Embed Size (px)
Citation preview
23
ABSTRACT
A 54-y-old patient with rheumatoid arthritis (RA) and bilateral lower-limb lymphoedema is presented. Complete decongestive physical therapy (CDP) is the cornerstone of the management programme in all patients suffering from lymphoedema associated with RA, but it is not clear which therapy is the most effective in decreasing the oedema. We report on a patient with bilateral lower-limb lymphoedema associated with RA who, after receiving etanercept and CDP, showed moderate improvement. There is little infor-mation on the benefit of etanercept therapy for the extra-articular manifes-tations of RA. Further research is necessary to confirm the beneficial effect of etanercept and CDP.
Keywords: etanercept; lymphoedema; rheumatoid arthritis; treatment
Efficacy of Etanercept and Complete Decongestive Physical Therapy in Bilateral Lower-Limb Lymphoedema Associated with Rheumatoid Arthritis: a Case ReportSibel EyigorHale KarapolatYeşim KirazliUniversity of Ege, Faculty of Medicine, Department of Physical Medicine and Rehabilitation, Bornova, Izmir, Turkey
Address correspondence to: Sibel Eyigor, University of Ege, Faculty of Medicine, Department of Physical Therapy and Rehabilitation, 35100 Bornova, Izmir, Turkey. Email: [email protected]
Adv Ther. 2008:25(1):23–28DOI:10.1007/s12325-008-0006-1
Advances in Therapy® Rheumatoid Arthritis Lymphoedema Treatment
24
INTRODUCTION
Lymphoedema is an extra-articular manifestation rarely found in rheuma-toid arthritis (RA).1–3 To the best of our knowledge, fewer than 30 cases have been reported in the literature.2–11 A strategy of care has been introduced that exploits physical therapies. Physical treatment of affected limbs has been shown to result in partial resolution of the lymphoedema.1
Complete decongestive physical therapy (CDP) remains the cornerstone of the therapy in lymphoedema. There is little information on the benefit of antitumour necrosis factor alpha (TNF-alpha) thera-py for the extra-articular manifestations of RA.11,12 We report a case in which a pa-tient with disabling RA developed bilat-eral lower-limb lymphoedema, which was treated with etanercept and CDP.
CASE DESCRIPTION
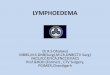
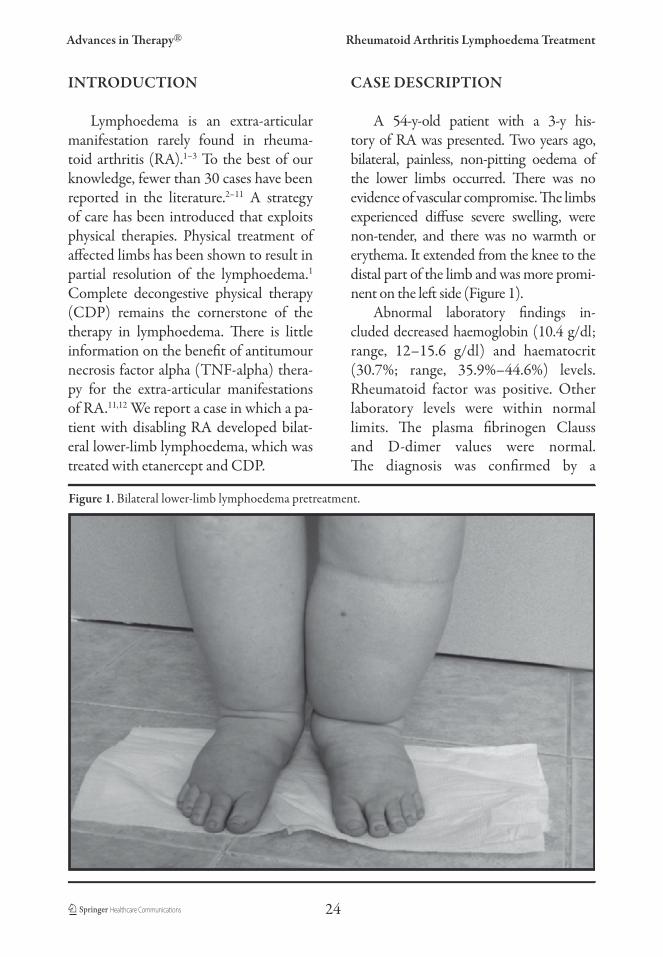
A 54-y-old patient with a 3-y his-tory of RA was presented. Two years ago, bilateral, painless, non-pitting oedema of the lower limbs occurred. There was no evidence of vascular compromise. The limbs experienced diffuse severe swelling, were non-tender, and there was no warmth or erythema. It extended from the knee to the distal part of the limb and was more promi-nent on the left side (Figure 1).
