Embed Size (px)
Citation preview

KNOWLEDGE, E
UNIVERSITY OF CALABAR TEACHING HOSPITAL
FACULTY OF HEALTH SCIENCES AND TECHNOLOGY
Ebere Omeje
EFIONG, MERCY. B. PG/M.Sc/08/47747
KNOWLEDGE, ATTITUDE AND PRACTICE OF CARE OF THE ELDERLY PATIENTS AMONG HEALTH WORKERS IN
UNIVERSITY OF CALABAR TEACHING HOSPITAL CROSS RIVER STATE, NIGERIA.
FACULTY OF HEALTH SCIENCES AND TECHNOLOGY
DEPARTMENT OF NURSING SCIENCES
Ebere Omeje Digitally Signed by: Content manager’s
DN : CN = Webmaster’s name
O= University of Nigeria, Nsukka
OU = Innovation Centre
1
AND PRACTICE OF CARE OF THE LDERLY PATIENTS AMONG HEALTH WORKERS IN
UNIVERSITY OF CALABAR TEACHING HOSPITAL CALABAR,
FACULTY OF HEALTH SCIENCES AND TECHNOLOGY
DEPARTMENT OF NURSING SCIENCES
: Content manager’s Name
Webmaster’s name
a, Nsukka

2
KNOWLEDGE, ATTITUDE AND PRACTICE OF CARE OF THE
ELDERLY PATIENTS AMONG HEALTH WORKERS IN UNIVERSITY OF CALABAR TEACHING HOSPITAL
CALABAR, CROSS RIVER STATE, NIGERIA.
BY
EFIONG, MERCY. B. PG/M.Sc/08/47747
DEPARTMENT OF NURSING SCIENCES
FACULTY OF HEALTH SCIENCES AND TECHNOLOGY UNIVERSITY OF NIGERIA
ENUGU CAMPUS
JULY, 2015.

3
TITLE PAGE KNOWLEDGE, ATTITUDE AND PRACTICE OF CARE OF THE
ELDERLY PATIENTS AMONG HEALTH WORKERS IN UNIVERSITY OF CALABAR TEACHING HOSPITAL
CALABAR, CROSS RIVER STATE, NIGERIA.
BY
EFIONG, MERCY B. PG/M.Sc/08/47747
M.SC DISSERTATION
PRESENTED TO THE DEPARTMENT OF NURSING SCIENCES FACULTY OF HEALTH SCIENCES AND TECHNOLOGY
UNIVERSITY OF NIGERIA, ENUGU CAMPUS
IN PARTIAL FULFILLMENT OF THE REQUIREMENT FOR THE AWARD OF MASTERS OF SCIENCE DEGREE IN NURSING
SUPERVISOR: DR (MRS) I. O. EHIEMERE
JULY, 2015.

4
APPROVAL
This dissertation has been approved for the award of Master of Science Degree in Nursing in the
Department of Nursing Sciences, Faculty of Health Sciences and Technology, University of
Nigeria, Enugu Campus.
By
………………………………………….. …………………………… Dr.(Mrs.) I. O. Ehiemere Date Supervisor ………………………………………. …………………………… Dr. A. C. Nwaneri Date Head, Department of Nursing Science ………………………………………… …………………………… External Examiner Date …………………………………………. …………………………… Prof. Obinna Onwujekwe Date Dean, FHST UNEC

5
CERTIFICATION
I Efiong, Mercy Bassey, Reg. No. PG/MSC/08/47747 hereby certifies that this dissertation is my
original work and that either the whole or part of it has been submitted to this University or any
other Institution for the award of Masters of Science degree.
……………………………………….. …………………………… EFIONG, MERCY BASSEY DATE ………………………………………… …………………………….. DR. (MRS) I.O.EHIEMERE DATE

6
DEDICATION
This work is dedicated to the ALMIGHTY GOD for the grace of longevity on my family
lineage.
My father passed on at the age of ninety five while his other siblings died between 85 to 93 years
of age. To God Be The Glory.

7
ACKNOWLEDGEMENTS
My greatest appreciation goes to the Almighty God, the most merciful, compassionate and
gracious for enabling me to conduct this research study.
My sincere appreciation to my diligent Supervisor Dr. (Mrs.) I. O. Ehiemere for her support,
constructive criticisms and assistance throughout this endeavor, she helped me establish realistic
goals for completing each phase of this thesis and proved to be a valuable proponent of this
research study. I am eternally grateful for her guidance, support and encouragement, throughout
this exercise. It was an honour to work with an expert like her. I remain grateful to the Head of
Nursing Science Department Dr. A. C. Nwaneri and the entire lecturers in Nursing Science
Department for their own contributions and intelligent corrections.
Special appreciation goes to my husband, children and family members for their support, Co-
operation and encouragement.
Special thanks to Mrs. Lilian Eyam, Diana John and Agbor Oben for helping make this a
scientifically sound, clear and readable research. A special expression goes to my friends
MaEfiom, Gupo, Helen, Salama, Afi Ekpenyong and Afi Eduwem for their suggestions that
contributed so much to this research
Finally, I am grateful to the research participants, Nurses, Doctors, Physiotherapists and Dentists
in University of Calabar Teaching Hospital, Calabar. If they had not shared their views, this
research would not have been complete.

8
TABLE OF CONTENTS
Title page i
Approval page ii
Certification Page iii
Dedication iv
Acknowledgement v
Table of Contents vi
List of Tables viii
List of Appendices ix
Abstract x
CHAPTER ONE: INTRODUCTION
Background to the Study 1
Statement of the Problem 3
Purpose of Study 4
Specific Objectives of the Study 4
Research Questions 4
Significance of the Study 5
Scope of the Study 5
Operational Definition of Terms used in this Study 6
CHAPTER TWO
: LITERATURE REVIEW
Conceptual Review 7
Theoretical Framework 25
Empirical Review 28
Summary of the Literature Review 33
CHAPTER THREE: RESEARCH METHOD
Research Design 34
Area of Study 34
Population of the Study 35
The Sample size for the Study 35
Sampling Procedure 35

9
Method of Data Collection 36
Validity of the Instrument 37
Reliability of the Instrument 37
Ethical Consideration 37
Procedure for Data Collection 38
Method of Data Analysis 38
CHAPTER FOUR: PRESENTATION OF RESULTS
CHAPTER FIVE: DISCUSSION, CONCLUSION AND RECOMMENDA TION
Discussion of the Findings 48
Implication of Findings to Nursing 51
Limitation of the Study 51
Summary 52
Conclusion 53
Recommendations 53
Suggestion for further studies 54
References
Appendices
Questionnaire

10
LIST OF TABLES
Table 1: Socio-Demographic Characteristics of the Respondents …………………… 39
Table 2a: Level of Knowledge of Health Workers towards the care of the Elderly …… 40
Table 2b: Categorization of knowledge Score …………………………………………. 41
Table 2c: Proportion of health workers and their level of knowledge on the care of the elderly patients ----------------------------------------------------------- 41
Table 3: Attitude of Health Workers towards the Care of the Elderly ………………… 42
Table 4a: Health Workers Practice of Care of the Elderly …………………..………….. 43
Table 4b: Categorization of Practice Score …………………………………………. 44
Table 4c: Proportion of health workers and their practice of care of the elderly patients 44
Table 5: Factors Influencing the Attitude of Health workers towards Care of the Elderly …45
Table 6a: Mean years of Experience of Health Workers and Attitude of care towards the Elderly ……………………………………………………… … 46
Table 6b: Years of Experience and Attitude of Health Workers 47
Table 6b Proportion of health workers with positive and negative altitude towards the care of the elderly patients. 47

11
LIST OF APPENDIXES
Appendix i: Sample Questionnaire
Appendix ii: Calculation of Sample size
Appendix iii: Informed Consent form
Appendix iv: Clearance before Seminar Presentation
Appendix va: Ministry of Health Ethical Approval
Appendix vb University of Calabar Teaching Hospital Ethical Approval
Appendix vi Clearance before Seminar Post Field
Appendix vii Calculation of Sample Size
Appendix viii Letter of Identification
Appendix ix Application for Permission to Collect Data
Appendix x: Letter of Introduction

12
ABSTRACT
With the global trend towards an increasing aging population, there is a corresponding increase in the health problems associated with elderly population especially in developing Countries including Nigeria. With this increase in the growth of the aging population, the number of people that will need health care will undoubtedly increase, which motivated this study. The study was aimed to assess the level of knowledge, attitude and practice of care of the elderly patients among health workers in University of Calabar Teaching Hospital, Calabar, Cross River State. The specific objective were to (i) determine the level of knowledge of the physical, emotional and social care of the elderly in the University of Calabar Teaching Hospital, Calabar (ii) determine the attitude of health workers in the care of the elderly, (iii) determine the health workers practices in the provision of care of the elderly, (iv) identify factors that influence the health workers attitude towards the elderly in University of Calabar Teaching Hospital, Calabar. The hypothesis for the study tested the association between years of experience of health workers and their attitude towards care of the elderly in UCTH. Calabar. The study adopted a cross sectional descriptive design. The population of the study was 1023 health workers, which was made up of 402 Doctors, 600 Nurses, 10 Dentists and 11 Physiotherapists that provided direct clinical care of elderly patients. The sample was calculated using Taro-Yamane (1967) simplified formula for finite population giving a sample of 461 health workers. The instrument for data collection was questionnaires, the reliability of the instrument was done using test retest method and a reliability co-efficient of 0.91 was obtained. The questionnaires had five sections, section A covered socio demographic data, section B, C, D consisted of items which explored level of knowledge. Attitude, practice and section E elicited information on factors influencing the care of the elderly. The completed questionnaire was coded and analyzed using E.P.I info-7. Descriptive statistics of percentage, mean, standard deviation were used for data analysis. The criterion mean of 2.5 was also used and results of the study revealed that 95% of the health workers had good knowledge of care of the elderly. Majority of the health workers had positive attitude above rating scale of 2.5. The health workers moderately practiced care of the elderly. The factors that positively influenced health workers attitude to the care of the elderly were years of experience, age and mental state of the elderly. There was significant association (P<0.05) between attitude of Health Workers and mean years of experience. Workers with less years of experience had negative attitude, while those with more years of experience had positive attitude, towards the care of the elderly. In conclusion, health care professionals need to have the right skills to manage a more demanding role in the future. In order to offer effective services for the elderly, a skilled workforce of health professionals is therefore very necessary. The study recommended that Geriatric Nursing content in the curriculum be strengthened and also geriatric wards be established in all general hospitals.

13
CHAPTER ONE
INTRODUCTION
Background to the Study
Ageing is the accumulation of changes in a person over time (Bowen and Atwood 2004).
It involves a multidimensional process of physical, psychological and social change. Some
dimensions of aging grow and expand over time, while others decline. Research shows that even
in late life, potentials exist for physical, mental and social growth and development (Papalia,
Sterns, Feldman, and Camp, 2002). It is not a disease; but phase of life where there is retrograde
biological process in growth and development which leads to decreased powers for survival and
adjustment. Aging is an important part of all human societies reflecting the biological changes
that occur and also reflecting cultural and societal convention.
An estimated 100,000 people worldwide die each day of age related causes (Aubrey de
Grey, 2007). According to National Population Commission (NPC, 2006), persons who are old
enough to receive pension who are between ages of 60-65 years are regarded as the elderly. The
elderly are classified by age into young old for those aged 60-74years, middle old for those aged
75-84years, old for those aged 85-94 years and oldest old for those 95years and above. (Barman,
Snyder, Kozier & Erb , 2008).
Care of the elderly is the fulfillment of the special needs and requirements that are unique to
senior citizens. It covers such services as assisted living, adult day care, long term care, nursing
homes, hospice care and home care. Elderly care emphasizes the social and personal
requirements of senior citizens who need some assistance with daily activities and health care,
but who desire to age with dignity. The care of the elderly is multidimensional and these include
physical, emotional, spiritual and social care (Ayres, 2008).

14
However, improvement in primary health care with focus on prevention of childhood diseases
through immunization did not highlight the care of the elderly which should be one of the
components of primary health care programme in most developing countries (Olise, 2011). A
cursory look at the implementation of Millennium Development Goals (MDGs) by the federal
government shows that there is little or no consideration of this very important segment of the
population – the elderly. Also most curricula for training Health Manpower in Nigeria do not
highlight the care of the elderly (Donatelle, 2011). Yet the population of this segment of the
society is increasing in developing countries with their special care needs. Traditionally, in
Nigeria elderly care has been the responsibility of family members and was provided within the
extended family system (Ting and Woo, 2009).But with modernization, elderly care is now being
provided by state or charitable institutions. This is attributable to decreasing family size, the
greater life expectancy of elderly people, the geographical dispersion of families, and the
tendency for women to be educated and work outside the home (Lee, 2009).
In most developing countries including Nigeria the population of the elderly is increasing
rapidly but the government does not seem to be making any major commitments to elderly
healthcare (Adio-Moses, 2001). The government is still assuming that families should take care
of their elderly without recognizing that the extended family system is at the verge of collapse.
Currently most families find it difficult to manage their own homes and face their challenges.
This is gradually leading to neglect and abuse of the elderly (Gubrium, 2002). Care of the elderly
requires adequate knowledge of the ageing process, nutrition and daily needs of the elderly. In
Nigeria, marginalization of the elderly especially in their care is a common episode
(Abdulraheem & Parakoyi, 2005). Those involved in the provision of health care have important
roles to play in programmes relating to elderly care especially in screening and detecting abuse.

