Embed Size (px)
Citation preview
International Journal of Dermatology
2003,
42
, 572–575 © 2003
The International Society of Dermatology
572
Abstract
Background
Betamethasone valerate foam (BVF) is a new topical corticosteroid formulation.
In scalp psoriasis patients BVF has induced a significantly greater clinical improvement in
comparison with corticosteroid lotions. No data are available to date regarding the efficacy and
safety of BVF in mild-to-moderate alopecia areata (AA).
Study aim
To evaluate the efficacy, tolerability and safety of BVF treatment in patients with
mild-to-moderate AA.
Subjects and Methods
Sixty-one patients (26 men and 35 women; mean age 41
±
13 years)
with mild-to-moderate AA (hair loss < 26%) were enrolled in a parallel-group, investigator-
blinded trial. Subjects were assigned randomly to BVF (31 patients) or to betamethasone
dipropionate lotion (BDL) (30 subjects). Both treatments were applied to the affected areas
twice a day for 12 consecutive weeks.
Outcomes
The primary study outcome was to compare the hair regrowth rate. Efficacy was
evaluated at weeks 8 and 12 and at follow up (week 20), using a hair regrowth score (RGS) with
a scale ranging from 0 (regrowth < 10%) to 4 (regrowth > 75%).
Results
Fifty-seven subjects (93%) completed the trial. At week 20, the RGS was 3.1
±
1.5 and
1.8
±
1.6 in the BVF and BDL groups, respectively (
P
< 0.01). A RGS > 3 was observed in 61%
of patients in the BVF group (19/31) in comparison with 27% (8/30) in the BDL group (
P
< 0.03).
No serious adverse events were observed in both groups during the study.
Conclusion
Betamethasone valerate foam has shown to be an effective and well-tolerated
treatment of mild-to-moderate AA. Further trials are warranted to evaluate the role of this new
formulation in comparison or in combination with intralesional corticosterioids in AA treatment.
Blackwell Publishing Ltd.Oxford, UKIJDInternational Journal of Dermatology0011-9059Blackwell Publishing Ltd, 200345
Pharmacology and Therapeutics Clinical trial
Efficacy of betamethasone foam in alopecia areataMancuso et al.PHARMACOLOGY and THER
Efficacy of betamethasone valerate foam formulation in comparison with betamethasone dipropionate lotion in the treatment of mild-to-moderate alopecia areata: A multicenter, prospective, randomized, controlled, investigator-blinded trial
Giuseppe Mancuso,
MD
, Antonella Balducci,
MD
, Chiara Casadio,
MD
, Paolo Farina,
MD
, Mauro Staffa,
MD
, Lorenzo Valenti,
MD
, and Massimo Milani,
MD
From the Dermatologic Services of Lugo di Romagna, of Bagnacavallo, of Alfonsine and of Russi, Ravenna, Italy, and from the R & D Department, Mipharm S.p.A., Milan, Italy
Correspondence
Dr Massimo Milani,
MD
R & D MipharmVia B. Quaranta 1220141 MilanItalyE-mail: [email protected]
Background
Alopecia areata (AA) affects almost 2% of the population inindustrialized countries.
1
Alopecia areata is an unpredictable,recurring, nonscarring, chronic inflammatory disease.
2
Anautoimmune response, mediated by T cells to an unknownhair-associated antigen, is believed to be the cause of hairloss.
3
Intralesional glucocorticoids are considered as first-line therapy for AA. However pain during injections anddermal atrophy are common, even if transient, side-effects.
4
Inaddition intralesional steroids are time- and cost-consuming.Some authors have reported promising clinical results in thetreatment of AA with topical corticosteroids.
5
In comparisonwith placebo, 12-week topical desoximetasone has shown
a moderately higher hair regrowth rate in AA patients.
6
Furthermore, topical fluocinolone and betamethasonedipropionate have shown satisfactory responses in patchyAA patients.
