Embed Size (px)
Citation preview
EKG 101
Deborah Goldstein
Georgetown University
Department of Internal Medicine
Steps to Interpreting an EKG
• Rate• Rhythm• Axis• Intervals (PR, QRS, QTc)• Hypertrophy• ST segments• T waves• Q waves
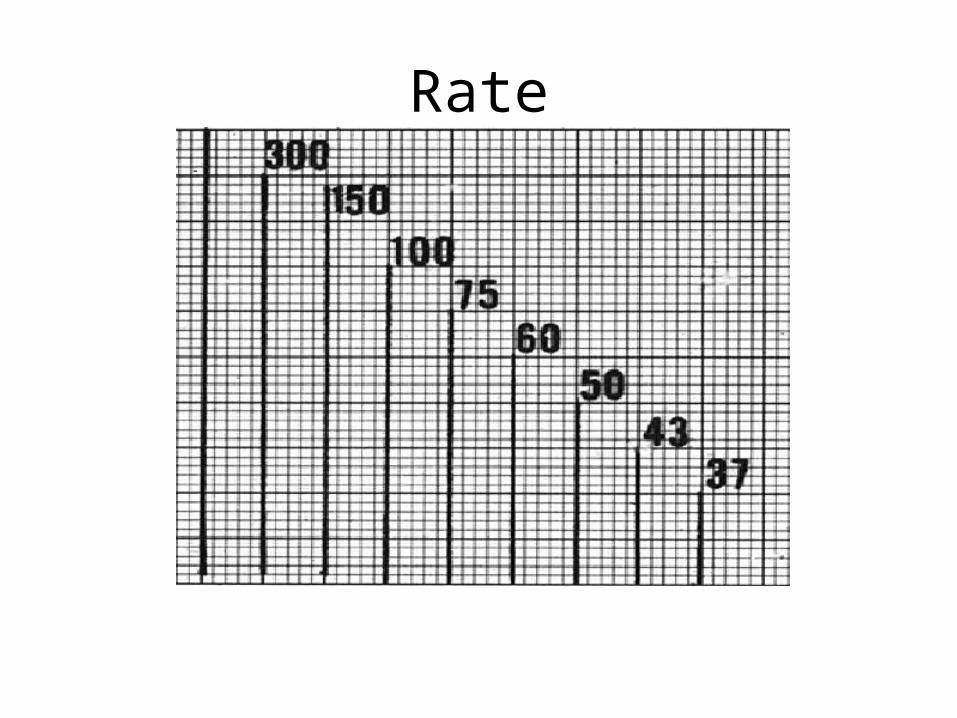
Rate
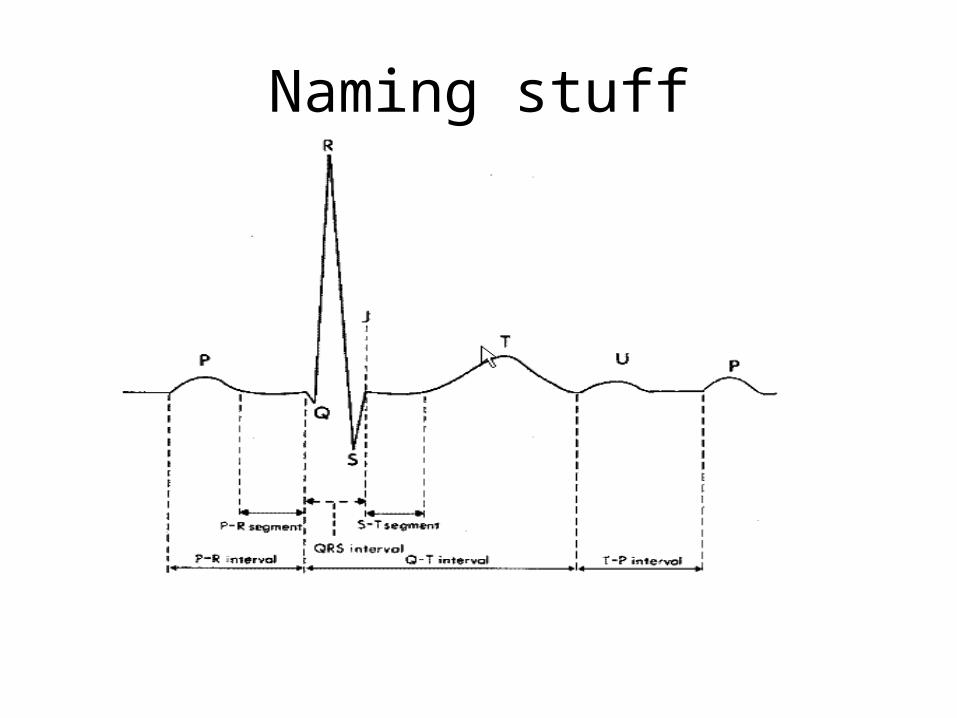
Naming stuff
Normal Sinus Rhythm
• P before every QRS – Best places to look: II, V1
• QRS after each P
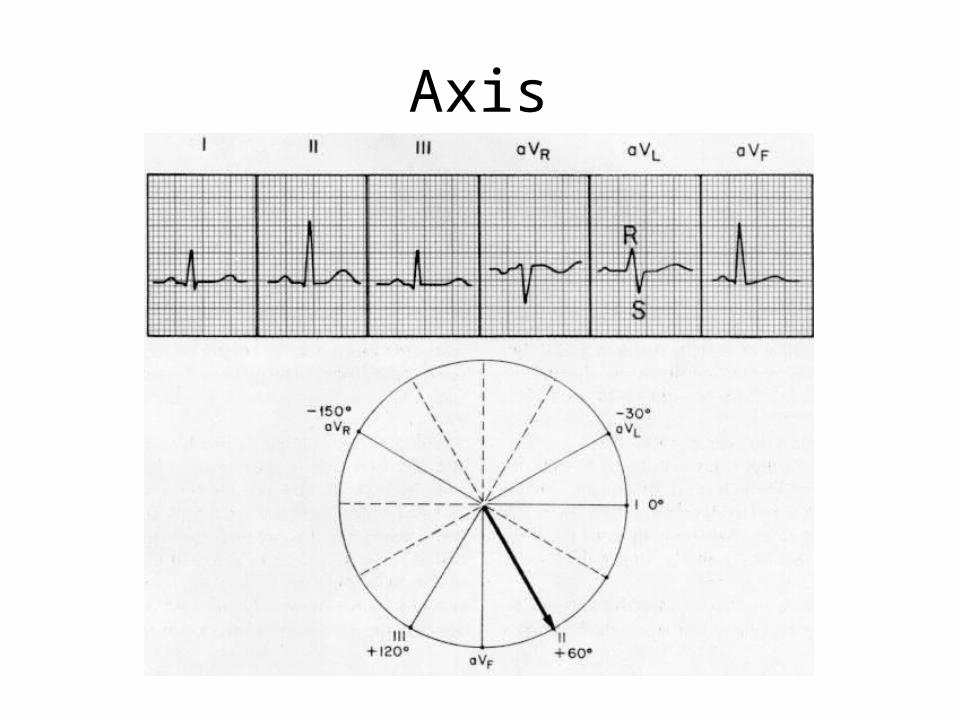
Axis
1. The direction of the mean electrical vector, representing the average of current flow in the frontal plane.
2. Normal axis: –30 to +90 degrees.
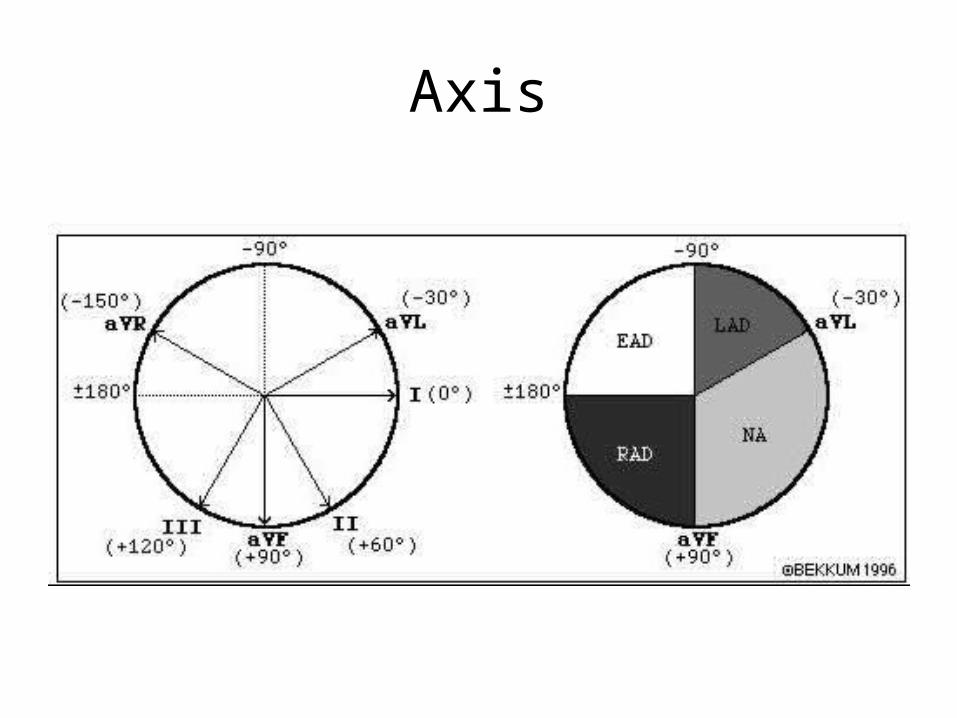
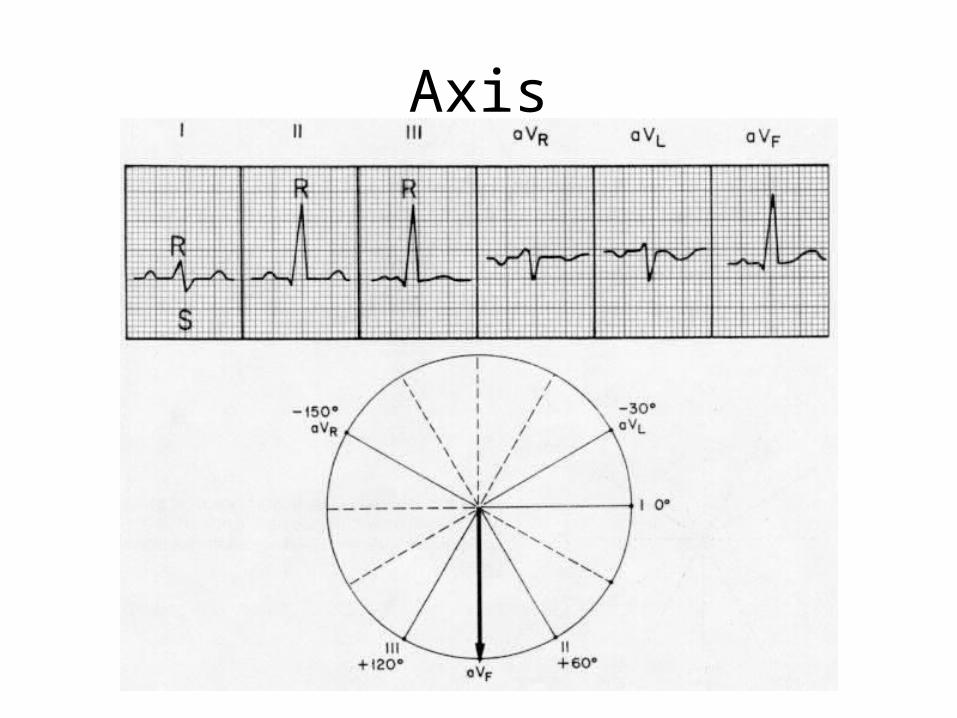
Axis
Axis
• Look at lead I and aVF.• Then find the isoelectric lead (where the QRS
complex is most nearly biphasic).• Then go 90 degrees perpendicular to the isoelectric
lead.
