Embed Size (px)
Citation preview

EHRA KEY MESSAGES
Learn more aboutEHRA Activities
Educational Courses
Certification Exams
EHRA EUROPACE CongressTraining Fellowships
MembershipEP Europace Journal
Webinars
The European Heart House, Specialty Centre (EHRA)Les Templiers - 2035 route des colles
CS 80179 Biot06903 Sophia Antipolis Cedex, France
Tel: +33 (0)4 92 94 76 00 - Fax: +33 (0)4 92 94 86 46Email: [email protected]/EHRA
EHRAKEY MESSAGES
www.escardio.org/EHRA
EHRA Consensus Document on Syncope Unit: Rationale and Requirement
Syncope series

Medtronic
The full article and its related educational material were producedby and under the sole responsibility of EHRA.
The EHRA writing committee collaborated with medical experts fromthe different companies to assure data accuracy and completeness.
Syncope Key Messages are supported by an unrestrictededucational grant from

1
EHRA Key MessagesEHRA Consensus Document on Syncope Unit: Rationale and Requirement(Original title: Consensus Statement of the European Heart Rhythm Association on the Rationale and Requirements for a Syncope Unit (endorsed by Heart Rhythm Society)
Table of Contents
1. Scope of the document ..............................................................................................................................................................................................................................................................................................................................................................................................................................................................................Page 2 2. Definitions ..............................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................Page 23. Rationale for a Syncope Unit - Expected benefit and barriers to set-up a Syncope Unit ...................................................................................................................................Page 34. Structure of the EHRA Syncope Unit ........................................................................................................................................................................................................................................................................................................................................................................................................Page 55. Comprehensive Care........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................Page 12
• 5.1 Referrals, access criteria ..........................................................................................................................................................................................................................................................................................................................................................................................................................Page 13• 5.2 Management modalities ..........................................................................................................................................................................................................................................................................................................................................................................................................................Page 14• 5.3 Final report and follow-up..............................................................................................................................................................................................................................................................................................................................................................................................................Page 17• 5.4 Follow-up .................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................Page 19
6. Quality Indicators...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................Page 20

2
1. Scope of the documentThis Position Paper offers a pragmatic approach to the rationale and requirement for a syncope unit (SU).The document is addressed to physicians and others in administration, who are interested in establishing a Syncope Unit in their hospital, so that they can meet the standards proposed by ESC-EHRA-HRS.
2. Definitions2.1 Definition of Transient Loss of Consciousness and Syncope Transient loss of consciousness (T-LOC) or faint is a term that encompasses all disorders characterized by self-limited loss of consciousness (LOC), irrespective of mechanism. Syncope is a transient loss of consciousness (T-LOC) due to transient global cerebral hypoperfusion, and is characterized by rapid onset, short duration and spontaneous complete recovery. By including the mechanism of unconsciousness, i.e. transient global cerebral hypoperfusion, the current syncope definition excludes other causes of T-LOC such as epileptic seizures and concussion, as well as certain common syncope mimics, such as psychogenic pseudosyncope.
2.2 Definition of a Syncope UnitAn SU is a facility featuring a standardized approach to the diagnosis and management of T-LOC and related symptoms, with dedicated staff and access to appropriate diagnostics and therapies. The SU should also take the lead in educating and training clinicians who encounter syncope. Even if the most appropriate term describing such an organization should be the more general T-LOC Unit (or Faint Unit), this Task Force decided to maintain the term of SU, because it is most frequently used worldwide.

3
3. Rationale for a Syncope Unit - Expected benefit and barriers to set-up a Syncope Unit There is wide variation in practice of syncope evaluation, and wide variation in adoption of recommendations from published guidelines. Absence of a systematic approach to T-LOC incurs higher health and social care costs, unnecessary hospitalisations, and diagnostic procedures, prolongation of hospital stays, lower diagnostic rates and higher rates of symptom recurrences. Therefore, a systematic approach, by a dedicated service (a SU), equipped to evaluate and manage this common problem may ensure better management of T-LOC, from risk stratification to diagnosis, therapy and follow-up. The available literature suggests that: • SU reduces underdiagnosis and misdiagnosis of syncope • SU reduces hospitalization • SU reduces cost of syncope
SUs are not widely established in clinical practice. Possible reasons for this are outlined in Table 1. Barriers to establishing an SU include lack of resources, lack of trained dedicated staff and complex presentations to multiple settings, necessitating involvement from multiple disciplines.