7
However most authors consider monotherapywith topical steroid of little benefit in AA treatment. Beta-methasone valerate is a medium potency glucocorticoidmolecule utilized for the treatment of corticosteroid-responsivedermatoses.
8
Betamethasone for topical application is cur-rently available in three formulations: cream, ointment andlotion. A new formulation of betamethasone valerate 0.1%in thermo phobic, low-residue, high bioavailability foamvehicle (BVF) is available for the topical treatment of scalpdermatoses.
9
Two controlled randomized trials involving 396patients have demonstrated that BVF is clinically superior

© 2003
The International Society of Dermatology International Journal of Dermatology
2003,
42
, 572–575
573
Mancuso
et al. Efficacy of betamethasone foam in alopecia areata
Pharmacology and Therapeutics Clinical trial
to betamethasone and other corticosteroid lotions in thetreatment of scalp psoriasis.
10,11
This clinical greater efficacyof BVF in comparison with steroid lotions could be because ofan enhanced skin penetration of the foam in comparison withother standard topical formulations.
12
No data are availableto date regarding the efficacy and safety profiles of BVF in thetreatment of mild-to-moderate patchy AA. The primary aimof our study was to evaluate the efficacy, tolerability andsafety of BVF treatment in comparison with betamethasonedipropionate lotion in patients with mild-to-moderate AA.The major trial outcome was to compare the hair regrowthscore between the two treatments at follow up (week 20).The secondary end-points were to evaluate the safety andtolerability profiles of the two drugs.
Methods
The study was a prospective, randomized, parallel groups,
investigator-blinded controlled trial. Between May 2001 and
June 2002, 98 outpatients with patchy AA were screened for the
study. A total of 61 patients (26 men and 35 women; mean age
41
±
13 years, range 18–69) with mild-to-moderate AA were
enrolled after obtaining their written informed consent. The
baseline assessment of alopecia grading was performed using a
6-point scale score: S0 = No alopecia, S1 = hair loss < 10%, S2 =
hair loss 11–25%, S3 = hair loss 26–50%, S4 = hair loss 51–75%
and S5 = hair loss > 75%. Main inclusion criteria were: male and
female patients, aged > 18 years, with mild-to-moderate (S1 or S2
grade, i.e. hair loss < 26%) patchy AA. Exclusion criteria were:
severe AA (= S3), positive history of steroid allergy, previous
(< 4 weeks) topical or systemic treatments for AA, and pregnant
or lactating women. Subjects were assigned randomly to BVF
(31 patients; 13 men and 18 women) (Bettamousse™, Mipharm,
Italy) or to betamethasone dipropionate lotion 0.05% (BDL) (30
subjects; 13 men and 17 women) (Diprosone™, Essex, Italy). Both
treatments were applied to the affected areas twice a day for 12
consecutive weeks with a subsequent 2-month follow-up period
without therapy (week 20). Randomization was performed using a
computer-generated randomization list (Arcus Quickstat™,
Cambridge, UK) with a block of eight patients in a 1 : 1 ratio. Treatment
allocation concealment was obtained using a phone-call
centralized procedure for each eligible patient. The sample size
calculation was based on the assumption of an absolute difference
of 1.5
±
1.4 at the end of the 20-week study period, in the RG score
in favor of BVM. With a power of 95% and a type I error of 0.05, a
total of at least 30 patients per arm (total 60) would have to be
recruited in the trial.
The Fisher exact test was used to compare categorical variables and
the Mann–Whitney test was used to compare continuous variables.
Patients were evaluated at baseline and at weeks 8 and 12 and at
follow up (week 20) to record the progress of hair regrowth.
Efficacy was evaluated on an intention-to-treat basis, using a
hair regrowth score (RGS) with a scale ranging from 0 (regrowth
< 10%) to 1 (11–25%), 2 (26–50%), 3 (51–75%) and 4 (regrowth
> 75%). All clinical evaluations were performed by two investigators
unaware of the patient’s treatment allocation. At baseline and at each
visit the target bald areas were traced onto transparent films and
reported in the Case Report form for regrowth score calculations.
