Embed Size (px)
Citation preview
ELECTROCONVULSIVE THERAPY
ELECTROCONVULSIVE THERAPY
Jon Lehrmann MDAssistant Professor of PsychiatryMedical College of WIVAMC Milwaukee, WI
Mental Health Care Pre-1930’s
History of ECT
• Von Meduna (1934)- Autopsies of patients w/ Seizure disorders and of patients w/ Schizophrenia.
• Difference in Glial cell proliferation
Chemically induced seizures- (camphor, pentylenetetrazol)
Insulin Shock Therapy
• In the 1930’s , Dr Sakel developed Insulin Shock Therapy
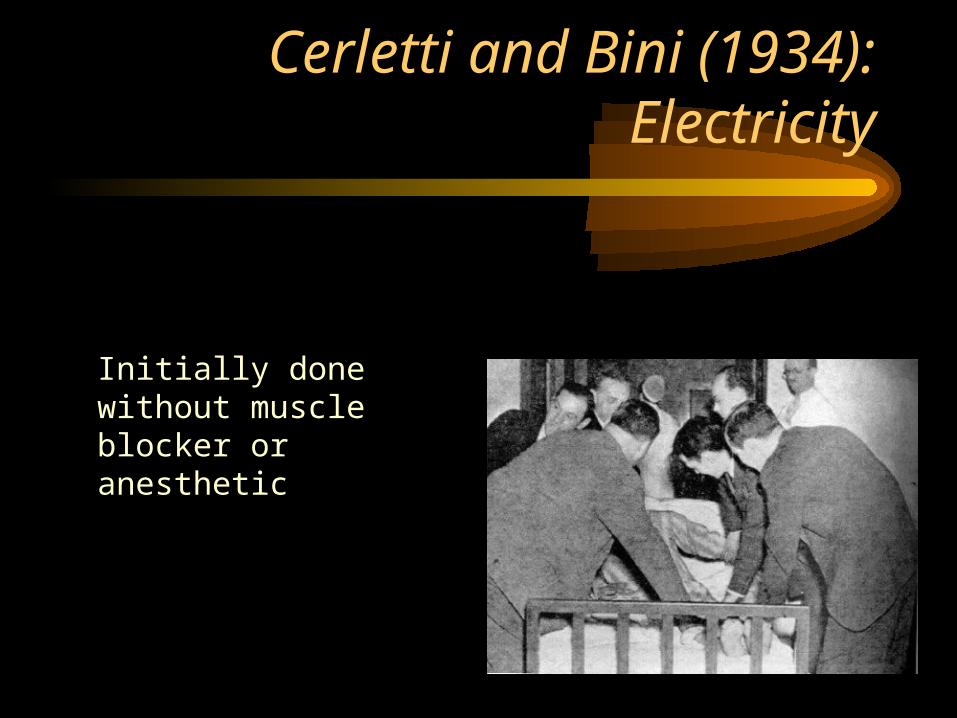
Cerletti and Bini (1934): Electricity
Initially done without muscle blocker or anesthetic
Early ECT
• Assylums• Few effective medications• Many often severe side effects• 1950’s- ether, and curare extract developed (Abram
Bennett- a psychiatrist helped develop a method for extracting curare).
• In 1950’s antidepressant and antipsychotic meds introduced- significantly decreased utilization of ECT
Electrophysiological Principles
• Ohm’s Law: I=E/R (I=current, E=voltage, and R=resistance)
• Dose of electricity in ECT= 100-500 milliCoulombs• Brain has low impedance (resistance), skull has
very high impedance. Only 20% of applied charge actually enters the brain.
• Seizure involves propagation of action potentials in a large percentage of neurons.
Mechanism of Action
• Neurotransmitter levels all increased in CSF after seizure. Results in down regulation of Beta adrenergic receptors.
• During seizure- PET studies show an increase in BBB permeability and in cerebral blood flow and metabolism.
• After seizure, blood flow and metabolism is decreased especially in the frontal lobes. Research shows this correlated w/ response.
Indications
• Major Depression w/ or w/o psychotic features
• Bipolar disorder - manic or depressed phase• Acute or Catatonic Schizophrenia• Some studies have shown efficacy in treating
OCD, Delirium, NMS, Chronic pain syndromes, and intractable seizure disorders
Major Depression
• Efficacy vs antidepressants• When is it a first line treatment
consideration?• Length of Antidepressant effect• Maintenance ECT
Bipolar Mania
• Efficacy vs Lithium• Indications for First Line Treatment:• -Recent Myocardial Infarction w/ Acute Mania• -Pregnancy w/ Acute mania
Pre ECT Workup
• Physical Exam• Head CT• CXR• CBC, Basic Chem• EKG• ? Spinal Films
Contraindications?
• No Absolute Contraindications• Relative Contraindications: Recent MI,
Berry Aneurysm, Brain Mass, Increased Intracranial Pressure
Treatments
• Premedicate w/ Glycopyrrolate, consider short acting Beta blocker
• Patient not intubated• Bite block• Cuff leg to monitor sz• EEG and EMG• Length of sz- 20 sec to 1 min.
Number and Spacing of ECT
• 2-3x/wk- efficacy vs less memory impairment
• 5-12 sessions/ treatment (although up to 20 is possible)
• Point of maximum improvement- no more improvement after 2 further treatments.
Adverse Effects
• Mortality rate: .002% per treatment session, .01% per patient.
• Sore Muscles• Head ache• Short term confusion/ delirium• Memory
Transcranial Magnetic Stimulation (TMS)
• Rt Frontal lobe- TMS pulses suppress activity and causes happiness and increased energy
• Left Frontal lobe- TMS pulses suppress activity and leads to sadness
• 4/250 had seizure• 10Hz stimulation 20x/day, 11/17 patients w/
Major Depression showed significant improvement.
TMS continued
• So far positive effects have not lasted as long as positive effects from ECT
• Handful of case reports show efficacy w/ anxiety disorders.





