Abnormal laboratory findings in-cluded decreased haemoglobin (10.4 g/dl;range, 12–15.6 g/dl) and haematocrit (30.7%; range, 35.9%–44.6%) levels.Rheumatoid factor was positive. Other laboratory levels were within normal limits. The plasma fibrinogen Claussand D-dimer values were normal.The diagnosis was confirmed by a
Figure 1. Bilateral lower-limb lymphoedema pretreatment.
Eyigor et al.
25
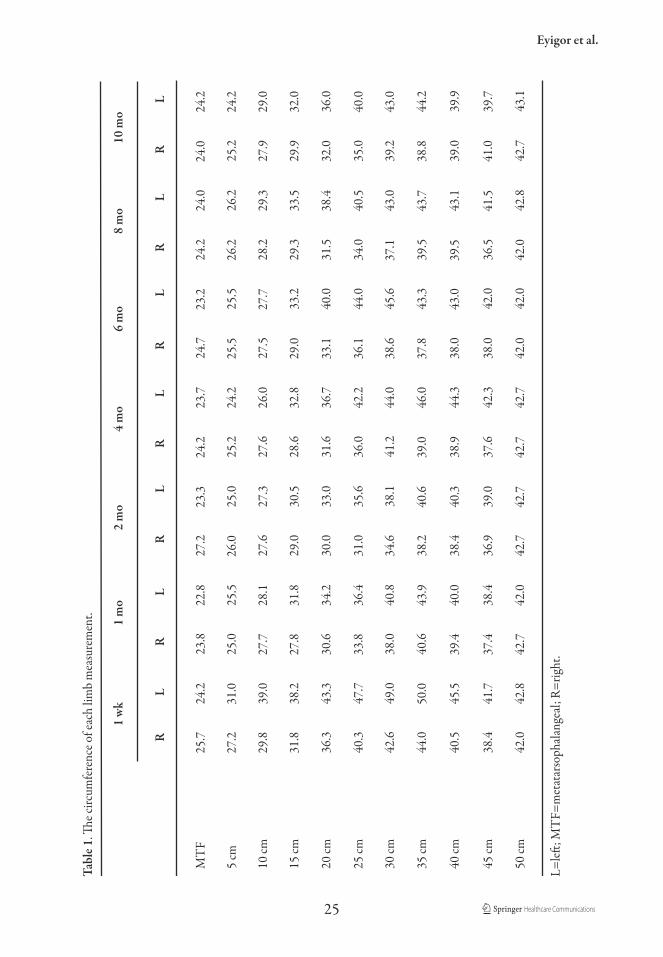
Tabl
e 1. Th
e circ
umfe
renc
e of e
ach
limb
mea
sure
men
t.
1
wk
1
mo
2 m
o
4 m
o
6 m
o
8 m
o
1
0 m
o
R
L
R
L
R
L
R
L
R
L
R
L
R
L
MT
F
25.7
24.2
23.
822
.8
2
7.2
23.3
24.
2
2
3.7
24.
723
.2
2
4.2
24.0
24.0
24.
2
L=left
; MT
F=m
etat
arso
phal
ange
al; R
=rig
ht.
5 cm
27.2
31.0
25.
025
.526
.0
2
5.0
25.
