Embed Size (px)
Citation preview
J Cutan Pathol 2011: 38: 492–502doi: 10.1111/j.1600-0560.2011.01673.xJohn Wiley & Sons. Printed in Singapore
Copyright © 2011 John Wiley & Sons A/S
Journal ofCutaneous Pathology
EGFR in melanoma: clinicalsignificance and potential therapeutictarget
Background: The role of epidermal growth factor receptor (EGFR)has been established in a range of neoplasms. In melanoma, data onEGFR protein expression are conflicting. Fluorescence in situhybridization (FISH) analysis for EGFR gene expression in melanomashowed EGFR gene amplification to be linked with worse prognosis.Cetuximab has been shown to suppress the formation of metastasis inmice.Methods: EGFR protein expression and gene copy number statuswere evaluated by means of immunohistochemistry and FISH inmelanoma samples of patients with known clinicopathological data.Associations between EGFR expression and prognostic parameterswere investigated. The effect of different cetuximab concentrations onthe BLM melanoma cell line was evaluated by means of methyltetrazolium (MTT), sulforhodamine B (SRB) and Matrigel invasionassays.Results: EGFR protein expression was more frequently observed inpatients with a positive sentinel lymph node. However, EGFRimmunostaining has no predictive value. The presence of EGFRpolysomy was associated with thicker tumors. Treatment of the BLMmelanoma cell line with different concentrations of cetuximab reducedthe invasive capacity of the cells, but did not alter cell viability orgrowth.Conclusion: EGFR appears to be involved in progression andmetastasis of a subset of melanomas. Targeting EGFR could thereforerepresent a therapeutic option for these melanomas.
Keywords: cancer research, dermatopathology, malignant melanoma
Boone B, Jacobs K, Ferdinande L, Taildeman J, Lambert J, Peeters M,Bracke M, Pauwels P, Brochez L. EGFR in melanoma: clinicalsignificance and potential therapeutic target.J Cutan Pathol 2011; 38: 492–502. © 2011 John Wiley & Sons A/S.
Barbara Boone1, Koen Jacobs2,Liesbeth Ferdinande3, JasmienTaildeman3, Jo Lambert1, MarcPeeters4, Marc Bracke2,Patrick Pauwels3 andLieve Brochez1
1Department of Dermatology, UniversityHospital Ghent, Ghent, Belgium,2Department of Experimental Cancerology,University Hospital Ghent, Ghent, Belgium,3Department of Pathology, UniversityHospital Ghent, Ghent, Belgium, and4Department of Gastroenterology, UniversityHospital Ghent, Ghent, Belgium
Dr. Barbara Boone,Department of Dermatology,University Hospital Ghent, De Pintelaan 185,Ghent 9000, BelgiumTel: 00 329 332 2298Fax: 00 329 332 4996e-mail: [email protected]
Accepted for publication July 27, 2010
Malignant melanoma represents 4% of all cancercases and 1–2% of all cancer deaths in devel-oped countries. The disease mainly affects a youngpopulation. The lifetime risk is still increasing andmetastatic disease is refractory to all current forms oftherapy and has a very poor prognosis. The under-lying mechanisms driving melanoma developmentand progression have not been fully unraveled yet.
Melanoma appears to be a complex multigenic dis-ease, which is determined by several parallel andstepwise progressive pathways. Better understandingof molecules and pathways involved in melanomaprogression can contribute to better prognostic infor-mation and identification of possible new therapeutictargets. Within this scope, this article focused on theexamination of the clinical value of EGFR gene and
492

EGFR in melanoma
protein expression in melanoma tissue and on the invitro effect of the monoclonal anti-EGFR antibody,cetuximab, on cell viability, growth and invasivecapacity of a melanoma cell line.
The epidermal growth factor receptor (EGFR,ErbB1 or HER1) gene is located at chromosomalregion 7p12 and encodes a 170-kDa transmembranetyrosine kinase receptor, which is a member of theErbB family of receptor tyrosinase kinases (TKIs),including ErbB2 (HER2 or Neu), ErbB3 (HER3)and ErbB4 (HER4). Binding of ligands such asepidermal growth factor (EGF) or transforminggrowth factor-α (TGF-α) leads to homodimerizationor heterodimerization with another member of theHer family resulting in the activation of differentpathways.1 EGFR is of fundamental importancein the regulation of epithelial differentiation andproliferation.2 EGFR is often overexpressed inhuman carcinomas and in vitro and in vivo studieshave shown that these proteins are able to inducecell transformation.3 EGFR protein overexpressionhas been associated with tumor progression andpoor outcome in many human neoplasms.4 Geneticalterations important in carcinogenesis compriseEGFR gene amplification and mutations.5 Basedon these findings, a number of therapeutic strategiesinfluencing this receptor have been developed forcancer therapy. In particular, monoclonal antibodiestargeting the extracellular domain of the receptor(e.g. cetuximab, panitumumab) and small moleculesblocking tyrosine kinase activation (e.g. erlotinib,gefitinib) have already shown activity in clinical phaseI–III trials.6
EGFR immunoreactivity has been shown tobe present in non-pigmented, less-differentiatedmelanoma cell lines with epithelioid morphology.7
Increasing EGFR protein expression levels andintensity has been linked with the progression ofmelanocytic lesions in most studies,8– 10 whereas thishas been contradicted by others.11 An immuno-histochemical study performed in primary cuta-neous melanoma showed no consistent associationsbetween EGFR immunostaining and clinicopatho-logical phenotype.12
More recently, genetic studies using compara-tive genomic hybridization or fluorescence in situhybridization (FISH) have shown amplification ofchromosome 7 and the 7p12 region, including theEGFR gene, in a number of melanoma cases.13
Chromosome 7 gain has been associated with thickerlesions,14 reduced survival15 and has been shownto occur more frequently in melanoma metastasescompared to primary melanomas.16 A recent studyinvestigating EGFR gene alterations in melanomatissues showed EGFR amplification to be asso-ciated with the nodular subtype, thicker tumors,
ulceration and metastasis formation.13 Analysis ofthe hot-spot mutation on exon 19 of the EGFRgene in 27 primary melanomas was negative.13
Direct sequencing of EGFR (exons 18–21) in 156benign and malignant melanocytic lesions showed nomutations.12
In vitro treatment of the human melanoma cellline M24met with different anti-EGFR antibodiesshowed no effect on cell growth.17,18 Two of thethree monoclonal antibodies were able to induceantibody-dependent cellular cytotoxicity (ADCC) invitro. All antibodies induced suppression of sponta-neous melanoma metastasis of M24met in severecombined immune deficient (SCID) mice. In thisstudy, we evaluated the EGFR status in a largenumber of primary cutaneous melanoma tissues ofpatients with known clinicopathological follow-up bymeans of immunohistochemistry (IHC) and FISH.We investigated whether EGFR protein expressionand/or gene copy number was associated with clin-icopathological parameters and disease-free/overallsurvival. In addition, we investigated the in vitro effectof cetuximab on the viability, growth and invasivecapacity of an EGFR-expressing melanoma cell lineby means of methyl tetrazolium (MTT), sulforho-damine B (SRB) and Matrigel invasion assays.
Materials and methodsPatient and biopsy selectionPatients were identified retrospectively from themelanoma unit database of the dermatology depart-ment of the University Hospital Ghent, Belgium. Intotal, 114 patients, with known sentinel node status,who were diagnosed with melanoma between Jan-uary 1996 and August 2005, gave their informedconsent for their tissue material and clinical data tobe incorporated in the study database. The collectionof skin biopsies was performed after written informedconsent. The study was approved by the InstitutionalEthical Committee (project number: 2004/041) andwas conducted in accordance with institutionalguidelines on the Declaration of Helsinki principles.