4
Table 1: Expected benefits and barriers in setting up an SU
Expected Benefits Barriers to establishing an SU
• Specialist opinion for patients • Earlyaccurateandefficientdiagnosis• Timely treatment • Betterapplicationofrecommendedguidelines• Lessduplicationandfragmentationofservices• Singlesourceofcommunicationforallstakeholders• Shorterlengthofstayforhospitalinpatients• Reduction of total care costs • Bettersystemsformonitoringandevaluationofpractice atlocal,nationalandinternationallevel• Better quality control at local, national and internationallevel• Accesstoharmoniseddataacrossdifferenthospitals• Highquality,evidencebaseddataforresearch• Evidencebasedinnovationindiagnosis,treatments andhealthcaremodel
•LackofawarenessofthebenefitsofanSUdueto inadequateresearchtrialscomparinganSUtonormal practice • Underestimationofconsequencesofsyncope• LackofawarenessofbenefitofanSUonqualityoflife• Lownumbersofsyncopespecialists• Lackofformalsyncopetrainingprograms• Wideagerangefrompaediatrictooldestpatients• Skillsetsrequiredinanumberofdomainssuchas cardiology,geriatrics,paediatrics,physiology,neurology andpsychiatry• Syncopenotarecognizedsubspecialty• Reluctancetointroduceinnovativeproposals• Necessitytoengagemultiplestakeholders• Inadequatereimbursementofsyncopecoremanagement• NeweconomiccostmodelsrequiredtoevaluateanSU• Fearofincreasingcostsbythedevelopmentofanew structureinsteadofreducingthem

5
4. Structure of the EHRA Syncope Unit 4.1. General attributes for a Syncope Unit The SU can be virtual or based in a predefined location such as a unit associated with the ED, an ambulatory clinic or employ a combination of approaches. The model of SU should be the best fit for local practice. No single syncope care service model is suitable for all health care systems. The skill mix of the model and leadership depends on the specialty designated to take a lead, the setting and referral sources. There are existing models in which cardiologists (commonly with an interest in cardiac pacing and electrophysiology), neurologists (commonly with an interest in autonomic disorders and/or epilepsy), internists (commonly with an interest in cardiovascular physiology and autonomic disorders), emergency doctors and geriatricians (commonly with an interest in age-related cardiology or falls) each may lead syncope facilities. There is no evidence for superiority of any model.When establishing a unit the lead clinician should have knowledge of catchment area for referrals and projected volume in order to estimate staff requirements and to tailor the scope of referrals to available resources. The volume of activity and the number of personnel largely varies based on the model of SU and local organization. No empirical figures can therefore be given. However, since the aim of this document is to provide practical advice to stakeholders who are interested in setting-up an SU, as a general guide, this Task Force estimates that one syncope specialist and one technician need to work the equivalent of one full working day per week for every 100,000 inhabitants of the catchment area.
4.3 Structure of the EHRA Syncope UnitThe proposed structure of the EHRA SU is shown in the Consensus Statement 1. The role of physician and staff in performing procedures and tests is shown in the Table 2.

6
Consensus Statement 1 – Structure of the EHRA Syncope Unit
Staffing of an SU is composed of:1. Oneormorephysiciansofanyspecialtywhoaresyncopespecialists.OwingtothemultidisciplinarynatureofT-LOC management,eachSUshouldidentifyspecificspecialistsforSUandforconsultancies.2. Ateamcomprisedofprofessionalswhowilladvancethecareofsyncopepatients.Thesemaybephysicians,specialised/trained nursesorotherswhobringmultidisciplinaryskillstothefacility,coupledwithadministrativesupport.Theroles playedbymembersoftheteammayvaryaccordingtolocalcircumstancesandindividualskill.Nursesmaybeexpected totakeveryimportantrolesincludinginitialevaluationofpatients,follow-upclinicassessments,selectionofinvestigations includingtilttestingandimplantation/insertionofECGlooprecordersaccordingtopre-definedprotocolsandlocalregulations.3. GiventhattheSUisintegratedwithinahospitalorganization,syncopespecialistsandstaffarenotnecessarilyemployed full-time,butfrequentlyhaveotherdutiesdependingonthevolumeofactivityintheSU.
Facility, Protocol and Equipment1. AnSUwilldelivermostofitscaretoout-patientsinadditiontoEDandin-patients2.TheSUshouldfollowaninternalprotocol,whichappliestodiagnosisandmanagementandisagreedbystakeholders3. Anequippedfacilitymustbeavailable4. EssentialEquipment/tests: -12-leadECGand3-leadECGmonitoring -non-invasivebeat-to-beatbloodpressuremonitorwithrecordingfacilitiesforsubsequentanalysis -tilt-table -Holtermonitors -externallooprecorders -follow-upofimplantablelooprecorders(*) -24-hourbloodpressuremonitoring -Basicautonomicfunctiontests

