Embed Size (px)
Citation preview

ECZTRA 1 & 2
Efficacy Assessment & C-SSRS Manual
LP0162‐1325 and LP0162‐1326 Efficacy Assement & C‐SSRS Manual, v 1.0, 15‐May‐2017
TMF-000010481 - Version 1.0

LP0162‐1325 and LP0162‐1326 Efficacy Assement & C‐SSRS Manual, v 1.0, 15‐May‐2017
Efficacy Assessments
General instruction
Investigator assessments should be performed after the subject has completed the Patient Reported Outcome (PROs) assessments.
The efficacy assessments should be administered in the following order:
• SCORAD, part C, then part A and B
• IGA
• EASI
Whenever possible, the efficacy assessments should be assessed by the same investigator at each visit to
reduce inter-rater variability.
The assessments will be based on the condition of the disease at the time of evaluation and not in relation
to the condition at a previous visit.
TMF-000010481 - Version 1.0

LP0162‐1325 and LP0162‐1326 Efficacy Assement & C‐SSRS Manual, v 1.0, 15‐May‐2017
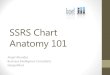
SCORAD
The SCORAD is a validated tool to evaluate the extent and severity of AD lesions, along with subjective
symptoms. The maximum total score is 103, with higher values indicating more severe disease. SCORAD
will be assessed according to the Schedule of Procedures in the protocol (Section 4).
The assessment consists of 3 components: A = extent, B = intensity, and C = subjective symptoms
The subject must evaluate the subjective symptoms (C) prior to investigator assessment of A and B.
The scores from A, B and C must be entered in a provided spreadsheet and the eCRF where the total
SCORAD score will be generated.
Extent (A)
The extent of AD is assessed as a percentage of each defined body area and reported as the sum of all
areas (maximum score = 100%)
Intensity (B)
The intensity of 6 specific symptoms of AD (erythema, edema/papulation, oozing/crusting, excoriation,
lichenification, and dryness) is assessed by the investigator on an average representative area using the
following scale:
0 = None/absent
1 = Mild
2 = Moderate
3 = Severe
Note: dryness is evaluated on uninvolved areas.
The sum of intensity score of the 6 symptoms will be reported (maximum score = 18).
Subjective symptoms (C)
A visual analogue scale for itch and sleep loss. The subject should be instructed to assess and mark the
average itch over the last 3 days on the visual analogue scale, where 0 is no itch and 10 is the worst
imaginable itch. Likewise the subject should be instructed to assess and mark the average sleep loss over
the last 3 nights, where 0 is no sleep loss and 10 is the worst imaginable sleep loss.
The combined score for the subjective symptoms with a maximum possible score of 20 will be reported
(maximum one decimal).
TMF-000010481 - Version 1.0
Date
Subject ID
Site ID
Visit Type
English Master SCORAD
Visual analog scale (average for the last 3 days or nights)
PRURITUS (0 to 10)
0 10
SLEEP LOSS (0 to 10) 0 10
LP0162-1325 and LP0162-1326
SCORAD, v 1.0, 27-Apr-2017 TMF-000010481 - Version 1.0

IGA
The IGA is an instrument used in clinical trials to rate the severity of the subject’s global AD and is based
on a 5-point scale. The IGA score will be assessed according to the Schedule of Procedures in the protocol
(Section 4).
Score Disease severity
Standard IGA scale IGA morphological descriptors
0
Clear
No inflammatory signs of atopic dermatitis
No erythema and no elevation
(papulation/infiltration).
1
Almost clear
Just perceptible erythema, and just perceptible papulation/infiltration
Barely perceptible erythema
and/or minimal lesion elevation
(papulation/infiltration) that is
not widespread.
2
Mild disease
Mild erythema and mild papulation/infiltration
Visibly detectable, light pink
erythema and very slight
elevation
(papulation/infiltration).
3
Moderate disease
Moderate erythema and moderate papulation/infiltration
Dull red, clearly distinguishable
erythema and clearly perceptible
but not extensive elevation
(papulation/infiltration).