ImmunohistochemistryFour-micrometer sections were prepared fromparaffin-embedded melanoma specimens. Sectionswere deparaffinized and subsequently slides wereloaded onto the Ventana autostainer (NexES, Ven-tana Medical Systems Inc, Tucson, AZ, USA)and stained with the iView DAB detection system(Ventana Medical Systems Inc) according to the man-ufacturer’s instructions. Antigen retrieval was per-formed using protease pretreatment (Ventana Med-ical Systems Inc). Sections were then incubated with
493

Boone et al.
anti-EGFR mouse monoclonal immunoglobulin G(IgG)1 antibody (Zymed Laboratories Inc, CA, USA;clone 31G7) for 32 min at 37◦C (1 : 100 dilution).Negative controls were performed by substituting theprimary antibody with irrelevant mouse IgG (ZymedLaboratories Inc). Immunostained sections wereviewed under an Axiophot microscope (Carl ZeissNV-SA, Zaventem, Belgium) at different magnifica-tions. Pictures were taken using a PixeLINK cameraand IrfanView software. All sections were investi-gated by three observers (BB, LF, PP), who wereblinded to the clinicopathological information of thepatient. EGFR immunoreactivity was scored as a per-centage of the total tumor area. Staining intensity wasscored as weak to moderate vs. strong. Attention waspaid to the intracellular distribution of EGFR expres-sion. Associations between EGFR immunostainingand clinicopathological parameters were analyzedusing the Mann–Whitney U and Fisher’s exact test.Kaplan–Meier survival analysis was used to obtainoverall survival and disease-free survival curves thatwere compared using the log-rank test.
FISH utilizing melanoma tissueDual-color FISH was performed on 114 melanomatissues with the Vysis LSI EGFR Dual Color probe(Abbott Molecular, IL, USA), which hybridizes tothe band region 7p12 in SpectrumOrange andthe centromere of chromosome 7 (7p11.1-q11.1,D7Z1 locus) in SpectrumGreen. FISH was carriedout according to the protocol of the supplier.Sections were viewed under a BX40 fluorescencemicroscope (Olympus, Aartselaar, Belgium) using a100× oil immersion lens and selective filters forthe detection of SpectrumGreen, SpectrumOrangeand 4′,6′-diamidino-2-phenylindole (DAPI) . Imageswere acquired with the Radiance 2100 confocalsystem mounted on a Nikon Diaphot 300 ona Carl Zeiss inverted microscope and collectedwith the Lasersharp 2000 software. The numberof hybridization signals for the EGFR gene andcep7 (chromosome 7) was assessed in 20 interphasenuclei. The average EGFR gene signals per cell wascalculated per sample and was called the EGFR genecopy number index. Similarly, the cep7 gene copynumber index was calculated. We then classified thetumors into six groups according to the frequencyof tumor cells with specific numbers of copies ofthe EGFR gene and chromosome 7 centromere.This classification is analogous to the one used ina large study investigating EGFR gene status in102 non-small cell lung cancer (NSCLC) patients.19
Categories in the present study were defined asfollows:
Disomy Two copies in ≥90% of cellsLow trisomy Two copies in ≥40% of cells, 3 copies in 10–40%
of cells, ≥4 copies in <10% of cellsHigh trisomy Two copies in ≥40% of cells, 3 copies in >40%
of cells, ≥4 copies in <10% of cellsLow polysomy ≥4 copies in 10–40% of cellsHigh polysomy ≥4 copies in >40% of cellsAmplification Ratio of EGFR gene copies/cep7 gene copies is
>2 in >10% of cellsor ≥15 EGFR gene copies in >10% of cells
Chromosome 7 polyploidy was defined as the pres-ence of >2 cep7 gene copies in more than 10% ofcells. Associations between EGFR gene alterationsand chromosome 7 ploidy status with clinicopatho-logical parameters and EGFR protein expressionwere analyzed using the Mann–Whitney U andFisher’s exact test. Kaplan–Meier survival analysiswas used to obtain overall survival and disease-free survival curves that were compared using thelog-rank test.
Cell cultureThe melanoma cell lines BLM, MeWo and HMB2were maintained in Dulbecco’s modified Eagle’smedium (DMEM), whereas G361 was cultured inRoswell Park Memorial Institute (RPMI) medium.Both media were supplemented with 10% heat-inactivated fetal bovine serum (Greiner Bio-One,Belgium), 100 IU/ml penicillin (NV InvitrogenSA, Merelbeke, Belgium), 100 μg/ml streptomycin(Invitrogen) and 2.5 μg/ml fungizone (Invitrogen).Cells were maintained as monolayer cultures at 37◦Cunder a humified atmosphere of 10% CO2. Cellswere passaged using 0.05% (w/v) trypsin and 0.02%(w/v) ethylenediaminetetraacetic acid (EDTA). Forthe experiments, cell cultures were harvested at80% confluency.
ReagentCetuximab (Erbitux, Merck) is a recombinant,human/mouse chimeric monoclonal antibody thatbinds specifically to the extracellular domain ofEGFR. It is composed of the Fv regions of a murineanti-EGFR antibody with human IgG1 heavy andkappa light chain. In the Matrigel, MTT and SRBassays, BLM melanoma cells were treated with cetux-imab at different concentrations (30, 300, 3000 nM).
Western blottingTotal cell lysate of the melanoma cells was solubi-lized and denaturated by boiling in 1×/4× Laemmlisample buffer, containing 5% β-mercaptoethanoland 5% bromophenol blue. Proteins were sepa-rated by sodium dodecyl sulfate-poly acrylamide
494

EGFR in melanoma
gel electrophoresis (SDS-PAGE) (6% gel) andelectroblotted onto nitrocellulose membranes (Amer-sham Biosciences UK Ltd, Buckinghamshire, UK).Membranes were blocked for 4 × 5 min in 5% non-fat dry milk dissolved in phosphate buffered saline D−(PBSD−) with 0.5% Tween-20, followed by an incu-bation at room temperature with anti-EGFR mousemonoclonal IgG1 primary antibody (Zymed Labo-ratories Inc; clone 31G7) at 1 : 1000 dilution during1 h. Following several washing steps with PBSD−and 0.5% Tween-20, membranes were incubatedwith a horseradish peroxidase (HRP)-conjugatedanti-mouse IgG secondary antibody (GE Healthcare,Diegem, Belgium, NXA931) at 1 : 3000 dilution dur-ing 30 min at room temperature. After final washingsteps with PBSD− and 0.5% Tween-20, proteinbands were visualized with the enhanced chemilumi-nescence detection kit (Amersham Biosciences UKLtd) according to the manufacturer’s protocol andthe membrane was exposed to X-ray films. To con-trol for equal loading of total lysates, immunostainingwith anti-tubulin antibody (Sigma-Aldrich, Bornem,Belgium) was performed routinely.
MTT cytotoxicity assayCell viability was assessed using the MTT assay.Metabolically active mitochondrial dehydrogenasesconvert the tetrazolium salt MTT to insoluble pur-ple formazan crystals at a rate that is proportionalto cell viability. The cultured BLM melanoma cellswere treated during 2 h with increasing concentra-tions of cetuximab (30, 300, 3000 nM). Afterwards,cells were seeded in 96-well plates. In a secondexperiment, cells were further cultured during 96 hafter cetuximab treatment and then seeded in the96-well plate in order to perform the assay. Twentymicroliters of MTT solution (Sigma, St. Louis, MO,USA) (5 mg/ml in PBS) was added to each well andplates were returned to incubate for 2 h at 37◦Cin the dark. Subsequently, the growth medium wastaken off and the formazan crystals were resuspendedin 200 μl dimethylsulfoxide (DMSO). The 490-nmabsorbance was read using a microplate reader(Molecular Devices, Sunnyvale, CA, USA). Relativecell viability (in percentage) was expressed as: (Abs490treated cells/Abs490 untreated cells) × 100. All exper-iments were performed in duplicate and repeatedthree times. Statistical significance was determinedby the paired Student’s t-test; p < 0.05 was consid-ered significant.
