Embed Size (px)
Citation preview
ELECTROCARDIOGRAMs ELECTROCARDIOGRAMs (ECGs)(ECGs)
Cardiac Wellness Institute of Calgary
Updated May 2010
Material to be CoveredMaterial to be Covered
− ACSM’s Resource Manual for Guidelines for ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription (6th ed.)Exercise Testing and Prescription (6th ed.)− Chapter 27Chapter 27
− Rapid Interpretation of EKG’s (6Rapid Interpretation of EKG’s (6thth ed.) ed.)

LEAD PLACEMENTLEAD PLACEMENT
• Limb Leads - 6 in all - I, II, III, aVL, aVR, aVF
• Chest leads - 6 in all -V1,V2,V3,V4,V5,V6
Standard 12-lead ECG:
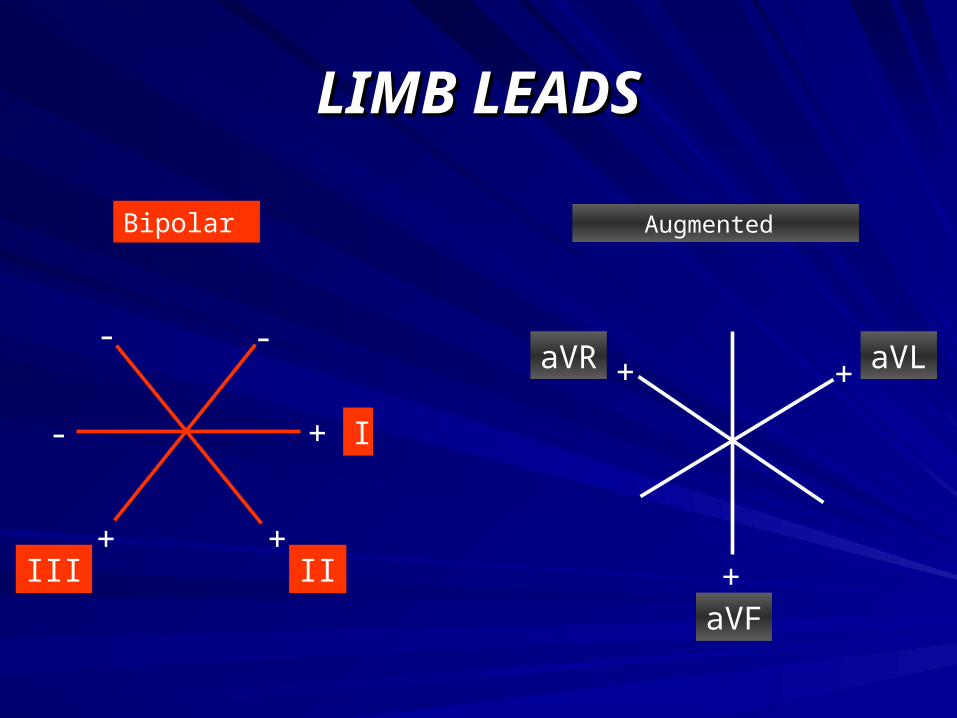
LIMB LEADSLIMB LEADS
aVLaVR
Augmented
+aVF
++
III II
I
Bipolar
+
-
+
--
+
CHEST LEADSCHEST LEADS
Along the horizontal plane:
• V1 and V2 - Right side of the heart
• V3 and V4 - Intraventricular septum
• V5 and V6 - Left side of the heart
PROCESSPROCESS
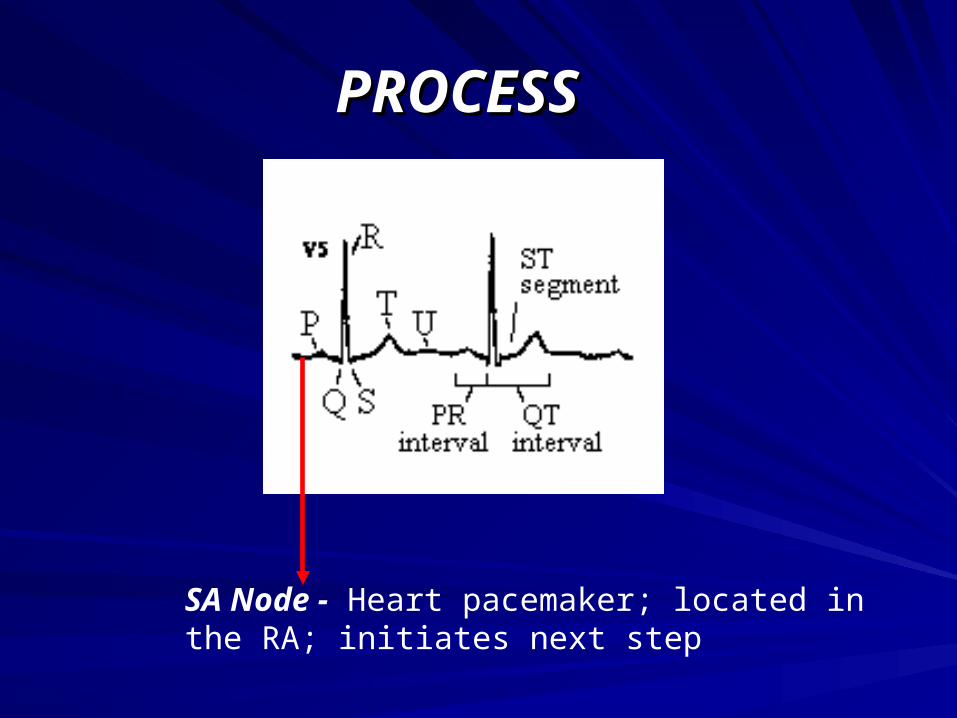
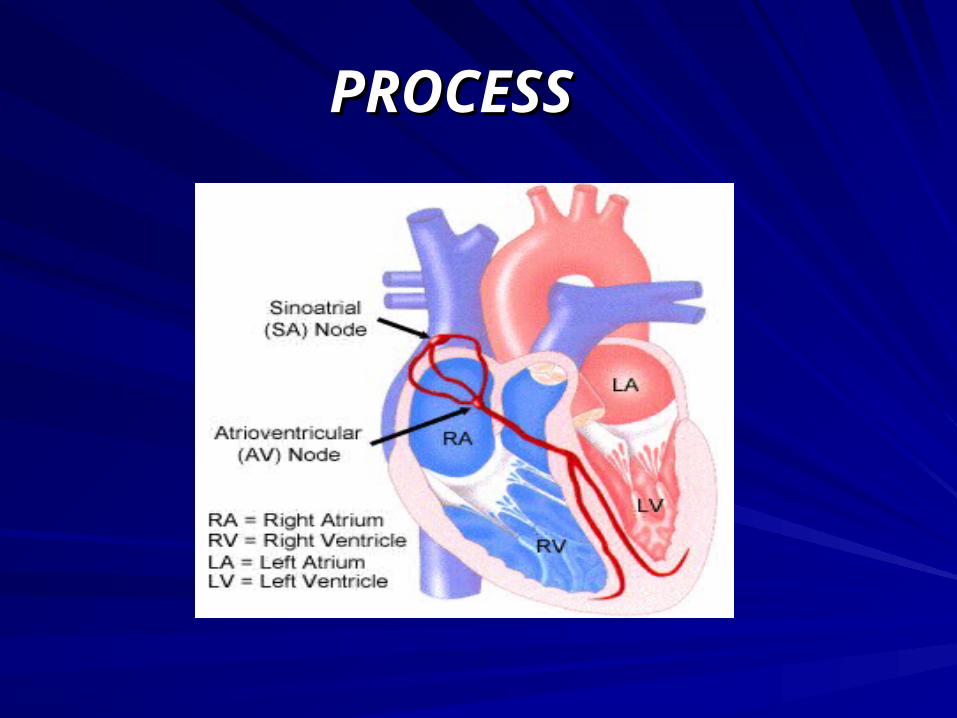
SA Node - Heart pacemaker; located in the RA; initiates next step
PROCESSPROCESS
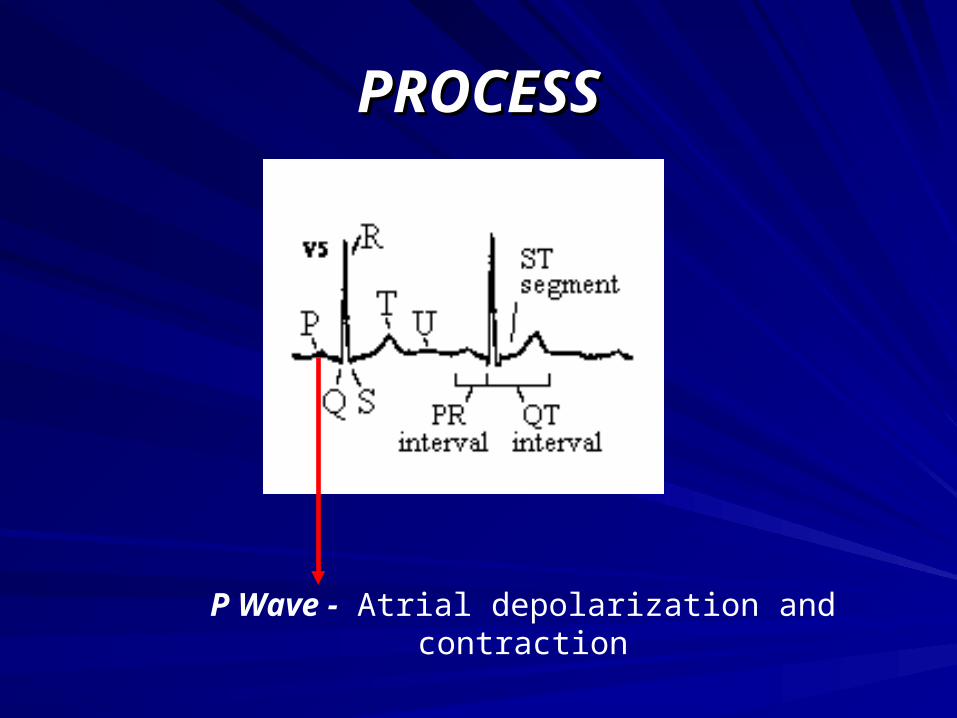
P Wave - Atrial depolarization and contraction
PROCESSPROCESS
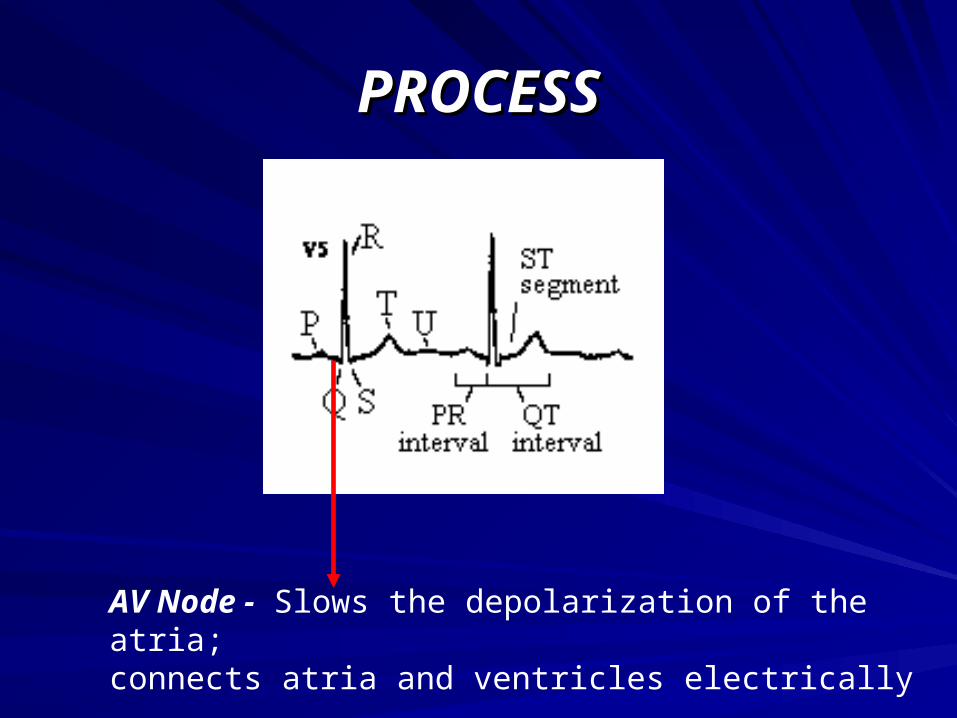
AV Node - Slows the depolarization of the atria;connects atria and ventricles electrically
PROCESSPROCESS
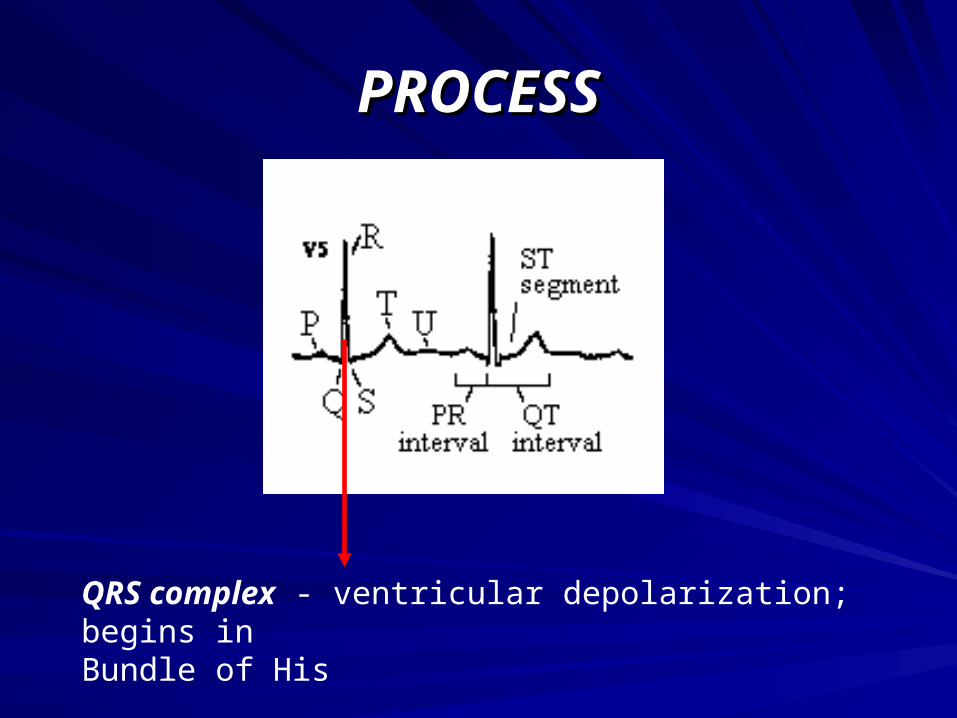
QRS complex - ventricular depolarization; begins inBundle of His
PROCESSPROCESS