4
Severe disease
Severe erythema and severe papulation/infiltration
Deep/dark red erythema,
marked and extensive elevation
(papulation/infiltration).
LP0162‐1325 and LP0162‐1326 Efficacy Assement & C‐SSRS Manual, v 1.0, 15‐May‐2017
TMF-000010481 - Version 1.0
EASI
The EASI is a validated measure used to assess the severity and extent of AD. The EASI is a composite
index with scores ranging from 0-72, with higher values indicating more severe and/or more extensive
condition.
The severity of 4 AD disease characteristics (erythema, induration/papulation, excoriation and
lichenification) on the 4 body regions (head/neck, trunk, upper extremities, lower extremities) will be
assessed. The severity assessed according to the severity score scale of 0-3 (half points may be used). The
affected area in each body region will be assessed according to the area score scale of 0-6. The scores for
severity and area will be entered in the scoring table.
For each body region a score will be calculated based on the severity sum score, area score and a
weighting factor. The calculation will be done in the eCRF.
EASI will be assessed according to the Schedule of Procedures in the protocol (Section 4).
At baseline and screening the EASI-score is needed for assessment of inclusion criteria 7. When the EASI
score is needed immediately, the provided spread sheet (EASI-calculator) should be used for calculation of
the EASI-score.
At week 16 and throughout maintenance treatment period, %-reduction from baseline is used to determine if
the subject is eligible for maintenance treatment or should be transferred to open-label treatment. Please
refer to section 7.1 of the protocol for criteria for transfer to open-label treatment. The provided spreadsheet
(EASI-calculator) should be used to calculate the %-reduction from baseline of EASI-score.
LP0162‐1325 and LP0162‐1326 Efficacy Assement & C‐SSRS Manual, v 1.0, 15‐May‐2017
TMF-000010481 - Version 1.0

Modified from EASI guidance December 14
0 None
1 Mild
2 Moderate
3 Severe
How to Use EASI The EASI scoring system uses a defined process to grade the severity of the signs of eczema and the
extent affected:
1. Select a body region
Four body regions are considered separately:
• Head and neck
• Trunk (including the genital area)
• Upper extremities
• Lower Extremities (including the buttocks)
2. Assess the extent of eczema in that body region
Each body region has potentially 100% involvement. Using the table below, give each respective body region a score of between 0 and 6 based on the percentage involvement. Precise measurements are not required.
% involvement 0 1‐9% 10 ‐ 29% 30 ‐ 49% 50 ‐ 69% 70 ‐ 89% 90 ‐ 100%
Region score 0 1 2 3 4 5 6
To aid in your body region grading you can use the diagrams in Appendix 1.
3. Assess the severity of each of the four signs in that body region:
1. Erythema
2. Edema/papulation
3. Excoriation
4. Lichenification
Further explanations of these terms can be found in FAQ’s
(Appendix 4)
Grade the severity of each sign on a scale of 0 to 3: Take an average of the severity across the
involved region.
Half points may be used.
Palpation may be useful in assessing edema/papulation as well as lichenification
To aid your severity grading, a photographic atlas of suggested categories is available in Appendix 2
.
Remember: Include only inflamed areas in your assessment; do not include xerosis (dryness), ichthyosis, keratosis pilaris, urticaria, infection (unless there is underlying eczema), or post inflammatory pigmentation changes.
