Embed Size (px)
Citation preview
DOI: 10.1542/peds.2009-0333; originally published online September 7, 2009; 2009;124;e782Pediatrics
Annaleise M. Riethmuller, Rachel A. Jones and Anthony D. OkelySystematic Review
Efficacy of Interventions to Improve Motor Development in Young Children: A
http://pediatrics.aappublications.org/content/124/4/e782.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from
Efficacy of Interventions to Improve MotorDevelopment in Young Children: A Systematic Review
abstractOBJECTIVE: The objective of this study was to systematically reviewevidence from controlled trials on the efficacy of motor developmentinterventions in young children.
METHODS: A literature search of interventions was conducted of 14electronic databases. Three reviewers independently evaluated stud-ies to determine whether they met the inclusion criteria. Studies werecompared on 5 components: design, methodologic quality, interventioncomponents, efficacy, and alignment with the Consolidated Standard ofReporting Trials (CONSORT) and Transparent Reporting of Evaluationwith Nonrandomized Designs (TREND) statements.
RESULTS: Seventeen studies met the inclusion criteria. More than half(65%) were controlled trials and delivered at child care settings orschools (65%). Three studies had high methodologic quality. Studieswere�12 weeks in duration and delivered by teachers, researchers,and students. Parents were involved in only 3 studies. Nearly 60% of thestudies reported statistically significant improvements at follow-up.Three studies aligned with the CONSORT and TREND statements.
CONCLUSIONS: This review highlights the limited quantity and qualityof interventions to improve motor development in young children. Thefollowing recommendations are made: (1) both teachers and re-searchers should be involved in the implementation of an intervention;(2) parental involvement is critical to ensuring transfer of knowledgefrom the intervention setting to the home environment; and (3) inter-ventions should be methodologically sound and follow guidelines de-tailed in the CONSORT or TREND statement. Pediatrics 2009;124:e782–e792
AUTHORS: Annaleise M. Riethmuller, BEd, Rachel A.Jones, PhD, and Anthony D. Okely, EdD
Child Obesity Research Centre, Faculty of Education, Universityof Wollongong, Wollongong, New South Wales, Australia
KEY WORDSintervention, physical activity, fundamental movement skills,early childhood, preschool children
ABBREVIATIONSCONSORT—Consolidated Standard of Reporting TrialsTREND—Transparent Reporting of Evaluation withNonrandomized Designs
www.pediatrics.org/cgi/doi/10.1542/peds.2009-0333
doi:10.1542/peds.2009-0333
Accepted for publication May 29, 2009
Address correspondence to Rachel A. Jones, PhD, Child ObesityResearch Centre, Faculty of Education, University of Wollongong,Wollongong, NSW 2522, Australia. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
e782 RIETHMULLER et al at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from
Physical activity is important for boththe health and the overall growth anddevelopment of young children.1 Partof the rationale for promoting physicalactivity in this age group is that it de-velops motor skills.2 This is supportedby research that shows a consistentrelationship, albeit cross-sectionally,between physical activity and motordevelopment.3–5
Motor skill proficiency levels amongyoung children have been describedas suboptimal,6 which is concerninggiven that proficiency levels track intochildhood and adolescence7,8 and arerelated to health outcomes such as ad-iposity,9 self-esteem,10 cardiorespira-tory fitness,11 and physical activity.12,13
As such, developing interventions toimprove motor skills in young childrenis a priority. This is in line with currentrecommendations fromNorth Americathat state that the emphasis of physi-cal activity during preschool yearsshould be on the development ofmotorskills.1,14,15
Better understanding of the poten-tial of motor development interven-tions to improve motor skills inyoung children is important in in-forming pediatricians and otherhealth care providers of its efficacyas an intervention strategy. Unfortu-nately, the efficacy of interventionsto develop motor skills is not clear.Limitations with previous reviews in-clude the focus on children who haveor at risk for developmental disor-ders,16,17 operationalization of motordevelopment as the dependent butnot also the independent variable,18
and the inclusion of motor develop-ment as an independent but not adependent variable.19 The aim ofthis study, therefore, was to reviewsystematically evidence from con-trolled trials on the efficacy of motordevelopment interventions in youngchildren.
METHODS
Identification of Studies
A literature search of interventions toimprove motor development in pre-school children (mean age:�5 years)was conducted of 14 electronic data-bases (A� Education, ERIC [Ovid], Med-line [Ovid], Health Reference Centre Ac-ademic, Sports Discuss, CurrentContents Connect, PubMed, ISI Web ofScience, CINAHL [Cumulative Index toNursing and Allied Health Literature],PsychInfo, Australian Family and Soci-ety Plus, Expanded Academic ASAP,Dissertation Abstracts, and EbscoMegafile Premier) from January 1987to June 2007. The search strategy fo-cused on 3 elements: motor develop-ment (key words: play, coordination,motor development, motor skills), age(key words: toddler, preschool), andintervention (key words: program,trial, intervention). There was also acitation search of included articlesand relevant published reviews.
Criteria for Inclusion/Exclusion
Articles were included when they werereported on an intervention that tar-geted children with a mean age of�5years and measured motor develop-ment objectively (eg, fundamental
movement skill proficiency). Articleswere excluded when they were pub-lished in a language other than Englishor published before. 1987; when the in-tervention targeted children with aspecific disease or health problem;when the full article was not available;or when the intervention was �4weeks, had �10 participants, had nocontrol group, or reported only quali-tative data.
Articles were initially excluded onscreening of title and abstract. Whenappropriateness of the article couldnot be determined, the full article wasobtained. Three reviewers indepen-dently evaluated, using a standardizedchecklist, full text copies of all ob-tained articles to determine whetherthey met the inclusion criteria. Whenopinions differed, a consensus wasreached through discussion.