VENTRICULAR DEPOLARIZATIONVENTRICULAR DEPOLARIZATION
His Bundle
Left Bundle Branch & Right Bundle Branch
Purkinje Fibers
VENTRICULAR DEPOLARIZATIONVENTRICULAR DEPOLARIZATION
• Q Wave - 1st downward wave of the complex
• R Wave - 1st upward wave of the complex
• S Wave - downward wave preceded by an upward wave
PROCESSPROCESS
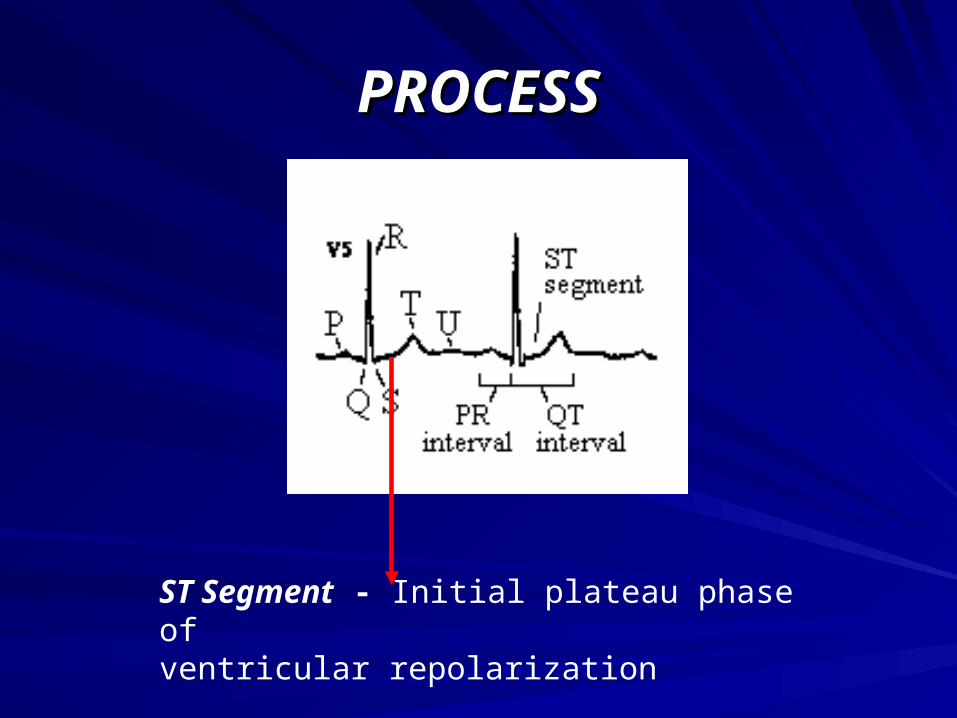
ST Segment - Initial plateau phase ofventricular repolarization

PROCESSPROCESS
T wave - Rapid phase of ventricular repolarization
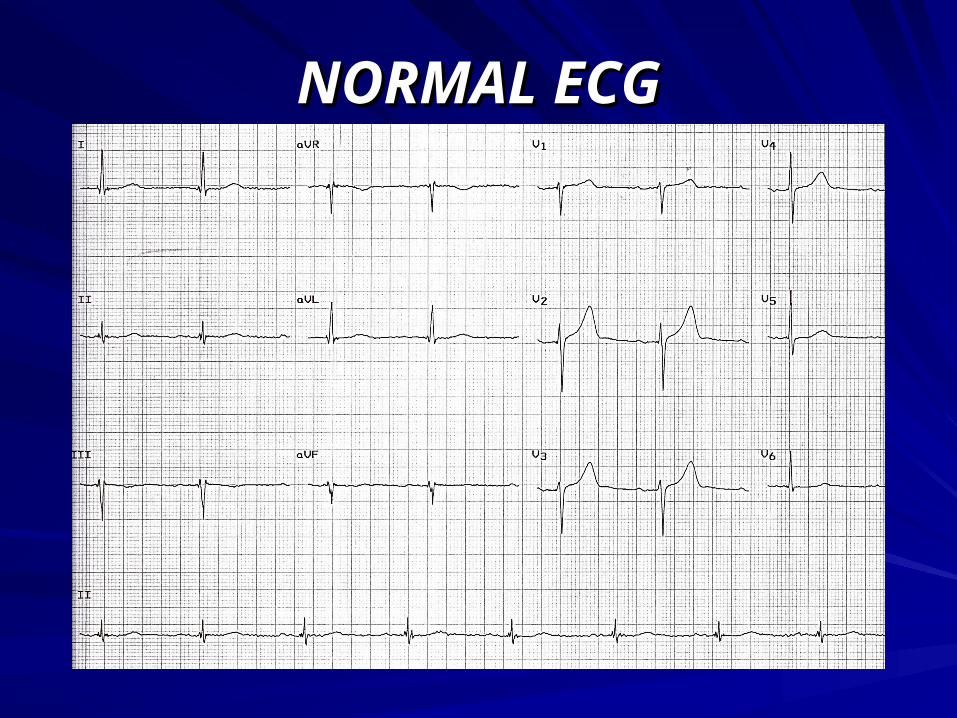
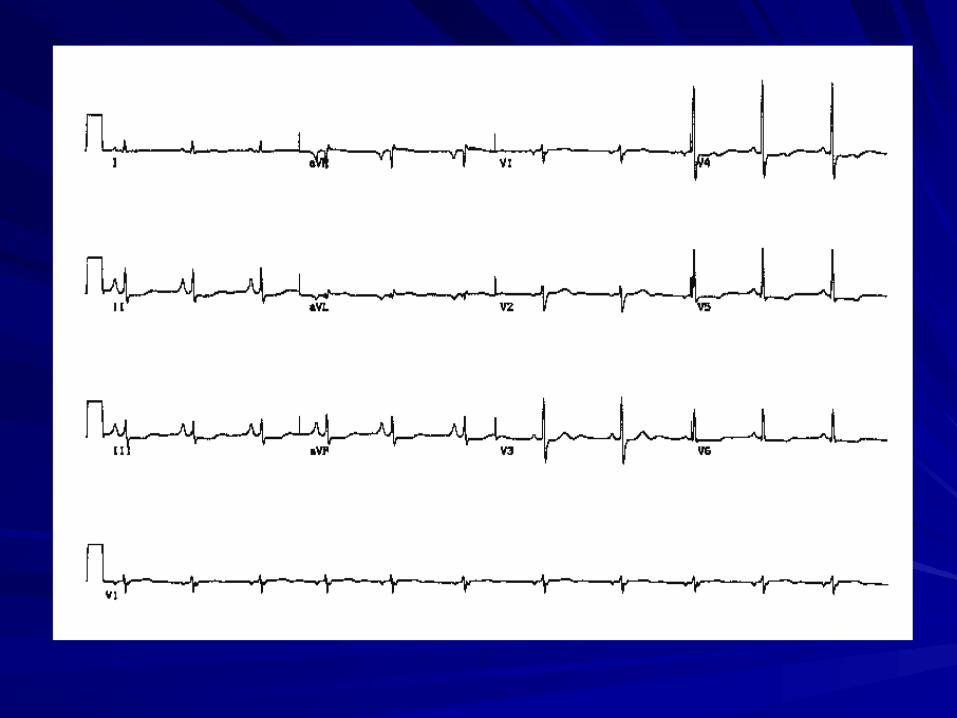
NORMAL ECGNORMAL ECG
RHYTHMRHYTHM
Normal sinus rhythm:
• Each P wave is followed by a QRS
• Regular or irregular
RATERATE• P wave rate 60 - 100 bpm with <10% variation - Normal
• Rate < 60 bpm = Sinus Bradycardia- Results from:
- Excessive vagal stimulation - SA nodal ischemia (Inferior MI)
• Rate > 100 bpm = Sinus Tachycardia- Results from:
- Pain / anxiety - CHF - Volume depletion - Pericarditis - Chronotropic Drugs (Dopamine)
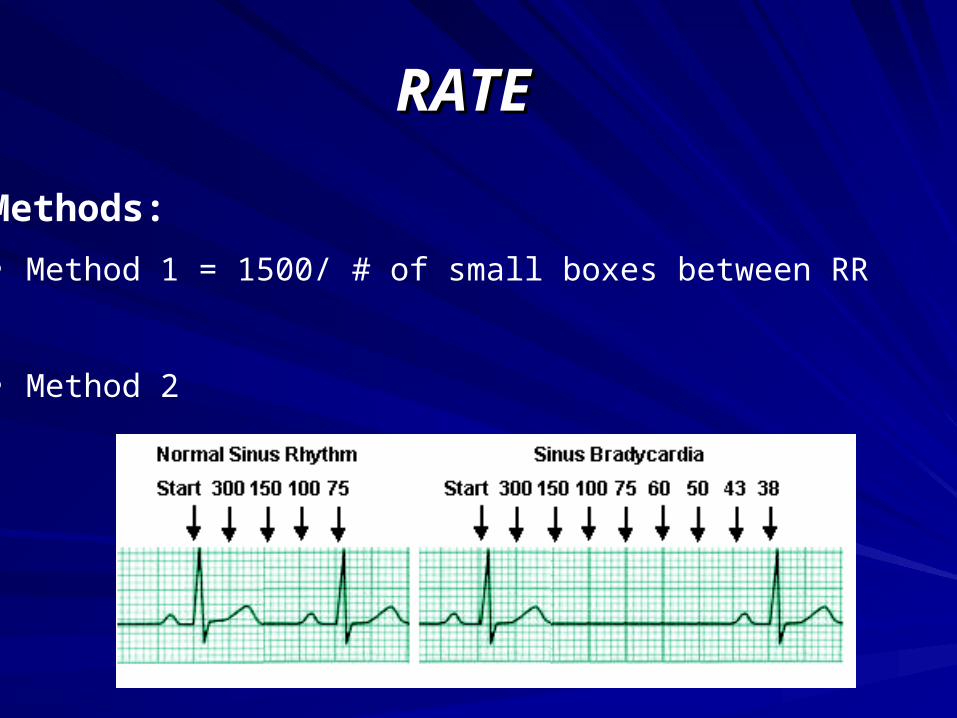
RATERATE
Methods:
• Method 1 = 1500/ # of small boxes between RR
• Method 2