TMF-000010481 - Version 1.0

Modified from EASI guidance December 14
Appendix 1: Eczema Area and Severity Index (EASI) ‐ Extent of eczema per body region
Score each region from 0 to 100%
Head & neck Upper extremities
Trunk Lower extremities
TMF-000010481 - Version 1.0

Modified from EASI guidance December 14
Appendix 2: Eczema Area and Severity Index (EASI) -lesion severity atlas
None = 0 Mild = l
Faintly detectable,pink Moderate = 2 Severe = 3
Clearly distinguishable dull red Deep dark or fiery bright red
Edema/Papulation
None = 0 Mild = l
Barely perceptible elevation
Moderate = 2 Clearly perceptible elevation
but not prominent
Severe = 3 Prominent elevation
Excoriation
None = 0 Mild =l Scant, superficial
excoriations
.. Moderate = 2 Severe = 3
Many superficial and/or some Diffuse extensive superficial deeper excoriations and/or many deep excoriations
lichenification
None = 0 Mild =l Slightthickeni ng of the skin with
skin markings minimalty
exaggerated
Moderate = 2 Clea rly thickened skin with
exaggerated skin markings
and/or some
prurigo nodules
Severe = 3 Prominent skin
thickeningwith exaggerated
skin markings creatingdeep
furrows and/or many
prurigo nodules
TMF-000010481 - Version 1.0

0 None
1 Mild
2 Moderate
3 Severe
Appendix 3.1: Eczema Area and Severity Index (EASI) case report form
Area of Involvement: Each body region has potentially 100% involvement. Score 0 to 6 based on the following table:
% involvement 0 1‐9% 10 ‐ 29% 30 ‐ 49% 50 ‐ 69% 70 ‐ 89% 90 ‐ 100%
Region score 0 1 2 3 4 5 6
Severity of Signs: Grade the severity of each sign on a scale of 0 to 3:
Take an average of the severity across the involved area.
Half points may be used.
Scoring table:
Body region
Erythema
(0‐3)
Edema/
Papulation
(0‐3)
Excoriation
(0‐3)
Lichenification
(0‐3)
Region score
(0‐6)
Multiplier
Head/neck ( + + + ) X X 0.1
Trunk ( + + + ) X X 0.3
Upper extremities ( + + + ) X X 0.2
Lower extremities ( + + + ) X X 0.4
Modified from EASI guidance December 14 TMF-000010481 - Version 1.0
Modified from EASI guidance December 14
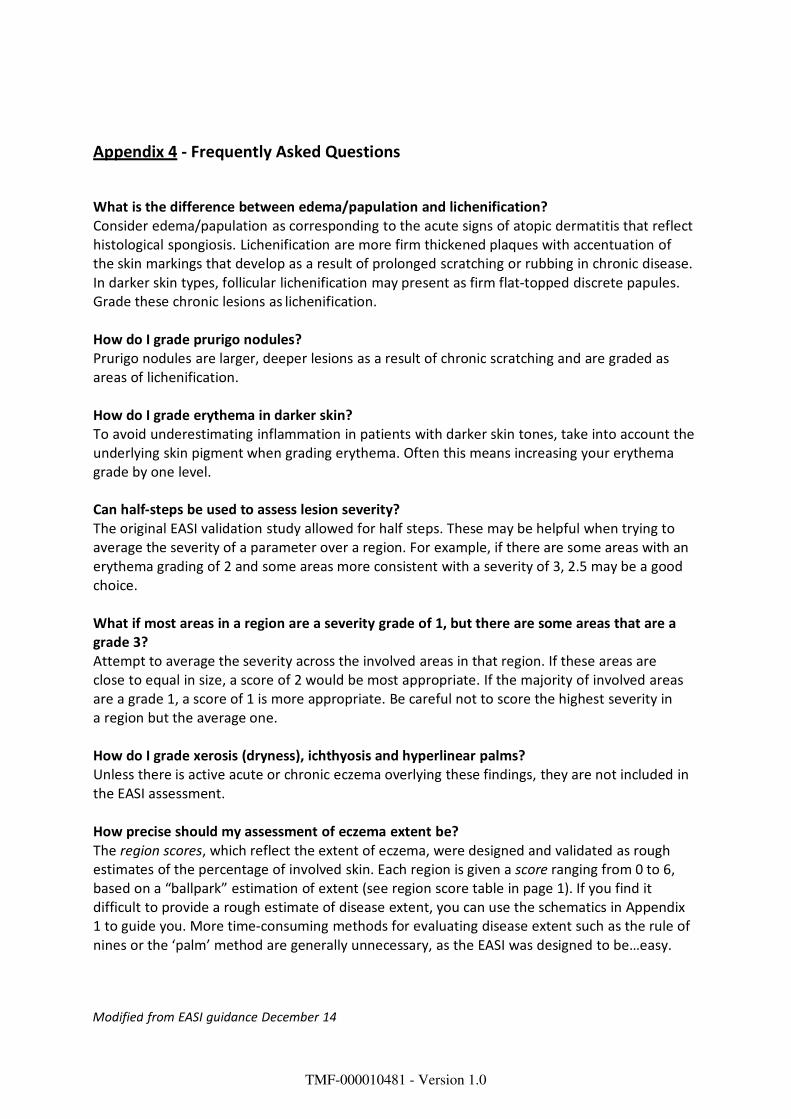
Appendix 4 ‐ Frequently Asked Questions
What is the difference between edema/papulation and lichenification? Consider edema/papulation as corresponding to the acute signs of atopic dermatitis that reflect histological spongiosis. Lichenification are more firm thickened plaques with accentuation of the skin markings that develop as a result of prolonged scratching or rubbing in chronic disease. In darker skin types, follicular lichenification may present as firm flat‐topped discrete papules. Grade these chronic lesions as lichenification.