SRB growth inhibition assayThe SRB assay was performed to assess the growthinhibition of cetuximab to BLM melanoma cells. Cell
proliferation, measured as total protein synthesis, is avery sensitive toxicology marker. SRB is an anionicdye that binds to proteins electrostatically. The fixeddye, measured photometrically (490 nm) after solu-bilization, correlates with the total protein synthesisrate and therefore with cell proliferation. The cul-tured BLM melanoma cells were treated during 2 hwith increasing concentrations of cetuximab (30, 300,3000 nM). Afterwards, cells were seeded in 96-wellplates. In a second experiment, cells were furthercultured during 96 h after cetuximab treatment andthen seeded in the 96-well plate in order to performthe assay. Fifty microliters of a 50% trichoroaceticacid solution (Sigma) was added (1-h incubationat 4◦C) to assure fixation of the cells. Thereafter,plates were rinsed with water, dried and stained with200 μl of SRB (Sigma) solution per well (0.4% in1% ice acetic acid). After 30 min unbound dye wasremoved by rinsing with 1% ice acetic acid. Subse-quently, cell bound dye was extracted with Tris buffer(200 μl, 10 mM, pH 10.5) and determined photomet-rically on a microplate reader (Molecular Devices) at490 nm. Inhibition of growth was expressed as rel-ative viability (Abs490 treated cells/Abs490 untreatedcells) × 100. The experiments were performed induplicate and repeated three times. Statistical signif-icance was determined by the paired Student’s t-test;p< 0.05 was considered significant.
Invasion assayFor Matrigel invasion assay, transwell chambers withpolycarbonate membrane filters (6.5 mm diameter,8 μm pore size; Costar, Corning, NY, USA) werecoated with 20 μl of a Matrigel solution (BectonDickinson Benelux NV, Erembodegem, Belgium).BLM melanoma cells were exposed during 2 h toincreasing concentrations of cetuximab (30, 300,3000 nM). A total of 5 × 104 cells were addedto the upper compartment of the chamber. Inthe lower compartment, conditioned cell culturemedium of the MRC-5 human embryonic lungfibroblast cell line, containing high concentrations ofhepatocyte growth factor/scatter factor, was addedas a chemoattractant. After 24 h of incubation at37◦C, the upper surface of the filter was clearedfrom non-migratory cells with a cotton swab andwashes with serum-free DMEM. The remaining(invasive) cells at the lower surface of the filter werefixed with cold methanol and stained with 4′,6′-diamidino-2-phenylindole (Sigma-Aldrich). Blindedfor the treatment conditions, invasive cells werescored by counting 30 fields per filter with afluorescence microscope, at ×200 of magnification.Each experiment was performed in duplicate andrepeated three times. Statistical significance was
495
Boone et al.
determined by the paired Student’s t-test; p < 0.05was considered significant.
ResultsImmunohistochemistryPatient population
Patient characteristics are summarized in Table 1.
EGFR immunoreactivity in melanoma tissue
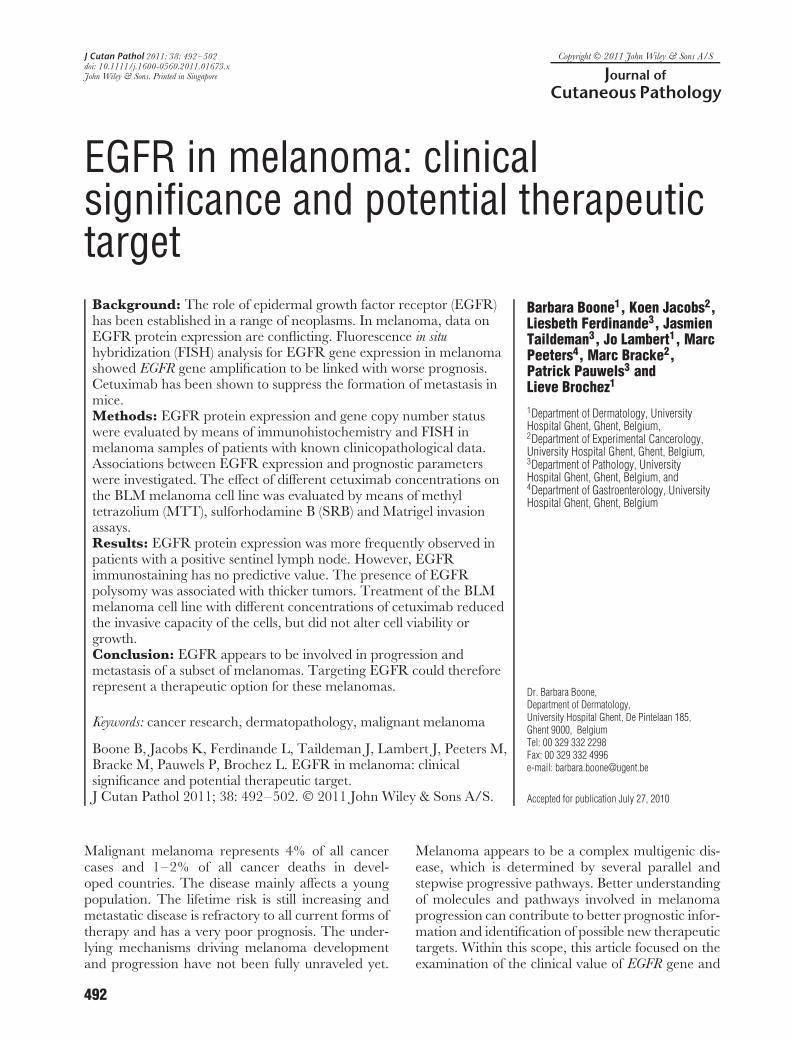
Immunohistochemical staining showed the percent-age of EGFR-positive tumor area to vary from 1 to70%. In analogy to a large study trial performed inNSCLC samples,20 positive staining was defined asthe presence of more than 10% of the total tumor areaexpressing EGFR, and was observed in 13 (11.4%)melanoma tissues. The staining intensity was weakto moderate in 7/13 samples and strong in 6/13samples. EGFR-expressing melanoma cells predom-inantly exhibited membranous staining and in 5/13samples an additional cytoplasmic EGFR expressionwas observed. Membranous EGFR immunoreac-tivity was consistently present in normal epithelium,which was used as an internal positive control (Fig. 1).
Associations between EGFR immunoreactivityand clinicopathological parameters
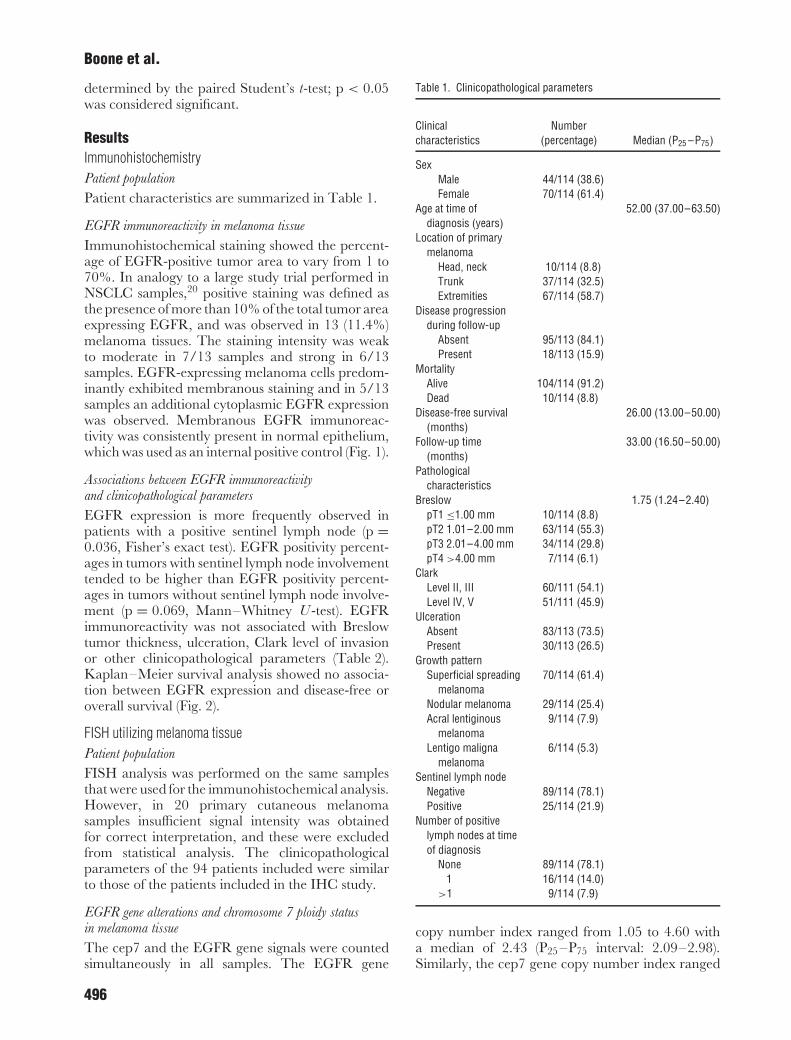
EGFR expression is more frequently observed inpatients with a positive sentinel lymph node (p =0.036, Fisher’s exact test). EGFR positivity percent-ages in tumors with sentinel lymph node involvementtended to be higher than EGFR positivity percent-ages in tumors without sentinel lymph node involve-ment (p = 0.069, Mann–Whitney U -test). EGFRimmunoreactivity was not associated with Breslowtumor thickness, ulceration, Clark level of invasionor other clinicopathological parameters (Table 2).Kaplan–Meier survival analysis showed no associa-tion between EGFR expression and disease-free oroverall survival (Fig. 2).