P WAVEP WAVE
Normal:
• Height < 2.5 mm in lead II
• Width < 0.11 s in lead II
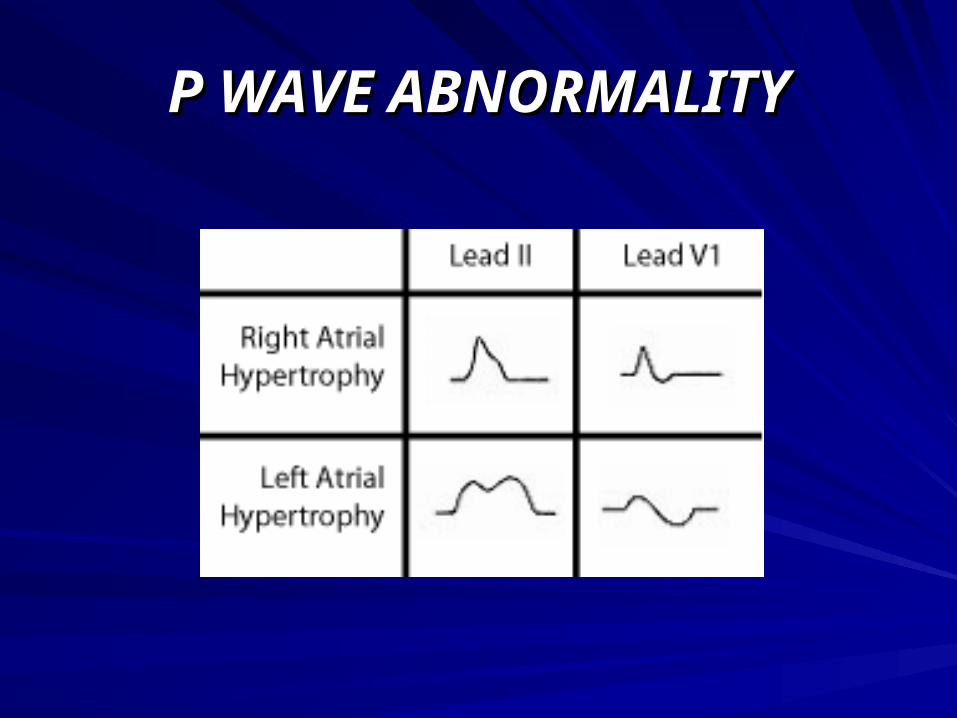
P WAVE ABNORMALITYP WAVE ABNORMALITY

P WAVE ABNORMALITIESP WAVE ABNORMALITIES
Right atrial hypertrophy:
• A P wave in lead II taller then 2.5 mm (2.5 small squares)
• The P wave is usually pointed

P WAVE ABNORMALITIESP WAVE ABNORMALITIES
Left atrial abnormality (dilatation or hypertrophy):
• M shaped P wave in lead II
• Prominent terminal negative component to P wave in lead V1

P WAVE ABNORMALITIESP WAVE ABNORMALITIES
Premature Atrial Complex (PAC):• An abnormal P wave (arrowed in figure below)
• As P waves are small and rather shapeless, the difference in a PAC is usually subtle; the one shown here is a clear example
• Occurs earlier than expected
• Followed by a compensatory pause - but not a full compensatory pause
P WAVE ABNORMALITIESP WAVE ABNORMALITIES
Hyperkalemia:• The following changes may be seen in hyperkalemia
- Small or absent P waves
- Atrial fibrillation
- Wide QRS
- Shortened or absent ST segment
- Wide, tall and tented T waves
- Ventricular fibrillation
P WAVE ABNORMALITIESP WAVE ABNORMALITIES
Arrhythmias (will cover later):
• Premature atrial complex (PAC)
• Atrial flutter
• Atrial fibrillation
• Paroxysmal reentrant tachycardia (SVT)
• Multifocal atrial tachycardia
PR INTERVALPR INTERVAL
Normal PR interval:
• 0.12 to 0.20 s (3 - 5 small squares)

PR INTERVAL ABNORMALITIESPR INTERVAL ABNORMALITIES
Shorter PR interval:
• Wolf-Parkinson-White syndrome- Short PR interval, less than 3 small squares (120 ms)
- Slurred upstroke to the QRS indicating pre-excitation (delta wave)
- Broad QRS
- Secondary ST and T wave changes
PR INTERVAL ABNORMALITIESPR INTERVAL ABNORMALITIES
Long PR interval (will cover later):
• AV blocks

QRS COMPLEXQRS COMPLEX
• QRS Axis
• Normal duration of complex is < 0.12 s (3 small squares)
• NO pathological Q waves
• NO left or right ventricular hypertrophy
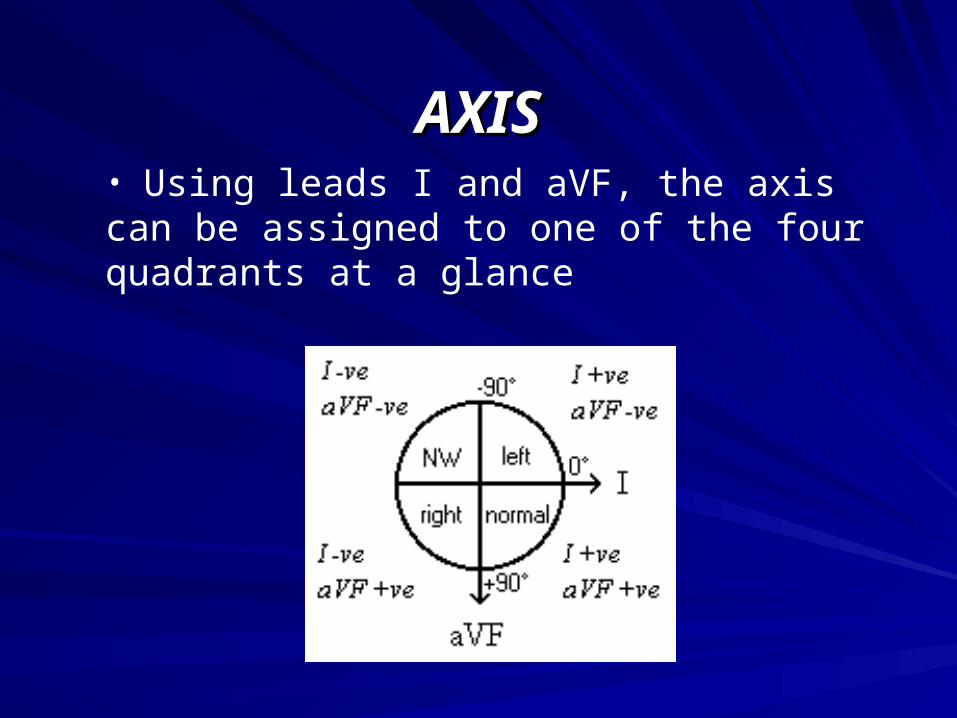
AXISAXIS• Using leads I and aVF, the axis can be assigned to one of the four quadrants at a glance
AXIS - NORMALAXIS - NORMAL
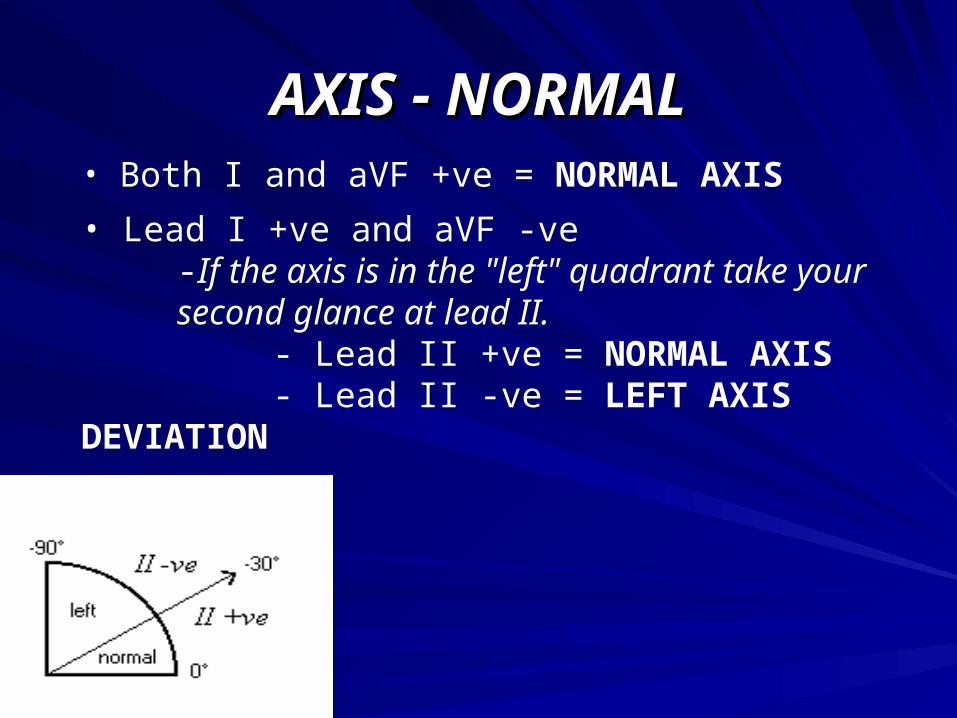
• Both I and aVF +ve = NORMAL AXIS
• Lead I +ve and aVF -ve -If the axis is in the "left" quadrant take your
second glance at lead II. - Lead II +ve = NORMAL AXIS- Lead II -ve = LEFT AXIS DEVIATION
AXIS - LEFT AXIS DEVIATIONAXIS - LEFT AXIS DEVIATION Left anterior hemiblock Left ventricular hypertrophy Q waves of inferior myocardial infarction Artificial cardiac pacing Emphysema Hyperkalemia Wolff-Parkinson-White syndrome - right sided accessory pathway Tricuspid atresia Ostium primum ASD Injection of contrast into left coronary artery
AXIS - NORTHWEST TERRITORYAXIS - NORTHWEST TERRITORY
• Both I and aVF -ve = axis in the NORTHWEST TERRITORY
• Causes of “No man’s land”
- Emphysema
- Hyperkalemia
- Lead transposition
- Artificial cardiac pacing
- Ventricular tachycardia

AXIS - RIGHT AXIS DEVIATIONAXIS - RIGHT AXIS DEVIATION
• Lead I -ve and aVF +ve = RIGHT AXIS DEVIATION• Causes:
- Normal finding in children and tall thin adults - Right ventricular hypertrophy - Chronic lung disease even without pulmonary
hypertension - Anterolateral myocardial infarction - Left posterior hemiblock - Pulmonary embolus - Wolff-Parkinson-White syndrome - left sided accessory pathway - Atrial septal defect - Ventricular septal defect