How do I grade prurigo nodules? Prurigo nodules are larger, deeper lesions as a result of chronic scratching and are graded as areas of lichenification.
How do I grade erythema in darker skin? To avoid underestimating inflammation in patients with darker skin tones, take into account the underlying skin pigment when grading erythema. Often this means increasing your erythema grade by one level.
Can half‐steps be used to assess lesion severity? The original EASI validation study allowed for half steps. These may be helpful when trying to average the severity of a parameter over a region. For example, if there are some areas with an erythema grading of 2 and some areas more consistent with a severity of 3, 2.5 may be a good choice.
What if most areas in a region are a severity grade of 1, but there are some areas that are a grade 3? Attempt to average the severity across the involved areas in that region. If these areas are close to equal in size, a score of 2 would be most appropriate. If the majority of involved areas are a grade 1, a score of 1 is more appropriate. Be careful not to score the highest severity in a region but the average one.
How do I grade xerosis (dryness), ichthyosis and hyperlinear palms? Unless there is active acute or chronic eczema overlying these findings, they are not included in the EASI assessment.
How precise should my assessment of eczema extent be? The region scores, which reflect the extent of eczema, were designed and validated as rough estimates of the percentage of involved skin. Each region is given a score ranging from 0 to 6, based on a “ballpark” estimation of extent (see region score table in page 1). If you find it difficult to provide a rough estimate of disease extent, you can use the schematics in Appendix 1 to guide you. More time‐consuming methods for evaluating disease extent such as the rule of nines or the ‘palm’ method are generally unnecessary, as the EASI was designed to be…easy.
TMF-000010481 - Version 1.0

Modified from EASI guidance December 14
My patient has responded well to treatment and significantly improved since the last visit. Should I adjust the grading based on the patient’s relative improvement? No. The EASI is a static score, meaning that it is done independently at each time point to reflect current severity. You should grade the EASI per visit regardless of the previous status. Studies have shown that the EASI score has good responsiveness, meaning that overall it is sensitive to change and the improvement will be reflected in the total score.
What do the terms erythema, edema/papulation, excoriation and lichenification mean? These are key signs of atopic dermatitis. Recognizing and grading them properly requires training on the visual and physical exam consistent with these signs. Generally speaking, erythema is skin redness; edema/papulation refers to an elevation or swelling of the skin (that should be differed from lichenification below); excoriations are scratch marks that have broken the skin surface; and lichenification is a leathery thickening of the skin with exaggerated skin markings.
TMF-000010481 - Version 1.0
LP0162‐1325 and LP0162‐1326 Efficacy Assement & C‐SSRS Manual, v 1.0, 15‐May‐2017
Columbia-Suicide Severity Rating Scale (C-SSRS) The C-SSRS Screening version is a rater-administered instrument used to identify whether someone
is at risk for suicide and assess the severity of suicidal ideation and suicidal behaviour through a
series of simple, plain-language questions. Raters administering the Columbia-Suicide Severity Rating Scale (C-SSRS) are not required to
have a background in clinical psychology, nursing, psychiatry, or similar fields.