Assessment of MethodologicQuality
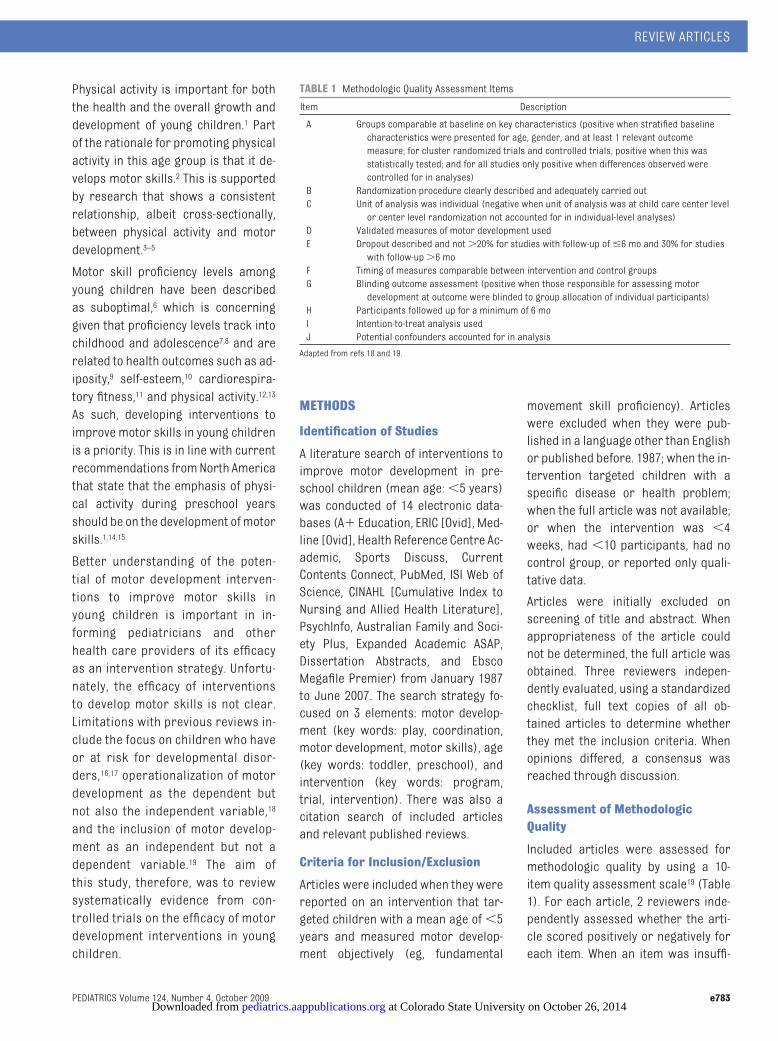
Included articles were assessed formethodologic quality by using a 10-item quality assessment scale19 (Table1). For each article, 2 reviewers inde-pendently assessed whether the arti-cle scored positively or negatively foreach item. When an item was insuffi-
TABLE 1 Methodologic Quality Assessment Items
Item Description
A Groups comparable at baseline on key characteristics (positive when stratified baselinecharacteristics were presented for age, gender, and at least 1 relevant outcomemeasure; for cluster randomized trials and controlled trials, positive when this wasstatistically tested; and for all studies only positive when differences observed werecontrolled for in analyses)
B Randomization procedure clearly described and adequately carried outC Unit of analysis was individual (negative when unit of analysis was at child care center level
or center level randomization not accounted for in individual-level analyses)D Validated measures of motor development usedE Dropout described and not�20% for studies with follow-up of�6 mo and 30% for studies
with follow-up�6 moF Timing of measures comparable between intervention and control groupsG Blinding outcome assessment (positive when those responsible for assessing motor
development at outcome were blinded to group allocation of individual participants)H Participants followed up for a minimum of 6 moI Intention-to-treat analysis usedJ Potential confounders accounted for in analysis
Adapted from refs 18 and 19.
REVIEW ARTICLES
PEDIATRICS Volume 124, Number 4, October 2009 e783 at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from
ciently described, it was allocated anegative score. Agreement betweenreviewers for each article was set apriori at 80%19,20; that is, for each arti-cle, reviewers were required to agreethat the items were either present orabsent for 8 of 10 items. In the case of�80% agreement, consensus wasreached by additional discussion. Thescores were then summed for each ar-ticle to determine the overall quality ofthe article. An article was deemed tohave high methodologic quality when itscored�5 for a controlled trial and�6for a randomized, controlled trial.19
Comparing Results
To facilitate comparison between stud-ies, we extracted the following datafrom each article: (1) design, includingrandomization procedures and set-tings; (2) methodologic quality (de-scribed already); (3) intervention com-ponents, including sample size, lengthof the intervention, hours of instruc-tion, program deliverer, and parentalinvolvement; (4) effectiveness of the in-tervention immediately after interven-tion and at subsequent follow-up (eg,12 months); and (5) alignment with theConsolidated Standard of ReportingTrials (CONSORT) and Transparent Re-porting of Evaluation with Nonrandom-ized Designs (TREND) statements.21,22
This review includes interventions thatreport motor skill development by us-ing different instruments, thereby al-lowing more interventions to be in-cluded; however, this does not make itpossible to pool the results. Ratherthan using a set change standard forassessing whether an interventionwas or was not efficacious, each inter-vention’s efficacy was assessed on thebasis of its own reported results. Anintervention was deemed efficaciouswhen the intervention group showed astatistically significant improvementin comparison with the control group.
RESULTS
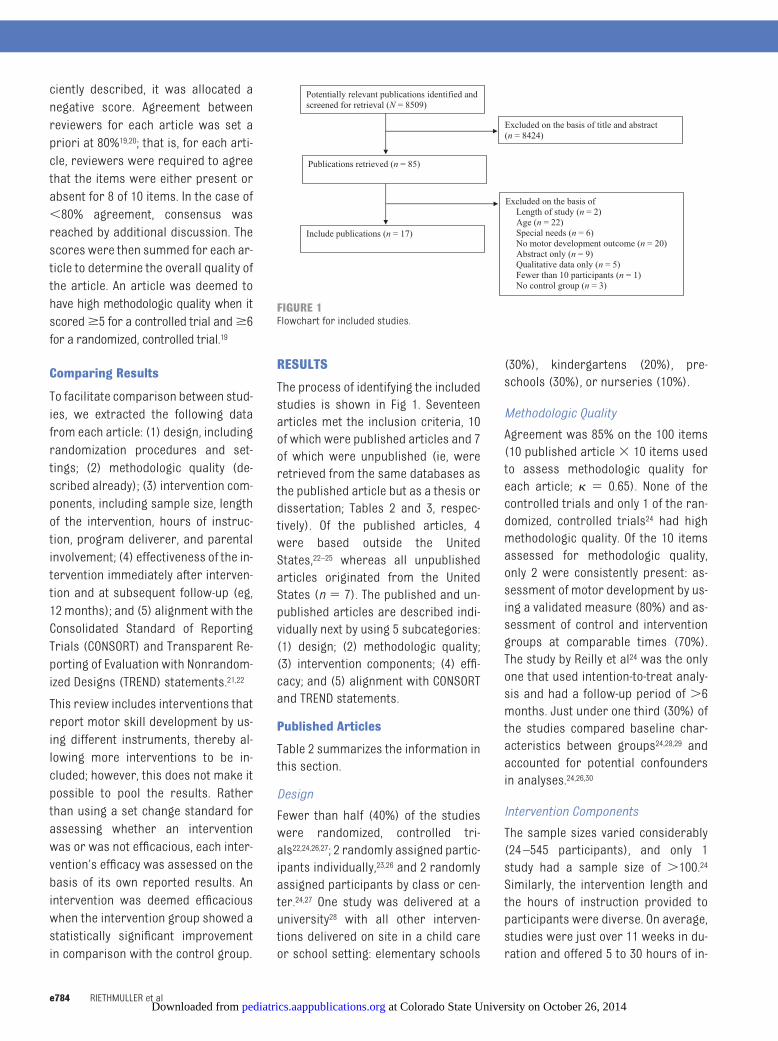
The process of identifying the includedstudies is shown in Fig 1. Seventeenarticles met the inclusion criteria, 10of which were published articles and 7of which were unpublished (ie, wereretrieved from the same databases asthe published article but as a thesis ordissertation; Tables 2 and 3, respec-tively). Of the published articles, 4were based outside the UnitedStates,22–25 whereas all unpublishedarticles originated from the UnitedStates (n � 7). The published and un-published articles are described indi-vidually next by using 5 subcategories:(1) design; (2) methodologic quality;(3) intervention components; (4) effi-cacy; and (5) alignment with CONSORTand TREND statements.
Published Articles
Table 2 summarizes the information inthis section.
Design
Fewer than half (40%) of the studieswere randomized, controlled tri-als22,24,26,27; 2 randomly assigned partic-ipants individually,23,26 and 2 randomlyassigned participants by class or cen-ter.24,27 One study was delivered at auniversity28 with all other interven-tions delivered on site in a child careor school setting: elementary schools
(30%), kindergartens (20%), pre-schools (30%), or nurseries (10%).