Safety and tolerability were assessed evaluating self-reported
adverse reactions at each visit during the entire study duration.
Results
A total of 57 subjects (93%) completed the trial. For patientswho concluded the trial prematurely, the LOCF (Last Obser-vation Carried Forward) method was utilized. Figure 1 showsthe trial profile. One patient in the BVF group and threepatients in the BPL group discontinued prematurely the study.The reason for the discontinuation was the lack of efficacy ofthe treatments. At baseline, both groups were well matchedfor the relevant demographic and clinical indicators. Table 1
Table 1 Demographic and clinical characteristics at baseline
BVF (n = 31) BDL (n = 30)
Mean age (SD) 40 (13) 42 (12)Men/Women 13/18 13/17Mean alopecia grading (SD) 1.25 (0.4) 1.23 (0.4)Mean affected area cm2 (SD) 11.6 (8) 10.5 (9)Family history of AA 3/31 2/30
BVF = betamethasone valerate foam; BDP = betamethasone dipropionate lotion; AA = alopecia areata.
Figure 1 Design of the trial
International Journal of Dermatology
2003,
42
, 572–575 © 2003
The International Society of Dermatology
574 Pharmacology and Therapeutics Clinical trial
Efficacy of betamethasone foam in alopecia areata
Mancuso
et al.
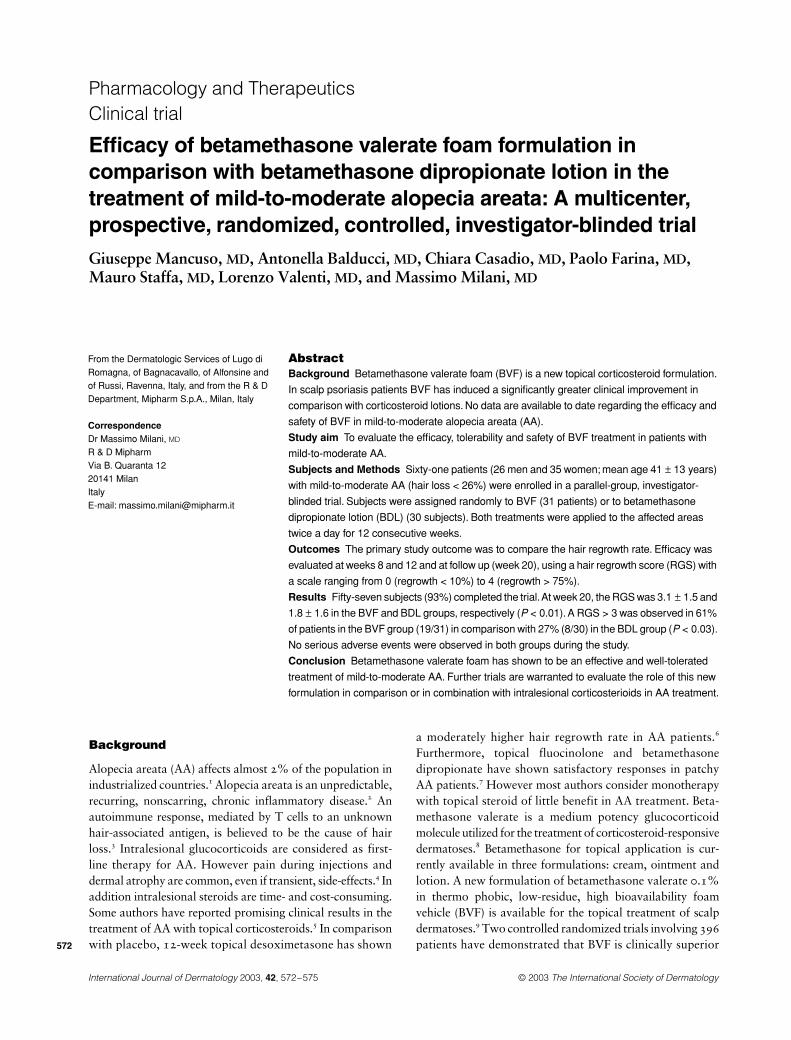
shows the main demographic and clinical characteristics ofthe enrolled patients. At week 20, the RGS was 3.1
±
1.5 and1.8
±
1.6 in the BVF and BPL groups, respectively (
P
< 0.01;Mann–Whitney test). At the end of the study period, theabsolute difference in the RGS in favor of BVF was
−
1.3 (95%CI =
−
2.7/
−
0.5). Figure 2 shows the RGSs during the studyduration. At week 20, a complete or nearly completeregrowth rate in the BVF group (i.e. RGS > 3) was observedin 61% (19/31) of the patients (95% CI = 45–80%) in com-parison with 27% (8/30) of the patients (95% CI = 12–45%)in the BDL group (
P
< 0.03; Fisher’s exact test) (Table 2).No serious adverse events were observed in both treatmentgroups during the study. Two patients in the BVF and one inthe BDL group reported mild folliculitis in the treated areas.