Axis
Axis
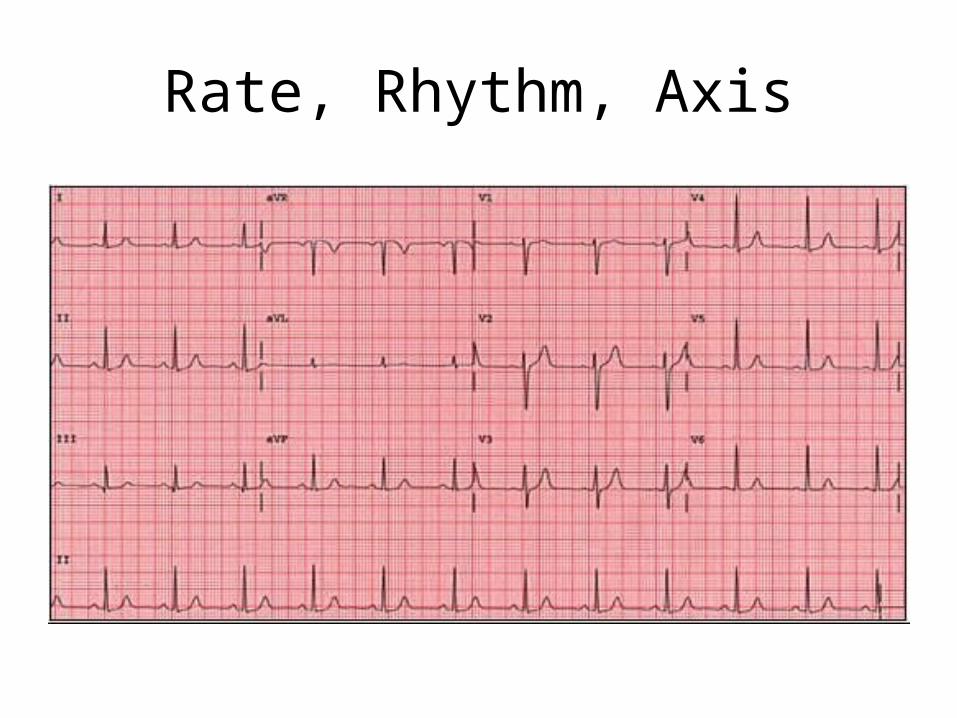
Rate, Rhythm, Axis
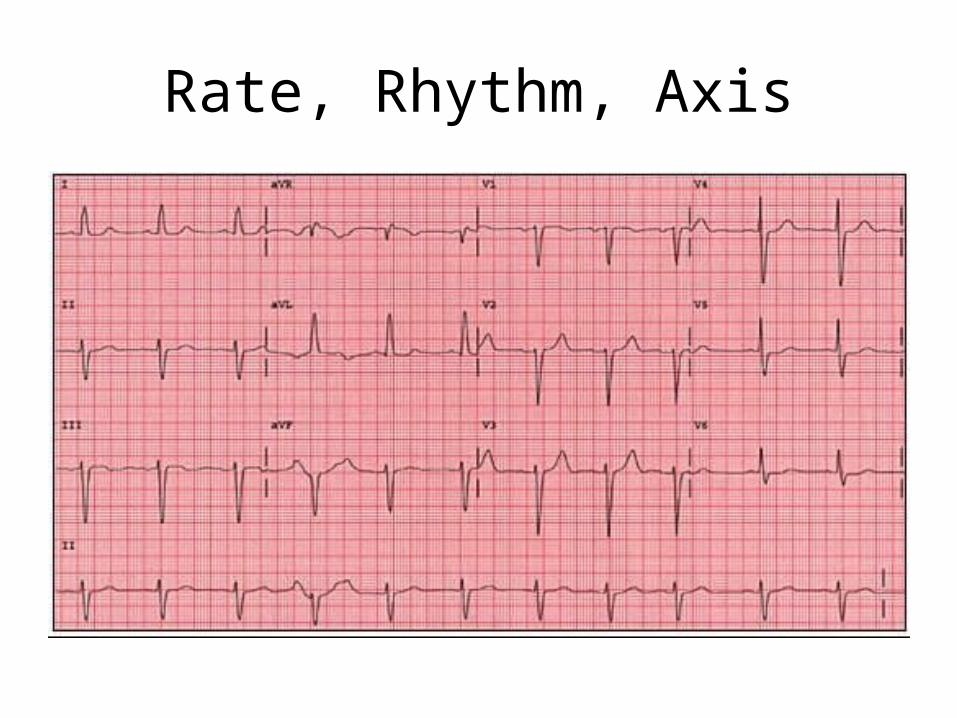
Rate, Rhythm, Axis
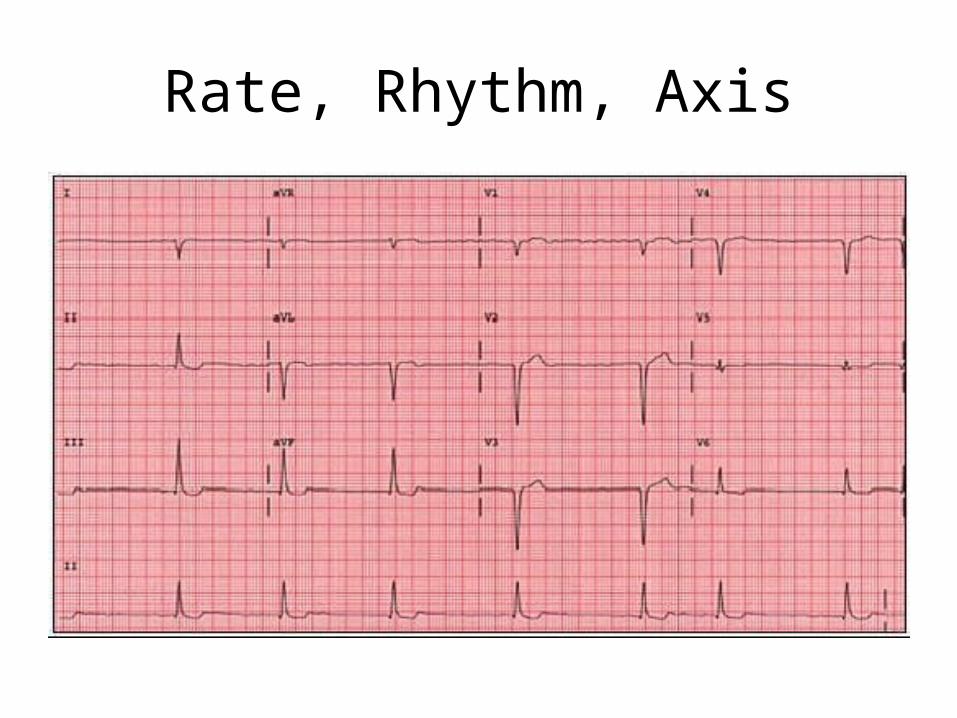
Rate, Rhythm, Axis
Ddx of Axis Deviation
LAD• Left ventricular hypertrophy, Left anterior fascicular
block, LBBB, Inferior wall MI• Pregnant, ascites, short/fat
RAD• Right ventricular hypertrophy, Left posterior
fascicular block, RBBB, lateral wall MI• PE
PR Interval
• Normal PR = 0.12 – 0.20 seconds (3-5 little boxes)
• Long PR >0.20 seconds (>5 little boxes)=Delayed conduction from atria to ventricles
• First-degree AV block– PR>0.20 seconds– NO dropped QRS
Second Degree AV Block
• Wenckebach (Type 1) =block within AV node– PR interval progressively lengthens...then dropped
QRS• Mobitz (Type 2)
=block within His-Purkinje system– Fixed PR with dropped QRS– WORSE!– Sarcoid, Lyme....– Pacemaker!
Third Degree AV Block
=Failure of conduction of any atrial impulses to get to the ventricles
=Complete AV block
Causes of Acute AV Block:• Calcium channel blockers• Acute RCA occlusion• Digoxin toxicity
What kind of AV Block?
What kind of AV Block?
What kind of AV Block?
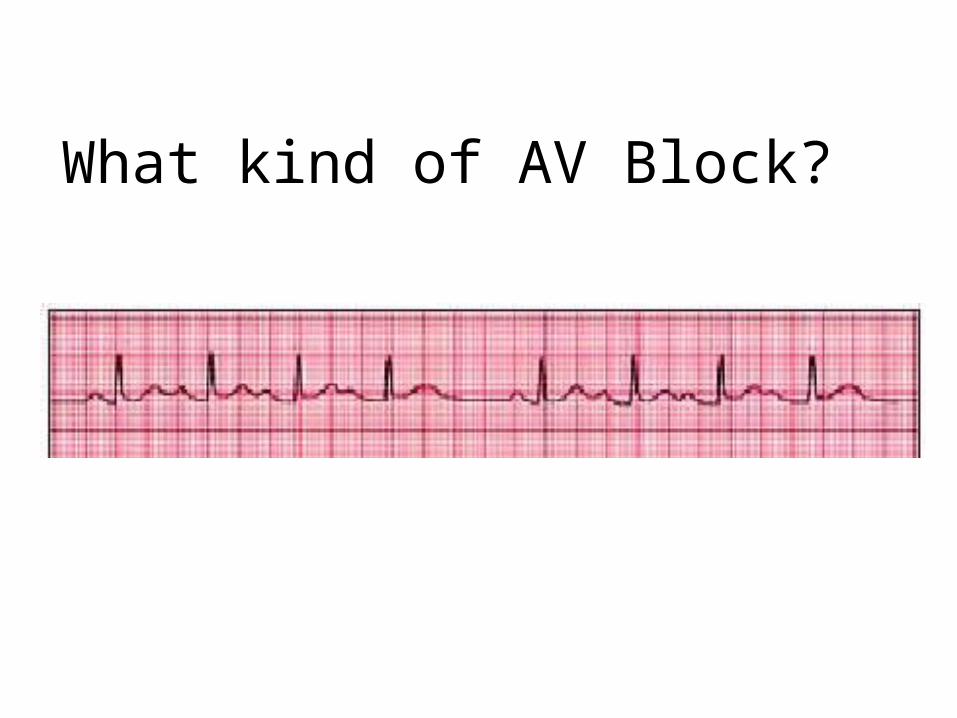
What kind of AV Block?