Methodologic Quality
Agreement was 85% on the 100 items(10 published article� 10 items usedto assess methodologic quality foreach article; � � 0.65). None of thecontrolled trials and only 1 of the ran-domized, controlled trials24 had highmethodologic quality. Of the 10 itemsassessed for methodologic quality,only 2 were consistently present: as-sessment of motor development by us-ing a validated measure (80%) and as-sessment of control and interventiongroups at comparable times (70%).The study by Reilly et al24 was the onlyone that used intention-to-treat analy-sis and had a follow-up period of �6months. Just under one third (30%) ofthe studies compared baseline char-acteristics between groups24,28,29 andaccounted for potential confoundersin analyses.24,26,30
Intervention Components
The sample sizes varied considerably(24–545 participants), and only 1study had a sample size of �100.24
Similarly, the intervention length andthe hours of instruction provided toparticipants were diverse. On average,studies were just over 11 weeks in du-ration and offered 5 to 30 hours of in-
Potentially relevant publications identified and screened for retrieval (N = 8509)
Publications retrieved (n = 85)
Include publications (n = 17)
Excluded on the basis of title and abstract (n = 8424)
Excluded on the basis of Length of study (n = 2) Age (n = 22) Special needs (n = 6) No motor development outcome (n = 20) Abstract only (n = 9) Qualitative data only (n = 5) Fewer than 10 participants (n = 1) No control group (n = 3)
FIGURE 1Flowchart for included studies.
e784 RIETHMULLER et al at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from
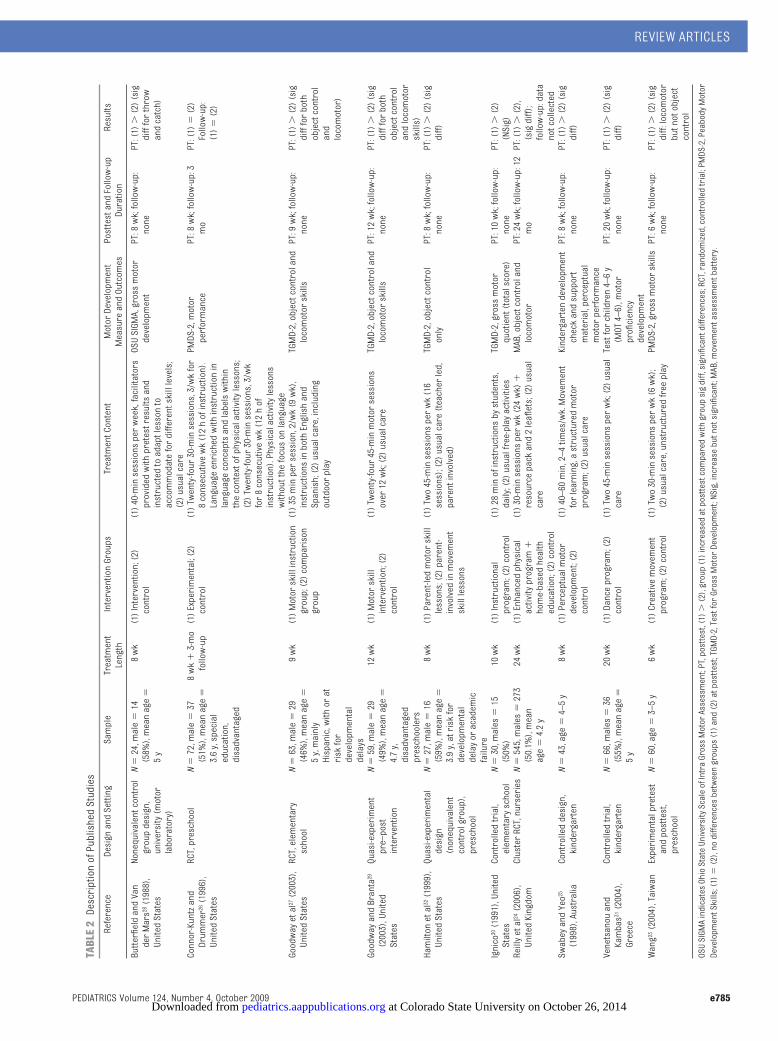
TABLE2DescriptionofPublishedStudies
Reference
DesignandSetting
Sample
Treatment
Length
InterventionGroups
TreatmentContent
MotorDevelopment
MeasureandOutcomes
PosttestandFollow-up
Duration
Results
ButterfieldandVan
derMars28(1988),
UnitedStates
Nonequivalentcontrol
groupdesign,
university(motor
laboratory)
N�24,male
�14
(58%),meanage
�5y
8wk
(1)Intervention;(2)
control
(1)40-minsessionsperweek,facilitators
providedwithpretestresultsand
instructedtoadaptlessonto
accommodatefordifferentskilllevels;
(2)usualcare
OSUSIGMA,grossmotor
development
PT:8wk;follow-up:
none
PT:(1)
�(2)(sig
diffforthrow
andcatch)
Connor-Kuntzand
Drummer26(1996),
UnitedStates
RCT,preschool
N�72,male
�37
(51%),meanage
�3.6y,special
education,
disadvantaged
8wk
�3-mo
follow-up(1)Experimental;(2)
control
(1)Twenty-four30-minsessions,3/wkfor
8consecutivewk(12hofinstruction).
Languageenrichedwithinstructionin
languageconceptsandlabelswithin
thecontextofphysicalactivitylessons;
(2)Twenty-four30-minsessions,3/wk
for8consecutivewk(12hof
instruction).Physicalactivitylessons
withoutthefocusonlanguage
PMDS-2,motor
performance
PT:8wk;follow-up:3
mo
PT:(1)
�(2)
Follow-up:
(1)�(2)
Goodwayetal27(2003),
UnitedStates
RCT,elementary
school
N�63,male
�29
(46%),meanage
�5y,mainly
Hispanic,withorat
riskfor
developmental
delays
9wk
(1)Motorskillinstruction
group;(2)comparison
group
(1)35minpersession,2/wk(9wk),
instructionsinbothEnglishand
Spanish;(2)usualcare,including
outdoorplay
TGMD-2,objectcontroland
locomotorskills
PT:9wk;follow-up:
none
PT:(1)
�(2)(sig
diffforboth
objectcontrol
andlocomotor)
GoodwayandBranta29
(2003),United
States
Quasi-experiment
pre–post
intervention
N�59,male
�29
(49%),meanage
�4.7y,
disadvantaged
preschoolers
12wk
(1)Motorskill
intervention;(2)
control
(1)Twenty-four45-minmotorsessions
over12wk;(2)usualcare
TGMD-2,objectcontroland
locomotorskills
PT:12wk;follow-up:
none
PT:(1)
�(2)(sig
diffforboth
objectcontrol
andlocomotor
skills)
Hamiltonetal32(1999),
UnitedStates
Quasi-experimental
design
(nonequivalent
controlgroup),
preschool
N�27,male
�16
(59%),meanage
�3.9y,atriskfor
developmental
delayoracademic
failure
8wk
(1)Parent-ledmotorskill
lessons;(2)parent-
involvedinmovement
skilllessons
(1)Two45-minsessionsperwk(16
sessions);(2)usualcare(teacherled,
parentinvolved)
TGMD-2,objectcontrol
only
PT:8wk;follow-up:
none
PT:(1)
�(2)(sig
diff)
Ignico30(1991),United
States
Controlledtrial,
elementaryschoolN
�30,males
�15
(50%)
10wk
(1)Instructional
program;(2)control(1)28minofinstructionsbystudents,
daily;(2)usualfree-playactivities
TGMD-2,grossmotor
quotient(totalscore)
PT:10wk;follow-up:
none
PT:(1)
�(2)
(NSig)
Reillyetal24(2006),
UnitedKingdom
ClusterRCT,nurseriesN
�545,males
�273
(50.1%),mean
age
�4.2y
24wk
(1)Enhancedphysical
activityprogram
�home-basedhealth
education;(2)control
(1)30-minsessionsperwk(24wk)
�resourcepackand2leaflets;(2)usual
care
MAB,objectcontroland
locomotor
PT:24wk;follow-up:12
mo
PT:(1)
�(2),
(sigdiff);
follow-up:data
notcollected
SwabeyandYeo25
(1998),Australia
Controlleddesign,
kindergarten
N�43,age
�4–5y
8wk
(1)Perceptualmotor
development;(2)
control
(1)40–60min,2–4times/wk.Movement
forlearning,astructuredmotor
program;(2)usualcare
Kindergartendevelopment
checkandsupport
material,perceptual
motorperformance
PT:8wk;follow-up:
none
PT:(1)
�(2)(sig
diff)
Venetsanouand
Kambas31(2004),
Greece
Controlledtrial,
kindergarten
N�66,males
�36
(55%),meanage
�5y
20wk
(1)Danceprogram;(2)
control
(1)Two45-minsessionsperwk;(2)usual
care
Testforchildren4–6y
(MOT4–6),motor
proficiency
development
PT:20wk;follow-up:
none
PT:(1)
�(2)(sig
diff)
Wang23(2004),Taiwan
Experimentalpretest
andposttest,
preschool
N�60,age
�3–5y
6wk
(1)Creativemovement
program;(2)control(1)Two30-minsessionsperwk(6wk);
(2)usualcare,unstructuredfreeplayPMDS-2,grossmotorskillsPT:6wk;follow-up:
none
PT:(1)
�(2)(sig
diff:locomotor
butnotobject
control
OSUSIGMAindicatesOhioStateUniversityScaleofIntraGrossMotorAssessment;PT,posttest,(1)�(2),group(1)increasedatposttestcomparedwithgroupsigdiff,significantdifferences;RCT,randomized,controlledtrial;PMDS-2,PeabodyMotor
DevelopmentSkills;(1)
�(2),nodifferencesbetweengroups(1)and(2)atposttest;TGMD-2,TestforGrossMotorDevelopment;NSig,increasebutnotsignificant;MAB,movementassessmentbattery.