7
Consensus Statement 1 – Structure of the EHRA Syncope Unit (continued)
Facility, Protocol and Equipment (continued)5.Establishedproceduresfor: -Echocardiography -Electrophysiologicalstudies -Stresstest -Neuroimagingtests6.Specialists’consultancies(cardiology,neurology,internalmedicine,geriatric,psychology),whenneeded
TherapySyncopepatientswillreceivetheirtherapyunderthecareoftheSUunlessexpertiseoutsidethatoftheunitisrequired.
Database ManagementTheSUisrequiredtokeepmedicalrecordsthatshouldalsoincludefollow-upwhenappropriate.ThedatabasewillalsoofferthepossibilityofcollaborativeresearchwithotherSUs.
(*) implantation of loop recorders may be performed either by SU physicians or by external cardiologists upon request of the SU physicians

8
The“SyncopeSpecialist”The Syncope Specialist has responsibility for the comprehensive management of the patient from risk stratification to diagnosis, therapy and follow-up, through a standardized protocol. The syncope specialist requires specific knowledge. A syncope specialist is a physician who has sufficient knowledge of historical clues and physical findings to recognise all major T-LOC forms, including mimics, as well as syndromes of orthostatic intolerance.
Syncope specialists need not all have the same skill levels, but the SU as a whole must be able to provide a minimum skill set, so a combination of specialty skills is optimal. These conclusions are specified in Consensus Statement 2
ThestaffMost of the work is undertaken by nursing/technical staff. This requires specific skill and competence. In addition to assisting the syncope specialist, the specialized nurse/technician will perform procedures and tests (under physician supervision) provided that they are based on internal protocols and rules. (Table 2)

9
Procedure or test SU Physician
SU Staff
Non-SU personnel
Historytaking x
Structuredhistorytaking(e.g.,applicationofsoftwaretechnologiesandalgorithms)
x
12-leadECG x
Blood tests x
Echocardiogramandimaging x
Carotidsinusmassage x
Activestandingtest x
Tilttabletest (x)* x
Basic autonomic function test x x
ECGmonitoring(Holter,externallooprecorder):administration and interpretation
x x
Implantablelooprecorder x (x)**
Procedure or test SU Physician
SU Staff
Non-SU personnel
Remotemonitoring x
Othercardiactests(Stresstest,electrophysiologicalstudy,angiograms)
x
Neurologicaltests(CT,MRI,EEG,video-EEG)
x
PacemakerandICDimplantation,catheterablation
x
Patient’s education, biofeedbacktraining(***).andinstructionsheetoncounterpressuremanoeuvres
x x
Final report and clinic note x
Communicationwithpatients,referringphysiciansandstakeholders.
x x
Follow-up x x
Table 2: The role of physician and staff in performing procedures and tests
* physician need not to be in the room, but a physician adequately trained in resuscitation needs to be in the area of the test** current practice limited to few countries *** Biofeedback means that the training session of the counter pressure manoeuvres consists of biofeedback training using a continuous blood pressure monitor. Each manoeuvre is demonstrated and explained. The manoeuvres are practiced under supervision, with immediate feedback of the recordings to gain optimal performance (54)

10
Consensus Statement 2 - Competence and skills mix of physicians and staff required for syncope management in a Syncope Unit
Major and minor category 1. Diagnostic Skills per syncope specialist
2.SU access to Ancillary Tests 3. SU ancillary tests
Syncope Reflex Specialistknowledge Full TT,CSM,24hrBP,ELR-ILR
Syncope due to OH Specialistknowledge Full TT,24hrBP,autonomictesting
Cardiacsyncope Specialistknowledge Full/preferential ECG,telemetry,ELR-ILR,Echo,EPS
Epileptic seizures
Generalmedicalknowledge Preferential EEG,video-EEGmonitoring,homevideo,neuroimaging
Psychogenic T-LOC
PPS Generalmedicalknowledge Full/Preferential TT,preferentiallywithvideo-EEGmonitoring,homevideo
PNES Generalmedicalknowledge Preferential video-EEGmonitoring,homevideoBP = blood pressure; CSM = Carotid sinus massage; Echo = echocardiogram; EEG = electroencephalogram; ELR = external loop recorder; EPS = electrophysiological testing; ILR = implantable loop recorder; OH = orthostatic hypotension; PNES = psychogenic non-epileptic seizure;PPS = psychogenic pseudosyncope; TT = tilt table test