Discussion
Betamethasone valerate foam is a new, low-residue, highbioavalability delivery formulation of this steroid. It wasdeveloped to provide increased efficacy with high acceptabilityand compliance in patients with cortico-responsive scalpdermatoses. When applied to the scalp, at body temperature,
the foam rapidly breaks down (quick-break foam) and theactive ingredient (betamethasone valerate) is deposited on theskin with little residue. Most of the vehicle componentsquickly volatilize and the active compound is rapidlyabsorbed into the skin.
An experimental study on a human skin model hasshown that skin penetration of BVF is more than two-fold incomparison with skin penetration of betamethasone valeratelotion.
10
As a result of these characteristics BVF is particularlysuitable for the treatment of corticosteroid-responsive scalpdermatoses. In randomized, double-blind, controlled trials,involving more than 350 patients with scalp psoriasis, BVFhas shown greater clinical efficacy in comparison with othertopical steroids.
10,11
Our results have shown, for the first time, that BVF is aneffective and well-tolerated topical treatment of mild-to-moderate patchy AA. In addition, in this clinical setting,BVF has shown greater clinical efficacy in comparison withbetamethasone dipropionate lotion.
Intralesional glucocorticoids are considered as first-linetherapy for AA.
4
However, pain during injections and dermalatrophy are common, even if transient, side-effects. Inaddition, intralesional steroids are time- and cost-consuming.Some authors have reported promising clinical results fromAA treatment with topical corticosteroids.
6
However, mostauthors consider monotherapy with topical steroid to be oflittle benefit in AA treatment.
13
Our results suggest that the foam formulation could bean interesting first-line therapy in patients with mild-to-moderate patchy AA. However, some study limitations haveto be taken in account in evaluating the results of the presentstudy. First, this was not a double-blind trial. However, weutilized the investigator-blinded methods in assessing themajor outcome (i.e. the hair regrowth score) of the study. Asecond point is that we compared BVF (topical corticosteroidpotency Class 4) with a Class 3 topical steroid lotion (beta-methasone dipropionate). Some authors suggest thatClass 1 topical steroids, such as clobetasol propionate, are anappropiate topical treatment in AA patient.
4
However, nolotion formulations of clobetasol propionate are to date avail-able in our country. Our trial did not compare BVF with anintralesional steroid treatment regimen. However, the primaryend-point of our study was to evaluate if this new topicalfoam formulation had a clinically relevant efficacy, if any, inthis clinical setting. The results show that the 12-week treat-ment with BVF induced good clinical response in a remarkablepercentage (i.e. 61%; 95% CI = 45–80%) of patchy mild-to-moderate AA patients. It is well known that the clinicalhistory of AA is high unpredictable. As many as 50% of AApatients could present with hair regrowth without treatmentwithin 1 year.
