Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
y 42 (2009) 367–373www.jecgonline.com
Journal of Electrocardiolog
Effects of verapamil on anterior ST segment and ventricular fibrillationcycle length in patients with Brugada syndrome
Masaomi Chinushi, MD,a,⁎ Kenichi Iijima, MD,b Minoru Tagawa, MD,b Satoru Komura, MD,b
Hiroshi Furushima, MD,b Yoshifusa Aizawa, MDb
aSchool of Health Science, Niigata University School of Medicine, Niigata, JapanbFirst Department of Internal Medicine, Niigata University School of Medicine, Niigata, Japan
Received 28 January 2009
Abstract Purpose: This study examined the effects of verapamil (5-10 mg intravenous) on the cardiac
⁎ Corresponding aSchool of Medicine, 2
E-mail address: m
0022-0736/$ – see frodoi:10.1016/j.jelectroc
electrical activity of 10 Brugada syndrome (BS) patients having vasospastic angina, atrial fibrillation,and/or hypertension.Results: Verapamil showed no significant change in the ST-segment elevation. Likewise, there wasno significant change in the lengths of QRS complex, HV and corrected QT intervals, or effectiverefractory period at the right ventricle. The conduction time between right ventricular apex andoutflow tract, measured at 400-millisecond pacing, was mildly prolonged by verapamil. At baseline,induced ventricular fibrillation (VF) was terminated by a 200-J shock in all patients. After verapamil,VF was reinduced in 7, was noninducible in 2, and self-terminated in 1 patient. Mean F-F intervalwas shorter after than before verapamil, and a 360-J shock was required in 2 of the 7 patients.Conclusion: In some BS patients, calcium channel blockade may modify the electricalcharacteristics of VF.© 2009 Elsevier Inc. All rights reserved.
Keywords: Brugada syndrome; Calcium channel blockade; Ventricular fibrillation; Cardiac defibrillation
Introduction
In patients without structural heart disease, ST-segmentelevation with coved-type morphology in leads V1 to V3 ofthe electrocardiogram (ECG) is a diagnostic sign of Brugadasyndrome (BS).1,2 The infusion of isoproterenol attenuatesthe ST-segment elevation and limits the frequency ofventricular arrhythmic episodes in BS.3,4 This observationsupports that hypothesis because the augmentation of theinward calcium (Ca2+) current by isoproterenol promotes thecreation of the phase 2 dome of the action potential andmitigates the dispersion of right ventricular (RV) repolariza-tion. Conversely, the inhibition of the inward Ca2+ current byCa2+ channel blockers may be proarrhythmic, though thishas not been confirmed clinically.
Calcium channel blockers have been prescribed as first-line therapy in patients with vasospastic angina, atrial
uthor. School of Health Science, Niigata University-746 Chuo-ku Asahimachi, Niigata 951-8518, [email protected]
nt matter © 2009 Elsevier Inc. All rights reserved.ard.2009.03.009
fibrillation or hypertension, and cardiovascular disordersthat sometimes coexist in patients with BS.5,6 Therefore, in10 BS patients having vasospastic angina, atrial fibrillation,and/or hypertension, we examined the electrophysiologiceffects of verapamil, 5 to 10 mg, administered intravenously.