224
.225
.5
2
5.5
26.2
26.
2
2
5.2
24.2
10
cm
29
.839
.027
.728
.1
2
7.6
27.3
27.
626
.0
2
7.5
27.7
28.
229
.3
2
7.9
29.0
15
cm
31
.838
.227
.831
.8
2
9.0
30.5
28.
632
.829
.0
3
3.2
29.3
33.5
29.
932
.0
20
cm
36
.343
.330
.634
.2
3
0.0
33.0
31.
636
.733
.1
4
0.0
31.
538
.4
3
2.0
36.
0
25
cm
40
.347
.733
.836
.4
3
1.0
35.6
36.
042
.236
.1
4
4.0
34.0
40.5
35.
040
.0
30
cm
42
.649
.038
.040
.834
.6
3
8.1
41.
244
.038
.6
4
5.6
37.1
43.
0
3
9.2
43.0
35
cm
44
.050
.0
4
0.6
43.9
38.
240
.6
3
9.0
46.
037
.8
4
3.3
39.5
43.7
38.
8
4
4.2
40
cm
40
.545
.539
.440
.0
3
8.4
40.3
38.
9
4
4.3
38.0
43.0
39.5
43.
1
3
9.0
39.
9
45
cm
38
.441
.737
.438
.4
3
6.9
39.0
37.
6
4
2.3
38.0
42.
036
.541
.5
4
1.0
39.
7
50
cm
42
.042
.842
.742
.0
4
2.7
42.7
42.
7
4
2.7
42.0
42.
042
.0
4
2.8
42.
7
4
3.1
Advances in Therapy® Rheumatoid Arthritis Lymphoedema Treatment
26
lymphoscintigraphy, which showed very slow, low-level lymphatic drain-age in the bilateral lower limbs.Doppler ultrasound studies did not re-veal venous and arterial abnormalities. Soft-tissue ultrasonography showed diffuse oedema of the bilateral lower limb, which was more apparent in the lateral cruris. Magnetic resonance im-aging (MRI) disclosed that the diam-eter of the left cruris was larger than the right and the increase in diameter included the difference in subcutane-ous fat tissue. Chest x-ray and com-puted tomography of the thorax were unremarkable. Previous therapies (methyl prednisolone 4 mg/d, meth-otrexate 7.5 mg/wk, sulphasalazine 2x500 mg/d) were continued and treat-ment with etanercept began at a twice-
weekly dose of 25 mg. At the same time, CDP of the affected limbs was started 5 d per wk. Treating lymphoedema us-ing CDP involves 4 main components: skin care, manual lymph drainage, compression (multilayer bandaging) and exercise. Outcomes related to the lymphoedema were measured weekly using the sum of each limb’s circumfer-ence. The measurements were evalu-ated according to the distances from the medial malleoli (Table 1).