C-SSRS will only be performed at the screening visit. The C-SSRS must be completed at
screening to ensure that exclusion criterion no. 24 does not apply. The C-SSRS Screening version consists of two sections, suicidal ideation and suicidal behaviour. The section on suicidal ideation is a 1-5 rating for suicidal ideation (from a wish to die to an active
thought of killing oneself with plan and intent). It should be assessed over the past 36 months. If the
subject answers ‘No’ to questions 1 and 2, no more questions on ideation is needed. As the C-SSRS
Screening version is used for screening purposes, the ‘intensity of ideation’ section is not required. The section on suicidal behavior is a series of questions concerning suicidal attempts. The questions in
this section should be assessed for the lifetime of the subject. As the C-SSRS Screening version is
used for screening purposes, the ‘Answer for Actual Attempts Only’ section is not required. Raters administering the Columbia-Suicide Severity Rating Scale (C-SSRS) are not required to
have a background in clinical psychology, nursing, psychiatry, or similar fields. Training in the administration of the scale must be completed including an available certificate of
completion prior to rating subjects in the trial. The training will consist of watching a 30-minute
instructional video and completing an optional 8-question self-assessment. The online training is
available on the following web-site: http://cssrs.columbia.edu/training/training-research-setting/
TMF-000010481 - Version 1.0

Date_____________________________________ SiteID__________________________________
SubjectID______________________________ VisitType______________________________
COLUMBIA-SUICIDE SEVERITY
RATING SCALE
(C-SSRS)
Screening
Version 14/01/2009
Posner, K.; Brent, D.; Lucas, C.; Gould, M.; Stanley, B.; Brown, G.; Fisher, P.; Zelazny, J.; Burke, A.; Oquendo, M.; Mann, J.
Disclaimer:
This scale is intended to be used by individuals who have received training in its administration. The questions contained in the Columbia-Suicide Severity Rating Scale (C-SSRS) are suggested probes. Ultimately, the determination of the presence of
suicidal ideation or behaviour depends on the judgment of the individual administering the scale.
Definitions of behavioural suicidal events in this scale are based on those used in The Columbia Suicide History Form, developed by John Mann, MD and Maria Oquendo, MD, Conte Center for the Neuroscience of Mental Disorders (CCNMD), New York State Psychiatric Institute, 1051 Riverside Drive, New York, NY, 10032. (Oquendo M. A., Halberstam B. & Mann J. J., Risk factors for suicidal behavior: utility and limitations of research instruments. In M.B. First [Ed.] Standardized Evaluation in Clinical Practice, pp. 103 -130, 2003.)
For reprints of the C-SSRS contact Kelly Posner, Ph.D., New York State Psychiatric Institute, 1051 Riverside Drive, New York, New York, 10032; enquiries and training requirements contact [email protected]
© 2008 The Research Foundation for Mental Hygiene, Inc.
C-SSRS Screening - United Kingdom/English - Version of 16 Jun 14 - Mapi. ID7947 / C-SSRS-Screening_AU5.1_eng-GB.doc
TMF-000010481 - Version 1.0

© 2008 Research Foundation for Mental Hygiene, Inc. C-SSRS—Screening (Version 14/01/2009) Page 1 of 2
SUICIDAL IDEATION Ask questions 1 and 2. If both are negative, proceed to the "Suicidal Behaviour" section. If the answer to question 2 is "yes", ask questions 3, 4 and 5. If the answer to question 1 and/or 2 is "yes", complete the "Intensity of Ideation" section below.
Past 36 Months
1. Wish to be Dead Subject endorses thoughts about a wish to be dead or not alive any more, or a wish to fall asleep and not wake up. Have you wished you were dead or wished you could go to sleep and not wake up?
If yes, describe:
Yes No
2. Non-Specific Active Suicidal Thoughts General non-specific thoughts of wanting to end one's life / commit suicide (e.g. "I've thought about killing myself") without thoughts of ways to kill oneself / associated methods, intent, or plan. Have you actually had any thoughts of killing yourself?
