Embed Size (px)
Citation preview

EKG ROUNDSBundle Branch Blocks
07. 04. 2005
Nadim Lalani

OUTLINE
• RBBB• LBBB• HEMiBLOCKS/ FaSCicULAR BLOCKS

Case
• A 13-year-old male.presents with a history of Syncpoe:
• What else do you want to know on hx?


Brugada Syndrome: • Described in 1992:
• Syndrome consisting of syncopal episodes and/or sudden death in patients with a structurally normal heart.
• Characteristic ECG with a pattern of right bundle branch block with an ST segment elevation in leads V1 to V3 was
• In 1998 recognised poor prognosis of patients with the syndrome not receiving an implantable defibrillator.

Brugada Syndrome:
• Epid:incidence of 0.05% to 0.6%. Mostly SE Asian / Japanan autosomal dominant mode of transmission.
• Who?: Adults 30-40 (first case reports were kids)
• Related to defect of SCN5a Fast sodium channel predisposing pt to re-entry circuit.

Brugada Syndrome: Clinical manifestations
• The complete syndrome is characterised by episodes of rapid polymorphic VT in patients. Resulting in syncopal attacks.
• When the episodes are sustained, cardiac arrest and eventually sudden death occur.
• There exist asymptomatic individuals in whom the atypical ECG is detected during routine examination.
• NB now known some variation in the EKG (three types of ST changes/ a-fib &c)

Brugada Syndrome:
• Diagnosis:• the typical ECG pattern and there is a history of aborted
sudden death or syncopes caused by a polymorphic VT. • There are also many patients with a normal ECG.
Syndrome only recognised a posteriori when the typical pattern appears in a follow-up ECG or after the administration of pro-arrythmics.
• Additional diagnostic problems are caused by the changes in the ECG induced by the autonomous system and by antiarrhythmic drugs.

Brugada Syndrome:
• Prognosis and treatment:
implantation of a cardioverter-defibrillator is mandatory in these patients.
Case report of a 23 yold patient being managed on amiodarone until implantation

Case
• Mrs M. 39 yo female had a pulmonary artery prosthesis and ASD repair 3 weeks ago. Helathy otherwise . On Lipitor. Presents with migratory arthralgias/myalgias.
• EKG Diagnosis?• Axis?

RBBB, axis 0-30 deg

RBBB
• Three phases:Septal depolarisation.Left ventricular depolarization. Delayed stimulation of the right
ventricle.

RBBB
septal depolarization produces a small septal r wave in V1 and a small septal q wave in V6
depolarization of LV produces an S in V1 and an R in V6
delayed right ventricular depolarization produces a wide R wave in V1 and a wide S wave in V6

RBBB Summary
• Right Leads ( V1 eg) show an rSR’ complex with a wide R wave.
• Occasionally, however, the S wave never quite makes its way below the baseline. Consequently, the complex in lead V1 has the appearance of a large notched R wave (“rabbit ears”)
• Left Leads (I,V6) show a qRS pattern with a wide S wave.

Case 2
• Mr R . 55 yo admited to FMC after head-on MVC in which he sustained Multiple rib #s,# L Hip and # L ulna. 2 days post-admit develops acute SOB with sat 80%.
• EKG Diagnosis?• Axis?• Comment on T waves?

RBBB, ?RAD, TWI’s
Primary TWI’s

ST changes
• TWI’s in the right chest leads are a characteristic finding with RBBB.
• These inversions are referred to as secondary changes because they reflect just the delay in ventricular stimulation.
• By contrast, TWI’s in V5,V6 are primary T wave abnormalities reflect an actual change in repolarization (ie ischemia &c.)

Case 3
• 80 yo guy with HTN. Presents with this EKG:

RBBB, Axis apprx 30-90deg, Atrial Flutter

Sometimes can be Rate Dependent

COMPLETE AND INCOMPLETE RBBB
• Depends on the width of the QRS complex:
Complete RBBB is defined by a QRS that is 0.12 second or more with an rSR in lead V1 and a qRS in lead V6.
Incomplete RBBB shows the same QRS patterns, but its duration is between 0.1 and 0.12 second


Case 4:
• 77 yo M with HTN, and known CAD:

LBBB

Left Bundle Branch Block
• With LBBB the septum depolarizes from right to left .Therefore the EKG loses the normal septal r wave in lead V1 and the normal septal q wave in lead V6.
• Left ventricular depolarization is prolonged, yielding a wide QRS.
• Lead V6 you see a wide, entirely positive (R) wave.
• In the right chest leads (e.g., V1 ) you see a negative QRS (QS) complex.
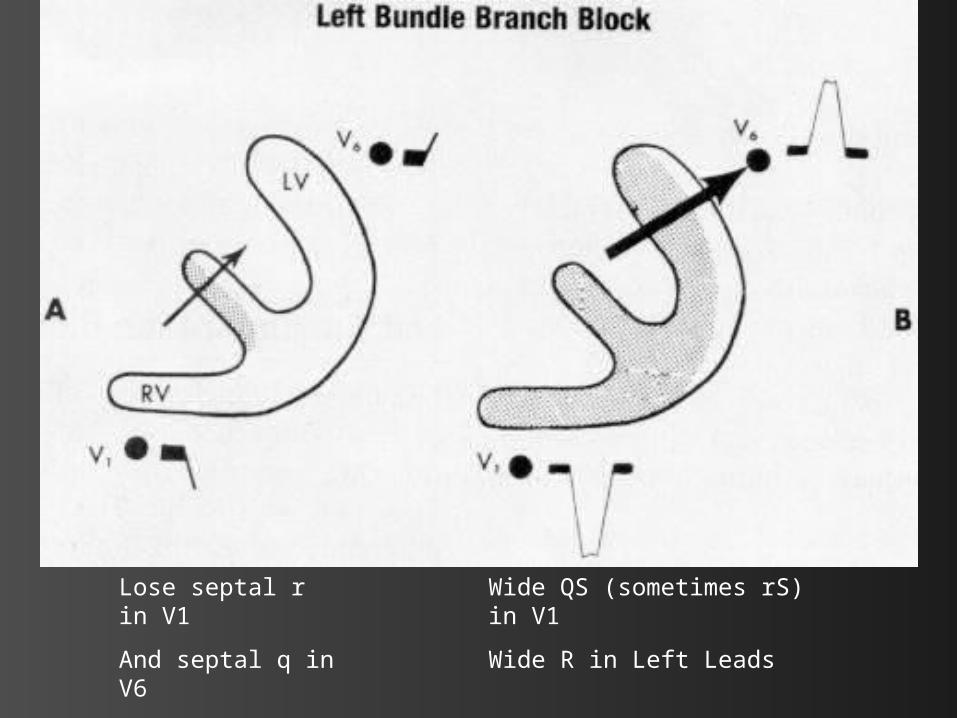
Lose septal r in V1
And septal q in V6
Wide QS (sometimes rS) in V1
Wide R in Left Leads


• Congenital septal lesions, CAD, anterior MI (occlusion of proximal LAD), pulmonary
hypertension, normal variant in 0.2% adults

Summary RBBB vs LBBB:

r
S
R’
q
R
S
QS
R

Fascicular Blocks (Hemiblocks)
• The RBB is a single pathway consisting of just one main fascicle or bundle.
• In contrast the LBB has an anterior fascicle and a posterior fascicle.

The “Trifascicular Highway”

EKG Changes:
• Hemiblock (unlike a full LBBB or RBBB) does not widen the QRS complex.
• Main effect is a change in the QRS axis: Left anterior fascicular block results in
marked left axis deviation (-30° or more) Left posterior fascicular block produces
marked right axis deviation (+120° or more).


• Left anterior hemiblock shifts the QRS axis to the left by delaying activation of the more superior and leftward portions of the left ventricle.
• Left posterior hemiblock shifts it to the right by delaying activation of the more inferior and rightward portions of the left ventricle.
• In both cases the QRS axis therefore is shifted toward the direction of delayed conduction.

Axis?
Between -30 and -90 deg LAD

Axis?RAD

Case
• 67 yo M Obese, Hx CHF. Presents with SOB:
• EKG Dx?• Is he having an MI?


LBBB and acute MI
Sgarbossa et. al. :
• 131 patients from GUSTO-I trial who had LBBB with MI. Matched with controls. Came up with following criteria:
ST-segment elevation . 1 mm concordant with QRS complex – 73 % sens and 92 % spec for acute MI.
ST-segment depression . 1 mm in lead V1, V2 or V3 – highly specific (96%) but less sensitive (25%) for MI
ST-segment elevation . 5 mm discordant with QRS complex – 31 % sens, 92 % spec.

ST ↓Concordant
ST ↑
Discordant
ST ↑ ST ↓
Shlipak MG, Lyons WL, Go AS, et al. Should the electrocardiogram be used to guide therapy for patients with left bundle branch block and suspected myocardial infarction?
JAMA 1999;281:714–19.:
• Reviewed patients presenting with LBBB and an acute cardiopulmonary history and assessed the usefulness of the Sgarbossa criteria.
• Criteria had a sensitivity of 10% and a specificity of 100%.
• Most (90%) patients with AMI will not meet the criteria.
• Support thrombolysing all patients (except those with contraindications) who have a history suggestive of AMI and LBBB.

Practice Time:

Case A
• 65 yo M smoker with DM presents with 4 hours RSCP:
• EKG Diagnosis?• Axis?


Case BRBBB, ? Primary TWI’s V4,V5

Case CLBBB

Case D

LBBB, ? LAD

Case ERBBB

Case FLBBB

Case GRBBB with PAC’s

Case HBifascular: RBBB with LAFB

Case IRBBB with Primary TWI’s

Case J
RAD

Case KRAD ?LPFB
References
• Goldberger: Clinical Electrocardiography: A Simplified Approach, 6th ed.,1999 Mosby, Inc.
• Brugada P, Brugada J: Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol 1992 Nov 15; 20(6): 1391-6