11
Legend • The levels described here concern the SU as a whole, not those of individual physicians, except for column 1: the requested level of minimum basic diagnostic skills applies to each syncope specialist.
1.DiagnosticSkillsperSyncopeSpecialistThese skills refer to history taking and physical examination only. • ‘General medical knowledge’: this is the level stipulated by medical education, i.e., the knowledge medical students are required to have in order to pass medical examinations. • ‘Specialist knowledge’: this is the level required for specialty examination; when no specialty demands are available as for reflex syncope, the specialist level denotes the ability to recognise rare forms occurring once in about 200 cases. 2.SUAccesstoAncillaryTestsAncillary diagnostic skills concern all diagnostic tests not covered under column 1. • Full access: the SU carries out the test. • Preferential access : the SU does not usually carry out the test but has preferential access to the tests/services in question
3.SUAncillarytestsThis is an overview of the most likely test required for the disorder in question

12
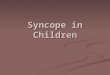
5. Comprehensive CareThe possibility of providing a comprehensive standardized syncope management of the patient from risk stratification to diagnosis, therapy and follow-up characterizes and distinguishes a Syncope Unit (Figure 1).
TLOC – certain/suspected syncope
Follow-up
Diagnosis pathway
Risk stratification
Core evaluation & testsdirectly performedby SU personnel
Other tests/consultationsFast track access to testsor the proper specialist
Core therapydirectly performedby SU personnel
Other therapiesFast track tothe specialist
Admit patientsat high risk
directly performed by SU orother specialty as appropriate
Treatment pathway
Diagnosis not yet establisheddiagnosis needed
Diagnosis already establishedtreatment needed
Figure 1: Framework for a comprehensive management of patients with T-LOC of certain/suspected syncopal nature referred to the Syncope Unit. Core evaluation and therapy depend on each model of care delivery, with a minimum acceptable set described in Consensus Statement 1.

13
5.1 Referrals, access criteriaReferral can be directly from family practitioners, ED, in-hospital and out-hospital services, or self-referral from the patient. A fast track access, with separate waiting list and scheduled follow-up visits is recommended. In particular, patients at low/intermediate risk admitted to the ED should benefit from such a fast track (so-called “protected discharge” or “advanced access”’ with an appointment for early assessment), in order to reduce hospitalization rate, directly from the ED or after a short stay in the Short Observation unit of the ED as part of an internal protocol for risk stratification of intermediate risk ED patients.
Who should access the SU? • Patients affected by T-LOC of suspected syncopal nature who, because of frequency or severity of the episodes, need to establish a diagnosis and to ascertain the need for a specific therapy. • Patients with an already established diagnosis in order to receive a specialist’s consultancy on the best evidence-based therapy or to start specific treatment, i.e., those listed in Consensus Statement 4. • Patients who need follow-up to make a final diagnosis or assess efficacy of therapy (see section 5.3)
Who should not access the SU? • Patients with a certain diagnosis and/or an established indication for therapy, e.g., patients with bradycardia with guideline-based indications for cardiac pacing. • Patients in whom syncope is a symptom secondary to underlying disease which requires urgent and specific diagnostic and therapeutic pathways which cannot be followed within an SU e.g., syncope due to acute myocardial infarction or acute bleeding.