QRS Interval
Normal = 0.06-0.10 seconds
Wide QRS = >0.12 seconds (>3 little boxes)
• PVC...if >3 in a row or >6/min=VTach
• RBBB, LBBB
• Left fascicular hemiblock
• Hyperkalemia
Narrow QRS= <0.06 sec
• SVT (150-250 bpm)
• Idiojunctional rhythm (40-60 bpm)
• Premature junctional complex
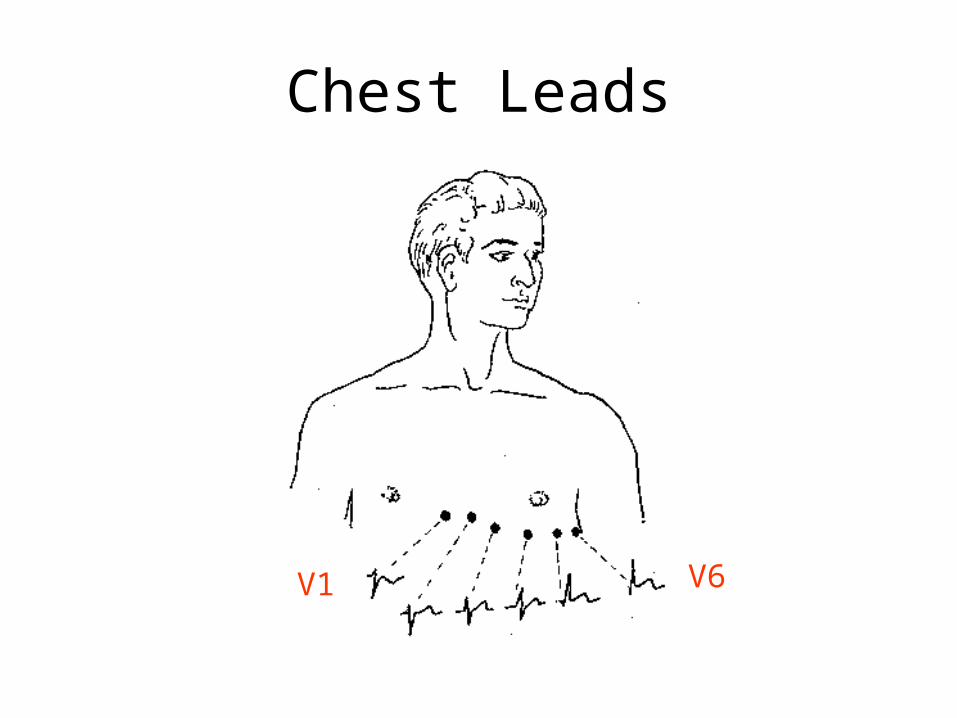
Chest Leads
V1 V6
Bundle Branch Block
V1-V2 = Right precordial leads
V5-V6 = Left precordial leads
LBBB• Rabbit ears in V6 represent delay between
depolarization from the septum to the LV
RBBB• Rabbit ears in V1 represent delay between
depolarization from the septum to the RV
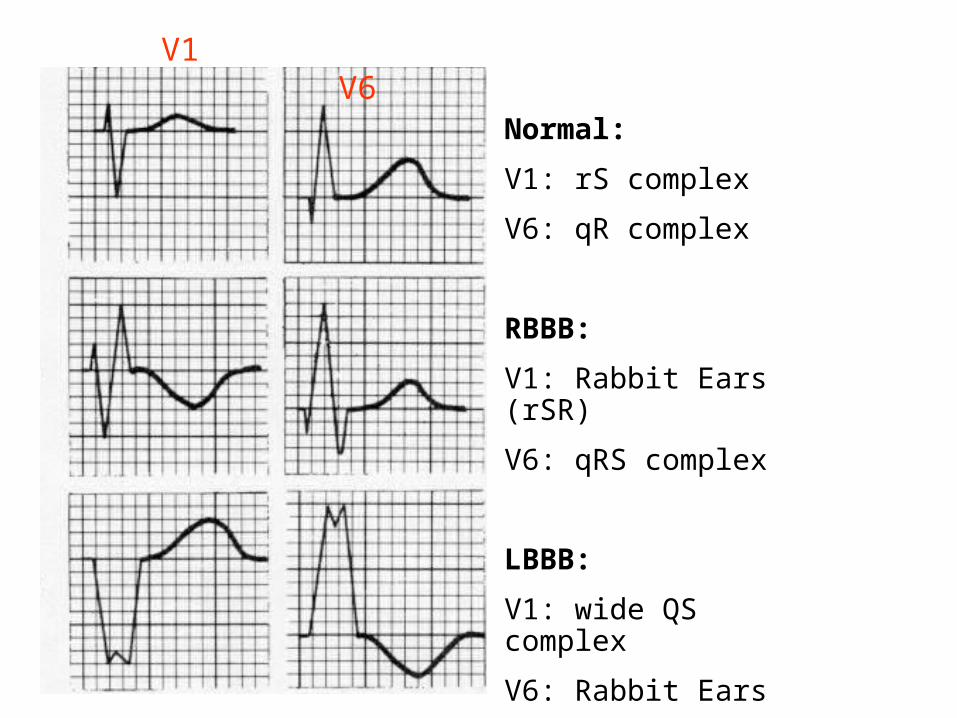
Normal:
V1: rS complex
V6: qR complex
RBBB:
V1: Rabbit Ears (rSR)
V6: qRS complex
LBBB:
V1: wide QS complex
V6: Rabbit Ears
V1 V6
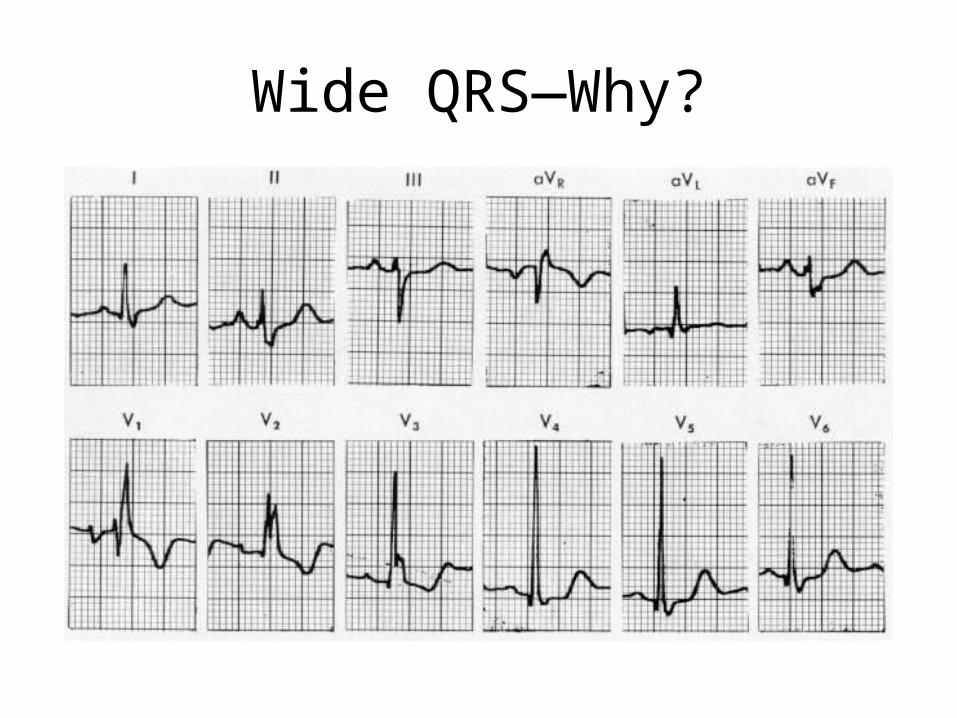
Wide QRS—Why?
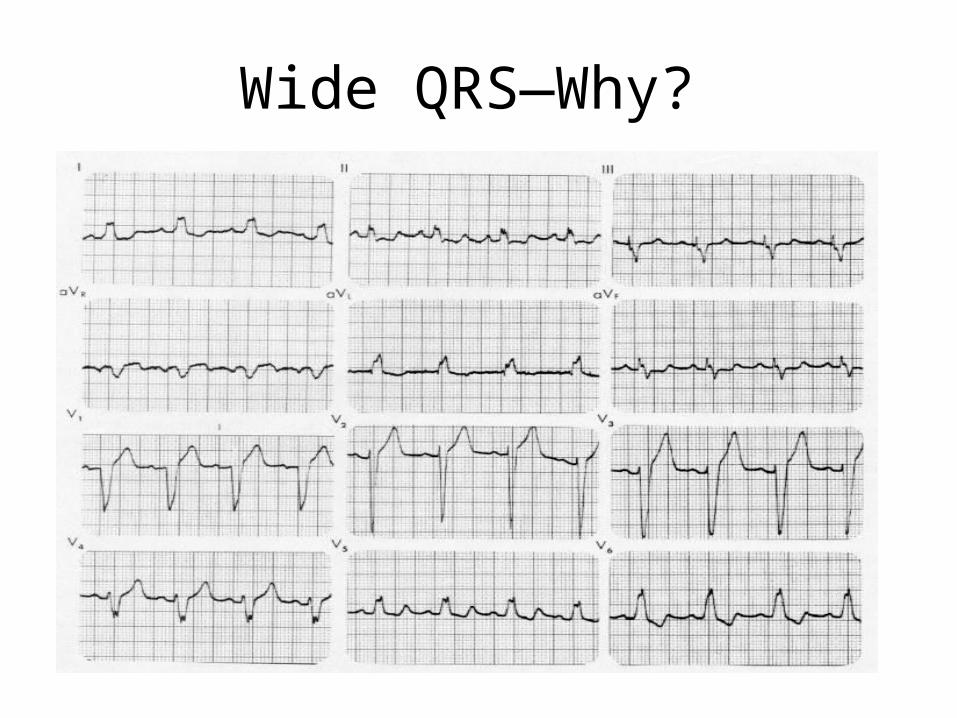
Wide QRS—Why?