FISH utilizing melanoma tissuePatient population
FISH analysis was performed on the same samplesthat were used for the immunohistochemical analysis.However, in 20 primary cutaneous melanomasamples insufficient signal intensity was obtainedfor correct interpretation, and these were excludedfrom statistical analysis. The clinicopathologicalparameters of the 94 patients included were similarto those of the patients included in the IHC study.
EGFR gene alterations and chromosome 7 ploidy statusin melanoma tissue
The cep7 and the EGFR gene signals were countedsimultaneously in all samples. The EGFR gene
Table 1. Clinicopathological parameters
Clinicalcharacteristics
Number(percentage) Median (P25 –P75)
SexMale 44/114 (38.6)Female 70/114 (61.4)
Age at time ofdiagnosis (years)
52.00 (37.00–63.50)
Location of primarymelanoma
Head, neck 10/114 (8.8)Trunk 37/114 (32.5)Extremities 67/114 (58.7)
Disease progressionduring follow-up
Absent 95/113 (84.1)Present 18/113 (15.9)
MortalityAlive 104/114 (91.2)Dead 10/114 (8.8)
Disease-free survival(months)
26.00 (13.00–50.00)
Follow-up time(months)
33.00 (16.50–50.00)
Pathologicalcharacteristics
Breslow 1.75 (1.24–2.40)pT1 ≤1.00 mm 10/114 (8.8)pT2 1.01–2.00 mm 63/114 (55.3)pT3 2.01–4.00 mm 34/114 (29.8)pT4 >4.00 mm 7/114 (6.1)
ClarkLevel II, III 60/111 (54.1)Level IV, V 51/111 (45.9)
UlcerationAbsent 83/113 (73.5)Present 30/113 (26.5)
Growth patternSuperficial spreading
melanoma70/114 (61.4)
Nodular melanoma 29/114 (25.4)Acral lentiginous
melanoma9/114 (7.9)
Lentigo malignamelanoma
6/114 (5.3)
Sentinel lymph nodeNegative 89/114 (78.1)Positive 25/114 (21.9)
Number of positivelymph nodes at timeof diagnosis
None 89/114 (78.1)1 16/114 (14.0)
>1 9/114 (7.9)
copy number index ranged from 1.05 to 4.60 witha median of 2.43 (P25 –P75 interval: 2.09–2.98).Similarly, the cep7 gene copy number index ranged
496
EGFR in melanoma
Fig. 1. EGFR immunostaining in melanoma sections. (A, B) The EGFR protein is strongly expressed in the epithelium. Melanoma cells revealmembranous EGFR immunoreactivity with weak to moderate staining intensity. (C, D) A strong cytoplasmic EGFR staining was observed inthe melanoma cell nests of a patient with a positive sentinel lymph node. Original magnification 100× (A, C), 400× (B) and 200× (D).
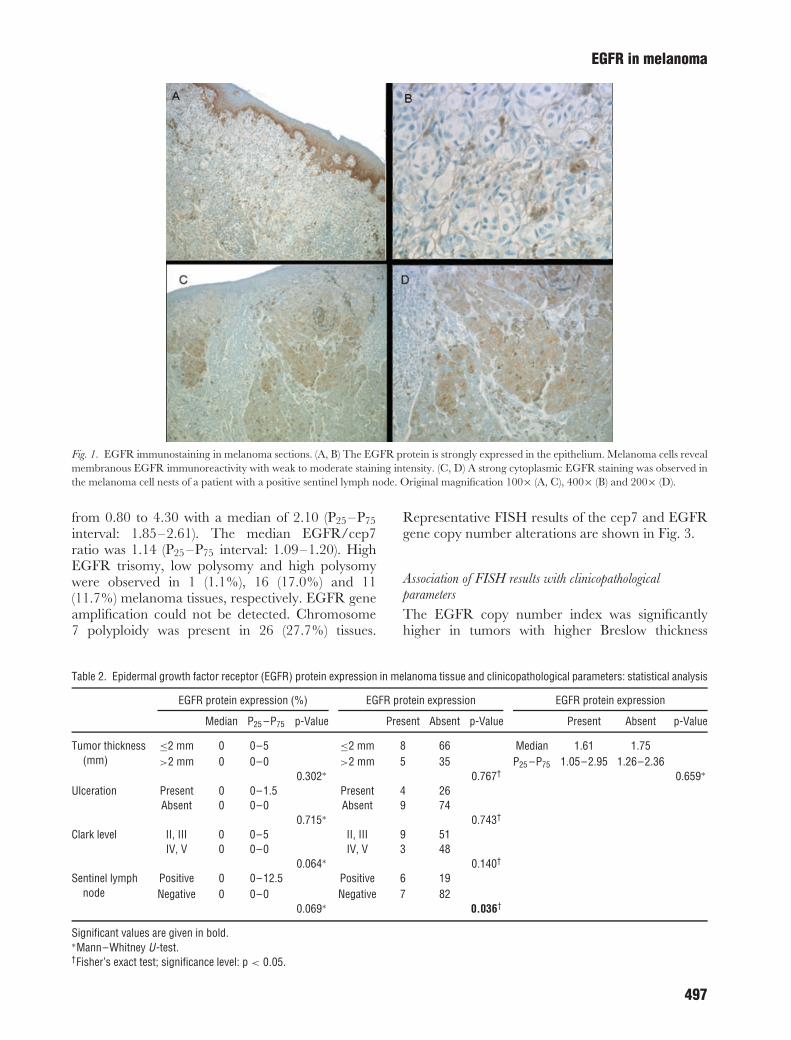
from 0.80 to 4.30 with a median of 2.10 (P25 –P75interval: 1.85–2.61). The median EGFR/cep7ratio was 1.14 (P25 –P75 interval: 1.09–1.20). HighEGFR trisomy, low polysomy and high polysomywere observed in 1 (1.1%), 16 (17.0%) and 11(11.7%) melanoma tissues, respectively. EGFR geneamplification could not be detected. Chromosome7 polyploidy was present in 26 (27.7%) tissues.
Representative FISH results of the cep7 and EGFRgene copy number alterations are shown in Fig. 3.