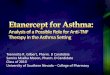
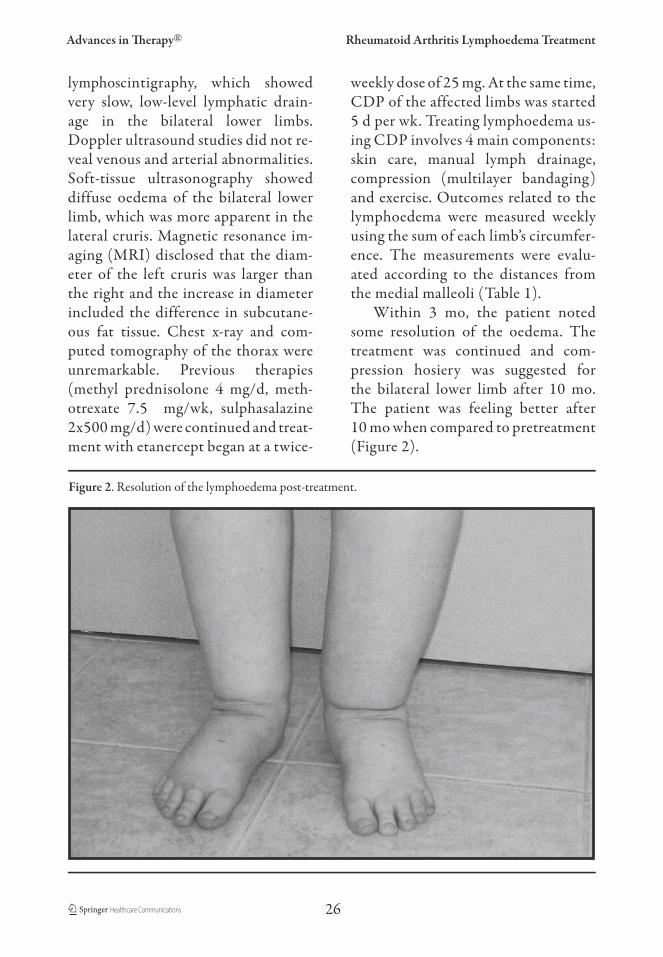
Within 3 mo, the patient noted some resolution of the oedema. The treatment was continued and com-pression hosiery was suggested for the bilateral lower limb after 10 mo. The patient was feeling better after 10 mo when compared to pretreatment (Figure 2).
Figure 2. Resolution of the lymphoedema post-treatment.

Eyigor et al.
27
DISCUSSION
Lymphoedema associated with RA was first described by Kalliomaki and Vas-tamaki in 1968,13 and it thus appears to be a relatively rare complication of RA.14
Doppler ultrasonography, ultrasonogra-phy, MRI, lymphoscintigraphy and his-topathological examination can be used to confirm the diagnosis of lymphoede-ma.14,15 Several reports indicate that lym-phoedema as a complication of RA is not restricted to seropositive arthritis but also occurs in other forms of inflammatory ar-thropathy.14–16 Although the aetiology is unknown in inflammatory arthropathy, several hypotheses have been suggested on the pathogenesis in patients with RA, such as lymphangitis, lymphatic obstruc-tion caused by fibrin, capillary perme-ability increase, abnormal fibrinolysis and possible fibrosis of the superficial lymph vessels. There was no positive correlation between the rheumatoid factor and the severity of the disease.9,14 In our patient, the rheumatoid factor was positive but rheumatoid factor-negative cases have also been reported.7
Cases described in the literature are predominantly of the upper limbs, some-times bilateral, and occasionally occur on lower limbs such as that seen in our patient. In these cases the diagnosis is clinical, as 1 or more limbs have been observed to undergo painless swelling.2,10 Some cases presented an increase of the plasma fibrinogen deg-radation products or hipoalbuminsemia.9We did not find any laboratory abnormal-ity of these symptoms in our case study. Ostrov reported a case where qualitative lymphoscintigraphy disclosed abnormal lymphatic drainage of the affected limb.11
In our patient, lymphoscintigraphy of both limbs showed impaired lymph flow.
Treatment for lymphoedema is inef-ficient and is usually limited to symp-tomatic treatment, and treatment of the underlying RA does not improve the lymphoedema. Treatment options for rheumatoid lymphoedema include rest-ing, use of diuretics and physical ther-apy, although none have been highly effective.2,7,8,14,15 In most cases, disease-modifying therapy does not improve the lymphoedema.8 Anti-TNF therapy has been found to be efficient on peripheral articular manifestations.11,12 However, there is little information available on its efficacy for extra-articular manifesta-tions. Ostrov11 reported that etanercept dramatically reduced the lymphoedema in a patient with RA. Almodovar et al.12
described the first case of a patient diag-nosed with ankylosing spondylitis that was complicated with lymphoedema who, after receiving treatment with inf-liximab, showed complete disappearance of the lymphoedema. The way in which anti-TNF therapy acts on lymphoedemas is not known, but the drugs are believed to act on the inflammatory response of the lymphatic vessels. Assuming synovitis causes adjacent lymphatic inflammation and ultimate fibrosis, maximal control of active rheumatoid synovitis could abro-gate this reaction. Therefore, anti-TNF therapy can be considered for the treat-ment of extra-articular manifestations in RA, such as lymphoedema. In our patient, moderate improvement was seen with anti-TNF therapy and CDP, although physical treatment of the affected limb showed impressive results. Although most of the research related to intervention

Advances in Therapy® Rheumatoid Arthritis Lymphoedema Treatment
28
for lymphoedema has focused on upper-extremity problems following breast cancer, many studies have addressed the effective-ness of CDP for both upper- and lower-extremity lymphoedema.1
Evidence of the benefits of this treat-ment is insufficient in the literature and this is only the second case to bediagnosed with RA combined with bi-lateral lower-limb lymphoedema which, after receiving etanercept, showed moder-ate improvement. There is little informa-tion on the benefit of etanercept therapy for the extra-articular manifestations of RA. Further research is necessary to con-firm the beneficial effect of etanercept and CDP.