15
Unfortunately doctors do not diagnose abuse because it is not part of their formal or professional
training hence does not feature in their list of differential diagnosis (Donatelle, 2011). The health
worker, according to Abdulrahem & Parakoyi (2005) plays major roles in determining and
implementing desirable standards of health care, acting as a professional in developing core of
professional knowledge and should have ability to impart same to others. They are often the
providers of services designed to maintain health and prevent illness. Research has also shown
that the quality of health care service provided to older population is strongly influenced by care
givers attitude towards older people (Gallaghar, Bennet & Halford, 2006). This underscores the
need to assess the knowledge, attitude and practice of care of the elderly among health workers
in University of Calabar, Calabar Cross River State.
Statement of the Problem
The population of the elderly in the world is increasing rapidly (United Nations, 2004)
and the rate of increase is higher in developing countries including Nigeria. Currently, Nigeria
has the highest number of the elderly people in Africa estimated to be about 5.6% of the Nigeria
population (NPC, 2008). With this increase in the growth of the aging population, the number of
people that will need health care will undoubtedly increase. Donatelle (2011) posited that in most
curricula for health professionals, little or nothing is indicated about the care of the elderly
showing absolute neglect in this area Mclafferly and Morrison (2004) stated also that most health
workers have very poor knowledge of mental health conditions which are common with the
elderly and as such health workers come to service with deep seated, negative, diluted and
superstitious belief about caring for the elderly. This lack of adequate knowledge and negative
attitude towards the care of the elderly may result in serious problems in our society in the near
future. In a recent study of the elderly in Ibadan by Oyetunde, Ojo & Ojewale (2013) show that

16
attitudinal relational gaps exist, resulting in negative patient outcome. From my clinical practice
in different hospitals in Calabar, frequent misunderstanding between elderly patients and health
care providers especially the young ones, was observed. Based on these, the researcher seeks to
find out the knowledge, attitude and practice of care of the elderly among health workers in the
only tertiary health facility in Calabar, University of Calabar Teaching hospital.
Purpose of the study
The purpose of the study is to determine the level of knowledge, attitude and practice of
care of the elderly among health workers in University of Calabar Teaching Hospital, Calabar,
Cross River State.
Objectives of the study
Specifically the objectives of the study include to:
1. determine the health workers level of knowledge of the physical, emotional and social
care of the elderly in University of Calabar Teaching Hospital ,Calabar, Cross River State
2. determine the attitude of the health workers towards the care of the elderly.
3. determine the health workers practices in the provision of care for the elderly.
4. identify the factors that influence health workers attitude of care towards the elderly in
University of Calabar Teaching Hospital, Calabar.
Research Questions
1. What is the level of knowledge of the care of the elderly among health workers in a tertiary
health facility in Calabar, Cross River State?
2. What is the attitude of health workers towards care of the elderly in a tertiary health facility
in Calabar?

17
3. What are the health workers practices in the provision of care of the elderly in a tertiary
health facility in Calabar, Cross River State?
4. What are the factors that influence health workers attitude of care towards the elderly?
Hypothesis.
1. There is no association between years of experience of health workers and their attitude
towards care of the elderly in UCTH, Calabar.
Significance of Study
The result will help to provide basic information for designing structures and
programmes for the care of the elderly in the community. It will also provide evidence based
information for health education on graceful ageing. It will serve as a reference material to other
researchers in the field of community health practice.
Findings of the study will help in showing the level of knowledge and attitude of the health
workers towards the care of the elderly and will help improve the decision making. The result
will also help in building up knowledge base on the care of the elderly patients. Improving data
base on elderly health nutrition and standard of living which will help for further research,
advocacy, policy dialogue and programming.
Scope of Study
The study focused on the level of knowledge, attitude and practice of the care of the
elderly among health workers in University of Calabar Teaching Hospital, Calabar. The study
was delimited to only health workers providing direct clinical care (hand on care to the elderly)
consisting of nurses, doctors, dentists and physiotherapists in University of Calabar Teaching
Hospital.

18
Operational Definition of Terms
Knowledge of physical care are expressing understanding of bed bath, skin care, oral hygiene,
feeding, elimination and ambulation.
Knowledge of Emotional care; refers to expressing attention, acceptance and love.
Knowledge of social care; means financial support and visitation by family members and friends
(co-workers, church member’s, social club, and neighbors).
Practice of physical care expressing competence in providing skin care, oral hygiene, feeding,
ambulation and elimination.
Attitude means health workers’ expression of cheerfulness, listening to patient’s complaints and
prompt attention, positive attitude while negative attitude means expression of harsh words, lack
of respect and “stone face”.
Health Workers refers only to Nurses, Doctors, Physiotherapists and dentists that are directly
involved in the clinical care of the elderly.
Elderly refers to people aged 60 years and above.

19
CHAPTER TWO
LITERATURE REVIEW
This chapter presents the review of literature related to the work, from books, Journals,
Abstracts, and internet materials, under the following subheadings:
Conceptual Review,(Concept of ageing, Biopsychosocial challenges of the care of the elderly,
Knowledge of care of the elderly amongst health workers, Attitude / practice of health workers
on the care of the elderly, Problems associated with the care of the elderly, Factors influencing
health workers practice of care towards the elderly), Theoretical Review, Empirical Review and
Summary of review.
Conceptual Review
Concept of Ageing
Aging is a universal phenomenon that is obvious as well as inevitable. Old age is a
significant stage in life and normally related to life expectancy of given area, hence the
conditions and the needs of the aged becomes imperative. Preparation for old age cannot be over
emphasized. Aging can be observed as a consistent pattern of change that every human being
undergoes, starting at a very slow rate at around age 30, and progressing at a more rapid rate
beyond age 65 (Olowookere, 2003). Aging is a sensitive and seriously regarded issue and it is a
process of becoming older. The aged in Nigeria are highly revered, respected and often held in
high esteem. The aged constitute a repository of wisdom and experiences.
The aged are often seen as the custodians of knowledge due to their experience in life.
The population of old people throughout the world is increasing at a very rapid rate (Population
Reference Bureau, 2011). The most rapid increase is taking place in the developing world with
Africa alone projected to have between 204 and 210 million old people by the year 2050. This

20
unprecedented rise in the number old people presents fundamental socio-economic difficulties
(Olaleye, 2011). Nigeria with a population of 140.8 million people (NPC 2006) is the most
populated nation in Africa and the ninth in the world (UN, 2005). Life expectancy at birth stands
at 57.6 years (NPC, 2008). The population growth rate (2000 – 2005) is 2.5% with 5.6% of the
total population aged 60 and above. As the most populous country in Africa, Nigeria currently
has the highest number of aged or elderly people in Africa Population Reference Bureau(PRB,
2011) with the largest population in Africa and the ninth in the world, it is estimated that by year
2025, the population of Nigeria aged 60 and above will constitute 6 percent of the entire
population as projected by (UN population Division, 2005)
Old age is not a disease; it is the phase of retrograde biological process in growth and
development which leads to decreased powers of survival and adjustment. The World Health
Organization has always designated as “Elderly” people aged 65 years and above. In 1980, the
United Nations defined 60 years as the age of transition of people. (U N 2004). Older people
make up an increasing proportion of the population in developed world and this demographic
transition also affects some developing countries. Generally older people are at increased risk of
disease, disability, social and financial deprivation compared to the younger generation in the
same population (National Council on Ageing and older people (NCAOP) , 2005). An increase
in the number of older people will lead to increased demands on health and support services
including aged care residential services and acute health service (Mccormacks, 2004).
Mcmurdo (2000) also stated that the elderly have reduced ability to generate resources;
they lack the basic needs that affect their health status. Where one finds well developed Maternal
and Child Health Services, a vacuum exists in the elderly health policy. Population growth
combined with ageing will mean that greater number of older people will need health and

21
community care services, more older people in the hospital mean more people with dementia
needing appropriate care. Varice (2010) indicated that society where the elderly population is
expanding and cultural values are changing, the needs of the elderly become increasing by
entwined with appropriate health care needs. Death of older people both in institutional settings
and the community have often been attributed to natural, accidental or undetermined causes
when in fact they were consequences of abusive or neglectful behavior. As long as older people
are devalued and marginalized by society they will suffer from loss of self identity and remain
highly susceptible to discrimination and all forms of abuse (Szucs, 2001)
The concept of aging is multifaceted. This is because its in-depth description or
explanation covers diverse areas of human development. There are chronological, biological,
psychological and social, functional dimensions of aging (Papalia, Feldman and Camp, 2002;
Hoyer and Roodin, 2003). The chronological dimension describes the number of years that have
slipped away since one’s birth while the biological explains the status of vital organs of the body
as an individual advances in age. The psychological dimension focuses on individuals’ ability to
adapt to environmental demands/challenges while social dimension sheds light on how an
individual conforms to written and unwritten norms, roles expected of him/her by the society in
which he/she operates. The functional dimension measures how effective an individual is in
physical and social environment when compared with other people within his/ her age bracket
(Hoyer and Rodin, 2003). The concept of aging to some scholars is not a single or one-way
process, Berger, Dev, Mutrie & Hannah (2005) posits that there are three distinct but interrelated
processes of ageing. These are primary, secondary and tertiary aging. The primary ageing
represents the inevitable age – related changes, which all human beings are expected to pass
through. The period is characterized by inability of human organism to replace damaged parts of

22
the body. The secondary aging involves all the age related changes, which are consequences of
individual and societal failure to eradicate unhealthy conditions. It is at this period that certain
diseases such as Cancer, diabetes, arthritis, visit the elderly. The tertiary ageing on the other
hand, deals with numerous losses or unpleasant experiences associated with old age. Most
developed world countries have accepted the chronological age of 65years as a definition of
‘elderly’ or older person, but like many westernized concepts, this does not become accustomed
to the situation in Africa, while this definition is somewhat arbitrary, it is associated with the age
at which one can begin to receive pension benefits. At the moment, there is no United Nations
standard numerical criterion, but the UN agreed cut –off is 60+ years to refer to the older
population (UN, 2004)
Bio-psychosocial challenges of the elderly in Nigeria
Physical changes
According to Berger Dev, Mutrie and Hannah (2005) the first sign of ageing begins with
the skin which becomes drier, thinner and has elastic wrinkles, visible blood vessels and pocket
of fat under the skin appear as irrefutable evidence of the passage of time. Merrill and verbrugge
(2001) also revealed that with time pockets of fat settle on various parts of the body most
noticeable around the abdomen, but also on the upper arms, the buttocks, eyelids and double
chin, bones become fragile and more easily broken and difficult to heal. The Muscles loose
power and become atrophy while joints stiffen or wear out, circulation slows down, blood
pressure rises and because the lungs hold less oxygen the aged has less energy, reaction to
stimuli is slower and there is less resistance to illness. There are difficulties to fall asleep and
remaining asleep and vision, hearing and sense of smell became less acute (Nur et al, 2009).
Disability significantly affects quality of life in old age though it is considered to be

23
consequences of the normal ageing process; they are often caused by chronic diseases which the
elderly are at risk (Szucs, 2001). There seems to be a problem with providing the appropriate
care for these disabilities for this segment of the population yet the population is growing rapidly
in both developed and developing countries (Vitalianie, Zhang and Scsarian, 2003).
Accessibility to Care
The lack of health care for senior citizens is a crucial problem with the assumption that
Provision of healthcare services has always been adequate. This assumption is wrong as recent
research has shown that Medical care is not easily accessible. This is because the geographical
distance to get to these services makes it difficult, if not impossible for many older people to
access, particularly in the rural areas (Nussbaum, 2003). Hence, their health needs still has to be
met by visiting traditional medical men and herbalists. At the family level care services provided
do not adequately meet the needs of the old persons. Diminishing economic power has hindered
the willing family members. However these changes demand that governments, the private
sector, nongovernmental organizations and the civil society in general be prepared to deal with
them, bearing in mind the special needs of the people.
Affordability
Nevertheless, most elderly persons cannot afford quality medical care. A survey of more
than 3,200 senior citizens found that many people would be prepared to pay for high quality
elderly care, while wanting a safety net for those who cannot afford to pay(O’ Neil, 2010).
Essy (2002)opines that old people are particularly disadvantaged due to lack of social security
especially in this part of the world, for their everyday social and economic needs. The care and
support by the family and community that were taken for granted in the past have stopped,
because of changes in the society associated with urbanization and development in general (Ting

24
and Woo, 2009). In some communities in Africa instead of relaxing and enjoying old age, the
senior citizens are obliged, once again, to take up the responsibility of caring for children and
young adults suffering from HIV/AIDs related problems or migrate. Apart from the children, old
people are the social group most vulnerable to the numerous ills facing Africa, poverty, food
insecurity, civil strife, armed conflict, violence and inadequate social welfare services.
Culture
According to Mullick (2005) the traditional African culture has ways of taking care of the
elderly. For example, their extended family and children are expected to provide for them and
young people in the immediate environment are supposed to help them run errands whether the
elder are their relative or not. These types of caring are fast becoming a thing of the past.
However, African family structure is changing, although the family is an institution which is not
disappearing, rather, families are responding and adapting to new conditions, while older persons
are adopting new roles within the families (Mullick, 2005). Harrision (2005) also observes that
family structures are changing and traditional patterns of care are no longer guaranteed.
Depression and Anxiety
According to Philips (2003) the elderly often have uniformed feelings that are ubiquitous,
such feeling include, mourning that results from loss of dear ones, guilt that emanates from
resurgence of past conflicts and regrets, depression and anxiety brought about by loneliness and
fear of death. Other major problems faced by the elderly are often from the mass media that are
supposed to be the custodian and promoters of successful and better aging. But they rather
portray them as being stereotypical, cantankerous, deteriorating, unproductive, slow, senile,
stubborn, and useless or irrelevant to the society. These negative portrayals do contribute to the
lower psychological performance of elderly in Africa where the family remains the most

25
important source of support for the old people (Moemeka 2001). Gubrium (2002) suggest that
sensory loss will make any elderly person to forget something that is immediate, but may
sometimes remember things in the far past. Most elderly are afraid to being hospitalized, for they
had already assumed hospital to be dying places (Lecovich, 2008). Humphries, Brugha and
Mcgee (2008) also observed that living patterns are changing as urbanization has resulted in
many elderly people living alone in rural areas. This occurs, when their children might have
migrated to the urban centre, in search for greener pasture. Economic pressure and changing
social values mean that many families are either unable or unwilling to care for the aged. The
contributions that elderly people make to the family are seldom acknowledged and programmes
designed to support families fail to take into account the valuable role that old people do play
(Abdulraheem and Parakoyi, 2005).
Poor Policy Implementation
National Centre for Protection of Older People (NCPOP), (2009) recommends that,
member states, ought to design, develop and implement practical, realistic and appropriate social
welfare strategies which will include the concerns of the people. Also they should develop
review and implement strategies, which emphasize traditional community support and care
mechanism for their elders. According to Essy (2002), member states as a matter of importance
should discourage the institutionalization of elderly people and retain the cultural respect from
them; encourage the emphasis of community based support such as kinship, extended family and
neighborhood support. Elderly people are abused by family and community members and are
accused of everything from witchcraft to preventing or causing too much rain for which they are
tortured and assaulted. Economically, they suffer, as their assets are stolen and financial
institutions refuse them credit and other services. Age based discrimination is pervasive and