Study population and methods
This study included 10 men from different families,between the ages of 30 and 72 years (mean, 49 ± 11), referredto our hospital for evaluation of ST-segment elevation inleads V1 to V3 (Table 1). Two patients had a history ofsyncope (2 times in patient no. 1 and one time in patient no.8), and 4 other patients were reported having chestoppression. No patient had a history of rescue from a cardiacarrest, though 2 patients had family histories of sudden deathfrom unknown causes (b45 years old). Hypertension wasdemonstrated in 6 patients, and paroxysmal atrial fibrillationwas observed in 3 patients (Table 1). Structural heart diseasewas ruled out by detailed cardiac investigations. The patientswith histories of syncope underwent brain computed

Table 1Clinical characteristics of 10 men presenting with BS
Patient no. Age/sex Family history Clinical symptoms ECG type at rest Hypertension/PAF Pilsicainide test Spasm provocation
1 30 Negative Syncope 2 PAF Positive Negative2 40 Positive Chest oppression 1 & 2 None Positive RCA3 43 Negative Chest oppression 1 & 2 None Positive LADA & RCA4 46 Negative None 1 & 2 Hypertension Positive Negative5 47 Negative None 1 & 2 Hypertension Positive Negative6 49 Negative Chest oppression 1 & 2 Hypertension Positive Negative7 50 Negative None 1 & 2 Hypertension Positive Negative8 53 Negative Syncope 1 Hypertension, PAF Not performed Negative9 58 Positive None 1 Hypertension Positive RCA10 72 Negative Chest oppression 1 & 2 PAF Positive Negative
LADA indicates left anterior descending artery; RCA, right coronary artery; PAF, paroxysmal atrial fibrillation.
368 M. Chinushi et al. / Journal of Electrocardiology 42 (2009) 367–373
tomography, electroencephalogram, and head-up tilt testing,all of which were normal. No patient had receivedmedications for cardiovascular diseases before the initialevaluation. Genetic analysis of SCN5A was performed inpatient no. 9, revealing the presence of a R893H mutation.7
Surface ECGs
At baseline, all patients were in normal sinus rhythmand presented with abnormal repolarization patterns onsurface ECG.1 Type 1 (coved-type) more than 2-mm ST-segment elevation followed by an inverted T wave wasobserved in 2 patients. Type 2 (saddleback-type) with a2-mm or more ST-segment takeoff, followed by a troughwith 1-mm or more ST-segment elevation, and a positive orbiphasic T wave, was observed in 1 patient. Type 2 and,occasionally, type 1 abnormalities were both observed atbaseline in the other 7 patients. After the administration ofpilsicainide, type 1 ST-segment elevation manifested andbecame prominent in all patients.
Pharmacologic testing
Pharmacologic testing was performed after informedconsent was obtained from the patient.
Pilsicainide testPilsicainide, 1 mg/kg for 5 minutes, was administered
intravenously at the bedside during continuous monitoring.8
In patients presenting with type 2 repolarization abnorma-lities before administration of the drug, the test wasconsidered positive when there is development of type 1repolarization abnormalities.9 In patients presenting with type1 repolarization abnormalities at baseline, the test wasconsidered positive when the ST segment rose by more than2 mm compared with baseline. We discontinued the druginfusion immediately after confirmation of a positive response.
Verapamil testOn a separate day, verapamil, up to 10 mg, was
administered intravenously during electrophysiologicstudy (EPS) and discontinued if the systolic bloodpressure decreased by more than 20 mm Hg or theheart rate decreased or increased by more than 10%. Thereason behind this was thought to be augmentation ofsympathetic nerve activity in association with a negativeinotropic effect of verapamil that might counteract with
the cardiac electrical instability of BS. Neither prematureventricular complexes nor ventricular tachycardia deve-loped as a result of the intravenous administration ofverapamil or pilsicainide.
Cardiac catheterization
After informed consent was obtained, a cardiaccatheterization was performed in the nonsedated, post-absorptive state. After confirming the absence of signifi-cant stenosis in all epicardial coronary arteries, aprovocation test of coronary vasospasms was performedby the intracoronary administration of ergonovine maleate(50 μg) in all patients. This was because 6 patients in thisstudy had episodes of syncope and/or chest oppression,and previous studies suggested that the incidence ofcoronary vasospasms was relatively high in patients withBS even if the patients had not complained of chestoppression.10 If the coronary vasospasm was induced,isosorbide dinitrate (5 mg) was immediately injected in thecoronary artery to relieve the spasm. Angiograms of theleft and right coronary arteries were repeated in all patientsafter the injection of isosorbide dinitrate.
