects Orig Artic
Ser 1990;26:131-88.
10. Waber D. Neuropsychological aspects of Turner syndrome. Develop
Med Child Neurol 1979;21:58-70.
11. McCauley E, Kay T, Ito J, Treder R. The Turner syndrome: cognitive def-
icits, affective discrimination, and behavior problems. Child Dev 1987;
58:464-73.
12. Bender BG, Linden MG, Robinson A. Neuropsychological impairment
in 42 adolescents with sex chromosome abnormalities. Am J Med Genet
1993;48:169-73.
13. Bender B, Puck M, Salbenblatt J, Robinson A. Cognitive development of
unselected girls with complete and partial X monosomy. Pediatrics 1984;
73:175-82.
14. Romans SM, Stefanatos G, Roeltgen DP, Kushner H, Ross JL. Transition
to young adulthood in Ullrich-Turner syndrome: neurodevelopmental
changes. Am J Med Genet 1998;79:140-7.
15. Buchanan L, Pavlovic J, Rovet J. A reexamination of the visuospatial def-
icit in Turner syndrome: contributions of working memory. Dev Neuro-
psychol 1998;14:341-67.
16. Ross JL, Kushner H, Roeltgen DP. Developmental changes in motor
function in girls with Turner syndrome. Pediatr Neurol 1996;15:
317-22.
17. Haberecht MF, Menon V, Warsofsky IS, White CD, Dyer-Friedman J,
Glover GH, et al. Functional neuroanatomy of visuo-spatial working
memory in Turner syndrome. Hum Brain Mapp 2001;14:96-107.
18. Mazzocco M. Math learning disability and math LD subtypes: evidence
from studies of Turner syndrome, Fragile X syndrome, and neurofibro-
matosis Type 1. J Learn Disabil 2001;34:520-33.
19. Mazzocco MM. A process approach to describing mathematics difficul-
ties in girls with Turner syndrome. Pediatrics 1998;102:492-6.
Effects of Treatment with Oxandrolone for 4 Years on the FrequTurner Syndrome
20. Rovet J, Szekely C, Hockenberry MN. Specific arithmetic calculation def-
icits in children with Turner syndrome. J Clin Exp Neuropsychol 1994;
16:820-39.
21. Rovet JF. The psychoeducational characteristics of children with Turner
syndrome. J Learn Disabil 1993;26:333-41.
22. Murphy MM, Mazzocco MM, Gerner G, Henry AE. Mathematics learn-
ing disability in girls with Turner syndrome or fragile X syndrome. Brain
Cogn 2006;61:195-210.
23. Temple CMMA. Arithmetic ability and disability in Turner’s syndrome:
a cognitive neuropsychological analysis. Dev Neuropsychol 1996;14:47-67.
24. Ross JL, Roeltgen D, Feuillan P, Kushner H, Cutler GB Jr. Effects of
estrogen on nonverbal processing speed and motor function in girls
with Turner’s syndrome. J Clin Endocrinol Metab 1998;83:3198-204.
25. Ross JL, Roeltgen D, Feuillan P, Kushner H, Cutler GB Jr. Use of estrogen
in young girls with Turner syndrome: effects on memory. Neurology
2000;54:164-70.
26. Ross JL, Roeltgen D, Kushner H, Wei F, Zinn AR. The Turner syndrome-
associated neurocognitive phenotype maps to distal Xp. Am J Hum
Genet 2000;67:672-81.
27. Hedges LV, Nowell A. Sex differences in mental test scores, variability,
and numbers of high-scoring individuals. Science 1995;269:41-5.
28. Arceneaux JM, Cheramie GM, Smith CW. Gender differences in WAIS-R
age-corrected scaled scores. Pecept Mot Skills 1996;83:1211-5.
29. Snow WG, Weinstock J. Sex differences among non-brain-damaged
adults on the Wechsler Adult Intelligence Scales: a review of the litera-
ture. J Clin Exp Neuropsychol 1990;12:873-86.
30. Ross J, Roeltgen D, Stefanatos GA, Feuillan F, Kushner H, Bondy C,
Cutler GB Jr. Androgen-responsive aspects of cognition in girls with
Turner syndrome. J Clin Endocrinol Metab 2003;88:292-6.