14
5.2 Management modalitiesDiagnosticpathwayDiagnostic assessment consists of core assessment directly performed by the personnel of the Syncope Unit and, when appropriate, by a fast track access to any other tests and specialist visits which are not directly performed in the SU.
Consensus Statement 3 – Tests and assessments available in a Syncope Unit
Initial assessment History&physicalevaluationincluding3-minorthostaticBPmeasurement*12-leadstandardECG
Subsequent tests and assessments (only when indicated)
Blood tests Electrolytes,Haemoglobin,troponin,BNP,glucose,D-dimer,Hemogasanalysis/O2saturation,
Provocative tests Carotidsinusmassage,Tilttabletest
Monitoring Externallooprecording,Implantablelooprecording,Ambulatory1-7daysECGmonitoring,24-48hourBPmonitoring
Autonomic function tests Standingtest,Valsalvamanoeuvre,deepbreathingtest,coldpressortestand/orestablishedproceduresforaccesstootherautonomicfunctiontests
Cardiac evaluation Establishedproceduresforaccesstoechocardiogram,stresstest,electrophysiologicalstudy,coronaryangiography
Neurological evaluation Establishedproceduresforaccesstoneurologicaltests(CT,MRI,EEG,video-EEG)

15
Consensus Statement 3 – Tests and assessments available in a Syncope Unit (continued)
Geriatric evaluation Establishedproceduresforaccesstofallriskassessment(cognitive,gaitandbalance,visual,environmental)andforgaitandbalanceretraining
Psychological or psychiatric evaluation
Establishedproceduresforaccesstopsychologicalorpsychiatricconsultancy(mentalhealthproblemorpsychogenicsyncope)
Consensus Statement 4 – Treatments available in a Syncope Unit
Reflex syncope - Structurededucationonmanagementofriskfactorforpreventionofreflexsyncope (includingadequatefluidandsaltintake)- Biofeedbacktraining*andinstructionsheetoncounterpressuremanoeuvresandleg/abdomen elasticstocking- Establishedproceduresforaccesstopacemakerimplantation- Modificationofculpritdrugs- Prescriptionofvasoconstrictordrugs
*Postural Orthostatic tachycardia may require longer stands
TreatmentpathwayEven if the model of therapy delivery is that which is most appropriate to existing practice and resources, those listed in Consensus Statement 4 are the minimum core treatments that should be provided directly by the SU staff.

16
Consensus Statement 4 – Treatments available in a Syncope Unit (continued)
Orthostatic hypotension - Structurededucationsessiononmanagementofriskfactorforpreventionoforthostatic hypotension(includingadequatefluidandsaltintakeandcareduringorthostaticchangesafter prolongedperiodslyingorsitting)- leg/abdomenelasticstocking- Modificationofculprithypotensivedrugs- Prescriptionofantihypotensivedrugs,vasoconstrictordrugs
Cardiac syncope - Establishedproceduresforaccesstopacemakerimplantation,catheterablationofarrhythmias, ICDtherapyandothersurgicalinterventions- Prescriptionofantiarrhythmicdrugs
Falls Structurededucationonmanagementofriskfactorforfallprevention
Psychogenic pseudosyncope (functional)
Establishedproceduresforaccesstopsychotherapy
Epilepsy Establishedproceduresforaccesstoneurologycare
ICD = Implantable cardiac defibrillator.* Biofeedback means that the training session of the counter pressure manoeuvres consists of biofeedback training using a continuous blood pressure monitor. Each manoeuvre is demonstrated and explained. The manoeuvres are practiced under supervision, with immediate feedback of the recordings to gain optimal performance (54).

17
5.3 Final report Once the work-up is complete and a therapy is prescribed, the patient and referring practitioner should receive a written comprehensive final report and be referred back to the referring physician. The framework of a structured final report is described in Table 3 and Table 4.Table 3: Framework of a structured final report (clinic note)
Chief complaint UsedefinitionrecommendedbytheESCguidelinesonsyncopereportedinthetable6
Present illness 1) CircumstancesjustpriortotheT-LOCevent(predisposingfactors,triggers,bodyposition, activity,signsandsymptomsofautonomicactivation,accompanyingsymptoms,prodromes)2) Featuresoftheattack(eyewitness),duration,recovery,consequences(trauma)3) PreviousT-LOCepisodes(number,dateofoccurrence,features,previoustestsandtreatments)
Past medical history 1) Descriptionofunderlyingdiseases2) Medications3) Socialhistory4) Familyhistory
Physical examination Findings
Electrocardiogram Findings
Tests Listandreportoftherelevantfindingsofthetestsperformed
Assessment and diagnosis Descriptionofthefindingsthatledtothefinaldiagnosis
Plan/Treatment Suggestedfurtherdiagnostictestsortreatmentwithanexplanationoftheexpectedresults,asappropriate
Follow-up modality Descriptionandeventualappointmentforfurthervisits