26
prevents old people from accessing basic rights such as adequate health care and legal protection
(Olaleye, 2011)
Social and economic problems
Sociologically, the elderly are seen as the organizers of the society, and as people through
whom intergenerational beliefs and customs are transferred to the younger generations (Olaleye,
2011). Currently, social and economic Implications state that the lack of state provision of elder
care in Nigeria requires the family to provide the needs for the survival of the older people
(Lecovich, 2008). Family members provide food, shelter, clothing, drugs and other basic
necessities. Children now play the most important role of providing economic security in old
age. Older parents live in their adult children homes and receive care. On the other hand, they
support their children in taking care of their grandchildren, when they live in their own homes,
grandchildren or other relatives often live with them to give support such as washing clothes,
running errands, cooking meals and taking general care of the older people’s environment
(Lecovich, 2008). At the family level, care services provided do not adequately meet the needs of
the elderly person in Nigeria. Diminishing economic power has hindered the willing family
member’s capability to give. Priorities are given to the needs of the members of the nuclear
family – spouse and children at the expense of older family members, parents or grandparents.
Care provided by the family attempts to satisfy the needs of elderly persons. With the changing
social and economic configurations, elderly persons are most of the time left in the care of
strangers i.e. people who are not properly trained to be care givers given that many of them are
uneducated, young and frustrated. Adio-Moses (2001) suggests that inadequate preparation for
retirement or sudden retirement from previous lucrative job may lead to financial worries and
property loss. Especially, to those who have enjoyed political or official position in the past, as

27
they reminisced on their past lives (Vansina, 2003). They are most likely left with nothing but
grievous frustrations about themselves.
Lack of Adequate Facilities
W.H.O.(2004) in the survey on health status and health seeking behaviors of the elderly
persons in Nairobi revealed that most of the health facilities accessible to the elderly persons do
not have service for their degenerative condition which is very common in these age groups, no
special health services for geriatrics and negative attitude of health workers towards care of the
elderly was due to lack of knowledge to identify those conditions that can be treated effectively
and inadequate resources to treat the degenerative conditions.
Health Worker’s Knowledge of Care towards the Elderly
It is important for health workers to have adequate knowledge on the basic needs of the
elderly than the rest of the population (Okoye and Asa, 2011). This is necessary because these
needs must be met every day for the elderly to be able to live independently for as long as
possible and Caretakers would be able to help the aged meet these needs without compromising
their health and safety. These needs include personal Hygiene, mobility, nutrition, doctors’ visit
and prescription and physical activity (exercise). (Okoye and Asa, 2011)
Personal Hygiene: The aged needs to have proper hygiene. Teeth need to be brushed and
dentures need to be soaked. Whether elderly people under your care want to shower or bath daily
or every few days, safety need to be a top concern. Railings and nonslip mats can help them
maintain balance and prevent falls. Some safety seats fit directly into bathtubs, and another kind
actually lifts the person into the tub from the outside. If incontinence is a concern, adult diapers
will need to be worn and changed regularly. (Brog, Hallberg and Blomgrist, 2006).

28
Mobility: Mobility is a concern for the elderly if the person under care has muscle weakness,
vision loss or other health conditions that can occur with aging. If the elderly person needs a
wheelchair; a ramp will be needed and other wheelchair accessible features. Similarly, walkers
and canes are required to help the aged get around safely. (Sarrimaki and Stenbock – Hult,
2000) .
Nutrition: According to Less, Hoerr, Weatherspoon & Schiffma (2008), it is important to
ensure that an elderly person continues to eat proper meals, especially if he is living alone and
may have difficulty cooking. Check labels and fridge items frequently and throw out all expired
items. A caretaker can prepare food in advance and freeze the meals to be reheated and eaten.
Volunteer and paid services also can bring healthy meals regularly. However, the care of the
older people in acute care settings has been increasingly criticized for lack of attention on patient
dignity and the fundamental aspects of care such as nutrition and hygiene (Bridges, 2012).
Health: According to Lee, Wong & Loh (2006) health issues that require attention is a greater
concern with age. If the elderly person has any condition requiring medications prescribed by a
doctor, it is vital that he takes the medications at the right time and in the proper dosage. If he
uses over the counter products as well, the labels should be read and a doctor or pharmacist
consulted to ensure that the products do not have possible interactions with prescribed
medications. Watch for possible side effects from medication and health. Ensure that the elderly
maintain regular doctor visits by providing transportation and making the appointment if
necessary.
Exercise and Activity: Exercise is important to maintain muscle function and to keep elderly
people as healthy as possible, Socializing with other people and engaging in mind stimulating

29
activities will need to be planned according to mobility and health issue. (Iwasaki and Jones,
2008).
Pain Management in the elderly Patients without Drugs.
Pain is not a normal part of aging, and may be a sign that something is wrong. Pain is a common
complaint that is often poorly treated in elderly adults. Sometimes there is no clear or exact cause
of pain. Pain management is an important part of elderly care.
- According to Truven Health Analytics information (2015) on how to manage pains
without medicine caregivers should try to treat the cause of the pain. This may include
treating infections or cancer the following may be needed to control pain:
- Heat: Heat helps decrease pain and muscle spasms. Heat should be applied on the area 20
to 30 minutes every two hours or as directed.
- Ice: Ice helps to decrease swelling and pain: ice helps to prevent tissue damage. Ice pack
should be used or ice crushed and put in plastic bag. Cover with towel and place on the
area for 15 to 20 minutes every hour or as directed.
- Rehabilitation: A physical therapist can teach the patient exercises to help improve
movement and strength and to decrease pain. An occupational therapist can teach the
patient skills to help in her daily activities.
- Assistive devices: A care, walker, or crutches can help the patient to move around and
decrease her risk of falling. Caregivers should teach the patients how to use these devices
correctly.
- Electrical stimulation: A device sends mild and safe electrical signals. The signals
decreases pain when used over a painful body part.

30
- Surgery and other procedures: Caregiver may use ultrasound, radiowaves, thermal
(heat) or laser therapy to relieve an elderly patients pain.
Health Workers Attitude and Practice towards the Care of the Elderly
Negative Attitudes (Ageism)
According to O’ Neil (2010) ageism is the systematic, stereotyping of discrimination
against people because they are old. This is perpetuated by the portrayal of older people as frail,
ill, suffering mental deterioration, poor and dependent, and the alternative portrayal of living
affluent life styles and scrounging off the welfare state (Vincent, Patterson & Wale, 2001).
Health workers are at risk of developing ageist attitudes because they are exposed to a
disproportionate percentage of ill or dependent older people (Mandy, Elizabeth and O’Neil,
2011). Lee (2009) asserted that negative attitudes towards older people and instances of ageism
in American society can become an obstacle to training qualified elder care providers. Also
Doherty Mitchel and Elisbeth (2011) opined that attribution of ill health to ageing, low economic
status and negative attitude of health workers towards the care of the elderly are some of the
factors associated with delay in seeking health care. Unfavorable attitudes and stereotypes of
older people among staff are also believed to act as a barrier to the successful delivery of health
information and education and overall health management (Lee, Wong, & Loh, 2006). In
contrast, nurses that express negative attitude towards old people indicated that they prefer to
work with younger patients. When caring for older patients, these nurses were more likely to use
physical restrictions, to disrespect the patient’s autonomy and dignity and discriminate against
them (Weiss 2005).
According to Redmond, Guerin & Devitt, (2008) ageism has been found to negatively
affect the health care services that older persons receives, both implicitly through unfair resource

31
allocation by stakeholders and explicitly by providing offensive and poor quality treatment.
Maltreatment of older people has been identified in facilities for continuing care such as nursing
home, residential care, hospitals and day care facilities. The spectrum of these within institution
may be related to any of the following, the provision of care for example resistance to changes in
geriatric medicine, erosion of individuality of care, inadequate nutrition and deficient nursing
care problem with staffing, poor interaction/communication and poor environment, and
organization policies – bureaucratic or unsympathetic attitudes toward residents. (Alliance for
Aging Research, 2003).
Positive Attitudes
Positive attitudes among healthcare students and staff are essential in the education and training
and in the delivery of good healthcare for older people (Nelson, 2004). In a study that examined
nurse’s attitude towards older acute care patients in United States, it was revealed that nurses
have positive attitude towards older patients in Geriatrics and surgical departments of various
hospitals (Mclafferty, and Morisson 2004). However similar attitudes of nurses has been noticed
in studies done in Australia and Jordan by several researches (Mitchell and McCance, 2010)
(Brown, Nolan, Davis and Keady, 2008).
On attitude of health workers towards older people, Mandy, Elizabeth and O. Neil (2011)
in a survey using the Kogan scale to assess the attitude of health care workers toward older
people in a rural population revealed positive attitude of health care workers toward older
people. Abyad (2006) stipulated that in the care of the elderly, the severely impaired and
dependent aged will need range of professional care as well as with their families so in the
process of creating adequate services home care and institutional service are complementary and
multi directional and care of such patients need shared responsibility of both families and

32
professional service provider. This may be alternately provided at home, community or the
institution with the role of providing communities and concerned professionals with the
knowledge and the skills to solve their problems. Bowling (2005) suggests that quality aged care
requires positive attitude towards empowering elderly patients to take active part in maintaining
their health and ability to deal with and prioritize the numerous problems that the aged may
present with (including associated diagnostic and management dilemmas).
Problems associated with the care of the Elderly
The Health workers experience different health problems when taking care of the elderly.
These problems results from the responsibilities and task involved in caring for the elderly. The
daily tasks involved include bathing, dressing, feeding, lifting, turning him or her in bed,
cooking, shopping, paying of bills, running errands, giving medicine, keeping him or her
company, providing emotional support (Okoye and Asa, 2011). All these help can be time
consuming and emotionally, physically and psychologically draining and may expose the health
worker to stress, risk of diseases, neglect of one self, poor health and depression. (Donatelle,
2011).
Stress: According to Donatelle (2011) Health workers get easily irritated when taking care of the
aged than when taking care of other age groups because of the daily task involved. The stress
impact negatively on the health of the health workers or cause the health workers to be
physically or verbally aggressive towards the care receiver. Studies have shown that one reason
for elderly abuse and neglect is caregivers stress (Lecovich, 2008). It is also very common for
health workers to get angry, feel frustrated, guilt, isolated, unhappy in marriage, anxiety,
depressed, diminished socially, loss of self-esteem from time to time and dissatisfaction with life.
According to Okoye and Asa (2011) feeling guilty about all the things that are not going on right

33
is the cardinal feature of a health workers experience. Stress of caregivers has been shown to be
influenced by many factors which include the attitude of the health worker or care giver (Okoye
and Asa, 2011).
Self-Neglect: Losada et al (2009) in a study of leisure and distress in care givers for elderly
patients revealed that health worker taking care of the elderly are more likely to neglect their
own needs because care of the elderly is time consuming and tasking. They may not recognize or
may ignore the signs of illness, exhaustion or depression that they are experiencing. Frustration
is also one of the feelings that may occur as a result of taking care of the elderly. This arises out
of trying to change an uncontrollable condition in taking care of the elderly especially
Alzheimer’s disease or other kinds of dementia (Alzheimer’s, Society, 2009).
Risk of Diseases: Health workers taking care of the elderly are at risk of contracting diseases
because of the closeness and commitment needed in the care of the aged. (Lecovich, 2008).
Accordingly, Merril and Verbuge, (2011) common diseases that affect the elderly that can be
transmitted to the caregivers are Tuberculosis, HIV/AIDS etc.
Factors influencing Health worker’s Attitude of care towards the elderly
Research demonstrates that many factors have influence on attitude and practice of elderly care
and these include age (Soderhamm et al.2001) gender (Lookinland 2002) education, exposure to
well older people (Gallagher, Bennet and Halford 2006), area of practice (Mclafferty and
Morrison 2004) and professional socialization (Mandy et al 2011). However numerous previous
studies has also argued that several other factors including those mentioned above can also affect
attitudes toward the care of the elderly these include culture, ethnicity, spirituality, education,
personal traits, clinical-experiences and past experience with older people (Brown, Nolan, Davis
and Keady 2008, Lookinland 2002).