REVIEW ARTICLES
PEDIATRICS Volume 124, Number 4, October 2009 e785 at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from
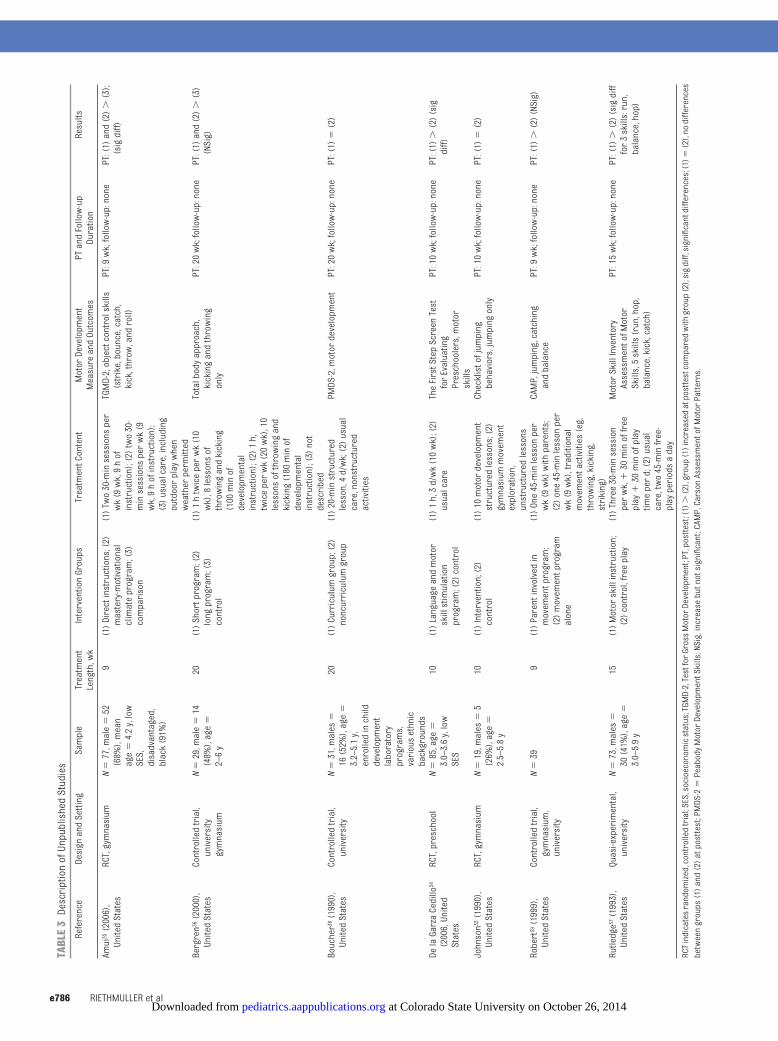
TABLE3DescriptionofUnpublishedStudies
Reference
DesignandSetting
Sample
Treatment
Length,wk
InterventionGroups
TreatmentContent
MotorDevelopment
MeasureandOutcomes
PTandFollow-up
Duration
Results
Amui35(2006),
UnitedStates
RCT,gymnasium
N�77,male
�52
(68%),mean
age
�4.2y,low
SES,disadvantaged,
black(91%)
9(1)Directinstructions;(2)
mastery-motivational
climateprogram;(3)
comparison
(1)Two30-minsessionsper
wk(9wk,9hof
instruction);(2)two30-
minsessionsperwk(9
wk,9hofinstruction);
(3)usualcare,including
outdoorplaywhen
weatherpermitted
TGMD-2;objectcontrolskills
(strike,bounce,catch,
kick,throw,androll)
PT:9wk;follow-up:none
PT:(1)and(2)�(3);
(sigdiff)
Bergren36(2000),
UnitedStates
Controlledtrial,
university
gymnasium
N�29,male
�14
(48%),age
�2–6y
20(1)Shortprogram;(2)
longprogram;(3)
control
(1)1htwiceperwk(10
wk),8lessonsof
throwingandkicking
(100minof
developmental
instruction);(2)1h,
twiceperwk(20wk),10
lessonsofthrowingand
kicking(180minof
developmental
instruction);(3)not
described
Totalbodyapproach,
kickingandthrowing
only
PT:20wk;follow-up:none
PT:(1)and(2)�(3)
(NSig)
Boucher38(1990),
UnitedStates
Controlledtrial,
university
N�31,males
�16(52%),age
�3.2–5.1y,
enrolledinchild
development
laboratory
programs,
variousethnic
backgrounds
20(1)Curriculumgroup;(2)
noncurriculumgroup
(1)20-minstructured
lesson,4d/wk;(2)usual
care,nonstructured
activities
PMDS-2,motordevelopmentPT:20wk;follow-up:none
PT:(1)
�(2)
DelaGarzaCedillo34
(2006,United
States
RCT,preschool
N�85,age
�3.0–3.6y,low
SES
10(1)Languageandmotor
skillstimulation
program;(2)control
(1)1h,3d/wk(10wk);(2)
usualcare
TheFirstStepScreenTest
forEvaluating
Preschoolers,motor
skills
PT:10wk;follow-up:none
PT:(1)
�(2)(sig
diff)
Johnson33(1990),
UnitedStates
RCT,gymnasium
N�19,males
�5
(26%),age
�2.5–5.8y
10(1)Intervention;(2)
control
(1)10motordevelopment
structuredlessons;(2)
gymnasiummovement
exploration,
unstructuredlessons
Checklistofjumping
behaviors,jumpingonly
PT:10wk;follow-up:none
PT:(1)
�(2)
Robert39(1999),
UnitedStates
Controlledtrial,
gymnasium,
university
N�39
9(1)Parentinvolvedin
movementprogram;
(2)movementprogram
alone
(1)One45-minlessonper
wk(9wk)withparents;
(2)one45-minlessonper
wk(9wk),traditional
movementactivities(eg,
throwing,kicking,
striking)
CAMP,jumping,catching
andbalance
PT:9wk;follow-up:none
PT:(1)
�(2)(NSig)
Rutledge37(1993),
UnitedStates
Quasi-experimental,
university
N�73,males
�30(41%),age
�3.0–5.9y
15(1)Motorskillinstruction;
(2)control,freeplay
(1)Three30-minsession
perwk,
�30minoffree
play
�30minofplay
timeperd;(2)usual
care,two45-minfree-
playperiodsaday
MotorSkillInventory
AssessmentofMotor
Skills,5skills(run,hop,
balance,kick,catch)
PT:15wk;follow-up:none
PT:(1)
�(2)(sigdiff
for3skills:run,
balance,hop)
RCTindicatesrandomized,controlledtrial;SES,socioeconomicstatus;TGMD-2,TestforGrossMotorDevelopment;PT,posttest;(1)�(2),group(1)increasedatposttestcomparedwithgroup(2);sigdiff,significantdifferences;(1)
�(2),nodifferences
betweengroups(1)and(2)atposttest;PMDS-2
�PeabodyMotorDevelopmentSkills;NSig,increasebutnotsignificant;CAMP,CarsonAssessmentofMotorPatterns.