Electrophysiologic study was performed after the cor-onary angiogram, using 6F quadripolar electrode catheters.Endocardial stimulation was performed between the distaland third electrodes, and the intracardiac electrograms wererecorded at a band-pass filter set at 30 to 500 Hz, between thesecond and proximal electrodes. Programmed electricalstimulation (PES) was delivered at twice the late diastolicthreshold and a 2-millisecond pulse width. Our stimulationprotocol includes (a) up to 3 extrastimuli delivered duringRV apical and outflow tract (OT) pacing, at drive cyclelengths of 600 and 400 milliseconds, and (b) rapid pacing atfixed cycle lengths (400, 353, 316, and 286 ms) at the RVapex and OT. The effective refractory period (ERP) at the RVapex and OT and conduction time between OT and apexwere measured during pacing at a cycle length of 400 milli-seconds. The HV interval was measured during sinusrhythm. If ventricular fibrillation (VF) was induced duringPES, the mean F-F interval, during consecutive 3-secondintervals after the initiation of VF, was calculated. Theinducibility of VF was reexamined after the administration ofverapamil, using the same number of ventricular extrastimulithat were delivered at baseline.

369M. Chinushi et al. / Journal of Electrocardiology 42 (2009) 367–373
Statistical analysis
The surface ECG and endocardial measurements weremade before and after the intravenous administration ofverapamil and compared. Values are presented as means ±SD. Statistical comparisons were made by Student t test andFisher exact test. P values of less than .05 were consideredstatistically significant.
Results
All 10 patients in this study were diagnosed to have BS.This was because (1) we observed type 1 repolarizationabnormalities on surface ECG at baseline and/or after theadministration of pilsicainide and (2) VF was inducible byPES at baseline.1 No significant stenosis of a majorcoronary artery was observed at baseline, whereas theintracoronary administration of ergonovine provoked coro-nary vasospasm of the left and right coronary arteries inpatient no. 3 and of the right coronary artery in patients no.2 and no. 9 (Table 1). In the 3 patients with vasopasticangina, anginal attacks were suppressed after the treatmentwith isosorbide mononitrate in patient no. 2 and with Ca2+
channel blockers in patients no. 3 and no. 9. Although theST-segment elevation was not augmented by the treatment,patient no. 9 (presence of the family history and SCN5Amutation) had VF episodes, and these were terminated byan implantable cardioverter defibrillator.
Surface ECG observations
During EPS, the ECG before verapamil showed type 1repolarization abnormalities in 3 patients. The intracoronaryadministration of verapamil decreased the mean systemicblood pressure from 146 ± 15/82 ± 8 mm Hg to 134 ± 13/74 ± 7 mm Hg (P b .001), whereas the heart rate was 75 ±9 beats per minute before and 74 ± 9 beats per minute afterverapamil (not significant). The PQ interval, QRS duration,and corrected QT interval were similar before and afteradministration of verapamil (Table 2). Likewise, the degreeof ST-segment elevation in leads V1 and V2 did not change
Table 2Surface and intracardiac ECG measurements
Patient no. Verapamil(mg)
HR(bpm)
Intervals (ms)
PQ QRS QTc HV
1 5 74 (72) 140 (155) 90 (90) 400 (383) 50 (50)2 10 62 (64) 110 (100) 90 (100) 396 (403) 30 (30)3 10 68 (68) 140 (140) 100 (120) 426 (404) 45 (45)4 5 95 (95) 175 (170) 100 (100) 416 (415) 35 (35)5 7.5 68 (73) 150 (150) 80 (80) 426 (418) 40 (40)6 7.5 81 (81) 190 (260) 90 (90) 395 (407) 45 (45)7 10 77 (65) 120 (140) 60 (100) 385 (375) 30 (40)8 10 80 (80) 160 (160) 120 (120) 460 (416) 45 (45)9 5 75 (70) 320 (350) 100 (100) 414 (410) 45 (45)10 5 70 (70) 140 (140) 70 (70) 398 (410) 40 (45)Mean ± SD 7.5 ± 2.4 75 ± 9
(74 ± 9)165 ± 60(177 ± 73)
90 ± 17(97 ± 16)
412 ± 22(404 ± 14)
41 ± 7(42 ± 6)
P .427 .146 .132 .201 .193
Values in parentheses indicate measurements made after the administration of verapam
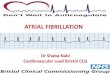
significantly between before and after the administration ofverapamil. Verapamil induced a more than 1-mV increasein ST-segment elevation in patients no. 3 and no. 4. Itchanged the ECG morphology from type 2 to type 1 inpatient no. 4 (Fig. 1), whereas in 9 patients, the ECGpattern remained unchanged.