If yes, describe:
Yes No
3. Active Suicidal Ideation with Any Methods (Not Plan) without Intent to Act Subject endorses thoughts of suicide and has thought of at least one method during the assessment period. This is different from a specific plan with time, place or method details worked out (e.g. thought of method to kill self but not a specific plan). Includes person who would say, "I thought about taking an overdose but I never made a specific plan as to when, where or how I would actually do it… and I would never go through with it". Have you been thinking about how you might do this?
If yes, describe:
Yes No
4. Active Suicidal Ideation with Some Intent to Act, Without Specific Plan Active suicidal thoughts of killing oneself and subject reports having some intent to act on such thoughts, as opposed to "I have the thoughts but I definitely will not do anything about them". Have you had these thoughts and had some intention of acting on them?
If yes, describe:
Yes No
5. Active Suicidal Ideation with Specific Plan and Intent Thoughts of killing oneself with details of plan fully or partially worked out and subject has some intent to carry it out. Have you started to work out or worked out the details of how to kill yourself? Do you intend to carry out this plan?
If yes, describe:
Yes No
INTENSITY OF IDEATION The following features should be rated with respect to the most severe type of ideation (i.e. 1-5 from above, with 1 being the least severe and 5 being the most severe). Ask about time he/she was feeling the most suicidal.
Most Severe Ideation:
Type # (1-5) Description of Ideation
Most
Severe
Frequency How many times have you had these thoughts?
(1) Less than once a week (2) Once a week (3) 2-5 times a week (4) Daily or almost daily (5) Many times each day
Duration When you have the thoughts, how long do they last?
(1) Fleeting - few seconds or minutes (4) 4-8 hours/most of day (2) Less than 1 hour/some of the time (5) More than 8 hours/persistent or continuous (3) 1-4 hours/a lot of time
Controllability Could/can you stop thinking about killing yourself or wanting to die if you want to?
(1) Easily able to control thoughts (4) Can control thoughts with a lot of difficulty (2) Can control thoughts with little difficulty (5) Unable to control thoughts (3) Can control thoughts with some difficulty (0) Does not attempt to control thoughts
Deterrents Are there things - anyone or anything (e.g. family, religion, pain of death) - that stopped you from wanting to die or acting on thoughts of committing suicide?
(1) Deterrents definitely stopped you from attempting suicide (4) Deterrents most likely did not stop you (2) Deterrents probably stopped you (5) Deterrents definitely did not stop you (3) Uncertain that deterrents stopped you (0) Does not apply
Reasons for Ideation What sort of reasons did you have for thinking about wanting to die or killing yourself? Was it to end the pain or stop the way you were feeling (in other words you couldn't go on living with this pain or how you were feeling) or was it to get attention, revenge or a reaction from others? Or both?
(1) Completely to get attention, revenge or a reaction from others (4) Mostly to end or stop the pain (you couldn't go on living (2) Mostly to get attention, revenge or a reaction from others with the pain or how you were feeling) (3) Equally to get attention, revenge or a reaction from others and (5) Completely to end or stop the pain (you couldn't go on
to end/stop the pain living with the pain or how you were feeling) (0) Does not apply
TMF-000010481 - Version 1.0

© 2008 Research Foundation for Mental Hygiene, Inc. C-SSRS—Screening (Version 14/01/2009) Page 2 of 2
SUICIDAL BEHAVIOUR (Tick all that apply, so long as these are separate events; must ask about all types)
Lifetime
Actual Attempt: A potentially self-injurious act committed with at least some wish to die, as a result of act. Behaviour was in part thought of as method to kill oneself. Intent
does not have to be 100%. If there is any intent/desire to die associated with the act, then it can be considered an actual suicide attempt. There does not have to be any injury or harm, just the potential for injury or harm. If person pulls trigger while gun is in mouth but gun is broken so no injury results, this is considered an attempt. Inferring Intent: Even if an individual denies intent/wish to die, it may be inferred clinically from the behaviour or circumstances. For example, a highly lethal act that is clearly not an accident so no other intent but suicide can be inferred (e.g. gunshot to head, jumping from window of a high floor/storey). Also, if someone denies intent to die, but they thought that what they did could be lethal, intent maybe inferred. Have you made a suicide attempt? Have you done anything to harm yourself? Have you done anything dangerous where you could have died?