Association of FISH results with clinicopathologicalparameters
The EGFR copy number index was significantlyhigher in tumors with higher Breslow thickness
Table 2. Epidermal growth factor receptor (EGFR) protein expression in melanoma tissue and clinicopathological parameters: statistical analysis
EGFR protein expression (%) EGFR protein expression EGFR protein expression
Median P25 –P75 p-Value Present Absent p-Value Present Absent p-Value
Tumor thickness(mm)
≤2 mm 0 0–5 ≤2 mm 8 66 Median 1.61 1.75>2 mm 0 0–0 >2 mm 5 35 P25 –P75 1.05–2.95 1.26–2.36
0.302∗ 0.767† 0.659∗
Ulceration Present 0 0–1.5 Present 4 26Absent 0 0–0 Absent 9 74
0.715∗ 0.743†
Clark level II, III 0 0–5 II, III 9 51IV, V 0 0–0 IV, V 3 48
0.064∗ 0.140†
Sentinel lymphnode
Positive 0 0–12.5 Positive 6 19Negative 0 0–0 Negative 7 82
0.069∗ 0.036†
Significant values are given in bold.∗Mann–Whitney U-test.†Fisher’s exact test; significance level: p < 0.05.
497
Boone et al.
Fig. 2. Epidermal growth factor receptor (EGFR) expression in melanoma tissue vs. overall and disease-free survival.
Fig. 3. Epidermal growth factor receptor (EGFR) by fluorescencein situ hybridization (FISH) analysis in melanomo sections. EGFRgene-specific probe was labeled with SpectrumOrange (appearingas red signals) and chromosome 7 centromeric probe was labeledwith SpectrumGreen (appearing as green signals), cell nuclei werelabeled with blue fluorescent DAPI. A and B) EGFR gene disomy,(C and D) EGFR gene polysomy. Original magnification 2580×(A) and 2940× (C).
(median of 2.75 in tumors thicker than 2.00 mm vs.2.35 in tumors thinner or equal to 2.00 mm,p = 0.024, Mann–Whitney U -test). In addition,the presence of EGFR polysomy (high trisomy, lowpolysomy or high polysomy) in primary cutaneousmelanoma samples was also associated with thickertumors (p = 0.019, Fisher’s exact test). The medianBreslow thickness in melanoma tissues with EGFRpolysomy was 2.11, whereas it was only 1.73in the absence of EGFR polysomy (p = 0.042,Mann–Whitney U -test). No differences in Breslow
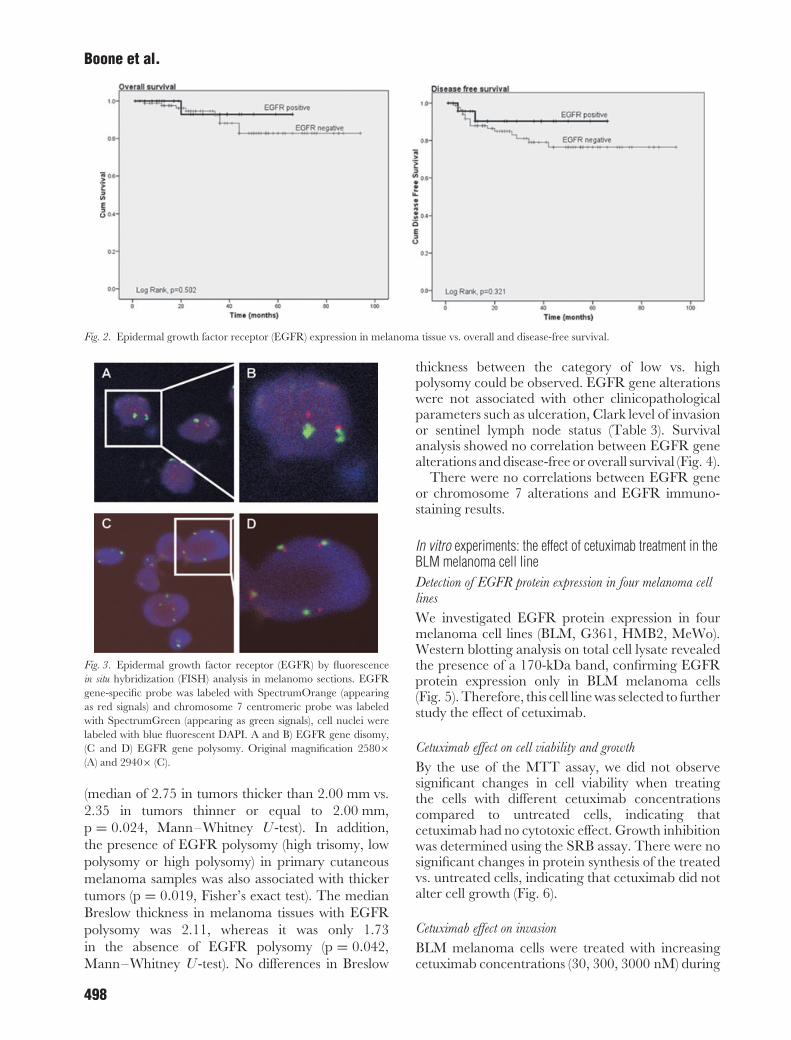
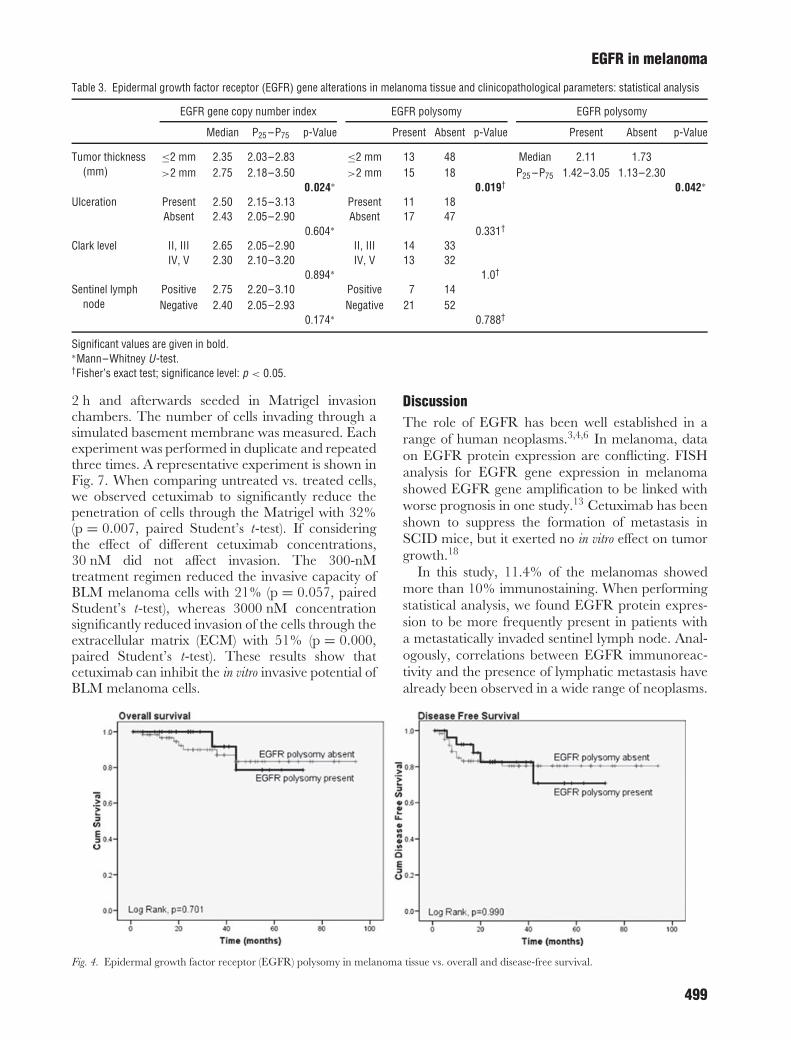
thickness between the category of low vs. highpolysomy could be observed. EGFR gene alterationswere not associated with other clinicopathologicalparameters such as ulceration, Clark level of invasionor sentinel lymph node status (Table 3). Survivalanalysis showed no correlation between EGFR genealterations and disease-free or overall survival (Fig. 4).
There were no correlations between EGFR geneor chromosome 7 alterations and EGFR immuno-staining results.