Intracardiac ECG measurements and inducibility of VF
The HV interval duration was normal before and after theadministration of verapamil in all patients, whereas theconduction time between RV apex and OT lengthenedslightly from 42 ± 17 milliseconds to 47 ± 16 milliseconds(P = .049; Table 2). The effects exerted by verapamil on theERP were significant neither at the RVOT nor at the apex(Table 2).
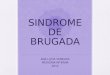
At baseline, PES induced VF in all patients (Table 3;Fig. 2), promptly terminated by a single 200-J, anteropos-terior, monophasic, transthoracic direct current (DC) shock.After the administration of verapamil and more than20 minutes after the delivery of DC shock, PES was resumed,after returning a stable hemodynamic state and confirming nomarked ST-segment augmentation compared with baseline.Ventricular fibrillation was reinduced in 7 of the 10 patients,whereas it was not reinduced with the same number ofventricular extrastimuli in 2 patients. In patient no. 5, VF wasreinduced, though ended spontaneously within 3 seconds.Compared with baseline, the F-F cycles during VF inducedafter the administration of verapamil were significantlyshorter at 0 to 3, 3 to 6, 6 to 9, and 9 to 12 seconds(Table 3; Fig. 2). Furthermore, in patients no. 3 and no. 9, thesame 200-J shock failed to terminate the VF induced, and anadditional 360-J shock was delivered to restore sinus rhythm.One of the patients has been described in a previous report.11
Discussion
ST-segment elevation
In a recent experimental study of BS, verapamil enhancedthe elevation of the ST segment and facilitated the initiation
ST elevation (mV) ERP (ms) Conduction time(ms)
V1 V2 OT Apex OT-apex
0.20 (0.25) 0.20 (0.20) 200 (190) 180 (180) 31 (34)0.20 (0.20) 0.30 (0.30) 200 (200) 210 (180) 25 (25)0.10 (0.15) 0.15 (0.25) 190 (190) 220 (200) 30 (30)0.10 (0.15) 0.20 (0.30) 190 (180) 180 (180) 75 (75)0.10 (0.10) 0.20 (0.25) 210 (220) 220 (220) 65 (65)0.05 (0.05) 0.20 (0.20) 190 (190) 180 (190) 36 (46)0.10 (0.10) 0.20 (0.20) 190 (200) 220 (220) 30 (45)0.15 (0.15) 0.35 (0.35) 210 (210) 220 (220) 48 (50)0.10 (0.10) 0.25 (0.25) 200 (200) 210 (210) 40 (52)0.10 (0.10) 0.20 (0.20) 210 (210) 200 (210) 40 (40)0.12 ± 0.05(0.14 ± 0.06)
0.23 ± 0.06(0.25 ± 0.05)
199 ± 9(199 ± 12)
204 ± 18(201 ± 17)
42 ± 17(47 ± 16)
.081 .096 1 .468 .049
il. HR indicates heart rate; bpm, beats per minute; QTc, corrected QT interval
.
Fig. 1. Twelve-lead ECG. Twelve-lead ECG of representative cases with increase in ST-segment elevation (cases 3 and 4) and without (case 7). A, BaselineECGs. B, After the administration of verapamil.