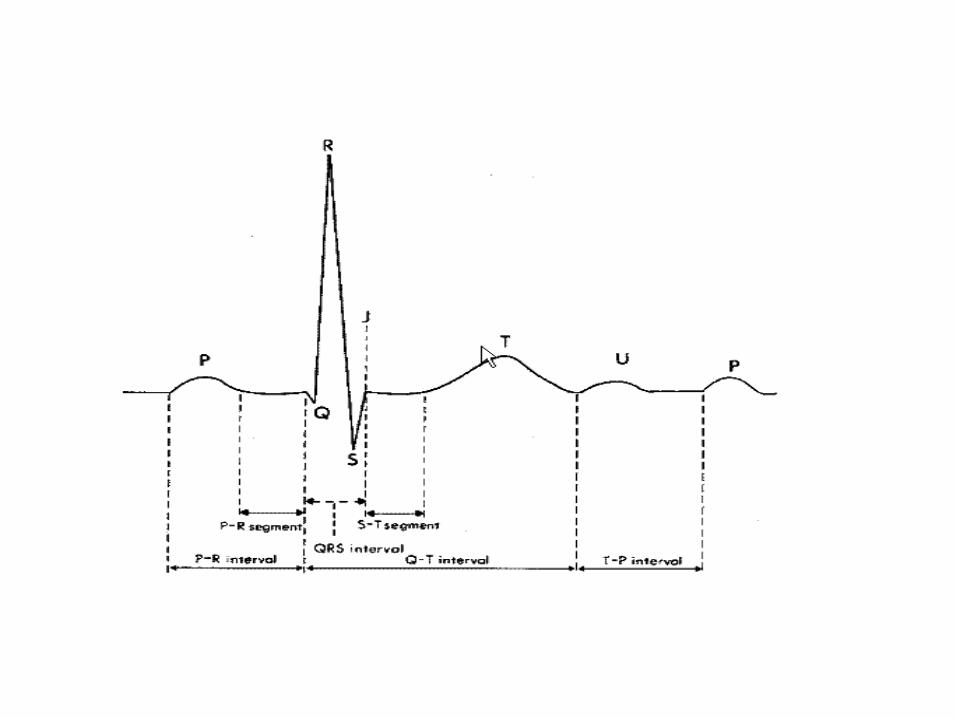
QT Interval
• Should be < ½ (R-R’ interval)• Measure from the start of the QRS to end of T wave• Varies with heart rate, so correct for RR interval• Normal QTc: women=0.44, men=0.42• QTc = QT (#of small squares) x 0.04
√RR
• Long QT can lead to ‘R on T’Death
Causes of Long QT**Think ‘Lytes and Meds first!• Low K, Low Ca, Low Mg• Macrolides, Quinolones• All Antipsychotics (Haldol worst, Geodon
least)• SSRIs• Sotalol, Quinidine, Ondansetron, Amio, TCAs• Pts w/LVH or CHF are predisposed to medication-
related lengthening of QT interval! – Avoid Macrolides, Quinolones in them!
Long QT: Less common causes
• Hypothyroid• Hypothermia• AV Block• MI• CVA• Head injury• Congenital long QT
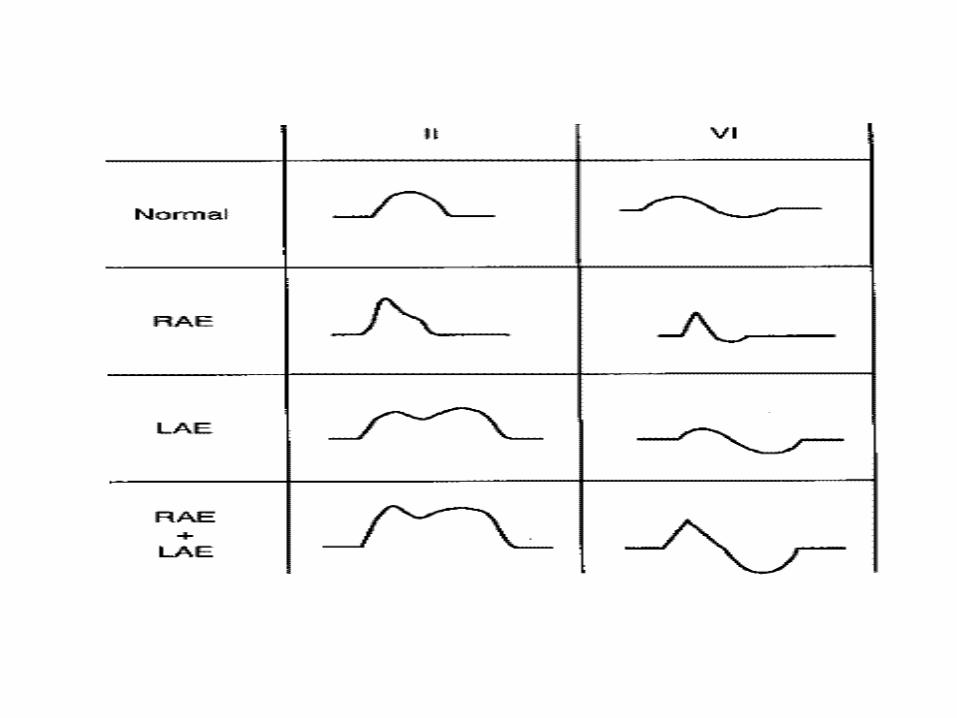
Atrial Enlargement
RAE• P wave is tall and peaked (>2.5mm high)• OR Biphasic P wave with initial positive inflection• Ddx: Pulmonary HTN, COPD, PE
LAE• P wave is wide (>0.12 sec) and notched in the middle
“M”• OR Biphasic P wave with terminal negative inflection• Ddx: Systemic HTN, Aortic Insufficiency, Mitral
Stenosis
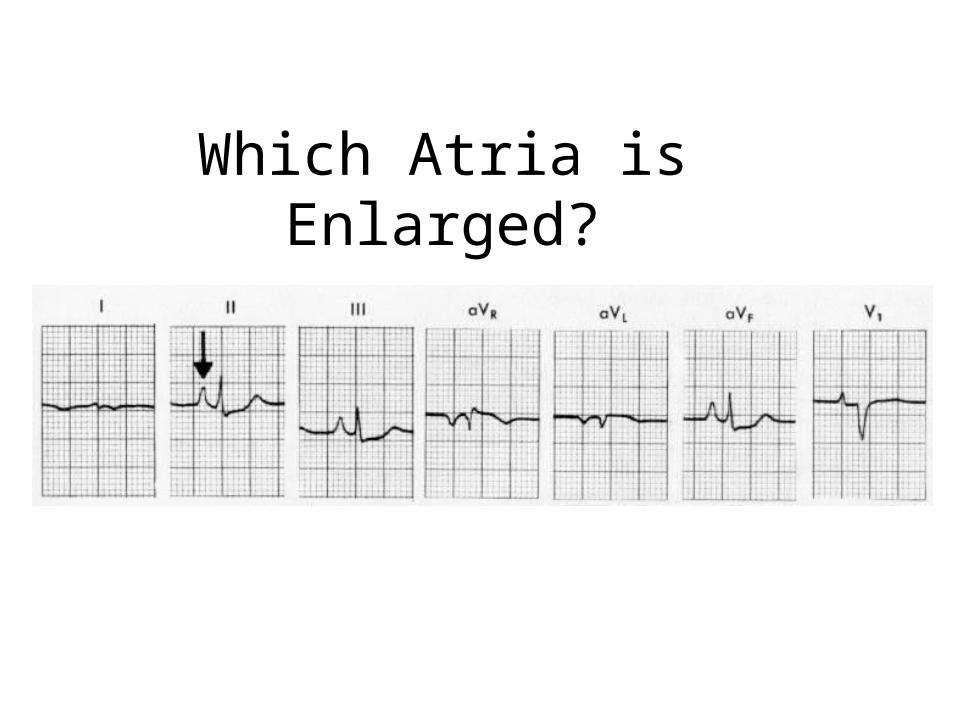
Which Atria is Enlarged?
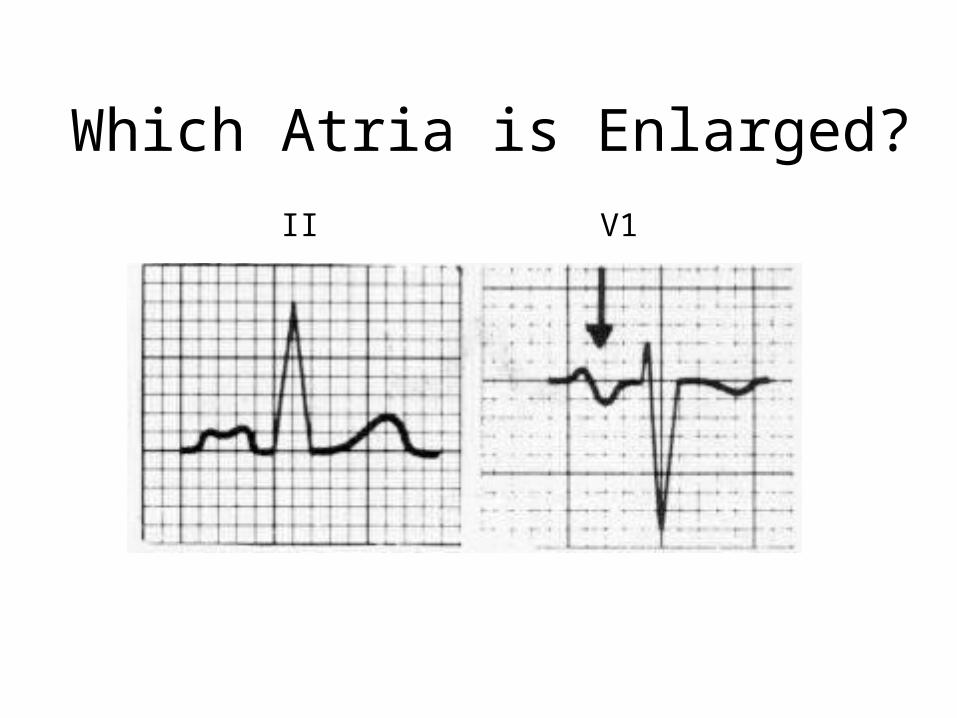
Which Atria is Enlarged?