e786 RIETHMULLER et al at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from

struction. Only 2 studies were �20weeks.24,25 Reilly et al24 conducted a 24-week (3 times per week) randomized,controlled trial aimed at preventingobesity through increasing physicalactivity and fundamental movementskills in 36 United Kingdom nurseriesand followed up participants for 12months. Motor development was a sec-ondary outcome. Vanesanou and Kam-bas25 implemented a 20-week (twiceper week) controlled trial, focusing ontraditional Greek dances. Follow-updata were collected at the conclusionof the intervention only (20 weeks).Motor development was the primaryoutcome for this study.
All except 1 of the published studies31
clearly described implementation pro-cedures. For 3 (30%) studies, the pri-mary researcher was responsible forintervention delivery26,27,29; for 2 ofthese 3 studies, researchers workedclosely with setting staff to ensure ef-fective and appropriate implementa-tion. University undergraduate stu-dents who were enrolled in physicaleducation classes were involved inprogram implementation for 2 (20%)studies.28,30
Only 20% of studies involved par-ents.24,32 In the controlled trial by Ham-ilton et al,32 parents delivered the in-tervention (16 sessions, each �45minutes) in the presence of the pri-mary researcher. Parents arrived 15minutes before the sessions and dis-cussed elements of the pending ses-sion with the primary researcher, anda visual demonstration of the key com-ponents was also provided. Parentswere required to attend every sessionand stay for the entire length of thesession. In contrast, the study by Reillyet al24 indirectly involved parents. Par-ents were provided with a resourcepack, which detailed physical activitiesin which children participated in thechild care setting and information onincreasing physical activity participa-
tion in the home environment, and 2health education leaflets, which fo-cused on the benefits of physical activ-ity. Both studies were effective in im-proving motor development.
Efficacy
Nine (90%) studies were efficacious inimproving motor development; 8 ofthese reported statistically significantfindings. Improvements in motor de-velopment were documented byConnor-Kuntz and Drummer26; how-ever, results were not statistically sig-nificant. Of the 2 studies that includedpostintervention follow-up measures,1 did not measure motor developmentat the 12-month follow-up24 and theother reported no differences betweenthe intervention group and the controlgroup at 3-month follow-up.26 Morethan half (60%) of the published stud-ies reported results separately forboth boys and girls.24–28,30
Alignment With CONSORT and TRENDStatements
Although only 1 study closely alignedwith either statement,24 all studies diddescribe participants and the inter-vention and half (50%) reported somecomponents of participant flow (eg, in-tervention exposure, reported as at-tendance rates) and 3 (30%) detailedretention rates.24,26,30 Connor-Kuntz andDrummer26 and Ignico30 retained allparticipants at postintervention, andIgnico30 retained 83% at 3-monthfollow-up. Reilly et al24 retained�90%of participants at both 6- and 12-monthfollow-ups.
Unpublished Articles
Table 3 summarizes the information inthis section.
Design
Two (29%) of the 7 unpublished studieswere randomized, controlled trials,33,34
both of which randomly assigned par-ticipants at the individual level. Two
studies randomly assigned partici-pants to 3 groups (2 treatment groupsand a control group).35,36 Two (29%) ofthe studies were implemented at apreschool34,37; all other studies wereimplemented off-site, at either a uni-versity38 or gymnasium.33,35,36,39
Methodologic Quality
Agreement was 80% on the 70 items (7unpublished articles � 10 items usedto assess methodologic quality foreach article; � � 0.57). Unlike the pub-lished articles, 2 (29%) of the unpub-lished controlled trials had high meth-odologic quality.35,38 Neither of therandomized, controlled trials had highmethodologic quality.33,34 Similar to thepublished trials, few items were con-sistently present, the exceptions beingthat a validated instrument was usedto measure motor development (71%),the unit of analysis was individual(86%), and the time of assessments atbaseline and follow-up were compara-ble between the intervention and thecontrol groups (86%). None of the un-published studies used intention-to-treat analysis or followed participantsfor �6 months, with the longestfollow-up period being 20 weeks.36,38
Intervention Components
The average sample size was�50 par-ticipants. Four studies had�50 partic-ipants,33,36,38,39 and none had�100. Theintervention length ranged from 9 to20 weeks, and the amount of instruc-tional hours ranged from �7 to 40hours. The hours of instruction werenot detailed for 1 study.33
The primary researcher or universityundergraduate students, trained bythe primary researcher, implementedall studies except 1.34 De la Garza Ce-dilli34 implemented a randomized, con-trolled trial that involved 85 partici-pants. Participants were randomlyassigned to a cognitive, language, mo-tor skills stimulation class (interven-tion) or usual care (control). The inter-
REVIEW ARTICLES
PEDIATRICS Volume 124, Number 4, October 2009 e787 at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from

vention was delivered triweekly by aclassroom teacher andwith the help ofan assistant. The teacher was trainedin the program content before thecommencement of the intervention.The researcher attended some of thesessions but was not regularlypresent. At follow-up, no significant dif-ferences in motor development werereported.
One (14%) study involved parents.39
Robert39 implemented a controlledtrial involving 39 dyads, each consist-ing of 1 preschool-aged child and 1parent. Participants were allocated toeither a parent-led movement pro-gram (intervention) or a student-ledmovement program (usual care, con-trol). Parents and children attended a45-minute session each week for 9weeks. In each session, parents wereencouraged to be the primary teacherof motor skills and movement con-cepts and were responsible for in-structing their child in the correct per-formance of the skills. Universitystudents who were trained in the pro-gram content were also present ateach session to answer questionsfrom parents or to modify parental in-structions to ensure that they werecorrectly delivered. Although not sta-tistically significant, differences in mo-tor development were reported atfollow-up between the 2 groups.