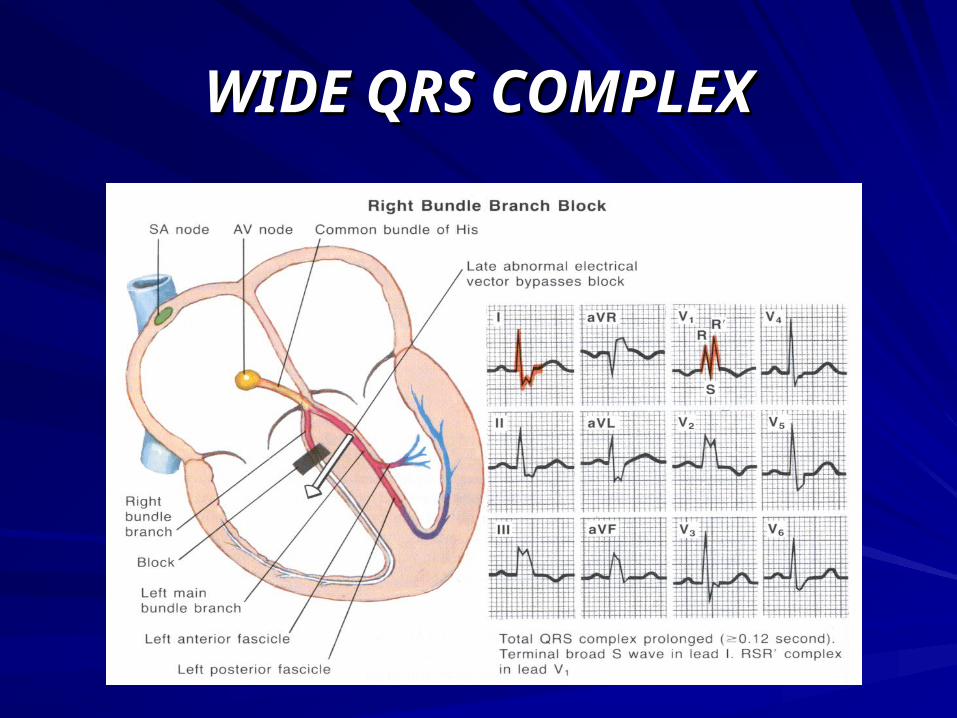
WIDE QRS COMPLEXWIDE QRS COMPLEX
Right Bundle Branch Block:• Wide QRS, more than 120 ms (3 small squares)
• Secondary R wave in lead V1 (RSR)
•Other features include slurred S wave in lateral leads and T wave changes in the septal leads
WIDE QRS COMPLEXWIDE QRS COMPLEX
WIDE QRS COMPLEXWIDE QRS COMPLEX
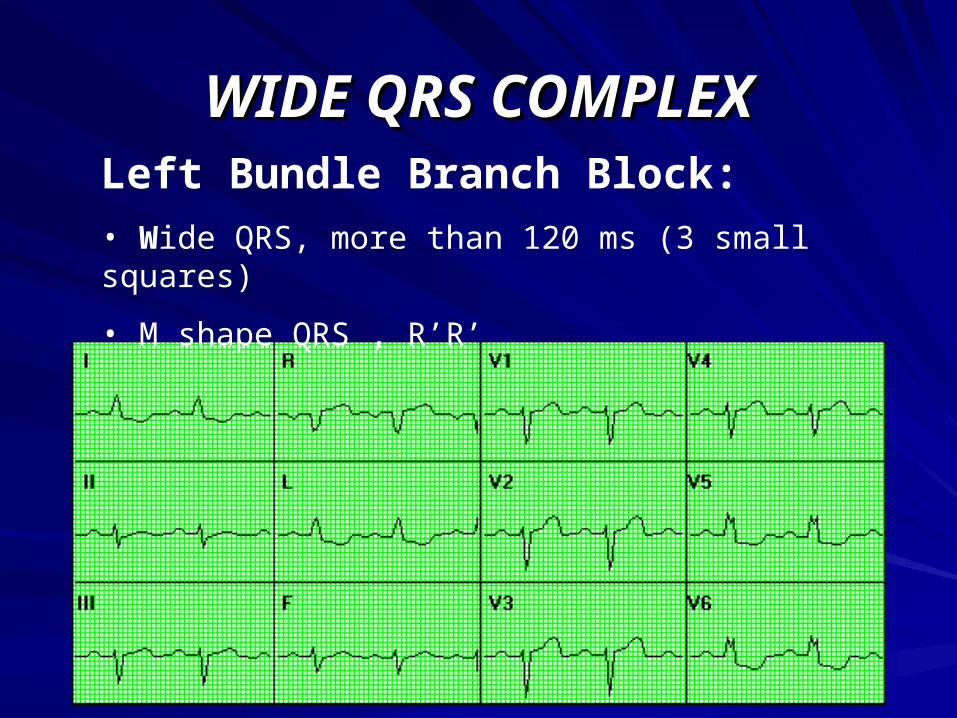
Left Bundle Branch Block:• Wide QRS, more than 120 ms (3 small squares)
• M shape QRS , R’R’
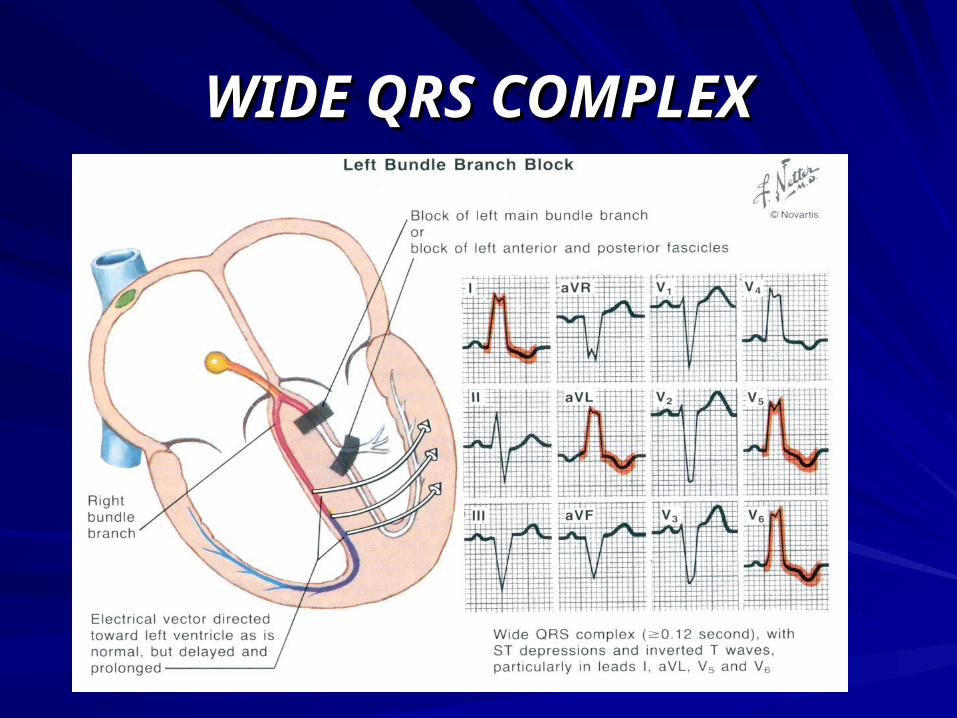
WIDE QRS COMPLEXWIDE QRS COMPLEX
WIDE QRSWIDE QRS
- Small or absent P waves
- Atrial fibrillation
- Wide QRS
- Shortened or absent ST segment
- Wide, tall and tented T waves
- Ventricular fibrillation
Hyperkalemia:• Changes that can be seen:

WIDE QRSWIDE QRS
Ventricular rhythm (will cover later):
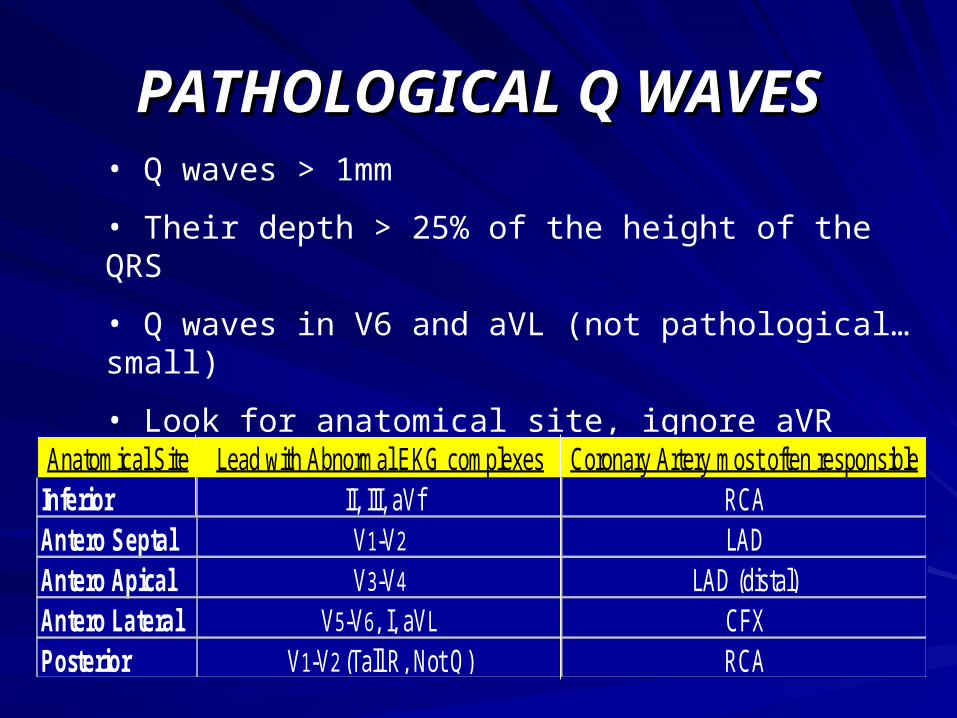
PATHOLOGICAL Q WAVESPATHOLOGICAL Q WAVES
• Q waves > 1mm
• Their depth > 25% of the height of the QRS
• Q waves in V6 and aVL (not pathological…small)
• Look for anatomical site, ignore aVR
Anatomical Site Lead with Abnormal EKG complexes Coronary Artery most often responsibleInferior II, III, aVf RCAAntero Septal V1-V2 LADAntero Apical V3-V4 LAD (distal)Antero Lateral V5-V6, I, aVL CFXPosterior V1-V2 (Tall R, Not Q) RCA