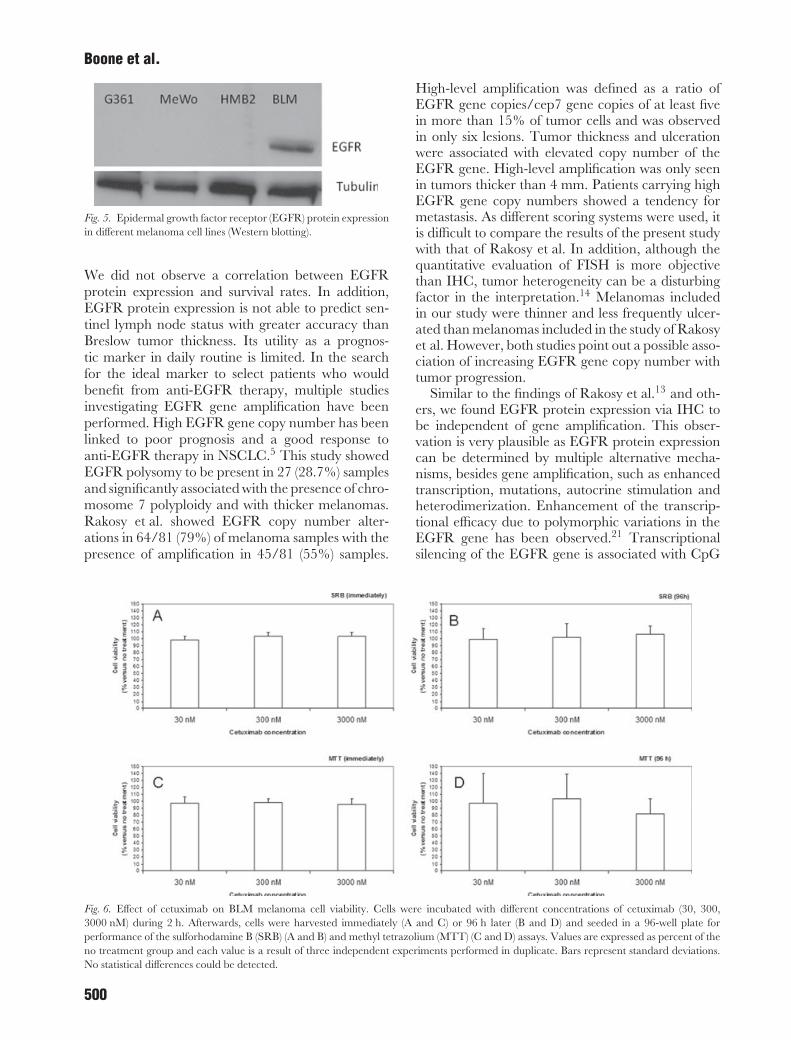
In vitro experiments: the effect of cetuximab treatment in theBLM melanoma cell lineDetection of EGFR protein expression in four melanoma celllines
We investigated EGFR protein expression in fourmelanoma cell lines (BLM, G361, HMB2, MeWo).Western blotting analysis on total cell lysate revealedthe presence of a 170-kDa band, confirming EGFRprotein expression only in BLM melanoma cells(Fig. 5). Therefore, this cell line was selected to furtherstudy the effect of cetuximab.
Cetuximab effect on cell viability and growth
By the use of the MTT assay, we did not observesignificant changes in cell viability when treatingthe cells with different cetuximab concentrationscompared to untreated cells, indicating thatcetuximab had no cytotoxic effect. Growth inhibitionwas determined using the SRB assay. There were nosignificant changes in protein synthesis of the treatedvs. untreated cells, indicating that cetuximab did notalter cell growth (Fig. 6).
Cetuximab effect on invasion
BLM melanoma cells were treated with increasingcetuximab concentrations (30, 300, 3000 nM) during
498
EGFR in melanoma
Table 3. Epidermal growth factor receptor (EGFR) gene alterations in melanoma tissue and clinicopathological parameters: statistical analysis
EGFR gene copy number index EGFR polysomy EGFR polysomy
Median P25 –P75 p-Value Present Absent p-Value Present Absent p-Value
Tumor thickness(mm)
≤2 mm 2.35 2.03–2.83 ≤2 mm 13 48 Median 2.11 1.73>2 mm 2.75 2.18–3.50 >2 mm 15 18 P25 –P75 1.42–3.05 1.13–2.30
0.024∗ 0.019† 0.042∗
Ulceration Present 2.50 2.15–3.13 Present 11 18Absent 2.43 2.05–2.90 Absent 17 47
0.604∗ 0.331†
Clark level II, III 2.65 2.05–2.90 II, III 14 33IV, V 2.30 2.10–3.20 IV, V 13 32
0.894∗ 1.0†
Sentinel lymphnode
Positive 2.75 2.20–3.10 Positive 7 14Negative 2.40 2.05–2.93 Negative 21 52
0.174∗ 0.788†
Significant values are given in bold.∗Mann–Whitney U-test.†Fisher’s exact test; significance level: p < 0.05.
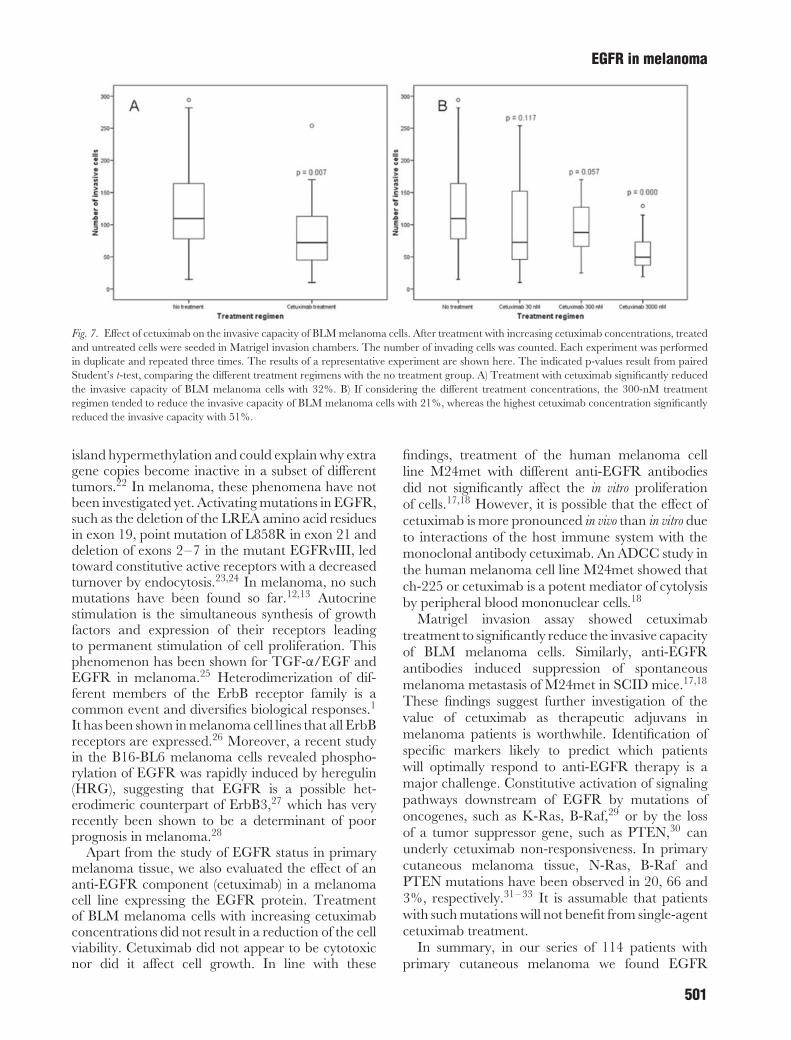
2 h and afterwards seeded in Matrigel invasionchambers. The number of cells invading through asimulated basement membrane was measured. Eachexperiment was performed in duplicate and repeatedthree times. A representative experiment is shown inFig. 7. When comparing untreated vs. treated cells,we observed cetuximab to significantly reduce thepenetration of cells through the Matrigel with 32%(p = 0.007, paired Student’s t-test). If consideringthe effect of different cetuximab concentrations,30 nM did not affect invasion. The 300-nMtreatment regimen reduced the invasive capacity ofBLM melanoma cells with 21% (p = 0.057, pairedStudent’s t-test), whereas 3000 nM concentrationsignificantly reduced invasion of the cells through theextracellular matrix (ECM) with 51% (p = 0.000,paired Student’s t-test). These results show thatcetuximab can inhibit the in vitro invasive potential ofBLM melanoma cells.