II V1
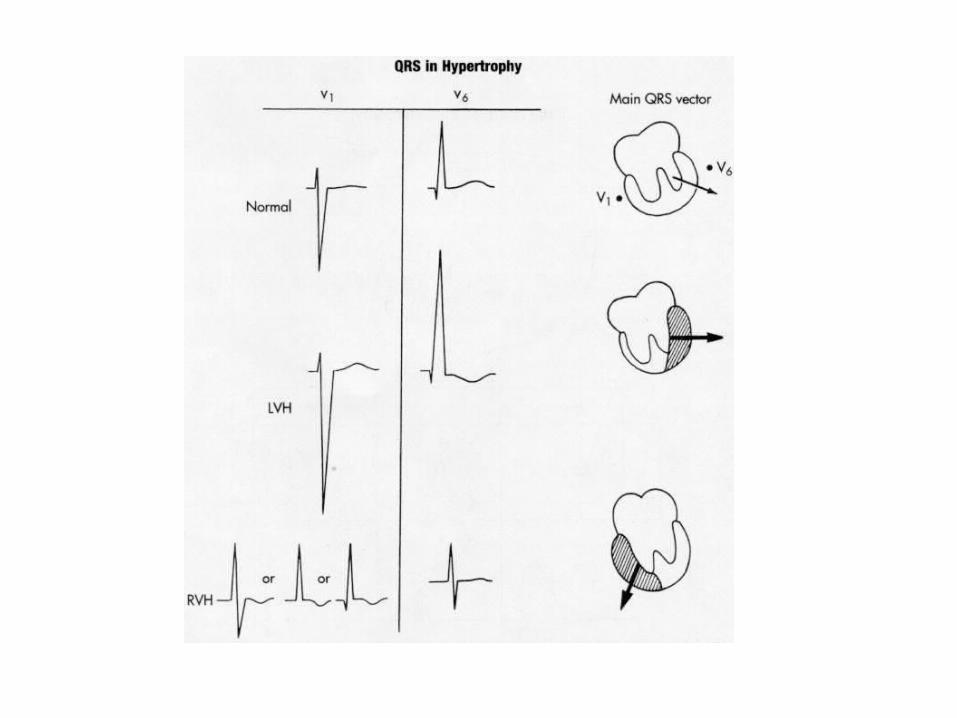
LVH Criteria
• Sokolow + Lyon– S V1+ R V5 or V6 > 35 mm
• Cornell criteria (Circulation, 1987;3: 565-72) – S V3 + R avl > 28 mm in men – S V3 + R avl > 20 mm in women
• Framingham criteria (Circulation,1990; 81:815-820) – R avl > 11mm, R V4-6 > 25mm – S V1-3 > 25 mm, S V1 or V2 + – R V5 or V6 > 35 mm, R I + S III > 25 mm
• Romhilt + Estes (Am Heart J, 1986:75:752-58) – Point score system (Am Heart J, 1999;37:161)
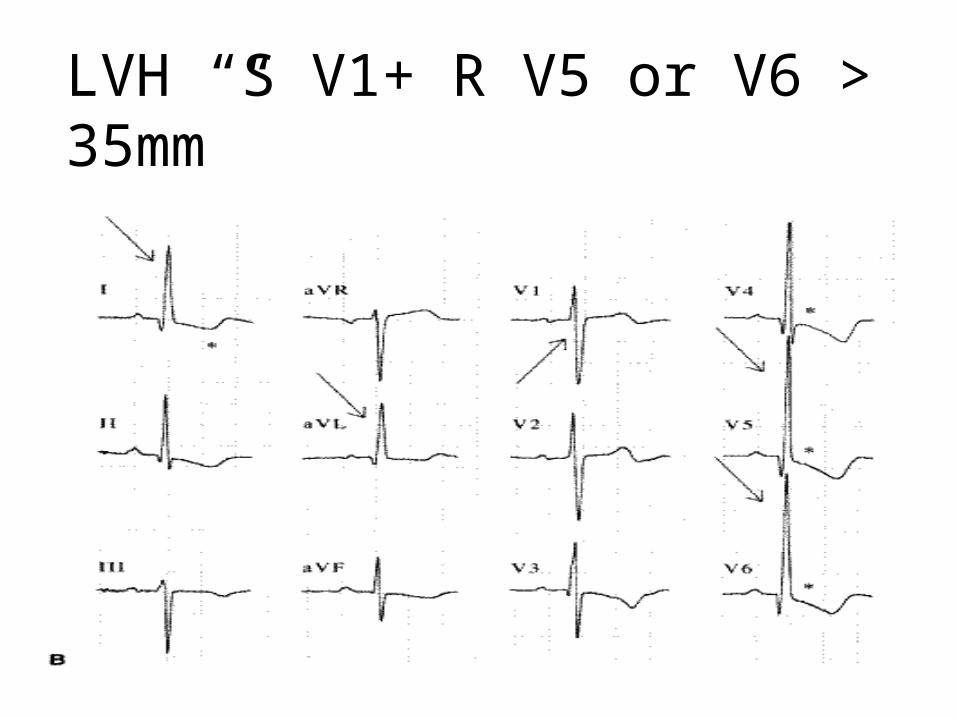
LVH “S V1+ R V5 or V6 > 35mm”
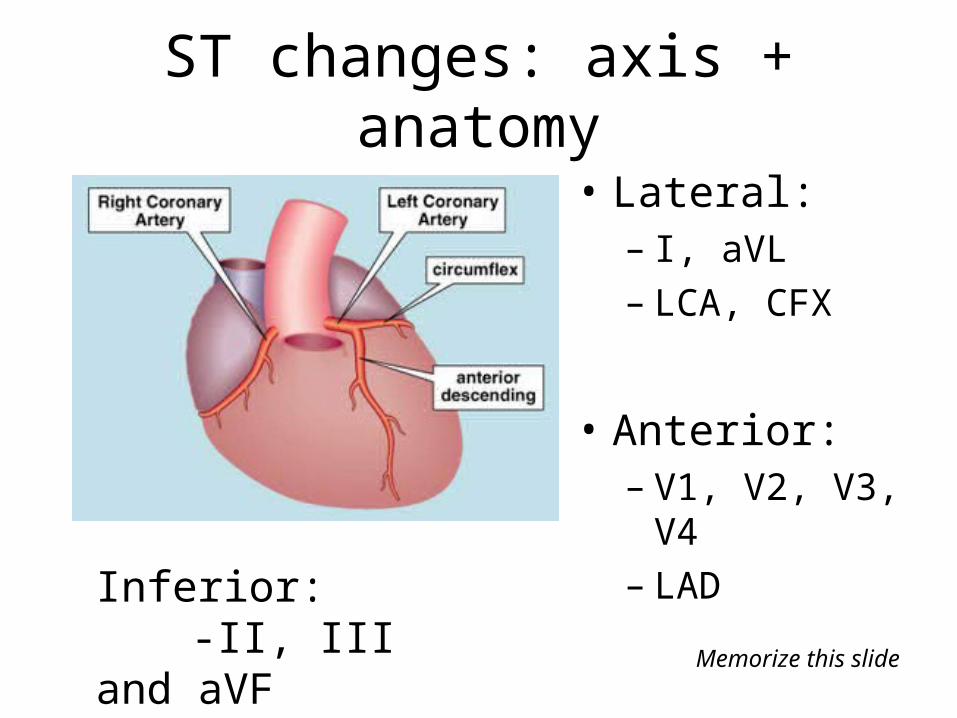
ST changes: axis + anatomy
• Lateral: – I, aVL– LCA, CFX
• Anterior:– V1, V2, V3, V4– LAD
Inferior:-II, III and aVF-RCA (or LCA)
Memorize this slide
Q waves
• Normal Q wave:– Small septal Qs in I, aVL, V5, V6– Isolated Qs in III, V1