Efficacy
Most (71%) studies reported improve-ment in motor skills for the interven-tion group at follow-up; however, only 2reported statistically significant differ-ences: 1 controlled trial35 and 1 ran-domized, controlled trial.34 Three stud-ies reported results for both boys andgirls.35,36,38
Alignment With CONSORT and TRENDStatements
None of the unpublished studiesaligned strongly with the statements.Similar to the published studies, 4 re-
ported intervention exposure (eg, at-tendance rates)33,34,37,39 and 3 reportedretention rates.33,34,38 In the controlledtrial by Boucher,38 6 (14%) participantswithdrew from the program after pre-test, and another 2 (5%) withdrew be-cause they could not maintain their as-signed conditions for the duration ofthe study. Johnson33 and De la GarzaCedilli34 retained�70% of control par-ticipants (75% and 80%, respectively)and�80% of intervention participants(83% and 86%, respectively).
DISCUSSION
To the best of our knowledge, this isthe first systematic review to focus oninterventions to improve motor devel-opment in preschool-aged children. Ithighlights the limited quantity andquality of interventions and the dearthof evidence available in this importantarea. Although conclusive evidence forsuccessful interventions remains un-known, several important recommen-dations for future research and prac-tice can be suggested. Seventeenstudies, both published and unpub-lished, were included to expand thebreadth of the review.
Design
In both published and unpublishedstudies, there were more controlledtrials than randomized, controlled tri-als; however, controlled trials weresubstantially more prominent in theunpublished studies. The fact that allunpublished studies were retrieved aspostgraduate theses, which are typi-cally restricted by budget and time,may explain the high percentage ofcontrolled trials. Although this is un-derstandable, randomization is nodoubt important, because it minimizesbias during and after assignment oftreatments and also prevents con-founding biases.20
Overall, 65% of studies were imple-mented in a child care setting (nurser-
ies, elementary schools, and pre-schools), 60% of which were effective. Inolder children, physical activity interven-tions delivered in a variety of settingshave generally been effective18,40; how-ever, in young children, we hypothesizethat the setting in which the interventionis delivered may be highly influential inhaving an impact on outcomes.
Methodologic Quality
Of the 17 studies reviewed, �20% hadhigh methodologic quality. This is con-cerning considering that only 5 of the 10items for controlled trials and 6 of the 10items for the randomized trials wereneeded for a study to be categorized ashaving high methodologic quality. Fur-thermore, although the criteria used toassess methodologic quality have beenused in several other large systematicreviews18,41 and are considered a robustchecklist, they are not exhaustive. For ex-ample, it isunknownwhether thesestud-ies were adequately powered for statis-tical analysis. If additional items hadbeen included, then the methodologicqualitymay have been even lower. Sevenof the 10 items used to assess method-ologic quality were consistently missing.We suggest that results that are re-ported frommethodologically poor stud-ies be interpreted with caution, becausepotentially fatal flaws within a studymethod may mask, overinflate, or biasfindings; however, we acknowledge thatthe criteria used to measure quality areextremely specific. For example, 1 pointwas awarded when the study comparedgroups at baseline on 3 key characteris-tics (age, gender, and at least 1 relevantoutcome). When only 2 of these werepresent, a point was not awarded. De-spite the specificity of the methodologicquality criteria, we suggest that it isa helpful tool to ensure transparentreporting.
Intervention Components
Intervention components varied con-siderably for all studies. Sample sizes
e788 RIETHMULLER et al at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from

were more diverse for published stud-ies (range: 24–545), compared withunpublished studies (range: 19–85).Recruiting whole groups or child carecenters may be a beneficial mecha-nism of maximizing sample size to al-low appropriate statistical analyses.
Studies were on average 12 weeks induration and incorporated�1 hour ofinstruction per week. For older chil-dren, longer and more intense physi-cal activity interventions have beenrecommended.42,43 This may also betrue for interventions that targetyoung children; however, their re-duced cognitive capacity and shorterconcentration levels need to be con-sidered. Although it is not knownwhether longer and more intensephysical activity interventions thattarget young children are beneficial,it is clear that longer follow-up peri-ods are advisable.18,39
Setting staff (eg, teachers) deliveredthe intervention in only 5 of 17 studiesreviewed. There are several advan-tages to having setting staff deliver in-terventions: (1) maximizing potentialsustainability of the program; (2) min-imizing cost associated with imple-mentation; and (3) enhancing partici-pation levels. As suggested already,young children are more likely to bephysically active when they have posi-tive interactions with their teacherand peers and are in a better re-sourced play environment.44 Althoughthese are advantages, it is importantto note that successful implementa-tion requires substantial additional re-sponsibilities for staff, adding to theiralready crowded work schedules. Fur-thermore, we suggest, on the basis ofour own research, that staff may lackconfidence in delivering physical activ-ity interventions, particularly thosethat focus on motor development andmay require substantial training andguidance.45 Using a combined or part-nership approach, which has been
shown to be beneficial in interventionsthat target older children,46 may behelpful. This approach, which involvesresearchers and setting staff workingtogether, distributes responsibility be-tween key stakeholders, minimizesburden, and offers a forum of supportfor teachers who may not be confidentin delivering motor development phys-ical activity interventions.
Current recommendations for chil-dren who are aged 0 to 5 years empha-size the critical role that parents playin providing opportunities, encourage-ment, and support for physical activi-ty.14,15,47,48 Despite this, only 3 studies—�20%—involved parents. Althoughinvolving parents in interventions is lo-gistically difficult and often complex, itis imperative that they be involved tosome extent, even if it is indirectly as inthe study by Reilly et al.24 Using thehome environment to support whathappens in the intervention setting isessential to ensuring that instruc-tional messages received are consis-tent and reinforced, maximizing thesustainability of changes in outcomes.This notion has been supported inother recent reviews that focused onphysical activity among school chil-dren and adolescents.18,39,49
Efficacy
More than half of the interventionswere efficacious in significantly im-proving motor skills. Of the efficaciousinterventions, most were longerthan 8 weeks,* and the interventionwas implemented � times perweek.23,25,27,31,32,34,35,37 In addition, 5 ofthe successful studies were imple-mented by teachers and/or with theassistance of the researcher23–25,27,29;however, it is difficult to identify spe-cific intervention components thatcontributed to efficacy, because eachstudy was uniquely distinct in design,length, instructional time, and partici-
pants (eg, some studies included dis-advantaged children or those at riskfor disadvantage26). Efficacy may havebeen affected by a number of other fac-tors. First, although most studies useda validated measure of motor develop-ment, there were variations in thenumber of skills assessed and re-ported. Some studies assessed �3skills32,35,38; others assessed and re-ported only object-control skills (eg,strike, kick, catch, throw, bounce,roll),30,34 whereas others assessedboth object-control and locomotorskills.26,27 Second, the poor method-ologic quality of most studies possiblybiased the results away from the null.For example, it was difficult to ascer-tain who assessed the skills andwhether assessors were blind togroup allocation. Assessors who werenot blind to group allocation may havebiased results. Third, the demograph-ics of the facilitator (eg, gender, expe-rience, competence and confidence,training) may have influenced how theintervention was implemented andhow participants received the inter-vention. These details were absent foralmost all of the studies. Finally, thediffering underpinning theoreticalframework may have also affected theoutcomes. The theoretical frameworkwas reported only for 3 studies,24–26
and each of these reported a differentframework.
Alignment With the CONSORT andTREND Statements
The CONSORT21 and TREND22 statementsprovide guidelines for transparent re-porting of randomized, controlled tri-als and controlled trials, respectively.They have been developed to ensureaccurate reporting of external and in-ternal validity intervention compo-nents and to facilitate comparisons be-tween studies. The use of suchstatements in reporting data has im-proved the quality of studies in the*Refs 24, 25, 27–29, 31, 32, 34, 35, and 37.