34
Age
According to Okoye and Asa (2011) health workers age has an effect towards the attitude of care
giver to the aged. The younger the health worker the greater the stress experienced during the
care. This is because the care given to the aged is time consuming and emotionally, physically
and psychologically draining. In a study on knowledge and attitude carried out in Greece it was
noticed that age influenced attitude and knowledge of health workers positively in the care of the
aged (Lambrinou, Sourtzip, Kalokerinou and Lemonidou, 2009).
Gender
Gender has also being seen to influence attitude of health workers positively or negatively
(Cummings, Kroff and Deweaver, 2000). Studies have shown that gender influences the attitude
of care of the aged positively although female caregivers are easily stressed up and have
frustrating feeling and a feeling of guilt when their care receivers are not satisfied (Herdman,
2002).
Education
According to Lee (2009) education seems to influence the attitude and knowledge of
nurses towards the care of the aged. Although the study concluded that the curriculum of the
nursing education should be revised and improved on for there to be a holistic understanding of
care of the aged. In a study that was done in Greece it was revealed that the higher the level of
education the more positive the attitude towards the care of the elderly amongst Health workers
.Kaemffer, Wellman and Himburg (2002) suggested that gerontology education should be
provided to nurses in all settings regardless of their ethnicity, especially those with less education
and those working in acute patient care settings. Findings has also shown that registered nurses

35
with masters degree hold positive attitude towards the care of the elderly while retired nurses and
less educated nurses display the most negative attitude ( Loh , 2006).
Area of Specialization
Health care professionals and nurses in particular tend to be gate keepers for health
information, and play a key role in health promotion and education for older people (Lee 2006).
A large body of research has focused on the association between health student’s attitudes
towards older people and ageing and their interest or willingness to work in geriatric care.
Redmond, Guerin and Devitt (2008) for example, proposed that the attitude of social work
students before they enter practice could have a significant impact on their occupational choices
as professionals. Discriminatory practices by staff may not necessarily be based on intent but
rather provoked by a lack of skills and confidence in working with older people (Nussbaum
2003). Serious shortcomings in training for healthcare professionals and a need for further
education in the care of older people have been identified (Alliance for Aging Research 2003,
Brown et al. 2008). As populations continue to age there is increasing concern globally about the
quality of health care currently available to older people, and the availability of suitably qualified
health and social care staff with an interest in working with older people (Happel 2002; Brown et
al. 2008). However, the identification of unfavorable views towards geriatrics as a career choice
amongst students in health and social care appears to be a long standing and current theme in the
literature. (Happel 2002; Alliance for Ageing Research 2003; Brown et al. 2008). Studies across
many countries (e.g. Australia, Brazil, England, Germany, Hungry, Isreal, and the United State)
have found working with older people to be amongst the lowest preference career choice
(Fitzgerald et al (2003) Weiss (2005) Lee et al. (2008), Redmond et al. (2008). Happel (2002),
for example found out that just under 2% of nursing students cited care of the elderly as their

36
most desired area for future employment, while over two third of nursing students ranked this
area within their last three preferences. Caring for the elderly is often considered basic,
unchallenging and unrewarding based on the commonly held perception that older patients do
not get better and therefore work in this area is of limited value (Brown et al. 2008). A recent
study in Ireland revealed that health and social service staff felt that there was little opportunity
for career development within the care of the elderly, particularly for home helps and care
assistants (NCAOP, 2005b). Working with children or in areas perceived as more technical such
as acute care tend to be preferred as they are considered more worthwhile, more exciting and
dynamic and result in observable and useful outcomes (Happel, 2002).
Conversely, a smaller number of studies (Tan, Zhang and Fan, 2004, Lee et al, 2006)
have uncovered neutral or positive feeling among university students about working with the
elderly in their future careers. As the population is growing older, it is imperative that healthcare
services have highly skilled and trained staff; however care of the elderly is among the least
favored areas of healthcare as it is considered unrewarding and to have few opportunities
(NCPOP, 2009).
Culture and ethnicity
It is evident that cultural competence and ethnicity can play a major role in the attitudes
of health workers towards the care of the elderly. Many studies have shown that the general level
of cultural competence may be a predictor of positive attitude amongst nurses. According to
Beard (2004) who examined the attitude of nurses toward the elderly in a study that explored the
relationship of cultural competence to attitudes and also assessed demographic and work
characteristics. It was concluded that cultural competence had a very strong positive attitude
towards elderly care.

37
Theoretical Review
Theory of Planned Behavior and Theory of Reasoned Action
The theory of planned behavior, a derivative of the theory of reasoned action, postulates
that people are motivated to change based on their perception of norms, attitudes, and control
over behaviors. Each of these factors can either increase or decrease a person’s intent to change
his or her behavior. The theory shows several important constructs that are involved in these
value expectancy theories: attitude, subjective norm, perceived behavioral control, intention, and
behavior (Montano & Kasprzyk, 2008). The theory of planned behavior explains how behavioral
intention determines behavior, and how attitude toward behavior, subjective norms, and
perceived behavioral control influence behavioral intention. According to the theory, attitudes
toward behavior are shaped by beliefs about what is entailed in performing the behavior and
outcomes of the behavior. Beliefs about social standards and motivation to comply with those
norms affect subjective norms. The presence or lack of things that will make it easier or harder to
perform the behaviors affects perceived behavioral control. Thus a chain of beliefs, attitudes and
intentions drive behavior. The strength of the relationship between the first three constructs i.e.
attitude, intention and behavior varies, depending on the population and the specific topic being
studied (Hardeman, (2002).
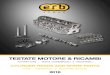
Application of the theory
This theory is applicable, in this study in that the health workers intention and their
beliefs are what influence their behavior and attitudes. The demographic factors and the
resources available have a role to play in the outcome which is the result of the health workers
care towards the elderly. Health workers perception of norms and beliefs that is knowledge of the
health worker on the care of the elderly build-up his intention and this is what influences the

38
( P e r f o r m e d
b e h a v i o u r )
A t t i t u d e
a n d
p r a c t i c e o f
c a r e
Knowledge ,
Social experience and
resources available
• D e m o g r a p h i c f a c t o r s• P e r c e p t i o n o f
n o r m s a n d
b e l i e f s
• C u l t u r a l v a l u e s• S u b j e c t i v e n o r m s
I n t e n t io n
A n d b e h a v io u r
H e a l t h w o r k e r s
A p p l i c a t i o n o f t h e T h e o r y o f
r e a s o n e d a c t i o n a n d p l a n n e d
b e h a v i o u r b y M o n t a n o a n d
K a s p r z k y , 2 0 0 8 t o t h e s t u d y .
health workers attitude and practice of care towards the elderly. Thus, the theory of planned
behavior views attitude, subjective norms and perceived behavioral control as contributing to the
formation of behavioral intention, based on the assumptions that human behavior is often
reasoned than illogical.
This theory is also used in this study because it highlights potential meanings of attitudes,
beliefs, subjective norms and perceived behavioral control as determinants of intention to
perform behavior. Moreover, in this theory demographic factor, values and variables are
considered as background factors. These factors are presumed to influence intention and
behavior, normative and control beliefs. This study will assume that the intentions of health
workers towards the elderly are influenced by cultural values, religion, social experiences,
education etc.

39
Social Network and Social Support Theory
It is widely recognized that social networks and the social relationships that are derived
from them have powerful effects on important aspect of both physical and mental health. Social
network refers to the existence of social ties. Research into how aspect of social networks
influence health (positively and negatively) offers insights into the pathways through which
social ties influence health provision of social support (2) social influence (3) social engagement
(4) person- to- person contact; and (5) access to resources and material goods (Ayres, 2008
Twoy, Connolly, and Novak, (2007).
Most obviously, the structure of network ties influence health via the provision of social
support. Social support has been defined as the physical and emotional comfort given to us by
our family, friends, co-workers, and others (Uchino, 2004). Social support is typically divided
into five subtypes (constructs): emotional, instrumental, appraisal, sharing points of view, and
informational support. Equally important are the ways in which social relationships provide a
basis for intimacy and attachment. Intimacy and attachment have meaning not only in
relationships that are traditionally thought of as intimate (for example, between couples or
between parents and children) but also in more extended ties to the community. For instance,
scholars have recently focused on the role of social capital in overall health (Stephens, 2008).
Social capital refers to the degree to which a community or society collaborates and cooperates
(through such mechanisms as networks, shared trust, norms, and values) in order to achieve
mutual benefits (Baum and Ziersch, 2003). When relationships are solid at the community level,
individuals feel strong bonds and attachment into places (for example, a neighborhood) and
organizations (for example, voluntary or any or religious organizations) bonds that may lead to
improvements in psychological and physical health.

40
Application of these theories to the study
The social network theory applies to the study of knowledge, attitude and practice of the
care of the elderly in that health workers form a social network and caring for the elderly does
not just involve a group of health workers but involves several groups and several health workers
that forms a network. This implies that many health workers may have to work together in
providing the care for the elderly in order to achieve the desired goal. The social support theory
works in collaboration with the social network and it is also applicable in this study in that for
the effective care of the elderly to occur, the health workers should be able to establish a
relationship with the elderly that will allow the health worker to love and be ready to care for the
elderly. This may affect the attitude of the health worker resulting to the health worker either
having negative or positive attitude. This has to do with passion for the job or willingness to
specialize in this area. Liaising with other support groups to support in the care of the elderly
may also be very necessary. For example inviting the priest or Church members to visit and pray
for the elderly.
Empirical Review
Knowledge
In a study conducted by Kaur, Kumar, Kaur, Rani, Ghai, & Singla (2014) in India to
assess the knowledge and attitude regarding care of the elderly among nursing students. A cross
sectional study was undertaken on 267 undergraduate nursing students. A pre-validated, self-
administered questionnaire was used for the assessment. The knowledge questionnaire consisted
of 28 multiple choice questions with one right answer. The total score was further categorized as
poor, average and good as per the score obtained by the subject. The attitude was assessed on a
Likert five point scale and it consisted of 16 items. The total score was further categorized as

41
unfavorable, neutral and favorable attitude as per the scores obtained. Majority (95.5%) of the
subjects were females. Mean age (yrs) +- SD was 22.61 + - 3.31 with the range of 19-48yrs mean
knowledge score + - SD was 22.10 + - 2.91, with the range of 9-27. Around two third (76.4)
were in good category of knowledge score. Mean attitude score + - SD was 60.38 + - 8.95 with
the range of 22 -78. 64.6% were in the positive category of attitude. Knowledge and attitude
were positively correlated. According to Kaur et al (2014) nurses need to be well equipped with
knowledge and should also have positive attitude regarding elderly care.
In a study conducted in Australia by Mellor, Chew & Greenhill (2006) it was explored
that the attitudes of nurses working in a multi-purpose health service (MPHS) towards elderly
people and their understanding of gerontic care. A descriptive, non-experimental quantitative
research design using a self report questionnaire was used for the study. A sample group of thirty
–one (31) staff members from a single MPHs were the participants for the study. Multi outcome
measures were used. Nurse’s attitudes were assessed using Kogan’s old people scale (KOPs).
Nurse’s knowledge was measured using Palmore’s facts of aging Quiz (PFAQ) and a second
instrument, the nurse’s knowledge of elderly patients Quiz (NKEPQ), which was developed by
the authors of the study. The key findings indicated that even though nurses in this MPHs have
strong positive attitude towards the elderly people, they had knowledge deficits in key clinical
areas both gerontic nursing and socio-economic understanding of the ageing population in
Australia. In conclusion the result of the study assisted in the identification of knowledge gaps
and also highlighted areas for improved education which are essential in the delivery of high
quality, effective care.
According to Olayiwola, Olusanya and Ketiku (2013) in a study on the knowledge of
population of ageing nutrition among undergraduates in a Nigerian University. The result

42
showed that 50% have the knowledge that biological age of the elderly begins at 60 years and
50% also have the knowledge that life expectancy in Nigeria has increased while 70% strongly
agreed on health policy of the elderly. The above study concluded that the knowledge of the
subjects on the nutrition of the elderly was very high amongst the subjects especially those with
background in food science and nutrition while those with very low scores did not have such
background. It was also reported that there was a very strong correlation between knowledge of
the elderly and knowledge of nutrition. Large gaps still exist in the knowledge on health status
and health seeking behaviors of the elderly person (Fitzgerald, Wray and Halter 2003). In survey
on staff perception of patients with dementia survey on evaluation of education and training of
staff in Dementia indicated that most acute care staff does not find caring for people with
dementia unrewarding or difficult but that caring for patients with dementia gave no job
satisfaction. (Nur Asyura et al, 2009)
Attitude
In a study conducted by Oyetunde, Ojo & Ojewale (2013) in Ibadan, Nigeria measuring
the attitude of nurses towards the care of the elderly in two (2) selected hospitals in Ibadan, with
130 self-administered questionnaires were administered to nurses. Results showed that 73% of
the respondents agreed that elderly are difficult to care for and over 80% agreed that effective
care for the elderly requires special training and more than 90% believed that effective care of
the elderly will require the hospital to provide a special geriatric ward for the elderly and their
complications. The respondents in above study also showed positive attitude towards the care of
the elderly and good knowledge of ageing process. According to Oyetunde, Ojo & Ojewale
(2013) effective care of the elderly requires special training, provision of geriatric ward,
adequate staffing to reduce stress and improved quality care.

43
In a study done by Mandy, Mitchel & O’ Niel (2011) in Ireland on 109 health workers to
identify and evaluate attitude and knowledge of health workers towards the elderly, reported that
higher level of education increases the health workers knowledge of care of the elderly. The
study was undertaken in a rural country, on various caders of health workers e.g. ward managers,
registered staff nurses, health care assistants, public health nurses and student nurses. The aim of
the study was to explore the attitudes held by these health care workers towards older people in
rural population. The variation of intensity of attitude was illustrated by dividing the potential
range of scores into six equal categories and this showed that healthcare workers held positive
attitudes towards older people, indeed 97.3% of the scores fell into the Slightly positive to very
positive score range. An independent T-test was conducted to compare KOP scores for those
who had attained a university degree, higher diploma or M. Sc and those who had not attained
qualification at university. There was a significant difference in score for university graduates
M= 149.34, S. D 15-4) compared to those who had not attained university qualifications (M =
144.88 = 12.45) t (161) = 202, P = 044). In conclusion the study revealed that vast majority of
the participants had positive attitude. In addition it was revealed that study to a higher level of
education appears to mitigate towards holding more positive attitude and this is an important
finding in light of the shift towards nursing as an all-graduate profession. Research has shown
that the quality of health care services provided to older population is strongly influenced by care
givers attitude towards older people (Gallagher, Bennet & Halford, 2006). The affirmative
attitudes of nurses have a positive influence on the health of older patients (Courtney, Tong &
Walsh, 2000). Nurses with constructive attitude towards older people have been noted to listen
attentively, bond deeply, assist respectfully and engage in friendly relationships with their clients
(Courtney et al, 2000).