• Pathologic Q wave: – wider than 1 small box (0.04 sec)– OR >25% height of the R wave in that complex
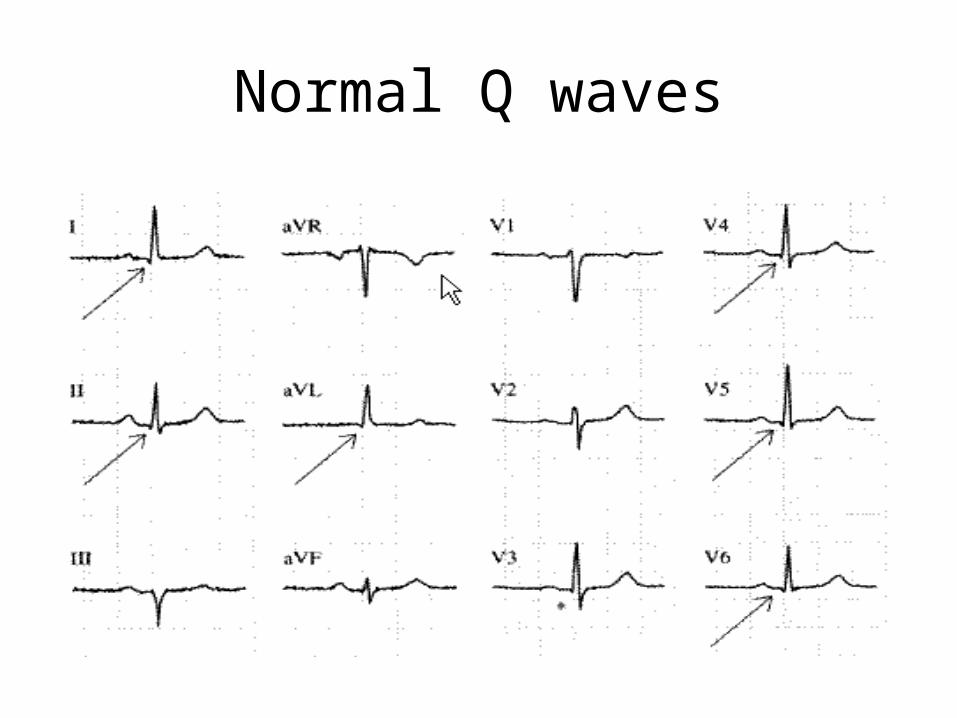
Normal Q waves
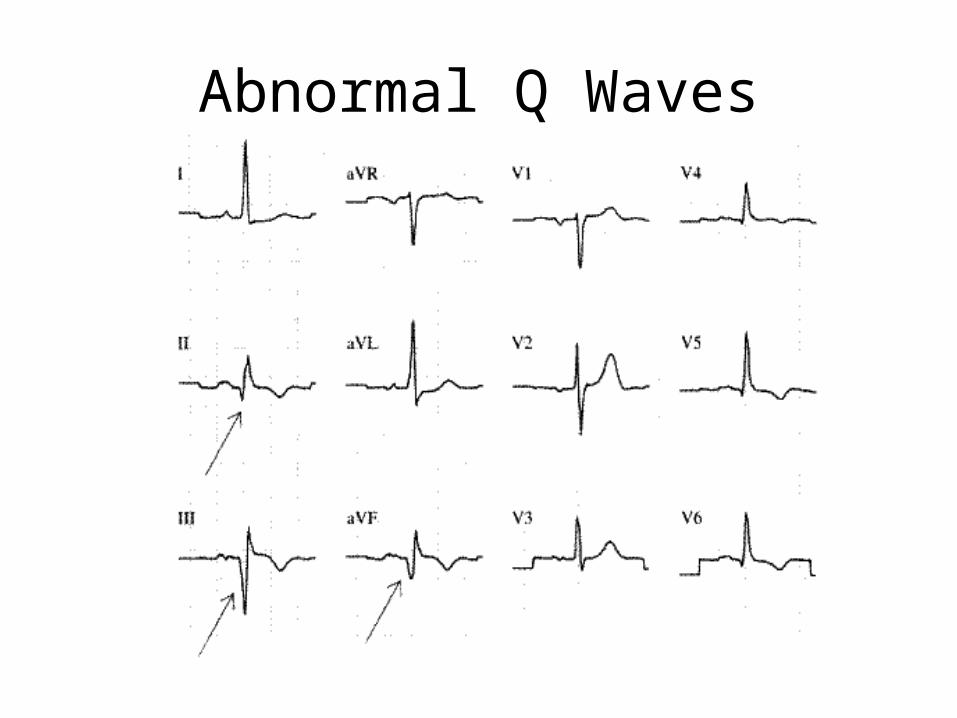
Abnormal Q Waves
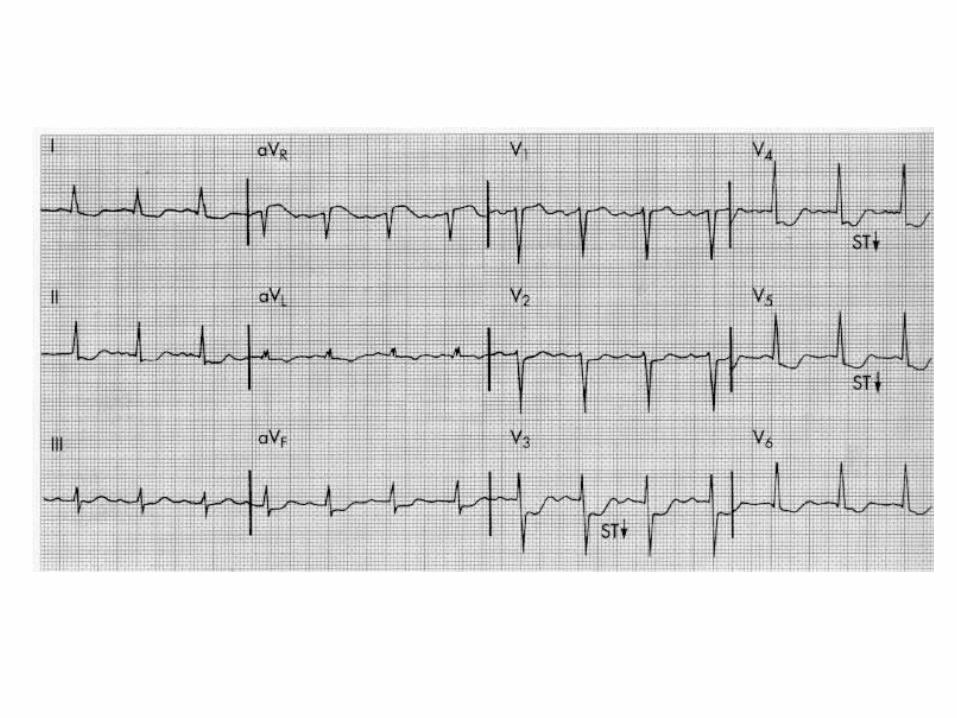
Non-ST Elevation MI
=Severe subendocardial ischemia• Marked, diffuse ST depressions in I, II, III, aVL ,
aVF , V2-V6
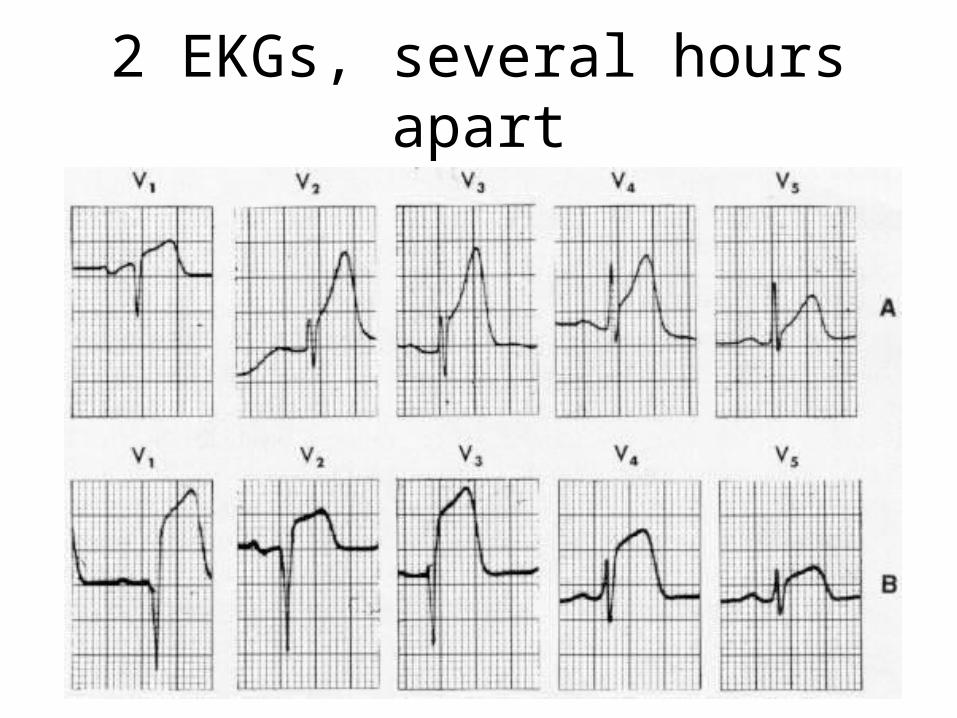
2 EKGs, several hours apart
Acute ST Elevation MI
1. Normal2. Hyperacute
• T wave Elevation3. Acute
• ST Elevation4. Hours Later
• ST Elev, Q begins to form, T wave inverts5. Days Later
• Q wave, T wave inversion6. Weeks Later
• Q wave
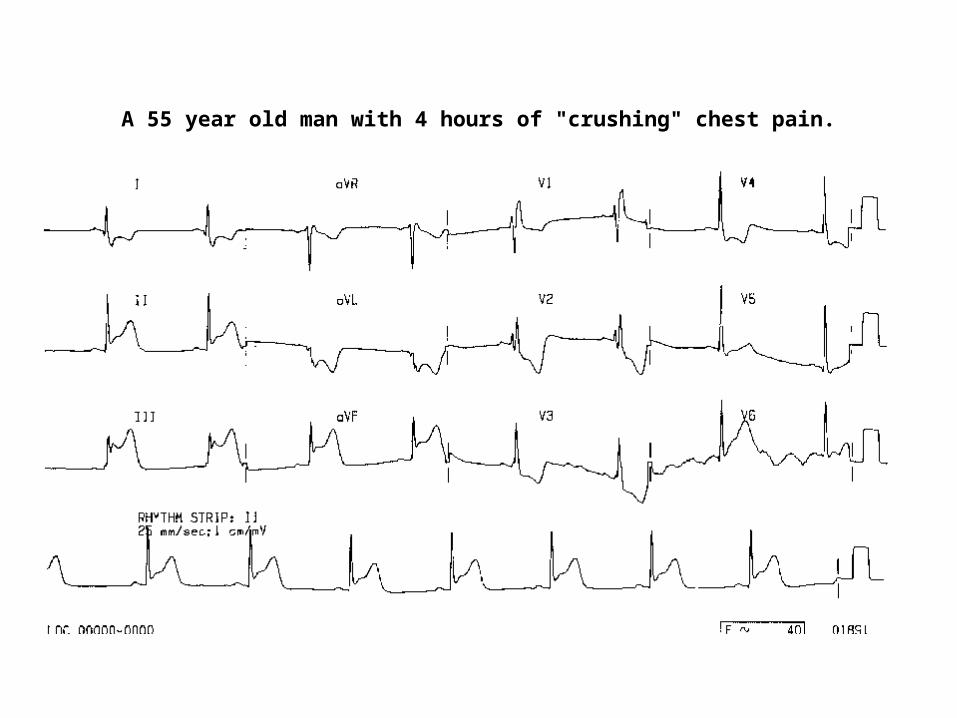
A 55 year old man with 4 hours of "crushing" chest pain.