370 M. Chinushi et al. / Journal of Electrocardiology 42 (2009) 367–373
of VF.12 In this study, the magnitude of ST-segmentelevation in lead V1 and V2 remained unchanged afterverapamil, and a more than 1.0-mV increase was observed inonly 2 patients. The RV ERP did not shorten after verapamil,suggesting that the phase 2 dome of the action potential inthe right ventricle was preserved. However, the actionpotential duration in the epicardial layer could not beestimated by means of PES at the RV endocardium.
Several factors may explain the absence of effectsexerted by verapamil on ST-segment elevation in this study.
Table 3Inducibility of VF and measurements of F-F interval
Patient no VF induction Time after induction of ventricular fibrillati
0-3 3-6
F-F intervals (ms)
1 + (+) 176 (150)⁎ 167 (150)⁎
2 + (+) 167 (167)⁎ 167 (150)⁎
3 + (+) 188 (176)⁎ 167 (142)⁎
4 + (+) 176 (158)⁎ 167 (142)⁎
5 + (self-terminated) 176 (NA) 167 (NA)6 + (−) 176 (NA) 150 (NA)7 + (+) 167 (158)⁎ 167 (142)⁎
8 + (+) 188 (176)⁎ 188 (158)⁎
9 + (+) 214 (200)⁎ 188 (188)⁎
10 + (−) 170 (NA) 176 (NA)Mean ± SD⁎ 182 ± 16 (169 ± 17) 173 ± 10 (153 ± 16P .005 (n = 7) .002 (n = 7)
Values in parentheses indicate observations made after the administration of verap
First, unlike in the experimental study, we used a small,though clinically relevant, dose of verapamil.12 Largeramounts of verapamil might have more prominent effectson ST-segment elevation, although it is also possible thatthe associated decrease in systemic blood pressure wouldenhance sympathetic activity and counteract the cardiacelectrical instability of BS during the EPS. Second, beforethe administration of verapamil, type 1 ECG abnormalitieswere present in the 3 patients. Indeed, in this study, 7 of the10 patients showed day-to-day variability of the repolariza-
on (s)
6-9 9-12 12-15
158 (142)⁎ 158 (NA) NA (NA)167 (NA) 150 (NA) 142 (NA)150 (136)⁎ 150 (136)⁎ 167 (120)⁎
167 (125)⁎ 158 (NA) NA (NA)167 (NA) 176 (NA) NA (NA)142 (NA) 142 (NA) 142 (NA)158 (136)⁎ NA (NA) NA (NA)176 (150)⁎ 158 (142)⁎ 158 (142)⁎
188 (176)⁎ 176 (158)⁎ NA (NA)167 (NA) 158 (NA) 158 (NA)
) 166 ± 14 (144 ± 18) 161 ± 13 (145 ± 11) 163 ± 6 (131 ± 16).005 (n = 6) .005 (n = 3) – (n = 2)
amil. + indicates VF induced; −, VF not induced; NA, not applicable.

Fig. 2. Electrophysiologic study. Electrocardiogram tracing obtained during VF in the same cases of Fig. 1, before (A) and after (B) verapamil administration
371M. Chinushi et al. / Journal of Electrocardiology 42 (2009) 367–373
tion abnormality on ECG, and none of the patients had anepisode of VF or aborted sudden cardiac death. This mightsuggest a less arrhythmogenic potential in our patients'population. Furthermore, because we performed EPS in thenonsedated state, the enhanced sympathetic nervousactivity associated with EPS might have attenuated thebaseline arrhythmogenic state and resulted in a lessprominent proarrhythmic effect of verapamil. Third, arecent study has reported that loss-of-function mutations inthe cardiac Ca2+ channel were associated with the clinicalcharacteristics of BS.13 Therefore, the effects of Ca2+
channel blockade on ST-segment elevation may varyamong patients, depending on the genetic determinants ofthe syndrome.