REVIEW ARTICLES
PEDIATRICS Volume 124, Number 4, October 2009 e789 at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from

past several years22; however, as evi-denced by this review, in which only 1article was framed by using the CON-SORT statement and none by using theTREND statement, a large number ofarticles are not guided by these state-ments. Most studies provided some in-formation about participants, the in-terventions, and some aspects ofparticipant flow, including attendance(as a measure of intervention expo-sure) and retention rates; however,several other important CONSORT andTREND items were noticeably missing,such as blinding, randomization proce-dure, and baseline data. It is extremelydifficult to determine the true treat-ment effect and compare and contrastfindings when the CONSORT and TRENDstatements are not followed.
Strengths and Limitations
There are 3 main strengths to this re-view. First, published and unpublishedstudies were retrieved for a 20-yearperiod. Second, to allow comparisonbetween studies, we extracted exten-sive detailed information from eacharticle. Finally, the inclusion criteriawere kept broad, which allowed for theinclusion of studies from several coun-tries with varying designs.
Several limitations existed in the stud-ies reviewed. Only 2 (12%) recordedthe height and weight of the partici-pants, making it impossible to deter-mine whether these results are con-founded by growth.24,28 Quality controlmeasures were reported in only 2 ofthe studies,24,28 meaning that we wereunable to determine whether the deliv-ery of the interventions was consistentthroughout the individual studies. Fi-nally, although we were able to com-pare the studies broadly, we were notable to determine whether the motordevelopment component was differen-tially affected by the interventions. Di-rect comparison between quantitativedata was not possible because a di-
verse range (eg,�10) of motor devel-opment instruments were used. More-over, those that did use similarinstruments reported different out-comes (eg, some reported both loco-motor and object control scoresand/or only locomotor and object con-trol scores).
Recommendations for Practiceand Future Research
The development of motor skillsamong children may be an importantpredictor of later physical activity lev-els.8,50 School children with high levelsof motor development are more likelyto perform better on a number of phys-ical and psychological health out-comes. Children have the potential to beproficient in most fundamental move-ment skills by approximately the age of 6when they are given the encouragementand opportunity to learn and practice51;therefore, more high-quality interven-tions that target motor development arecritical for enhancing the habitual phys-ical activity of children. In light of this,several recommendations can be madefrom this review:
1. Physical activity motor skill inter-ventions should be implementedthrough a combined or partnershipapproach, thereby sharing the re-sponsibilities and burden betweenresearchers and setting staff.
2. Program facilitators should be cho-sen carefully because their experi-ence, competence, and confidenceare likely to influence children’sparticipation and enthusiasm forthe program. Similarly, the pro-gram setting should be consideredbefore implementation to ensurethat children will be comfortable intheir surroundings and with theequipment provided.
3. Parents should be involved, eitherdirectly or indirectly, in motor de-velopment interventions to comple-ment and support the translation of
knowledge and skills from the inter-vention setting to the home environ-ment. Parental involvement is a keyelement for habitual and lifelongmotor skill development.
4. Physical activity motor skill pro-grams should be underpinned by asound theoretical framework.
5. Sample size calculations should becompleted before recruitment toensure that appropriate statisticalanalysis can be conducted. Wholegroups or child care centers mayneed to be recruited to maximizesample size. If whole groups orchild care centers are recruited,then a cluster randomized, con-trolled trial would be required.
6. Physical activity intervention thatfocuses on motor skill outcomesshould be methodologically soundand follow guidelines detailed in theCONSORT21 or TREND22 statement,which will ensure transparent re-porting. Greater attention shouldbe given to longer interventions andfollow-up periods, randomizationprocedures, using assessors whoare blind to group allocation, usingvalidated measures of motor devel-opment, and comparing baselinecharacteristics.
CONCLUSIONS
During preschool years, it is importantto promote physical activity throughthe development of motor skills. Pedi-atricians and other health profession-als have an influential role in counsel-ing parents and caregivers on theirresponsibilities in this process.Through their advisory role for pre-schools and licensing boards and asan advocate for child health in theirlocal community, they can ensure thatyoung children are encouraged inthese settings to develop their motorskills through structured and unstruc-tured play.
e790 RIETHMULLER et al at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from
REFERENCES
1. Strong WB, Malina RM, Blimkie CJ, et al. Evidence based physical activity for school-age youth.J Pediatr. 2005;146(6):732–737
2. Malina RM. Fitness and performance: adult health and the culture of youth, new paradigms? In:Park RJ, Eckert MH, eds. New Possibilities, New Paradigms? Champaign, IL: Human Kinetics;1991:30–38 American Academy of Physical Education paper No. 24
3. Williams HG, Pfeiffer KA, O’Neill JR, et al. Motor skill performance and physical activity in preschoolchildren. Obesity (Silver Spring). 2008;16(6):1421–1426
4. Fisher A, Reilly JJ, Kelly LA, et al. Fundamental movement skills and habitual physical activity inyoung children. Med Sci Sports Exerc. 2005;37(4):684–688
5. Trevlas E, Matsouka O, Zachopoulou E. Relationship between playfulness and motor creativity inpreschool children. Early Child Dev Care. 2003;173(5):535–543
6. Okely AD, Booth ML. Mastery of fundamental movement skills among children in New South Wales:prevalence and socio-demographic distribution. J Sci Med Sport. 2004;7(3):358–372
7. Branta C, Haubenstricker J, Seefeldt V. Age change in motor in motor skills during childhood andadolescence. Exerc Sport Sci Rev. 1984;12:467–520
8. McKenzie TL, Sallis JF, Broyles SL, et al. Childhood movement skills: predictors of physical activityin Anglo American and Mexican American adolescents. Res Q Exerc Sport. 2002;73(3):238–244
9. Okely AD, Booth ML, Chey T. Relationships between body composition and fundamental movementskills among children and adolescents. Res Q Exerc Sport. 2004;75(3):238–248
10. Ulrich BD. Perceptions of physical competence, motor competence and participation in organizedsport: their interrelationships in young children. Res Q Exerc Sport. 1987;58(1):57–67
11. Okely AD, Booth ML, Patterson JW. Relationship of cardiorespiratory endurance to fundamentalmovement skill proficiency among adolescents. Pediatr Exerc Sci. 2001;13(4):380–391
12. Wrotniak BH, Epstein LH, Dorn JM, Jones KE, Kondilis VA. The relationship between motor profi-ciency and physical activity in children. Pediatrics. 2006;118(6). Available at: www.pediatrics.org/cgi/content/full/118/6/e17585
13. Okely AD, BoothML, Patterson JW. Relationship of physical activity to fundamentalmovement skillsamong adolescents. Med Sci Sports Exerc. 2001;33(11):1899–1904
14. National Association for Sport and Physical Education. Active Start: A Statement of PhysicalActivity Guidelines for Children Birth to Five Years. Reston, VA: NASPE Publications; 2002
15. Timmons BW, Naylor PJ, Pfeiffer KA. Physical activity for preschool children: how much and how?Can J Public Health. 2007;98(suppl 2):S122–S134