Acute Inferior Wall MI
• ST elev in II, III, AVF• Reciprocal ST depression in anterior leads (V2-V4)
=RCA occlusion (some LCx)
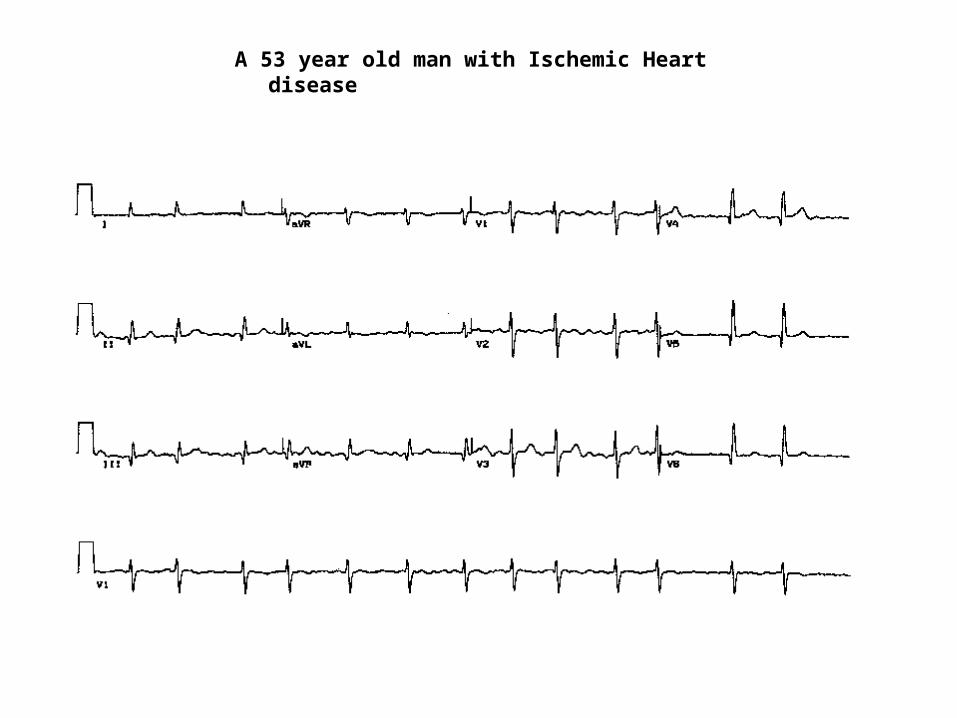
A 53 year old man with Ischemic Heart disease
Old Inferior Wall MI
• Pathologic Q wave in II, III, AVF: – wider than 1 small box (0.04 sec)– OR >25% height of the R wave in that complex
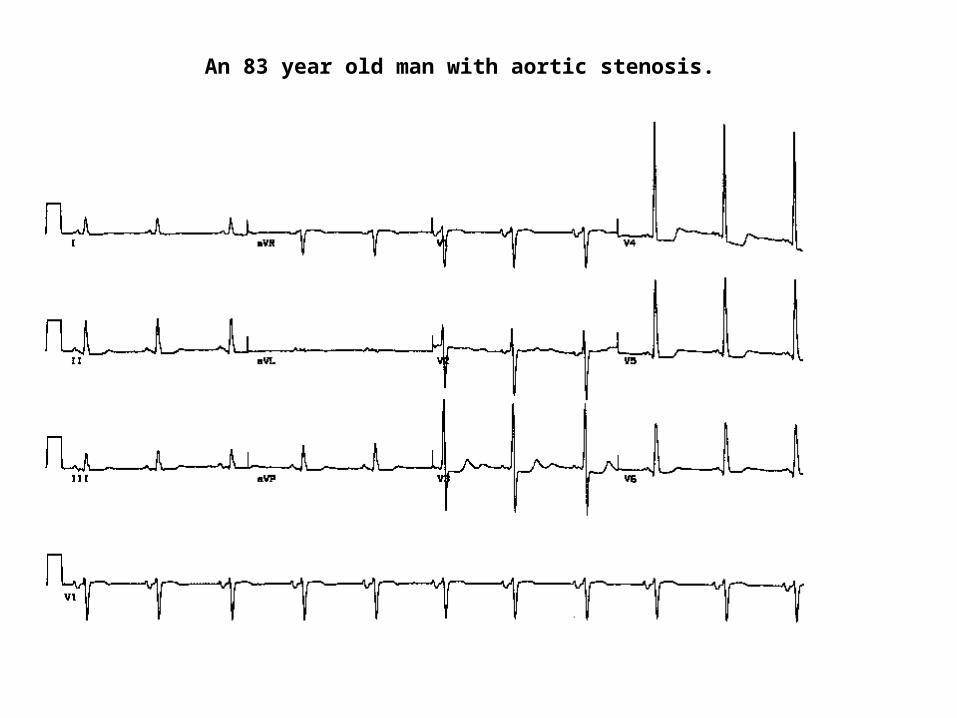
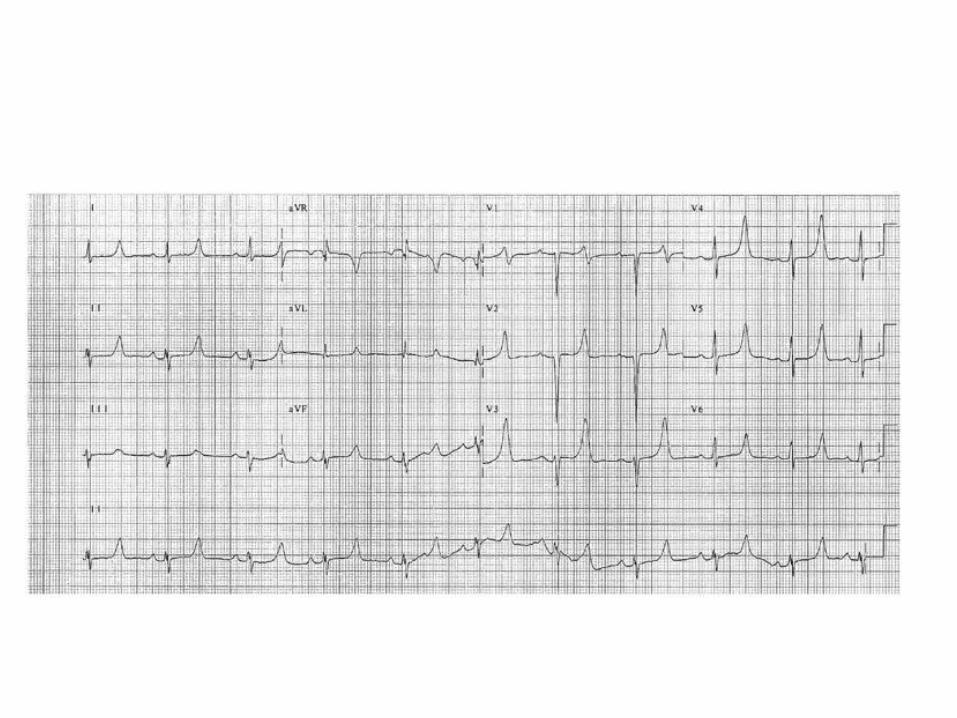
An 83 year old man with aortic stenosis.
LVH, LAE
• Romhilt-Estes LVH Point System:• 3 points for Left Atrial Enlargement
– M shaped P wave in II – P has prominent terminal negative component in
V1
• 3 points for:– R wave in V5 or V6 >30mm– or S wave in V1 or V2 >30mm– or R or S in limb leads>20mm
• >5 points: definite LVH
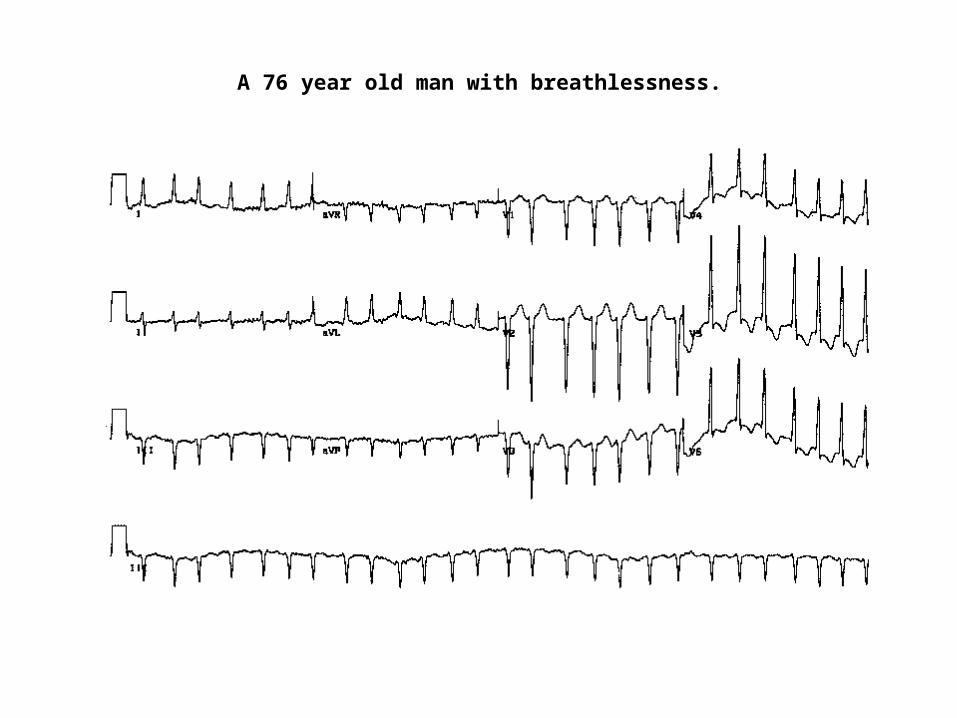
A 76 year old man with breathlessness.
Afib with RVR
• Irregularly irregular ventricular rhythm. • Must look carefully to see it is NOT regular
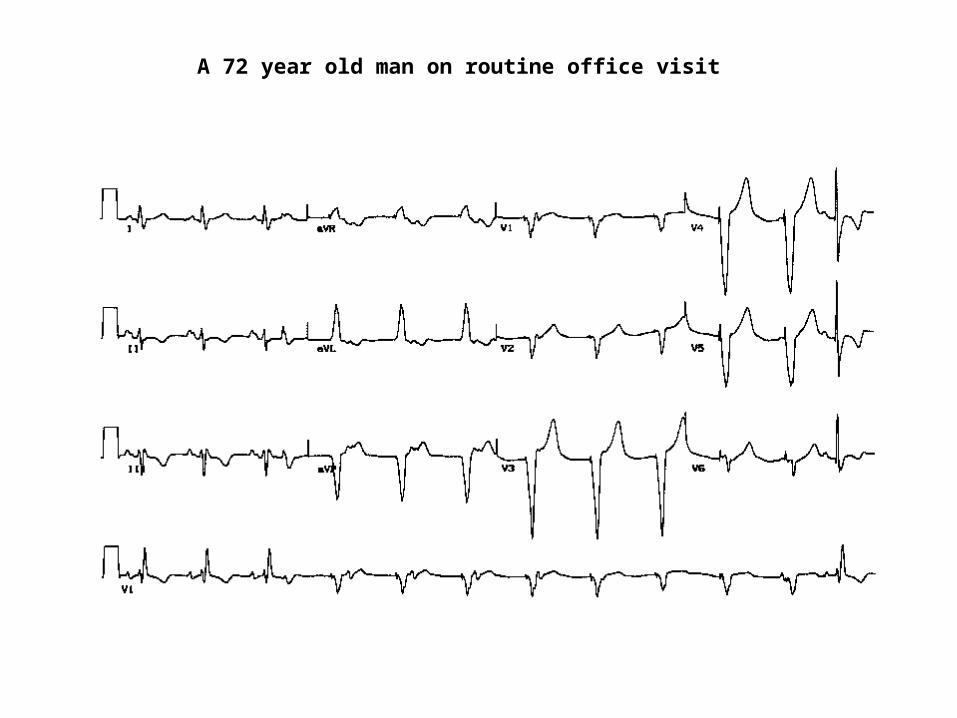
A 72 year old man on routine office visit