REFERENCES
1. Holtgrefe KM. Twice-weekly complete de-congestive physical therapy in the manage-ment of secondary lymphedema of the lower extremities. Phys Ther. 2006;86:1128–1136.
2. Joos E, Bourgeois P, Famaey JP. Lymphatic disorders in rheumatoid arthritis. Semin Arthritis Rheum. 1993;22:392–398.
3. Hidalgo CC, Cuesta AM, Llorente MMJ, Espinosa CA, Balsa CA, Gijon BJ. Lympho-scintigraphic study in a case of rheumatoid arthritis-related lymphoedema. Clin Exp Rheumatol. 1993;11:421–423.
4. Kiely PD, Joseph AE, Mortimer PS, Bourke BE. Upper limb lymphedema associated with polyarthritis of rheumatoid type. JRheumatol. 1994;21:1043–1045.
5. Dippy JE. Lymphoedema complicating rheumatoid arthritis. Ann Rheum Dis.1991;50:658.
6. Bamji A. Limb lymphoedema in rheuma-toid arthritis. Ann Rheum Dis. 1991;50:407.
7. Lacroix HR, Gruwez JA, Casteels-Van Daele MC, Dequeker J. Lymphedema of the leg associated with rheumatoid arthritis. Lymphology. 1991;24:68–70.
8. Dacre JE, Scott DL, Huskisson EC. Lym-phoedema of the limbs as an extra-articular feature of rheumatoid arthritis. Ann Rheum Dis. 1990;49:722–724.
9. Minari C, Cecconami L, Fioravanti A, Montemerani M, Scola C, Marcon-longo R. Lymphoedema of the limbs in rheumatoid arthritis. Clin Rheumatol.1994;13:464–469.
10. Sant SM, Tormey VJ, Freyne P, Casey EB. Lymphatic obstruction in rheumatoid ar-thritis. Clin Rheumatol. 1995;14:445–450.
11. Ostrov BE. Beneficial effect of etanercept on rheumatoid lymphedema. Arthritis Rheum. 2001;44:240–241.
12. Almodovar R, Zarco P, Quiros FJ, Maz-zucchelli R. Infliximab treatment efficacy in lymphedema associated with ankylos-ing spondylitis. Rheumatology (Oxford).2004;43:1456.
13. Kalliomaki JL, Vastamaki M. Chronic dif-fuse oedema of the rheumatic hand: a sign of local lymphatic involvement. Ann Rheum Dis. 1968;27:167–169.
14. Bohm M, Riemann B, Luger TA, Bonsmann G. Bilateral upper limb lymphedema associ-ated with psoriatic arthritis: a case report and review of the literature. Br J Dermatol. 2000;143:1297–1301.
15. Schmit P, Prieur AM, Brunelle F. Juvenile rheumatoid arthritis and lymphedema: lymphangiographic aspects. Pediatr Radiol.1999;29:364–366.
16. Kiely PD, Mortimer PS, Bourke BE. Lym-phatic function in inflammatory arthritis. Br J Rheumatol. 1995;34:689–691.