16. Baranek GT. Efficacy of sensory and motor interventions for children with autism. J Autism DevDisord. 2002;32(5):397–422
17. Parette HP, Hourcade JJ. A review of therapeutic intervention research on gross and fine motorprogress in young children with cerebral palsy. Am J Occup Ther. 1984;38(7):462–468
18. Sachdev HPS, Gera T, Nestel P. Effect of iron supplementation on mental and motor developmentin children: systematic review of randomised controlled trials. Public Health Nutr. 2005;8(2):117–132
19. Van Sluijs EM, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity inchildren and adolescents: systematic review of controlled trials. BMJ. 2007;335(7622):703
20. Alderson P, Green S, Higgins JP, eds. Assessment of study quality [Cochrane Review] In: TheCochrane Library. Issue 1. Chichester, United Kingdom: John Wiley & Sons Ltd. Update Software;2005
21. Altman DG, Schulz KF, Moher D, et al. The revised CONSORT statement for reporting randomizedtrials: explanation and elaboration. Ann Intern Med. 2001;134(8):663–694
22. Des Jarlais DC, Lyles C, Crepaz N. Improving the reporting quality of nonrandomized evaluations pfbehavioural and public health interventions: the TREND statement. Am J Public Health. 2004;94(3):361–366
23. Wang J. A study on gross motor skills of preschool children. J Res Child Ed. 2004;19(fall):32–42
24. Reilly JJ, Kelly L, Montgomery C, et al. Physical activity to prevent obesity in young children: clusterrandomized controlled trial. BMJ. 2006;333(7577):1041–1046
25. Swabey KJ, Yeo SM. The effect of an adapted version of a structured motor program on kinder-garten children’s perceptual motor skills. In: Proceedings From Key Into Life: The 21st BiennialNational/International ACHPER Conference. Adelaide, South Australia: ACHPER; 1998:172–174
26. Connor-Kuntz FJ, Drummer GM. Teaching across the curriculum: language-enriched physicaleducation for preschool children. Adapt Phys Activ Q. 1996;13(3):302–315
27. Goodway J, Crowe H, Ward P. Effects of motor skill instruction on fundamental motor skill devel-opment. Adapt Phys Activ Q. 2003;20(3):298–314
REVIEW ARTICLES
PEDIATRICS Volume 124, Number 4, October 2009 e791 at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from

28. Butterfield SA, van derMars H. The effects of a performance based curriculum on the grossmotordevelopment of preschool children during teacher training: a pilot study. Int J Phys Ed. 1988;25(3):20–25
29. Goodway J, Branta CF. Influence of a motor skill intervention on fundamental motor skill develop-ment of disadvantaged preschool children. Res Q Exerc Sport. 2003;74(1):36–48
30. Ignico AA. Effects of a competency-based instruction on kindergarten children’s gross motordevelopment. Phys Educ. 1991;48(4):188–199
31. Venetsanou F, Kambas A. How can a traditional Greek dances programme affect the motor profi-ciency of pre-school children? Res Dance Ed. 2004;5(2):127–138
32. Hamilton M, Goodway J, Haubenstricker J. Parent-assisted instruction in a motor skill programfor at-risk preschool children. Adapt Phys Activ Q. 1999;16(4):415–426
33. Johnson LG. The Effect of Intervention on the Jumping Behavior of Preschool Children [doctoralthesis]. Alberta, Ontario, Canada: University of Alberta; 1990
34. De la Garza Cedilli G. The Effect of a Cognitive, Language, Motor Skill Stimulation Program on theCognitive Language and Motor Skills of Children in Childcare Centres [doctoral thesis]. Houston,TX: University of Houston; 2006
35. Amui HN. The Effect of Two Instructional Approaches on the Object Control Skills of ChildrenConsidered Disadvantaged [doctoral thesis]. Columbus, OH: Ohio State University; 2006
36. Bergen M. The Effects of a Motor Development Program on Preschool Children Motor Skills[doctoral thesis]. Dekalb, IL: University of Northern Illinois; 2000
37. Rutledge CD. The Level of Motor Skill Development of Preschool Children Provided a PhysicalEducation Program and Preschool Children ProvidedWith Free Play [doctoral thesis]. Greeley, CO:University of Northern Colorado; 1993
38. Boucher BH. Preschool Children’s Motor Development and Perceived Competence [doctoral the-sis]. Corvallis, OR: Oregon State University; 1990
39. Robert DL. The Effects of Preschool Movement Program on Motor Skill Acquisition, MovementConcept Formation and Movement Practice Behavior [doctoral thesis]. Morgantown, WV: Univer-sity of West Virginia; 1999
40. Salmon J, Booth ML, Phongsavan P, Murphy N, Timperio A. Promoting physical activity participa-tion among children and adolescents. Epidemiol Rev. 2007;29:144–159
41. Summerbell CD, Waters E, Edmunds LD, Kelly S, Brown T, Campbell KJ. Interventions for preventingobesity in children. Cochrane Database Syst Rev. 2005;(3):CD001871
42. Weintraub DL, Tirumalai CE, Hayel F, Fujimoto M, Fulton JE, Robinson TN. Team sports for over-weight children: the Stanford Sports to Prevent Obesity Randomized Trail (SPORT). Arch PediatrAdolesc Med. 2008;162(3):232–237
43. Webber LS, Catellier DJ, Lytle LA, et al. Promoting physical activity in middle school girls: Trial ofActivity for Adolescent Girls. Am J Prev Med. 2008;34(3):173–184
44. Dowda M, Pate RR, Trost SG, Almeida MJ, Sirard JR. Influences of preschool policies and practiceson children’s physical activity. J Community Health. 2004;29(3):183–196
45. Riethmuller A, McKeen K, Okely AD, Bell AC, van Hewerden L, Sanigorski AM. Developing an activeplay resource for a range of Australian early childhood settings: formative findings and recom-mendations. Aust J Early Child. 2009;31:43–52
46. Neumark-Sztainer D, Story M, Hannan PJ, Rex J. New Moves: a school-based obesity preventionprogram for adolescent girls. Prev Med. 2003;37(1):41–51
47. American Academy of Pediatrics. Council on Sports Medicine and Fitness. Fitness, activity, andsports participation in the preschool child. Pediatrics. 1992;90(6):1002–1004
48. Hagan JF, Shaw JS, Duncan PM, eds. Bright Futures: Guidelines for Health Supervision of Infants,Children and Adolescents. 3rd ed. Elk Grove Village, IL: American Academy of Pediatrics; 2008
49. Sallis JF, Prochaska JJ, Taylor WC. A review of correlates of physical activity of children andadolescents. Med Sci Sports Exerc. 2000;32(5):963–975
50. Barnett LM, van Beurden E, Morgan PJ, Brooks LO, Beard JR. Childhood motor skill proficiency asa predictor of adolescent physical activity. J Adolesc Health. 2009;44(3):252–259
51. Gallahue DL, Ozmun JC. Understanding Motor Development: Infants, Children, Adolescents, Adults.6th ed. New York, NY: McGraw-Hill; 2006
e792 RIETHMULLER et al at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2009-0333; originally published online September 7, 2009; 2009;124;e782Pediatrics
Annaleise M. Riethmuller, Rachel A. Jones and Anthony D. OkelySystematic Review
Efficacy of Interventions to Improve Motor Development in Young Children: A
ServicesUpdated Information &
tmlhttp://pediatrics.aappublications.org/content/124/4/e782.full.hincluding high resolution figures, can be found at:
References
tml#ref-list-1http://pediatrics.aappublications.org/content/124/4/e782.full.hat:This article cites 36 articles, 4 of which can be accessed free
Citations
tml#related-urlshttp://pediatrics.aappublications.org/content/124/4/e782.full.hThis article has been cited by 4 HighWire-hosted articles:
Subspecialty Collections
_subhttp://pediatrics.aappublications.org/cgi/collection/neurologyNeurology
velopment_milestones_subhttp://pediatrics.aappublications.org/cgi/collection/growth:deGrowth/Development Milestones
nt:behavioral_issues_subhttp://pediatrics.aappublications.org/cgi/collection/developmeDevelopment/Behavioral Issuesthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Colorado State University on October 26, 2014pediatrics.aappublications.orgDownloaded from