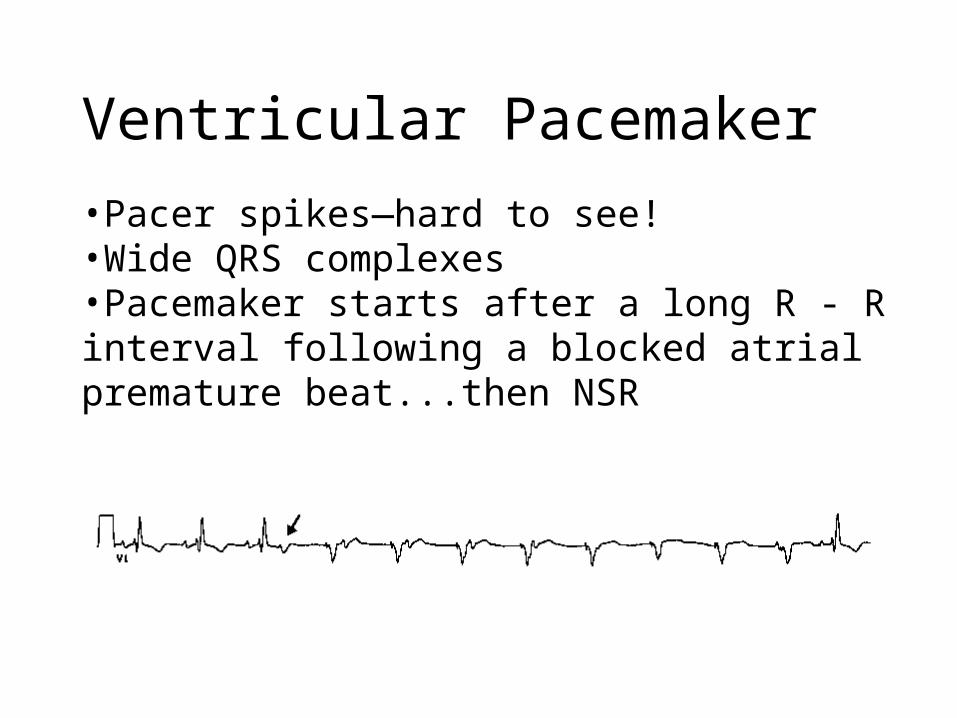
Ventricular Pacemaker
•Pacer spikes—hard to see! •Wide QRS complexes•Pacemaker starts after a long R - R interval following a blocked atrial premature beat...then NSR
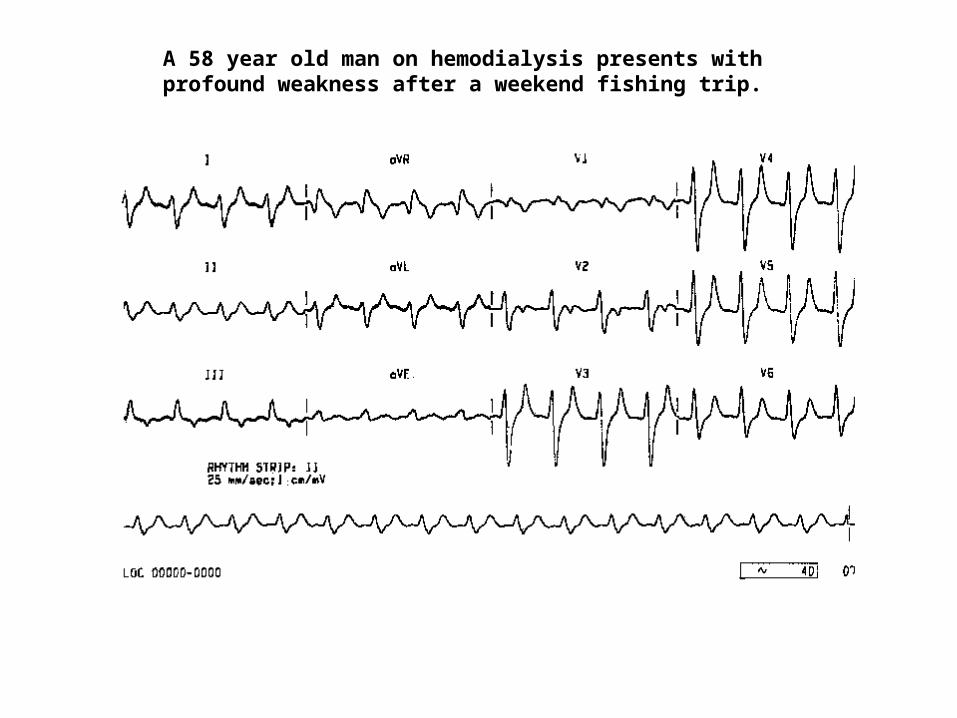
A 58 year old man on hemodialysis presents with profound weakness after a weekend fishing trip.
Hyperkalemia
K >8.0• Wide, tall and tented T waves • Wide QRS • Small or absent P waves • Atrial fibrillation • Shortened or absent ST segment • Ventricular fibrillation
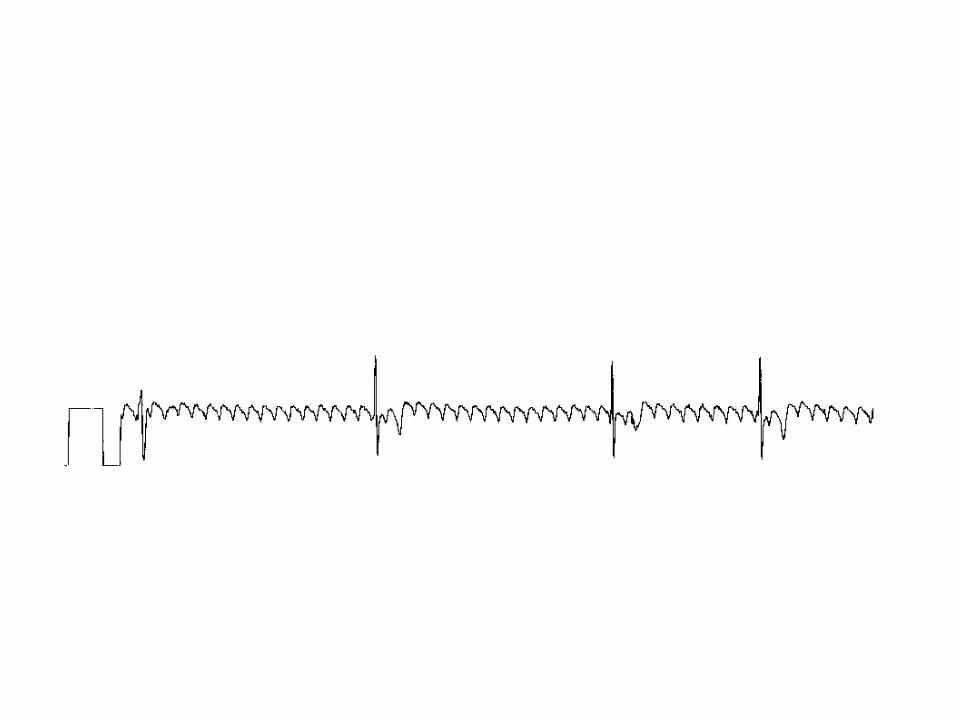
Atrial Flutter
• Saw tooth baseline with rate of 250-300
• Causes:– Ischemic heart disease– Hypertension– Mitral valve disease– Thyrotoxicosis– Cardiomyopathy
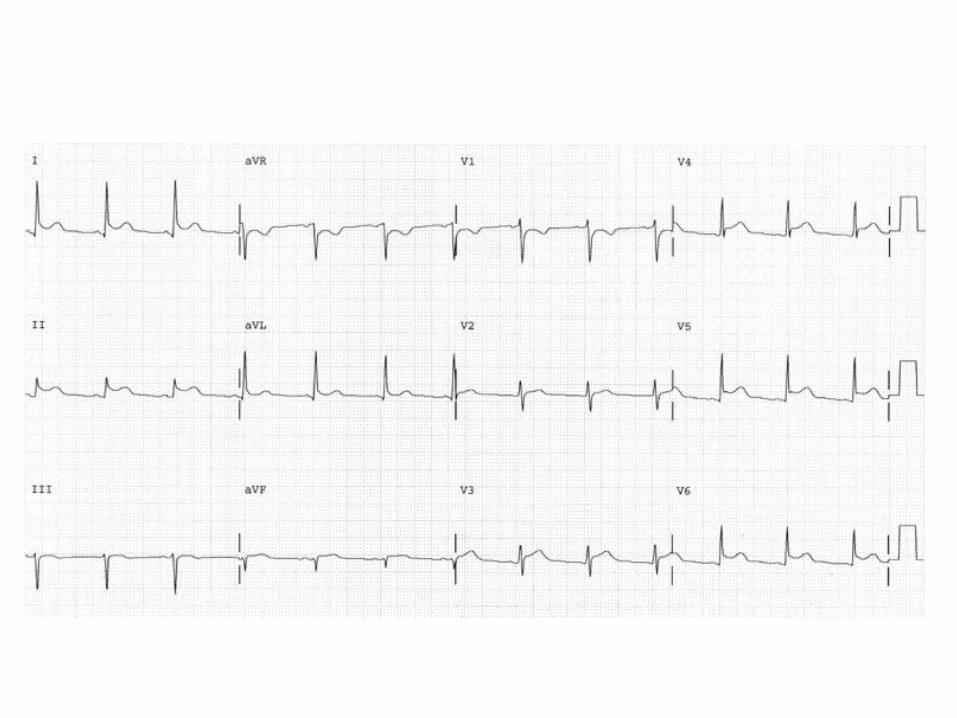
Pericarditis
Evolves over hours-weeks
1. PR depression, ST elevation (concave up) in same leads, upright T
2. Normal P, normal ST, flat T
3. Normal P, normal ST, T Wave inversion
4. normal P, normal ST, upright T
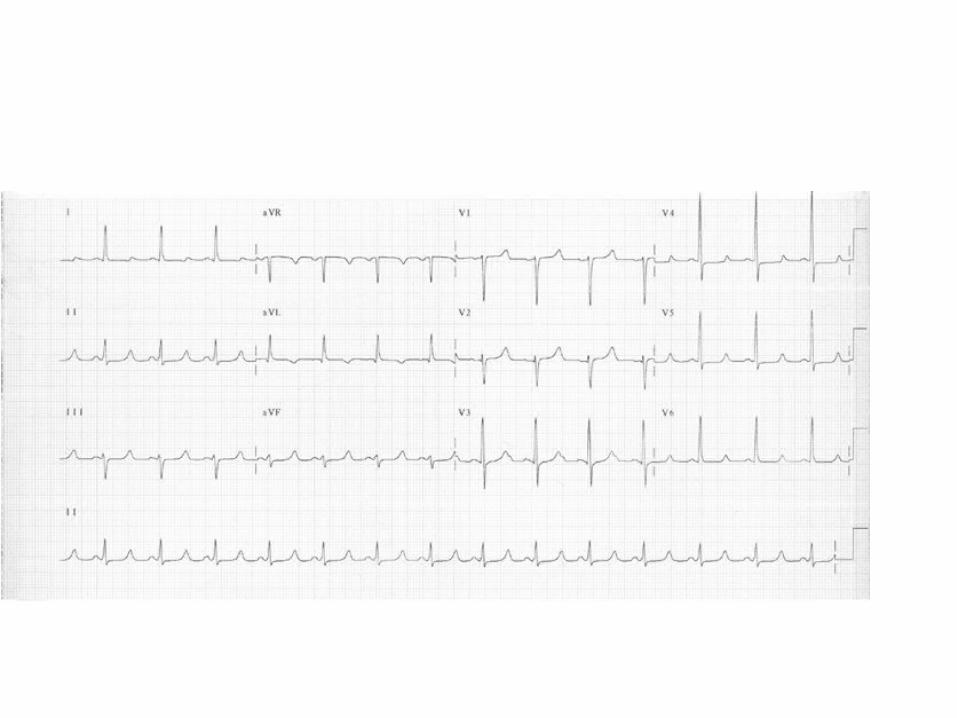
Hypocalcemia
• Long QT
• Inverted T waves