18
Table 4: Classification and criteria used to establish a certain/likely diagnosis (derived from the 2009 ESC guidelines) on syncope to be reported in the final report
Classification of T-LOCs Diagnostic features
Reflex syncope (neurally-mediated)
ClassicalVasovagalSyncope(VVS)
Ifthesyncopewasprecipitatedbyemotionaldistress(fear,severepain,medicalinstrumentationprocedures)orprolongedstandingandwasassociatedwithtypicalprodrome.
Carotidsinussyncope
Ifthesyncopewasreproducedby10secondsofbilateralsequentialcarotidsinusmassage,supineanderect,inthepresenceofasystole>3sand/orfallinsystolicbloodpressure>50mmHgandintheabsenceofcompetingdiagnoses.
Situational Syncope
ifthesyncopeoccurredduringorimmediatelyafterurination,defecation,coughing,laughingorswallowing,etc.
Atypical Form Ifthesyncopeoccurredwithuncertainorevenapparentlyabsenttriggers.Thediagnosisthenrestslessonhistorytakingalone,andmoreontheexclusionofothercausesofsyncope(absenceofstructuralheartdisease)andonreproducingsimilarsymptomswithtilttesting.
Orthostatic Intolerance
Orthostatichypotension
Ifsyncopeoccurredafterstandingupandsymptomaticorthostatichypotensionwasdocumented.Inthe“Initialform”,orthostatichypotensionoccursimmediatelyonstandingthenspontaneouslyandrapidlyreturnstonormalwithin30s.IntheClassicalformorthostatichypotensionoccursafter30sbutwithin3minutesafteractivestandingup,whileinProgressive(delayed)form–usuallydiagnosedbymeansoftilttesting-progressiveorthostatichypotensionoccursmorethan3minuteafterstandingup.
Postural tachycardiasyndrome(POTS)
Ifthesymptomsoforthostaticintoleranceareprecipitatedbyanincreaseinheartrate>30bpm(>40bpminpatients12to19yearold)vs.supineandabsenceoforthostatichypotension.

19
Table 4: Classification and criteria used to establish a certain/likely diagnosis (derived from the 2009 ESC guidelines) on syncope to be reported in the final report (continued)
Classification of T-LOCs Diagnostic featuresCardiac Cardiacarrhythmia IftheclassIdiagnosticcriteriaoftheESCguidelines(1,2)weremetduringprolonged
ECGmonitoringorbymeansofelectrophysiologicalstudy;cardiacarrhythmiaalsoincludedthecaseofpatientswithseverelydepressedejectionfractionwhohadadefiniteindicationforICDregardlessofthemechanismofsyncope.
Structural cardiac or cardiopulmonary
Ifthepatientwasaffectedbyacutecardiacischaemiaorotheracutecardiopulmonarydiseasesorprolapsingatrialmyxomaorsevereaorticstenosisorhypertrophicobstructivecardiomyopathy,etc.
Non-syncopal attacks
Epilepsy,unexplainedfall,psychogenicpseudosyncope(functional),vertebro-basilar,metabolicdisorders,etc.
Iftheepisodeoftransientlossofconsciousnesswasinitiallyattributedtoasyncopalconditionbutthesubsequentevaluationdemonstratedanon-syncopalmechanism(i.e.,epilepsy,vertebro-basilarischemicattack,unexplainedfall,orpsychogenic[functional]pseudo-syncope),hypoxia,intoxication,cataplexy,dropattacks).
Unexplained syncope/T-LOC Inthosepatientswithoutanyoftheabovediagnosis.
5.4 Follow-up The patient should still be periodically followed-up by the SU staff for three main purposes: 1. to assess the efficacy of treatment and re-evaluation in the case of syncope recurrence 2. to establish a diagnosis in those patients with unexplained syncope who are undergoing prolonged ECG monitoring with external or implantable loop recorders 3. to contribute to the program of quality control of the SU (follow-up database, audit, etc.).
The follow-up process can be easily performed via phone interview or other tools e.g. web-based.