DiscussionThe role of EGFR has been well established in arange of human neoplasms.3,4,6 In melanoma, dataon EGFR protein expression are conflicting. FISHanalysis for EGFR gene expression in melanomashowed EGFR gene amplification to be linked withworse prognosis in one study.13 Cetuximab has beenshown to suppress the formation of metastasis inSCID mice, but it exerted no in vitro effect on tumorgrowth.18
In this study, 11.4% of the melanomas showedmore than 10% immunostaining. When performingstatistical analysis, we found EGFR protein expres-sion to be more frequently present in patients witha metastatically invaded sentinel lymph node. Anal-ogously, correlations between EGFR immunoreac-tivity and the presence of lymphatic metastasis havealready been observed in a wide range of neoplasms.
Fig. 4. Epidermal growth factor receptor (EGFR) polysomy in melanoma tissue vs. overall and disease-free survival.
499
Boone et al.
Fig. 5. Epidermal growth factor receptor (EGFR) protein expressionin different melanoma cell lines (Western blotting).
We did not observe a correlation between EGFRprotein expression and survival rates. In addition,EGFR protein expression is not able to predict sen-tinel lymph node status with greater accuracy thanBreslow tumor thickness. Its utility as a prognos-tic marker in daily routine is limited. In the searchfor the ideal marker to select patients who wouldbenefit from anti-EGFR therapy, multiple studiesinvestigating EGFR gene amplification have beenperformed. High EGFR gene copy number has beenlinked to poor prognosis and a good response toanti-EGFR therapy in NSCLC.5 This study showedEGFR polysomy to be present in 27 (28.7%) samplesand significantly associated with the presence of chro-mosome 7 polyploidy and with thicker melanomas.Rakosy et al. showed EGFR copy number alter-ations in 64/81 (79%) of melanoma samples with thepresence of amplification in 45/81 (55%) samples.
High-level amplification was defined as a ratio ofEGFR gene copies/cep7 gene copies of at least fivein more than 15% of tumor cells and was observedin only six lesions. Tumor thickness and ulcerationwere associated with elevated copy number of theEGFR gene. High-level amplification was only seenin tumors thicker than 4 mm. Patients carrying highEGFR gene copy numbers showed a tendency formetastasis. As different scoring systems were used, itis difficult to compare the results of the present studywith that of Rakosy et al. In addition, although thequantitative evaluation of FISH is more objectivethan IHC, tumor heterogeneity can be a disturbingfactor in the interpretation.14 Melanomas includedin our study were thinner and less frequently ulcer-ated than melanomas included in the study of Rakosyet al. However, both studies point out a possible asso-ciation of increasing EGFR gene copy number withtumor progression.
Similar to the findings of Rakosy et al.13 and oth-ers, we found EGFR protein expression via IHC tobe independent of gene amplification. This obser-vation is very plausible as EGFR protein expressioncan be determined by multiple alternative mecha-nisms, besides gene amplification, such as enhancedtranscription, mutations, autocrine stimulation andheterodimerization. Enhancement of the transcrip-tional efficacy due to polymorphic variations in theEGFR gene has been observed.21 Transcriptionalsilencing of the EGFR gene is associated with CpG
Fig. 6. Effect of cetuximab on BLM melanoma cell viability. Cells were incubated with different concentrations of cetuximab (30, 300,3000 nM) during 2 h. Afterwards, cells were harvested immediately (A and C) or 96 h later (B and D) and seeded in a 96-well plate forperformance of the sulforhodamine B (SRB) (A and B) and methyl tetrazolium (MTT) (C and D) assays. Values are expressed as percent of theno treatment group and each value is a result of three independent experiments performed in duplicate. Bars represent standard deviations.No statistical differences could be detected.
500
EGFR in melanoma
Fig. 7. Effect of cetuximab on the invasive capacity of BLM melanoma cells. After treatment with increasing cetuximab concentrations, treatedand untreated cells were seeded in Matrigel invasion chambers. The number of invading cells was counted. Each experiment was performedin duplicate and repeated three times. The results of a representative experiment are shown here. The indicated p-values result from pairedStudent’s t-test, comparing the different treatment regimens with the no treatment group. A) Treatment with cetuximab significantly reducedthe invasive capacity of BLM melanoma cells with 32%. B) If considering the different treatment concentrations, the 300-nM treatmentregimen tended to reduce the invasive capacity of BLM melanoma cells with 21%, whereas the highest cetuximab concentration significantlyreduced the invasive capacity with 51%.
island hypermethylation and could explain why extragene copies become inactive in a subset of differenttumors.22 In melanoma, these phenomena have notbeen investigated yet. Activating mutations in EGFR,such as the deletion of the LREA amino acid residuesin exon 19, point mutation of L858R in exon 21 anddeletion of exons 2–7 in the mutant EGFRvIII, ledtoward constitutive active receptors with a decreasedturnover by endocytosis.23,24 In melanoma, no suchmutations have been found so far.12,13 Autocrinestimulation is the simultaneous synthesis of growthfactors and expression of their receptors leadingto permanent stimulation of cell proliferation. Thisphenomenon has been shown for TGF-α/EGF andEGFR in melanoma.25 Heterodimerization of dif-ferent members of the ErbB receptor family is acommon event and diversifies biological responses.1
It has been shown in melanoma cell lines that all ErbBreceptors are expressed.26 Moreover, a recent studyin the B16-BL6 melanoma cells revealed phospho-rylation of EGFR was rapidly induced by heregulin(HRG), suggesting that EGFR is a possible het-erodimeric counterpart of ErbB3,27 which has veryrecently been shown to be a determinant of poorprognosis in melanoma.28
Apart from the study of EGFR status in primarymelanoma tissue, we also evaluated the effect of ananti-EGFR component (cetuximab) in a melanomacell line expressing the EGFR protein. Treatmentof BLM melanoma cells with increasing cetuximabconcentrations did not result in a reduction of the cellviability. Cetuximab did not appear to be cytotoxicnor did it affect cell growth. In line with these
findings, treatment of the human melanoma cellline M24met with different anti-EGFR antibodiesdid not significantly affect the in vitro proliferationof cells.17,18 However, it is possible that the effect ofcetuximab is more pronounced in vivo than in vitro dueto interactions of the host immune system with themonoclonal antibody cetuximab. An ADCC study inthe human melanoma cell line M24met showed thatch-225 or cetuximab is a potent mediator of cytolysisby peripheral blood mononuclear cells.18
Matrigel invasion assay showed cetuximabtreatment to significantly reduce the invasive capacityof BLM melanoma cells. Similarly, anti-EGFRantibodies induced suppression of spontaneousmelanoma metastasis of M24met in SCID mice.17,18
These findings suggest further investigation of thevalue of cetuximab as therapeutic adjuvans inmelanoma patients is worthwhile. Identification ofspecific markers likely to predict which patientswill optimally respond to anti-EGFR therapy is amajor challenge. Constitutive activation of signalingpathways downstream of EGFR by mutations ofoncogenes, such as K-Ras, B-Raf,29 or by the lossof a tumor suppressor gene, such as PTEN,30 canunderly cetuximab non-responsiveness. In primarycutaneous melanoma tissue, N-Ras, B-Raf andPTEN mutations have been observed in 20, 66 and3%, respectively.31– 33 It is assumable that patientswith such mutations will not benefit from single-agentcetuximab treatment.
In summary, in our series of 114 patients withprimary cutaneous melanoma we found EGFR
501

Boone et al.
protein expression to be associated with a positivesentinel lymph node but not with survival. The pres-ence of EGFR polysomy was linked to thicker tumorsbut was not predictive of survival. Treatment ofthe EGFR-expressing BLM melanoma cell line withdifferent concentrations of cetuximab reduced theinvasive capacity of the cells, but did not alter cellviability or growth. These results point out a possiblerole for EGFR in melanoma progression and metas-tasis. Further investigation of the value of anti-EGFRas a therapeutic adjuvant is worthwhile even if this isonly suitable in a selected patient subgroup.