2
However, we found a clear difference in theregrowth rate between the BVF and control groups. Thissuggests that BVF could be considered an interesting option in
Table 2 Distribution of the regrowth score at week 20
RGSBVF (n = 31)n (%)
BDP (n = 30)n (%)
0 2 (6) 9 (30)1 5 (16) 11 (36)2 1 (3) 1 (3)3 4 (12) 1 (3)4 19 (61) 8 (27)
BVF = betamethasone valerate foam; BDP = betamethasone dipropionate lotion; RGS = regrowth score: 0 (regrowth < 10%), 1 (11–25%), 2 (26–50%), 3 (51–75%) and 4 (> 75%).
Figure 2 Evolution of regrowth score (RGS) during treatments

© 2003
The International Society of Dermatology International Journal of Dermatology
2003,
42
, 572–575
575
Mancuso
et al. Efficacy of betamethasone foam in alopecia areata
Pharmacology and Therapeutics Clinical trial
the therapeutic approach of patients with mild-to-moderateAA. Further trials are warranted to evaluate the role of thisnew topical formulation in comparison or in combinationwith intralesional corticosterioids or different immunomodifier topical agents in AA treatment.
References
1 Safavi KH, Muller SA, Suman VJ. Incidence of alopecia areata in Olmsted County, Minnesota, 1975 trough 1989.
Mayo Clin Proc
1995;
70
: 628–633.2 Shapiro J, Madani S. Alopecia areata: diagnosis and
treatment.
Int J Dermatol
1999;
38
: 19–24.3 Todes-Tailor N, Turner R, Wood GS,
et al.
T cell subpopulations in alopecia areata.
J Am Acad Dermatol
1984;
11
: 216–223.4 Price VH. Treatment of hair loss.
N Eng J Med
1999;
341
: 964–973.
5 Fielder VC, Alati S. Treatment of alopecia areata.
Dermatol Clin
1996;
14
: 733–738.6 Charuwichitratana S. Randomised double-blind placebo-
controlled trial in the treatment of alopecia areata with 0.25% desoximetasone cream.
Arch Dermatol
2000;
10
: 241–243.
7 Pascher F, Kurtin S, Andrade R. Assay of 0.2% fluocinolone acetonide cream for alopecia areata and totalis.
Dermatologica
1970;
141
: 193–202.8 Samson C, Peets E, Winter-Sperry R,
et al.
Batamethasone valerate – Valisone® – establishment of a new standard for topical corticosteroid potency. In: Maibach HI, Surber C, eds.
Topical Corticosteroids
. Basel: Karger, 1992: 335–348.9 Feldman SRN, Sangha V. Setaluri: Topical corticosteroid in
foam vehicle offers comparable coverage compared with traditional vehicles.
J Am Acad Dermatol
2000;
42
: 1017–1020.
10 Franz TJ, Parsell DA, Halualani RM,
et al.
Betamethasone valerate foam 0.12%. a novel vehicle with enhanced delivery and efficacy.
International J Dermatol
1999;
38
: 628–632.11 Andreassi L, Giannetti A, Milani M. Efficacy of
betamethasone valerate mousse in comparison with standard therapies on scalp psoriasis: an open, multi-centre, randomised, controlled, cross-over study on 241 patients.
Br J Dermatol
; in press.12 Franz TJ, Parsell DA, Meyers JA,
et al.
Clobetasol propionate foam 0.05% a novel vehicle with enhanced delivery.
Int J Dermatol
2000;
39
: 535–538.13 Shapiro J, Price V. Hair regrowth: therapeutic agents.
Dermatol Clin
1998;
16
: 341–356.


![Studies on cleaning validation for a cream and ointment … · 2016-12-14 · carryover (MACO) of betamethasone valerate, tolnaftate and cliquinol [27]. Stock standard solutions were](https://img.pdfslide.net/doc/110x75/5e7e40ebc853814cc0452a54/studies-on-cleaning-validation-for-a-cream-and-ointment-2016-12-14-carryover-maco.jpg)


