31. Rudman D, Goldsmith M, Kutner M, Blackston D. Effect of growth hor-
mone and oxandrolone singly and together on growth rate in girls with X
chromosome abnormalities. J Pediatr 1980;96:132-5.
32. Rosenfeld RG, Frane J, Attie KM, Brasel JA, Burstein S, Cara JF, et al. Six-
year results of a randomized, prospective trial of human growth hor-
mone and oxandrolone in Turner syndrome. J Pediatr 1992;121:49-55.
33. Dixon WJ. Analysis of extreme values. Ann Math Statist 1950;21:488-506.
34. Hollingshead AB, Redlich F. Social Class and Mental Illness. New York,
NY: John Wiley; 1958.
35. Wechsler D. Manual for the Wechsler Intelligence Scale for Children-
Revised. New York, NY: Psychological Corporation; 1974.
36. Wilkinson G. WRAT3 Administration Manual. Wilmington, DE: Wide
Range, Inc; 1993.
37. Wechsler D. Manual: Wechsler Individual Achievement Test. San Anto-
nio, TX: The Psychological Corporation; 1992.
38. Shalev RS, Manor O, Auerbach J, Gross-Tsur V. Persistence of develop-
mental dyscalculia: what counts? Results from a 3-year prospective fol-
low-up study. J Pediatr 1998;133:358-62.
39. Ross JL, Stefanatos GA, Kushner H, Zinn A, Bondy C, Roeltgen D. Per-
sistent cognitive deficits in adult women with Turner syndrome. Neurol-
ogy 2002;58:218-25.
40. Mazzocco MM, Singh Bhatia N, Lesniak-Karpiak K. Visuospatial skills
and their association with math performance in girls with fragile X or
Turner syndrome. Child Neuropsychol 2006;12:87-110.
41. Cutter WJ, Daly EM, Robertson DM, Chitnis XA, van Amelsvoort TA,
Simmons A, et al. Influence of X chromosome and hormones on human
brain development: a magnetic resonance imaging and proton magnetic
resonance spectroscopy study of Turner syndrome. Biol Psychiatry 2006;
59:273-83.
42. Scherf KS, Sweeney JA, Luna B. Brain basis of developmental change in
visuospatial working memory. J Cogn Neurosci 2006;18:1045-58.
43. MacLusky NJ, Hajszan T, Prange-Kiel J, Leranth C. Androgen modu-
lation of hippocampal synaptic plasticity. Neuroscience 2006;138:
957-65.
44. Molko N, Cachia A, Riviere D, Mangin JF, Bruandet M, Le Bihan D, et al.
Functional and structural alterations of the intraparietal sulcus in a devel-
opmental dyscalculia of genetic origin. Neuron 2003;40:847-58.
45. Dehaene S, Molko N, Cohen L, Wilson AJ. Arithmetic and the brain.
Curr Opin Neurobiol 2004;14:218-24.
ency of Severe Arithmetic Learning Disability in Girls with 719

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 155, No. 5
46. Kesler SR, Menon V, Reiss AL. Neuro-functional differences associated
with arithmetic processing in Turner syndrome. Cereb Cortex 2006;16:
849-56.
47. Molko N, Cachia A, Riviere D, Mangin JF, Bruandet M, LeBihan D, et al.
Brain anatomy in Turner syndrome: evidence for impaired social and
spatial-numerical networks. Cereb Cortex 2004;14:840-50.
720
48. Dehaene S, Spelke E, Pinel P, Stanescu R, Tsivkin S. Sources of mathematical
thinking: behavioral and brain-imaging evidence. Science 1999;284:970-4.
49. Kosc L. Developmental dyscalculia. J Learn Disabil 1974;7:46-59.
50. Murphy MM, Mazzocco MM. Mathematics learning disabilities in girls
with fragile X or Turner syndrome during late elementary school. J Learn
Disabil 2008;41:29-46.
Ross et al





![Klinische Richtlijn Turner Syndroom - VKGN richtlijn Turner... · Klinische Richtlijn Turner Syndroom Nederlands-Vlaams Multidisciplinair Netwerk Turner Syndroom Oktober 2012 [2]](https://img.pdfslide.net/doc/110x75/6051868ca1b38602122de530/klinische-richtlijn-turner-syndroom-vkgn-richtlijn-turner-klinische-richtlijn.jpg)