Embed Size (px)
DESCRIPTION
Top 10 Considerations when implementing an ambulatory EHR
Citation preview


Electronic Health RecordsAn opportunity 900 years in the making….
Tim Burdick MDFamily Physician, Montpelier Health CenterMedical Director, Outpatient EHR, CVMC

Castle Urquhart, Loch NessThe year is 1207. The technology is paper and pen.

The Age of Electronic Records:
1940: Dartmouth College – first computer to be controlled telephonically
1951: UNIVAC – first commercially-available, mass-produced computer (US Census)
1951: LEO – first computer built for private, commercial use (large bakery firm)
1559: ERMA – GE machine purchased by Bank of America
1964: SABRE – IBM computer for American Airlines reservation tracking
1969: COSTAR – Harvard’s Computer Stored Ambulatory Record
1970: PROMIS – Medical Center Hospital of VT computer problem-oriented medical records, drug-drug interactions, and guidelines for diagnosis & treatment of 600 conditions
1973: RMRS – Regenstrief Medical Records System in continuous operation for 34 years, now covering the entire population of Indianapolis
Yet 38 yrs later, >60% of charts are still paper…..

EHR Selection
So many choices! How do I know which one to pick?

10. You can please 1% of the doctors some of the time.
Ask 10 doctors for their opinions and you will get 12 different answers.
Nevertheless, get several physicians involved in the selection process
Include primary care & medical and surgical specialties.
Improved selection and increased buy-in.
Speak with other physicians already using the system, preferably not just the practices mentioned by the vendor as good contacts.

9. With great power comes great responsibility.
Be careful what you ask for – it might come true.
A large EHR with infinite flexibility and capacity may come at a cost.
Hardware, training, maintenance fees, tech support, provider time.
A powerful system which fails implementation is worse than a simple system which is adopted fully.
Sometimes less really is more.

8. I’ll gladly pay you tomorrow for a hamburger today.
Vendors make great sales pitches with lots of promises.
If it’s only a promise for the future version, it’s vaporware not software.
Identify the system requirements that are keystones for your organization.
Have the vendor demonstrate the capability with the current software.
Verify with a user that the capability is functional.

7. Read my lips: no new taxes.
“It’s covered with a one-time application license. Trust me.”
Contracts exist to prevent misunderstandings between parties.
EHR contracts are a unique beast. Get somebody qualified to review it.
Everything is negotiable.
Vendors often have penalties for delays with implementation deadlines.(so they can move on to the next customer with cash).Be sure that delays caused by the vendor itself are exempted!

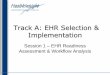
EHR ImplementationThe reality is that the implementation, despite the technology of 2007, is still costly and full of unknown monsters lurking beneath the surface.
Implementation and interface flow diagram for MPI & ADT.

6. Don’t buy the extended services...
Unless the service is extra training.
Training is one of the most expensive parts of implementation.
Neglecting training is one of the leading causes of EHR failure.
In larger organizations, training will be an ongoing concern.
This person is eager for more training.

5. Pandora’s box is EHR customization.
Customization allows all the joy and all the grief of EHRs.
Customization allows providers to make the system feel comfortable and familiar.
Customization by individual users can corrupt some systems quickly.
Customization by HIT can be expensive, slow, and clinically irrelevant.
Pandora’s jar (proper translation of pithos) by Nicolas Regnier c.1626
Ask the questions:
1) Which fields can be customized?
2) Can System Admin limit customization of certain fields?
3) When a field is customized, is it changed for the user or the system?
4) Who will do the customization in your organization?

4. It takes a village to raise an electronic health record:
HIT department-project manager-software programmers-hardware techies-medical director
QA analysts/P4P leadersBilling, coding specialistsOffice staff
-office managers-nurse managers
Hospital department liasons-diagnostic imaging-laboratory (micro, path)
Financial-CEO, CFO, VPs
Physicians -team leader-office super-users

3. If you ask a barber for help, you get a haircut:
HIT staff will build a logical system designed for efficient programming, not for clinical relevance.
Don’t leave the EHR process to a group of people who have never seen a patient,never stayed 3 hours after work to finish dictations and prior authorizations.
HIT departments may assume all doctors want EHR, can use a computer, are willing and able to teach themselves the new technology.
Successful implementation requires finding a physician to sit behind the computer and work alongside the HIT staff during the entire process.

2. One person’s treasure in is another person’s garbage out.
Building the EHR database does not lead to improved clinical care.
Quality improvement using the EHR, as always, requires constant re-evaluation, feedback, and willingness to change our practices.

1. Let us not be afraid to chase after new possibilities.

Resources:
Academy of Family Physicianshttp://www.centerforhit.org/http://www.aafp.org/online/en/home/publications/journals/fpm/indexes/index2007.html#8
Medical Economicshttp://www.memag.com/memag/static/staticHtml.jsp?id=114289
American Medical Associationhttp://www.ama-assn.org/ama/pub/category/16195.html
US Dept Health & Human Serviceshttp://www.hhs.gov/healthit/
Certification Commission for HIT (CCHIT)http://www.cchit.org/