44
However, according to Engstrom and Fagerbreg (2011) in a study ‘on the attitude
towards older people among Swedish health care students and health professionals working in
eldercare’ The study included 928 health care students and three groups of professional health
care givers with university degrees and certified nursing assistants selected by convenient
sampling method in a variety of health settings in Sweden. The result that was analyzed using the
Kogan scale revealed that the statement made score of 17 to 85 respectively. A significant
difference in positive and negative scores was observed among the three professional care givers.
Registered nurses had the highest positive score as well as the lowest negative score. Health care
students in the first semester had the most unfavourable attitude towards older people while
students in semester two had the most favorable attitude towards older people. Registered Nurses
had a high positive score as well as low negative score compared to nurses without academic
degree. Progression in ones educational level was also seen to contribute in the reduction of
unfavorable attitude towards the elderly.
Practice
According to Okoye and Asa (2011) providing care especially to the elderly, takes a huge
toll, both physically and emotionally on the caregiver. With the population of the elderly
growing in Nigeria, one of the emerging issues is the care and support of elderly persons in years
to come. Few people are prepared for the responsibilities and tasks of caring for the aged because
of the stress involved. In a study conducted in Nsukka Enugu State by Okoye and Asa (2011) to
investigate the experiences of caregivers of elderly relatives. Questionnaires were distributed to
330 respondents result shows that there exists a significant relationship between caregiver’s age
and level of stress (P = 0.001). the sex of the receiver, the level of education of caregivers, level
of education of care receiver are all significantly related to the level of stress.

45
Summary of Literature Review
A review of literature on the concept of the ageing, the biopsychosocial challenges of the
elderly receiving care and the knowledge, attitude and practice of care of the elderly among
health workers was done. According to Papalia, Feldman & Camp, (2002) the concept of aging
is multifaceted, this is because it’s in depth description covers diverse areas of human
development which includes the chronological, biological, psychological, social and functional
dimensions of age. The biopsychosocial challenges of the elderly in receiving care include
physical changes, insensibility problems, affordability, anxiety and depression and poor policy
implementation. Data based literature review and empirical studies, revealed the elderly needing
care due to the natural ageing process, and marginalization of the elderly is very common. There
is poor knowledge of elderly care by the health professional and negative attitude towards the
elderly, in terms of practice, there are no special health services provided for them while most of
the facilities do not have services for their degenerative problems, leaving a wide vacuum to be
filled and addressed by the current study on knowledge, attitude and practice of care of the
elderly among health workers in a tertiary health facility UCTH in Calabar, Cross River State

46
CHAPTER THREE
RESEARCH METHOD
This chapter presents research design, area of study, population of study,
sample, sampling procedure, research instrument, validation of the instrument, reliability testing,
ethical consideration, procedure for data collection and method of data analysis.
Research Design
A Cross sectional descriptive study design was used to determine the level of knowledge,
attitude and practice of care of elderly among health workers in University of Calabar Teaching
Hospital Calabar Cross River State. According to Isangedihi, Joshua, Asim & Ekuri (2004), the
descriptive study survey allows orderly collection of data. The cross sectional approach involves
the collection of data at a point in time and considered suitable for the phenomenon being studied
(Polit & Beck, 2006).
Area of the Study
The area of study was University of Calabar Teaching hospital (UCTH). It is a tertiary
institution located in Calabar, Cross River State. UCTH Calabar is a research, training and
service centre for health professionals and health care needs of all age groups are met. It has the
permanent site in Calabar and an annex at Okoyong in Odukpani local government area. It
consists of so many units namely casualty, Outpatient Department, Medical, Surgical, Theatre,
orthopedic, Pediatric, Maternity, community Health, E.N.T and Administration to mention but
few. It has 600 beds for inpatients and is headed by a Chief Medical Director and other
subordinates in sub units.

47
Population of Study
The population of study consisted of (402) doctors, (600) nurses,(10) dentists and
(11)physiotherapists that provide direct clinical health care to elderly patients making up a total
of one thousand and twenty three (1023) health workers .
Sample and Sampling Procedure
The sample was calculated using the Taro - Yamane (1967) simplified formula for finite
population proportions. The sample was 461 respondents made up of 200 Doctors, 240 Nurses,
11 Physiotherapists and 10 Dentists
n = N 1+N(e)2
n = sample size
N = population size
e = acceptable sample error (See Appendix II)
95% confidence level and P = 0.05 are assumed
Sampling Procedure
A multistage sampling technique was used to select respondents for the study. The health
workers were stratified according to profession (Nurses, Doctors, Dentists and physiotherapies)
For the nurses, six wards were selected using random sampling method and the duty roaster of
each ward was used as the sampling frame. The number of the nurses in the duty roaster was
copied out and written on pieces of paper. This was placed in a basket and shuffled and for each
ward 40 nurses were selected making a sum of 240 nurses. For doctors, ten (10) departments
were selected using simple random sampling and 20 doctors were selected from each selected
department by random sampling technique using the duty roaster as the sampling frame making a
sum of 200. Where the health workers or professional in a selected cadre were not up to 20 all
the health workers were used for the study (Pls see Appendix vii)

48
Inclusion criteria
• Should be Nurses, Doctors, Dentists or Physiotherapists
• Should have direct contact with the patient
• Willingness to participate in the study
Instrument for Data Collection
The instrument used for data collection was questionnaire. It had five sections A, B, C, D and E.
- Section A had seven items which elicited information on socio demographic profile of
the respondents
- Section B had eighteen items on the level of knowledge of care of the elderly. Yes and
No responses were used and 1 point was allocated to correct responses.
- Section C with twelve items elicited information on attitude of health workers towards
care of the elderly.
- Section D consisted of nine items on practice of the Care of the Elderly. The variables
were weighted as follows. Always 2 points, Sometimes 1 point, Never No point.
- Section E was made up of nine items on factors influencing the attitude of health workers
on care of the elderly.
A rating scale 1- 4 was used.
The negative statements were coded in the reverse.
1 =strongly disagree (strongly unfavorable to the concept)
2 = Disagree (somewhat unfavorable to the concept)
3 = Agree (somewhat favorable to the concept)
4 = strongly agree (strongly favorable to the concept)
(See Appendix I)

49
Validity of the Instrument:
Face and content validity of the instrument was done by the Researchers Supervisor, a
Community Health Specialist and two others who are experts in measurement and evaluation.
Their observations were used to make necessary modifications before final approval and
administration.
Reliability of the Instrument :
Test retest method was adopted. Ten percent of the sample which is Forty six (46) copies
of the questionnaire was administered on health workers in University of Uyo Teaching Hospital
entirely outside the area of study setting with similar population characteristics. 20 copies of the
questionnaires were administered to doctors, 24 were administered to nurses and 1 each was
administered to a dentist and a physiotherapist. The questionnaires were administered on 46
health workers and after two weeks interval the same questionnaires were administered to the
same health workers in the same hospital and the data obtained from the two administrations
were used to calculate the reliability coefficient. Using Pearson product measurement correlation
coefficient statistics giving a reliability coefficient of 0.91.
Ethical Consideration
Application for ethical approval and introduction letter endorsed by the Head of
Department of Nursing Sciences, University of Nigeria, Enugu Campus and abridged copy of the
research proposal were submitted to the Research and Ethical committee of the Cross River
State, Ministry of Health Calabar and UCTH ethical committee and approval was given, after
due consideration by the ethical committees. The ethical clearance was granted for the study.
(See Appendix Va and Vb)

50
Finally, individual informed consent was obtained from each study participant who met
the inclusion criteria. Confidentiality and anonymity were assured to the respondents with
respect to the information they have shared. These enabled them to give the necessary assistance
on the collection of data. (See Appendix III)
Procedure of Data collection
The researcher recruited six research assistants and trained them on the purpose of the
study to ease data collection With the letter from the Department of Nursing Science, permission
to carry out the study was obtained from the hospital administration. The data were collected by
the researcher and six trained research assistants. The researcher and her assistants administered
the questionnaires to the selected health workers at their work place between 2pm and 4pm when
work in the ward is minimal. The questionnaires were collected on the spot. This was to ensure a
high return rate and avoid the problems usually associated with the posting of instrument and to
offer explanation where and when necessary. Data collection lasted for 6 weeks.
Method of Data Analysis
Data collected was collated, tallied and analyzed using E.P.I info-7. Descriptive statistics
of percentages, mean, standard deviation and mean decision rule of any score greater than 2.5 is
positive. Inferential statistics (Chi-square) was used to test the association of the variables at 0.05
significance level.

51
CHAPTER FOUR
PRESENTATION OF RESULTS
The results are presented in Tables and figures according to the research
questions. Out of 461 questionnaires that were administered 460 questionnaires were returned
giving a returned rate of 99.9%.
Table 1 Socio-Demographic characteristics n = 460
Demographic Characteristic Frequency Percentage (%) Age Category
20-29 168 37 30-39 186 40 40-49 86 19 >50 20 4 Gender Male 172 38 Female 288 62 Professional Status Doctors 200 44 Nurses 240 52 Dentists 10 2 Physiotherapist 10 2 Years of Experience 1-8 250 54 9-16 123 27 17-24 51 12 25-32 25 5.0 33 and above 11 2.0 Marital Status Single 300 64.7 Married 150 32.6 Widow 7 1.5 Divorced 3 0.6 Educational Status Primary 0 0 Secondary 0 0 Tertiary 460 100 Categories of patients you will like to care for by gender
Male 300 64.7 Female 160 35.3

52
From Table 1data analysis of the socio demographic characteristics of the respondents revealed
that age ranged from 20 >50 years with a mean age of 34 years and standard deviation of 4.8.
More than half of the respondents 62% percent were females, For educational status all the
health workers were educated 460 (100%) up to tertiary level.
RESEARCH QUESTION 1. What is the level of knowledge of care of the elderly among the
health workers in UCTH, Calabar
Table 2a: Level of Knowledge of Care of the Elderly among Health Workers
Table 2a: shows the responses given by the subject regarding their level of knowledge of care of
the elderly. For majority of the items more than 90% of the subjects gave the correct answers.
Items Yes No Mean correct Answer
The elderly people need regular exercise 440 (96%) 20(4%) 96 Proper mouth care is a basic need for the elderly 448(97%) 12(3%) 97 Aging process leads to anatomical and physiological changes 452(98%) 8 (2%) 98 Lung capacity tends to decrease in old age 418(91%) 42(9%) 91 Railings and nonslip can help maintain balance and prevent falls in old age
434 (94%) 26(6%) 94
Elderly people need to eat regularly and properly 432(94%) 28(6%) 94 The fear and anxiety related to inability to perform usual roles by the elderly can be reduced by maintaining calm, unhurried, confident manner when interacting with the patient
446 (97%) 14(3%) 97
Sound sleep in the elderly can be encourage by restricting visitors during rest periods and providing care in groups
460(100%) 0 100
Bedsores in the elderly is prevented by keeping the skin clean and dry and bed linens wrinkle free and dry
448(97%) 12(3%) 97
Memorizing capabilities in the elderly person is affected due to structural changes in the brain
450(98%) 10(2%) 98
Care can be rendered to the elderly with altered sensory perception by reducing environmental noise and speaking louder and slowly with nonverbal cues when appropriate
437(95%) 23(5%) 95
Sleep patterns among the elderly steadily increase compared to persons under 60 years
10(2%) 450(98%) 98
Most of the elderly in Nigeria live above the poverty level 13(3%) 447(97%) 97 Elderly workers have the highest rate of absentism than younger workers
430(93%) 30(7%) 93
Majority of the elderly are able to adapt to change more easily compared to young people
40(9%) 420(91%) 91
As a healthy person reaches old age, his/her voluntary participation in organization usually
418(91%) 42(9%) 91
In Nigeria, majority of the elders whose children have left home suffer from empty nest syndrome
413(90%) 47(10%) 90
The elderly have more fear of crime compared to younger persons 454(99%) 6(1%) 99

53
TABLE 2b
Categorization of knowledge score n%
Poor – 01-8 Mean +
16.2± 1.4
Range 01-18
3(0.7%)
Average 9-14 20(4.3%)
Good 15-18 437(95%)
Table 2b: shows categorization of knowledge score regarding the care of the elderly (maximum
attainable score 18) most of the subjects (95%) had good knowledge regarding care of the
elderly, 4.3% had average knowledge while 0.7% of the subjects had poor knowledge regarding
care of the elderly. Mean knowledge score was 16.2 SD ± 1.4 with the range of 01-18.
TABLE 2c
Proportion of health workers and their level of knowledge on the care of the elderly patients Health workers Poor Average Good Total
Doctors 0(0%) 8(4) 192(96) 200(100)
Nurses 1(0.1) 8(3) 23(96) 240(100)
Dentists 1(10) 2(20) 7(70) 10(100)
Physiotherapist 1(10) 2(20) 7(70) 10(100)
Total 3(0.7) 20(4.3) 437(95) 460(100)

54
Research Question 2: What is the attitude of health workers towards the care of the elderly?
Table 3: Attitude of health workers towards the care of the elderly
Items Strongly Agree n (%)
Agree n (%) Disagree n (%)
Strongly Disagree n (%)
Mean SD Decision
I feel good taking care of the elderly
122(27%) 276(60%) 48(10%) 14(3%) 3.0 0.75 •
I see care of the elderly as
being time consuming 136(29.6%) 182(39.6%) 120(26%) 14(3%) 2.7 0.68 •
I prefer giving attention to younger patients than the elderly ones
74(16%) 150(33%) 180(39%) 56(12%) 2.3 0.57 #
The older the elderly the more demanding he/she becomes
220(48%) 176(38%) 54(12%) 10(2%) 3.2 0.8 •
The elderly are difficult to care for
124(27.1%) 214(46.7%) 104(22.7%) 14(3.5%) 2.8 0.7 •
Time should not be wasted for elderly with terminal illness
18(3.9%) 68(14.8%) 218(47.4%) 156(33.9%) 1.8 0.45 #
The elderly do not deserve the care health workers give them
12(2.6%) 58(12.6%) 162(35.2%) 228(49.6%) 1.8 0.45 #
Some elderly look untidy and dirty. And as such I do not like caring for them
32(7.8%) 96(20.9%) 198(43%) 130(28.3%) 2.0 0.5 #
The elderly can often provoke the care giver
93 (21.3%) 238(51.7%) 80(21.3%) 44(9.6%) 2.7 0. 67 •
The majority of the elderly are senile
42(9.6%) 228(50%) 154(34%) 34(7.4%) 2.3 0.57 #
I get stressed up when taking care of the elderly
92(20%) 220(48%) 128(28%) 18(4%) 2.6 0.65 •
Calling the patient by name when treating or caring for the elderly is very important
238(51.7%) 168(36.5) 42(9.1%) 12(2.6%) 3.3 0.82 •
Level of Decision = 2.5 Positive = • Negative = #
Table 3 above indicates the attitude of health workers on the care of the elderly. On those that
feel good taking care of the elderly 60% agreed while 27 % strongly agreed and 3% and 10%
strongly disagreed and agreed respectively with a mean of 3.0. On the item that sees care of the
elderly as time consuming 29.6 % strongly agreed while 39.6% agreed that caring for the elderly