PATHOLOGICAL Q WAVESPATHOLOGICAL Q WAVES
NON Q WAVE MINON Q WAVE MI
• Not all MIs develop Q waves (up to 1/3 never do or they develop and resolve)
• WHY?• Infarct was not complete (transmural)• Infarct occurred in a electrically “silent” area of the heart, where an EKG cannot record the injury• Acute Infarct (Q waves will eventually appear)
RIGHT VENTRICULAR RIGHT VENTRICULAR HYPERTROPHY (RVH)HYPERTROPHY (RVH)
• Right axis deviation
• Deep S waves in the lateral leads
• A dominant R wave in lead V1
LEFT VENTRICULAR LEFT VENTRICULAR HYPERTROPHY (LVH)HYPERTROPHY (LVH)
Sokolow + Lyon (Am Heart J, 1949;37:161)
S in V1+ R in V5 or V6 > 35 mm
Cornell criteria (Circulation, 1987;3: 565-72)
S in V3 + R in aVL > 28 mm in men
S in V3 + R in aVL > 20 mm in women
Framingham criteria (Circulation,1990; 81:815-820)
R in aVL > 11mm, R in V4-6 > 25mm
S in V1-3 > 25 mm,
S in V1 or V2 + R in V5 or V6 > 35 mm,
R in I + S in III > 25 mm
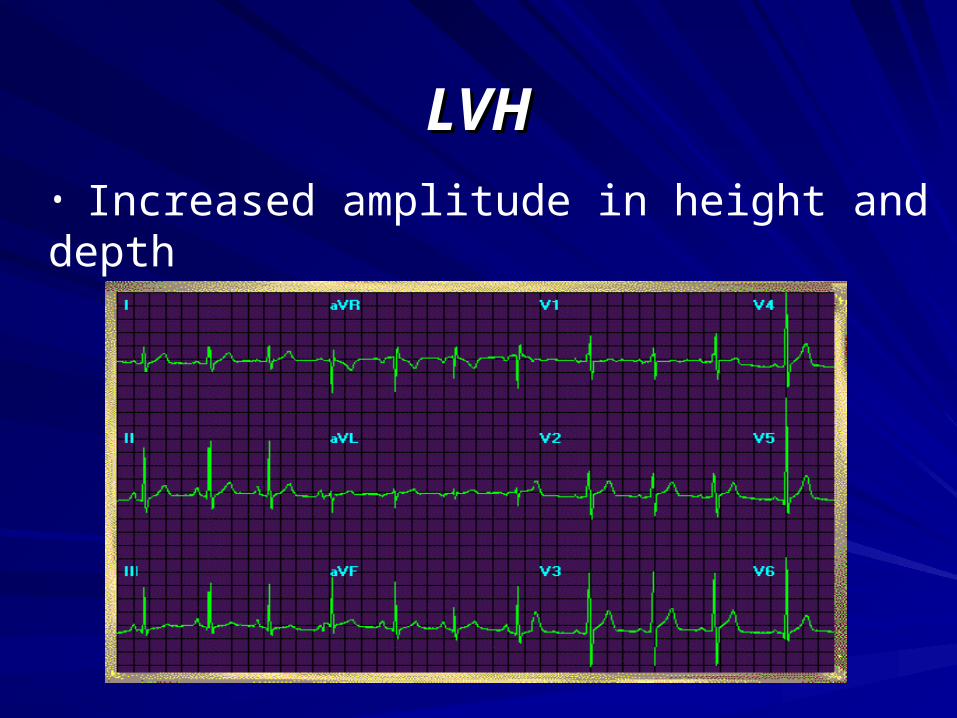
LVHLVH
• Increased amplitude in height and depth
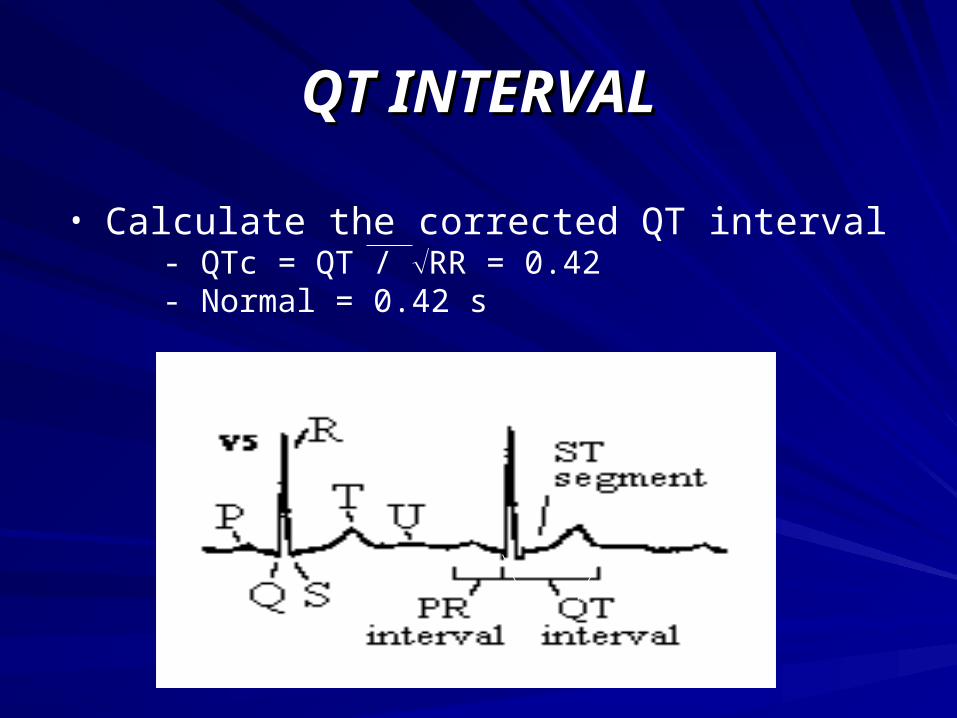
QT INTERVALQT INTERVAL
• Calculate the corrected QT interval - QTc = QT / RR = 0.42- Normal = 0.42 s

LONG QT INTERVALLONG QT INTERVAL
Causes:• Myocardial infarction, myocarditis, diffuse myocardial disease
• Hypocalcemia, Hypercalcemia (Short QT), hypothyrodism
• Subarachnoid hemorrhage, intracerebral hemorrhage
• Drugs (e.g. Sotalol, Amiodarone)
• Heredity
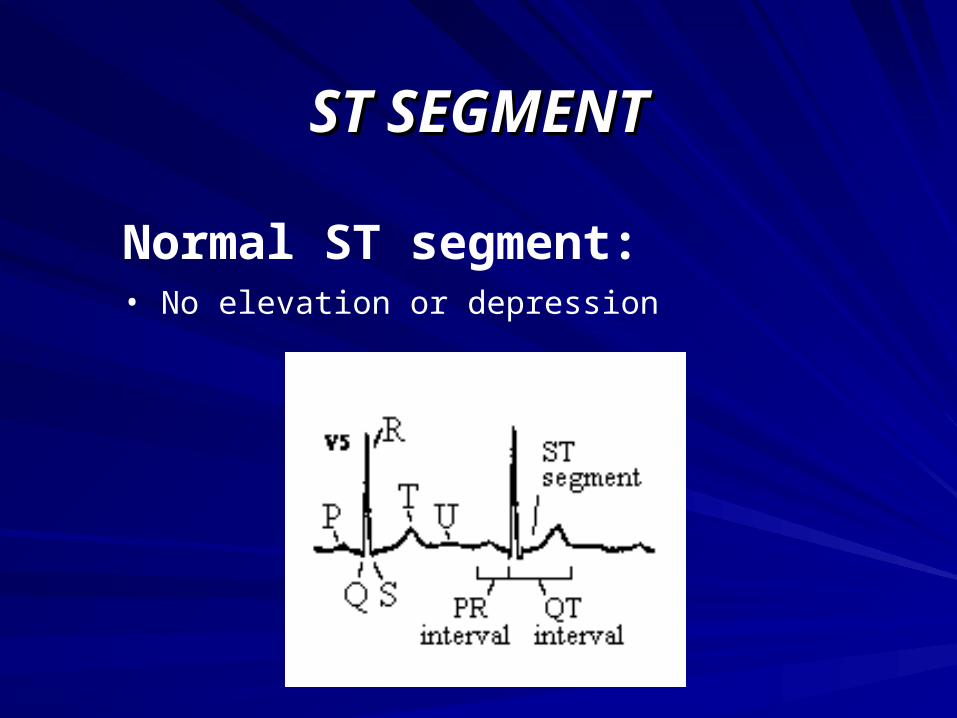
ST SEGMENTST SEGMENT
Normal ST segment:• No elevation or depression
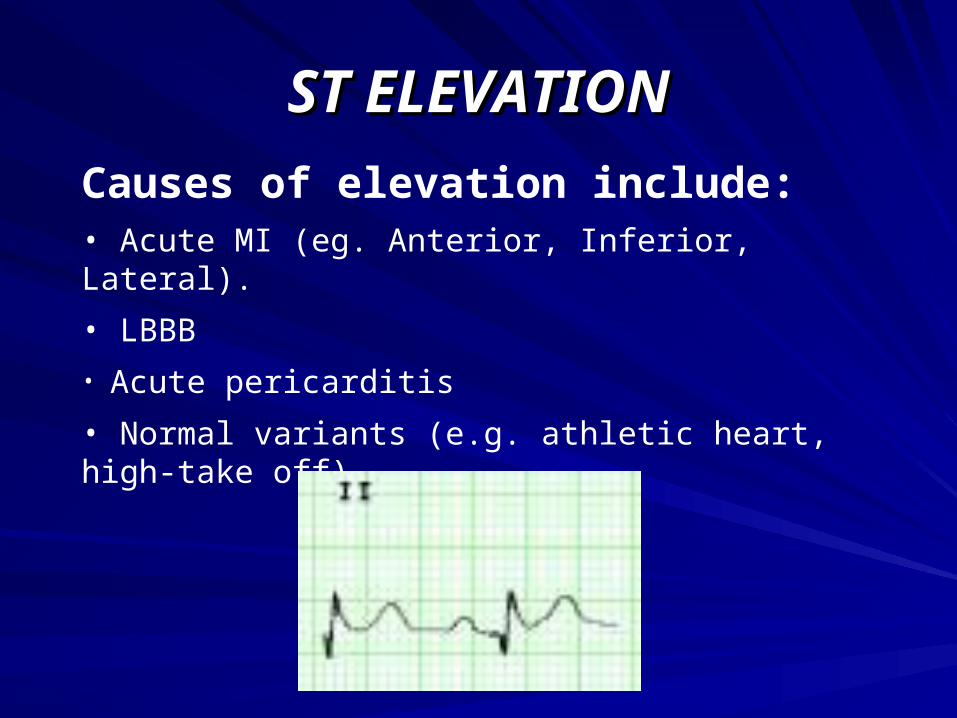
ST ELEVATIONST ELEVATION
Causes of elevation include:• Acute MI (eg. Anterior, Inferior, Lateral).
• LBBB
• Acute pericarditis
• Normal variants (e.g. athletic heart, high-take off),
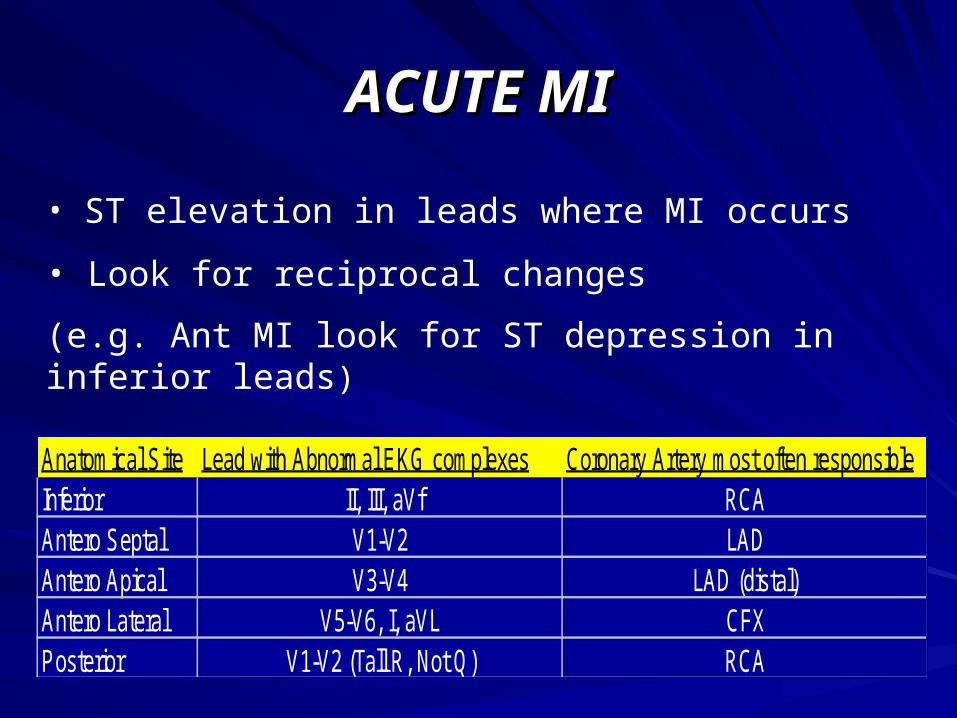
ACUTE MIACUTE MI
• ST elevation in leads where MI occurs
• Look for reciprocal changes
(e.g. Ant MI look for ST depression in inferior leads)
Anatomical Site Lead with Abnormal EKG complexes Coronary Artery most often responsibleInferior II, III, aVf RCAAntero Septal V1-V2 LADAntero Apical V3-V4 LAD (distal)Antero Lateral V5-V6, I, aVL CFXPosterior V1-V2 (Tall R, Not Q) RCA