Characteristics of ventricular fibrillation
The explanation for the unexpected development of fasterVF after administration of verapamil is unclear and may beunrelated to the administration of verapamil becauseverapamil has no or little effects on the conduction propertiesor refractoriness of the normal ventricular myocardium atphysiologic heart rates.14 However, because the electro-physiologic properties of verapamil are use-dependent, theintraventricular conduction delays that probably occurred
.
during very rapid ventricular activation might have shor-tened the activation wavelength and contributed to thedevelopment of faster VF. Indeed, the conduction timebetween RVOT and apex was mildly prolonged afterverapamil, although we used a relatively long pacing cyclelength of 400 milliseconds in our evaluation of intraven-tricular conduction. Furthermore, we have recently reportedthat, in BS, VF is usually characterized by shorter F-Fintervals than in other patient populations.15 Therefore, inthese patients, the electrophysiologic effects of Ca2+ channelblockers may be more marked than in patients with othertypes of heart disease. On the other hand, as a beneficialeffect of verapamil to VF, the conversion of VF tomonomorphic ventricular tachycardia, in presence ofverapamil, has been observed in experimental studies.16,17
Likewise, verapamil showed beneficial effect in 3 patients inthis study (VF became noninducible in 2 patients andbecame self-terminated in other 1 patient). The reasons of thevarious effects of verapamil in this study is unclear, butverapamil might work as either a proarrhythmic or antiar-rhythmic agent depending on the degree of slow conductionwithin certain arrhythmogenic areas in the ventricles.
Myocardial injury caused by the first defibrillationshock might be another explanation for the subsequentinduction of a faster VF in some patients. However, this

372 M. Chinushi et al. / Journal of Electrocardiology 42 (2009) 367–373
seems unlikely because the second VF induction wasattempted at more than 20 minutes after the first DC shock,when hemodynamic stability had returned. In 10 patientswith BS in our institution, no statistical difference wasfound in the F-F interval between the first and second VFs,which were induced at 15 to 20-minute intervals duringdefibrillation testing of the implantable cardioverter defi-brillator (184 ± 15 ms at 0-3 seconds, 174 ± 13 ms at 3-6 seconds, and 167 ± 12 ms at 6-9 seconds in the firstVF vs 183 ± 11 ms at 0-3 seconds, 179 ± 14 ms at 3-6seconds, and 169 ± 14 ms at 6-9 seconds in the second VF)(M. Chinushi, et al. October 2008; unpublished data).Furthermore, statistical analysis revealed that F-F intervalof VF induced after administration of verapamil was shortercomparing to the F-F interval in the second induced VF atthe defibrillation testing. This result may support ourobservation that verapamil could shorten F-F interval of VFin some patients of BS.
A slight difference in the timing of the DC shocksdelivered after the first vs second VF induction could havecaused the unsuccessful defibrillation of the second episodeby the 200-J shock in 2 patients, though this seemsunlikely. It is noteworthy that, during the second episode,the acceleration of the rhythm and shorter F-F intervalsbecame apparent within 6 to 9 seconds after the onset ofVF (Table 3). The coexistence of coronary vasospasmmight be related to the development of faster VF andrequiring a higher energy shock. This seems improbablebecause, before starting EPS, all patients received intraco-ronary isosorbide dinitrate, and the absence of coronaryvasospasm was verified. Furthermore, Ca2+ channel block-ade effectively prevents the development of coronaryvasospasm. Further studies with larger and homogeneouspatients' population as the study subjects will be requiredto clarify the opaque results of the verapamil-related changein the F-F interval of VF in this study.
Clinical implications
Our results suggested that small doses of verapamil (5-10 mg) may not exert severe proarrhythmic effects inpatients with BS. Therefore, small doses of verapamil mayhave clinical benefits in certain circumstances in patientswith BS such as atrial fibrillation where the rate control isimmediately required.