AcknowledgementsThe authors thank Mrs R. Heyse, Mrs S. D’Hont and Mrs A.Nuyts for their technical support and assistance in completing thisstudy. Barbara Boone is a research fellow of the Fund for ScientificResearch-Flanders. This work was also financially supported by theFund for Scientific Research-Flanders (grant number G.0128.06).Koen Jacobs was supported by a doctoral grant from the Institutefor the Promotion of Innovation through Science and Technologyin Flanders (IWT-Vlaanderen, SB/63065). Jasmien Taildeman wassupported by a doctoral grant from the Institute for the Promotionof Innovation through Science and Technology in Flanders (IWT-Vlaanderen, SB/33271) and by a grant of the Research Council ofthe Ghent University (GOA B/05975/01).
References1. Riese DJ II, Stern DF. Specificity within the
EGF family/ErbB receptor family signalingnetwork. Bioessays 1998; 20: 41.
2. Miettinen PJ, Berger JE, Meneses J, et al.Epithelial immaturity and multiorgan fail-ure in mice lacking epidermal growth factorreceptor. Nature 1995; 376: 337.
3. Normanno N, De Luca A, Bianco C, et al.Epidermal growth factor receptor (EGFR)signaling in cancer. Gene 2006; 366: 2.
4. Nicholson RI, Gee JM, Harper ME. EGFRand cancer prognosis. Eur J Cancer 2001; 37(Suppl. 4): S9.
5. Sequist LV, Bell DW, Lynch TJ, Haber DA.Molecular predictors of response to epidermalgrowth factor receptor antagonists in non-small-cell lung cancer. J Clin Oncol 2007; 25:587.
6. Rowinsky EK. The erbB family: targets fortherapeutic development against cancer andtherapeutic strategies using monoclonal anti-bodies and tyrosine kinase inhibitors. AnnuRev Med 2004; 55: 433.
7. Real FX, Rettig WJ, Chesa PG, MelamedMR, Old LJ, Mendelsohn J. Expression ofepidermal growth factor receptor in humancultured cells and tissues: relationship to celllineage and stage of differentiation. CancerRes 1986; 46: 4726.
8. Elder DE, Rodeck U, Thurin J, et al. Anti-genic profile of tumor progression stages inhuman melanocytic nevi and melanomas.Cancer Res 1989; 49: 5091.
9. de Wit PE, Moretti S, Koenders PG, et al.Increasing epidermal growth factor receptorexpression in human melanocytic tumor pro-gression. J Invest Dermatol 1992; 99: 168.
10. Sparrow LE, Heenan PJ. Differential expres-sion of epidermal growth factor receptorin melanocytic tumors demonstrated byimmunohistochemistry and mRNA in situhybridization. Australas J Dermatol 1999;40: 19.
11. Ellis DL, King LE Jr, Nanney LB. Increasedepidermal growth factor receptors inmelanocytic lesions. J Am Acad Dermatol1992; 27: 539.
12. Akslen LA, Puntervoll H, Bachmann IM,et al. Mutation analysis of the EGFR-NRAS-BRAF pathway in melanomas from black
Africans and other subgroups of cutaneousmelanoma. Melanoma Res 2008; 18: 29.
13. Rakosy Z, Vizkeleti L, Ecsedi S, et al. EGFRgene copy number alterations in primary cuta-neous malignant melanomas are associatedwith poor prognosis. Int J Cancer 2007; 121:1729.
14. Bastian BC, LeBoit PE, Hamm H, BrockerEB, Pinkel D. Chromosomal gains and lossesin primary cutaneous melanomas detected bycomparative genomic hybridization. CancerRes 1998; 58: 2170.
15. Trent JM, Meyskens FL, Salmon SE, et al.Relation of cytogenetic abnormalities andclinical outcome in metastatic melanoma. NEngl J Med 1990; 322: 1508.
16. Udart M, Utikal J, Krahn GM, Peter RU.Chromosome 7 aneusomy. A marker formetastatic melanoma? Expression of the epi-dermal growth factor receptor gene andchromosome 7 aneusomy in nevi, primarymalignant melanomas and metastases. Neo-plasia 2001; 3: 245.
17. Mueller BM, Romerdahl CA, Trent JM,Reisfeld RA. Suppression of spontaneousmelanoma metastasis in SCID mice withan antibody to the epidermal growth factorreceptor. Cancer Res 1991; 51: 2193.
18. Naramura M, Gillies SD, Mendelsohn J, Reis-feld RA, Mueller BM. Therapeutic poten-tial of chimeric and murine anti-(epidermalgrowth factor receptor) antibodies in a metas-tasis model for human melanoma. CancerImmunol Immunother 1993; 37: 343.
19. Cappuzzo F, Hirsch FR, Rossi E, et al. Epi-dermal growth factor receptor gene and pro-tein and gefitinib sensitivity in non-small-celllung cancer. J Natl Cancer Inst 2005; 97:643.
20. Tsao MS, Sakurada A, Cutz JC, et al.Erlotinib in lung cancer – molecular and clini-cal predictors of outcome. N Engl J Med 2005;353: 133.
21. Liu W, Innocenti F, Wu MH, et al. A func-tional common polymorphism in a Sp1 recog-nition site of the epidermal growth factorreceptor gene promoter. Cancer Res 2005;65: 46.
22. Montero AJ, Diaz-Montero CM, Mao L,et al. Epigenetic inactivation of EGFR by
CpG island hypermethylation in cancer. Can-cer Biol Ther 2006; 5: 1494.
23. Shtiegman K, Kochupurakkal BS, Zwang Y,et al. Defective ubiquitinylation of EGFRmutants of lung cancer confers prolongedsignaling. Oncogene 2007; 26: 6968.
24. Grandal MV, Zandi R, Pedersen MW,Willumsen BM, van Deurs B, Poulsen HS.EGFRvIII escapes down-regulation dueto impaired internalization and sortingto lysosomes. Carcinogenesis 2007; 28:1408.
25. Mattei S, Colombo MP, Melani C, SilvaniA, Parmiani G, Herlyn M. Expression ofcytokine/growth factors and their receptorsin human melanoma and melanocytes. IntJ Cancer 1994; 56: 853.
26. Gordon-Thomson C, Jones J, Mason RS,Moore GP. ErbB receptors mediate bothmigratory and proliferative activities inhuman melanocytes and melanoma cells.Melanoma Res 2005; 15: 21.
27. Ueno Y, Sakurai H, Tsunoda S, et al.Heregulin-induced activation of ErbB3 byEGFR tyrosine kinase activity promotestumor growth and metastasis in melanomacells. Int J Cancer 2008; 123: 340.
28. Reschke M, Mihic-Probst D, van derHorst EH, et al. HER3 is a determinant forpoor prognosis in melanoma. Clin Cancer Res2008; 14: 5188.
29. Benvenuti S, Sartore-Bianchi A, DiNicolantonio F, et al. Oncogenic activationof the RAS/RAF signaling pathway impairsthe response of metastatic colorectal cancersto anti-epidermal growth factor receptor anti-body therapies. Cancer Res 2007; 67: 2643.
30. Frattini M, Saletti P, Romagnani E, et al.PTEN loss of expression predicts cetux-imab efficacy in metastatic colorectal cancerpatients. Br J Cancer 2007; 97: 1139.
31. Whitwam T, Vanbrocklin MW, Russo ME,et al. Differential oncogenic potential of acti-vated RAS isoforms in melanocytes. Onco-gene 2007; 26: 4563.
32. Davies H, Bignell GR, Cox C, et al.Mutations of the BRAF gene in human can-cer. Nature 2002; 417: 949.
33. de Snoo FA, Hayward NK. Cutaneousmelanoma susceptibility and progressiongenes. Cancer Lett 2005; 230: 153.
502





