55
consumes time. On the item that examines the fact that the elderly do not deserve the care given
to them, 49.6% strongly disagreed while 35.2% disagreed with a mean of 1.8. The item of
Elderly is untidy and dirty, 43% disagreed and 28.3% strongly disagreed while 7.8% strongly
agreed and 20.9% agreed mean of 2.0. The item on the mental state of elderly shows the 50% of
the health workers agreed that elderly are senile while 34% disagreed. About 48% of health
workers agreed that they get stressed up when taking care of the elderly while 28% disagreed,
20% strongly agreed that they get stress-up and 4 % strongly disagreed with a mean of 2.6.
About 51.7% and 36.5% of the health workers strongly agreed and agreed respectively on calling
patient by name while 2.6% strongly disagreed with a mean of 3.3.
RESEARCH QUESTION 3: WHAT ARE THE HEALTH WORKERS PRACTICES OF CARE OF THE ELDERLY?
TABLE 4A: HEALTH WORKERS PRACTICE OF CARE OF THE ELDERLY .
Table4a. Above shows health workers practices of care of the elderly, 246 (54%) and 208 (45%)
respectively accepted that they always and sometimes give prompt attention to the elderly even
Items Always Sometimes Never
I like taking care of older people 122(27%) 276(60%) 63 (13%)
I attach titles to the names of elderly while taking care of them to create relationship
168(36.5%) 238(51.7%) 54(11.7%)
Nutritional assessment of the elderly is promoted and l also encourage the elderly to eat adequately and at times assists in feeding them
288(63%) 156(34%) 16(4%)
Prompt attention is given to elderly patients even in emergency
246(54%) 208(45%) 4(1%)
Assessment and evaluation are needed for effective care of the elderly
236(51%) 206(45%) 16 (4%)
Decreased mental ability of elderly patient often by aging process and illness affect response to care
200(43%) 238(52%) 20(4.4%)
I get so stressed up when taking care of the elderly
92(20%) 220(48%) 148 (32%)
Taking care of the elderly is time consuming
136(29.6%) 182(39.6%) 142(30.8%)
I neglect myself and concentrate only on the elderly when taking care of them
40(8.7%) 106(23%) 314(68.3%)

56
in emergency. 236(51%) and 206 (45%) respondents accepted respectively that they always and
sometimes carry out assessment and evaluation for effective care while 14 (3%) opined never to
do it. On the importance of nutritional assessment 288 (63%) accepted carrying it out always 156
(34%) sometimes while 16 (4%) never did it.
Table 4b
Categorization of practice score n%
Low (never) 01-8 Mean ± SD
12.02 ± 4.27
Range 01.18
87(19%)
Moderate (sometimes) 09-14 203(44%)
High (always) 15-18 170(36%)
Table 4b: shows categorization of responses given by respondents on their practice of care of
the elderly. 170 (36.9%) highly practiced (always) care of the elderly, 203 (44.1%) moderately
(sometimes) practiced care of the elderly while 87 (19%) never practiced care of the elderly.
Mean practice score was 12.02 SD ± 4.27 with the range of 01-18.
Table 4c
Proportion of health workers and their practice of care of the elderly patients Health workers Low Moderate High Total
Doctors 40(20%) 100(50) 60(30) 200(100)
Nurses 40(16) 100(42) 100(42) 240(100)
Dentists 3(30) 2(20) 5(50) 10(100)
Physiotherapist 4(40) 1(10) 5(50) 10(100)
Total 87(19) 203(44) 170(37) 460(100)

57
Research Question 4: What are the factors that influence health workers attitude towards the
elderly?
Table 5: Factors influencing the attitude of health worker towards care of the elderly.
N = 460 Items Strongly
Agree n (%) Agree n (%) Disagree
n(%) Strongly Disagree n(%)
Mean SD Decision
I choose this department because I like taking care of the elderly
76(16.7%) 182(40%) 158(34.8) 38(8.4%) 2.4 0.06 #
Taking care of the elderly is very demanding
144(31.4%) 250(54.6%) 58(12.7%) 6(1.3%) 3.0 0.075 •
Effective care of the elderly requires special training
230(50%) 176(38%) 52(12%) 0 3.3 0.083 •
Hospital should have special ward i.e. geriatric wards for effective care of the elderly
278(61%) 166(36%) 14(3%) 2(0.4%) 3.2 0.08 •
The health care policy of Nigeria has made the care of the elderly difficult
22(4.7%) 220(46%) 92(20%) 136(30%) 2.4 0.06 #
Mental status of the elderly patients affects their care and decision making
176(38%) 268(59%) 16(3.5%) 0 3.3 0.083 •
Elderly patient exhibit different behaviors which affect their care
138(30.1%) 290(63.3%) 26(5.7%) 4(0.9%) 3.2 0.08 •
It is difficult to persuade and convince reluctant about their care in the hospital
132(28.8%) 282(61.6%) 44(9.6%) 0 3.1 0.078 •
Some elderly are abandoned due to lack of social support
190(41.7%) 230(50.4%) 26(5.7%) 10(2.2%) 3.3 0.083 •
Level of Decision = 2.5 Positive = • Negative = #
Table 5: above shows factors that influence the health workers care of the elderly, 220 (46%)
Agreed that Nigeria health policy influence the care of the elderly while 136 (30%) strongly
disagreed with a mean of 2.4.On mental status 268 (59%) agreed that mental status of the elderly

58
influence the practice of care while 16 (3.5%) disagreed with a mean of 3.3.On training 230
(50%) strongly agreed that special training is required for health workers taking care of the
elderly while about 52(12%) disagreed with a mean of 3.3.On wards for admission, 278 (61%)
strongly agreed that there should be special wards while 14(3%) disagreed with mean of 3.2.
Hypothesis 1 There is no association between years of experience and the health workers
attitude towards the care of the elderly
Table 6a: Mean years of experience of health workers and attitude of care towards the
elderly.
Items Strongly Agreed
Agreed Disagreed Strongly disagreed
Mean F-S P. value
Care of the elderly is more demanding
220(48) 176 (38) 54(12) 10(2) 7.6 2.7 0.0085
I neglect my self
214(46.5) 180(39) 27(12) 10(2.2) 7.3 24. 0.022
It is time consuming
136(29.6) 182(39.6) 120(26) 14(3) 6.7 2.2 0.037
Time should not be wasted in care of elderly
18(3.9) 68(14.8) 218(47.4) 156(33.9) 6.4 2.6 0.017
Elderly people are difficult to care for
124(27.1) 214(46.7) 104(22.7) 14(3.5) 6.0 3.9 0.004
I feel good caring for the elderly
122(27) 276(60) 48(10) 14(3) 8.3 1.7 0.12
Calling the patient by name
238(51.7) 168(36.5) 42(9.1) 12(2.6) 10.5 4.8 0.001
I like taking care of the elderly
74(16) 316(68) 58(13) 12(2.5) 8.0 2.4 0.03
Elderly people are normal people
198(43) 242(52.6) 16(3.5) 2(0.4) 7.1 2.0 0.08
Table 6shows the mean years of working experience of health workers and their attitude towards
the care of the elderly. On the item of the caring for the elderly is more demanding 38% agreed
while 48% strongly agreed with a mean years of experience of 7.6 years and a P- value of 0.0085
which was statistically significant. The item of elderly care is time consuming was statistically

59
significant with a mean years of experience of 6.7 years and a P-value of 0.037. The elderly are
difficult to care for was statistically significant with a mean years of experience of 6 years and a
P- value of 0.004. On the item I feel good caring for the elderly was not statistically significant
with a P-value of 0.12 and mean years of experience of 8.3 while like taking care of elderly
people was statistically significant with mean years experience of 8.0 and P-value 0.03
Table 6b: Years of Experience and Attitude of Health Workers
Years of Experience Positive attitude Negative attitude Total
1-8 144(57%) 106 (43%) 250
9 - 16 77 (63%) 46 (37%) 123
17 – 24
25 -32
39 (76%)
21 (84%)
12 (24%)
4(16%)
51
25
33 and above 9 (81%) 2 (19%) 11
290 170 460
Table 6b above shows that there is a relative increase in positive attitude of health workers
towards the care of the elderly as the years of experience increases.
Table 6c Proportion of health workers with positive and negative altitude towards the care of the elderly patients. Health workers +ve -ve Total
Doctors 116(63) 84(37) 200(100)
Nurses 175(75) 75(25) 240(100)
Dentists 4(40) 6(60) 10(100)
Physiotherapist 5(50) 5(50) 10(100)
Total 290(67) 170(33) 460(100)
CHAPTER FIVE
DISCUSSION OF FINDINGS

60
This chapter presents discussion of major findings; conclusion, implication of findings to
nursing, recommendations, suggestions for further studies and summary as well as limitation of
the study.
Research Question 1
What is the level of knowledge of care of the elderly among health workers in UCTH,
Calabar. The findings in this study indicate that majority(95%) of the health workers had
adequate knowledge on the basic needs and care of the elderly. The findings also revealed that
health workers who had sufficient knowledge on the nutrition and personal hygiene of the elderly
were also in the majority. The explanation for this may be because all the health workers have
tertiary education and are already in specialized areas. This agrees with the finding of Okoye and
Asa (2011) that knowledge on the basic needs of the elderly will help care givers to assist the
elderly to meet their needs without compromising their health and safety. It is also in agreement
with Mandy, Mitehell and Oneil , (2011) that higher level of education increases health workers
knowledge of care of the elderly. However, this findings disagrees with Donatelle (2001)
and Mcfarely and Morrison(2004) that posits that most curricula of health professionals have
little or nothing to do about the elderly and as such most health workers have very poor
knowledge on the care of the elderly.
Research Question 2
What is the attitude of health workers towards the care of the elderly in UCTH Calabar
The study reveals that the positive attitude of the health workers was higher than the negative
attitude that they like taking care of the elderly; they called the patient by name and created a
relationship with the elderly. This agrees with Mandy, Mitchel and Oniel (2011) that reported
health workers have positive attitude towards the care of the elderly. It is also in line with the

61
Oyetunde, Ojo and Ojewale (2013) opinion that there is positive attitude of health workers
towards the care of the elderly. The positive attitude of health workers towards the care of the
elderly in the study is probably due to high level of education and well trained health workers.
This is in accordance with Nelson (2004) who concluded that trained health workers are more
likely to develop positive attitude to the care of the elderly. And also agrees with Kaempfer,
Wellam & Himburg, (2002) that opines that the higher the level of education the more positive
the attitude towards the care of elderly among health workers.
However the findings also revealed that a large proportion of health workers also (68%)
agreed that caring for the elderly is difficult and stressful so they prefer to take care of younger
patients, than elderly people. Also the fact that taking care of the elderly is time consuming, and
that the mental state of the elderly affects their response to care. This agrees with Lee, (2007)
and Weiss (2005), that reported negative attitude of health workers towards the care of the
elderly could be due to the inability of the health workers to identify those conditions that can be
treated effectively as well as inadequate resource to treat. It also agrees with Okoye & Asa,
(2011) that concluded that health workers experience stress when caring for the elderly greatly
because it is time consuming and emotionally, physically and psychologically draining.
Findings from the study also revealed that majority of the health workers prefer taking
care of younger people. This could be because taking care of the elderly is time consuming and
stressful. This agrees with Weiss (2005) and Lee (2007) that reported that health workers show
negative attitude towards the elderly by using physical restrictions to disrespect the patient
autonomy and dignity and discriminate against them.
Research Question 3
What are the health workers practices in the provision of care towards the elderly.

62
The findings revealed that majority of health workers (81%) provided adequate care for
the elderly. The practices included nutritional assessment, thorough assessment during
emergency, evaluation and effective care, calling patient by name and creating a relationship.
These findings are due to the high level of education and specialization of the health workers.
This is in accordance with Lecovich (2008) that concluded that calling patient by their name is
one of the good behavioral practices of care of the elderly. It is also in line with Oyetunde, Ojo
and Ojewale (2013) that also concluded that nutritional assessment is an integral part of clinical
assessment for the elderly. However this finding disagrees with Sulaimen et al (2010) who still
emphasizes on the preservation of the family and value of taking care of their parents at home.
Research Question 4
What are the factors that influence health workers attitude towards the care of the elderly?
These findings revealed that most of the respondents (97%) agreed that taking care of the
elderly requires special training and those special wards should be created for the elderly
(geriatric wards). This finding is probably because the elderly have some peculiarities that would
require special care and also a cordoned area. The study also reveals that most of the health
workers would not prefer this area of specialization except when they are being forced to. This
agrees with Happel (2002), alliance for ageing research, (2003) and Bowen et al, (2008), whose
findings showed that identification of geriatrics as a career choice amongst health workers and
social care workers appear to be a long standing theme in literature.
HYPOTHESIS 1. There is no association between the years of experience of the health workers
and their attitude towards the care of the elderly.