What did you do? Did you as a way to end your life? Did you want to die (even a little) when you ? Were you trying to end your life when you ? Or did you think it was possible you could have died from_ ?
Or did you do it purely for other reasons / without ANY intention of killing yourself (like to relieve stress, feel better, get sympathy, or get something else to happen)? (Self-Injurious Behaviour without suicidal intent) If yes, describe:
Has subject engaged in Non-Suicidal Self-Injurious Behaviour?
Yes No
Total # of Attempts
Yes No
Interrupted Attempt: When the person is interrupted (by an outside circumstance) from starting the potentially self-injurious act (if not for that, actual attempt would have occurred). Overdose: Person has pills in hand but is stopped from ingesting. Once they ingest any pills, this becomes an attempt rather than an interrupted attempt. Shooting: Person has gun pointed towards self, gun is taken away by someone else, or he/she is somehow prevented from pulling trigger. Once they pull the trigger, even if the gun fails to fire, it is an attempt. Jumping: Person is poised to jump, is grabbed and taken down from ledge. Hanging: Person has noose around neck but has not yet started to hang - is stopped from doing so. Has there been a time when you started to do something to end your life but someone or something stopped you before you actually did anything? If yes, describe:
Yes No
Total # of Interrupted
Aborted Attempt: When person begins to take steps towards making a suicide attempt, but stops themselves before they actually have engaged in any self-destructive behaviour. Examples are similar to interrupted attempts, except that the individual stops him/herself instead of being stopped by something else. Has there been a time when you started to do something to try to end your life but you stopped yourself before you actually did anything? If yes, describe:
Yes No
Total # of Aborted
Preparatory Acts or Behaviour: Acts or preparation towards imminently making a suicide attempt. This can include anything beyond a verbalisation or thought, such as assembling a specific method (e.g. buying pills, purchasing a gun) or preparing for one's death by suicide (e.g. giving things away, writing a suicide note). Have you taken any steps towards making a suicide attempt or preparing to kill yourself (such as collecting pills, getting a gun, giving valuables away or writing a suicide note)? If yes, describe:
Yes No
Suicidal Behaviour:
Suicidal behaviour was present during the assessment period?
Yes No
Answer for Actual Attempts Only Most Recent Attempt Date:
Most Lethal Attempt Date:
Initial/First Attempt Date:
Actual Lethality/Medical Damage: 0. No physical damage or very minor physical damage (e.g. surface scratches). 1. Minor physical damage (e.g. lethargic speech, first degree burns, mild bleeding, sprains). 2. Moderate physical damage; medical attention needed (e.g. conscious but sleepy, somewhat responsive, second degree
burns, bleeding of major vessel). 3. Moderately severe physical damage; medical hospitalisation and likely intensive care required (e.g. comatose with
reflexes intact, third degree burns less than 20% of body, extensive blood loss but can recover, major fractures). 4. Severe physical damage; medical hospitalisation with intensive care required (e.g. comatose without reflexes, third
degree burns over 20% of body, extensive blood loss with unstable vital signs, major damage to a vital area). 5. Death
Enter Code Enter Code Enter Code
Potential Lethality: Only Answer if Actual Lethality = 0 Likely lethality of actual attempt if no medical damage (the following examples, while having no actual medical damage, had potential for very serious lethality: put gun in mouth and pulled the trigger but gun failed to fire so no medical damage; lay on train tracks with oncoming train but pulled away before run over).
0 = Behaviour not likely to result in injury 1 = Behaviour likely to result in injury but not likely to cause death 2 = Behaviour likely to result in death despite available medical care
Enter Code Enter Code Enter Code
TMF-000010481 - Version 1.0