20
6. Quality IndicatorsBased on the data presented in the previous sections, this Task Force believes that reasonable goals (expected benefits) of the EHRA SU should be those listed in the Consensus Statement 5. Consensus Statement 5 – Quality indicators
Quality Indicator Process Indicator Desirable outcome target Comments
1 - Syncope UnitToreducetherateofunexplainedT-LOC
Atleast70%ofpatientsreceiveadefinitediagnosis(accordingtoESCguidelinesdefinitions)
AbsoluterateofunexplainedT-LOC≤20%
DatafrompublishedliteratureindicatethatareasonablegoalistoachieveanabsoluterateofunexplainedT-LOC≤20%(SeeSection3).
Toreducetherateofhospitalization(inpatientsatintermediate-highriskfromED)
Atleast20%ofpatientswithunexplainedsyncopeafterinitialEDevaluationhavefast-trackaccesstoSUforearlyassessment
≤20%ofpatientswithunexplainedT-LOCadmittedafterEDinitialevaluation(accordingtoESCguidelinesdefinition)
Datafrompublishedliteratureindicatethatareasonablegoalistoachieveanabsoluterateofadmissions≤20%(SeeSection3).
To reduce costs per patient
Atleast20%reductionincostsrelativetousuallocalpractice
Appliestonewservices
Toimprovetheoutcome
Lessthan5%re-admissionsforsyncope recurrence in patients withanestablishedandsuccessfullytreateddiagnosis(accordingtoESCguidelinesdefinitions)
Lessthan20%ofpacedpatientshaverecurrence of syncope at 1 year
OlderpatientswhohavemorethanoneattributablecauseofT-LOCmayexperiencerecurrenceofsymptomsduetoothercausessuchasautonomicdysfunction and medication

21
Consensus Statement 5 – Quality indicators (continued)
Quality Indicator Process Indicator Desirable outcome target Comments
2 - PersonnelLeadership OnephysicianleadingtheSU Theleaderisusuallyoneofthe
SyncopeSpecialistsoftheSU.(SeeSpecialistConsensusStatement1).
Staff Adedicatedtrainedstaff(specificsfortrainingshouldmaptheT-LOCdiagnosesandtreatments)
Thecredentialingandthenumberofstaffwouldvaryaccordingtothesizeandorganizationofthelocalpractice
Training Syncope Specialist and Staff attendregulartrainingprogramand conferences in addition to accreditationprogram
Atpresent,thefieldlacksstructuredaccreditationforT-LOC/Syncope
3 - OperationsNumberofpatients Atleast100newcasesperyear
perSUThisistheminimumnumbernecessaryinordertodevelopandmaintainexpertisefor1syncopespecialistand1staffpersonnelandfortheSUtobecost-efficient

22
Consensus Statement 5 – Quality indicators (continued)
Quality Indicator Process Indicator Desirable outcome target Comments
Tests - >95%ofpatientshavea documentedECG- >90%ofpatientshave documentedorthostatictests- >90%havecarotidsinusmassage, tilttabletest,externalloop recorderandimplantableloop recorderperformedaccordingto ESCguidelinesindications
Waitinglist(firstvisitandfollow-up)
- 70%oflowriskpatientsseen within3months- 90%ofintermediateriskpatients seenwithin2weeks- Nowaitinglistforhighrisk patients