63
The findings reveal that negative attitudes of health workers with mean years of
experience are statistically significant. With the item that health worker neglects themselves
when taking care of the elderly. Health workers with less years of experience strongly agreed
that they will neglect themselves while those with many years of experience disagreed.
This shows that there is association of attitude with many years of experience therefore rejects
the null hypothesis. There is association of mean years of experience with attitude of health
workers towards the care of the elderly. This may be due to the fact that the health workers with
lesser years of experience have not had enough experience of caring for the elderly. With
increased years of experience there may be improved attitude towards the care of the elderly.
Implication of Findings to Nursing
• Geriatric Nursing content in the curriculum to be strengthened.
• Consistent and frequent education programmes need to be implemented to address
knowledge gaps in contemporary Geriatric Nursing.
Limitation of the study
The study was conducted in University of Calabar Teaching Hospital, Calabar. This
means that there may not be much room for generalization because health workers in other
institutions may have different knowledge, attitude and practice of the care of the elderly. Also
only selected health workers in special professions were considered therefore the knowledge of
health workers in other disciplines of health were left out. Information was based on the
respondent’s perception which could have been influenced by other factors such as the time,
schedule, etc. Practice of health workers care was assessed by their knowledge on practice of
care, not by the process-outcome approach.
Summary

64
The study focused on the knowledge, Attitude and practice of care of the elderly patients among
health workers in University of Calabar Teaching Hospital, Calabar. The specific objectives were
to (i) determine the level of knowledge, the physical, emotional and social care of the elderly
patients in the University of Calabar Teaching Hospital, Calabar (ii) determine the attitude of
health workers in the care of the elderly patients, (iii) determine the level of health workers
practices in the provision of care of the elderly patients, (iv) identify factors that influence the
health workers attitude towards the elderly patients in University of Calabar Teaching Hospital,
Calabar. The hypothesis for the study tested the association between years of experience of
health workers and their attitude towards care of the elderly patients in UCTH. Calabar. The
study adopted a cross sectional descriptive design. The population of the study was 1023 health
workers, made up of 402 Doctors, 600 Nurses, 10 Dentists and 11 Physiotherapists that provided
direct clinical care to elderly patients. The sample was calculated using Taro-Yamane simplified
formula for finite population giving a sample of 461 health workers. The instrument for data
collection was questionnaire, the reliability of the instrument was done using test retest method
and a reliability co-efficient of 0.91 was obtained. The questionnaire had five sections, section A
covered socio demographic data, section B, C, D consisted of items which explored level of
knowledge. Attitude, practice and section E elicited information on factors influencing the care
of the elderly patients. The completed questionnaire was coded and analyzed using E.P.I info-7.
Descriptive statistics of percentage, mean, standard deviation were used for data analysis. The
criterion mean of 2.5 was also used and results the study revealed that 95% of the health workers
had good knowledge of care of the elderly patients. Majority of the health workers had positive
attitude above rating scale of 2.5. The health workers moderately practiced care of the elderly
patients. The factors that positively influenced health workers attitude to the care of the elderly

65
were years of experience, age and mental state of the elderly. There was significant association
(P<0.05) between attitude of Health Workers and mean years of experience. Workers with less
years of experience had negative attitude, while those with more years of experience had positive
attitude, towards the care of the elderly patients.
Conclusion
In conclusion, health care professionals need to have the right skills to manage a more
demanding role in the future. In order to offer effective services for the elderly patients, a skilled
workforce of health professionals is therefore very necessary.
Recommendations
Although the findings of the study show that health workers have good knowledge on the care of
the elderly, the attitude of the health workers was statistically significant with mean years of
experience i.e. the years of experience is associated with attitude of health workers. There is need
to provide more resources and also training of personnel in area of elderly care.
• Special wards / department should be created for the elderly in the hospitals with well
trained staff in the area of specialization.
The researcher also suggested that the government should develop a health policy for the elderly
that will capture the care of the elderly.
• Develop a system of periodical health workers evaluation to determine strategies of
upgrading their knowledge and enhancing practice.
• Development of follow up courses and in service training programs should be conducted
to maintain efficient performance of individuals previously trained in the care of the
elderly

66
• Encouraging health workers to attend national and international congresses, seminars
symposiums and workshops on care of the elderly.
Suggestion for further studies
The researcher suggests that similar study on the knowledge of care of the elderly should
be done in other health facilities in other States. Other studies that include the problems
associated with health workers attitude towards the care of the elderly.

67
REFERENCES
Abdulraheem I. S. and Parakoyi D.B. (2005) Improving Attitude towards Elderly People: Evaluation of an intervention Programme for Caregivers. Nigerian Journal Postgraduate Medical, (12),4 280-285.
Abyad A. (2001). Health Care for Older Persons: A Country Profile—Lebanon Journal of the
American Geriatrics Society. 1366–1370. Abyad A. (2006). Health care services for the elderly in the Middle East. The Middle East
journal of business. Administration and Aging U.S. Department of Health and Human Service. A profile of older Americans:
Adio-Moses, A. N, (2001) Pre-retirement education and improved welfare of retirees in some
selected industries in Lagos state Thesis, Dept. of Adult Education, University of Ibadan. Nigeria.
Alliance for Aging Research (2003) Ageism how healthcare fails the elderly. Alliance for aging
Research, Washington, D.C. available from http/www.agingresearch.org/ccontent/article/details/694
Aizheimer’s society (2009) Counting the cost: caring for people with Dementia in hospital
wards, Alzheimer’s society, London, UK. Aubrey de Gray D.N (2007) Life span extension. Research and public debate: societal
considerations (PDF) studies in Ethics, Law and Technology. ICI, Article 5 2202/1941-6008
Ayres, C. (2008). Mediators of the relationship between social support and positive health
practices among middle adolescents. Journal of Pediatric Healthcare, 22(2). 94-102. Beard R.L. (2004)In their voices: Identity preservation and experiences of Alzheimer's disease.
Journal of Aging Studies;18:415-428. Baum F. E, Ziersch A (2003) Social character department of public health. J. Epidemiology
community health 2003 57:320-323 do:10.1136/jech 57.5:320 Berger U, Dev. G, Mutrie N, Hannah Mk. (2005). The impact of retirement on physical activity.
Aging and society; 25: 181-195. Barman A, Snyder, S. J, Kozier .B, Erb. G (2008) Kozier and Erbs Fundamentals of Nursing 8
edition Pearson prentice Hall New Jersey 07458 Bowen, R. L, Atwood C. S [2004] Living and dying for sex. A theory of ageing based on
modulation of cell cycle signaling by productive hormones Gerontology 50[5]265-90.

68
Bowling A (2005) Ageing well: quality of life in old age. (Milton Keynes) Open University Press. ISBN 0-335-21509-2.
Bridges J. (2012) Meeting the acute care need of older people; the future is in our hands.
International Journal of older people Nursing. Blackwell Publishing LTDS. Brog C, Hallberg I R, Blomgrist K. (2006) Life satisfaction among older people (65th) with
reduced self-care capacity; relationship to social, health and financial aspects: J. Clin Nursing. 115, (5) 607-18.
Brown J, Nolan, M. Davis, S. and Keady J. (2008) Transforming students views of
gerontological nursing: Realizing the potential of ‘enriched’ environment of learning and care: a multi-method longitudinal study. International Journal of Nursing Studies, 45(8), 1214-1232.
Connolly, P. M. & Novak, J.M. (2007) Coping strategies used by parents of children with
autism, journal of the American Academy of Nurse Practitioners. 19(5):251-260. Csorba T, Bovi A, Dalmay T, Burgyan J.(2007) The P122 subunit of Tobacco Mosaic Virus
replicase is a potent silencing suppressor and compromises both small interfering RNA and Micro RNA-Mediated Pathways J. Virol. (81)11768-11780.
Courtney, M., Tong, S., & Walsh, A. (2000). Acute-care nurses' attitudes towards older patients:
A literature review. International Journal of Nursing Practice, 6(2), 62-69. Cummings, S. M., Kropf, N. P., & DeWeaver, K. L. (2000). Knowledge of and attitudes toward
ageing among non-elders: Gender and race differences. Journal of Women & Ageing, 12(1-2), 77-91.
Doherty M, Mitchell, E A, O’Neil Siobhan (2011) Attitude of healthcare workers towards older
people in rural population: A survey using the Kogan Scale. Nursing Research and practice. Article ID 352627 BT487JL, UK.
Donatelle J. R. (2011).The Basic-Health and Fitness : Pearson Education, Limited Reviewed
shttp//books:google.com Engstrom G and Fagerberg (2011) Attitude towards older people among Swedish health care
students and health care professionals working in elder care Doi http/dx’doi 10.4081/nurse rep. 2011.02
Essy, A. (2002) African union policy framework and plan of action on aging. Durban, African
union. 16-32 . Fitzgerald, J.T. Wray, L. A, Halter, J.B, Williams, B.C and Supiano, M. A. (2003). Relating
medical students knowledge, attitude and experience to an interest in geriatric medicine. The Gerontologist 43(6)849-855

69
Gallaghers S, Bennet M.K. and Halford J. C (2006). A comparism of acute and long term
health care personnel’s attitude toward older adults, international Journal of nursing practice Vol 12 (5) p- 273 – 279.
Gubrium N.Z. (2002) Violation of adult’s right. National Forum of Education Yaounde,
Ministry of Education. Happel, B. (2002) Nursing home employment for Nursing students: valuable experience or a
harsh deterrent? Journal of advanced Nursing 39(6),529-536. Harrison, V. O. (2005) Independent Adults, Chicago, Aldine. Hardman W, Kinmonth .A, Sutton .S (2009) and the proactive project team Theory of planned
behavior cognitions British Journal of Health Psychology (2009) 16:135-15 Herdman, E. (2002). Challenging the discourses of nursing ageism. International Journal of
Nursing Studies, 39(1), 105-114. Hoyer W. J and Roodin P.A (2003) Adult development and aging McGraw Hill Educate.
Com/sited 0857005774 Humphries, N; Brugha R, McGee H (2008) Overseas nurse recruitment: Ireland as an
illustration of the dynamic nature of migration “Health Policy, Vol. 87, No 2,pp 264-272. Isangedie D, Joshua M, Asim A & Ekuri E. (2004) Fundamentals of research and statistics,
Calabar, University Press. Iwasaki M. and Jones J. A. (2008) Attitude towards older adults: a reexamination of two major
scales Gerontology and Geriatrics Education, vol. 29, No 2, pp.139-157. Kaur, S, Kumar A, Kaur B, Ghai S, and Singla M. (2014) Knowledge and Attitude Regarding
Care of Elderly among Nursing students: an Indian prospectively. J. Nurse care 3:3 http//dx.doi.org/10 4172/2167-1168 1000161
Kaempfer, D., Wellman, N. S., & Himburg, S. P. (2002). Dietetics students low knowledge,
attitudes, and work preferences toward older adults indicate need for improved education about ageing. Journal of the American Dietetic Association, 102(2), 197-202.
Kogan N. (1961) Attitude toward old people: the development of a scale and an examination of
correlates. Journal of Abnormal & Social Psychology. ;62(1):44-54. Lambrinou, Esourtz. P Kalokerinou A, Lemonidou C. (2009). Attitudes and knowledge of the
greek nursing students towards older people. Nurse education today 29 (6), 617-622 doil 10/106

70
Lecovich E. (2008) Care giving Burden, community service and quality of life primary caregivers of frail elderly persons. Journal of applied Gerontology, 27:309-330.
Lee S.Y. (2006) Successful delivery of health information and education and overall health
management. Int J Med. Inform. 75 supp 2: S302-5 Lee, S Y (2009).The geographical dispersion of families and the tendency for women education
outside the home in Korea (http/www.mw.gokr) Lee, A.C.K, Wong, A.K.P and Loh, E.K.Y (2006) Score in the palmores Aging Quiz,
knowledge preference of undergraduate students toward the elderly in Hong Kong. Nurse Education Today 26(4),269-276.
Lee, S Y (2007) Interest in working with the elderly: A cross-national study of graduating social
work students. Journal of social work education 41(3), 379-391. Lee, S. Y, Hoerr, S.L, wealtherspoon, L and Schiffman, R.F (2008) Nutrition students improve
attitudes after a guided experimental with older adults. Journal of nutrition and behavior 40(5),279-287
Lee Y, Paik D, Bary S, Kary J, Chury B, Lee S, Bae E, Churg J, Kim J.(2008). Loss of spastic
paraplegias gare atlastin induces age dependent death of dopaminergic neurons in drosophilis. Neurobio Aging 29(1):84-94.
Lookinland S (2002). Perpetuation ofageist attitudes among present and future health care
personnel; implications for elder care. Journal of Advanced Nursing. Vol 21 (1) P 47 -56. Losada A, Perez-panaranda A, Rodrigue-sanchez E, Gome-z-Marcas M.A.-Rios C, Ramos-
Carrea IR, Campo da laTorre M A, Garcia-Ortiz L, (2009). Leisure and distress in caregivers for elderly patients. Archives of Gerontology and Gariatrics, 50:347-50.
Mandy D, Elizabeth A, M & O neils S. (2011); Attitudes of health care workers towards older
people in a rural population: a survey using the Kogan scale nursing research and practice vol 20, (11). 7
Mccormacks. B (2004) “Person centeredness in Gerontology nursing an overview of the
literature” journal of clinical Nursing. Vol. 13. No. 3pp31-38. Mclafferty I and Morisson F (2004). Attitude towards hospitalized older adults. Journal of
Advanced Nursing M 47 (4) p 466 -453 McMurdo M. E. (2000) A healthy old age: realistic or futile goal? BMJ 2000;321(7269)1149-
1151 Merill S.S and Verbrugge, L.M (2001) Health and disease in midlife. In S.L Willis and JD
Reids (Eds) life in the middle, San Diego. CA Academic Press.