LOCATING THE DAMAGELOCATING THE DAMAGE
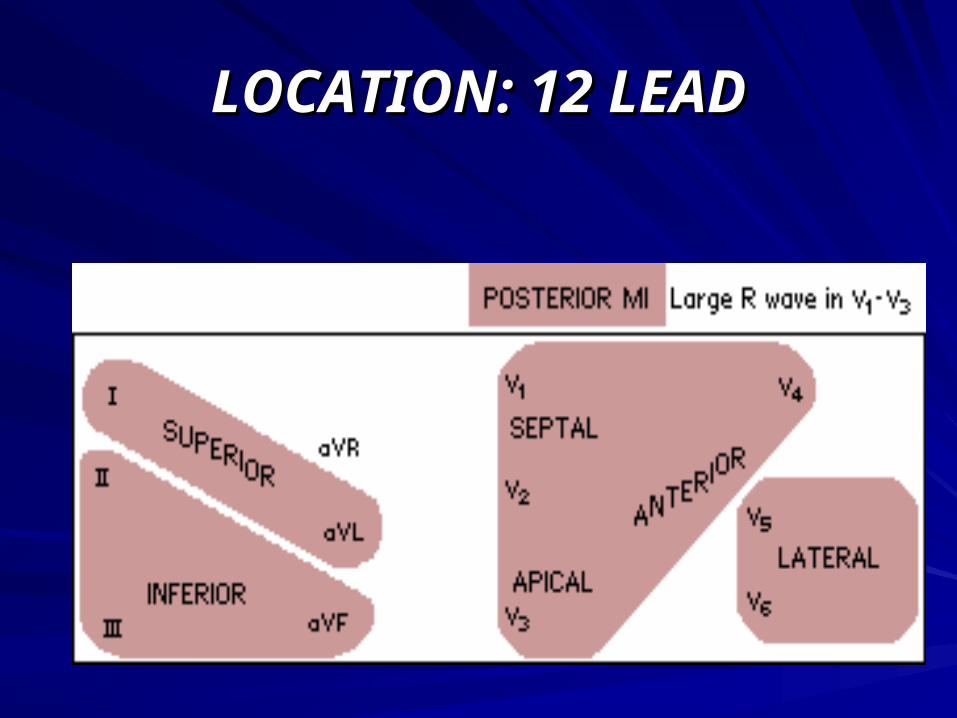
LOCATION: 12 LEADLOCATION: 12 LEAD
ST DEPRESSIONST DEPRESSION
Causes of depression include: • Myocardial ischemia
• Digoxin Effect
• Ventricular Hypertrophy
• Acute Posterior MI
• Pulmonary Embolus
• LBBB
DIGOXIN EFFECTDIGOXIN EFFECT
• Shortened QT interval• Characteristic down-sloping ST depression• Dysrhythmias
- Ventricular / atrial premature beats - PAT (paroxysmal atrial tachycardia) with variable AV block - Ventricular tachycardia and fibrillation - Many others
ACUTE POSTERIOR MIACUTE POSTERIOR MI
• The mirror image of acute injury in leads V1 - 3 • (Fully evolved) tall R wave, tall upright T wave in leads V1 -V3 • Usually associated with inferior and/or lateral wall MI
Mirror Test: Once you have determined an inferior (or other) MI has occurred, you begin looking for reciprocal changes. If there is ST depression in V1, V2, and V3, flip the EKG over and hold it up to the
light. Now read those leads flipped over. Are there significant Q waves? Is the ST segment elevated with a coved appearance? Are the T waves inverted? Answering yes tells you, there is a posterior infarct as well.

ST DEPRESSIONST DEPRESSION
In diagnosis with ischemia:• Looking for at least 1mm (1 square)
• This can be
1. Upsloping
2. Horizontal (can be combined w/ 1 or 3)
3. Downsloping
T WAVEST WAVES
• Repolarization of the ventricles is signaled by the T wave
TALL T WAVESTALL T WAVES
Causes:• Hyperkalemia
• Hyperacute MI
• LBBB

SMALL, FLATTENED OR SMALL, FLATTENED OR INVERTED T WAVES INVERTED T WAVES
Causes are plenty:• Ischemia, age, race, hyperventilation, anxiety
• LVH, drugs, pericarditis, I-V conduction delay (RBBB),
• Electrolyte disturbances
• The most important thing to consider is INVERTED T waves associated with Ischemia
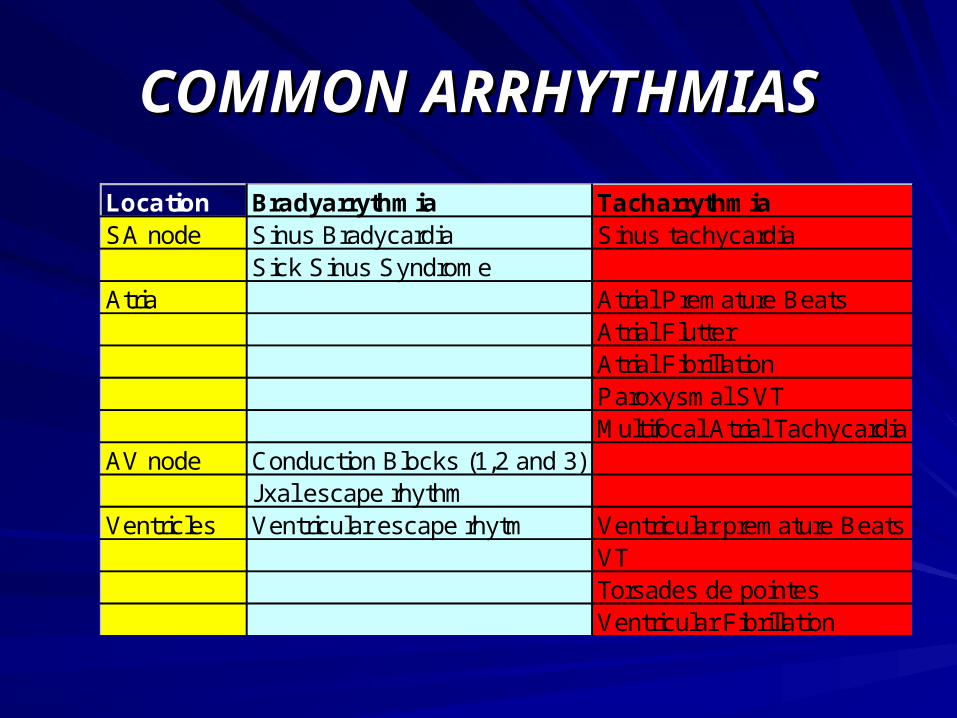
COMMON ARRHYTHMIASCOMMON ARRHYTHMIAS
Location Bradyarrythmia TacharrythmiaSA node Sinus Bradycardia Sinus tachycardia
Sick Sinus SyndromeAtria Atrial Premature Beats
Atrial FlutterAtrial FibrillationParoxysmal SVTMultifocal Atrial Tachycardia
AV node Conduction Blocks (1,2 and 3)Jxal escape rhythm
Ventricles Ventricular escape rhytm Ventricular premature BeatsVTTorsades de pointesVentricular Fibrillation
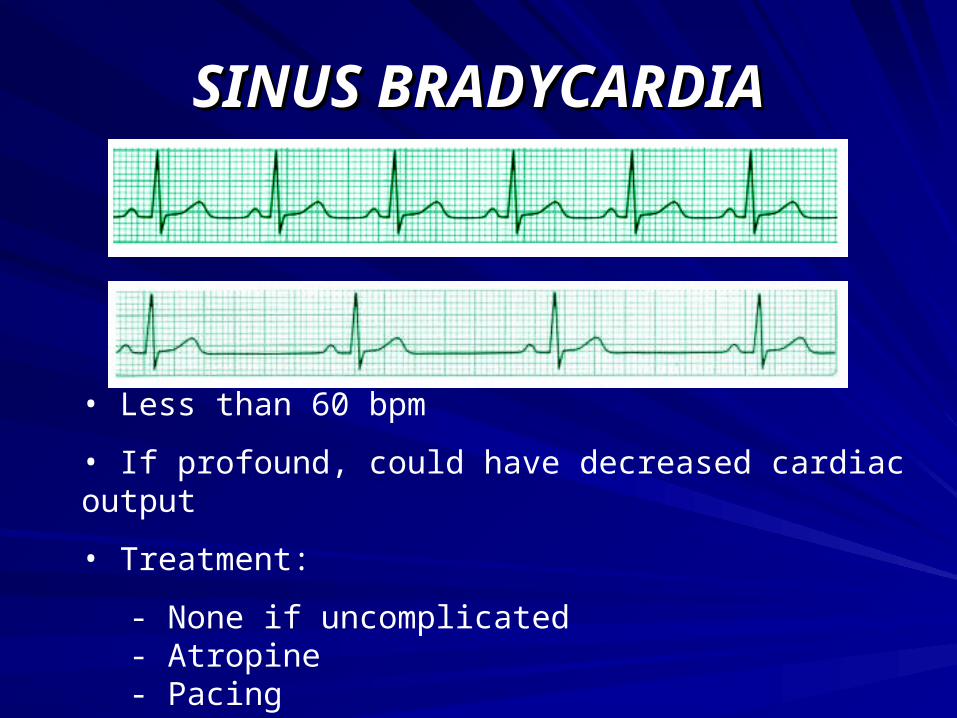
SINUS BRADYCARDIASINUS BRADYCARDIA
• Less than 60 bpm
• If profound, could have decreased cardiac output
• Treatment:
- None if uncomplicated- Atropine- Pacing

SINUS TACHYCARDIASINUS TACHYCARDIA
• Greater than 100 bpm
• Myocardial oxygen demand and may coronary artery perfusion resulting in angina in CAD
• Decreased cardiac output could be exhibited
SSS (SICK SINUS SYNDROME)SSS (SICK SINUS SYNDROME)
• Deceased cardiac output, related to periods of excessive bradycardia, AV block and/or tachycardia
• Treatment:
- Pacemaker- Anti coagulation therapy