Limitations of the study
This study has 5 main limitations. First, it included asmall number of patients of heterogeneous clinical back-ground. Unlike in other studies, the patients had nohistories of VF. All patients in this study were fromdifferent families, and a family history of sudden cardiacdeath was present in 2 patients. Indeed, in contrast to NorthAmerica or Europe, most cases of BS in Japan are sporadic,and asymptomatic patients have a relatively benignprognosis.18-21 A small incidence of adverse cardiac eventsin asymptomatic patients and in patients with histories ofsyncope has also been observed in a recent Europeanstudy.22 These clinical characteristics and the little effects
exerted by verapamil on the ST segment might be linked.Second, although we only examined the effects ofverapamil administered intravenously, other types of Ca2+
channel blockers, or their long-term oral administration,may have different effects on the arrhythmogenic char-acteristics of BS. Furthermore, we evaluated the effects ofverapamil on ECG 15 to 20 minutes after intravenousadministration, but this timing might have been inappropri-ate. A previous study reported that verapamil showedsignificant effects on ECG within a short period afterintravenous administration (b15 minutes).23 Third, in agiven patient, the energy required to defibrillate may varyamong induced episodes of VF.24 Because we were unableto measure the “defibrillation threshold” during EPS,whether the higher energy required in 2 patients was dueto the shorter F-F interval after verapamil is uncertain,particularly because, in the other 5 patients, the same 200-Jshock successfully terminated the second episode of VFdespite shorter F-F intervals. Fourth, it is still a matter ofcontroversy as to the clinical significance of VF inducibilityby PES25 and the correlation between induced VF andspontaneous VF episodes in BS. Therefore, we should becareful about clinical relevance of the results in this study.Finally, a larger patient population with similar clinical andgenetic profiles and longer-term follow-ups will be neededto understand more precisely the consequences of admin-istering intravenous verapamil in patients with BS.
Conclusions
Small doses of verapamil had no apparent effect on the STsegment in most patients included in this study. Although itmight have adversely modified the characteristics of VF,small doses of verapamil may be used in certain circum-stances in patients with BS under careful monitoring.However, caregivers should be aware of the possibledevelopment of faster VF, of an increase in the defibrillationenergy requirements, after the administration of a Ca2+
antagonist in patients with BS.
References
1. Antzelevitch C, Brugada P, BorggrefeM, et al. Brugada syndrome. Reportof the second consensus conference. Endorsed by the Heart RhythmSociety and the European Heart Rhythm Association. Circulation 2005;111:659.
2. Antzelevitch C. Brugada syndrome. Pacing Clin Electrophysiol 2006;29:1130.
3. Maury P, Couderc P, Delay M, Boveda S, Brugada J. Electrical storm inBrugada syndrome successfully treated using isoprenaline. Europace2004;6:130.
4. Ohgo T, Okamura H, Noda T, et al. Acute and chronic management inpatients with Brugada syndrome associated with electrical storm ofventricular fibrillation. Heart Rhythm 2007;4:695.
5. Chinushi M, Furushima H, Tanabe Y, Washizuka T, Aizawaz Y.Similarities between Brugada syndrome and ischemia-induced ST-segment elevation. Clinical correlation and synergy. J Electrocardiol2005;38:18.
6. Bigi MA, Aslani A, Shahrzad S. Clinical predictors of atrial fibrillationin Brugada syndrome. Europace 2007;9:947.
7. Hong K, Brugada J, Oliva A, et al. Value of electrocardiographicparameters and ajmaline test in the diagnosis of Brugada syndromecaused by SCN5A mutations. Circulation 2004;110:3023.

373M. Chinushi et al. / Journal of Electrocardiology 42 (2009) 367–373
8. Chinushi M, Komura S, Izumi D, et al. Incidence and initialcharacteristics of pilsicainide-induced ventricular arrhythmias inpatients with Brugada syndrome. Pacing Clin Electrophysiol 2007;30:662.