71
Mellor P, Chew D, Greenhill J . (2007) Nurses Attitudes towards elderly people and knowledge
of gerontic care in a multipurpose health service (MPHS) Australian Journal of Advanced Nursing 24:37-41
Mitchell E.A, McCance T. (2010) Nurse patient encounter in the hospital ward, from the
perspective of older persons: consciousness framework. International Journal of Older People Nursing.
Moemeka, A. (2001) Local Radio: Community education for development. Zaria: Ahamadu
Bello University Press Ltd 18-28. Monteno D. and Kasprzyk (2008).The theory of reasoned action, the theory of planned behavior
and integrated behavioral model, in Glanz, K. M Rimer, B K and Viswanath, K. (Eds) Health behaviors and health education, theory research and practice, PP67-96, 4th Edition, San Francisco, Calfonia jossel Bass
Moyer A. E, Rodin J, Grilo C. M, Cummings N. L. M, & Rebufle-Scive M. (2011) Stress-
induced Cartsol response & fat distribution in women. Obesity Research, 2,255-261. Mullick. A (2005) Centre for inclusive Design and Environmental Access: Bathing for older
people with disability 73-81 National Centre for Protection of Older People (NCPOP)(2009): Public perception of older
people and ageing: a Literature Review : Review 1, Nov. 2009 UCN Dublin. National Council on Ageing and Older People (NCAOP)(2005b) Perception of ageism in health
and social service in Ireland (Report No. 85) Dublin. National Council on Ageing and Older People (NCAOP) 2005; Ageing and attitudes, ageing in
Ireland fact file No.3 Dublin Ireland National Population Commission (2008) Population census, projection Abuja Nigeria. National Population Commission, (2006) Population census of the Federal Republic of Nigeria:
Macro Preliminary Report. Nelson, T.D (2004) Ageism: Stereotyping and prejuidice against older persons, Cambridge,
MA; MIT press. Nur Asyura Adznam S, Shahar S,Rahman S.A, Yusof NA, Arshad F, Yassin Z, Salleh M,
Samah A. A & Sakian N. I (2009). An action research on Promotion of Health Ageing and Risk Reduction of chronic disease, a need assessment study among Rural Elderly Malays, care giver and health professionals J. N Health Aging 13 (10) 925 -30
Nussbaum, F.J (2003) Old people and their problems. Washington: Open University Press 26-
27

72
O’Neill D & O’Keeffe S (2003) Health Care for Older people in Ireland Journal of the
American Gematrics society, 51(9),1280-1286. O. Neil D. (2010) Leas Cross Report http//www.midstaffinquiry.com/assets/docs/inquirt-
report-vol.i.pdf
Olaleye, Y.L (2011) Socio Psychological Problems of the aged. jPsychologies. P41219(2) Okoye U.O and Asa S.S (2011) Caregiver and Stress: Experience of people Taking care of the
Elderly Relations in South Eastern Nigeria Arts and social sciences Journal Vol .( 2) Olayiwola I.O, Ketiku A.O (2006). Social demographic & nutritional improvement on the
elderly Yoruba in Nigeria. Pacific Journal of clinical Nutrition.;15:1:95-101. Olayiwola. I. O, Olusanya E. O, Ketiku A.O (2004) Nutritional vulnerability, food habit and
antwropometric indices of the elderly in the southwest of Nigeria. West Africa Journal of food & Nutrition ;7:1:46-52
Olise P, (2011) Essentials of Primary Health Care. For sustainable development printmarks
Ibadan. RA427.9.047. Olowookere, J (2003) Aging and the Keys longevity. Triumph providential publishers Nigeria:
82-88 Ife Oyetunde, M O. OJo. OO and Ojewale, LY (2013).Nurses attitude toward the care of the
elderly, implication for geroutological nursing training, journal of Nursing Education and practice 3:150-58
Papalia, D E, Sterns, HL, Feldman, RD, Camp, C.J (2002) Adult development and aging. Boston McGraw Hill.
Philips, J (2003) Caring for the elderly Australia, Parliament of Australia. 23-28 Population Reference Bureau, (2011) American’s Aging Population, Network of cities tackle
age-old problem, “Bulletin of the World Health Organization 88(2010): 406-07 Polit D. and Beck C , (2006) Essentials of Nursing Research; methods, appraisal and
utilization. 6th Edn. Lippincott Williams and Wilkins, Philadelphians. Redmond, B, Guerin, S and Devitt, C (2008) Attitudes, perception and concerns of social
worker: First two years of longitudinal study. Social Work Education: the International Journal, 27(8),868-882.
Sarrimaki A, and Stenbock – Hult B.(2000) Quality of life in old age described as a sense of
well-being meaning and value. J. Adv Nursing 2000:32:1025-35 (pub med)

73
Smith GC, Kohn S, J. Savage-Steven S. E, Finch J, J. Ingate R, Lim Y, (2000) The effects of interpersonal and personal agency or perceived control and psychological well being in adulthood Gerontologists. 40 (4) 458-68.
Soderhamn O, Lindercrona C, and Gustrarsson S M (2001). Attitude toward older people
among nursing students and registered nurses in Sweden, Nurse education today Vol 21 (3) p 225 -229
Stephens, J. K (2008). The role of social capital in overall health:www.urmc.rochester.edu Sulaiman M, Matta MJ, Sunderesan NR, Gupta MP, Pertasamy M, Gupta. (2010) Resuratrol, an
activator of SIRT1, up regulates sarcoplasmic calcium AT phase and improve cardiac function in diabetic cardiomyopathy. AM J physiol Heart circ physiol 2010; 298:1+833-843. Diabetic
Szucs TD (2001) Future disease burden in the elderly: rationale for economic planning.
Cardiovasc drugs there: 15: 359-361. Tan, P.P, Zhang, N.H. and Fan, L(2004) Students attitude towards the elderly in the people
Republic of China. Educational Gerontology, 30(40) 305-314 Ting G, and Woo J, (2009) Eldercare: is Legislation of family responsibility, the solution: Asian
Journal of Gerontology and Geriatrics Vol. 4 No. 2, 2009. Truven Health Analytics Information (2015) online. Twoy, R. Connolly P.M and Novak J. N (2007) Coping strategies used by parents of children
with autism article Vol 19. PP online Uchino, B. (2004) Social support and Physical Health: understanding the Health Consequences
of Relationships. New Haven. CT Yale University Press P.17 United Nations Population Division (2002) Projected growth in the global population aged 60
years and older -20 -25 in abuse of the elderly p 125. United Nations,(2004). Population facts on 2004/I. Department of Economic and Social
Affairs, Population Division. UN
United Nations, (2005). Population facts on 2005/12. Department of Economic and Social Affairs, population Division UN
Varice T (2010): Caring and the professional practice of nursing R N Journal. Vansina, W (2003) A shift from pedagogy to andragogy, Bemenda, Unique press. Vincent J. A, Patterson G, and Wale K (2001) Politics and old age: older citizens and political
processes in Britain, Ashgate, Hampshire, U.K.

74
Vitalianie P, Zhang T, scanlan JM, (2003); Is caregiving hazardous to one’s Physical health? A
meta-analysis. Psychology Bulletin 129:946-972. Weiss, I. (2005) Interest in working with the elderly: A cross-national study of graduating social
work students. Journal of social work education 41(3),379-391. Waweru I. M, Kabine, E, W. Mbutu J. N. and Some E. S. (2003): Health status and health
seeking behavior of the elderly person in Dagoreiti durisueri Nairobi East Africa Medical Journal, Vol. 20:2.
World Health Organization, (2004)International day of older persons: older people a new
perceptive for development. http//www.who.int/en World Health Organization (2005) Towards policy for health and aging
http/www.who.int/health. Settings/types/ageing/en/index.htm Windsor TD, Anstey KJ, Butterworth P, Luszcz, Andrews GR (2007) The role of perceived
control in explaining depressive symptoms associated with driving cessation in a longitudinal study “Gerontologist 47(2):215-23.
WPP (World Population Prospects); the 2002 Revision, Highlights. New York United Nations
Population Division 2003. (ESA/wp.186). Yamane, Taro,(1967)Statistics: An Introductory Analysis 2nd Ed. New York: Harper and Row.
APPENDIX 1
DEPARTMENT OF NURSING SCIENCE,
UNIVERSITY OF NIGERIA,
ENUGU CAMPUS.

75
SAMPLE QUESTIONNAIRE
Dear Respondents,
I am a Postgraduate Student in the Department of Nursing Sciences conducting a survey on
knowledge, attitude and practice of care of the elderly among health workers in the University of
Calabar Teaching Hospital, Calabar.
This survey seeks your views on knowledge, attitude and practice of care of the elderly.
The information will be treated with utmost confidentiality. The research will appreciate
genuine, direct, specific and clear answer.
Yours faithfully,
Mercy B. Efiong
SECTION A
INSTRUCTIONS
Please answer the following questions
Socio Demographic Data
1. What is your Age Range?
A. 20 - 29
B. 30 - 39
C. 40 - 49
D. 50 and above
2. Gender
A. Male [ ]
B. Female [ ]
3. Marital Status
A. Single [ ]
B. Married [ ]
4. Educational level

76
A. Primary [ ]
B. Secondary [ ]
C. Tertiary [ ]
D. None [ ]
5. What is your year(s) of experience-------
6. Professional status
A Doctor [ ]
B. Nurse [ ]
C. Dentists [ ]
D. Physiotherapist [ ]
7. Categories of elderly patient that you would like to care for by gender
a. Male [ ]
b. Female [ ]
SECTION B
Knowledge of Health Workers in the Care of the Elderly
Yes No
8 The elderly people need regular exercise. 9 Proper mouth care is a basic need for the elderly 10 Aging process will lead to anatomical and

77
physiological changes. 11 Railing and nonslip can Help maintain balance and
prevent falls in old age.
12 Elderly people need to eat regularly and properly. 13 Lung capacity tends to decline in old age. 14 The fear and anxiety related to inability to perform
usual roles by the elderly can be reduced by maintain calm, unhurried confident manner when interacting with the patient
15 Sound sleep in the elderly can be encouraged by restricting visitors during rest periods and providing care in groups
16 Bedsores in the elderly is prevented by keeping the skin clean and dry and bed lines wrinkle free and dry
17 Memorizing capability in the elderly person is affected due to structural changes in the brain
18 Care can be rendered to the elderly with altered sensory perception by reducing louder and slowly with nonverbal cues when appropriate
19 Sleep patterns among the elderly steadily increase compared to person under 60 years
20 Most of the elderly in Nigeria live above the poverty level
21 Elderly workers have the highest rates of absentism than younger workers
22 Majority of the elderly are able to adapt to change more easily compared to young people
23 As a healthy person reaches old age, his/her voluntary participation in organization usually declines
24 In Nigeria, majority of the elders whose children have left home suffer from empty nest syndrome
25 The elderly have more fear of crime compared to younger persons
SECTION C
Attitude of Nurses towards the care of the Elderly
Strongly
Agreed
Agreed Disagreed Strongly
Disagreed

78
SECTION D
Practice of Care of the Elderly by Health Workers
Always Sometimes Never
26 I feel good taking care of the elderly.
27 I see the care of the elderly patients
as being time consuming.
28 I prefer giving attention to younger
patients than the elderly ones.
29 The older the elderly the more
demanding he/she becomes.
30 Time should not be wasted for
elderly persons with terminal
illnesses.
31 The elderly do not deserve the care
health workers give them.
32 Some elderly look untidy and dirty.
And as such I do not like caring for
them.
33 The elderly can often provoke the
care giver.
34 The majority of the elderly are senile.
35 I get stressed up when taking care of
the elderly
36 Calling the patient by name when
treating or caring for the elderly is
very important

79
2 1 0
37 I like taking care of older people.
38 I attach titles to the names of the elderly
while taking care of them to create
relationship
39 I encourage the elderly to eat adequately
and at times assists in feeding them
40 Prompt attention is given to elderly
patients even in emergency
41 Assessment and evaluation are needed for
effective care.
Decreased mental ability of elderly
patients often by aging process and illness
affect response to care.
42 I get so stressed up when taking care of the
aged.
43 Taking care of the aged is time consuming.
44 I neglect myself and concentrate only on
the aged when taking care of them.
45 Categories of Elderly People you will like to care for by age
a. Young old (60 - 74)[ ]
b. Middle old (75 -84)[ ]
c. Old old (85 -94)[ ]
d. Oldest old (≥ - 95) [ ]
SECTION E
Factors influencing the Health Workers attitude towards the Care of the Elderly

80
Strongly
Agreed
Agreed Disagreed Strongly
Disagreed
46 I choose this department because I
like taking care of the aged.
47 Taking care of the aged is very
demanding.
48 Effective care of the elderly requires
special training
49 Hospitals should have special wards
i.e. geriatric wards for effective care
of the elderly
50 The health care policy of Nigeria has
made the care of the elderly difficult.
51 mental status of the elderly patients
affects their care and decision
making
52 Elderly patients exhibit different
behaviors which affect their care
53 It is difficult to persuade and
convince reluctant patient about their
care in the hospital
54 Some elderly are abandoned due to
lack of social support
APPENDIX II
Calculation for sample size

81
n = N 1+N(e)
For Doctors
n = 402 1+402(0.05)2 n = 402 2.005 n = 200 For Nurses n = N 1+N(e)2
n = 600 1+600(0.05)2 = 600 2.5 n = 240 For Dentist n = N 1+N(e)2
n = 10 1+10(0.05)2 n = 10 1.025 n = 9.7561 n = 10 For Physiotherapist n = N 1+N(e)2

82
n = 11 1+11(0.005)2 = 11 1.0275 = 10.7056
n = 11
Doctors = 200
Nurses = 240
Dentists = 10
Physiotherapist = 11 461
APPENDIX III

83
INFORMED CONSENT FORM
I agree to be participant in this study being conducted by Mrs. Mercy B. Efiong of the
Department of Nursing Sciences, university of Nigeria, Enugu Campus.
I have made this decision based on the information l have read in the information letter.
As a respondent in this study, I have realized that I will be asked to complete several
questionnaires. I may decline answering any question, if I so choose.
All information which I provide will be he in confidence and I will not be identified in
any way in the final report. I understand that I may withdraw this consent at any time by ceasing
to fill out the questionnaires
……………………………… ………………………… Signature and Date Signature and Date (Respondent) (Witness)
…………………………………………….. Signature and date
(Principal Investigator)

84
Appendix vii
Composition of Sample of Nurses used for the study
Composition of Doctors per Departments used for the study
Wards Surgical
ward (MS
Wsoopd)
Medical
ward
(FMMW)
MMW
MOP
Orthopedic
Ward and
Dental
ward
Eye ward
and Clinic
ENT ward
ENT Clinic
Family
Medical and
Casualty
Population 44 44 45 53 50 41
Sample of
Nurses
selected for
the study
40 40 40 40 40 40
Department Population Sample selected
Surgical ward/ Cardio Thoracic
ward/ intensive care unit
50 20
Internal Medicine/ Medical ward 46 20
Orthopedic ward 42 20
Eye ward and clinic 37 20
ENT ward and clinic 37 20
Family medicine 42 20
Casualty/ Accident and Emergency 41 20
Community Medicine 30 20
Obstetric and Gynecology 47 20
Dental clinic 30 20
Total 402 200