ATRIAL PREMATURE BEATATRIAL PREMATURE BEAT
• Can be in a healthy heart or with CAD
• They are well tolerated because cardiac output is not altered
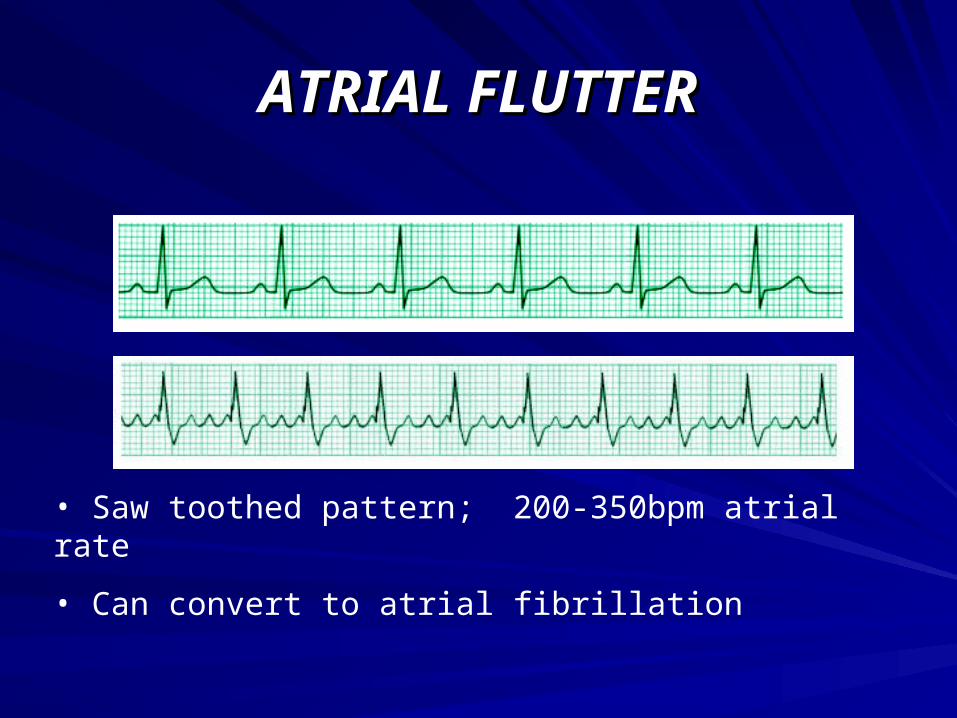
ATRIAL FLUTTERATRIAL FLUTTER
• Saw toothed pattern; 200-350bpm atrial rate
• Can convert to atrial fibrillation
ATRIAL FLUTTER (CONT’D)ATRIAL FLUTTER (CONT’D)
• People can feel flutter sensation… if short lived then no complication; however, with an increased ventricular rate, people can experience decreased cardiac output.
• Treatment:
- Veramapril, vagal stimulation - Digoxin (perhaps in combo with other drugs) - Cardioversion or pacing
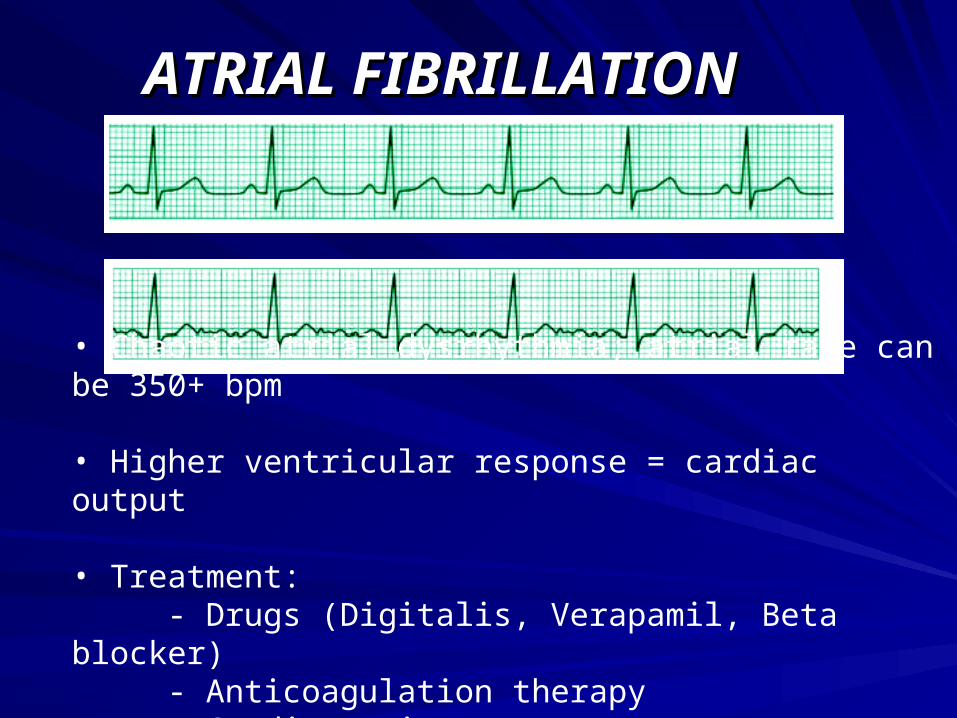
ATRIAL FIBRILLATIONATRIAL FIBRILLATION
• Chaotic atrial dysrhythmia; atrial rate can be 350+ bpm
• Higher ventricular response = cardiac output
• Treatment: - Drugs (Digitalis, Verapamil, Beta blocker) - Anticoagulation therapy - Cardioversion
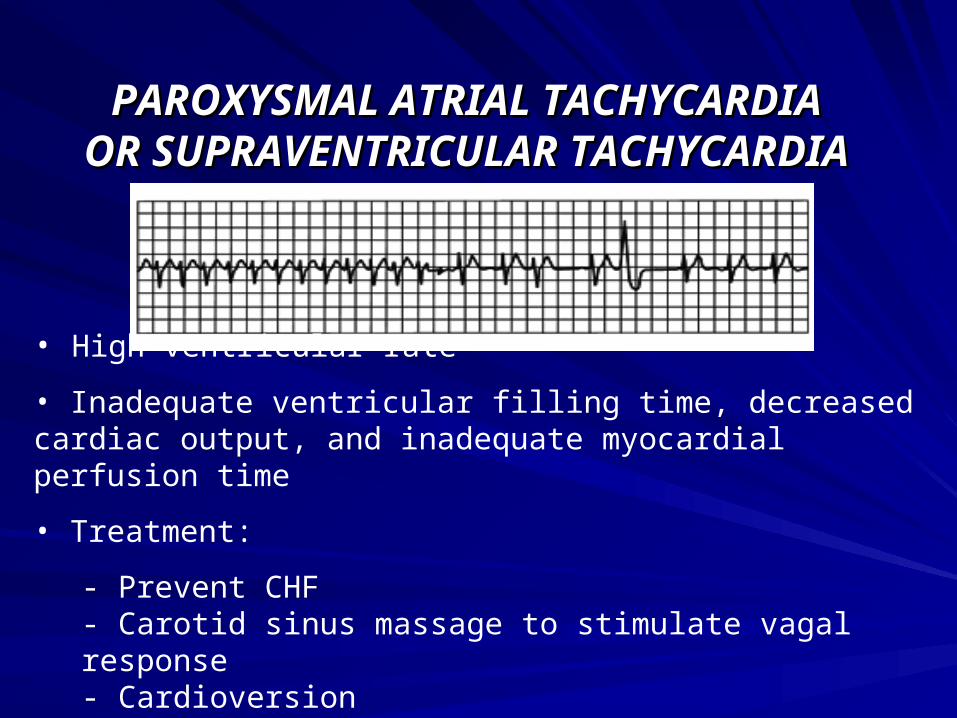
PAROXYSMAL ATRIAL TACHYCARDIAPAROXYSMAL ATRIAL TACHYCARDIAOR SUPRAVENTRICULAR TACHYCARDIAOR SUPRAVENTRICULAR TACHYCARDIA
• High ventricular rate
• Inadequate ventricular filling time, decreased cardiac output, and inadequate myocardial perfusion time
• Treatment:
- Prevent CHF- Carotid sinus massage to stimulate vagal response - Cardioversion- Drugs (Verapamil, Propranolol, and Digoxin)
MULTIFOCAL ATRIAL TACHYCARDIAMULTIFOCAL ATRIAL TACHYCARDIA• Irregular rhythm with multiple (at least 3) P wave morphologies in same lead with an irregular and usually rapid ventricular response.
• Pulmonary disease, hypoxia.
• Rate is greater than 100 bpm.
• Treatment:
- Verapamil - Resolve causative disorder
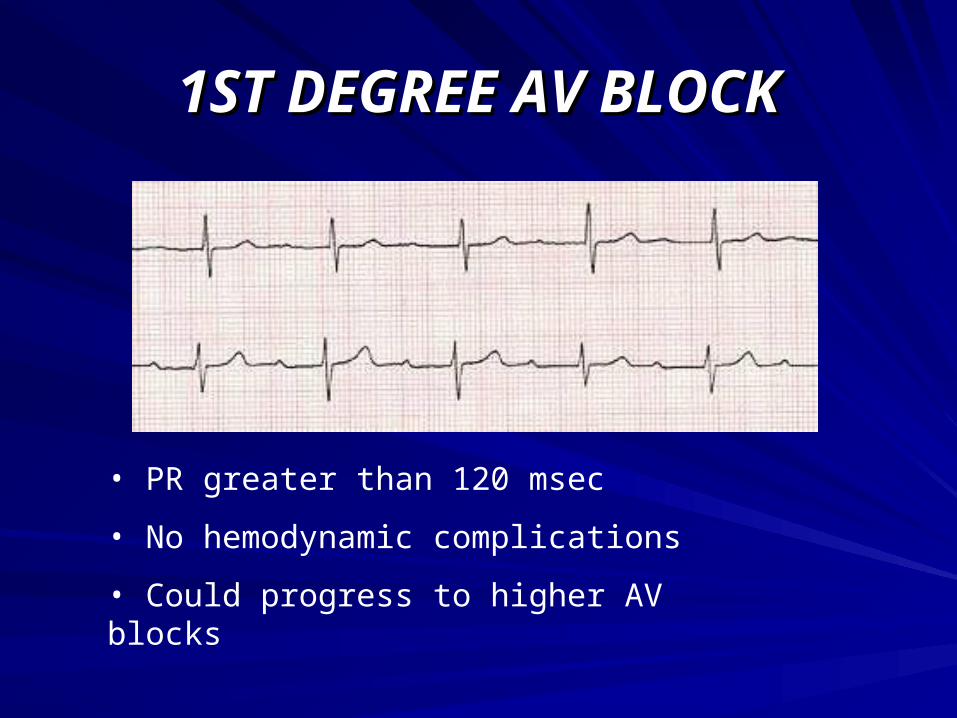
1ST DEGREE AV BLOCK1ST DEGREE AV BLOCK
• PR greater than 120 msec
• No hemodynamic complications
• Could progress to higher AV blocks

2ND DEGREE AV BLOCK 2ND DEGREE AV BLOCK MOBITZ TYPE 1 MOBITZ TYPE 1 (WENCKEBACH)(WENCKEBACH)
• PR interval progressively lengthens with each beat until it is completely blocked• If bradycardic, could have decreased cardiac output • Treatment:
- Only if brady (Atropine)- Rare pacemaker

2ND DEGREE AV BLOCK 2ND DEGREE AV BLOCK MOBITZ TYPE 2MOBITZ TYPE 2
• Rare, occurs with large ant MI
• PR interval fixed and p waves occur in a regular ratio to QRS (atrial rate is regular) until conduction is blocked

• Symptoms of decreased cardiac output occur with slowing ventricular rate - Could progress to complete block
• Treatment:
- Atropine initially - Permanent pacemaker
2ND DEGREE AV BLOCK 2ND DEGREE AV BLOCK MOBITZ TYPE 2 (CONT’D)MOBITZ TYPE 2 (CONT’D)
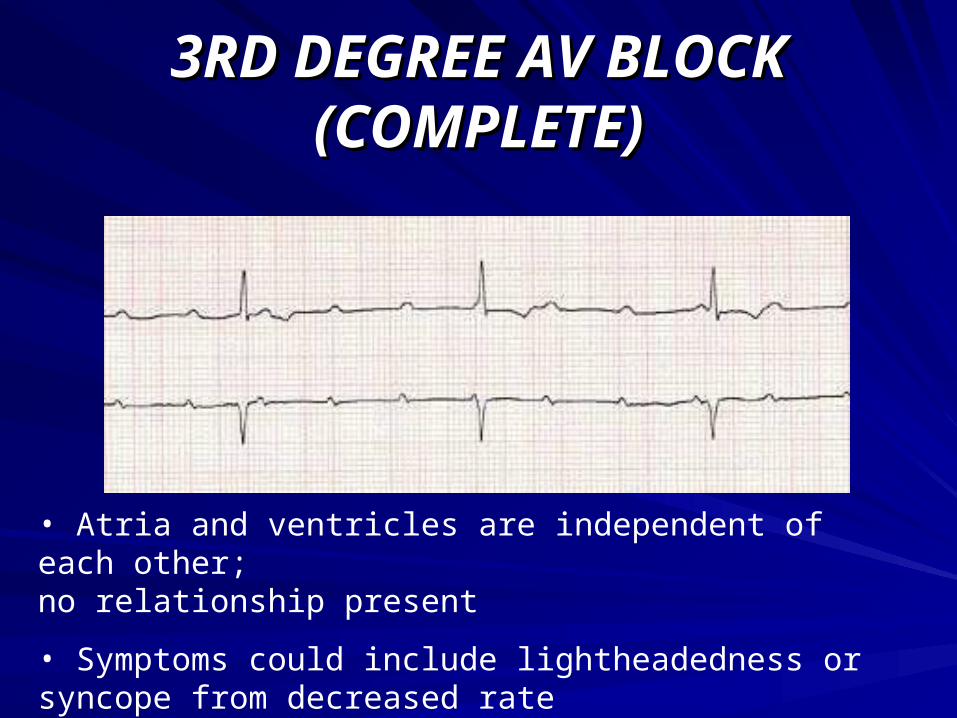
3RD DEGREE AV BLOCK 3RD DEGREE AV BLOCK (COMPLETE)(COMPLETE)
• Atria and ventricles are independent of each other; no relationship present
• Symptoms could include lightheadedness or syncope from decreased rate
3RD DEGREE AV BLOCK 3RD DEGREE AV BLOCK (COMPLETE) (CONT’D)(COMPLETE) (CONT’D)
• Decreased cardiac output, compromised coronary perfusion
• Treatment:
- Emergency
- Atropine
- Pacemaker
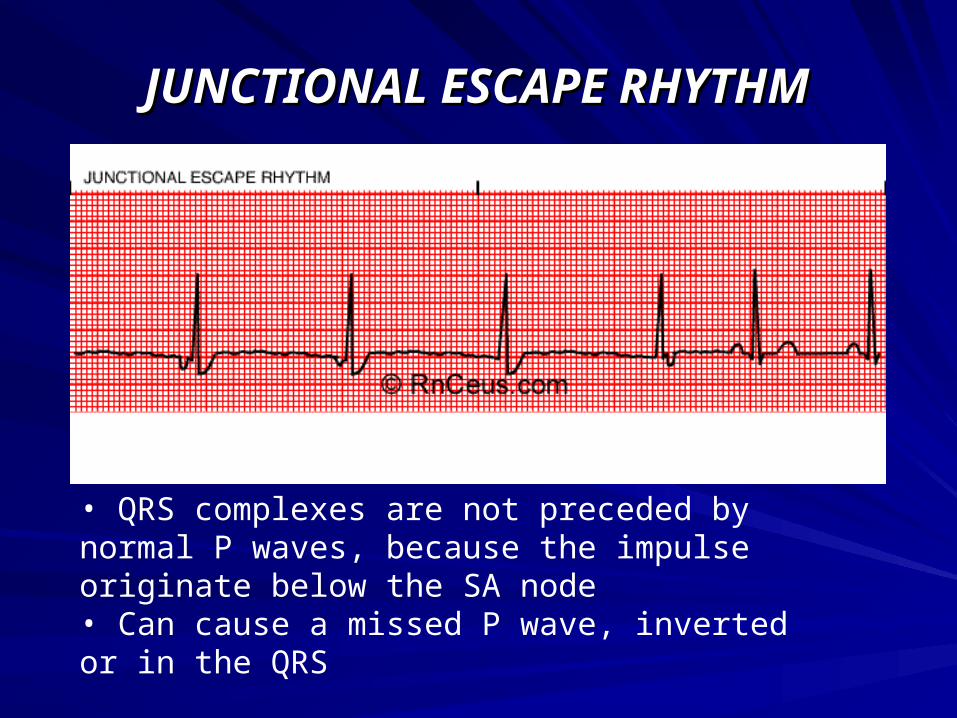
JUNCTIONAL ESCAPE RHYTHMJUNCTIONAL ESCAPE RHYTHM
• QRS complexes are not preceded by normal P waves, because the impulse originate below the SA node • Can cause a missed P wave, inverted or in the QRS