23
Task Force members: Rose-Anne Kenny (Chairperson)1, Michele Brignole (Co-chairperson)2, Gheorghe-Andrei Dan3, Jean Claude Deharo4, Gert van Dijk5, Colin Doherty6, Mohamed Hamdan7, Angel Moya8, Steve Parry9, Richard Sutton10, Andrea Ungar11, Wouter Wieling12
1 Falls and Syncope Unit, St. James’s Hospital Dublin Ireland2 Ospedali Del Tigullio, Lavagna-Italy3 Colentina University Hospital, Bucharest - Romania4 Hopital Timone Adultes, Marseille - France5 Leiden University Medical Centre, Netherlands6 St James’s Hospital/Trinity College Dublin, Ireland7 University of Wisconsin Hospital and Clinics, Wisconsin United States of America
8 Hospital Vall D’hebron, Barcelona, Spain9 Tyne and Wear United Kingdom10 Emeritus Professor of Clinical Cardiology, National Heart & Lung Institute, Imperial College, London, UK11 University Of Florence - Italy12 Academic Medical Centre, Amsterdam, Netherlands
External contributors to the Task Force: Europe: Mehran Asgari1, Gonzalo Baron-Esquivias2, Jean Jacques Blanc3, Ivo Casagranda4, Conal Cunnigham5, Artur Fedorowski6, Raffello Furlan7, Nicholas Gall8,Frederik J de Lange9, Geraldine McMahon10, Peter Mitro11, Artur Pietrucha12, Cristian Podoleanu13, Antonio Raviele14,North America: David Benditt15, Andrew Krahn16, Carlos Arturo Morillo17, Brian Olshansky18, Satish Raj19, Robert Sheldon20, Win Kuang Shen21, Benjamin Sun22;South America: Denise Hachul23; Asia: Haruhiko Abe24, Toshyuki Furukawa25
1 William Harvey Hospital, Kent, UK2 Hospital Universitario Virgen del Rocio, Sevilla, Spain3 Hopital de la Cavale Blanche, Brest, France4 Ospedale Santi Antonio e Biagio e Cesare Arri, Alessandria, Italy5 St. James’s Hospital, Dublin, Ireland6 Skane University Hospital; Malmo, Sweden7 Humanitas Research Hospital, Rozzano, Italy8 King’s College Hospital, London, UK9 Amsterdam, Netherlands10 Dublin, Ireland11 Institute Of Heart Disease And Vascular Disea, Kosice, Ireland12 Uniwersytet Jagiellonski, Krakow, Poland13 Univ. Clinical Hospital, 4th Medical Clinic, Targu Mures, Romania14 Cardiologist, Arrhythmologist, Mestre, Venice, Italy
15 University Of Minnesota Medical School, Minnesota) United States of America16 Vancouver General Hospital, British Columbia Canada17 Mcmaster University, Phri, Hamilton, Ontario Canada18 University of Iowa Hospitals and Clinics, Iowa United States of America19 Vanderbilt University, Tennessee United States of America20 University Of Calgary, Canada21 Mayo Clinic, AZ United States of America22 Emergency Medicine, Oregon Health & Science University, Oregon United States of America23 Instituto Do Coracao, Sao Paulo, Brazil24 Department Of Heart Rhythm Management, Univ. Occup. & Environment Health, Kitakyushu, Japan25 Division of Cardiology, St. Marianna University School of Medicine, Kawasaki, Kanagawa Japan

24
EHRA Scientific Document CommitteeProf. Gregory Y.H. Lip (EHRA Scientific Documents Committee Chair)Prof. Bulent Gorenek (EHRA Scientific Documents Committee Co-Chair)
Prof. Christian SticherlingProf. Laurent Fauchier Prof. Hein Heidbuchel
Dr. Angel Moya MitjansProf. Marc A VosDr. Michele Brignole
Prof. Gheorghe-Andrei DanDr. Michele GuliziaDr. Francisco Marin
Prof. Giuseppe BorianiDr. Deirdre Lane Dr. Irina Savelieva
Document reviewersReview coordinators: Bulent Gorenek1 and Gregory Y.H. Lip2
Michael Glikson3, Philippe Ritter4, Jodie Hurwitz5, Robert MacFadyen6, Andrew Rankin7, Lluis Mont8, Jesper Svendsen9, Fred Kusumoto10, Mitchell Cohen11
Corresponding author Professor Rose Anne KennyFalls and Syncope Unit, St. James’s Hospital Dublin IrelandChemistry Extension building, Lincoln Gate, Trinity College Dublin, [email protected]
List of topicsAFibSyncope
Inheredited / SCD / VTDevices
1 Eskisehir Osmangazi University, Turkey2 University Of Birmingham, (West Midlands) United Kingdom3 Sheba Medical Center, Ramat Gan, Israel4 Electrophysiologie-Stimulation cardiaque, Chu Haut Leveque, Pessac, France5 North Texas Heart Center, Dallas, Texas United States of America6 Ballarat Base Hospital, Victoria Australia
7 Glasgow Royal Infirmary, (Scotland) United Kingdom8 Hospital Clinic, University of Barcelona, Spain9 Rigshospitalet, Copenhagen, Denmark10 Mayo Clinic Hospital, United States of America11 Chief, Pediatric Cardiology, Phoenix Children’s Hospital, United States of America

EHRAKEY MESSAGES
Learn more aboutEHRA Activities
Educational Courses
Certification Exams
EHRA EUROPACE CongressTraining Fellowships
Membership EP Europace Journal
Webinars
The European Heart House, Specialty Centre (EHRA)Les Templiers - 2035 route des colles
CS 80179 Biot06903 Sophia Antipolis Cedex, France
Tel: +33 (0)4 92 94 76 00 - Fax: +33 (0)4 92 94 86 46Email: [email protected]/EHRA
EHRA KEY MESSAGES
www.escardio.org/EHRA
EHRA Consensus Document on Syncope Unit: Rationale and Requirement
Syncope series