9. Wilde AAM, Antzelevitch C, Borggrefe M, et al, for the study group onthe molecular basis of arrhythmia of the European Society ofCardiology. Proposed Diagnostic Criteria for the Brugada syndrome.Consensus report. Circulation 2002;106:2514.
10. Noda T, Shimizu W, Taguchi A, et al. ST-segment elevation andventricular fibrillation without coronary spasm by intracoronaryinjection of acetylcholine and/or ergonovine maleate in patients withBrugada syndrome. J Am Coll Cardiol 2002;40:1841.
11. Chinushi M, Tagawa M, Nakamura Y, Aizawa Y. Shortening of theventricular fibrillatory intervals after administration of verapamil in apatient with Brugada Syndrome and vasospastic angina. J Electro-cardiology 2006;39:331.
12. Fish JM, Antzelevitch C. Role of sodium and calcium channel block inunmasking the Brugada syndrome. Heart Rhythm 2004;1:210.
13. Antzelevitch C, Pollevick GD, Cordeiro JM, et al. Loss-of-functionmutations in the cardiac calcium channel underlie a new clinical entitycharacterized by ST-segment elevation, short QT intervals, and suddencardiac death. Circulation 2007;115:442.
14. Lee KS, Tsien RW. Mechanism of calcium channel blockade byverapamil, D600, diltiazem and nitrendipine in single dialysed heartcell. Nature 1983;302:790.
15. Watanabe H, Chinushi M, Sugiura H, et al. Unsuccessful internaldefibrillation in Brugada syndrome. Focus on refractoriness andventricular fibrillation cycle length. J Cardiovasc Electrophysiol 2005;16:262.
16. Samie FH, Mandapati R, Gray RA, et al. A mechanism of transitionfrom ventricular fibrillation to tachycardia. Effect of calcium channelblockade on the dynamics of rotating waves. Circ Res 2000;86:684.
17. Kawahara K, Takase M, Yamauchi Y, Kimura H. Spectral andcorrelation analyses of the verapamil-induced conversion of ventricularfibrillation to tachycardia in isolated rat hearts. J Electrocardiol 2004;37:89.
18. Takenaka S, Kusano KF, Hisamatsu K, et al. Relatively benign clinicalcourse in asymptomatic patients with Brugada type electrogram withoutfamily history of sudden cardiac death. J Cardiovasc Electrophysiol2001;12:2.
19. Atarashi H, Ogawa S, Harumi K, et al. Idiopathic ventricular fibrillationinvestigators. Three-year follow-up of patients with right bundle branchblock and ST segment elevation in the right precordial leads: JapaneseRegistry of Brugada syndrome. Idiopathic Ventricular FibrillationInvestigators. J Am Coll Cardiol 2001;37:1916.
20. Priori SG, Napolitano C, Gasparini M, et al. Natural history of Brugadasyndrome: insights for the risk stratification and management.Circulation 2002;105:1342.
21. Brugada J, Brugada R, Antzelevitch C, Towbin J, Nademanee K,Brugada P. Long-term follow-up of individuals with the electrophysio-logic pattern of right bundle-branch block and ST-segment elevation inprecordial leads V1 to V3. Circulation 2002;5:73.
22. Eckardt L, Probst V, Smits JP, et al. Long-term prognosis of individualswith right precordial ST-segment elevation Brugada syndrome.Circulation 2005;111:257.
23. Dilger K, Eckhardt K, Hofmann U, Kucher K, Mikus G, EichelbaumM.Chronopharmacology of intravenous and oral modified releaseverapamil. Br J Clin Pharmacol 1999;47:413.
24. Ruffy R, Schechtman K, Monje E, Sandza J. Adrenergically mediatedvariation in the energy required to defibrillate the heart: observations inclosed-chest, nonanesthetized dogs. Circulation 1986;73:374.
25. Paul M, Gerss J, Schulze-Bahr E, et al. Role of programmed ventricularstimulation in patients with Brugada syndrome: a meta-analysis ofworldwide published data. Eur Heart J 2007;28:2126.