VENTRICULAR ESCAPE RHYTHMVENTRICULAR ESCAPE RHYTHM
• Wide QRS complex (> 120ms)
• Decreased cardiac output , lightheadedness and syncope due to decreased heart rate
• Treatment:
- Atropine
- Electronic pacemaker
PREMATURE VENTRICULAR PREMATURE VENTRICULAR CONTRACTION (PVC)CONTRACTION (PVC)
• Occasional PVC’s have minimal consequences
• Increased frequency or multifocal PVCs can lead to ventricular tachycardia
• Make sure it does not progress to more PVCs
• Couplet is 2 PVCs in a row
• Triplet is 3 PVCs in a row

VENTRICULAR BIGEMINYVENTRICULAR BIGEMINY
• Premature Ventricular contraction (PVC) in a bigeminal pattern
• Can be trigeminy (every third is a PVC), quadrigeminy
• Can be multifocal - increased irritability of the ventricle could lead to more severe dysrhythmia
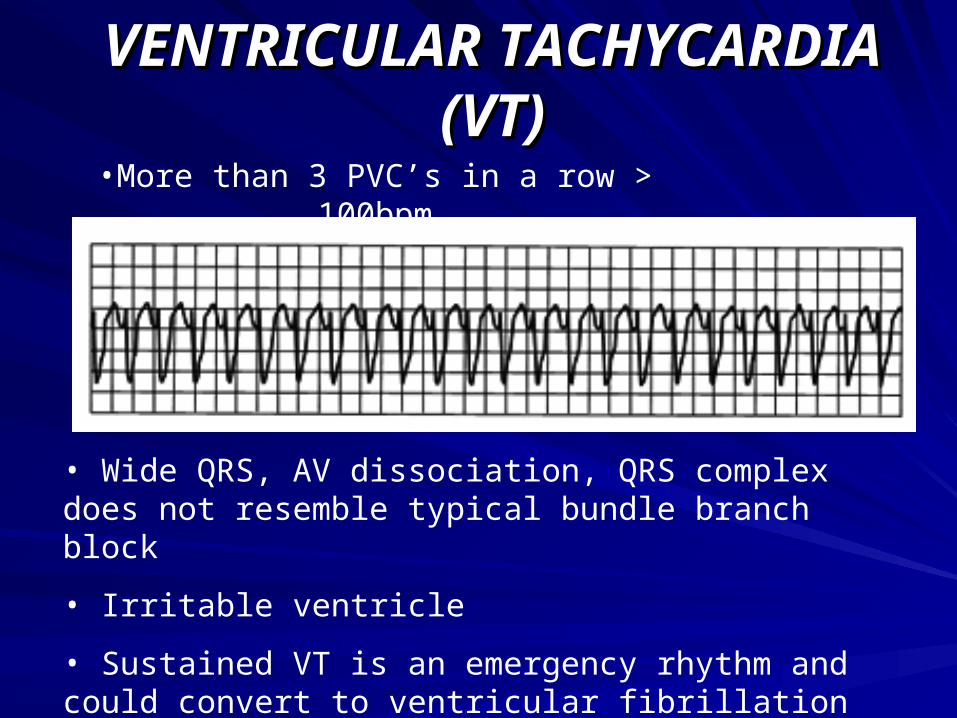
VENTRICULAR TACHYCARDIA VENTRICULAR TACHYCARDIA (VT)(VT)
•More than 3 PVC’s in a row > 100bpm
• Wide QRS, AV dissociation, QRS complex does not resemble typical bundle branch block
• Irritable ventricle
• Sustained VT is an emergency rhythm and could convert to ventricular fibrillation

VTVT
• Decreased cardiac output , irritable ventricle
• Treatment:
- Cardioversion - Lidocaine or Procainamide to get NSR - Emergent care - Long term care: ICD (implantable
cardioverter defibrillator)
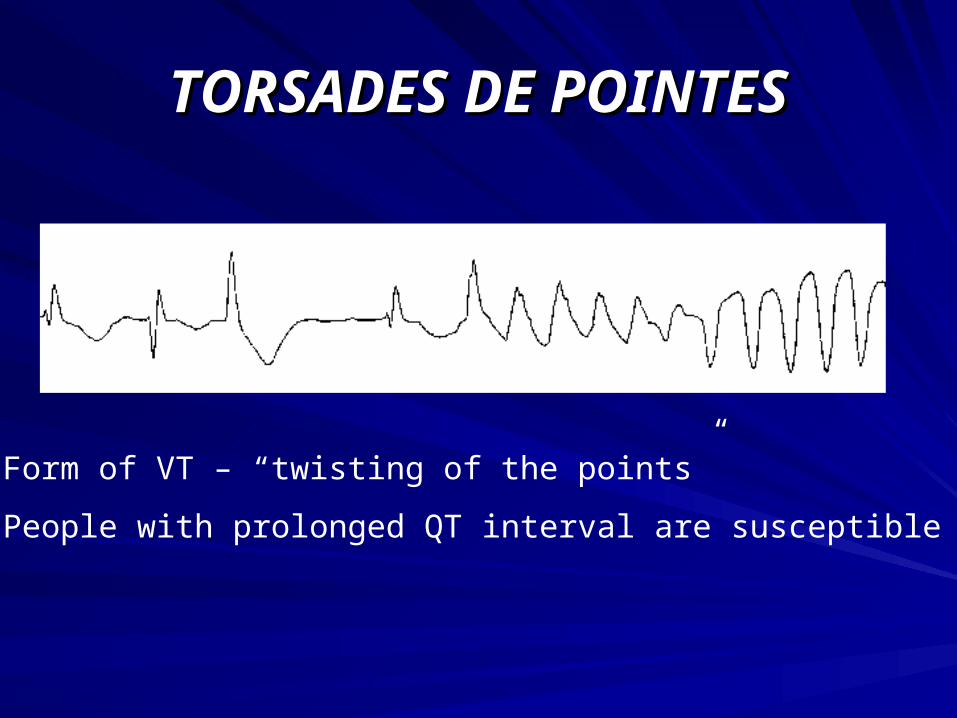
TORSADES DE POINTESTORSADES DE POINTES
• Form of VT – “twisting of the points”
• People with prolonged QT interval are susceptible
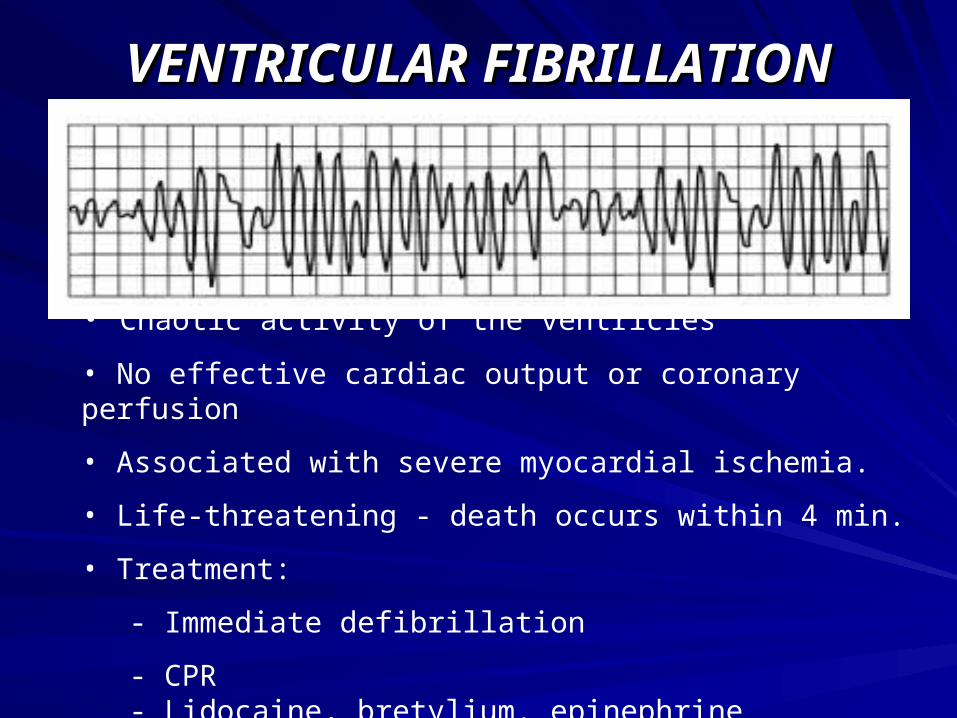
VENTRICULAR FIBRILLATIONVENTRICULAR FIBRILLATION
• Chaotic activity of the ventricles
• No effective cardiac output or coronary perfusion
• Associated with severe myocardial ischemia.
• Life-threatening - death occurs within 4 min.
• Treatment:
- Immediate defibrillation
- CPR- Lidocaine, bretylium. epinephrine

SINUS ARRESTSINUS ARREST

How to read the ECGHow to read the ECG– Look at the whole tracing.Look at the whole tracing.
Rhythm:Rhythm: Is there a P wave before each QRS complex? Is there a P wave before each QRS complex? − Yes: sinus rhythm No: AV junctional or heart blockYes: sinus rhythm No: AV junctional or heart block
RateRate: Count boxes; use caliper, ruler : Count boxes; use caliper, ruler PR intervalPR interval: Normal - 0.20 sec. or less : Normal - 0.20 sec. or less QRS complexQRS complex: Skinny (0.10 sec. or less) or broad (BBB or : Skinny (0.10 sec. or less) or broad (BBB or ventricular)ventricular)ST segmentST segment: Isoelectric (normal), elevated or depressed: Isoelectric (normal), elevated or depressedT waveT wave: Upright, flat or inverted: Upright, flat or inverted
InterpretationInterpretation: : NormalNormal or or abnormalabnormal. . − Is the rhythmIs the rhythm dangerous?dangerous?